Embed Size (px)
Citation preview

Effect of Healing Time on New BoneFormation After Tooth Extraction andRidge Preservation With DemineralizedFreeze-Dried Bone Allograft ARandomized Controlled Clinical TrialJeremiah Whetman and Brian L Mealey
Background Clinicians and patients continually searchfor procedures to decrease time from tooth extraction to res-toration Evidence to date is limited concerning timing ofridge preservation healing and reentry for implant place-ment The first objective of this study is to histologically eval-uate new bone formation 8 to 10 weeks versus 18 to 20weeks after extraction of non-molar teeth and ridge preserva-tion using demineralized freeze-dried bone allograft (DFDBA)The second objective is to compare dimensional changesincluding ridge width and height at the two healing timepoints
Methods Forty-four patients had tooth extraction andridge preservation with DFDBA that was obtained froma single donor Clinical measurements were made to evalu-ate ridge height and width Patients were randomly allo-cated to short-term (8 to 10 weeks) and long-term (18 to20 weeks) healing groups Sites were reentered at the ap-propriate healing time core biopsy was obtained anda dental implant was placed The same ridge dimensionswere measured at time of implant placement Histomor-phometric analysis was performed to determine percentageof new vital bone formation residual graft and connectivetissue (CT)other
Results A significantly higher percentage (4741) ofnew vital bone formation was found in the long-term healinggroup compared with the short-term healing group (3263)(P = 001) There was no significant difference in percentageof residual graft percentage of CTother or ridge dimen-sional changes
Conclusion This study indicates significantly greater newvital bone formation occurs after tooth extraction and ridgepreservation with DFDBA when sites healed for 18 to 20weeks compared with 8 to 10 weeks prior to dental implantplacement J Periodontol 2016871022-1029
KEY WORDS
Alveolar bone grafting alveolar bone loss bone resorptionbone transplantation dental implants tooth extraction
For many years implant therapyhas been used to replace extractedand missing teeth with great pre-
dictability1 After tooth extraction sig-nificant changes in ridge dimensionboth horizontal and vertical can takeplace in a short period of time2-6 posinga potential challenge for clinicians tosurgically place dental implants prop-erly in a restoratively driven positionAdditional treatment is often then neededresulting in increased significant cost topatients patient morbidity and techni-calities in procedure6
Ridge preservation has been shown tobe a successful treatment for maintaininghorizontal and vertical ridge dimensionafter extraction347-9 The simple appli-cation of placing grafting material into anextraction socket significantly reducesdimensional changes38 This procedureis more predictable offering reduction inpatient morbidity and cost comparedwith other lateral and vertical ridge aug-mentation techniques thatmay be neededin the absence of ridge preservation7
Various materials including autog-enous grafts allografts xenografts andalloplasts have been used for ridge pres-ervation procedures with varying suc-cess9 Mineralized freeze-dried boneallograft (FDBA) and demineralized
Department of Periodontics University of Texas Health Science Center San Antonio SanAntonio TX doi 101902jop2016160139
Volume 87 bull Number 9
1022
FDBA (DFDBA) are well-supported common prod-ucts used to reduce changes in ridge dimension aftertooth extraction and provide adequate new vital bonefor implant placement410-12 FDBA maintains socketspace and acts as a scaffold for host osteoprogenitorcells during the healing phase1314 However thedemineralization process of DFDBA additionally re-leases bone morphogenetic proteins (BMPs)1516
Released BMPs give the allograft the added benefit ofosteoinductivity17 FDBA contains these same BMPshowever they remain sequestered in graft materialaway from osteoprogenitor cells until demineralizationoccurs in situ Available BMPs in DFDBA stimulatehost osteoprogenitor cells to differentiate into osteo-blasts and begin new bone formation Wood andMealey11 reported an increase in new vital bone for-mation in ridge preservation using DFDBA comparedwith FDBA Borg and Mealey12 also showed a com-bination FDBADFDBA grafting material increasedvital bone formation compared with FDBA alone
Dental implant placement timing after ridge pres-ervation continues to be a controversial topic Patientsand practitioners are continually searching for waysto expedite the process of dental implant therapyBranemarkrsquos original protocol of endosteal root-formdental implant placement recommended at least 12months of healing time after tooth extraction prior toimplant placement18 This process can be shortenedin two areas 1) extraction to implant placement and2) implant placement to implant restoration Imme-diate placement protocols continue to receive supportfrom the scientific literature with regard to success andpredictability compared with conventional placementtechniques19-22 Even in the presence of periapicalpathology extraction and immediate implant place-ment remains a successful and comparable treatmentto implants placed in healed ridges23-25 Beck andMealey10 allowed ridges to heal after extraction andridge preservation with a mineralized allograft for 3and 6 months Histologically there was no differencein new vital bone formation between 3- and 6-monthpostextraction healing periods suggesting that im-plant placement at either time point would be ap-propriate However bone used in that study was notprocessed in the samemanner (ie via freeze-drying)as the bone allograft used in the current study
To the best of the authorsrsquo knowledge few studieshave histologically evaluated healing of ridge pres-ervation grafts at differing time points Therefore thepurpose of this study is to evaluate differences inhealing after tooth extraction and ridge preservation ofnon-molar teeth using DFDBA at 8 to 10 weeks ofhealing compared with 18 to 20 weeks of healing Theprimary objective of this study is to histologicallycompare amounts of new vital bone formation re-sidual graft material and connective tissue (CT)other
present Secondary objectives include comparing di-mensional changes in ridge height and width aftertooth extraction and ridge preservation with DFDBA
MATERIALS AND METHODS
Participant EnrollmentThe Institutional Review Board of the University of TexasHealth Science Center at San Antonio (UTHSCSA) SanAntonio TX reviewed and approved the researchprotocol This parallel arm clinical trial was registeredat ClinicalTrialsgov (NCT02154386) and conductedin accordance with the Helsinki Declaration of 1975as revised in 2013 To reach statistical power to detecta significant mean difference of at least one standarddeviation (SD) in percentage of new vital bone for-mation using MannndashWhitney U test with a power of885 at a 005 level a sample size of at least 14 ridgepreservation sites was required per healing periodOther studies by the authorsrsquo group have demon-strated SDs ranging from 119 to 224 for per-centage of vital bone formation10-12 To accommodatea potential 30 dropout rate 46 patients (21 malesand 25 females aged 23 to 81 years mean age 557years) were enrolled from October 2013 to December2014 (Fig 1)26 Patient inclusion criteria comprisedthe following 1) single-rooted teeth needing extrac-tion 2) patient desiring restoration with a dental im-plant 3) at least 10 mm of apicocoronal bone heightfrom vital anatomic structures 4) adequate space forrestoration 5) root of tooth in a spatial orientation suchthat a restoratively driven implant position could beobtained that was totally within the former socket areathus including only grafted bone in the biopsy core 6)less than 50 dehiscence after tooth extraction Ex-clusion criteria were 1) patients not fulfilling inclusioncriteria or not compliant with necessary proceduralfollow-up 2) pregnancy 3) active systemiclocal in-fection not including periodontitis 4) medical condi-tions or medications known to alter soft tissue orbony healing (poorly controlled diabetesmellitus [DM]bisphosphonates immunosuppressives etc) 5) teethwith short roots or roots that were malpositioned suchthat the core biopsy might include bone along thesocket wall Females of childbearing age without tuballigation menopause or hysterectomy were required tohave a negative pregnancy test prior to surgery
DFDBA used for all patients in the study wasprocured from a single donor a 42-year-oldmale andhad residual calcium content of 26 and a particlesize of 250 to 1000 microns Osteoinductivity wastested in vivo by implantation into a gluteal musclepouch of an athymic mousedagger and was scored aspercentage of new bone formation in the whole im-planted area (grade of 0 to 4) DFDBA used in thisstudy received a grade of 2 out of 4 corresponding
dagger WuXi AppTec St Paul MN
J Periodontol bull September 2016 Whetman Mealey
1023
with an area of new bone formation between 1 and25 of total area of implanted bone product
Surgical ProtocolAfter enrollment custom thermoplastic acrylic mea-suring stentsDagger were made from alginate impressionsand stone casts for each patient Mucoperiosteal flapswere reflected no more than 2 to 3 mm beyond thecrest of the alveolus and the tooth was extractedAfter thorough debridement and irrigation presenceor absence and extent of dehiscence and number ofbony walls were recorded Clinical measurementswere made using a periodontal probesect with a customacrylic measuring stent Measurements included 1)depth of socket on buccal and lingual sides 2) buccaland lingual alveolar crest heights 3) buccal platethickness 1 mm apical to alveolar crest using a dentalcaliperi and 4) total ridge width 4 mm apical to al-veolar crest using a ridge caliperpara All measurements
were made to the nearest 05 mmexcept buccal plate thicknesswhich was measured to the nearest01mm To facilitate reproducibilityholes in the acrylic measuring stentwere made directly over buccal andlingual plates and 4 mm apical tothe alveolar crest for ridge widthmeasurements After clinical mea-surements the ridge was preservedusing DFDBA
Bone graft material was hydratedwith sterile saline for 10 minutesand increments of bone graft ma-terial were placed in the extractionsocket to not overfill the socketIf dehiscence of 50 or less waspresent on the buccal or lingualplate the patient remained in thestudy and a collagen repair mem-brane was used to replace themissing bone wall No periosteal re-leasing incision was performed andprimary closure was not attemptedWhen no dehiscence was presenta collagen-orifice barrier was placedover the extraction socketdaggerdagger Thearea was sutured using 4-0 chromicgut sutures Where dehiscence wasgreater than 50 the patient wasexited from the study
After the surgical procedure wascompleted each patient was ran-domized into the short-term group(8 to 10 weeks of healing) or thelong-term group (18 to 20 weeks ofhealing) by random selection from
a group of opaque envelopes Each patient was pre-scribed 500 mg of amoxicillin three times daily for7 days and 012 chlorhexidine mouthrinse for plaquefor 30 seconds twice daily for 4 weeks If allergic topenicillin the patient was prescribed 100 mg ofdoxycycline twice daily for 7 days Postoperative painmanagement included non-steroidal anti-inflammatorydrugs and narcotic analgesics as indicated Each pa-tient was seen at 2 weeks and 4 weeks to monitorhealing and to remove plaque from surgical areas
At the appropriate randomized time point thepatient returned for the second surgical visit Upon
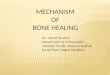
Figure 1Consolidated Standards of Reporting Trials (CONSORT)26 study flowchart
Dagger Clear Splint Biocryl 075mm125mm Round Great Lakes OrthodonticsTonawanda NY
sect UNC-15 periodontal probe G Hartzell amp Son Concord CAi Iwanson gauge Salvin Dental Specialties Charlotte NCpara Castroviejo ridge caliper Salvin Dental Specialties LifeNet Health Virginia Beach VA Socket repair membrane Zimmer Dental Warsaw INdaggerdagger Oraplug Salvin Dental Specialties
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1024
mucoperiosteal flap reflection the custom acrylicstent of the patient was used to obtain clinical mea-surements in the same manner namely buccal andlingual alveolar crest heights and ridge width Anyresidual socket defect was measured to the nearestmillimeter A 20-mm internal diameter30-mm ex-ternal diameter trephine drillDaggerDagger with depth indicatormarkings was used to obtain a core biopsy at least8 mm in length and initiate the osteotomy for implantplacement The bone biopsy was placed in 10 neu-tral buffered formalin solution The remaining os-teotomy was completed according to the protocolof the manufacturer to receive an appropriate sizediameter and length implant Any additional bonyaugmentation was recorded and performed If ridgewidth was unable to accommodate implant place-ment the implant was not placed and the ridge wasaugmented at the discretion of the operator Thepatient was seen at 7 to 10 days postoperatively andfor a prerestorative check at approximately 3 months
Histologic Processing and AnalysesHistologic processing was completed as described inother studies conducted by the authorsrsquo researchgroup10-12 Briefly bone cores were removed fromtrephines and placed directly into 10 neutral buff-ered formalin Cores were decalcified dehydratedembedded in paraffin and sectioned to 4-mm-thicksections for histomorphometric analysis Tissue wasstained with a routine staining procedure of hema-toxylin and counterstained with a slightly acidifiedcombination of orange G and eosin Y with acidfuchsinsectsect
Histomorphometric analysis was performed ina similar manner as done by the authorsrsquo group inprevious studies10-12 The sole examiner (JW) wasmasked to treatment groups during the analysisprocess A minimum of nine sections were made foreach core Each section was examined at 1middot todetermine which provided the best section for high-power evaluation with preference given to the in-nermost section of the core whenever possible Thesection was examined at power between 20middot and 40middotmagnification in its entiretyii to ensure accurateanalysis of new vital bone residual graft and CTother Residual graft particles were identified as re-gions of lamellar bone having lacunae without pres-ence of osteocytes vital bone was identified by thepresence of osteocytes in lacunae CTother includedvasculature loose fibrous CT and inflammatory cellsOnce the core was separated into its respectivecomponents (vital bone residual graft and CTother)using image editing softwareparapara separated imageswere converted to a binary black and white image
Total number of pixels was calculated and summedfor each image and percentage of pixels for each
image was calculated to find percentage area of eachcomponent of bone core
Statistical Analyses Each study participant con-tributed a single value of each outcome variable tostatistical analysis A two-sample Student t test wasperformed for histologic outcomes as well as clinicalridge dimensional changes to evaluate differencesbetween the two treatment groups Box plots wereused to assess whether parametric statistical tests wereappropriate In the event of extreme outliers or sig-nificant departures from symmetry MannndashWhitney Utests were performed to confirm findings from Studentt tests To evaluate treatment group differences in archlocation of site presence or absence of a dehiscenceat extraction toothbound versus non-toothboundextraction site and need for additional grafting atthe time of implant placement Fisher exact testswere performed For all statistical analyses P lt005 wasconsidered significant Spearman rank and Pearsoncorrelations between clinical and histologic parameterswere also analyzed
RESULTS
Of 46 patients enrolled two patients consented toparticipate and subsequently elected to withdrawfrom the study (Fig 1) After extraction one patientstarted treatment with a medication (teriparatide)known to alter bone metabolism and was exited fromthe study There was one smoker in each group Fourpatients had well-controlled DM two from eachgroup Of the 43 patients who completed the study41 core biopsies were taken After healing one pa-tient in the long-term group had inadequate ridgewidth for core biopsy and implant placement how-ever ridge dimensional changes were recorded Onepatient had poor quality bone core that could not becontained for processing but an implant was suc-cessfully placed Thus 42 of 43 patients who re-ceived extraction and ridge preservation had implantsplaced successfully Of 41 core biopsies taken twowere lost to processing one from each group In theshort-term group clinical data were collected to per-form dimensional analysis for all 22 patients In thelong-term group data for ridge dimensional analysiswere collected for 19 of 21 patients In this group thecustomized acrylic measuring stent was lost for onepatient and clinical measurements were not made atthe implant surgery for the other patient
The short-term group healed for a mean of 903 ndash069 weeks and the long-term group healed fora mean of 1911 ndash 087 weeks At baseline sites in
DaggerDagger Salvin Dental Specialtiessectsect Treosin Statlab Medical Products McKinney TXii CellSens Version 14 software Olympus Center Valley PAparapara Adobe Photoshop CS51 Adobe San Jose CA ImageJ National Institutes of Health Bethesda MD
J Periodontol bull September 2016 Whetman Mealey
1025
both groups were similar Fisher exact test found nosignificant differences for study sites between groupsHowever there was a statistically significant differ-ence in buccal plate thickness between the twogroups (P = 0001) Mean buccal plate thickness inthe short-term group was 0614 ndash 0273 mm com-pared with 1010 ndash 0446mm in the long-term groupMost sites were maxillary sites with 14 in the short-term group and 13 in the long-term group There wasno significant difference in initial ridge width betweenthe two treatment groups (P = 051) The short-termgroup had a mean initial ridge width of 939 ndash169 mm compared with 978 ndash 205 mm in the long-term group
