Embed Size (px)
Citation preview

Effect of Diltiazem on Lid Tension DuringLight-Flash-Induced Eye Blinks in the Rabbit
M. Farbowitz* H. Furst* R. Kastner,* N. Patel* and J. Jacoby
Purpose. The purpose of this study was to examine the effect of the Ca blocker diltiazem incombination with the Ca chelator EGTA (ethyleneglycol-bis-ta-amino-ethyl ether]N,N'-tetra-acetic acid) on eyelid tension generated during the light-induced eyeblink reflex in the adultrabbit. The goal is to develop nontoxic, nonsurgical therapies for blepharospasm.
Methods. Blinks were triggered in the alert rabbit, and tension was measured with a straingauge attached to the eyelid. Strain gauge output was amplified, digitized, and stored oncomputer for later analysis. Experiments consisted of a set of trials in which identical lightstimuli were delivered at 0.1 Hz for 5 min.
Results. In control trials, blink tensions decreased dramatically for the first seven to nine blinksand then levelled off, indicating that with respect to muscle tension output, blinks containedboth rapidly habituating and nonhabituating components. After diltiazem and EGTA wereinjected in the lid, blinks were reduced 30% to 90% over those in control trials. Reductionscould not be explained by injection trauma or irritation due to fluid volume, because injectionsof saline alone did not produce such tension depression.
Conclusions. Diltiazem-EGTA produces a transient reduction in blink tension. A clinical appli-cation will depend on developing methods for the sustained release of these drugs in theeyelid. Invest Ophthalmol Vis Sci. 1993; 34:293-304.
ISenign essential blepharospasm is a variably progres-sive, bilateral, involuntary focal cranial dyskinesia ofunknown etiology. It is characterized by spasmodic,forceful, and involuntary contractions of the orbicu-laris oculi (OO) muscles, frequently resulting in pro-longed eyelid closure and severe visual disability.
From the Department of Ophthalmology, New York University MedicalCenter, Neiu York, Neiu York.* Medical students working in the Honors Program, Neiu York UniversityMedical. School.Supported by a grant from the Benign Essential BlepharospasmFoundation (JJ), an unrestricted grant to the department from Researchto Prevent Blindness, inc., New York, Neiu York, a Core grant to thedepartment from NEI EY-01297, by the Eye Surgeiy Fund, New York,New York, and NEI grant EYO6232 (JJ).Submitted for publication: June 17, 1992; accepted September 21, 1992.Proprietary interest category: N.Reprint requests: Dr. Jean Jacoby, Department of Ophthalmology, NewYork University Medical Center, 550 First Avenue, New York, NY10016.
Blepharospasm often is associated with and may pro-gress to Meige's syndrome, a form of craniocervicaldystonia involving eyelid, facial, and oromandibularmovements. Surgical and nonsurgical methods havebeen developed to alleviate benign essential blepharo-spasm symptoms, but none of them have been entirelysatisfactory. Among these, facial nerve transection hasa high recurrence rate and untoward side effects, in-cluding partial facial paralysis. Myectomy results innumbness of the forehead, chronic lymphedema in theperiorbital region, and exposure keratitis. Pharmaco-therapy (antipsychotics, stimulants, sedatives, antimus-carinics, antihistamines, anticonvulsants and anti-Par-kinsonian drugs) has been useful to ameliorate specifictypes of blepharospasm by weakening the OO; how-ever, efficacy seems to be limited and temporary inmost cases, and significant side effects are a problemhere as well.1
Investigative Ophthalmology & Visual Science, February 1993, Vol. 34, No. 2Copyright © Association for Research in Vision and Ophthalmology 293
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018

294 Investigative Ophthalmology & Visual Science, February 1993, Vol. 34, No. 2
One fairly successful nonsurgical approach usesbotulinum A toxin (Oculinum, Botox), which inducesthe best temporary relief for orbicularis spasms.23
Here too, however, there are undesirable side effects,including lagophthalmos, exposure keratitis, and dif-fusion of toxin to undesirable locations, causing ptosisand diplopia.45 Although there may be no entirely sat-isfactory symptomatic, nonsurgical treatment for be-nign essential blepharospasm, the development of ef-fective alternative nonsurgical therapies with less toxicdrugs would be desirable, particularly those in whichthe risk of spread and involvement of adjacent tissue isminimized.
The benzothiazepine Ca2+ channel blocker dilti-azem in combination with the Ca2+ chelator EGTA(ethyleneglycol-bis-ta-amino-ethyl ether] N,N'-tetraa-cetic acid) has been shown to reduce tonic contrac-tures in extraocular muscle (EOM) in vitro.6"8 Diltia-zem-EGTA also was found to reduce the contractilityof EOM in vivo8'9 (andj. Jacoby, unpublished observa-tions). The effect in vivo might not be due exclusivelyto the effect on the tonic fibers, because in other ex-periments carried out in EOM in vitro it was foundthat electrically stimulated twitch responses also werereduced in the presence of diltiazem with EGTA8 (andJ. Jacoby, unpublished observations). The findings inEOM are consistent with findings in other studies dem-onstrating that in vitro diltiazem has a depressant ef-fect on mammalian skeletal muscles.10"14 The results ofthese studies suggest the possibility that diltiazem-EGTA also might reduce the contractility of a mam-malian twitch muscle in vivo, including the fast-twitchOO muscle. If so, diltiazem, a mild drug that has beenin extensive clinical use for years, might provide a po-tential alternative, nontoxic, nonsurgical treatmentfor benign essential blepharospasm. To test this hy-pothesis, a study was undertaken to investigate the ef-fect of diltiazem-EGTA on eyelid tension generatedduring the light-induced eye blink reflex in the adultrabbit. Some of the results reported here have beenpublished previously in abstract form.15
MATERIALS AND METHODS
Adult New Zealand white rabbits, both male and fe-male and weighing 3.0 to 5.0 kg, were selected to serveas experimental animals. They were handled andhoused in the animal facility of New York UniversityMedical Center in compliance with the ARVO andNIH Guidelines for the Care and Use of LaboratoryAnimals.
