Embed Size (px)
Citation preview

Pédiatrie Dentistry
Effect of pulpotomies on eruption of succedaneous premolarsHannelore T, Loevy*/John G. Crawford**
The effect of a formocresol pulpotomy of a primary tooth on the eruption pattet-n ofthe suceedaneous tooth is an important cotisideration for long-range treattnent planning.This retrospective study evaluated the eruption pattern of permanent teeth using serialradiographs of children in whom a primary molar was tt-eated. The contralateral teethserved as controls. Twenty-seven children (14 boys and 13 girls) urtderweni a tmilatera!pulpotomy of a primary molar. In three cases, the contralateral tooth erupted earlierthan the sticcedaneous tooth: in tune cases, both teeth erupted at approximately thesame time: and in 15 cases, the succedaneous tooth erupted before the antimere.Differences among the groups were statistically significant.(Quintessence Int 1991:22:795-800.)
Introduction
Many genetic and environmental factors affect tootheruption, and accurate prediction of tooth develop-ment is an important consideration in planning long-range dental treatment for children. Among the en-vironmental factors that may affect eruption of per-manent teeth are tooth extraction, dental caries, andpulpal therapy of primary teeth. Disagreement existsabout the effect of pulpal therapy of primar>' teeth onthe eruption of the succedaneous tooth. Some inves-tigators have demonstrated an early eruption of thesuccedaneotjs tooth, while other investigators haveshown a delay in the eruption.
Because of the small number of patients in whompulpotomieK have been performed on one side only,leaving the other side as a control, investigations ofthis question have been limited. The purpose of thepresent study was to evaluate the time of eruption of
Professor Department of PediaTric Dentistry, UniverMty ofIllinois, College of Dennstry, 801 South Paulina Street, Chicago,Illinois 60612.Private Practice ¡tl Pédiatrie Dentistry and Orthodontics, 505North Ridgeland Avenue, Oak Park, Illinois 603Ü2.
maxillary and mandibular premolars following pul-potomies of the antecedents, using the eontralateralside as the control. Each individual was evaluated as aunit, and the eruption time on the pulp-treated sidewas compared to the eruption time of the other sidefor the calculation of tooth exchange interval. In thismanner, individual variations could be disregarded.
Review of the literature
The evaluation of symmetry in normal tooth eruptionhas been studied by several investigators, '̂̂ Few differ-ences were found in eruption patterns when right andleft sides were compared under normal conditions andwere studied longitudinally. In patients with prem-ature loss of primary teeth, however, different findingshave been described. In a group of 236 children, Loand Moyers^ concluded that children in whom no prim-ary teeth were extracted showed no statistically signif-icant difference in the eruption age between eontralat-eral permanent teeth. In patients in whom bone lossoccurred because of pathosis of the primary tooth,premature eruption of permanent teeth occasionallytook place, in 1946, MacGregor'' concluded that prem-olars erupt early in patients with periapical infectionin the area of the primary molar extraction. Adler^evaluated tooth eruption in a large number of childrenand also concluded that premature extraction of prim-
Quintessence International Volume 23, Number 10/1991 795
Pédiatrie Dentistry
ary molars exerts an accelerating effect on the erup-tion of the permanent siiecessor- On the other hand, ina study of 10 ehildren in whom a maxillary centrai in-eisor had heen lost prematurely and in whom the adjac-ent central incisor was allowed to exfohate normally,Korf'' found delayed eruption of the sueeedaneous cen-tral incisor on the affected side in nine cases.
Since its introduction in 1904, the formocresol pul-potomy' has been used with varying success by manyprofessionals. The prognosis of pulpotomy of primarymolars and the survival rate of these teeth have beenstudied by several investigators. However, the ques-tion of timing of tooth eruption of the permanentteeth needs ftirther evaluation.