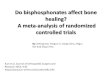
Histologic ObservationsVital bone was identified as areas of bone with oste-ocytes occupying lacunae and was most often wovenbone (Fig 2) Residual graft particles were identifiedas areas of primarily lamellar bone and no osteocytesoccupying the lacunae Apposition of new vital boneon residual graft particles was often noted The lastcategory was CTother which comprised loose fi-brovascular CT
There was a significantly different percentage newvital bone between the short-term group and thelong-term group (P = 001) The short-term grouphad a mean of 3263 vital bone compared with4741 in the long-term group (Table 1) With regardto percentage residual graft there was no significantdifference between treatment groups (test = 3742control = 2680) however it did trend towardstatistical significance (P = 006) There was no sig-nificant difference among treatment groups with re-gard to fraction of CTother (P = 042) A Fisher exact
test showed no significant difference in percentagenew vital bone among sites in the maxillary archcompared with sites in the mandibular arch (P = 043)anterior versus posterior tooth position (P = 074) andpresence or absence of a dehiscence at the time ofextraction (P = 057)
Dimensional ChangesIn analyzing ridge dimensional changes no statis-tically significant differences were found betweentreatment groups (Table 2) Specifically there wasno statistical difference in ridge width change (P =021) buccal ridge height change (P = 029) orlingual ridge height change (P gt099) Mean decreasein ridge width was 141 mm in the short-term groupand 066 mm in the long-term group Mean loss ofbuccal and lingual ridge height was between 084 and182 mm No significant correlation was found be-tween buccal plate thickness at time of extraction andfinal ridge width change
DISCUSSION
The primary objective of this study is to evaluate effectof healing time on new bone formation after ridgepreservation with DFDBA specifically at time pointsaveraging 9 weeks and 19 weeks after tooth extrac-tion Significantly more new vital bone was found inthe long-term healing group compared with the short-term healing group with no significant differences inridge dimensional changes between groups
This study design which has been used by theauthorsrsquo research group before10-12 eliminates manypotential confounding variables by 1) utilizing a singledonor as the source of bone graft material for bothexperimental groups 2) testing osteoinductivity ofallograft material 3) including only sites with at least10 mm of socket depth and root angulation similar tothe desired final implant position and 4) using stan-dardized custom acrylic stents to compare ridge di-mensional change This allowed direct comparison ofnew vital bone formation between the two groups withfew confounding variables There is great variabilityamong donors and among processing lots of demin-eralized bone allografts17 Using bone derived from thesame donor and having the same residual calciumcontent allowed for comparison between groupswithout concern for donor and processing variabilityIncluding only sites with 10 mm of radiographic bonesupport and root orientation similar to the plannedrestoratively driven implant placement eliminated thepotential of including native bone in core biopsieswhich could confound histomorphometric analysis ofpercentage new bone formation10-1227-29
Wood and Mealey11 also used DFDBA in ridgepreservation and found an average of 3243 newvital bone formation 20 weeks after grafting In the
Figure 2Long-term healing group (Hematoxylin and counterstained withacidified combination of eosin-Y orange-G and acid fuchsin originalmagnification middot10) VB = vital bone RG = residual graft
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1026
current study using DFDBA an average new vitalbone formation of 4741 was found after 19 weeksof healing This result coincides with knowledge ofdonor variability as the in vivo inductivity score ofDFDBA used by Wood and Mealey11 was graded as 1on a scale of 0 to 4 compared with an inductivityscore of 2 on the same scale for DFDBA used in thecurrent study Thus when an allograft with higherinductivity was used after essentially the same amountof wound healing time more new vital bone formationwas found
Borg and Mealey12 compared ridge preservationwith an allograft consisting of 100 mineralizedFDBA to a combination allograft with a ratio of 30DFDBA70 FDBA at 19 weeks of healing The donorinductivity score for graft material in that study wasgraded as 3 of 4 and mean new vital bone formationwas 3616 in the combination allograft group Thiswas significantly more new bone formation comparedwith the group grafted with FDBA alone (247) andvery similar to 3243 new vital bone formation fromWood and Mealeyrsquos11 study using 100 DFDBA It ispossible that the higher inductivity of DFDBA in theBorg and Mealey12 study resulted in induction of newvital bone formation equivalent to that in Wood andMealeyrsquos11 study despite the demineralized allograftmaking up only 30 of the graft material in the formerstudy compared with 100 DFDBA in the latter Inconsidering these studies and the current studyDFDBA results in significantly greater formation ofnew vital bone after ridge preservation comparedwith FDBA
The significance of new vital bone formation onimplant survival and success is unclear at this pointIntuitively a higher percentage of new vital bone isdesirable as increased vital bonemay increase bone-to-implant contact or at least increase the rate at whichthe implant achieves stability andmaximum bone-to-implant contact However the authors are unawareof published literature clearly demonstrating thatpercentage of vital bone at an implant site directlyaffects implant survival or success including bone-to-implant contact esthetics or peri-implant boneloss
When an implant osteotomy is prepared tactilesensation may give the operator a subjective senseof bone density at the site At sites that have hadridge preservation is it often difficult to assessquality of bone at the grafted site during implantosteotomy or placement The authors of the currentstudy noted great variability in both treatmentgroups with some sites in each group having poordensity and others having good density It is theauthorsrsquo opinion that poor bone quality at the time ofcore biopsy and osteotomy preparation was morecommon in the short-term healing group than in thelong-term healing group It is important to note thathistomorphometric analysis showed wide variabilityin percentage of new vital bone residual graft mate-rial and CTother with large standard deviations foreach parameter in both groups Therefore subjectivedifferences in density during osteotomy preparationmay be reflective of actual differences in percentageCTother new vital bone or residual graft material
Table 1
Histologic Analysis ()
Groups
Vital Bone
Mean ndash SD
Residual Graft
Mean ndash SD
CTOther
Mean ndash SD
Test group (short-term healing group) 3263 ndash 2145 3742 ndash 1853dagger 2994 ndash 1751
Control group (long-term healing group) 4741 ndash 1166 2680 ndash 1520dagger 2578 ndash 1382
P = 001 for test group versus controldagger P = 006 for test group versus control
Table 2
Alveolar Ridge Dimensional Changes
Groups
Change in Ridge
Width Mean ndash SD
Change in Ridge
Width (mm)
Mean ndash SD
Change in Ridge
Height Buccal (mm)
Mean ndash SD
Change in Ridge
Height Lingual (mm)
Mean ndash SD
Test group (short-term healing group) -1393 ndash 2036 -141 ndash 211 -182 ndash 223 -084 ndash 148
Control group (long-term healing group) -745 ndash 1658 -066 ndash 155 -118 ndash 131 -084 ndash 096
No significant difference between groups for any measurements (P gt005)
J Periodontol bull September 2016 Whetman Mealey
1027
among patients No attempt was made in this studyto correlate objective histomorphometric data withsubjective assessment of bone density during os-teotomy preparation
Cardaropoli et al3 reported a meaningful negativecorrelation between baseline buccal plate thicknessand ridge width change at sites receiving tooth ex-traction but no ridge preservation procedures Thussites with a thinner buccal plate had greater loss ofridge width At baseline in the current study therewas a significant difference of approximately 04 mmin buccal plate thickness between treatment groupsHowever difference in loss of ridge width betweengroups was not statistically significant There wasalso no meaningful correlation between buccal platethickness and ridge dimensional changes It is pos-sible that use of a ridge preservation bone graftcounteracts the impact of a thin buccal plate on loss ofridge width after tooth extraction Other studies per-formed by the authorsrsquo research group also showed nomeaningful correlation between initial buccal platethickness and change in ridge width when ridge pres-ervation grafting was performed10-1227-29
CONCLUSIONS
The current study indicates there is significantly greaternew vital bone formation after tooth extraction andridge preservation with DFDBAwhen the clinician waits19 weeks prior to dental implant placement comparedwith only 9 weeks In addition there is no difference inridge dimensional change between sites healing for anaverage of 9 weeks compared with 19 weeks
ACKNOWLEDGMENTS
The authors thank Dr Michael Mills Dr David Lashoand Dr Kevin Gureckis UTHSCSA for their help inthe design and completion of this project The au-thors thank Ms Sonja A Bustamante at UTHSCSAfor the excellent histology provided for the studyand Ms Shirley Kraft for administrative assistancein manuscript preparation The authors also thankLifeNet Health for providing the bone allograft usedin this study This trial was registered at ClinicalTrialsgov (NCT02154386) The authors report no conflictsof interest related to this study
REFERENCES1 Lekholm U Grondahl K Jemt T Outcome of oral
implant treatment in partially edentulous jaws followed20 years in clinical function Clin Implant Dent RelatRes 20068178-186
2 Van der Weijden F DellrsquoAcqua F Slot DE Alveolarbone dimensional changes of post-extraction socketsin humans A systematic review J Clin Periodontol2009361048-1058
3 Cardaropoli D Tamagnone L Roffredo A Gaveglio LRelationship between the buccal bone plate thickness
and the healing of postextraction sockets withwithoutridge preservation Int J Periodontics Restorative Dent201434211-217
4 Iasella JM Greenwell H Miller RL et al Ridge preser-vation with freeze-dried bone allograft and a collagenmembrane compared to extraction alone for implantsite development A clinical and histologic study inhumans J Periodontol 200374990-999
5 Schropp L Wenzel A Kostopoulos L Karring T Bonehealing and soft tissue contour changes followingsingle-tooth extraction A clinical and radiographic12-month prospective study Int J Periodontics Re-storative Dent 200323313-323
6 Lekovic V Camargo PM Klokkevold PR et al Preser-vation of alveolar bone in extraction sockets usingbioabsorbable membranes J Periodontol 1998691044-1049
7 Frost N Banjar A Galloway P Huynh-BaGMealey BLThe decision-making process for ridge preservationprocedures after tooth extraction Clin Adv Periodon-tics 2014456-63
8 Avila-Ortiz G Elangovan S Kramer KW Blanchette DDawson DV Effect of alveolar ridge preservation aftertooth extraction A systematic review andmeta-analysisJ Dent Res 201493950-958
9 Chan HL Lin GH Fu JH Wang HL Alterations in bonequality after socket preservation with grafting mate-rials A systematic review Int J Oral Maxillofac Im-plants 201328710-720
10 Beck TM Mealey BL Histologic analysis of healingafter tooth extraction with ridge preservation usingmineralized human bone allograft J Periodontol 2010811765-1772
11 Wood RA Mealey BL Histologic comparison of healingafter tooth extraction with ridge preservation usingmineralized versus demineralized freeze-dried boneallograft J Periodontol 201283329-336
12 Borg TD Mealey BL Histologic healing following toothextraction with ridge preservation using mineralizedversus combinedmineralized-demineralized freeze-driedbone allograft A randomized controlled clinical trialJ Periodontol 201586348-355
13 Burchardt H The biology of bone graft repair ClinOrthop Relat Res 198317428-42
14 Goldberg VM Stevenson S Natural history of autograftsand allografts Clin Orthop Relat Res 19872257-16
15 UristMR StratesBSBonemorphogenetic protein JDentRes 1971501392-1406
16 Shigeyama Y DrsquoErrico JA Stone R Somerman MJCommercially-prepared allograft material has bi-ological activity in vitro J Periodontol 199566478-487
17 Schwartz Z Mellonig JT Carnes DL Jr et al Ability ofcommercial demineralized freeze-dried bone allograftto induce new bone formation J Periodontol 199667918-926
18 Adell R LekholmU Rockler B Branemark PI A 15-yearstudy of osseointegrated implants in the treatment of theedentulous jaw Int J Oral Surg 198110387-416
19 Paolantonio M Dolci M Scarano A et al Immediateimplantation in fresh extraction sockets A controlledclinical and histological study in man J Periodontol2001721560-1571
20 Quirynen M Van Assche N Botticelli D Berglundh THow does the timing of implant placement to extractionaffect outcome Int J Oral Maxillofac Implants 200722(Suppl)203-223
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1028
21 Cooper LF Reside GJ Raes F et al Immediateprovisionalization of dental implants placed in healedalveolar ridges and extraction sockets A 5-year pro-spective evaluation Int J Oral Maxillofac Implants201429709-717
22 Kinaia BM Shah M Neely AL Goodis HE Crestal bonelevel changes around immediately placed implants Asystematic review and meta-analyses with at least 12monthsrsquo follow-up after functional loading J Peri-odontol 2014851537-1548
23 Waasdorp JA Evian CI Mandracchia M Immediateplacement of implants into infected sites A systematicreview of the literature J Periodontol 201081801-808
24 Fugazzotto P A retrospective analysis of immediatelyplaced implants in 418 sites exhibiting periapicalpathology Results and clinical considerations Int JOral Maxillofac Implants 201227194-202
25 Fugazzotto PA A retrospective analysis of implantsimmediately placed in sites with and without periapicalpathology in sixty-four patients J Periodontol 201283182-186
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 statement Updated guidelines for
reporting parallel group randomized trials Ann InternMed 2010152726-732
27 Hoang TN Mealey BL Histologic comparison of heal-ing after ridge preservation using human demineralizedbone matrix putty with one versus two different-sizedbone particles J Periodontol 201283174-181
28 Cook DC Mealey BL Histologic comparison of healingfollowing tooth extraction with ridge preservation usingtwo different xenograft protocols J Periodontol 201384585-594
29 Eskow AJ Mealey BL Evaluation of healing followingtooth extraction with ridge preservation using corticalversus cancellous freeze-dried bone allograft J Peri-odontol 201485514-524
Correspondence Dr Brian L Mealey University of TexasHealth Science Center San Antonio Department of Peri-odontics MSC 7894 7703 Floyd Curl Drive San AntonioTX 78229-3900 Fax 210-567-3761 e-mail mealeyuthscsaedu
Submitted March 4 2016 accepted for publication April13 2016
J Periodontol bull September 2016 Whetman Mealey
1029

FDBA (DFDBA) are well-supported common prod-ucts used to reduce changes in ridge dimension aftertooth extraction and provide adequate new vital bonefor implant placement410-12 FDBA maintains socketspace and acts as a scaffold for host osteoprogenitorcells during the healing phase1314 However thedemineralization process of DFDBA additionally re-leases bone morphogenetic proteins (BMPs)1516
Released BMPs give the allograft the added benefit ofosteoinductivity17 FDBA contains these same BMPshowever they remain sequestered in graft materialaway from osteoprogenitor cells until demineralizationoccurs in situ Available BMPs in DFDBA stimulatehost osteoprogenitor cells to differentiate into osteo-blasts and begin new bone formation Wood andMealey11 reported an increase in new vital bone for-mation in ridge preservation using DFDBA comparedwith FDBA Borg and Mealey12 also showed a com-bination FDBADFDBA grafting material increasedvital bone formation compared with FDBA alone
Dental implant placement timing after ridge pres-ervation continues to be a controversial topic Patientsand practitioners are continually searching for waysto expedite the process of dental implant therapyBranemarkrsquos original protocol of endosteal root-formdental implant placement recommended at least 12months of healing time after tooth extraction prior toimplant placement18 This process can be shortenedin two areas 1) extraction to implant placement and2) implant placement to implant restoration Imme-diate placement protocols continue to receive supportfrom the scientific literature with regard to success andpredictability compared with conventional placementtechniques19-22 Even in the presence of periapicalpathology extraction and immediate implant place-ment remains a successful and comparable treatmentto implants placed in healed ridges23-25 Beck andMealey10 allowed ridges to heal after extraction andridge preservation with a mineralized allograft for 3and 6 months Histologically there was no differencein new vital bone formation between 3- and 6-monthpostextraction healing periods suggesting that im-plant placement at either time point would be ap-propriate However bone used in that study was notprocessed in the samemanner (ie via freeze-drying)as the bone allograft used in the current study
To the best of the authorsrsquo knowledge few studieshave histologically evaluated healing of ridge pres-ervation grafts at differing time points Therefore thepurpose of this study is to evaluate differences inhealing after tooth extraction and ridge preservation ofnon-molar teeth using DFDBA at 8 to 10 weeks ofhealing compared with 18 to 20 weeks of healing Theprimary objective of this study is to histologicallycompare amounts of new vital bone formation re-sidual graft material and connective tissue (CT)other
present Secondary objectives include comparing di-mensional changes in ridge height and width aftertooth extraction and ridge preservation with DFDBA
MATERIALS AND METHODS
