Embed Size (px)
Citation preview
Effect of hydroxyapatite/tricalcium-phosphate coating onosseointegration of plasma-sprayed titanium alloy implants
Matthew Stewart,1 Jean F. Welter,2 Victor M. Goldberg2
1Department of Veterinary Clinical Medicine, College of Veterinary Medicine, University of Illinoisat Urbana-Champaign, 1008W Hazelwood Drive, Urbana, Illinois 61802.2Department of Orthopaedics, Case Western Reserve University School of Medicine, 11100 Euclid Avenue,Cleveland, Ohio 44106.
Received 22 July 2003; accepted 28 July 2003
Abstract: This study determined the effects of a plasma-sprayed hydroxyapatite/tricalcium phosphate (HA/TCP)coating on osseointegration of plasma-sprayed titanium al-loy implants in a lapine, distal femoral intramedullarymodel. The effects of the HA/TCP coating were assessed at1, 3, and 6 months after implant placement. The HA/TCPcoating significantly increased new bone apposition onto theimplant surfaces at all time points. The ceramic coating alsostimulated intramedullary bone formation at the middle anddistal levels of the implants. Fluorescent bone labeling indi-cated that new bone formation occurred primarily duringthe first 3 months after implantation, with comparativelylittle activity detected in the latter stages of the study. Therewas no associated increase in pullout strength at either 3 or
6 months; however, post-pullout evaluation of the implantsindicated that the HA/TCP coating itself was not the pri-mary site of construct failure. Rather, failure was most com-monly observed through the periprosthetic osseous strutsthat bridged the medullary cavity. The demonstrated osteo-conductive activity of HA/TCP coating on plasma-sprayedtitanium alloy implant surfaces may have considerable clin-ical relevance to early host–implant interactions, by acceler-ating the establishment of a stable prosthesis–bone interface.© 2004 Wiley Periodicals, Inc. J Biomed Mater Res 69A: 1–10,2004
Key words: hydroxyapatite; osseointegration; plasma-sprayed titanium; implant stability; osteoconduction
INTRODUCTION
Development of a stable bone–implant interface iscritical to the successful use of orthopaedic and dentalprostheses. Enhanced interfacial stability permitsearly mobility and weight-bearing, and also reducesthe complications associated with microbial coloniza-tion and the generation and migration of wear de-bris.1–3 Implant stability is influenced by a number offactors including the implant design, recipient health,surgical technique and direct host–implant effects.
Several approaches have been developed to stimu-late favorable host–implant interactions, such as cre-ating implant surfaces with macroscopic irregularities,porous surfaces, and osteoconductive coatings. Hy-droxyapatite (HA) and similar calcium phosphatecoatings have been extensively evaluated as osteocon-ductive materials and have been shown to improve
osseointegration in experimental animal models4–11
and in human clinical studies.1,12–15
Hydroxyapatite and other ceramic coatings stimulatebone formation directly onto and around implant sur-faces. This bioactivity follows from the chemical andcompositional similarity of HA to bone, the provision ofsupplementary calcium and phosphate for peripros-thetic bone formation and the microtopographical envi-ronment provided for osteoblast colonization.16,17 Theiruse does introduce several potential complications in-cluding fatigue of the coatings, the possibility of separa-tion or delamination of the ceramic layer, prematurecoating dissolution, and contribution to wear particleload.18–25 Despite these concerns, several studies havedemonstrated beneficial effects of HA/TCP coating on avariety of implant surfaces, as cited above. The specificvalue of HA/TCP coating on plasma-sprayed titaniumalloy surfaces has received relatively little assessment.
The goal of this study was to determine the effectsof hydroxyapatite/tricalcium phosphate (HA/TCP)coating on the osseointegration of plasma-sprayed ti-tanium alloy implants. In particular, the study ad-dressed the influence of HA/TCP coating on apposi-
Correspondence to: M. Stewart; e-mail: [email protected] grant sponsor: Zimmer USA
© 2004 Wiley Periodicals, Inc.

tion of bone to the surface of the implant and the modeof failure of HA/TCP-coated implants.
METHODS
Implant characterization
The implants used in this study were cylindrical titaniumalloy (Ti6Al4V, ASTM F136) rods, 25 mm in length and 4.9 mmin diameter, and were supplied by Zimmer USA (Warsaw, IN).Each rod had a distal threaded end (4 mm in length and 4 mmin diameter) and a proximal capped end (2 mm in length and4 mm in diameter). A 0.25-mm-thick layer of titanium alloywas plasma-sprayed onto the surface of the cylinder, creating asurface with 20–50% porosity with pore sizes ranging from 50to 125 �m and surface roughness of 17.8 �m.
The raw material for the ceramic coating was 100% amor-phous HA. After application, 65–85% of the ceramic re-mained as HA, with approximately 50% of the applied HAin crystalline form. TCP constituted the bulk of the remain-ing calcium phosphates. The ceramic surface layer was ap-plied to a nominal thickness of 50–125 �m. All implantswere sterilized in an autoclave before surgical implantation.
Animal model and surgical procedure
We observed National Institutes of Health (NIH) guidelinesfor the care and use of laboratory animals (NIH Pub. No. 85-23,Rev. 1985) for all experiments involving animals in this study.Thirty skeletally mature male New Zealand White rabbits,weighing 3.5–3.9, kg were used in a well-characterized os-seointegration model.7,8,26,27 The rabbits were anesthetized byan intramuscular injection of ketamine (40 mg/kg), xylazine (5mg/kg), and acetylpromazine (0.75 mg/kg). Each rabbit re-ceived 25 mg gentamicin and 75,000 U procaine penicillin Gsubcutaneously at the start of surgery. Implants were insertedinto the medullary cavities of the distal femora via bilateralmedial parapatellar femorotibial arthrotomies. Preemptive an-algesia was administered at the start of each surgical procedureby infiltrating the subcutis proximal to the incisions withmepivicaine (0.25% Marcaine). Postoperatively, the rabbits re-ceived intramuscular injections of 0.2 mg buprenorphine/kgtwice daily for 48 h.
The distal femoral medullary cavity was accessed throughthe intercondylar notch using drill bits of incrementallyincreasing diameter (1.5-mm to 4.5-mm diameter). The med-ullary cavity was reamed manually with a circular file toaccommodate press-fitting of the implants at equivalentdepths. Each rabbit received a coated (HA/TCP) implantand an uncoated (control) implant, randomized to side. Atthe appropriate time points, rabbits were euthanized with alethal injection of pentobarbitone, administered through a24-g catheter inserted into a marginal ear vein.
The femora were radiographed 24 h after surgery to en-sure appropriate implant placement. In addition, the distalfemora were radiographed after collection using a Faxitron(Faxitron X-Ray Corporation, Buffalo Grove, IL) to docu-
ment uneventful implant incorporation and provide refer-ence images for equivalent sectioning of paired implants.