Animal PreparationFor the measurement of tension generated during arabbit eye blink, a strain gauge was connected to therabbit's eyelid via a 5-0 silk suture placed at midposi-tion of the upper eyelid margin. The suture was deep
to the OO muscle, but did not pierce the palpebralconjunctiva. For placement of the suture, the hair onthe eyelid was trimmed, and then the surface of theeyelid was cleaned with sterile swabs soaked in beta-dine followed by 70% ethanol. Suturing was carriedout using sterile techniques under ketamine-xylazinesedation (final concentrations: ketamine HC1, 43 mg/ml; xylazine HC1, 8.6 mg/ml; acepromazine, 1.4 mg/ml) at a dosage of 0.5 ml/kg delivered intramuscularly.The topical anesthetic proparacaine HC1 was appliedto the lid shortly before the suture was made. Aftersuturing, an antibiotic gel (tobramycin) was applied tothe suture site, and the eyelid was allowed to heal for48 hr before carrying out blink tension experiments.
Blinks were triggered by a bright, brief light flash.The rabbit was dark adapted for at least 0.5 hr before ablink trial to maximize any response to the light flash,and throughout the blink trials the room remaineddark. Trials also were carried out without distractingnoises or movements in the room to minimize anyhead movement artifacts in the recorded tension re-sponses.
For the injection of solutions into the eyelid, theroom remained dark and the rabbit was placed in arestrainer without any sedation. A 5% solution of pro-paracaine HC1 was applied at the suture site and cir-cumferentially around the eye on the upper and lowereyelids, using a sterile swab. A sterile 27 G needle at-tached to a tuberculin syringe was used to inject intothe lid a total volume of 0.10 to 0.15 ml of: 0 Ca-addedsaline (in mmol/1: NaCl, 136; KC1, 5; MgSO4, 3; imidaz-ole-SO4, 5; glucose, 11) with 15 to 30 mmol/1 diltiazemand 5 mmol/1 EGTA added, or diltiazem or EGTAalone, or normal saline alone. Four injections weremade 5 mm away from the eyelid margin, one each atthe superior and inferior aspects of the medial andlateral canthi. Immediately after injections, more pro-paracaine was applied at the injection sites, and therabbit was then given a 5-min rest period before theonset of the experimental blink trial.
For all blink trials, the animal was alert. No gen-eral sedation was given, because even ketamine, theusual drug of choice for rabbits, and believed to haveno direct effect on skeletal muscle, was noted to de-crease significantly the amplitude of light-flash-in-duced blinks (J. Jacoby, unpublished observations).For control blink trials, that is, those trials that werenot immediately preceded by eyelid injections of anykind, proparacaine was applied to the eyelid at 8 and 5min before the start of the control trial to reproduceas closely as possible the exact conditions of the experi-mental trials.
For the blink trial, the rabbit was placed in aheavily padded restrainer that minimized head move-ments without causing physical discomfort. Althoughmovement was minimized by the restrainer, it was notdesigned to immobilize the rabbit, which could move
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018

Diltiazem Reduces Eyeblink Tension in the Rabbit 295
both its head and its body if it chose to do so. Whensuch movements occurred for more than a few sec-onds, it was assumed that the animal was experiencingdistress. The blink trial was terminated and the animalwas removed from the restrainer.
The strain gauge was attached to the suture in therabbit's upper eyelid through a 1-inch long metal pinwith an open loop at its free end. For any set of trials,the strain gauge-eyelid attachment was adjusted toeliminate slackness and generate a maximal blink ten-sion response. The corresponding baseline tensionwas monitered and adjusted to the same level for sub-sequent trials within a series.
Experimental Setup
A white light source, originating from a 300 W projec-tor lamp, was used to trigger the blink reflex. The on-set and duration of the light stimulus was controlled bya Uniblitz shutter (A. W. Vincent Assoc. Inc, Roches-ter, NY), which was placed 9 inches from the eye. Thelight from the lamp was focused on the shutter open-ing by a condensor lens and a fiberoptic light guide.The light passing through the shutter was focused sothat a 2.5-cm diameter circle of light would fall on thepupil. The shutter was triggered to open by a transis-tor-to-transistor logic (TTL) stimulus controlled by theinvestigator.
Both the TTL stimulus signal and the voltage out-put from the strain gauge were recorded on a penrecorder and simultaneously digitized and stored oncomputer. The voltage output from the strain gaugewas first amplified by a Gould transducer amplifier(Gould Electronics, East Rutherford, NJ), and thenlow-pass band-filtered at 2.5 kHz using a two-pole bes-sel filter. Both the TTL stimulus and the amplified,filtered output from the strain gauge were recordedand stored in digital form as a running, "real time"record using the Axotape program (Axon Instru-ments, Burlingame, CA), a system consisting of an an-alog-to-digital converter (Labmaster) and data acquisi-tion and analysis software.
Experimental ProtocolThe experimental protocol was designed to elicit eyeblinks at as high a frequency as possible, to maximizeany putative effect on OO contractility by the use-de-pendent Ca-blocker diltiazem. For our set-up and lightsource, a light flash of 500-msec duration was neces-sary to elicit reliably a strong blink response, and thegreatest frequency at which this stimulus could be de-livered without failures in most cases was 0.1 Hz. Ablink trial thus consisted of a train of repetitive lightflash stimuli at 0.1 Hz delivered over 5 to 6 min. Everyexperiment consisted of a set of blink trials that in-cluded two to four control trials, an experimental trialfollowing 5 min after injections, then usually one tothree post-injection control trials.
The entire, uninterrupted tension record fromeach trial, including the quiescent intervals betweenblinks, was saved in data files on computer. For a givenblink, various components of the tension responsewere measured from the stored files off-line, includingmaximum tension amplitude (peak tension), time fromthe beginning of the stimulus to onset of tension rise(latency), time from the onset of tension rise to maxi-mum tension (time to peak), and time from maximum,to one-half maximum tension during the decliningphase of the tension (half relaxation time).
Statistical Analysis
The differences between trials for a given variablewere compared in two ways: (1) all responses in a trialwere averaged and compared with the averaged valuefor the blinks in other trials, using standard paramet-ric statistics; and (2) each blink of a trial was comparedwith the same blink in another trial (based on temporalorder) using the nonparametric Wilcoxon's signedrank test for matched pairs.1617
RESULTS
Tension Generated During Light-Flash-Induced Eye Blink
The effect of diltiazem on rabbit OO contractility invivo was evaluated indirectly, by recording isometriclid tension during an eye blink triggered with a bright,brief flash of light. There has been no systematic inves-tigation of the tensions generated during rabbit blinks,so the characteristics of a normal blink were examined.It also was necessary to characterize blink tension re-sponses to a train of light-flash stimuli correspondingto the experimental protocol used in this study. Asexpected, individual blink tension responses werecomplex; furthermore, the relative amplitude of ablink response was found to depend on recent blinkhistory, or the number of blinks immediately preced-ing it within a short time period.