Participant EnrollmentThe Institutional Review Board of the University of TexasHealth Science Center at San Antonio (UTHSCSA) SanAntonio TX reviewed and approved the researchprotocol This parallel arm clinical trial was registeredat ClinicalTrialsgov (NCT02154386) and conductedin accordance with the Helsinki Declaration of 1975as revised in 2013 To reach statistical power to detecta significant mean difference of at least one standarddeviation (SD) in percentage of new vital bone for-mation using MannndashWhitney U test with a power of885 at a 005 level a sample size of at least 14 ridgepreservation sites was required per healing periodOther studies by the authorsrsquo group have demon-strated SDs ranging from 119 to 224 for per-centage of vital bone formation10-12 To accommodatea potential 30 dropout rate 46 patients (21 malesand 25 females aged 23 to 81 years mean age 557years) were enrolled from October 2013 to December2014 (Fig 1)26 Patient inclusion criteria comprisedthe following 1) single-rooted teeth needing extrac-tion 2) patient desiring restoration with a dental im-plant 3) at least 10 mm of apicocoronal bone heightfrom vital anatomic structures 4) adequate space forrestoration 5) root of tooth in a spatial orientation suchthat a restoratively driven implant position could beobtained that was totally within the former socket areathus including only grafted bone in the biopsy core 6)less than 50 dehiscence after tooth extraction Ex-clusion criteria were 1) patients not fulfilling inclusioncriteria or not compliant with necessary proceduralfollow-up 2) pregnancy 3) active systemiclocal in-fection not including periodontitis 4) medical condi-tions or medications known to alter soft tissue orbony healing (poorly controlled diabetesmellitus [DM]bisphosphonates immunosuppressives etc) 5) teethwith short roots or roots that were malpositioned suchthat the core biopsy might include bone along thesocket wall Females of childbearing age without tuballigation menopause or hysterectomy were required tohave a negative pregnancy test prior to surgery
DFDBA used for all patients in the study wasprocured from a single donor a 42-year-oldmale andhad residual calcium content of 26 and a particlesize of 250 to 1000 microns Osteoinductivity wastested in vivo by implantation into a gluteal musclepouch of an athymic mousedagger and was scored aspercentage of new bone formation in the whole im-planted area (grade of 0 to 4) DFDBA used in thisstudy received a grade of 2 out of 4 corresponding
dagger WuXi AppTec St Paul MN
J Periodontol bull September 2016 Whetman Mealey
1023
with an area of new bone formation between 1 and25 of total area of implanted bone product
Surgical ProtocolAfter enrollment custom thermoplastic acrylic mea-suring stentsDagger were made from alginate impressionsand stone casts for each patient Mucoperiosteal flapswere reflected no more than 2 to 3 mm beyond thecrest of the alveolus and the tooth was extractedAfter thorough debridement and irrigation presenceor absence and extent of dehiscence and number ofbony walls were recorded Clinical measurementswere made using a periodontal probesect with a customacrylic measuring stent Measurements included 1)depth of socket on buccal and lingual sides 2) buccaland lingual alveolar crest heights 3) buccal platethickness 1 mm apical to alveolar crest using a dentalcaliperi and 4) total ridge width 4 mm apical to al-veolar crest using a ridge caliperpara All measurements
were made to the nearest 05 mmexcept buccal plate thicknesswhich was measured to the nearest01mm To facilitate reproducibilityholes in the acrylic measuring stentwere made directly over buccal andlingual plates and 4 mm apical tothe alveolar crest for ridge widthmeasurements After clinical mea-surements the ridge was preservedusing DFDBA
Bone graft material was hydratedwith sterile saline for 10 minutesand increments of bone graft ma-terial were placed in the extractionsocket to not overfill the socketIf dehiscence of 50 or less waspresent on the buccal or lingualplate the patient remained in thestudy and a collagen repair mem-brane was used to replace themissing bone wall No periosteal re-leasing incision was performed andprimary closure was not attemptedWhen no dehiscence was presenta collagen-orifice barrier was placedover the extraction socketdaggerdagger Thearea was sutured using 4-0 chromicgut sutures Where dehiscence wasgreater than 50 the patient wasexited from the study
After the surgical procedure wascompleted each patient was ran-domized into the short-term group(8 to 10 weeks of healing) or thelong-term group (18 to 20 weeks ofhealing) by random selection from
a group of opaque envelopes Each patient was pre-scribed 500 mg of amoxicillin three times daily for7 days and 012 chlorhexidine mouthrinse for plaquefor 30 seconds twice daily for 4 weeks If allergic topenicillin the patient was prescribed 100 mg ofdoxycycline twice daily for 7 days Postoperative painmanagement included non-steroidal anti-inflammatorydrugs and narcotic analgesics as indicated Each pa-tient was seen at 2 weeks and 4 weeks to monitorhealing and to remove plaque from surgical areas
At the appropriate randomized time point thepatient returned for the second surgical visit Upon
Figure 1Consolidated Standards of Reporting Trials (CONSORT)26 study flowchart
Dagger Clear Splint Biocryl 075mm125mm Round Great Lakes OrthodonticsTonawanda NY
sect UNC-15 periodontal probe G Hartzell amp Son Concord CAi Iwanson gauge Salvin Dental Specialties Charlotte NCpara Castroviejo ridge caliper Salvin Dental Specialties LifeNet Health Virginia Beach VA Socket repair membrane Zimmer Dental Warsaw INdaggerdagger Oraplug Salvin Dental Specialties
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1024
mucoperiosteal flap reflection the custom acrylicstent of the patient was used to obtain clinical mea-surements in the same manner namely buccal andlingual alveolar crest heights and ridge width Anyresidual socket defect was measured to the nearestmillimeter A 20-mm internal diameter30-mm ex-ternal diameter trephine drillDaggerDagger with depth indicatormarkings was used to obtain a core biopsy at least8 mm in length and initiate the osteotomy for implantplacement The bone biopsy was placed in 10 neu-tral buffered formalin solution The remaining os-teotomy was completed according to the protocolof the manufacturer to receive an appropriate sizediameter and length implant Any additional bonyaugmentation was recorded and performed If ridgewidth was unable to accommodate implant place-ment the implant was not placed and the ridge wasaugmented at the discretion of the operator Thepatient was seen at 7 to 10 days postoperatively andfor a prerestorative check at approximately 3 months
Histologic Processing and AnalysesHistologic processing was completed as described inother studies conducted by the authorsrsquo researchgroup10-12 Briefly bone cores were removed fromtrephines and placed directly into 10 neutral buff-ered formalin Cores were decalcified dehydratedembedded in paraffin and sectioned to 4-mm-thicksections for histomorphometric analysis Tissue wasstained with a routine staining procedure of hema-toxylin and counterstained with a slightly acidifiedcombination of orange G and eosin Y with acidfuchsinsectsect
Histomorphometric analysis was performed ina similar manner as done by the authorsrsquo group inprevious studies10-12 The sole examiner (JW) wasmasked to treatment groups during the analysisprocess A minimum of nine sections were made foreach core Each section was examined at 1middot todetermine which provided the best section for high-power evaluation with preference given to the in-nermost section of the core whenever possible Thesection was examined at power between 20middot and 40middotmagnification in its entiretyii to ensure accurateanalysis of new vital bone residual graft and CTother Residual graft particles were identified as re-gions of lamellar bone having lacunae without pres-ence of osteocytes vital bone was identified by thepresence of osteocytes in lacunae CTother includedvasculature loose fibrous CT and inflammatory cellsOnce the core was separated into its respectivecomponents (vital bone residual graft and CTother)using image editing softwareparapara separated imageswere converted to a binary black and white image
Total number of pixels was calculated and summedfor each image and percentage of pixels for each
image was calculated to find percentage area of eachcomponent of bone core
Statistical Analyses Each study participant con-tributed a single value of each outcome variable tostatistical analysis A two-sample Student t test wasperformed for histologic outcomes as well as clinicalridge dimensional changes to evaluate differencesbetween the two treatment groups Box plots wereused to assess whether parametric statistical tests wereappropriate In the event of extreme outliers or sig-nificant departures from symmetry MannndashWhitney Utests were performed to confirm findings from Studentt tests To evaluate treatment group differences in archlocation of site presence or absence of a dehiscenceat extraction toothbound versus non-toothboundextraction site and need for additional grafting atthe time of implant placement Fisher exact testswere performed For all statistical analyses P lt005 wasconsidered significant Spearman rank and Pearsoncorrelations between clinical and histologic parameterswere also analyzed
RESULTS
Of 46 patients enrolled two patients consented toparticipate and subsequently elected to withdrawfrom the study (Fig 1) After extraction one patientstarted treatment with a medication (teriparatide)known to alter bone metabolism and was exited fromthe study There was one smoker in each group Fourpatients had well-controlled DM two from eachgroup Of the 43 patients who completed the study41 core biopsies were taken After healing one pa-tient in the long-term group had inadequate ridgewidth for core biopsy and implant placement how-ever ridge dimensional changes were recorded Onepatient had poor quality bone core that could not becontained for processing but an implant was suc-cessfully placed Thus 42 of 43 patients who re-ceived extraction and ridge preservation had implantsplaced successfully Of 41 core biopsies taken twowere lost to processing one from each group In theshort-term group clinical data were collected to per-form dimensional analysis for all 22 patients In thelong-term group data for ridge dimensional analysiswere collected for 19 of 21 patients In this group thecustomized acrylic measuring stent was lost for onepatient and clinical measurements were not made atthe implant surgery for the other patient
The short-term group healed for a mean of 903 ndash069 weeks and the long-term group healed fora mean of 1911 ndash 087 weeks At baseline sites in
DaggerDagger Salvin Dental Specialtiessectsect Treosin Statlab Medical Products McKinney TXii CellSens Version 14 software Olympus Center Valley PAparapara Adobe Photoshop CS51 Adobe San Jose CA ImageJ National Institutes of Health Bethesda MD
J Periodontol bull September 2016 Whetman Mealey
1025
both groups were similar Fisher exact test found nosignificant differences for study sites between groupsHowever there was a statistically significant differ-ence in buccal plate thickness between the twogroups (P = 0001) Mean buccal plate thickness inthe short-term group was 0614 ndash 0273 mm com-pared with 1010 ndash 0446mm in the long-term groupMost sites were maxillary sites with 14 in the short-term group and 13 in the long-term group There wasno significant difference in initial ridge width betweenthe two treatment groups (P = 051) The short-termgroup had a mean initial ridge width of 939 ndash169 mm compared with 978 ndash 205 mm in the long-term group
Histologic ObservationsVital bone was identified as areas of bone with oste-ocytes occupying lacunae and was most often wovenbone (Fig 2) Residual graft particles were identifiedas areas of primarily lamellar bone and no osteocytesoccupying the lacunae Apposition of new vital boneon residual graft particles was often noted The lastcategory was CTother which comprised loose fi-brovascular CT
There was a significantly different percentage newvital bone between the short-term group and thelong-term group (P = 001) The short-term grouphad a mean of 3263 vital bone compared with4741 in the long-term group (Table 1) With regardto percentage residual graft there was no significantdifference between treatment groups (test = 3742control = 2680) however it did trend towardstatistical significance (P = 006) There was no sig-nificant difference among treatment groups with re-gard to fraction of CTother (P = 042) A Fisher exact
test showed no significant difference in percentagenew vital bone among sites in the maxillary archcompared with sites in the mandibular arch (P = 043)anterior versus posterior tooth position (P = 074) andpresence or absence of a dehiscence at the time ofextraction (P = 057)
Dimensional ChangesIn analyzing ridge dimensional changes no statis-tically significant differences were found betweentreatment groups (Table 2) Specifically there wasno statistical difference in ridge width change (P =021) buccal ridge height change (P = 029) orlingual ridge height change (P gt099) Mean decreasein ridge width was 141 mm in the short-term groupand 066 mm in the long-term group Mean loss ofbuccal and lingual ridge height was between 084 and182 mm No significant correlation was found be-tween buccal plate thickness at time of extraction andfinal ridge width change
DISCUSSION
The primary objective of this study is to evaluate effectof healing time on new bone formation after ridgepreservation with DFDBA specifically at time pointsaveraging 9 weeks and 19 weeks after tooth extrac-tion Significantly more new vital bone was found inthe long-term healing group compared with the short-term healing group with no significant differences inridge dimensional changes between groups
This study design which has been used by theauthorsrsquo research group before10-12 eliminates manypotential confounding variables by 1) utilizing a singledonor as the source of bone graft material for bothexperimental groups 2) testing osteoinductivity ofallograft material 3) including only sites with at least10 mm of socket depth and root angulation similar tothe desired final implant position and 4) using stan-dardized custom acrylic stents to compare ridge di-mensional change This allowed direct comparison ofnew vital bone formation between the two groups withfew confounding variables There is great variabilityamong donors and among processing lots of demin-eralized bone allografts17 Using bone derived from thesame donor and having the same residual calciumcontent allowed for comparison between groupswithout concern for donor and processing variabilityIncluding only sites with 10 mm of radiographic bonesupport and root orientation similar to the plannedrestoratively driven implant placement eliminated thepotential of including native bone in core biopsieswhich could confound histomorphometric analysis ofpercentage new bone formation10-1227-29
Wood and Mealey11 also used DFDBA in ridgepreservation and found an average of 3243 newvital bone formation 20 weeks after grafting In the
Figure 2Long-term healing group (Hematoxylin and counterstained withacidified combination of eosin-Y orange-G and acid fuchsin originalmagnification middot10) VB = vital bone RG = residual graft
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1026
current study using DFDBA an average new vitalbone formation of 4741 was found after 19 weeksof healing This result coincides with knowledge ofdonor variability as the in vivo inductivity score ofDFDBA used by Wood and Mealey11 was graded as 1on a scale of 0 to 4 compared with an inductivityscore of 2 on the same scale for DFDBA used in thecurrent study Thus when an allograft with higherinductivity was used after essentially the same amountof wound healing time more new vital bone formationwas found
Borg and Mealey12 compared ridge preservationwith an allograft consisting of 100 mineralizedFDBA to a combination allograft with a ratio of 30DFDBA70 FDBA at 19 weeks of healing The donorinductivity score for graft material in that study wasgraded as 3 of 4 and mean new vital bone formationwas 3616 in the combination allograft group Thiswas significantly more new bone formation comparedwith the group grafted with FDBA alone (247) andvery similar to 3243 new vital bone formation fromWood and Mealeyrsquos11 study using 100 DFDBA It ispossible that the higher inductivity of DFDBA in theBorg and Mealey12 study resulted in induction of newvital bone formation equivalent to that in Wood andMealeyrsquos11 study despite the demineralized allograftmaking up only 30 of the graft material in the formerstudy compared with 100 DFDBA in the latter Inconsidering these studies and the current studyDFDBA results in significantly greater formation ofnew vital bone after ridge preservation comparedwith FDBA
The significance of new vital bone formation onimplant survival and success is unclear at this pointIntuitively a higher percentage of new vital bone isdesirable as increased vital bonemay increase bone-to-implant contact or at least increase the rate at whichthe implant achieves stability andmaximum bone-to-implant contact However the authors are unawareof published literature clearly demonstrating thatpercentage of vital bone at an implant site directlyaffects implant survival or success including bone-to-implant contact esthetics or peri-implant boneloss
When an implant osteotomy is prepared tactilesensation may give the operator a subjective senseof bone density at the site At sites that have hadridge preservation is it often difficult to assessquality of bone at the grafted site during implantosteotomy or placement The authors of the currentstudy noted great variability in both treatmentgroups with some sites in each group having poordensity and others having good density It is theauthorsrsquo opinion that poor bone quality at the time ofcore biopsy and osteotomy preparation was morecommon in the short-term healing group than in thelong-term healing group It is important to note thathistomorphometric analysis showed wide variabilityin percentage of new vital bone residual graft mate-rial and CTother with large standard deviations foreach parameter in both groups Therefore subjectivedifferences in density during osteotomy preparationmay be reflective of actual differences in percentageCTother new vital bone or residual graft material