In a longitudinal study, Lauterstein et al** found thatinfection and pulpotomy of the overlying primarytooth altered the eruption pattern of the succcdan-eous tooth. In their group of 28 children, the premolarunder the pulpotomy-treated tooth erupted faster thanthe contralateral did in 13 cases. In two cases, a delaywas noted. Five cases showed internal résorption ofthe primary molar, but individual differences betweensides were not indicated in their paper- In 1973. Star-key^ stated that, in his clinical experience, pulpectomyusing formocresol was an effective treatment, but theprimary molars so treated were overretained. Rifkin"^found .50% '•normal" résorption in a series of 45 cases,but did not compare the antimeres. He also describedthree overretained molars that required extraction,but did not explain the cases fully. Coll et al" studied37 children in whom nonvital primary molars receivedpulpectomies. In half of the cases, pulp-treated teethresorbed more rapidly than did non-pulp-treatedteeth, although in some cases the contralateral teethhad been extracted.
An increased rate of root résorption in pulpotomy-treated primary teeth has been demonstrated by sev-eral investigators. Hobson'- demonstrated a 6- to 12-month early exfohation and sueeedaneous replace-ment after pulpotomy. Morawa et al'"* also found intheir sample that pulpotomized molars generally werelost 6 to 12 months earlier than usual and that sue-eedaneous teeth erupted earlier. No statisticaldocumentation was provided for these findings. Fuksand Bimstein"* noted an increased rate of root résorp-tion in 16 of 41 cases but made no clear indication ofthe differenee in time between the two sides. Wrightand Widmer''' also found that, in their sample of 101cases, 64 pulpotomy-treated molars had one or moreroots with extensive résorption, while only 34 of theantimere teeth were in this condition. However, chi-
square analysis of the different rate of exfoliation didnot show a signifieant difference between the twosides. Van Amerongen et al"' analyzed the life span offormocresol pulpotomy-treated primary teeth, eval-uated as a group, and compared it to that of the anti-meres, also as a group. They concluded that there wasno signifieant difference in the life spans of primaryteeth with or without pulpotomy.
In an earlier paper, the effect of pulpotomies on thespeed of root résorption of primary teeth was dis-cussed." When pulpotomized teeth were used as con-trols, it was found that their accelerated résorptionand premature loss were statistically significant.
Method and materials
The data used in this retrospeetive study were ob-tained from the records of 5,000 patients of the privatepractice of one author (JGC). The sample consisted of14 boys and 13 girls for whom serial dental radio-graphs were available. Ail pulpotomies were performedby the same dentist. The pulps of all teeth evaluatedwere judged to be cariously exposed. Age at pul-potomy varied from 3.23 to 9.00 years. The medianage at time of pulpotomy was 6.42 years,
Buckleys original formulation^ was used (10% for-maldehyde, 35% cresol, and 15% glycerol). An al-most-dry cotton pellet was placed on the pulpal stumpand left in place for approximately 15 days. The cottonpellet was then removed and zinc oxide-eugenol wasplaced into the pulp chamber. The pulp-treated toothwas then appropriately restored.
To be selected, the patient's record had to indicatethe exact date of pulpotomy of the primary molar andalso inelude follow-up records until the time the sue-eedaneous tooth and its antimere had erupted. Tootheruption was defined as the time at which the radio-graph showed that the tooth had pierced the gingivaand could be seen in the oral cavity if the patient wereexamined.
Children who required extraction of either the pul-potomized tooth or its antimere at any time during theevaiuation period were excluded from this study. Onlycases of unilateral pulpotomy were used- Also, sincewhen one side of an arch requires pulpal therapy, theantimere often is pathologically affected, clear indica-tion of type and timing of treatment of the primaryantimere had to have been recorded. Because of thesecriteria, many charts were eliminated, and only 27eases could be selected. The sample selected is hstedin Table 1.
796 Quintessence International Volume 22, Number 10/1991
Pédiatrie Dentistry
The criteria used for fhe selection of the patients were:1. Presence of radiographs showing the carious expos-
ure2. Availabihty of postoperative radiographs of both
sides of the patient demonstrating the eruption pat-tern of the treated tooth and of its antimere