Shape of an Individual Tension Response. The risingphase of a blink tension response consisted of at leastthree to five components that were resolvable due todifferences in latency of onset. The relaxation phaseusually contained at least two components. Figure 1Aillustrates a typical tension record, the third responsein a control blink trial, in which there are four clearlydiscernible components in its rising phase, and twocomponents in the relaxation phase. A characteristicof all responses, shown here, is that the first, or earliestcomponent of the tension is of very small amplituderelative to the total tension response. Despite a con-stant tension maintained on the lid by the strain gauge,in some blink trials this first small component is ob-scured by a small, transient tension drop (not shown),which initiates approximately 40 to 50 msec earlier
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018

296 Investigative Ophthalmology & Visual Science, February 1993, Vol. 34, No. 2
FIGURE l. Tension records from Axotape files of light-stimu-lated blinks from a control blink trial. (A) Third blink. (B)9th blink. (C) 16th blink.(D) 26th blink. Stimulus shown atbottom is 500 msec in duration. (Vertical scale bar = 10 gtension.)
than that of the tension rise, or about 45 to 55 msecafter the onset of the light stimulus. It is assumed thatthis brief tension drop corresponds to the relaxationof the levator palpebrae superioris muscle.
Decrement in Blink Tension Amplitude Over 3 to 8min at 0.1 Hz Stimulus Frequency. A blink "trial" con-sisted of the set of blink tension responses to lightHashes of constant amplitude and duration deliveredevery 10 sec (0.1 Hz) over 5 to 6 min. All trials wereinitiated only after the rabbit had been rested for atleast 30 min in a quiet, darkened room. Nevertheless,with every blink trial there was a sharp and immediatedecrement in the amplitude of the response over thecourse of the first seven to nine blinks (70-90 sec),followed by a very slight decrease or no decrease at allover the succeeding 10 to 30 blinks. Figure 1A-D il-lustrates this point by showing the 3rd, 9th, 16th, and26th blinks, respectively, from a blink trial (Fig. 2,open circles), in which there is no reduction in ampli-tude between the 16th and 26th blink.
Figure 2 plots all the blinks within a trial as a func-tion of blink number in a set of two consecutive con-trol trials, to emphasize the predictable, stereotypicalnature of the decrement in blink tension over thecourse of a trial. The inset to Figure 2 shows part of anactual tension record consisting of the first 10 blinksof one of the plotted trials (open circles). In summary,under the conditions of the experimental protocolused, there were two components to the pattern oftension responses in a blink trial: one that was subjectto immediate and rapid habituation, and a secondpart, fairly insensitive to habituation, in which therewas only a gradual decline or in some trials no signifi-
cant decline at all over the course of 25 to 35 blinkstriggered at 0.1 Hz (Fig. 2B).
Effect of Diltiazem With EGTAon Blink Tension
The effect on the light-induced blink of the benzothiaz-epine Ca-blocker diltiazem in combination with the Cachelator EGTA, was investigated by injecting the drugsdirectly into the rabbit's eyelid and measuring tensionduring a blink trial. Each such experiment (n = 7), wascomposed of a set of blink trials separated by 30-minrest periods as follows: two to four initial control blinktrials were carried out to establish an average tensionresponse; the eyelid was then injected with a salinesolution with (n = 7) or without (saline control, n = 7)drugs, immediately followed by an "experimental"blink trial. Finally, in most cases, one to four blinktrials were carried out subsequent to the experimentaltrial to chart the recovery from the effects of the injec-tion. For each experiment in which the two drugs wereinjected into an eyelid, a parallel experiment wascarried out on the same lid in which a control salineonly was injected. These saline injections, undertakenwithin several days of their "companion" diltiazem ex-periments, were made to assess the possible effect ofinjection trauma and the fluid volume alone on blinkperformance. The results of these experiments aresummarized in Table 1.
In six of six experiments in which a total of 0.1 mlof fluid was injected into the lid, injections of saline
25
20
15
10
0 20 40 60 80 100TIME (seconds)
V10 15 20
BLINK NUMBER
25 30
FIGURE 2. Blink tension for two consecutive control blinktrials plotted as a function of blink number within a trial.Open circles, first control. Filled circles, second control. In-set: actual axotape record of the first 10 blinks of the firstcontrol trial.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018

Diltiazem Reduces Eyeblink Tension in the Rabbit 297
TABLE l. Change in Blink Tension After Injections in the Eyelid
Experiment
15 mmol/1 diltiazem + 5 mmol/1 EGTA1.2.3.4. Without 5 min wait
First 7 blinks8th-28th blinks
30 mmol/1 Diltiazem + 5 mmol/1 EGTA5.6.7. 0.4 ml fluid volume
8. 15 mmol/1 diltiazem alone9. 5 mmol/1 EGTA alone
Change in Peak
DrugInjection
-55.4%f (n = 56)-45%* (n = 48)-42%* (n = 52)
-4% (n = 14)-31%*f(n = 39)
-64%*f (n = 57)-26%* (n = 56)-90%*f (n = 37)-20%* (n = 41)-13%J (n = 53)
Tension
SalineInjection
-20%t (n = 47)<- l%(n = 50)-11%* (n = 52)
+ 18.5%* (n = 14)+2% (n = 39)
+ 12.2% (n = 52)-11%§ (n = 47)-32%t (n = 50)
* Significance P < .001, Wilcoxon's signed rank for matched pairs.f Every "experimental" blink lower than its corresponding blinks in two preceding control trials.X Significance P < .01, Wilcoxon's signed rank for matched pairs.§ Based on comparison of experimental trial with 1st and 3rd, rather than 2nd and 3rd of three controlblink trials because of persistent head movements in the 2nd control trial.Experimental trials were compared with the two preceding control trials. Unless otherwise indicated,there was a 5 min wait after injections before the experimental trial was initiated, and the total volume offluid injected was 0.1-0.12 ml.
containing either 15 or 30 mmol/1 diltiazem and 5mmol/1 EGTA resulted in a highly significant reduc-tion in isometric blink tension (Table 1). Paired exper-iments carried out within several days of the drug ex-periment, in which saline only was injected into thesame eyelid, produced no effect or small reductions intension. Table 1 shows the results of these experi-ments. Figures 3 to 6 show the data from one such pairof drug and control saline experiments, correspond-ing to experiment number 2 in Table 1.