Table 1
Histologic Analysis ()
Groups
Vital Bone
Mean ndash SD
Residual Graft
Mean ndash SD
CTOther
Mean ndash SD
Test group (short-term healing group) 3263 ndash 2145 3742 ndash 1853dagger 2994 ndash 1751
Control group (long-term healing group) 4741 ndash 1166 2680 ndash 1520dagger 2578 ndash 1382
P = 001 for test group versus controldagger P = 006 for test group versus control
Table 2
Alveolar Ridge Dimensional Changes
Groups
Change in Ridge
Width Mean ndash SD
Change in Ridge
Width (mm)
Mean ndash SD
Change in Ridge
Height Buccal (mm)
Mean ndash SD
Change in Ridge
Height Lingual (mm)
Mean ndash SD
Test group (short-term healing group) -1393 ndash 2036 -141 ndash 211 -182 ndash 223 -084 ndash 148
Control group (long-term healing group) -745 ndash 1658 -066 ndash 155 -118 ndash 131 -084 ndash 096
No significant difference between groups for any measurements (P gt005)
J Periodontol bull September 2016 Whetman Mealey
1027
among patients No attempt was made in this studyto correlate objective histomorphometric data withsubjective assessment of bone density during os-teotomy preparation
Cardaropoli et al3 reported a meaningful negativecorrelation between baseline buccal plate thicknessand ridge width change at sites receiving tooth ex-traction but no ridge preservation procedures Thussites with a thinner buccal plate had greater loss ofridge width At baseline in the current study therewas a significant difference of approximately 04 mmin buccal plate thickness between treatment groupsHowever difference in loss of ridge width betweengroups was not statistically significant There wasalso no meaningful correlation between buccal platethickness and ridge dimensional changes It is pos-sible that use of a ridge preservation bone graftcounteracts the impact of a thin buccal plate on loss ofridge width after tooth extraction Other studies per-formed by the authorsrsquo research group also showed nomeaningful correlation between initial buccal platethickness and change in ridge width when ridge pres-ervation grafting was performed10-1227-29
CONCLUSIONS
The current study indicates there is significantly greaternew vital bone formation after tooth extraction andridge preservation with DFDBAwhen the clinician waits19 weeks prior to dental implant placement comparedwith only 9 weeks In addition there is no difference inridge dimensional change between sites healing for anaverage of 9 weeks compared with 19 weeks
ACKNOWLEDGMENTS
The authors thank Dr Michael Mills Dr David Lashoand Dr Kevin Gureckis UTHSCSA for their help inthe design and completion of this project The au-thors thank Ms Sonja A Bustamante at UTHSCSAfor the excellent histology provided for the studyand Ms Shirley Kraft for administrative assistancein manuscript preparation The authors also thankLifeNet Health for providing the bone allograft usedin this study This trial was registered at ClinicalTrialsgov (NCT02154386) The authors report no conflictsof interest related to this study
REFERENCES1 Lekholm U Grondahl K Jemt T Outcome of oral
implant treatment in partially edentulous jaws followed20 years in clinical function Clin Implant Dent RelatRes 20068178-186
2 Van der Weijden F DellrsquoAcqua F Slot DE Alveolarbone dimensional changes of post-extraction socketsin humans A systematic review J Clin Periodontol2009361048-1058
3 Cardaropoli D Tamagnone L Roffredo A Gaveglio LRelationship between the buccal bone plate thickness
and the healing of postextraction sockets withwithoutridge preservation Int J Periodontics Restorative Dent201434211-217
4 Iasella JM Greenwell H Miller RL et al Ridge preser-vation with freeze-dried bone allograft and a collagenmembrane compared to extraction alone for implantsite development A clinical and histologic study inhumans J Periodontol 200374990-999
5 Schropp L Wenzel A Kostopoulos L Karring T Bonehealing and soft tissue contour changes followingsingle-tooth extraction A clinical and radiographic12-month prospective study Int J Periodontics Re-storative Dent 200323313-323
6 Lekovic V Camargo PM Klokkevold PR et al Preser-vation of alveolar bone in extraction sockets usingbioabsorbable membranes J Periodontol 1998691044-1049
7 Frost N Banjar A Galloway P Huynh-BaGMealey BLThe decision-making process for ridge preservationprocedures after tooth extraction Clin Adv Periodon-tics 2014456-63
8 Avila-Ortiz G Elangovan S Kramer KW Blanchette DDawson DV Effect of alveolar ridge preservation aftertooth extraction A systematic review andmeta-analysisJ Dent Res 201493950-958
9 Chan HL Lin GH Fu JH Wang HL Alterations in bonequality after socket preservation with grafting mate-rials A systematic review Int J Oral Maxillofac Im-plants 201328710-720
10 Beck TM Mealey BL Histologic analysis of healingafter tooth extraction with ridge preservation usingmineralized human bone allograft J Periodontol 2010811765-1772
11 Wood RA Mealey BL Histologic comparison of healingafter tooth extraction with ridge preservation usingmineralized versus demineralized freeze-dried boneallograft J Periodontol 201283329-336
12 Borg TD Mealey BL Histologic healing following toothextraction with ridge preservation using mineralizedversus combinedmineralized-demineralized freeze-driedbone allograft A randomized controlled clinical trialJ Periodontol 201586348-355
13 Burchardt H The biology of bone graft repair ClinOrthop Relat Res 198317428-42
14 Goldberg VM Stevenson S Natural history of autograftsand allografts Clin Orthop Relat Res 19872257-16
15 UristMR StratesBSBonemorphogenetic protein JDentRes 1971501392-1406
16 Shigeyama Y DrsquoErrico JA Stone R Somerman MJCommercially-prepared allograft material has bi-ological activity in vitro J Periodontol 199566478-487
17 Schwartz Z Mellonig JT Carnes DL Jr et al Ability ofcommercial demineralized freeze-dried bone allograftto induce new bone formation J Periodontol 199667918-926
18 Adell R LekholmU Rockler B Branemark PI A 15-yearstudy of osseointegrated implants in the treatment of theedentulous jaw Int J Oral Surg 198110387-416
19 Paolantonio M Dolci M Scarano A et al Immediateimplantation in fresh extraction sockets A controlledclinical and histological study in man J Periodontol2001721560-1571
20 Quirynen M Van Assche N Botticelli D Berglundh THow does the timing of implant placement to extractionaffect outcome Int J Oral Maxillofac Implants 200722(Suppl)203-223
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1028
21 Cooper LF Reside GJ Raes F et al Immediateprovisionalization of dental implants placed in healedalveolar ridges and extraction sockets A 5-year pro-spective evaluation Int J Oral Maxillofac Implants201429709-717
22 Kinaia BM Shah M Neely AL Goodis HE Crestal bonelevel changes around immediately placed implants Asystematic review and meta-analyses with at least 12monthsrsquo follow-up after functional loading J Peri-odontol 2014851537-1548
23 Waasdorp JA Evian CI Mandracchia M Immediateplacement of implants into infected sites A systematicreview of the literature J Periodontol 201081801-808
24 Fugazzotto P A retrospective analysis of immediatelyplaced implants in 418 sites exhibiting periapicalpathology Results and clinical considerations Int JOral Maxillofac Implants 201227194-202
25 Fugazzotto PA A retrospective analysis of implantsimmediately placed in sites with and without periapicalpathology in sixty-four patients J Periodontol 201283182-186
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 statement Updated guidelines for
reporting parallel group randomized trials Ann InternMed 2010152726-732
27 Hoang TN Mealey BL Histologic comparison of heal-ing after ridge preservation using human demineralizedbone matrix putty with one versus two different-sizedbone particles J Periodontol 201283174-181
28 Cook DC Mealey BL Histologic comparison of healingfollowing tooth extraction with ridge preservation usingtwo different xenograft protocols J Periodontol 201384585-594
29 Eskow AJ Mealey BL Evaluation of healing followingtooth extraction with ridge preservation using corticalversus cancellous freeze-dried bone allograft J Peri-odontol 201485514-524
Correspondence Dr Brian L Mealey University of TexasHealth Science Center San Antonio Department of Peri-odontics MSC 7894 7703 Floyd Curl Drive San AntonioTX 78229-3900 Fax 210-567-3761 e-mail mealeyuthscsaedu
Submitted March 4 2016 accepted for publication April13 2016
J Periodontol bull September 2016 Whetman Mealey
1029

with an area of new bone formation between 1 and25 of total area of implanted bone product
Surgical ProtocolAfter enrollment custom thermoplastic acrylic mea-suring stentsDagger were made from alginate impressionsand stone casts for each patient Mucoperiosteal flapswere reflected no more than 2 to 3 mm beyond thecrest of the alveolus and the tooth was extractedAfter thorough debridement and irrigation presenceor absence and extent of dehiscence and number ofbony walls were recorded Clinical measurementswere made using a periodontal probesect with a customacrylic measuring stent Measurements included 1)depth of socket on buccal and lingual sides 2) buccaland lingual alveolar crest heights 3) buccal platethickness 1 mm apical to alveolar crest using a dentalcaliperi and 4) total ridge width 4 mm apical to al-veolar crest using a ridge caliperpara All measurements
were made to the nearest 05 mmexcept buccal plate thicknesswhich was measured to the nearest01mm To facilitate reproducibilityholes in the acrylic measuring stentwere made directly over buccal andlingual plates and 4 mm apical tothe alveolar crest for ridge widthmeasurements After clinical mea-surements the ridge was preservedusing DFDBA
Bone graft material was hydratedwith sterile saline for 10 minutesand increments of bone graft ma-terial were placed in the extractionsocket to not overfill the socketIf dehiscence of 50 or less waspresent on the buccal or lingualplate the patient remained in thestudy and a collagen repair mem-brane was used to replace themissing bone wall No periosteal re-leasing incision was performed andprimary closure was not attemptedWhen no dehiscence was presenta collagen-orifice barrier was placedover the extraction socketdaggerdagger Thearea was sutured using 4-0 chromicgut sutures Where dehiscence wasgreater than 50 the patient wasexited from the study
After the surgical procedure wascompleted each patient was ran-domized into the short-term group(8 to 10 weeks of healing) or thelong-term group (18 to 20 weeks ofhealing) by random selection from
a group of opaque envelopes Each patient was pre-scribed 500 mg of amoxicillin three times daily for7 days and 012 chlorhexidine mouthrinse for plaquefor 30 seconds twice daily for 4 weeks If allergic topenicillin the patient was prescribed 100 mg ofdoxycycline twice daily for 7 days Postoperative painmanagement included non-steroidal anti-inflammatorydrugs and narcotic analgesics as indicated Each pa-tient was seen at 2 weeks and 4 weeks to monitorhealing and to remove plaque from surgical areas
At the appropriate randomized time point thepatient returned for the second surgical visit Upon
Figure 1Consolidated Standards of Reporting Trials (CONSORT)26 study flowchart
Dagger Clear Splint Biocryl 075mm125mm Round Great Lakes OrthodonticsTonawanda NY
sect UNC-15 periodontal probe G Hartzell amp Son Concord CAi Iwanson gauge Salvin Dental Specialties Charlotte NCpara Castroviejo ridge caliper Salvin Dental Specialties LifeNet Health Virginia Beach VA Socket repair membrane Zimmer Dental Warsaw INdaggerdagger Oraplug Salvin Dental Specialties
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1024
mucoperiosteal flap reflection the custom acrylicstent of the patient was used to obtain clinical mea-surements in the same manner namely buccal andlingual alveolar crest heights and ridge width Anyresidual socket defect was measured to the nearestmillimeter A 20-mm internal diameter30-mm ex-ternal diameter trephine drillDaggerDagger with depth indicatormarkings was used to obtain a core biopsy at least8 mm in length and initiate the osteotomy for implantplacement The bone biopsy was placed in 10 neu-tral buffered formalin solution The remaining os-teotomy was completed according to the protocolof the manufacturer to receive an appropriate sizediameter and length implant Any additional bonyaugmentation was recorded and performed If ridgewidth was unable to accommodate implant place-ment the implant was not placed and the ridge wasaugmented at the discretion of the operator Thepatient was seen at 7 to 10 days postoperatively andfor a prerestorative check at approximately 3 months
Histologic Processing and AnalysesHistologic processing was completed as described inother studies conducted by the authorsrsquo researchgroup10-12 Briefly bone cores were removed fromtrephines and placed directly into 10 neutral buff-ered formalin Cores were decalcified dehydratedembedded in paraffin and sectioned to 4-mm-thicksections for histomorphometric analysis Tissue wasstained with a routine staining procedure of hema-toxylin and counterstained with a slightly acidifiedcombination of orange G and eosin Y with acidfuchsinsectsect
Histomorphometric analysis was performed ina similar manner as done by the authorsrsquo group inprevious studies10-12 The sole examiner (JW) wasmasked to treatment groups during the analysisprocess A minimum of nine sections were made foreach core Each section was examined at 1middot todetermine which provided the best section for high-power evaluation with preference given to the in-nermost section of the core whenever possible Thesection was examined at power between 20middot and 40middotmagnification in its entiretyii to ensure accurateanalysis of new vital bone residual graft and CTother Residual graft particles were identified as re-gions of lamellar bone having lacunae without pres-ence of osteocytes vital bone was identified by thepresence of osteocytes in lacunae CTother includedvasculature loose fibrous CT and inflammatory cellsOnce the core was separated into its respectivecomponents (vital bone residual graft and CTother)using image editing softwareparapara separated imageswere converted to a binary black and white image
Total number of pixels was calculated and summedfor each image and percentage of pixels for each
image was calculated to find percentage area of eachcomponent of bone core
Statistical Analyses Each study participant con-tributed a single value of each outcome variable tostatistical analysis A two-sample Student t test wasperformed for histologic outcomes as well as clinicalridge dimensional changes to evaluate differencesbetween the two treatment groups Box plots wereused to assess whether parametric statistical tests wereappropriate In the event of extreme outliers or sig-nificant departures from symmetry MannndashWhitney Utests were performed to confirm findings from Studentt tests To evaluate treatment group differences in archlocation of site presence or absence of a dehiscenceat extraction toothbound versus non-toothboundextraction site and need for additional grafting atthe time of implant placement Fisher exact testswere performed For all statistical analyses P lt005 wasconsidered significant Spearman rank and Pearsoncorrelations between clinical and histologic parameterswere also analyzed
RESULTS
Of 46 patients enrolled two patients consented toparticipate and subsequently elected to withdrawfrom the study (Fig 1) After extraction one patientstarted treatment with a medication (teriparatide)known to alter bone metabolism and was exited fromthe study There was one smoker in each group Fourpatients had well-controlled DM two from eachgroup Of the 43 patients who completed the study41 core biopsies were taken After healing one pa-tient in the long-term group had inadequate ridgewidth for core biopsy and implant placement how-ever ridge dimensional changes were recorded Onepatient had poor quality bone core that could not becontained for processing but an implant was suc-cessfully placed Thus 42 of 43 patients who re-ceived extraction and ridge preservation had implantsplaced successfully Of 41 core biopsies taken twowere lost to processing one from each group In theshort-term group clinical data were collected to per-form dimensional analysis for all 22 patients In thelong-term group data for ridge dimensional analysiswere collected for 19 of 21 patients In this group thecustomized acrylic measuring stent was lost for onepatient and clinical measurements were not made atthe implant surgery for the other patient
The short-term group healed for a mean of 903 ndash069 weeks and the long-term group healed fora mean of 1911 ndash 087 weeks At baseline sites in
DaggerDagger Salvin Dental Specialtiessectsect Treosin Statlab Medical Products McKinney TXii CellSens Version 14 software Olympus Center Valley PAparapara Adobe Photoshop CS51 Adobe San Jose CA ImageJ National Institutes of Health Bethesda MD
J Periodontol bull September 2016 Whetman Mealey
1025
both groups were similar Fisher exact test found nosignificant differences for study sites between groupsHowever there was a statistically significant differ-ence in buccal plate thickness between the twogroups (P = 0001) Mean buccal plate thickness inthe short-term group was 0614 ndash 0273 mm com-pared with 1010 ndash 0446mm in the long-term groupMost sites were maxillary sites with 14 in the short-term group and 13 in the long-term group There wasno significant difference in initial ridge width betweenthe two treatment groups (P = 051) The short-termgroup had a mean initial ridge width of 939 ndash169 mm compared with 978 ndash 205 mm in the long-term group
Histologic ObservationsVital bone was identified as areas of bone with oste-ocytes occupying lacunae and was most often wovenbone (Fig 2) Residual graft particles were identifiedas areas of primarily lamellar bone and no osteocytesoccupying the lacunae Apposition of new vital boneon residual graft particles was often noted The lastcategory was CTother which comprised loose fi-brovascular CT