3. No pulpal therapy or extraction of the antimere.
Radiographs were examined for the condition of thetooth at the time of pulpotomy and the condition ofthe antimere. Eollow-up radiographs were evaluatedfor the development of the teeth, exfoliation of thepulpotomized tooth and its antimere, and eruption ofthe succedaneous teeth on both sides. The data wereanalyzed with the Kruskal-Wallis test."^
Resultii
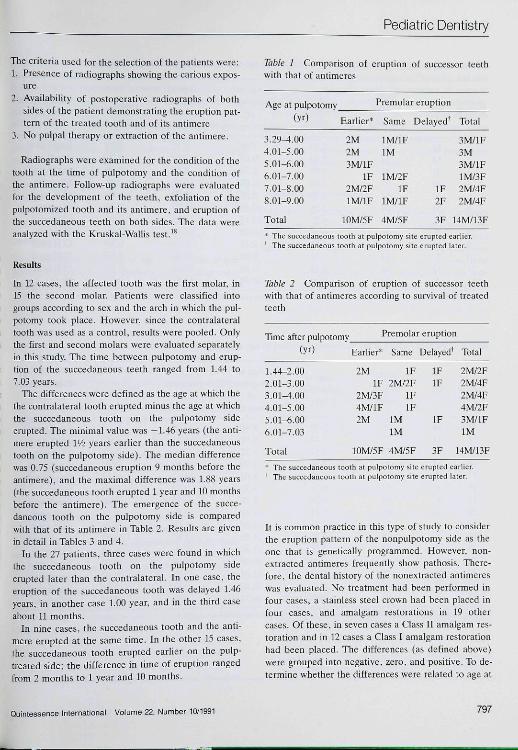
In 12 cases, the affected tooth was the first molar, in15 the second molar. Patients were classified intogroups according to sex and the arch in which the pul-potomy took place. However, since the contralateraltooth was used as a control, results were pooled. Onlythe first and second molars were evaluated separatelyin this study. The time between pulpotomy and erup-tion of fhe succedaneous teeth ranged from 1,44 to7.03 years.
The differences were defined as the age at which thethe contralateral tooth erupted minus the age at whichthe succedaneous tooth on the pulpotomy sideerupted. The minimal value was -1.46 years (the anti-mere erupted l'/2 years earlier than the succedaneoustooth on the pulpotomy side). The median differencewas 0.75 (succedaneous eruption 9 months before theantimere), and the maximal difference was 1.88 years(the succedaneous tooth erupted 1 year and 10 monthsbefore the antimere). The emergence of the succe-daneous tooth on the puipotomy side is comparedwith that of its antimere in Table 2. Results are givenin detail in Tables 3 and 4.
In the 27 patients, three cases were found in whichthe succedaneous tooth on the pulpotomy sideerupted later than the contralateral. In one case, theeruption of the succedaneous tooth was delayed 1.46years, in another case 1,00 year, and In the third caseabout 11 months.
In nine cases, the succedaneous tooth and the anti-mere erupted at the same time. In the other 15 cases,the succedaneous tooth erupted earlier on the pulp-treated side; the difference in time of eruption rangedfrom 2 months to 1 year and 10 months.
Table J Comparison of eruption of successor teethwith that of antimeres
Age at pulpotomy(yr)
3.29-4.004.01-5.005.01-6.006.01-7.007,01-8.008.01-9.00
Total
Earlier""
2M2M3M/1E
IF2M/2ElM/lF
I0M/5E
Premolar eruption
Same
lM/lFlM
1M/2FIF
lM/lF
4M/5F
Delayed^
IF2F
3F
Totai
3M/1F3M3M/1F1M/3F2M/4F2M/4F
14M/13F
* The suceedaneous tooth al pulpotomy site erupted eariier' The succedaneous tooth at pulpotomy siti: erupted later.
Table 2 Comparison of eruption of successor teethwith that of antimeres according to survival of treatedteeth
Time after pulpotomy(yr)
1.44-2.002.01-3.003.01-4.004.01-5.005.01-6.006.01-7.03
Total
Premolai
Earher*
2MIF
2M/3F4M/1F2M
10M/5F
Same
IF2M/2F
IFIF
IMlM
4M/5F
: eruptior
Delayed^
IFIF
IF
3F
1
Total
2M/2F2M/4F2M/4F4M/2F3M/1FlM
14M/13F
* The succedaneou5 tooth at pulpotumy sito erupted earlier.' The succedaneous tooth at pulpotomy site erupted later.