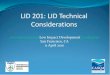
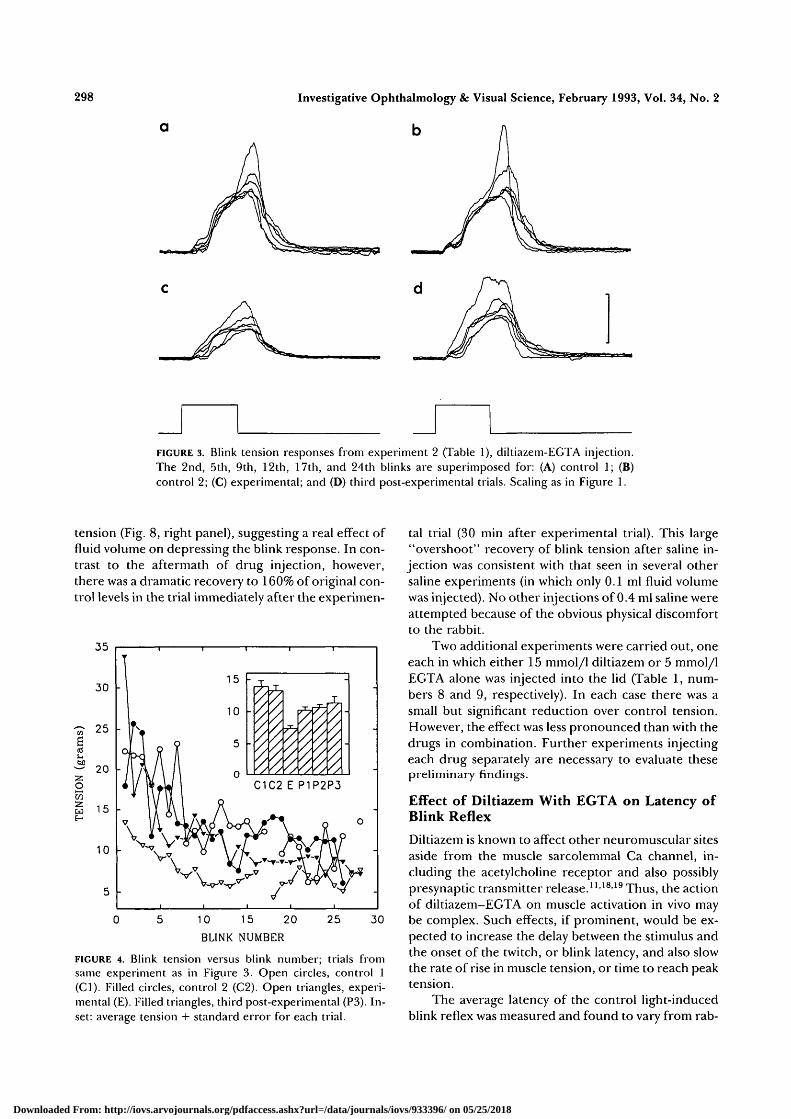
In Figure 3, a diltiazem-EGTA injection experi-ment, sample tension responses are shown superim-posed for two control trials (Figs. 3A, B), the experi-mental (or injection) trial (Fig. 3C), and the third post-injection trial (Fig. 3D). Figure 4 contains a plot oftension as a function of blink number within a trial forthe same experiment as shown in Figure 3. The inset toFigure 4 shows amplitude histograms representing theaverage blink tension for each trial. For all the experi-ments, there were two consistent characteristics to thechange in tension response after diltiazem-EGTA in-jections, and these are illustrated in the records shownin Figure 3: (1) a large reduction in tension amplitude,but (2) no change in the gross shape of the responsecompared with control blinks.
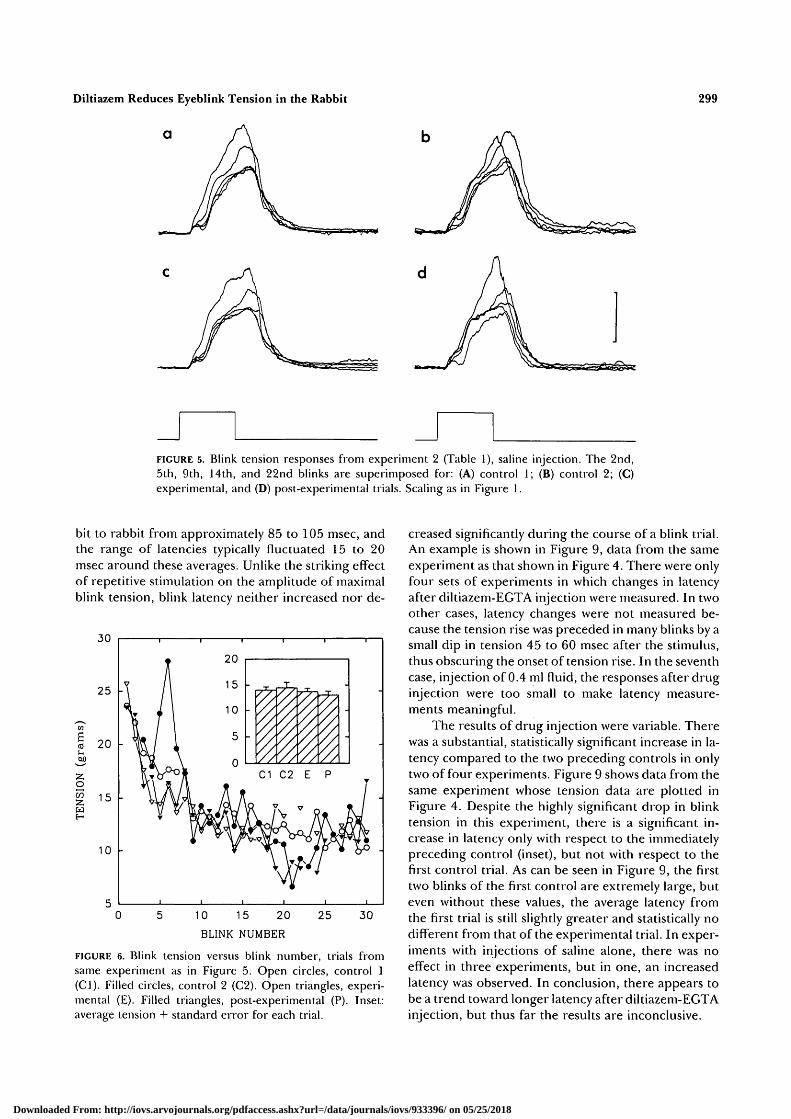
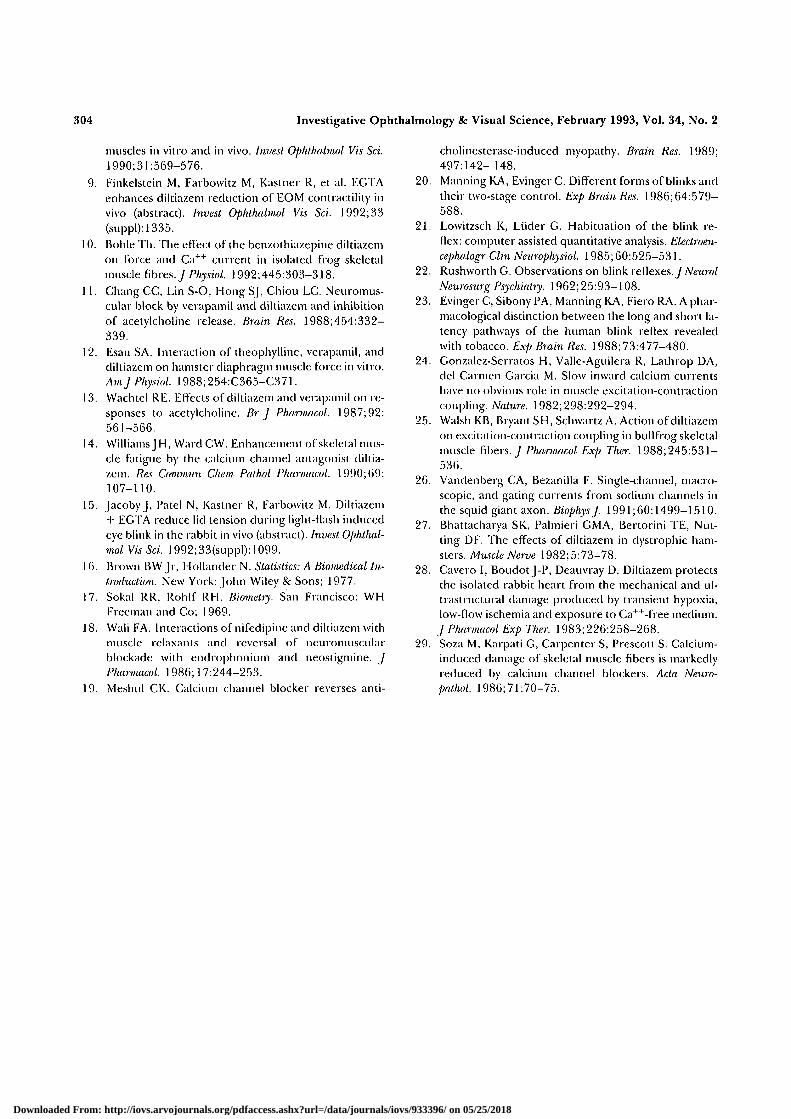
Figures 5 and 6 show the actual tension recordsand plotted data, respectively, of the companion salineinjection experiment to that shown in Figures 3 and 4.The records in Figure 5 show no reduction in tensionafter injection of saline alone, and this was the case infour of six such experiments. A small but significant
reduction in blink tension (over preceding controls),however, was observed in the remaining two experi-ments in which 0.1 ml of saline alone was injected (seeTable 1). One example is shown in Figure 7. Unlike thelarge reduction in tension after injection with dilti-azem-EGTA (Fig. 7, left panel), in this and one othercase, the reduction was small. These findings suggestthat there may be some effect of the fluid volumealone on blink tension; however, the results, as illus-trated in Figure 7, are equivocal.
Less equivocal were the results of another pair ofexperiments, shown in Figure 8, which involved injec-tion of four times the usual volume of saline (0.4 ml)into the lid. This experiment was carried out for twopurposes: to determine (1) if the putative effect ofdrug on the orbicularis oculi muscle would be aug-mented by "flooding" its extracellular environmentwith the solution, thus creating a higher effective con-centration of drug at the muscle sarcolemma and alonger washout time; and (2) whether, in the case ofsaline alone, the fluid volume itself might have a ten-dency to depress blink tension.