The effects of HA/TCP coating on implant osseointegrationwere assessed at 1, 3, and 6 months after surgery. Six rabbitswere euthanized at each time point for histological and histo-morphometric evaluation of the paired femora. An additionalsix rabbits were euthanized at 3 and at 6 months after surgeryfor biomechanical testing and evaluation of implant failure.
In vivo tetracycline labeling was used to monitor new boneformation during the course of the study. Before tetracyclineadministration, the rabbits were sedated with an intramus-cular injection of 50 mg ketamine, 10 mg xylazine, and 0.2mg acetylpromazine in a volume of 1 mL. Tetracycline (Bio-Mycin 200; Boehringer Ingelheim, 200 mg/mL) was dilutedto 65 mg/mL with sterile phosphate-buffered saline to re-duce viscosity and was administered intravenously at a doseof 50 mg/kg through a 24-g catheter inserted into a marginalear vein. Each rabbit received two tetracycline injections 24 hapart, to define new bone formation at a specific time point.Of the rabbits euthanized at 1 month (1-month group), threerabbits received injections 2 weeks after implant placement,whereas the remaining three rabbits received paired injec-tions on the days immediately before euthanasia. Of the3-month group, three rabbits were injected at 2 months andthe remaining three rabbits were injected at 3 months, justbefore euthanasia. Of the 6-month group, two rabbits wereinjected at 4 months, two at 5 months, and the remainingtwo at 6 months, just before euthanasia.
Histological and histomorphometric evaluation
Immediately after euthanasia, the distal femora were dis-sected from surrounding soft tissues, fixed in ethanol, and thenembedded in polymethylmethacrylate. Undecalcified serialcross sections were cut with a water-cooled diamond saw,mounted on Plexiglas slides, then ground and polished on aprecision grinder (Isomet; Buehler Corporation, Lake Bluff, IL)to a thickness of 50 �m. Two adjacent sections from the prox-imal (diaphyseal), middle (midmetaphyseal), and distal (distalmetaphyseal) levels of each implant [Fig. 1(A)] were stainedwith Toluidine blue for light microscopic examination. Adja-cent sections were left unstained for epifluorescent examina-tion of bone deposition. Three paired distal femora from the 3-and 6-month groups were prepared similarly after mechanicaltesting was carried out, for mode of failure evaluation.
We obtained histomorphometric measurements of sec-tions from each level using Scion Image software. The ante-rior, posterior, lateral, and medial quadrants of the femoralcross sections were defined using an overlay centered overthe implants [Fig. 1(B)]. The lengths of the titanium surfacesand, where applicable, the HA/TCP surfaces were mea-sured in each quadrant using a �10 objective. These quad-rant data were combined to provide values for both titaniumand HA/TCP perimeter lengths. The length of the implantsurfaces in direct contact with new bone was also deter-mined and converted to the percentage of new bone contactwith the implant surface at each level (the implant–boneindex). The percentage of new bone area at each level wascalculated from measurements of intramedullary area andintramedullary new bone area, using images obtained
2 STEWART, WELTER, AND GOLDBERG

through a �4 objective. There was considerable variation inthe transverse dimensions and geometries of the distal me-taphyseal sections. Therefore, the bone areas within an8-mm circle centered over the implant were measured andcompared from these distal sections. Ten measurements ofthe HA/TCP thickness were taken from each quadrant ofthe 1-month and 6-month midsections, using a �20 objec-tive, to assess changes in the ceramic coating over time.
Mechanical testing
The shear strength of the bone–implant surfaces was de-termined at 3 and 6 months with a pullout test, as previouslydescribed.8,26 The paired femora were dissected from thelimbs immediately after euthanasia, stripped of soft tissues,wrapped in PBS-soaked gauze, and stored at 4°C until test-ing. The implants were tested within 24 h of collection. Thefemoral condyles were removed to expose the distalthreaded portion of the implant. The femora were mountedin polymethylmethacrylate blocks and connected to a servo-hydraulic testing machine (Instron, Canton, MA) by thethreaded end. A pulling-force vector was applied to the longaxis of the implant at a constant displacement rate of 2mm/min and the force–displacement curve was recorded.The peak load before failure was divided by the exteriorsurface area of the implant to determine interface strength.
Statistical analyses
Histomorphological values obtained from adjacent sec-tions were averaged to provide a single data point for eachvariable at each level. The effects of HA/TCP coating onimplant perimeter lengths was assessed by analysis of vari-ance. We assessed differences between control and HA/TCP
implant–bone interfacial lengths, HA/TCP thicknesses overtime, and mechanical testing data by Student paired t test.For these analyses, data at each time point were comparedseparately. The effect of HA/TCP on intramedullary bonearea was assessed by a paired one-way t test to account forinteranimal variation. The control value of each pair wasgiven a value of 1, with the HA/TCP value representing thefold increase or decrease over the control.
RESULTS
Effects of HA/TCP coating on implant dimensionsand geometry
The measured HA/TCP coating varied from 70 to180 �m in thickness. This increased the diameter of thecoated implants by approximately 0.4 �m but effec-tively reduced the overall implant circumference be-cause irregularities of the plasma-sprayed titaniumsurface were filled in by the ceramic [Fig. 2(A)]. Figure2(B) shows comparative perimeter measurementsfrom the 6-month specimens. At all three levels, theouter (HA/TCP) perimeter of the treated implantswas slightly less than the outer (metallic) perimeter ofthe controls, although the differences were not statis-tically significant. Similar findings were obtained fromthe 1-month and 3-month specimens (data not shown).
Histological and histomorphometric analyses
Histology
At 1 month, the anterior and posterior regions of theintramedullary spaces of both the control and HA/
Figure 1. Intramedullary implant positioning. (A) Lateromedial radiograph showing implant positioning in the distalfemur. The proximal (P), middle (M), and distal (D) planes of histological evaluation are also shown. (B) Cross section of anHA/TCP-coated implant in situ. The anterior (A), posterior (P), lateral (L), and medial (M) quadrants, as defined forhistomorphological analyses, are indicated.