It is common practice in this type of study to considerthe eruption pattern of the nonpulpotomy side as tbeone that is genetically programmed. However, non-extracted antimeres frequently show pathosis. There-fore, the dental history of the nonextracted antimereswas evaluated. No treatment had been performed infour cases, a stainless steel crown had been placed infour cases, and amalgam restorations in 19 othercases. Of these, in seven cases a Class II amalgam res-toration and in 12 cases a Class I amalgam restorationhad been placed. The differences (as defined above)were grouped info negative, zero, and positive. To de-termine whether the differences were related to age at
Quintessence International Volume 22, Number 10/1991 797
Pédiatrie Dentistry
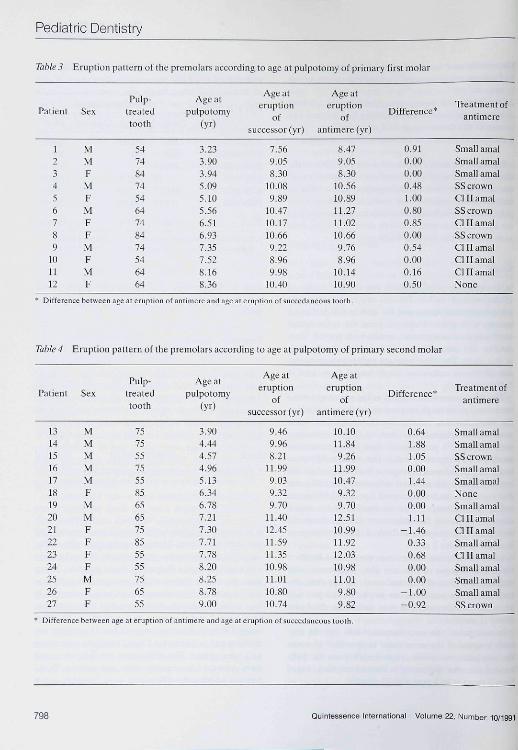
Table 3 Eruption pattern of the premolarsaccordingtoageat pulpotomy of primary first molar
Patient SexPulp-
treatedtooth
Age atpulpotomy
(yO
Age ateruption
ofsuccessor (yr)
Age ateruption
ofantimere (yr)
Difference"Treatment of
antimere
1234567S9
101112
MMFMFMFFMFMF
547484745464748474546464
3.233.9Ü3.945.095.105.566.516.937.357.528.168.36
7.569.058.30
10.Ü89.89
10.4710.1710.669.228.969.98
10.40
8.479.058.30
10.5610.8911.2711.0210.669.768.96
10.1410.90
0.910.000.000.481.000.800.850.000.540.000.160.50
Small am alSmall am alSmall amalSS crownCl II amalSS crownCl II amalSS crownCl II amalCl II amalCl II amalNone
Difference between age at eruption of antimere and age at eruption ofsuccedaneous tooth.
Table 4 Eruption pattern of the premolars according to age at pulpotomy of primary second molar
Patient
131415161718192021222324252627
Sex
MMMMMFMMFFFFMFF
Pulp-treated
tootti
757555755585656575855555756555
Age atpulpotomy
3.904.444.574.965.136.346.787.217.307.717.788.208.258.789.00
Age ateruption
oísuecessor(yr)
9.469.968.21
11.999.039.329.70
11.4012.4511.5911.3510.9811.0110.8010.74
Age ateruption
ofantimere (yr)
10.10n.849.26
11.9910.479.329.70
12.5110.9911.9212.0310.9811.019.809.82
Difference"'
0.641.881.050.001.440.000.00 -1.11
-1.460.330.680.000.00
-1.00-0.92
Treatment ofantimere
Small amalSmall amalSS crtjwnSmall amalSmall amalNoneSmall ama]Cl II amalCl II amalSmall amalCl 11 amalSmall amalSmall amalSmall amalSS erown
Difference between age at eruption of antimere and age at eruption of sucoedaneoiis tooth.