There was a significantly different percentage newvital bone between the short-term group and thelong-term group (P = 001) The short-term grouphad a mean of 3263 vital bone compared with4741 in the long-term group (Table 1) With regardto percentage residual graft there was no significantdifference between treatment groups (test = 3742control = 2680) however it did trend towardstatistical significance (P = 006) There was no sig-nificant difference among treatment groups with re-gard to fraction of CTother (P = 042) A Fisher exact
test showed no significant difference in percentagenew vital bone among sites in the maxillary archcompared with sites in the mandibular arch (P = 043)anterior versus posterior tooth position (P = 074) andpresence or absence of a dehiscence at the time ofextraction (P = 057)
Dimensional ChangesIn analyzing ridge dimensional changes no statis-tically significant differences were found betweentreatment groups (Table 2) Specifically there wasno statistical difference in ridge width change (P =021) buccal ridge height change (P = 029) orlingual ridge height change (P gt099) Mean decreasein ridge width was 141 mm in the short-term groupand 066 mm in the long-term group Mean loss ofbuccal and lingual ridge height was between 084 and182 mm No significant correlation was found be-tween buccal plate thickness at time of extraction andfinal ridge width change
DISCUSSION
The primary objective of this study is to evaluate effectof healing time on new bone formation after ridgepreservation with DFDBA specifically at time pointsaveraging 9 weeks and 19 weeks after tooth extrac-tion Significantly more new vital bone was found inthe long-term healing group compared with the short-term healing group with no significant differences inridge dimensional changes between groups
This study design which has been used by theauthorsrsquo research group before10-12 eliminates manypotential confounding variables by 1) utilizing a singledonor as the source of bone graft material for bothexperimental groups 2) testing osteoinductivity ofallograft material 3) including only sites with at least10 mm of socket depth and root angulation similar tothe desired final implant position and 4) using stan-dardized custom acrylic stents to compare ridge di-mensional change This allowed direct comparison ofnew vital bone formation between the two groups withfew confounding variables There is great variabilityamong donors and among processing lots of demin-eralized bone allografts17 Using bone derived from thesame donor and having the same residual calciumcontent allowed for comparison between groupswithout concern for donor and processing variabilityIncluding only sites with 10 mm of radiographic bonesupport and root orientation similar to the plannedrestoratively driven implant placement eliminated thepotential of including native bone in core biopsieswhich could confound histomorphometric analysis ofpercentage new bone formation10-1227-29
Wood and Mealey11 also used DFDBA in ridgepreservation and found an average of 3243 newvital bone formation 20 weeks after grafting In the
Figure 2Long-term healing group (Hematoxylin and counterstained withacidified combination of eosin-Y orange-G and acid fuchsin originalmagnification middot10) VB = vital bone RG = residual graft
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1026
current study using DFDBA an average new vitalbone formation of 4741 was found after 19 weeksof healing This result coincides with knowledge ofdonor variability as the in vivo inductivity score ofDFDBA used by Wood and Mealey11 was graded as 1on a scale of 0 to 4 compared with an inductivityscore of 2 on the same scale for DFDBA used in thecurrent study Thus when an allograft with higherinductivity was used after essentially the same amountof wound healing time more new vital bone formationwas found
Borg and Mealey12 compared ridge preservationwith an allograft consisting of 100 mineralizedFDBA to a combination allograft with a ratio of 30DFDBA70 FDBA at 19 weeks of healing The donorinductivity score for graft material in that study wasgraded as 3 of 4 and mean new vital bone formationwas 3616 in the combination allograft group Thiswas significantly more new bone formation comparedwith the group grafted with FDBA alone (247) andvery similar to 3243 new vital bone formation fromWood and Mealeyrsquos11 study using 100 DFDBA It ispossible that the higher inductivity of DFDBA in theBorg and Mealey12 study resulted in induction of newvital bone formation equivalent to that in Wood andMealeyrsquos11 study despite the demineralized allograftmaking up only 30 of the graft material in the formerstudy compared with 100 DFDBA in the latter Inconsidering these studies and the current studyDFDBA results in significantly greater formation ofnew vital bone after ridge preservation comparedwith FDBA
The significance of new vital bone formation onimplant survival and success is unclear at this pointIntuitively a higher percentage of new vital bone isdesirable as increased vital bonemay increase bone-to-implant contact or at least increase the rate at whichthe implant achieves stability andmaximum bone-to-implant contact However the authors are unawareof published literature clearly demonstrating thatpercentage of vital bone at an implant site directlyaffects implant survival or success including bone-to-implant contact esthetics or peri-implant boneloss
When an implant osteotomy is prepared tactilesensation may give the operator a subjective senseof bone density at the site At sites that have hadridge preservation is it often difficult to assessquality of bone at the grafted site during implantosteotomy or placement The authors of the currentstudy noted great variability in both treatmentgroups with some sites in each group having poordensity and others having good density It is theauthorsrsquo opinion that poor bone quality at the time ofcore biopsy and osteotomy preparation was morecommon in the short-term healing group than in thelong-term healing group It is important to note thathistomorphometric analysis showed wide variabilityin percentage of new vital bone residual graft mate-rial and CTother with large standard deviations foreach parameter in both groups Therefore subjectivedifferences in density during osteotomy preparationmay be reflective of actual differences in percentageCTother new vital bone or residual graft material
Table 1
Histologic Analysis ()
Groups
Vital Bone
Mean ndash SD
Residual Graft
Mean ndash SD
CTOther
Mean ndash SD
Test group (short-term healing group) 3263 ndash 2145 3742 ndash 1853dagger 2994 ndash 1751
Control group (long-term healing group) 4741 ndash 1166 2680 ndash 1520dagger 2578 ndash 1382
P = 001 for test group versus controldagger P = 006 for test group versus control
Table 2
Alveolar Ridge Dimensional Changes
Groups
Change in Ridge
Width Mean ndash SD
Change in Ridge
Width (mm)
Mean ndash SD
Change in Ridge
Height Buccal (mm)
Mean ndash SD
Change in Ridge
Height Lingual (mm)
Mean ndash SD
Test group (short-term healing group) -1393 ndash 2036 -141 ndash 211 -182 ndash 223 -084 ndash 148
Control group (long-term healing group) -745 ndash 1658 -066 ndash 155 -118 ndash 131 -084 ndash 096
No significant difference between groups for any measurements (P gt005)
J Periodontol bull September 2016 Whetman Mealey
1027
among patients No attempt was made in this studyto correlate objective histomorphometric data withsubjective assessment of bone density during os-teotomy preparation
Cardaropoli et al3 reported a meaningful negativecorrelation between baseline buccal plate thicknessand ridge width change at sites receiving tooth ex-traction but no ridge preservation procedures Thussites with a thinner buccal plate had greater loss ofridge width At baseline in the current study therewas a significant difference of approximately 04 mmin buccal plate thickness between treatment groupsHowever difference in loss of ridge width betweengroups was not statistically significant There wasalso no meaningful correlation between buccal platethickness and ridge dimensional changes It is pos-sible that use of a ridge preservation bone graftcounteracts the impact of a thin buccal plate on loss ofridge width after tooth extraction Other studies per-formed by the authorsrsquo research group also showed nomeaningful correlation between initial buccal platethickness and change in ridge width when ridge pres-ervation grafting was performed10-1227-29
CONCLUSIONS
The current study indicates there is significantly greaternew vital bone formation after tooth extraction andridge preservation with DFDBAwhen the clinician waits19 weeks prior to dental implant placement comparedwith only 9 weeks In addition there is no difference inridge dimensional change between sites healing for anaverage of 9 weeks compared with 19 weeks
ACKNOWLEDGMENTS
The authors thank Dr Michael Mills Dr David Lashoand Dr Kevin Gureckis UTHSCSA for their help inthe design and completion of this project The au-thors thank Ms Sonja A Bustamante at UTHSCSAfor the excellent histology provided for the studyand Ms Shirley Kraft for administrative assistancein manuscript preparation The authors also thankLifeNet Health for providing the bone allograft usedin this study This trial was registered at ClinicalTrialsgov (NCT02154386) The authors report no conflictsof interest related to this study
REFERENCES1 Lekholm U Grondahl K Jemt T Outcome of oral
implant treatment in partially edentulous jaws followed20 years in clinical function Clin Implant Dent RelatRes 20068178-186
2 Van der Weijden F DellrsquoAcqua F Slot DE Alveolarbone dimensional changes of post-extraction socketsin humans A systematic review J Clin Periodontol2009361048-1058
3 Cardaropoli D Tamagnone L Roffredo A Gaveglio LRelationship between the buccal bone plate thickness
and the healing of postextraction sockets withwithoutridge preservation Int J Periodontics Restorative Dent201434211-217
4 Iasella JM Greenwell H Miller RL et al Ridge preser-vation with freeze-dried bone allograft and a collagenmembrane compared to extraction alone for implantsite development A clinical and histologic study inhumans J Periodontol 200374990-999
5 Schropp L Wenzel A Kostopoulos L Karring T Bonehealing and soft tissue contour changes followingsingle-tooth extraction A clinical and radiographic12-month prospective study Int J Periodontics Re-storative Dent 200323313-323
6 Lekovic V Camargo PM Klokkevold PR et al Preser-vation of alveolar bone in extraction sockets usingbioabsorbable membranes J Periodontol 1998691044-1049
7 Frost N Banjar A Galloway P Huynh-BaGMealey BLThe decision-making process for ridge preservationprocedures after tooth extraction Clin Adv Periodon-tics 2014456-63
8 Avila-Ortiz G Elangovan S Kramer KW Blanchette DDawson DV Effect of alveolar ridge preservation aftertooth extraction A systematic review andmeta-analysisJ Dent Res 201493950-958
9 Chan HL Lin GH Fu JH Wang HL Alterations in bonequality after socket preservation with grafting mate-rials A systematic review Int J Oral Maxillofac Im-plants 201328710-720
10 Beck TM Mealey BL Histologic analysis of healingafter tooth extraction with ridge preservation usingmineralized human bone allograft J Periodontol 2010811765-1772
11 Wood RA Mealey BL Histologic comparison of healingafter tooth extraction with ridge preservation usingmineralized versus demineralized freeze-dried boneallograft J Periodontol 201283329-336
12 Borg TD Mealey BL Histologic healing following toothextraction with ridge preservation using mineralizedversus combinedmineralized-demineralized freeze-driedbone allograft A randomized controlled clinical trialJ Periodontol 201586348-355
13 Burchardt H The biology of bone graft repair ClinOrthop Relat Res 198317428-42
14 Goldberg VM Stevenson S Natural history of autograftsand allografts Clin Orthop Relat Res 19872257-16
15 UristMR StratesBSBonemorphogenetic protein JDentRes 1971501392-1406
16 Shigeyama Y DrsquoErrico JA Stone R Somerman MJCommercially-prepared allograft material has bi-ological activity in vitro J Periodontol 199566478-487
17 Schwartz Z Mellonig JT Carnes DL Jr et al Ability ofcommercial demineralized freeze-dried bone allograftto induce new bone formation J Periodontol 199667918-926
18 Adell R LekholmU Rockler B Branemark PI A 15-yearstudy of osseointegrated implants in the treatment of theedentulous jaw Int J Oral Surg 198110387-416
19 Paolantonio M Dolci M Scarano A et al Immediateimplantation in fresh extraction sockets A controlledclinical and histological study in man J Periodontol2001721560-1571
20 Quirynen M Van Assche N Botticelli D Berglundh THow does the timing of implant placement to extractionaffect outcome Int J Oral Maxillofac Implants 200722(Suppl)203-223
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1028
21 Cooper LF Reside GJ Raes F et al Immediateprovisionalization of dental implants placed in healedalveolar ridges and extraction sockets A 5-year pro-spective evaluation Int J Oral Maxillofac Implants201429709-717
22 Kinaia BM Shah M Neely AL Goodis HE Crestal bonelevel changes around immediately placed implants Asystematic review and meta-analyses with at least 12monthsrsquo follow-up after functional loading J Peri-odontol 2014851537-1548
23 Waasdorp JA Evian CI Mandracchia M Immediateplacement of implants into infected sites A systematicreview of the literature J Periodontol 201081801-808
24 Fugazzotto P A retrospective analysis of immediatelyplaced implants in 418 sites exhibiting periapicalpathology Results and clinical considerations Int JOral Maxillofac Implants 201227194-202
25 Fugazzotto PA A retrospective analysis of implantsimmediately placed in sites with and without periapicalpathology in sixty-four patients J Periodontol 201283182-186
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 statement Updated guidelines for
reporting parallel group randomized trials Ann InternMed 2010152726-732
27 Hoang TN Mealey BL Histologic comparison of heal-ing after ridge preservation using human demineralizedbone matrix putty with one versus two different-sizedbone particles J Periodontol 201283174-181
28 Cook DC Mealey BL Histologic comparison of healingfollowing tooth extraction with ridge preservation usingtwo different xenograft protocols J Periodontol 201384585-594
29 Eskow AJ Mealey BL Evaluation of healing followingtooth extraction with ridge preservation using corticalversus cancellous freeze-dried bone allograft J Peri-odontol 201485514-524
Correspondence Dr Brian L Mealey University of TexasHealth Science Center San Antonio Department of Peri-odontics MSC 7894 7703 Floyd Curl Drive San AntonioTX 78229-3900 Fax 210-567-3761 e-mail mealeyuthscsaedu
Submitted March 4 2016 accepted for publication April13 2016
J Periodontol bull September 2016 Whetman Mealey
1029

mucoperiosteal flap reflection the custom acrylicstent of the patient was used to obtain clinical mea-surements in the same manner namely buccal andlingual alveolar crest heights and ridge width Anyresidual socket defect was measured to the nearestmillimeter A 20-mm internal diameter30-mm ex-ternal diameter trephine drillDaggerDagger with depth indicatormarkings was used to obtain a core biopsy at least8 mm in length and initiate the osteotomy for implantplacement The bone biopsy was placed in 10 neu-tral buffered formalin solution The remaining os-teotomy was completed according to the protocolof the manufacturer to receive an appropriate sizediameter and length implant Any additional bonyaugmentation was recorded and performed If ridgewidth was unable to accommodate implant place-ment the implant was not placed and the ridge wasaugmented at the discretion of the operator Thepatient was seen at 7 to 10 days postoperatively andfor a prerestorative check at approximately 3 months
Histologic Processing and AnalysesHistologic processing was completed as described inother studies conducted by the authorsrsquo researchgroup10-12 Briefly bone cores were removed fromtrephines and placed directly into 10 neutral buff-ered formalin Cores were decalcified dehydratedembedded in paraffin and sectioned to 4-mm-thicksections for histomorphometric analysis Tissue wasstained with a routine staining procedure of hema-toxylin and counterstained with a slightly acidifiedcombination of orange G and eosin Y with acidfuchsinsectsect
Histomorphometric analysis was performed ina similar manner as done by the authorsrsquo group inprevious studies10-12 The sole examiner (JW) wasmasked to treatment groups during the analysisprocess A minimum of nine sections were made foreach core Each section was examined at 1middot todetermine which provided the best section for high-power evaluation with preference given to the in-nermost section of the core whenever possible Thesection was examined at power between 20middot and 40middotmagnification in its entiretyii to ensure accurateanalysis of new vital bone residual graft and CTother Residual graft particles were identified as re-gions of lamellar bone having lacunae without pres-ence of osteocytes vital bone was identified by thepresence of osteocytes in lacunae CTother includedvasculature loose fibrous CT and inflammatory cellsOnce the core was separated into its respectivecomponents (vital bone residual graft and CTother)using image editing softwareparapara separated imageswere converted to a binary black and white image
Total number of pixels was calculated and summedfor each image and percentage of pixels for each
image was calculated to find percentage area of eachcomponent of bone core
Statistical Analyses Each study participant con-tributed a single value of each outcome variable tostatistical analysis A two-sample Student t test wasperformed for histologic outcomes as well as clinicalridge dimensional changes to evaluate differencesbetween the two treatment groups Box plots wereused to assess whether parametric statistical tests wereappropriate In the event of extreme outliers or sig-nificant departures from symmetry MannndashWhitney Utests were performed to confirm findings from Studentt tests To evaluate treatment group differences in archlocation of site presence or absence of a dehiscenceat extraction toothbound versus non-toothboundextraction site and need for additional grafting atthe time of implant placement Fisher exact testswere performed For all statistical analyses P lt005 wasconsidered significant Spearman rank and Pearsoncorrelations between clinical and histologic parameterswere also analyzed