HA/TCP EFFECT ON PLASMA-SPRAYED Ti IMPLANT OSSEOINTEGRATION 3

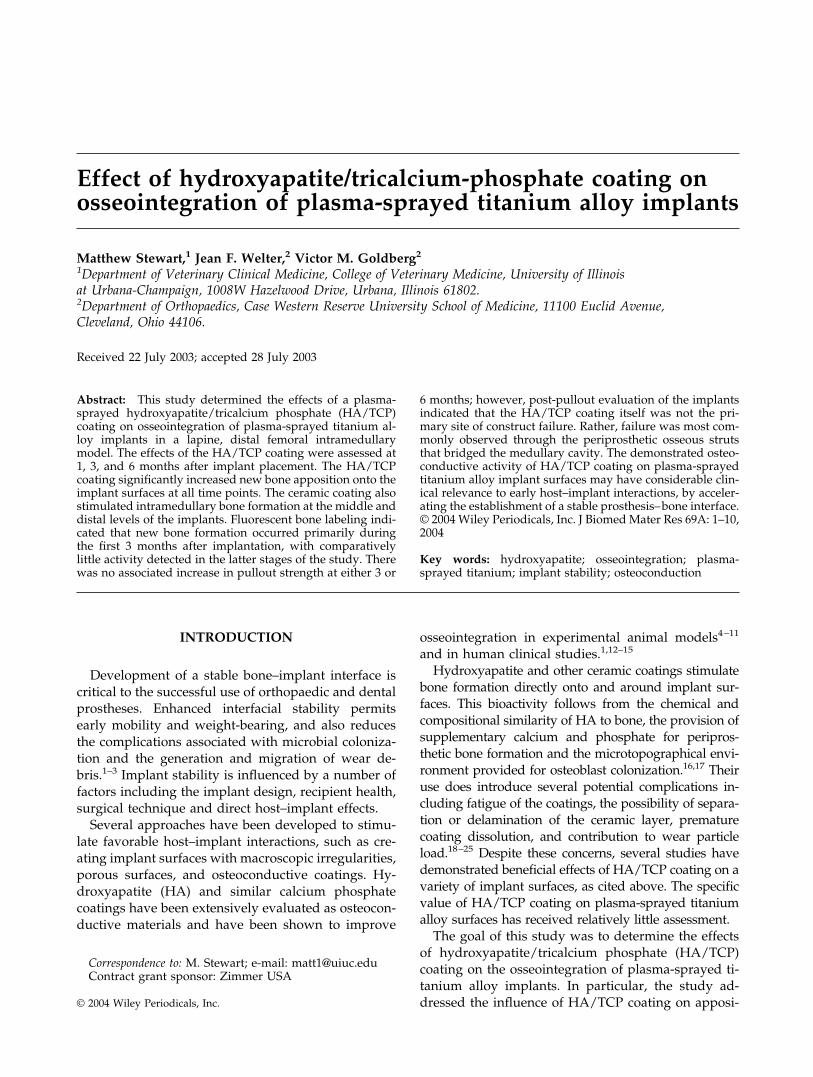
TCP femora contained interconnected trabeculae ofwoven bone. New bone formation and remodeling onthe endosteal surfaces of the femora were also evident.In the control limbs, the periphery of these trabeculaeconsisted of unmineralized osteoid, whereas this wasless apparent in the HA/TCP sections [Figs. 3(A, B)].Of note, much of the HA/TCP surfaces were coveredwith a thin layer of new bone. By 3 months, theintramedullary bone had undergone lamellar remod-eling in both groups [Figs. 3(C, D)]. By 6 months [Figs.3(E, F)], there were several (usually three or four)discreet osseous bridges evident in each section, span-ning the intramedullary space and buttressing the im-plant within the medullary cavity.
Bone–implant contact
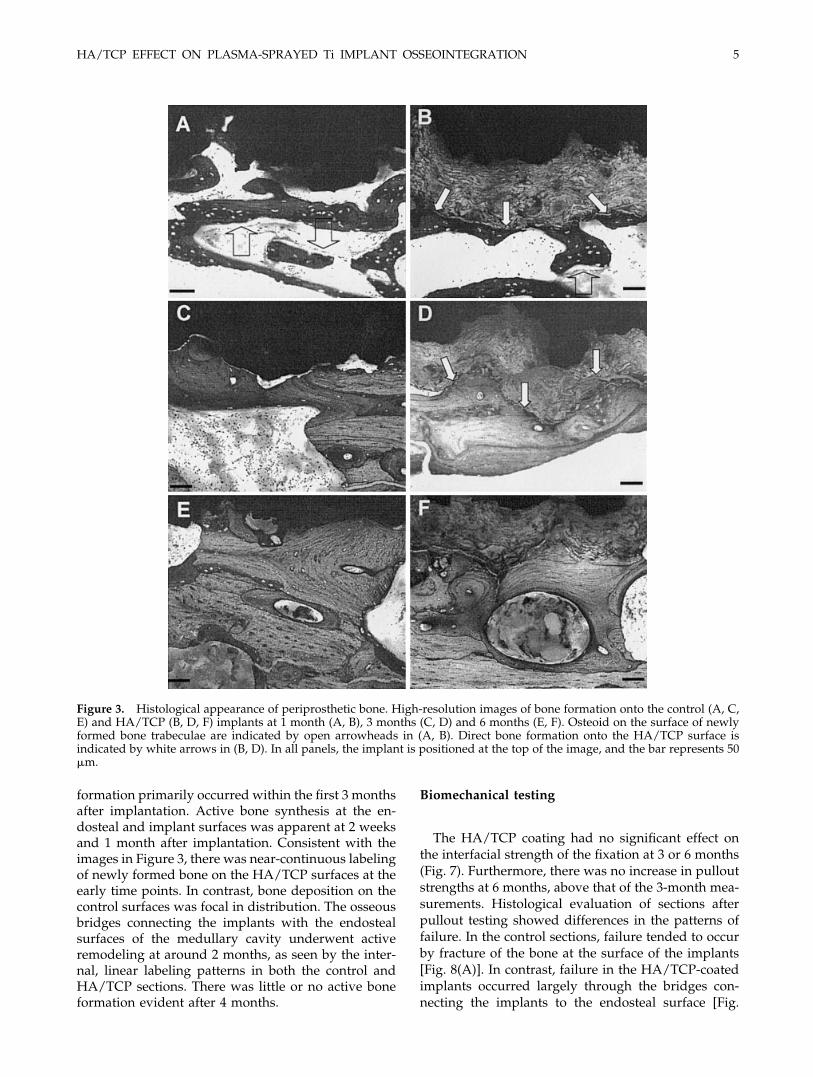
The HA/TCP significantly increased bone apposi-tion onto the implant surface at all three time points (1,3, and 6 months) and at all three levels (proximal,
middle, and distal). These results are shown in Figure4(A). Bone formation on the surface of the controlimplants gradually increased over the course of thestudy, starting at 10–16% at 1 month and increasing to24–38% by 6 months. In contrast, there was rapid andpersistent bone formation on the surface of HA/TCP-coated implants, with around 70–75% bone coveragethroughout the study.