798 Quintessence International Volume 22, Number 10/1991

Pédiatrie Dentistry
pulpotomy. a Kruskal-Wallis test was performed. Inthis test, ratiks rather thati numerical results are used,A rank test was performed because the normality andvariance of the actual distribution could not be as-stimed. The analysis showed that there was a sig-nificant difference among ihc groups (P <.fl5). Inspec-tion of the data showed that the three negative differ-ences occurred when pulpolomies were performed inrelatively older children. To determine whether thedifferences were related to the time span between thepulpotomy and eruption of the succedaneous tooth, aKruskal-Wallis test was performed. There was a sig-nificant difference among the groups {P <.O5).
Discussion
There was great variation in age at the time of pul-potomy and considerable variation in the time of toothemergence among the children. However, each ind-ividual was used as a unit and the age of eruption ofthe antimere was used as a eontrol. Tn a study of 98primary molars. Rolling and Thylstrup''' demonstratedthat the survival rate of teeth treated with formocresolpulpotomy was 70% after 36 months. Since we ev-aluated only teeth that exfoliated naturally, our samplemay have been biased because any teeth that were ex-tracted early were removed from the original sample.
The survival rate of our cases varied from 1.44 to7.03 years, indicating good condition of the remainingpulpal tissue as well as the periodontal tissues.
The three cases in which the pulpal treatment ex-tended the life of the Ireated tooth beyond that of theantimere were found among the patients who weretreated at an older age (7.30, ii.78. and 9.00 years).All of these teeth were primary second molars. Theteeth were retained longer by 11 months. 1 year, and1!̂ years.
The sample is too small for definite conclusions;however, among the children who had primary secondmolars treated, there were comparable ages at treat-ment and at eruption of the permanent teeth. In twopatients, the antimere control leeth erupted at theages of 9,80 and 9,82 years, and one case at almost 11years. In the other instances of second molar treat-ment, both successors erupted at the same time in fivecases; the age of eruption varied from 9.32 to 11.99years. Of the cases in which the pulpototny-treatedtooth was lost eariy, the age of eruption of the anti-mere successors varied from 9,26 to 12.03 years. Therewas a small difference in the average eruption age ofthe teeth in which both antimeres erupted at the same
time (10,60 years) and thai of the eases in which the anti-meres erupted at different times (1!,17 years), but thisdifference is relatively small. The number of cases ineach instance is too small to allow statistical evaluation.
It is possible that the age factor that has to be takeninto consideration will be better understood whenlarger samples are collected and analyzed. In general,it musl be concluded thai in many cases pulpotomywill not accelerate tooth exchange.
Summary and conclusion.s
The effect at diffeient ages of pulpotomy of a primarymolar on the development of the succedaneous pre-molar was studied utilizing the tooth on the untreatedside as the control. Eruption of the succedaneoustooth can take place earlier than, at the same timeas, or later than the anlimere, depending on the indi-vidual characteristics of the patient. In comparativestudies in which the antimere is used as a eontrol, thetreatment history of the control tooth must always beconsidered.
References
1, Nolla CM: The development of the permanent teeth. J DeniChitd 1960:27:254-266.
2, Leysell L. Magnusson B, Thilander B: Relations between tlictimes of eruption primary and permanent teeth, Ada OdontotScand 1969;27:271-2S1,
3, Lo RT, Meyers RE: The sequence of eruption of the perm-anent teeth. Am J. Orthod 1953;39:460-467,
4, MacGregor SA: Interception of mal occlusion, J Dent Child1946;13:2-11,
5, Adicr P,: Effect of some Environmental factors on sequenceof permanent tooth eruption. J Dem Res 1963;42:605-615,
6, Korf SR: The eruption of permanent central incisors follow-ing premature loss of their antecedents, J Deni Child 1965:32:39-44,
7, Buckley JP: A rational treatment for putrescent pulps. DentRev 1904:18:1193 1197.
8, Lauterstein AM, Pruzaniky S, Barger TK: Effect of decidu-ous mandibular molar pulpotomy on the eruption of suc-cedaneous premolar, .1 Dem Res 1962;4L13Ö7-137L
9, Starkey PE: Pulpeetomy and root canal filling in a primarymolar: report of a case. / Dem Child 1973;40:213-217,
10, Riftin AJ: A simple, effective, safe technique for the rootcanal treatment of abscessed primary teeth, J Dem Child198n;47:435-44l,
11, Coll JA, Josell S, Casper JS: Evaluation of a one-appoint-ment formocresol pulpectomy technique for primiiry molars.Pediair Dem 1985;7:123-I29,
12, Hobson P: Pulp treatment of deciduotis teeth, Bi DemJ 1970;12S:275-282,
13, Morawa AP, Straffon LH, Han SS, et al; Clinical evaluationof pulpotomies using dilute formocresol, / Dent Child 1975;42:360-363.