Injection of 0.4 ml saline containing 30 mmol/1diltiazem/5 mmol/1 EGTA resulted in a 90% reduc-tion in blink tension (Table 1). Furthermore, 25% ofthe light stimuli failed to elicit any tension response atall in the experimental trial (These nonresponses werenot included in the calculation of the 90% reduction).The profound depression of blink tension did not re-cover fully for several days. After injection of salinealone, there was a significant 32% reduction in blink
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018
298 Investigative Ophthalmology & Visual Science, February 1993, Vol. 34, No. 2
FIGURE 3. Blink tension responses from experiment 2 (Table 1), diltiazem-EGTA injection.The 2nd, 5th, 9th, 12th, 17th, and 24th blinks are superimposed for: (A) control 1; (B)control 2; (C) experimental; and (D) third post-experimental trials. Scaling as in Figure 1.
tension (Fig. 8, right panel), suggesting a real effect offluid volume on depressing the blink response. In con-trast to the aftermath of drug injection, however,there was a dramatic recovery to 160% of original con-trol levels in the trial immediately after the experimen-
10 15 20BLINK NUMBER
30
FIGURE 4. Blink tension versus blink number; trials fromsame experiment as in Figure 3. Open circles, control 1(Cl). Filled circles, control 2 (C2). Open triangles, experi-mental (E). Filled triangles, third post-experimental (P3). In-set: average tension + standard error for each trial.
tal trial (30 min after experimental trial). This large"overshoot" recovery of blink tension after saline in-jection was consistent with that seen in several othersaline experiments (in which only 0.1 ml fluid volumewas injected). No other injections of 0.4 ml saline wereattempted because of the obvious physical discomfortto the rabbit.