Bone apposition was influenced by the ellipsoidcross section of the rabbit femur [Fig. 1(B)]. With thecontrol implants, approximately 65–70% of bone for-mation occurred within the anterior and posteriorquadrants, adjacent to the endosteal surface. In con-trast, there was relatively little bone apposition in themedial and lateral quadrants where there was no di-rect contact with the host endosteum [Fig. 4(B)]. Thisdifference reached statistical significance at 3 and 6months. In contrast, there was no apparent quadranteffect on bone apposition in the treated implants, sug-gesting the osteoconductive effect of the HA/TCP wasnot dependent on immediate endosteal proximity.
Intramedullary bone areas
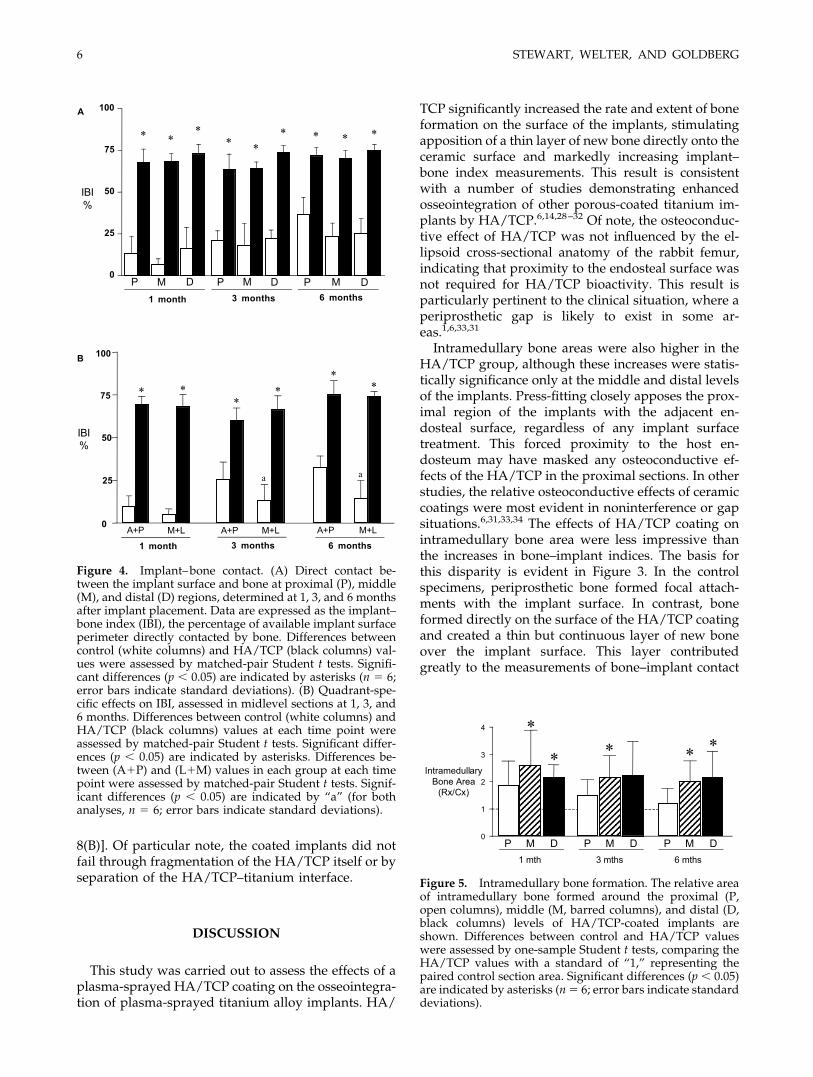
There was considerable interanimal variability inthe amounts of intramedullary bone formation. Toaccount for this, the intramedullary bone areas in HA/TCP sections were expressed as ratios of the boneareas in the corresponding control sections. The effectsof HA/TCP coating on intramedullary bone formationare shown in Figure 5. The relative intramedullarybone area in sections containing HA/TCP-coated im-plants was greater than that of control specimens at allthree levels of assessment at all three time points;however, this difference was not statistically signifi-cant in the proximal sections. In addition, the 3-monthdistal comparison approached but did not reach sta-tistical significance (p � 0.058).
HA/TCP thickness
Comparison of the HA/TCP coating thicknesses of1-month [74.4 � 16.60 �m, mean � standard deviation(SD)] and 6-month (78.4 � 22.83 �m) sections showedno significant change in thickness over time. Subjec-tively, the 6-month HA/TCP coatings appeared lessregular and homogeneous, as reflected in larger stan-dard deviations in all four quadrant data sets, but thedata indicate no significant reduction of the HA/TCPthickness occurred during the course of the experi-ment.
New bone deposition
Fluorescent imaging of tetracycline-labeled sections(Fig. 6) demonstrated that periprosthetic new bone
Figure 2. Effect of HA/TCP coating on implant perimeter.(A) Transverse section of an HA/TCP-coated implant, dem-onstrating the differences between the outer ceramic perim-eter (dashed line) and the underlying metallic surface (dot-ted line). (B) Mean values of the control (white bars), HA/TCP metallic (black bars), and HA/TCP outer (gray bars)perimeters of the 6-month implants. The arrow adjacent theY axis designates the theoretical perimeter of a 5-mm-diam-eter cylinder, 15.7 mm. The differences in perimeter lengthswere not statistically significant (n � 6; error bars indicatestandard deviations).
4 STEWART, WELTER, AND GOLDBERG
formation primarily occurred within the first 3 monthsafter implantation. Active bone synthesis at the en-dosteal and implant surfaces was apparent at 2 weeksand 1 month after implantation. Consistent with theimages in Figure 3, there was near-continuous labelingof newly formed bone on the HA/TCP surfaces at theearly time points. In contrast, bone deposition on thecontrol surfaces was focal in distribution. The osseousbridges connecting the implants with the endostealsurfaces of the medullary cavity underwent activeremodeling at around 2 months, as seen by the inter-nal, linear labeling patterns in both the control andHA/TCP sections. There was little or no active boneformation evident after 4 months.