RESULTS
Of 46 patients enrolled two patients consented toparticipate and subsequently elected to withdrawfrom the study (Fig 1) After extraction one patientstarted treatment with a medication (teriparatide)known to alter bone metabolism and was exited fromthe study There was one smoker in each group Fourpatients had well-controlled DM two from eachgroup Of the 43 patients who completed the study41 core biopsies were taken After healing one pa-tient in the long-term group had inadequate ridgewidth for core biopsy and implant placement how-ever ridge dimensional changes were recorded Onepatient had poor quality bone core that could not becontained for processing but an implant was suc-cessfully placed Thus 42 of 43 patients who re-ceived extraction and ridge preservation had implantsplaced successfully Of 41 core biopsies taken twowere lost to processing one from each group In theshort-term group clinical data were collected to per-form dimensional analysis for all 22 patients In thelong-term group data for ridge dimensional analysiswere collected for 19 of 21 patients In this group thecustomized acrylic measuring stent was lost for onepatient and clinical measurements were not made atthe implant surgery for the other patient
The short-term group healed for a mean of 903 ndash069 weeks and the long-term group healed fora mean of 1911 ndash 087 weeks At baseline sites in
DaggerDagger Salvin Dental Specialtiessectsect Treosin Statlab Medical Products McKinney TXii CellSens Version 14 software Olympus Center Valley PAparapara Adobe Photoshop CS51 Adobe San Jose CA ImageJ National Institutes of Health Bethesda MD
J Periodontol bull September 2016 Whetman Mealey
1025
both groups were similar Fisher exact test found nosignificant differences for study sites between groupsHowever there was a statistically significant differ-ence in buccal plate thickness between the twogroups (P = 0001) Mean buccal plate thickness inthe short-term group was 0614 ndash 0273 mm com-pared with 1010 ndash 0446mm in the long-term groupMost sites were maxillary sites with 14 in the short-term group and 13 in the long-term group There wasno significant difference in initial ridge width betweenthe two treatment groups (P = 051) The short-termgroup had a mean initial ridge width of 939 ndash169 mm compared with 978 ndash 205 mm in the long-term group
Histologic ObservationsVital bone was identified as areas of bone with oste-ocytes occupying lacunae and was most often wovenbone (Fig 2) Residual graft particles were identifiedas areas of primarily lamellar bone and no osteocytesoccupying the lacunae Apposition of new vital boneon residual graft particles was often noted The lastcategory was CTother which comprised loose fi-brovascular CT
There was a significantly different percentage newvital bone between the short-term group and thelong-term group (P = 001) The short-term grouphad a mean of 3263 vital bone compared with4741 in the long-term group (Table 1) With regardto percentage residual graft there was no significantdifference between treatment groups (test = 3742control = 2680) however it did trend towardstatistical significance (P = 006) There was no sig-nificant difference among treatment groups with re-gard to fraction of CTother (P = 042) A Fisher exact
test showed no significant difference in percentagenew vital bone among sites in the maxillary archcompared with sites in the mandibular arch (P = 043)anterior versus posterior tooth position (P = 074) andpresence or absence of a dehiscence at the time ofextraction (P = 057)
Dimensional ChangesIn analyzing ridge dimensional changes no statis-tically significant differences were found betweentreatment groups (Table 2) Specifically there wasno statistical difference in ridge width change (P =021) buccal ridge height change (P = 029) orlingual ridge height change (P gt099) Mean decreasein ridge width was 141 mm in the short-term groupand 066 mm in the long-term group Mean loss ofbuccal and lingual ridge height was between 084 and182 mm No significant correlation was found be-tween buccal plate thickness at time of extraction andfinal ridge width change
DISCUSSION
The primary objective of this study is to evaluate effectof healing time on new bone formation after ridgepreservation with DFDBA specifically at time pointsaveraging 9 weeks and 19 weeks after tooth extrac-tion Significantly more new vital bone was found inthe long-term healing group compared with the short-term healing group with no significant differences inridge dimensional changes between groups
This study design which has been used by theauthorsrsquo research group before10-12 eliminates manypotential confounding variables by 1) utilizing a singledonor as the source of bone graft material for bothexperimental groups 2) testing osteoinductivity ofallograft material 3) including only sites with at least10 mm of socket depth and root angulation similar tothe desired final implant position and 4) using stan-dardized custom acrylic stents to compare ridge di-mensional change This allowed direct comparison ofnew vital bone formation between the two groups withfew confounding variables There is great variabilityamong donors and among processing lots of demin-eralized bone allografts17 Using bone derived from thesame donor and having the same residual calciumcontent allowed for comparison between groupswithout concern for donor and processing variabilityIncluding only sites with 10 mm of radiographic bonesupport and root orientation similar to the plannedrestoratively driven implant placement eliminated thepotential of including native bone in core biopsieswhich could confound histomorphometric analysis ofpercentage new bone formation10-1227-29
Wood and Mealey11 also used DFDBA in ridgepreservation and found an average of 3243 newvital bone formation 20 weeks after grafting In the
Figure 2Long-term healing group (Hematoxylin and counterstained withacidified combination of eosin-Y orange-G and acid fuchsin originalmagnification middot10) VB = vital bone RG = residual graft
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1026
current study using DFDBA an average new vitalbone formation of 4741 was found after 19 weeksof healing This result coincides with knowledge ofdonor variability as the in vivo inductivity score ofDFDBA used by Wood and Mealey11 was graded as 1on a scale of 0 to 4 compared with an inductivityscore of 2 on the same scale for DFDBA used in thecurrent study Thus when an allograft with higherinductivity was used after essentially the same amountof wound healing time more new vital bone formationwas found
Borg and Mealey12 compared ridge preservationwith an allograft consisting of 100 mineralizedFDBA to a combination allograft with a ratio of 30DFDBA70 FDBA at 19 weeks of healing The donorinductivity score for graft material in that study wasgraded as 3 of 4 and mean new vital bone formationwas 3616 in the combination allograft group Thiswas significantly more new bone formation comparedwith the group grafted with FDBA alone (247) andvery similar to 3243 new vital bone formation fromWood and Mealeyrsquos11 study using 100 DFDBA It ispossible that the higher inductivity of DFDBA in theBorg and Mealey12 study resulted in induction of newvital bone formation equivalent to that in Wood andMealeyrsquos11 study despite the demineralized allograftmaking up only 30 of the graft material in the formerstudy compared with 100 DFDBA in the latter Inconsidering these studies and the current studyDFDBA results in significantly greater formation ofnew vital bone after ridge preservation comparedwith FDBA
The significance of new vital bone formation onimplant survival and success is unclear at this pointIntuitively a higher percentage of new vital bone isdesirable as increased vital bonemay increase bone-to-implant contact or at least increase the rate at whichthe implant achieves stability andmaximum bone-to-implant contact However the authors are unawareof published literature clearly demonstrating thatpercentage of vital bone at an implant site directlyaffects implant survival or success including bone-to-implant contact esthetics or peri-implant boneloss
When an implant osteotomy is prepared tactilesensation may give the operator a subjective senseof bone density at the site At sites that have hadridge preservation is it often difficult to assessquality of bone at the grafted site during implantosteotomy or placement The authors of the currentstudy noted great variability in both treatmentgroups with some sites in each group having poordensity and others having good density It is theauthorsrsquo opinion that poor bone quality at the time ofcore biopsy and osteotomy preparation was morecommon in the short-term healing group than in thelong-term healing group It is important to note thathistomorphometric analysis showed wide variabilityin percentage of new vital bone residual graft mate-rial and CTother with large standard deviations foreach parameter in both groups Therefore subjectivedifferences in density during osteotomy preparationmay be reflective of actual differences in percentageCTother new vital bone or residual graft material
Table 1
Histologic Analysis ()
Groups
Vital Bone
Mean ndash SD
Residual Graft
Mean ndash SD
CTOther
Mean ndash SD
Test group (short-term healing group) 3263 ndash 2145 3742 ndash 1853dagger 2994 ndash 1751
Control group (long-term healing group) 4741 ndash 1166 2680 ndash 1520dagger 2578 ndash 1382
P = 001 for test group versus controldagger P = 006 for test group versus control
Table 2
Alveolar Ridge Dimensional Changes
Groups
Change in Ridge
Width Mean ndash SD
Change in Ridge
Width (mm)
Mean ndash SD
Change in Ridge
Height Buccal (mm)
Mean ndash SD
Change in Ridge
Height Lingual (mm)
Mean ndash SD
Test group (short-term healing group) -1393 ndash 2036 -141 ndash 211 -182 ndash 223 -084 ndash 148
Control group (long-term healing group) -745 ndash 1658 -066 ndash 155 -118 ndash 131 -084 ndash 096
No significant difference between groups for any measurements (P gt005)
J Periodontol bull September 2016 Whetman Mealey
1027
among patients No attempt was made in this studyto correlate objective histomorphometric data withsubjective assessment of bone density during os-teotomy preparation
Cardaropoli et al3 reported a meaningful negativecorrelation between baseline buccal plate thicknessand ridge width change at sites receiving tooth ex-traction but no ridge preservation procedures Thussites with a thinner buccal plate had greater loss ofridge width At baseline in the current study therewas a significant difference of approximately 04 mmin buccal plate thickness between treatment groupsHowever difference in loss of ridge width betweengroups was not statistically significant There wasalso no meaningful correlation between buccal platethickness and ridge dimensional changes It is pos-sible that use of a ridge preservation bone graftcounteracts the impact of a thin buccal plate on loss ofridge width after tooth extraction Other studies per-formed by the authorsrsquo research group also showed nomeaningful correlation between initial buccal platethickness and change in ridge width when ridge pres-ervation grafting was performed10-1227-29
CONCLUSIONS
The current study indicates there is significantly greaternew vital bone formation after tooth extraction andridge preservation with DFDBAwhen the clinician waits19 weeks prior to dental implant placement comparedwith only 9 weeks In addition there is no difference inridge dimensional change between sites healing for anaverage of 9 weeks compared with 19 weeks
ACKNOWLEDGMENTS
The authors thank Dr Michael Mills Dr David Lashoand Dr Kevin Gureckis UTHSCSA for their help inthe design and completion of this project The au-thors thank Ms Sonja A Bustamante at UTHSCSAfor the excellent histology provided for the studyand Ms Shirley Kraft for administrative assistancein manuscript preparation The authors also thankLifeNet Health for providing the bone allograft usedin this study This trial was registered at ClinicalTrialsgov (NCT02154386) The authors report no conflictsof interest related to this study
REFERENCES1 Lekholm U Grondahl K Jemt T Outcome of oral
implant treatment in partially edentulous jaws followed20 years in clinical function Clin Implant Dent RelatRes 20068178-186
2 Van der Weijden F DellrsquoAcqua F Slot DE Alveolarbone dimensional changes of post-extraction socketsin humans A systematic review J Clin Periodontol2009361048-1058
3 Cardaropoli D Tamagnone L Roffredo A Gaveglio LRelationship between the buccal bone plate thickness
and the healing of postextraction sockets withwithoutridge preservation Int J Periodontics Restorative Dent201434211-217
4 Iasella JM Greenwell H Miller RL et al Ridge preser-vation with freeze-dried bone allograft and a collagenmembrane compared to extraction alone for implantsite development A clinical and histologic study inhumans J Periodontol 200374990-999
5 Schropp L Wenzel A Kostopoulos L Karring T Bonehealing and soft tissue contour changes followingsingle-tooth extraction A clinical and radiographic12-month prospective study Int J Periodontics Re-storative Dent 200323313-323
6 Lekovic V Camargo PM Klokkevold PR et al Preser-vation of alveolar bone in extraction sockets usingbioabsorbable membranes J Periodontol 1998691044-1049
7 Frost N Banjar A Galloway P Huynh-BaGMealey BLThe decision-making process for ridge preservationprocedures after tooth extraction Clin Adv Periodon-tics 2014456-63
8 Avila-Ortiz G Elangovan S Kramer KW Blanchette DDawson DV Effect of alveolar ridge preservation aftertooth extraction A systematic review andmeta-analysisJ Dent Res 201493950-958
9 Chan HL Lin GH Fu JH Wang HL Alterations in bonequality after socket preservation with grafting mate-rials A systematic review Int J Oral Maxillofac Im-plants 201328710-720
10 Beck TM Mealey BL Histologic analysis of healingafter tooth extraction with ridge preservation usingmineralized human bone allograft J Periodontol 2010811765-1772
11 Wood RA Mealey BL Histologic comparison of healingafter tooth extraction with ridge preservation usingmineralized versus demineralized freeze-dried boneallograft J Periodontol 201283329-336
12 Borg TD Mealey BL Histologic healing following toothextraction with ridge preservation using mineralizedversus combinedmineralized-demineralized freeze-driedbone allograft A randomized controlled clinical trialJ Periodontol 201586348-355
13 Burchardt H The biology of bone graft repair ClinOrthop Relat Res 198317428-42
14 Goldberg VM Stevenson S Natural history of autograftsand allografts Clin Orthop Relat Res 19872257-16
15 UristMR StratesBSBonemorphogenetic protein JDentRes 1971501392-1406
16 Shigeyama Y DrsquoErrico JA Stone R Somerman MJCommercially-prepared allograft material has bi-ological activity in vitro J Periodontol 199566478-487
17 Schwartz Z Mellonig JT Carnes DL Jr et al Ability ofcommercial demineralized freeze-dried bone allograftto induce new bone formation J Periodontol 199667918-926
18 Adell R LekholmU Rockler B Branemark PI A 15-yearstudy of osseointegrated implants in the treatment of theedentulous jaw Int J Oral Surg 198110387-416
19 Paolantonio M Dolci M Scarano A et al Immediateimplantation in fresh extraction sockets A controlledclinical and histological study in man J Periodontol2001721560-1571
20 Quirynen M Van Assche N Botticelli D Berglundh THow does the timing of implant placement to extractionaffect outcome Int J Oral Maxillofac Implants 200722(Suppl)203-223
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1028
21 Cooper LF Reside GJ Raes F et al Immediateprovisionalization of dental implants placed in healedalveolar ridges and extraction sockets A 5-year pro-spective evaluation Int J Oral Maxillofac Implants201429709-717
22 Kinaia BM Shah M Neely AL Goodis HE Crestal bonelevel changes around immediately placed implants Asystematic review and meta-analyses with at least 12monthsrsquo follow-up after functional loading J Peri-odontol 2014851537-1548
23 Waasdorp JA Evian CI Mandracchia M Immediateplacement of implants into infected sites A systematicreview of the literature J Periodontol 201081801-808
24 Fugazzotto P A retrospective analysis of immediatelyplaced implants in 418 sites exhibiting periapicalpathology Results and clinical considerations Int JOral Maxillofac Implants 201227194-202
25 Fugazzotto PA A retrospective analysis of implantsimmediately placed in sites with and without periapicalpathology in sixty-four patients J Periodontol 201283182-186
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 statement Updated guidelines for
reporting parallel group randomized trials Ann InternMed 2010152726-732
27 Hoang TN Mealey BL Histologic comparison of heal-ing after ridge preservation using human demineralizedbone matrix putty with one versus two different-sizedbone particles J Periodontol 201283174-181
28 Cook DC Mealey BL Histologic comparison of healingfollowing tooth extraction with ridge preservation usingtwo different xenograft protocols J Periodontol 201384585-594
29 Eskow AJ Mealey BL Evaluation of healing followingtooth extraction with ridge preservation using corticalversus cancellous freeze-dried bone allograft J Peri-odontol 201485514-524
Correspondence Dr Brian L Mealey University of TexasHealth Science Center San Antonio Department of Peri-odontics MSC 7894 7703 Floyd Curl Drive San AntonioTX 78229-3900 Fax 210-567-3761 e-mail mealeyuthscsaedu
Submitted March 4 2016 accepted for publication April13 2016
J Periodontol bull September 2016 Whetman Mealey
1029

both groups were similar Fisher exact test found nosignificant differences for study sites between groupsHowever there was a statistically significant differ-ence in buccal plate thickness between the twogroups (P = 0001) Mean buccal plate thickness inthe short-term group was 0614 ndash 0273 mm com-pared with 1010 ndash 0446mm in the long-term groupMost sites were maxillary sites with 14 in the short-term group and 13 in the long-term group There wasno significant difference in initial ridge width betweenthe two treatment groups (P = 051) The short-termgroup had a mean initial ridge width of 939 ndash169 mm compared with 978 ndash 205 mm in the long-term group