Two additional experiments were carried out, oneeach in which either 15 mmol/1 diltiazem or 5 mmol/1EGTA alone was injected into the lid (Table 1, num-bers 8 and 9, respectively). In each case there was asmall but significant reduction over control tension.However, the effect was less pronounced than with thedrugs in combination. Further experiments injectingeach drug separately are necessary to evaluate thesepreliminary findings.
Effect of Diltiazem With EGTA on Latency ofBlink Reflex
Diltiazem is known to affect other neuromuscular sitesaside from the muscle sarcolemmal Ca channel, in-cluding the acetylcholine receptor and also possiblypresynaptic transmitter release.111819 Thus, the actionof diltiazem-EGTA on muscle activation in vivo maybe complex. Such effects, if prominent, would be ex-pected to increase the delay between the stimulus andthe onset of the twitch, or blink latency, and also slowthe rate of rise in muscle tension, or time to reach peaktension.
The average latency of the control light-inducedblink reflex was measured and found to vary from rab-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018
Diltiazem Reduces Eyeblink Tension in the Rabbit
Q
299
FIGURE 5. Blink tension responses from experiment 2 (Table 1), saline injection. The 2nd,5th, 9th, 14th, and 22nd blinks are superimposed for: (A) control 1; (B) control 2; (C)experimental, and (D) post-experimental trials. Scaling as in Figure 1.
bit to rabbit from approximately 85 to 105 msec, andthe range of latencies typically fluctuated 15 to 20msec around these averages. Unlike the striking effectof repetitive stimulation on the amplitude of maximalblink tension, blink latency neither increased nor de-
10 15 20
BLINK NUMBER
30
FIGURE 6. Blink tension versus blink number, trials fromsame experiment as in Figure 5. Open circles, control 1(Cl). Filled circles, control 2 (C2). Open triangles, experi-mental (E). Filled triangles, post-experimental (P). Inset:average tension 4- standard error for each trial.
creased significantly during the course of a blink trial.An example is shown in Figure 9, data from the sameexperiment as that shown in Figure 4. There were onlyfour sets of experiments in which changes in latencyafter diltiazem-EGTA injection were measured. In twoother cases, latency changes were not measured be-cause the tension rise was preceded in many blinks by asmall dip in tension 45 to 60 msec after the stimulus,thus obscuring the onset of tension rise. In the seventhcase, injection of 0.4 ml fluid, the responses after drug-injection were too small to make latency measure-ments meaningful.
The results of drug injection were variable. Therewas a substantial, statistically significant increase in la-tency compared to the two preceding controls in onlytwo of four experiments. Figure 9 shows data from thesame experiment whose tension data are plotted inFigure 4. Despite the highly significant drop in blinktension in this experiment, there is a significant in-crease in latency only with respect to the immediatelypreceding control (inset), but not with respect to thefirst control trial. As can be seen in Figure 9, the firsttwo blinks of the first control are extremely large, buteven without these values, the average latency fromthe first trial is still slightly greater and statistically nodifferent from that of the experimental trial. In exper-iments with injections of saline alone, there was noeffect in three experiments, but in one, an increasedlatency was observed. In conclusion, there appears tobe a trend toward longer latency after diltiazem-EGTAinjection, but thus far the results are inconclusive.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018

300 Investigative Ophthalmology & Visual Science, February 1993, Vol. 34, No. 2
35
30
£tuO
• « _ •
55Oin
25
20
15
10
Diltiazem 20/EGTA
w W
10 15 20 25 30
BLINK NUMBER
^1
10 15 20 25 30
BLINK NUMBER
FIGURE 7. Blink tensions from experiment 1 (Table 1). Left: diltiazem-EGTA. Right: salineinjections. Symbols as in Figure 6, except at left: open boxes, control 3 (C3); and at right:open circles, control 3 (C3); filled circles, control 4 (C4). Insets: average tension.
Effect of Diltiazem With EGTA on Time toPeak and Relaxation of Blink Reflex
The time to reach peak tension (TTP) and half relax-ation time (RLT) of the tension response also wereinvestigated. There was no increase in TTP in any ex-periment after drug injection, and in fact there actu-
ally was a reduction in TTP after drug injection, corre-lated more with tension amplitude than with treat-ment. Figure 10 shows some of the data from oneexperiment, in which TTP is plotted as a function ofblink tension. The experimental data (open triangles),fall along a continuum that includes control (filled cir-cles) and post-injection (filled squares) data.
6u
» I
iniz;
15
10
0
30mM DILTIAZEM/5mM EGTA0.4ml
SALINE0.4ml
C1 C2 C3 EXP P1
BLINK TRIAL
P2 P3 C1 C2 C3 EXP
BLINK TRIAL
FIGURE 8. Average tension for each trial from experiment 7 (Table 1), in which 0.4 ml fluidvolume was injected into the eyelid. Left: diltiazem-EGTA. Right: saline injections. P3 wasrun 2.5 hr after the experimental trial.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018

Diltiazem Reduces Eyeblink Tension in the Rabbit
140
301
Diltiazem 10°A.
IV
Saline
V
10 15 20
BLINK NUMBER
25 30 10 15 20
BLINK NUMBER
25 30
control trial 1control trial 2
v d+e injection• post-injection 1
control trial 1control trial 2
v saline injection• post-injection
FIGURE 9. Blink latency versus blink number from experiment 2 (Table 1). Left: diltiazem-ECTA. Right: saline injections. Insets: average latency.
The decline in blink tension was examined as well,by measuring RLT. There was no consistent pattern ofchange in this variable either as a function of blinknumber, or after drug injection. In control trials,there was a wide variability in RLT, but the average
oCO2w
cuo
TIM
600
550
500
450
400
•
II 7̂ M \
w •
V *
"7
•
•
••
• ^
•
0 5 10 15 20 25 30BLINK TENSION (gms)
• control trial 2 • post-injection 1v d + e injection
FIGURE 10. Time from onset of blink tension to peak tension(time to peak), plotted as a function of peak tension. Datafrom experiment 2 (Table 1).
RLT for a trial fell within the range of 700 to 740 msec(time from stimulus to half relaxation). RLT was notcalculated as time from peak to half relaxation, for thefollowing reason: The tension response typically con-sisted of a plateau region, such that the time of thepeak tension value could fluctuate as much as 150msec. Even if one used the last occurrence of the max-imum tension value, this might fall at the beginning orend of the plateau, thus creating misleading estimatesof the true pattern of the relaxation of tension. Theonly unambiguous measure, therefore, was stimulusonset, or tension onset to half relaxation.