Biomechanical testing
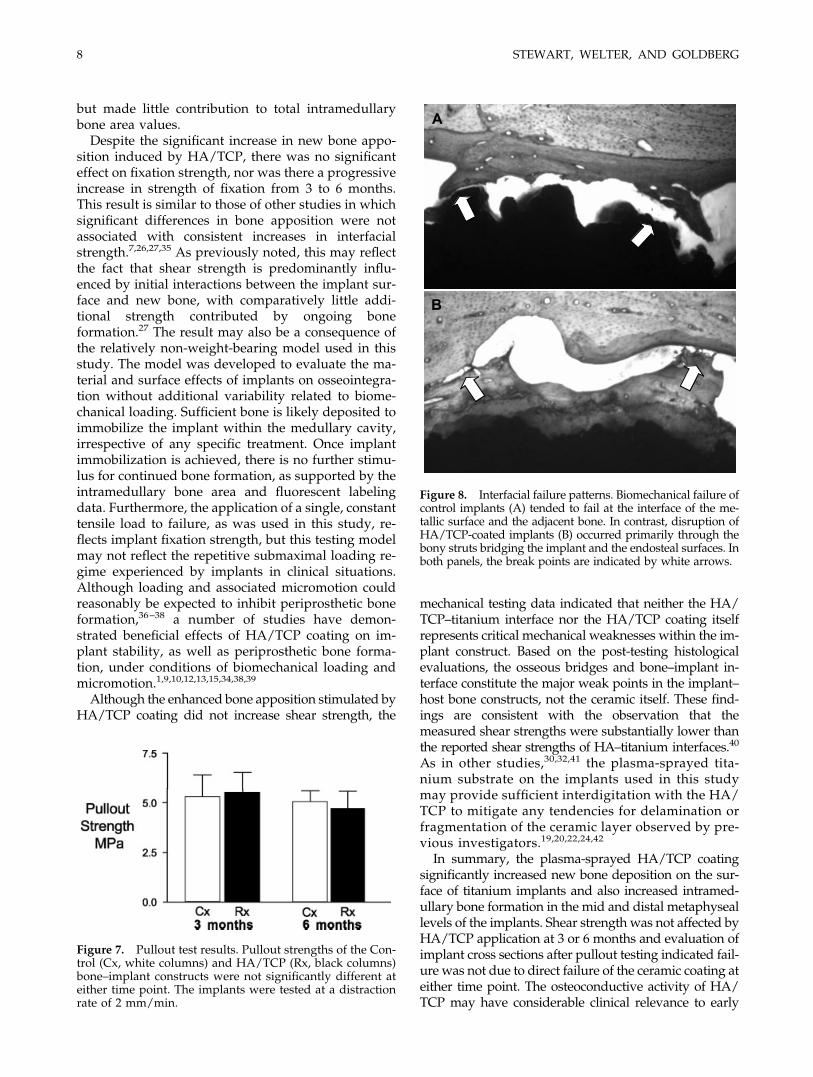
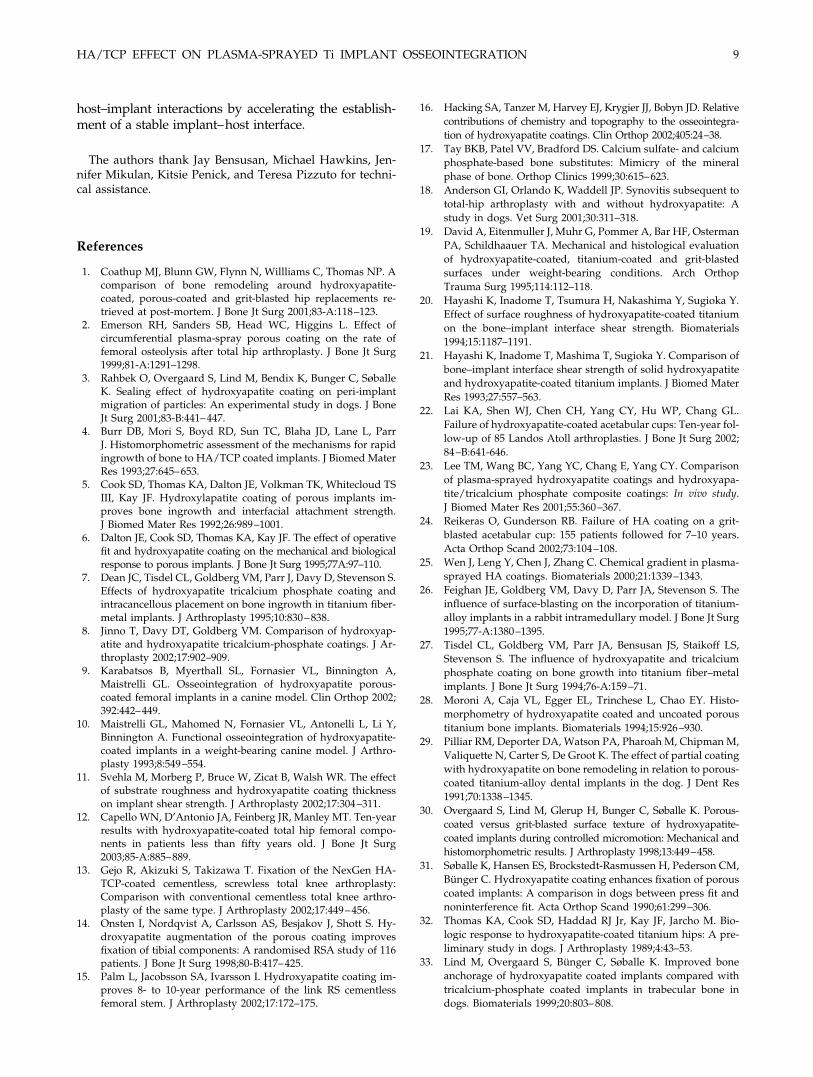
The HA/TCP coating had no significant effect onthe interfacial strength of the fixation at 3 or 6 months(Fig. 7). Furthermore, there was no increase in pulloutstrengths at 6 months, above that of the 3-month mea-surements. Histological evaluation of sections afterpullout testing showed differences in the patterns offailure. In the control sections, failure tended to occurby fracture of the bone at the surface of the implants[Fig. 8(A)]. In contrast, failure in the HA/TCP-coatedimplants occurred largely through the bridges con-necting the implants to the endosteal surface [Fig.
Figure 3. Histological appearance of periprosthetic bone. High-resolution images of bone formation onto the control (A, C,E) and HA/TCP (B, D, F) implants at 1 month (A, B), 3 months (C, D) and 6 months (E, F). Osteoid on the surface of newlyformed bone trabeculae are indicated by open arrowheads in (A, B). Direct bone formation onto the HA/TCP surface isindicated by white arrows in (B, D). In all panels, the implant is positioned at the top of the image, and the bar represents 50�m.
HA/TCP EFFECT ON PLASMA-SPRAYED Ti IMPLANT OSSEOINTEGRATION 5
8(B)]. Of particular note, the coated implants did notfail through fragmentation of the HA/TCP itself or byseparation of the HA/TCP–titanium interface.