Quintessence International Voltjme 22, Number 10/1991 799
Pédiatrie Dentistry
14. Fuks AB, Bimstein E: Clinical evaliiatiiiii ot' diluted formoi;-resol pulpototnies in primary teeth iil schiial children. PediiitrDfoll981i3:321-324.
15. Wright FAC, Widmer RP: Pulpal therapy in primary molarteeth: a rétrospective study../ PLY/O,/ I97Ç>;3:I<)5-2O6.
16. Van Amerongen WE, Mulder GR, Vingerling PA: Conse-quences of endodontie treatment in primary teeth. Part I: Aciinieal and radiographie study of the influence of formocresulpulpotomy on the life-span of primary molars. } DenI Ciiildiy86;55:364-370.
17. Loevy HT: The effeet of primary tooth extraction on theeruption of succedaneous premolars. J Am Dent Assoc 19S9;118:715-718.
t8, ConoverCJ: Practical Nonparametrii Slalislics. N&v/Yoik, JohnWiley & Sons, 1971.
ly. Rolling l,Thylstrup A: A 3-year clinical follow-up study of pui-potomomized primary molars treated with the formocresoitechnique. Scand J Dem Res 1975; 83:47-5 3. Ö
Books on
Orthodontics
Current Controversies inOrthodonticsedited by B. Meisen
^^Much needed information on bow controversieswitbin the field of' ortbodontics are shaping tbefuture of orthodontics,.
Orthodontics as a science is still very young, and a major part of the development of fhis profession has beenbased on "trial-and-error" approaches rather Ihan deductive research. Controversies have thus sprung upwifhin the field of orthodontics.
This book brings together contributors who arc experts in their fields, and who evaluate selected topics ofcontroversy in an attempt to differentiate between untried "traditions" and fact supported through scientific tests.
Contents; l. Esthetic .Need for Orthodontic Treatment; 2. Prediction in the Planning and Conduct of Orthodontic Treatment; 3. DentofacialMorphology and Breathing: A Century of Controversy: 4. Occlusion, Maiocclusion, and Craniomandihuiar Function; 5. FunctionalAppliances; 6. The Biomechanical Rationale of Orthodontic Therapy; 7. Limitations in Adult Orthodontics; a. Rigid Fixation forOrthognathic Surgery: Current Perspectives and Controversies; 9. Lingual Orthodontics in Adults: 10. Orthodontic Controversies: TheirOrigins, Consequences, and Resolution.
314 pp/538 illus/US S98/Coile; 1749
Functional Appliances inOrthodontic TreatmentAn Atlas of Clinical Prescription andLaboratory Construction
H. S. Orton
Presents a series of practical "design cards" forfunctional appliances. The cards give detailed noteson clinical selection of appliances and technicalconstruction. An invaluable tool for communication.
Contents include: Thp Fránket System; Expansion and LabialSegment Alignment Appliances (ELSAAs): and more.
103 PP/1B4 illus (48 in culor|/US S68/Code: 2184
Bench-Top OrthodonticsH. Lawson/J. L. Blazucki
Superb self-teaching book for fhe laboratory phasesof orthodontics. Dental students, technicians, andauxiliaries will appreciate the atlas format of clearpictures—no more guessing as to what fhe finishedproduct should look like! Proper sequence of sfepsis clearly laid out and illustrated.
Contents include: Orlhudontic Wire: Appliance Components;Hawley RBlainHr; Repairs; Brusism Appliance; Fixed TranspalatalArch; Hahit Apptiance: Orlhadontic Study Models; and more.
143 PP/3ZG it!us/US S38/Code: 2338
To order Quintessence Books, use the order card bound in this issue.
800 Quintessence International Volume 22, Number 10/1991