DISCUSSION
The results of this study demonstrate that, when in-jected into the rabbit eyelid, diltiazem in combinationwith EGTA significantly reduces the tension generatedduring the light-stimulated blink reflex, demonstrat-ing indirectly that these drugs act to reduce the con-tractility of the OO muscle. This reduction is bothstriking and consistently observed. Parallel experi-ments in which saline alone is injected into the eyeliddo not produce this result, indicating that the reduc-tion in OO contractility is not a response to the traumaof injections or the pressure or discomfort of the fluidvolume in the lid.
Crucial to this study was the ability to establish astimulus protocol for the blink trials that was identicalfor each and every trial, to be able to compare one trial
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018

302 Investigative Ophthalmology & Visual Science, February 1993, Vol. 34, No. 2
with another, and also to be able to make a pairedcomparison of data between trials. In our experimen-tal trials, a light flash of constant luminance and dura-tion sufficient to elicit an eye blink reliably was deliv-ered to the eye every 10 sec. The blink reflex showedimmediate habituation, in that even with the secondresponse the peak tension was reduced over that of theinitial response. Our experimental design probablymaximized this effect for the following reasons. It isknown that habituation to a light stimulus is reduced ifthe animal is distracted between stimuli, presumablybecause the predictability of the stimulus is therebyless apparent to the rabbit. In our trials, however, be-cause of the jumpiness of rabbits and the fact that theanimal was restrained but not actually immobilized, wetook pains to minimize any noises, movements, orother distracting stimuli in the room that might causethe animal to move. Any "distraction" to minimize ha-bituation would have had to be nonstartling to therabbit and also stereotypical to minimize variation,which itself would tend to become habituating. Be-cause of the predictable character of the stimulus pro-tocol and recording conditions, the pattern and timecourse of the habituation were consistent and predict-able from one trial to another. This allowed for theinvestigation not only of any general effect of thedrugs on blink tension overall, but also of any possibledifference in effect of the drugs on habituating andnonhabituating components of the response.
Our results show that diltiazem with EGTA re-duces the blink tension throughout a blink trial. How-ever, in general, the effect is proportionally more pro-nounced for the early, nonhabituated portion of thetrial. There also is a substantial reduction in the blink-to-blink variability of the tension response in the ex-perimental trial in comparison to control and postex-perimental trials. These effects could be explained byan average reduction in the safety factor for generat-ing an action potential and triggering contraction in amuscle fiber during neuromuscular transmission inthe presence of the drugs. There was one case in whichno reduction in tension was seen until the eighth blinkin the experimental trial, but this was an experiment inwhich a blink trial was initiated immediately after druginjection, rather than after the usual 5-min waitingperiod. In this one case, the delay in effect of the drugson tension is more likely due to diffusion time than toany use-dependent factor, such as spontaneous eyeblinks during the 5-min waiting period in the otherexperiments. Rabbits do not exhibit much spontane-ous blinking and, aside from the eyelid-closing duringinjection, the experimental animals were rarely ob-served to blink during the 5-min rest period after in-jection.
Electromyographic (EMG) studies have estab-lished that there are two clearly distinguishable compo-
nents to the blink reflex, regardless of the stimulus: anearly response (Rl), whose amplitude but not durationis related to the intensity of the stimulus, and that isresistant to habituation20; and the second, the so-called late response (R2), of variable duration, which issubject to strong habituation.21'22 The latter pathway isrelated to perception of a physical threat, and themagnitude of this component of the response is re-duced as the stimulus becomes predictable and thusno longer perceived as a potential threat. In our ex-periments, the tension that was generated during ablink exhibited at least four to five components. Thesecould be subdivided further into those componentsthat showed great decrement during the course of ablink trial and those that were resistant to decrementduring a blink trial, the latter including the initial smallcomponent and a second component unmasked dur-ing the course of the trial. The early small componentpersists throughout the blink trial with no increase inlatency, and in the late blinks (after 2 min) becomesalmost completely separated from the later part of theresponse, due primarily to the great reduction in am-plitude of the late component and the persistence ofthe small, but robust early component.
Whether these early and late components of thetension response correspond to Rl and R2, respec-tively, of the EMG, remains to be determined. On theother hand, the range of latencies for the onset intension rise in the rabbit blink reflex measured in thisstudy agrees closely with measurements by Manningand Evinger20 of the latency of onset of eyelid move-ment. Furthermore, the invariant latency of the earlysmall tension component is analogous to the lack ofvariation in latency of Rl after various protocols andtreatments that affect the latency of R2 and the ampli-tude of both Rl and R2.20>21-23
Manning and Evinger20 have proposed that theearly part of the blink is controlled entirely by the pre-programmed early component Rl, whereas R2 ap-pears only when stimulus duration extends beyond thetime of onset of the blink, altering the ongoing sensoryinput and thus triggering the late component andlengthening the duration of the blink. In our experi-ments, the duration of the light stimulus was 500 msec,which overlapped considerably the onset of the ten-sion response that occurred 80 to 100 msec after stim-ulus onset. Under the above hypothesis, the presenceof both components in these blink tension responses ispredicted by the pulse protocol, if it is assumed thatR2 and Rl give rise to the habituating and nonhabit-uating tension components, respectively.