DISCUSSION
This study was carried out to assess the effects of aplasma-sprayed HA/TCP coating on the osseointegra-tion of plasma-sprayed titanium alloy implants. HA/
TCP significantly increased the rate and extent of boneformation on the surface of the implants, stimulatingapposition of a thin layer of new bone directly onto theceramic surface and markedly increasing implant–bone index measurements. This result is consistentwith a number of studies demonstrating enhancedosseointegration of other porous-coated titanium im-plants by HA/TCP.6,14,28–32 Of note, the osteoconduc-tive effect of HA/TCP was not influenced by the el-lipsoid cross-sectional anatomy of the rabbit femur,indicating that proximity to the endosteal surface wasnot required for HA/TCP bioactivity. This result isparticularly pertinent to the clinical situation, where aperiprosthetic gap is likely to exist in some ar-eas.1,6,33,31
Intramedullary bone areas were also higher in theHA/TCP group, although these increases were statis-tically significance only at the middle and distal levelsof the implants. Press-fitting closely apposes the prox-imal region of the implants with the adjacent en-dosteal surface, regardless of any implant surfacetreatment. This forced proximity to the host en-dosteum may have masked any osteoconductive ef-fects of the HA/TCP in the proximal sections. In otherstudies, the relative osteoconductive effects of ceramiccoatings were most evident in noninterference or gapsituations.6,31,33,34 The effects of HA/TCP coating onintramedullary bone area were less impressive thanthe increases in bone–implant indices. The basis forthis disparity is evident in Figure 3. In the controlspecimens, periprosthetic bone formed focal attach-ments with the implant surface. In contrast, boneformed directly on the surface of the HA/TCP coatingand created a thin but continuous layer of new boneover the implant surface. This layer contributedgreatly to the measurements of bone–implant contact
Figure 5. Intramedullary bone formation. The relative areaof intramedullary bone formed around the proximal (P,open columns), middle (M, barred columns), and distal (D,black columns) levels of HA/TCP-coated implants areshown. Differences between control and HA/TCP valueswere assessed by one-sample Student t tests, comparing theHA/TCP values with a standard of “1,” representing thepaired control section area. Significant differences (p � 0.05)are indicated by asterisks (n � 6; error bars indicate standarddeviations).
Figure 4. Implant–bone contact. (A) Direct contact be-tween the implant surface and bone at proximal (P), middle(M), and distal (D) regions, determined at 1, 3, and 6 monthsafter implant placement. Data are expressed as the implant–bone index (IBI), the percentage of available implant surfaceperimeter directly contacted by bone. Differences betweencontrol (white columns) and HA/TCP (black columns) val-ues were assessed by matched-pair Student t tests. Signifi-cant differences (p � 0.05) are indicated by asterisks (n � 6;error bars indicate standard deviations). (B) Quadrant-spe-cific effects on IBI, assessed in midlevel sections at 1, 3, and6 months. Differences between control (white columns) andHA/TCP (black columns) values at each time point wereassessed by matched-pair Student t tests. Significant differ-ences (p � 0.05) are indicated by asterisks. Differences be-tween (A�P) and (L�M) values in each group at each timepoint were assessed by matched-pair Student t tests. Signif-icant differences (p � 0.05) are indicated by “a” (for bothanalyses, n � 6; error bars indicate standard deviations).
6 STEWART, WELTER, AND GOLDBERG
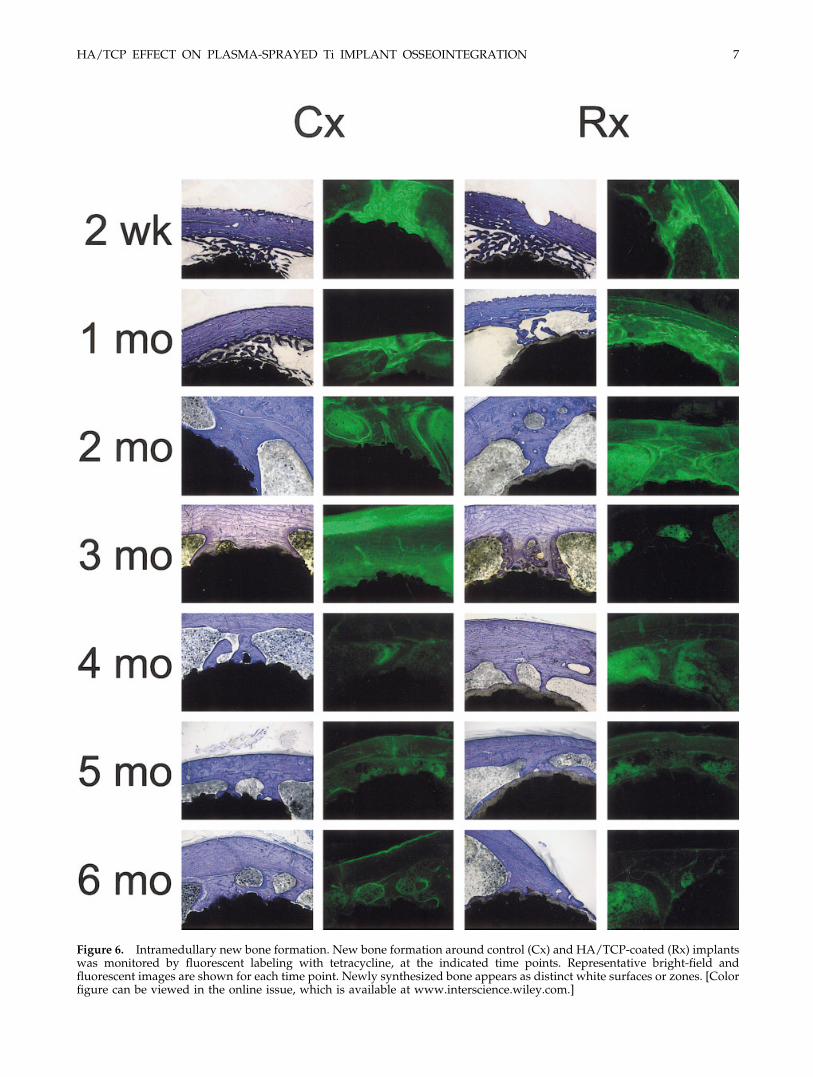
Figure 6. Intramedullary new bone formation. New bone formation around control (Cx) and HA/TCP-coated (Rx) implantswas monitored by fluorescent labeling with tetracycline, at the indicated time points. Representative bright-field andfluorescent images are shown for each time point. Newly synthesized bone appears as distinct white surfaces or zones. [Colorfigure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
HA/TCP EFFECT ON PLASMA-SPRAYED Ti IMPLANT OSSEOINTEGRATION 7
but made little contribution to total intramedullarybone area values.