Histologic ObservationsVital bone was identified as areas of bone with oste-ocytes occupying lacunae and was most often wovenbone (Fig 2) Residual graft particles were identifiedas areas of primarily lamellar bone and no osteocytesoccupying the lacunae Apposition of new vital boneon residual graft particles was often noted The lastcategory was CTother which comprised loose fi-brovascular CT
There was a significantly different percentage newvital bone between the short-term group and thelong-term group (P = 001) The short-term grouphad a mean of 3263 vital bone compared with4741 in the long-term group (Table 1) With regardto percentage residual graft there was no significantdifference between treatment groups (test = 3742control = 2680) however it did trend towardstatistical significance (P = 006) There was no sig-nificant difference among treatment groups with re-gard to fraction of CTother (P = 042) A Fisher exact
test showed no significant difference in percentagenew vital bone among sites in the maxillary archcompared with sites in the mandibular arch (P = 043)anterior versus posterior tooth position (P = 074) andpresence or absence of a dehiscence at the time ofextraction (P = 057)
Dimensional ChangesIn analyzing ridge dimensional changes no statis-tically significant differences were found betweentreatment groups (Table 2) Specifically there wasno statistical difference in ridge width change (P =021) buccal ridge height change (P = 029) orlingual ridge height change (P gt099) Mean decreasein ridge width was 141 mm in the short-term groupand 066 mm in the long-term group Mean loss ofbuccal and lingual ridge height was between 084 and182 mm No significant correlation was found be-tween buccal plate thickness at time of extraction andfinal ridge width change
DISCUSSION
The primary objective of this study is to evaluate effectof healing time on new bone formation after ridgepreservation with DFDBA specifically at time pointsaveraging 9 weeks and 19 weeks after tooth extrac-tion Significantly more new vital bone was found inthe long-term healing group compared with the short-term healing group with no significant differences inridge dimensional changes between groups
This study design which has been used by theauthorsrsquo research group before10-12 eliminates manypotential confounding variables by 1) utilizing a singledonor as the source of bone graft material for bothexperimental groups 2) testing osteoinductivity ofallograft material 3) including only sites with at least10 mm of socket depth and root angulation similar tothe desired final implant position and 4) using stan-dardized custom acrylic stents to compare ridge di-mensional change This allowed direct comparison ofnew vital bone formation between the two groups withfew confounding variables There is great variabilityamong donors and among processing lots of demin-eralized bone allografts17 Using bone derived from thesame donor and having the same residual calciumcontent allowed for comparison between groupswithout concern for donor and processing variabilityIncluding only sites with 10 mm of radiographic bonesupport and root orientation similar to the plannedrestoratively driven implant placement eliminated thepotential of including native bone in core biopsieswhich could confound histomorphometric analysis ofpercentage new bone formation10-1227-29
Wood and Mealey11 also used DFDBA in ridgepreservation and found an average of 3243 newvital bone formation 20 weeks after grafting In the
Figure 2Long-term healing group (Hematoxylin and counterstained withacidified combination of eosin-Y orange-G and acid fuchsin originalmagnification middot10) VB = vital bone RG = residual graft
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1026
current study using DFDBA an average new vitalbone formation of 4741 was found after 19 weeksof healing This result coincides with knowledge ofdonor variability as the in vivo inductivity score ofDFDBA used by Wood and Mealey11 was graded as 1on a scale of 0 to 4 compared with an inductivityscore of 2 on the same scale for DFDBA used in thecurrent study Thus when an allograft with higherinductivity was used after essentially the same amountof wound healing time more new vital bone formationwas found
Borg and Mealey12 compared ridge preservationwith an allograft consisting of 100 mineralizedFDBA to a combination allograft with a ratio of 30DFDBA70 FDBA at 19 weeks of healing The donorinductivity score for graft material in that study wasgraded as 3 of 4 and mean new vital bone formationwas 3616 in the combination allograft group Thiswas significantly more new bone formation comparedwith the group grafted with FDBA alone (247) andvery similar to 3243 new vital bone formation fromWood and Mealeyrsquos11 study using 100 DFDBA It ispossible that the higher inductivity of DFDBA in theBorg and Mealey12 study resulted in induction of newvital bone formation equivalent to that in Wood andMealeyrsquos11 study despite the demineralized allograftmaking up only 30 of the graft material in the formerstudy compared with 100 DFDBA in the latter Inconsidering these studies and the current studyDFDBA results in significantly greater formation ofnew vital bone after ridge preservation comparedwith FDBA
The significance of new vital bone formation onimplant survival and success is unclear at this pointIntuitively a higher percentage of new vital bone isdesirable as increased vital bonemay increase bone-to-implant contact or at least increase the rate at whichthe implant achieves stability andmaximum bone-to-implant contact However the authors are unawareof published literature clearly demonstrating thatpercentage of vital bone at an implant site directlyaffects implant survival or success including bone-to-implant contact esthetics or peri-implant boneloss
When an implant osteotomy is prepared tactilesensation may give the operator a subjective senseof bone density at the site At sites that have hadridge preservation is it often difficult to assessquality of bone at the grafted site during implantosteotomy or placement The authors of the currentstudy noted great variability in both treatmentgroups with some sites in each group having poordensity and others having good density It is theauthorsrsquo opinion that poor bone quality at the time ofcore biopsy and osteotomy preparation was morecommon in the short-term healing group than in thelong-term healing group It is important to note thathistomorphometric analysis showed wide variabilityin percentage of new vital bone residual graft mate-rial and CTother with large standard deviations foreach parameter in both groups Therefore subjectivedifferences in density during osteotomy preparationmay be reflective of actual differences in percentageCTother new vital bone or residual graft material
Table 1
Histologic Analysis ()
Groups
Vital Bone
Mean ndash SD
Residual Graft
Mean ndash SD
CTOther
Mean ndash SD
Test group (short-term healing group) 3263 ndash 2145 3742 ndash 1853dagger 2994 ndash 1751
Control group (long-term healing group) 4741 ndash 1166 2680 ndash 1520dagger 2578 ndash 1382
P = 001 for test group versus controldagger P = 006 for test group versus control
Table 2
Alveolar Ridge Dimensional Changes
Groups
Change in Ridge
Width Mean ndash SD
Change in Ridge
Width (mm)
Mean ndash SD
Change in Ridge
Height Buccal (mm)
Mean ndash SD
Change in Ridge
Height Lingual (mm)
Mean ndash SD
Test group (short-term healing group) -1393 ndash 2036 -141 ndash 211 -182 ndash 223 -084 ndash 148
Control group (long-term healing group) -745 ndash 1658 -066 ndash 155 -118 ndash 131 -084 ndash 096
No significant difference between groups for any measurements (P gt005)
J Periodontol bull September 2016 Whetman Mealey
1027
among patients No attempt was made in this studyto correlate objective histomorphometric data withsubjective assessment of bone density during os-teotomy preparation
Cardaropoli et al3 reported a meaningful negativecorrelation between baseline buccal plate thicknessand ridge width change at sites receiving tooth ex-traction but no ridge preservation procedures Thussites with a thinner buccal plate had greater loss ofridge width At baseline in the current study therewas a significant difference of approximately 04 mmin buccal plate thickness between treatment groupsHowever difference in loss of ridge width betweengroups was not statistically significant There wasalso no meaningful correlation between buccal platethickness and ridge dimensional changes It is pos-sible that use of a ridge preservation bone graftcounteracts the impact of a thin buccal plate on loss ofridge width after tooth extraction Other studies per-formed by the authorsrsquo research group also showed nomeaningful correlation between initial buccal platethickness and change in ridge width when ridge pres-ervation grafting was performed10-1227-29
CONCLUSIONS
The current study indicates there is significantly greaternew vital bone formation after tooth extraction andridge preservation with DFDBAwhen the clinician waits19 weeks prior to dental implant placement comparedwith only 9 weeks In addition there is no difference inridge dimensional change between sites healing for anaverage of 9 weeks compared with 19 weeks
ACKNOWLEDGMENTS
The authors thank Dr Michael Mills Dr David Lashoand Dr Kevin Gureckis UTHSCSA for their help inthe design and completion of this project The au-thors thank Ms Sonja A Bustamante at UTHSCSAfor the excellent histology provided for the studyand Ms Shirley Kraft for administrative assistancein manuscript preparation The authors also thankLifeNet Health for providing the bone allograft usedin this study This trial was registered at ClinicalTrialsgov (NCT02154386) The authors report no conflictsof interest related to this study
REFERENCES1 Lekholm U Grondahl K Jemt T Outcome of oral
implant treatment in partially edentulous jaws followed20 years in clinical function Clin Implant Dent RelatRes 20068178-186
2 Van der Weijden F DellrsquoAcqua F Slot DE Alveolarbone dimensional changes of post-extraction socketsin humans A systematic review J Clin Periodontol2009361048-1058
3 Cardaropoli D Tamagnone L Roffredo A Gaveglio LRelationship between the buccal bone plate thickness
and the healing of postextraction sockets withwithoutridge preservation Int J Periodontics Restorative Dent201434211-217
4 Iasella JM Greenwell H Miller RL et al Ridge preser-vation with freeze-dried bone allograft and a collagenmembrane compared to extraction alone for implantsite development A clinical and histologic study inhumans J Periodontol 200374990-999
5 Schropp L Wenzel A Kostopoulos L Karring T Bonehealing and soft tissue contour changes followingsingle-tooth extraction A clinical and radiographic12-month prospective study Int J Periodontics Re-storative Dent 200323313-323
6 Lekovic V Camargo PM Klokkevold PR et al Preser-vation of alveolar bone in extraction sockets usingbioabsorbable membranes J Periodontol 1998691044-1049
7 Frost N Banjar A Galloway P Huynh-BaGMealey BLThe decision-making process for ridge preservationprocedures after tooth extraction Clin Adv Periodon-tics 2014456-63
8 Avila-Ortiz G Elangovan S Kramer KW Blanchette DDawson DV Effect of alveolar ridge preservation aftertooth extraction A systematic review andmeta-analysisJ Dent Res 201493950-958
9 Chan HL Lin GH Fu JH Wang HL Alterations in bonequality after socket preservation with grafting mate-rials A systematic review Int J Oral Maxillofac Im-plants 201328710-720
10 Beck TM Mealey BL Histologic analysis of healingafter tooth extraction with ridge preservation usingmineralized human bone allograft J Periodontol 2010811765-1772
11 Wood RA Mealey BL Histologic comparison of healingafter tooth extraction with ridge preservation usingmineralized versus demineralized freeze-dried boneallograft J Periodontol 201283329-336
12 Borg TD Mealey BL Histologic healing following toothextraction with ridge preservation using mineralizedversus combinedmineralized-demineralized freeze-driedbone allograft A randomized controlled clinical trialJ Periodontol 201586348-355
13 Burchardt H The biology of bone graft repair ClinOrthop Relat Res 198317428-42
14 Goldberg VM Stevenson S Natural history of autograftsand allografts Clin Orthop Relat Res 19872257-16
15 UristMR StratesBSBonemorphogenetic protein JDentRes 1971501392-1406
16 Shigeyama Y DrsquoErrico JA Stone R Somerman MJCommercially-prepared allograft material has bi-ological activity in vitro J Periodontol 199566478-487
17 Schwartz Z Mellonig JT Carnes DL Jr et al Ability ofcommercial demineralized freeze-dried bone allograftto induce new bone formation J Periodontol 199667918-926
18 Adell R LekholmU Rockler B Branemark PI A 15-yearstudy of osseointegrated implants in the treatment of theedentulous jaw Int J Oral Surg 198110387-416
19 Paolantonio M Dolci M Scarano A et al Immediateimplantation in fresh extraction sockets A controlledclinical and histological study in man J Periodontol2001721560-1571
20 Quirynen M Van Assche N Botticelli D Berglundh THow does the timing of implant placement to extractionaffect outcome Int J Oral Maxillofac Implants 200722(Suppl)203-223
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1028
21 Cooper LF Reside GJ Raes F et al Immediateprovisionalization of dental implants placed in healedalveolar ridges and extraction sockets A 5-year pro-spective evaluation Int J Oral Maxillofac Implants201429709-717
22 Kinaia BM Shah M Neely AL Goodis HE Crestal bonelevel changes around immediately placed implants Asystematic review and meta-analyses with at least 12monthsrsquo follow-up after functional loading J Peri-odontol 2014851537-1548
23 Waasdorp JA Evian CI Mandracchia M Immediateplacement of implants into infected sites A systematicreview of the literature J Periodontol 201081801-808
24 Fugazzotto P A retrospective analysis of immediatelyplaced implants in 418 sites exhibiting periapicalpathology Results and clinical considerations Int JOral Maxillofac Implants 201227194-202
25 Fugazzotto PA A retrospective analysis of implantsimmediately placed in sites with and without periapicalpathology in sixty-four patients J Periodontol 201283182-186
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 statement Updated guidelines for
reporting parallel group randomized trials Ann InternMed 2010152726-732
27 Hoang TN Mealey BL Histologic comparison of heal-ing after ridge preservation using human demineralizedbone matrix putty with one versus two different-sizedbone particles J Periodontol 201283174-181
28 Cook DC Mealey BL Histologic comparison of healingfollowing tooth extraction with ridge preservation usingtwo different xenograft protocols J Periodontol 201384585-594
29 Eskow AJ Mealey BL Evaluation of healing followingtooth extraction with ridge preservation using corticalversus cancellous freeze-dried bone allograft J Peri-odontol 201485514-524
Correspondence Dr Brian L Mealey University of TexasHealth Science Center San Antonio Department of Peri-odontics MSC 7894 7703 Floyd Curl Drive San AntonioTX 78229-3900 Fax 210-567-3761 e-mail mealeyuthscsaedu
Submitted March 4 2016 accepted for publication April13 2016
J Periodontol bull September 2016 Whetman Mealey
1029

current study using DFDBA an average new vitalbone formation of 4741 was found after 19 weeksof healing This result coincides with knowledge ofdonor variability as the in vivo inductivity score ofDFDBA used by Wood and Mealey11 was graded as 1on a scale of 0 to 4 compared with an inductivityscore of 2 on the same scale for DFDBA used in thecurrent study Thus when an allograft with higherinductivity was used after essentially the same amountof wound healing time more new vital bone formationwas found
Borg and Mealey12 compared ridge preservationwith an allograft consisting of 100 mineralizedFDBA to a combination allograft with a ratio of 30DFDBA70 FDBA at 19 weeks of healing The donorinductivity score for graft material in that study wasgraded as 3 of 4 and mean new vital bone formationwas 3616 in the combination allograft group Thiswas significantly more new bone formation comparedwith the group grafted with FDBA alone (247) andvery similar to 3243 new vital bone formation fromWood and Mealeyrsquos11 study using 100 DFDBA It ispossible that the higher inductivity of DFDBA in theBorg and Mealey12 study resulted in induction of newvital bone formation equivalent to that in Wood andMealeyrsquos11 study despite the demineralized allograftmaking up only 30 of the graft material in the formerstudy compared with 100 DFDBA in the latter Inconsidering these studies and the current studyDFDBA results in significantly greater formation ofnew vital bone after ridge preservation comparedwith FDBA
The significance of new vital bone formation onimplant survival and success is unclear at this pointIntuitively a higher percentage of new vital bone isdesirable as increased vital bonemay increase bone-to-implant contact or at least increase the rate at whichthe implant achieves stability andmaximum bone-to-implant contact However the authors are unawareof published literature clearly demonstrating thatpercentage of vital bone at an implant site directlyaffects implant survival or success including bone-to-implant contact esthetics or peri-implant boneloss
When an implant osteotomy is prepared tactilesensation may give the operator a subjective senseof bone density at the site At sites that have hadridge preservation is it often difficult to assessquality of bone at the grafted site during implantosteotomy or placement The authors of the currentstudy noted great variability in both treatmentgroups with some sites in each group having poordensity and others having good density It is theauthorsrsquo opinion that poor bone quality at the time ofcore biopsy and osteotomy preparation was morecommon in the short-term healing group than in thelong-term healing group It is important to note thathistomorphometric analysis showed wide variabilityin percentage of new vital bone residual graft mate-rial and CTother with large standard deviations foreach parameter in both groups Therefore subjectivedifferences in density during osteotomy preparationmay be reflective of actual differences in percentageCTother new vital bone or residual graft material