Despite the significant increase in new bone appo-sition induced by HA/TCP, there was no significanteffect on fixation strength, nor was there a progressiveincrease in strength of fixation from 3 to 6 months.This result is similar to those of other studies in whichsignificant differences in bone apposition were notassociated with consistent increases in interfacialstrength.7,26,27,35 As previously noted, this may reflectthe fact that shear strength is predominantly influ-enced by initial interactions between the implant sur-face and new bone, with comparatively little addi-tional strength contributed by ongoing boneformation.27 The result may also be a consequence ofthe relatively non-weight-bearing model used in thisstudy. The model was developed to evaluate the ma-terial and surface effects of implants on osseointegra-tion without additional variability related to biome-chanical loading. Sufficient bone is likely deposited toimmobilize the implant within the medullary cavity,irrespective of any specific treatment. Once implantimmobilization is achieved, there is no further stimu-lus for continued bone formation, as supported by theintramedullary bone area and fluorescent labelingdata. Furthermore, the application of a single, constanttensile load to failure, as was used in this study, re-flects implant fixation strength, but this testing modelmay not reflect the repetitive submaximal loading re-gime experienced by implants in clinical situations.Although loading and associated micromotion couldreasonably be expected to inhibit periprosthetic boneformation,36–38 a number of studies have demon-strated beneficial effects of HA/TCP coating on im-plant stability, as well as periprosthetic bone forma-tion, under conditions of biomechanical loading andmicromotion.1,9,10,12,13,15,34,38,39
Although the enhanced bone apposition stimulated byHA/TCP coating did not increase shear strength, the
mechanical testing data indicated that neither the HA/TCP–titanium interface nor the HA/TCP coating itselfrepresents critical mechanical weaknesses within the im-plant construct. Based on the post-testing histologicalevaluations, the osseous bridges and bone–implant in-terface constitute the major weak points in the implant–host bone constructs, not the ceramic itself. These find-ings are consistent with the observation that themeasured shear strengths were substantially lower thanthe reported shear strengths of HA–titanium interfaces.40
As in other studies,30,32,41 the plasma-sprayed tita-nium substrate on the implants used in this studymay provide sufficient interdigitation with the HA/TCP to mitigate any tendencies for delamination orfragmentation of the ceramic layer observed by pre-vious investigators.19,20,22,24,42
In summary, the plasma-sprayed HA/TCP coatingsignificantly increased new bone deposition on the sur-face of titanium implants and also increased intramed-ullary bone formation in the mid and distal metaphyseallevels of the implants. Shear strength was not affected byHA/TCP application at 3 or 6 months and evaluation ofimplant cross sections after pullout testing indicated fail-ure was not due to direct failure of the ceramic coating ateither time point. The osteoconductive activity of HA/TCP may have considerable clinical relevance to early
Figure 7. Pullout test results. Pullout strengths of the Con-trol (Cx, white columns) and HA/TCP (Rx, black columns)bone–implant constructs were not significantly different ateither time point. The implants were tested at a distractionrate of 2 mm/min.
Figure 8. Interfacial failure patterns. Biomechanical failure ofcontrol implants (A) tended to fail at the interface of the me-tallic surface and the adjacent bone. In contrast, disruption ofHA/TCP-coated implants (B) occurred primarily through thebony struts bridging the implant and the endosteal surfaces. Inboth panels, the break points are indicated by white arrows.
8 STEWART, WELTER, AND GOLDBERG
host–implant interactions by accelerating the establish-ment of a stable implant–host interface.
The authors thank Jay Bensusan, Michael Hawkins, Jen-nifer Mikulan, Kitsie Penick, and Teresa Pizzuto for techni-cal assistance.
References
1. Coathup MJ, Blunn GW, Flynn N, Willliams C, Thomas NP. Acomparison of bone remodeling around hydroxyapatite-coated, porous-coated and grit-blasted hip replacements re-trieved at post-mortem. J Bone Jt Surg 2001;83-A:118–123.
2. Emerson RH, Sanders SB, Head WC, Higgins L. Effect ofcircumferential plasma-spray porous coating on the rate offemoral osteolysis after total hip arthroplasty. J Bone Jt Surg1999;81-A:1291–1298.
3. Rahbek O, Overgaard S, Lind M, Bendix K, Bunger C, SøballeK. Sealing effect of hydroxyapatite coating on peri-implantmigration of particles: An experimental study in dogs. J BoneJt Surg 2001;83-B:441–447.
4. Burr DB, Mori S, Boyd RD, Sun TC, Blaha JD, Lane L, ParrJ. Histomorphometric assessment of the mechanisms for rapidingrowth of bone to HA/TCP coated implants. J Biomed MaterRes 1993;27:645–653.
5. Cook SD, Thomas KA, Dalton JE, Volkman TK, Whitecloud TSIII, Kay JF. Hydroxylapatite coating of porous implants im-proves bone ingrowth and interfacial attachment strength.J Biomed Mater Res 1992;26:989–1001.
6. Dalton JE, Cook SD, Thomas KA, Kay JF. The effect of operativefit and hydroxyapatite coating on the mechanical and biologicalresponse to porous implants. J Bone Jt Surg 1995;77A:97–110.
7. Dean JC, Tisdel CL, Goldberg VM, Parr J, Davy D, Stevenson S.Effects of hydroxyapatite tricalcium phosphate coating andintracancellous placement on bone ingrowth in titanium fiber-metal implants. J Arthroplasty 1995;10:830–838.
8. Jinno T, Davy DT, Goldberg VM. Comparison of hydroxyap-atite and hydroxyapatite tricalcium-phosphate coatings. J Ar-throplasty 2002;17:902–909.
9. Karabatsos B, Myerthall SL, Fornasier VL, Binnington A,Maistrelli GL. Osseointegration of hydroxyapatite porous-coated femoral implants in a canine model. Clin Orthop 2002;392:442–449.
10. Maistrelli GL, Mahomed N, Fornasier VL, Antonelli L, Li Y,Binnington A. Functional osseointegration of hydroxyapatite-coated implants in a weight-bearing canine model. J Arthro-plasty 1993;8:549–554.
11. Svehla M, Morberg P, Bruce W, Zicat B, Walsh WR. The effectof substrate roughness and hydroxyapatite coating thicknesson implant shear strength. J Arthroplasty 2002;17:304–311.
12. Capello WN, D’Antonio JA, Feinberg JR, Manley MT. Ten-yearresults with hydroxyapatite-coated total hip femoral compo-nents in patients less than fifty years old. J Bone Jt Surg2003;85-A:885–889.
13. Gejo R, Akizuki S, Takizawa T. Fixation of the NexGen HA-TCP-coated cementless, screwless total knee arthroplasty:Comparison with conventional cementless total knee arthro-plasty of the same type. J Arthroplasty 2002;17:449–456.
14. Onsten I, Nordqvist A, Carlsson AS, Besjakov J, Shott S. Hy-droxyapatite augmentation of the porous coating improvesfixation of tibial components: A randomised RSA study of 116patients. J Bone Jt Surg 1998;80-B:417–425.
15. Palm L, Jacobsson SA, Ivarsson I. Hydroxyapatite coating im-proves 8- to 10-year performance of the link RS cementlessfemoral stem. J Arthroplasty 2002;17:172–175.
16. Hacking SA, Tanzer M, Harvey EJ, Krygier JJ, Bobyn JD. Relativecontributions of chemistry and topography to the osseointegra-tion of hydroxyapatite coatings. Clin Orthop 2002;405:24–38.
17. Tay BKB, Patel VV, Bradford DS. Calcium sulfate- and calciumphosphate-based bone substitutes: Mimicry of the mineralphase of bone. Orthop Clinics 1999;30:615–623.
18. Anderson GI, Orlando K, Waddell JP. Synovitis subsequent tototal-hip arthroplasty with and without hydroxyapatite: Astudy in dogs. Vet Surg 2001;30:311–318.
19. David A, Eitenmuller J, Muhr G, Pommer A, Bar HF, OstermanPA, Schildhaauer TA. Mechanical and histological evaluationof hydroxyapatite-coated, titanium-coated and grit-blastedsurfaces under weight-bearing conditions. Arch OrthopTrauma Surg 1995;114:112–118.
20. Hayashi K, Inadome T, Tsumura H, Nakashima Y, Sugioka Y.Effect of surface roughness of hydroxyapatite-coated titaniumon the bone–implant interface shear strength. Biomaterials1994;15:1187–1191.
21. Hayashi K, Inadome T, Mashima T, Sugioka Y. Comparison ofbone–implant interface shear strength of solid hydroxyapatiteand hydroxyapatite-coated titanium implants. J Biomed MaterRes 1993;27:557–563.
22. Lai KA, Shen WJ, Chen CH, Yang CY, Hu WP, Chang GL.Failure of hydroxyapatite-coated acetabular cups: Ten-year fol-low-up of 85 Landos Atoll arthroplasties. J Bone Jt Surg 2002;84–B:641-646.
23. Lee TM, Wang BC, Yang YC, Chang E, Yang CY. Comparisonof plasma-sprayed hydroxyapatite coatings and hydroxyapa-tite/tricalcium phosphate composite coatings: In vivo study.J Biomed Mater Res 2001;55:360–367.
24. Reikeras O, Gunderson RB. Failure of HA coating on a grit-blasted acetabular cup: 155 patients followed for 7–10 years.Acta Orthop Scand 2002;73:104–108.
25. Wen J, Leng Y, Chen J, Zhang C. Chemical gradient in plasma-sprayed HA coatings. Biomaterials 2000;21:1339–1343.
26. Feighan JE, Goldberg VM, Davy D, Parr JA, Stevenson S. Theinfluence of surface-blasting on the incorporation of titanium-alloy implants in a rabbit intramedullary model. J Bone Jt Surg1995;77-A:1380–1395.
27. Tisdel CL, Goldberg VM, Parr JA, Bensusan JS, Staikoff LS,Stevenson S. The influence of hydroxyapatite and tricalciumphosphate coating on bone growth into titanium fiber–metalimplants. J Bone Jt Surg 1994;76-A:159–71.
28. Moroni A, Caja VL, Egger EL, Trinchese L, Chao EY. Histo-morphometry of hydroxyapatite coated and uncoated poroustitanium bone implants. Biomaterials 1994;15:926–930.
29. Pilliar RM, Deporter DA, Watson PA, Pharoah M, Chipman M,Valiquette N, Carter S, De Groot K. The effect of partial coatingwith hydroxyapatite on bone remodeling in relation to porous-coated titanium-alloy dental implants in the dog. J Dent Res1991;70:1338–1345.
30. Overgaard S, Lind M, Glerup H, Bunger C, Søballe K. Porous-coated versus grit-blasted surface texture of hydroxyapatite-coated implants during controlled micromotion: Mechanical andhistomorphometric results. J Arthroplasty 1998;13:449–458.
31. Søballe K, Hansen ES, Brockstedt-Rasmussen H, Pederson CM,Bunger C. Hydroxyapatite coating enhances fixation of porouscoated implants: A comparison in dogs between press fit andnoninterference fit. Acta Orthop Scand 1990;61:299–306.
32. Thomas KA, Cook SD, Haddad RJ Jr, Kay JF, Jarcho M. Bio-logic response to hydroxyapatite-coated titanium hips: A pre-liminary study in dogs. J Arthroplasty 1989;4:43–53.
33. Lind M, Overgaard S, Bunger C, Søballe K. Improved boneanchorage of hydroxyapatite coated implants compared withtricalcium-phosphate coated implants in trabecular bone indogs. Biomaterials 1999;20:803–808.
HA/TCP EFFECT ON PLASMA-SPRAYED Ti IMPLANT OSSEOINTEGRATION 9

34. Mouzin O, Soballe K, Bechtold JE. Loading improves anchor-age of hydroxyapatite implants more than titanium implants.J Biomed Mater Res 2001;58:61–68.
35. Chang YL, Lew D, Park JB, Keller JC. Biochemical and mor-phometric analyses of hydroxyapatite-coated implants withvarying crystallinity. J Oral Maxillofac Surg 1999;57:1096–1108.
36. Heck DA, Nakajima I, Kelly PJ, Chao EY. The effect of loadalteration on the biological and biochemical performance of atitanium fiber–metal segmental prosthesis. J Bone Jt Res 1986;68-A:118–126.
37. Overgaard S, Søballe K, Josephsen K, Hansen ES, Bunger C.Role of different loading conditions on resorption of hydroxy-apatite coating evaluated by histomorphometric and stereo-logical methods. J Orthop Res 1996,14:888–894.
38. Søballe K, Hansen ES, Rasmussen HB, Jørgensen PH, BungerC. Tissue ingrowth into titanium and hydroxyapatite-coated
implants during stable and unstable mechanical conditions.J Orthop Res 1992;10:285–299.
39. Søballe K, Hansen ES, Brockstedt-Rasmussen H, Bunger C.Hydroxyapatite coating converts fibrous tissue to bone aroundloaded implants. J Bone Jt Surg 1993;75-B:270–278.
40. Zhang C, Leng Y, Chen J. In vitro mechanical integrity ofhydroxyapatite coatings on Ti-6Al-4V implants under shearloading. J Biomed Mater Res 2001;56:342–350.
41. Overgaard S, Lind M, Rahbek O, Bunger C, Søballe K. Im-proved fixation of porous-coated versus grit-blasted surfacetexture of hydroxyapatite-coated implants in dogs. Acta Or-thop Scand 1997;68:337–343.
42. Shen WJ, Chung KC, Wang GJ, McLaughlin RE. Mechanicalfailure of hydroxyapatite- and polysulfone-coated titaniumrods in a weight-bearing canine model. J Arthroplasty 1992;7:43–49.
10 STEWART, WELTER, AND GOLDBERG