Table 1
Histologic Analysis ()
Groups
Vital Bone
Mean ndash SD
Residual Graft
Mean ndash SD
CTOther
Mean ndash SD
Test group (short-term healing group) 3263 ndash 2145 3742 ndash 1853dagger 2994 ndash 1751
Control group (long-term healing group) 4741 ndash 1166 2680 ndash 1520dagger 2578 ndash 1382
P = 001 for test group versus controldagger P = 006 for test group versus control
Table 2
Alveolar Ridge Dimensional Changes
Groups
Change in Ridge
Width Mean ndash SD
Change in Ridge
Width (mm)
Mean ndash SD
Change in Ridge
Height Buccal (mm)
Mean ndash SD
Change in Ridge
Height Lingual (mm)
Mean ndash SD
Test group (short-term healing group) -1393 ndash 2036 -141 ndash 211 -182 ndash 223 -084 ndash 148
Control group (long-term healing group) -745 ndash 1658 -066 ndash 155 -118 ndash 131 -084 ndash 096
No significant difference between groups for any measurements (P gt005)
J Periodontol bull September 2016 Whetman Mealey
1027
among patients No attempt was made in this studyto correlate objective histomorphometric data withsubjective assessment of bone density during os-teotomy preparation
Cardaropoli et al3 reported a meaningful negativecorrelation between baseline buccal plate thicknessand ridge width change at sites receiving tooth ex-traction but no ridge preservation procedures Thussites with a thinner buccal plate had greater loss ofridge width At baseline in the current study therewas a significant difference of approximately 04 mmin buccal plate thickness between treatment groupsHowever difference in loss of ridge width betweengroups was not statistically significant There wasalso no meaningful correlation between buccal platethickness and ridge dimensional changes It is pos-sible that use of a ridge preservation bone graftcounteracts the impact of a thin buccal plate on loss ofridge width after tooth extraction Other studies per-formed by the authorsrsquo research group also showed nomeaningful correlation between initial buccal platethickness and change in ridge width when ridge pres-ervation grafting was performed10-1227-29
CONCLUSIONS
The current study indicates there is significantly greaternew vital bone formation after tooth extraction andridge preservation with DFDBAwhen the clinician waits19 weeks prior to dental implant placement comparedwith only 9 weeks In addition there is no difference inridge dimensional change between sites healing for anaverage of 9 weeks compared with 19 weeks
ACKNOWLEDGMENTS
The authors thank Dr Michael Mills Dr David Lashoand Dr Kevin Gureckis UTHSCSA for their help inthe design and completion of this project The au-thors thank Ms Sonja A Bustamante at UTHSCSAfor the excellent histology provided for the studyand Ms Shirley Kraft for administrative assistancein manuscript preparation The authors also thankLifeNet Health for providing the bone allograft usedin this study This trial was registered at ClinicalTrialsgov (NCT02154386) The authors report no conflictsof interest related to this study
REFERENCES1 Lekholm U Grondahl K Jemt T Outcome of oral
implant treatment in partially edentulous jaws followed20 years in clinical function Clin Implant Dent RelatRes 20068178-186
2 Van der Weijden F DellrsquoAcqua F Slot DE Alveolarbone dimensional changes of post-extraction socketsin humans A systematic review J Clin Periodontol2009361048-1058
3 Cardaropoli D Tamagnone L Roffredo A Gaveglio LRelationship between the buccal bone plate thickness
and the healing of postextraction sockets withwithoutridge preservation Int J Periodontics Restorative Dent201434211-217
4 Iasella JM Greenwell H Miller RL et al Ridge preser-vation with freeze-dried bone allograft and a collagenmembrane compared to extraction alone for implantsite development A clinical and histologic study inhumans J Periodontol 200374990-999
5 Schropp L Wenzel A Kostopoulos L Karring T Bonehealing and soft tissue contour changes followingsingle-tooth extraction A clinical and radiographic12-month prospective study Int J Periodontics Re-storative Dent 200323313-323
6 Lekovic V Camargo PM Klokkevold PR et al Preser-vation of alveolar bone in extraction sockets usingbioabsorbable membranes J Periodontol 1998691044-1049
7 Frost N Banjar A Galloway P Huynh-BaGMealey BLThe decision-making process for ridge preservationprocedures after tooth extraction Clin Adv Periodon-tics 2014456-63
8 Avila-Ortiz G Elangovan S Kramer KW Blanchette DDawson DV Effect of alveolar ridge preservation aftertooth extraction A systematic review andmeta-analysisJ Dent Res 201493950-958
9 Chan HL Lin GH Fu JH Wang HL Alterations in bonequality after socket preservation with grafting mate-rials A systematic review Int J Oral Maxillofac Im-plants 201328710-720
10 Beck TM Mealey BL Histologic analysis of healingafter tooth extraction with ridge preservation usingmineralized human bone allograft J Periodontol 2010811765-1772
11 Wood RA Mealey BL Histologic comparison of healingafter tooth extraction with ridge preservation usingmineralized versus demineralized freeze-dried boneallograft J Periodontol 201283329-336
12 Borg TD Mealey BL Histologic healing following toothextraction with ridge preservation using mineralizedversus combinedmineralized-demineralized freeze-driedbone allograft A randomized controlled clinical trialJ Periodontol 201586348-355
13 Burchardt H The biology of bone graft repair ClinOrthop Relat Res 198317428-42
14 Goldberg VM Stevenson S Natural history of autograftsand allografts Clin Orthop Relat Res 19872257-16
15 UristMR StratesBSBonemorphogenetic protein JDentRes 1971501392-1406
16 Shigeyama Y DrsquoErrico JA Stone R Somerman MJCommercially-prepared allograft material has bi-ological activity in vitro J Periodontol 199566478-487
17 Schwartz Z Mellonig JT Carnes DL Jr et al Ability ofcommercial demineralized freeze-dried bone allograftto induce new bone formation J Periodontol 199667918-926
18 Adell R LekholmU Rockler B Branemark PI A 15-yearstudy of osseointegrated implants in the treatment of theedentulous jaw Int J Oral Surg 198110387-416
19 Paolantonio M Dolci M Scarano A et al Immediateimplantation in fresh extraction sockets A controlledclinical and histological study in man J Periodontol2001721560-1571
20 Quirynen M Van Assche N Botticelli D Berglundh THow does the timing of implant placement to extractionaffect outcome Int J Oral Maxillofac Implants 200722(Suppl)203-223
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1028
21 Cooper LF Reside GJ Raes F et al Immediateprovisionalization of dental implants placed in healedalveolar ridges and extraction sockets A 5-year pro-spective evaluation Int J Oral Maxillofac Implants201429709-717
22 Kinaia BM Shah M Neely AL Goodis HE Crestal bonelevel changes around immediately placed implants Asystematic review and meta-analyses with at least 12monthsrsquo follow-up after functional loading J Peri-odontol 2014851537-1548
23 Waasdorp JA Evian CI Mandracchia M Immediateplacement of implants into infected sites A systematicreview of the literature J Periodontol 201081801-808
24 Fugazzotto P A retrospective analysis of immediatelyplaced implants in 418 sites exhibiting periapicalpathology Results and clinical considerations Int JOral Maxillofac Implants 201227194-202
25 Fugazzotto PA A retrospective analysis of implantsimmediately placed in sites with and without periapicalpathology in sixty-four patients J Periodontol 201283182-186
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 statement Updated guidelines for
reporting parallel group randomized trials Ann InternMed 2010152726-732
27 Hoang TN Mealey BL Histologic comparison of heal-ing after ridge preservation using human demineralizedbone matrix putty with one versus two different-sizedbone particles J Periodontol 201283174-181
28 Cook DC Mealey BL Histologic comparison of healingfollowing tooth extraction with ridge preservation usingtwo different xenograft protocols J Periodontol 201384585-594
29 Eskow AJ Mealey BL Evaluation of healing followingtooth extraction with ridge preservation using corticalversus cancellous freeze-dried bone allograft J Peri-odontol 201485514-524
Correspondence Dr Brian L Mealey University of TexasHealth Science Center San Antonio Department of Peri-odontics MSC 7894 7703 Floyd Curl Drive San AntonioTX 78229-3900 Fax 210-567-3761 e-mail mealeyuthscsaedu
Submitted March 4 2016 accepted for publication April13 2016
J Periodontol bull September 2016 Whetman Mealey
1029

among patients No attempt was made in this studyto correlate objective histomorphometric data withsubjective assessment of bone density during os-teotomy preparation
Cardaropoli et al3 reported a meaningful negativecorrelation between baseline buccal plate thicknessand ridge width change at sites receiving tooth ex-traction but no ridge preservation procedures Thussites with a thinner buccal plate had greater loss ofridge width At baseline in the current study therewas a significant difference of approximately 04 mmin buccal plate thickness between treatment groupsHowever difference in loss of ridge width betweengroups was not statistically significant There wasalso no meaningful correlation between buccal platethickness and ridge dimensional changes It is pos-sible that use of a ridge preservation bone graftcounteracts the impact of a thin buccal plate on loss ofridge width after tooth extraction Other studies per-formed by the authorsrsquo research group also showed nomeaningful correlation between initial buccal platethickness and change in ridge width when ridge pres-ervation grafting was performed10-1227-29
CONCLUSIONS
The current study indicates there is significantly greaternew vital bone formation after tooth extraction andridge preservation with DFDBAwhen the clinician waits19 weeks prior to dental implant placement comparedwith only 9 weeks In addition there is no difference inridge dimensional change between sites healing for anaverage of 9 weeks compared with 19 weeks
ACKNOWLEDGMENTS
The authors thank Dr Michael Mills Dr David Lashoand Dr Kevin Gureckis UTHSCSA for their help inthe design and completion of this project The au-thors thank Ms Sonja A Bustamante at UTHSCSAfor the excellent histology provided for the studyand Ms Shirley Kraft for administrative assistancein manuscript preparation The authors also thankLifeNet Health for providing the bone allograft usedin this study This trial was registered at ClinicalTrialsgov (NCT02154386) The authors report no conflictsof interest related to this study
REFERENCES1 Lekholm U Grondahl K Jemt T Outcome of oral
implant treatment in partially edentulous jaws followed20 years in clinical function Clin Implant Dent RelatRes 20068178-186
2 Van der Weijden F DellrsquoAcqua F Slot DE Alveolarbone dimensional changes of post-extraction socketsin humans A systematic review J Clin Periodontol2009361048-1058
3 Cardaropoli D Tamagnone L Roffredo A Gaveglio LRelationship between the buccal bone plate thickness
and the healing of postextraction sockets withwithoutridge preservation Int J Periodontics Restorative Dent201434211-217
4 Iasella JM Greenwell H Miller RL et al Ridge preser-vation with freeze-dried bone allograft and a collagenmembrane compared to extraction alone for implantsite development A clinical and histologic study inhumans J Periodontol 200374990-999
5 Schropp L Wenzel A Kostopoulos L Karring T Bonehealing and soft tissue contour changes followingsingle-tooth extraction A clinical and radiographic12-month prospective study Int J Periodontics Re-storative Dent 200323313-323
6 Lekovic V Camargo PM Klokkevold PR et al Preser-vation of alveolar bone in extraction sockets usingbioabsorbable membranes J Periodontol 1998691044-1049
7 Frost N Banjar A Galloway P Huynh-BaGMealey BLThe decision-making process for ridge preservationprocedures after tooth extraction Clin Adv Periodon-tics 2014456-63
8 Avila-Ortiz G Elangovan S Kramer KW Blanchette DDawson DV Effect of alveolar ridge preservation aftertooth extraction A systematic review andmeta-analysisJ Dent Res 201493950-958
9 Chan HL Lin GH Fu JH Wang HL Alterations in bonequality after socket preservation with grafting mate-rials A systematic review Int J Oral Maxillofac Im-plants 201328710-720
10 Beck TM Mealey BL Histologic analysis of healingafter tooth extraction with ridge preservation usingmineralized human bone allograft J Periodontol 2010811765-1772
11 Wood RA Mealey BL Histologic comparison of healingafter tooth extraction with ridge preservation usingmineralized versus demineralized freeze-dried boneallograft J Periodontol 201283329-336
12 Borg TD Mealey BL Histologic healing following toothextraction with ridge preservation using mineralizedversus combinedmineralized-demineralized freeze-driedbone allograft A randomized controlled clinical trialJ Periodontol 201586348-355
13 Burchardt H The biology of bone graft repair ClinOrthop Relat Res 198317428-42
14 Goldberg VM Stevenson S Natural history of autograftsand allografts Clin Orthop Relat Res 19872257-16
15 UristMR StratesBSBonemorphogenetic protein JDentRes 1971501392-1406
16 Shigeyama Y DrsquoErrico JA Stone R Somerman MJCommercially-prepared allograft material has bi-ological activity in vitro J Periodontol 199566478-487
17 Schwartz Z Mellonig JT Carnes DL Jr et al Ability ofcommercial demineralized freeze-dried bone allograftto induce new bone formation J Periodontol 199667918-926
18 Adell R LekholmU Rockler B Branemark PI A 15-yearstudy of osseointegrated implants in the treatment of theedentulous jaw Int J Oral Surg 198110387-416
19 Paolantonio M Dolci M Scarano A et al Immediateimplantation in fresh extraction sockets A controlledclinical and histological study in man J Periodontol2001721560-1571
20 Quirynen M Van Assche N Botticelli D Berglundh THow does the timing of implant placement to extractionaffect outcome Int J Oral Maxillofac Implants 200722(Suppl)203-223
New Bone Formation and Healing Time in Ridge Preservation Volume 87 bull Number 9
1028
21 Cooper LF Reside GJ Raes F et al Immediateprovisionalization of dental implants placed in healedalveolar ridges and extraction sockets A 5-year pro-spective evaluation Int J Oral Maxillofac Implants201429709-717
22 Kinaia BM Shah M Neely AL Goodis HE Crestal bonelevel changes around immediately placed implants Asystematic review and meta-analyses with at least 12monthsrsquo follow-up after functional loading J Peri-odontol 2014851537-1548
23 Waasdorp JA Evian CI Mandracchia M Immediateplacement of implants into infected sites A systematicreview of the literature J Periodontol 201081801-808
24 Fugazzotto P A retrospective analysis of immediatelyplaced implants in 418 sites exhibiting periapicalpathology Results and clinical considerations Int JOral Maxillofac Implants 201227194-202
25 Fugazzotto PA A retrospective analysis of implantsimmediately placed in sites with and without periapicalpathology in sixty-four patients J Periodontol 201283182-186
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 statement Updated guidelines for
reporting parallel group randomized trials Ann InternMed 2010152726-732
27 Hoang TN Mealey BL Histologic comparison of heal-ing after ridge preservation using human demineralizedbone matrix putty with one versus two different-sizedbone particles J Periodontol 201283174-181
28 Cook DC Mealey BL Histologic comparison of healingfollowing tooth extraction with ridge preservation usingtwo different xenograft protocols J Periodontol 201384585-594
29 Eskow AJ Mealey BL Evaluation of healing followingtooth extraction with ridge preservation using corticalversus cancellous freeze-dried bone allograft J Peri-odontol 201485514-524
Correspondence Dr Brian L Mealey University of TexasHealth Science Center San Antonio Department of Peri-odontics MSC 7894 7703 Floyd Curl Drive San AntonioTX 78229-3900 Fax 210-567-3761 e-mail mealeyuthscsaedu
Submitted March 4 2016 accepted for publication April13 2016
J Periodontol bull September 2016 Whetman Mealey
1029

21 Cooper LF Reside GJ Raes F et al Immediateprovisionalization of dental implants placed in healedalveolar ridges and extraction sockets A 5-year pro-spective evaluation Int J Oral Maxillofac Implants201429709-717
22 Kinaia BM Shah M Neely AL Goodis HE Crestal bonelevel changes around immediately placed implants Asystematic review and meta-analyses with at least 12monthsrsquo follow-up after functional loading J Peri-odontol 2014851537-1548
23 Waasdorp JA Evian CI Mandracchia M Immediateplacement of implants into infected sites A systematicreview of the literature J Periodontol 201081801-808
24 Fugazzotto P A retrospective analysis of immediatelyplaced implants in 418 sites exhibiting periapicalpathology Results and clinical considerations Int JOral Maxillofac Implants 201227194-202
25 Fugazzotto PA A retrospective analysis of implantsimmediately placed in sites with and without periapicalpathology in sixty-four patients J Periodontol 201283182-186
26 Schulz KF Altman DG Moher D CONSORT GroupCONSORT 2010 statement Updated guidelines for
reporting parallel group randomized trials Ann InternMed 2010152726-732
27 Hoang TN Mealey BL Histologic comparison of heal-ing after ridge preservation using human demineralizedbone matrix putty with one versus two different-sizedbone particles J Periodontol 201283174-181
28 Cook DC Mealey BL Histologic comparison of healingfollowing tooth extraction with ridge preservation usingtwo different xenograft protocols J Periodontol 201384585-594
29 Eskow AJ Mealey BL Evaluation of healing followingtooth extraction with ridge preservation using corticalversus cancellous freeze-dried bone allograft J Peri-odontol 201485514-524
Correspondence Dr Brian L Mealey University of TexasHealth Science Center San Antonio Department of Peri-odontics MSC 7894 7703 Floyd Curl Drive San AntonioTX 78229-3900 Fax 210-567-3761 e-mail mealeyuthscsaedu
Submitted March 4 2016 accepted for publication April13 2016
J Periodontol bull September 2016 Whetman Mealey
1029