The primary mechanism of action of diltiazem inthe in vivo experiments reported here is not known,nor can it be resolved from these studies. In in vitroexperiments with an EOM isolated in a chamber andattached to a strain gauge, twitch amplitude was signifi-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018

Diltiazem Reduces Eyeblink Tension in the Rabbit 303
cantly reduced by diltiazem, and there was a verysmall, late component with a long sustained relaxationat the end of an electrically stimulated twitch responsethat was blocked by diltiazem8 (and J. Jacoby, unpub-lished observations). In parallel experiments, this re-laxation also was blocked by curare alone, suggestingthat it arose from a leakage of transmitter from theremaining nerve stump, and that diltiazem as well ascurare acted to block neuromuscular transmission.The reduction in the large twitch response, on theother hand, was not duplicated by incubation in curarealone, indicating that this action of diltiazem was notrelated to neuromuscular transmission. Other studieshave provided concrete evidence that, aside from itswell known role of blocking Ca2+ entry into the musclethrough Ca2+ channels, diltiazem acts presynapticallyto reduce transmitter release at the neuromuscularjunction.1118. In phrenic nerve-diaphragm prepara-tion, diltiazem was found to reduce twitch response tonerve stimulation, a reduction that depended on fre-quency of nerve stimulation18 and enhanced in thepresence of low extracellular Ca2+. Furthermore, atvery high concentrations of diltiazem, the effect wasconsistent with complete axon conduction block, sug-gesting a direct effect on the presynaptic Na+
channel.11
After relatively short exposure times, moderateconcentrations and various conditions, diltiazem alsohas been reported to enhance twitch amplitude.24-25 Invivo, this might possibly be due in part to an inhibitoryaction of diltiazem on acetylcholinesterase at the neu-romuscular junction.1119 However, in vitro, the effectis more likely to be due to some other, as yet unknownproperty of diltiazem action probably related to itsCa2+-blocking activity at the muscle membrane. Ofpossible significance, extracellular Ca2+ has been re-ported to be an open channel blocker of Na+ chan-nels.26 One could hypothesize that under certain con-ditions and concentrations of drug, diltiazem mightcompetitively remove this Ca2+-mediated depressionof Na+ channel activity, thus increasing the safety fac-tor for triggering a muscle twitch with depolarization.By such an argument, the apparent twitch potentia-tion observed in these instances could be explained ascontractility with blocking activity removed. At higherdrug concentrations and longer incubation times, theblocking effect of diltiazem would presumably come topredominate. In this regard, in vitro experiments inwhich the muscle twitch amplitude is depressed afterprolonged exposure to diltiazem always show an initialincrease in twitch amplitude before the decline11 (andJ. Jacoby, unpublished observations). In any case, forthe in vivo condition, one would expect the concentra-tion of diltiazem and the presence of a Ca2+ chelator tobe critical to whether contractility is enhanced or de-pressed as a result of diltiazem treatment.
Whether diltiazem when applied in vivo acts toreduce muscle contractility predominantly presynapti-cally or postsynaptically, chronic, long-term treatmentclearly reduces Ca2+ influx into muscle.27 This prop-erty of the Ca2+ blocker is undoubtedly responsible forrecent findings that diltiazem can be beneficial in re-ducing damage caused by excess Ca2+ influx into mus-cle in various pathologic states.28'29
In summary, the results from this study lend sup-port to the possibility that chronic exposure of the OOmuscle to diltiazem, particularly in the presence of aCa2+ chelator such as EGTA, could provide long-termreduction in OO contractility. The use-dependent na-ture of this drug, at least with respect to its action atblocking the muscle Ca2+ channel, would make it anideal candidate in the symptomatic treatment of be-nign essential blepharospasm, a condition character-ized by chronic, pathologic activation of a muscle. Fu-ture experiments, in particular a detailed dose-re-sponse study and the development of a workablemechanism for the sustained release of diltiazem-Ca2+
chelator within the eyelid, will determine whether suchan approach has a realistic clinical application.
Key Words
calcium blocker, diltiazem, eyeblink, eyelid, muscle tension.
Acknowledgments
The authors thank Mr. Bernardo Bruno and Mr. GeorgeThomas for help in the design of the experimental setup,including rabbit restraint and some of the electronic compo-nents, and Ms. K. Ko for her assistance in the preparation ofthe manuscript.
References
1. Jordan DR, Patrinely JR, Anderson RL, Thiese SM.Essential blepharospasm and related dystonias. SurvOphthalmol. 1989; 34:123-132.
2. Kennedy RH, Bartley GB, Flanagan JC, Waller RR.Treatment of blepharospasm with botulinum toxin.Mayo Clin Proc. 1989;64:1085-1090.
3. Scott AB, Kennedy RA, Stubbs HA. Botulinum toxininjection as a treatment for blepharospasm. Arch Oph-thalmol. 1985; 103:347-350.
4. Dutton JJ, Buckley EG. Long-term results and compli-cations of botulinum A toxin in the treatment of bleph-arospasm. Ophthalmology. 1988;95:1529-1534.
5. Sanders DB, Massey EW, Buckley EG. Botulinumtoxin for blepharospasm: single-fiber EMB studies.Neurology. 1986;36:545-547.
6. Chiarandini DJ. Activation of two types of fibres in ratextraocular muscles. J Physiol. 1976;259:199-212.
7. Chiarandini DJ, Jacoby J. Dependence of tonic ten-sion on extracellular calcium in rat extraocular mus-cle. Am J Physiol. 1987;253:C375-C383.
8. Jacoby J, Kahn DN, Pavlica MR, Ko K, Breinin GM.Diltiazem reduces the contractility of extraocular
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018
304 Investigative Ophthalmology & Visual Science, February 1993, Vol. 34, No. 2
muscles in vitro and in vivo. Invest Ophthalmol Vis Sci.1990;31:569-576.
9. Finkelstein M, Farbowitz M, Kastner R, et al. EGTAenhances diltiazem reduction of EOM contractility invivo (abstract). Invest Ophthalmol Vis Sci. 1992; 33(suppl):1335.
10. Bohle Th. The effect of the benzothiazepine diltiazemon force and Ca++ current in isolated frog skeletalmuscle fibres. J Physiol. 1992;445:303-318.
1 1. Chang CC, Lin S-O, Hong SJ, Chiou LC. Neuromus-cular block by verapamil and diltiazem and inhibitionof acetylcholine release. Brain Res. 1988; 454:332-339.
12. Esau SA. Interaction of theophylline, verapamil, anddiltiazem on hamster diaphragm muscle force in vitro.AmJ Physiol. 1988; 254:C365-C371.
13. Wachtel RE. Effects of diltiazem and verapamil on re-sponses to acetylcholine. Br J Pharmacol. 1987;92:561-566.
14. Williams JH, Ward CW. Enhancement of skeletal mus-cle fatigue by the calcium channel antagonist diltia-zem. Res Comviun Chern Pathol Pharmacol. 1990; 69:107-110.
15. JacobyJ, Patel N, Kastner R, Farbowitz M. Diltiazem+ EGTA reduce lid tension during light-flash inducedeye blink in the rabbit in vivo (abstract). Invest Ophthal-mol Vis Sci. 1992;33(suppl): 1099.
I 6. Brown BW Jr, Hollander N. Statistics: A Biomedical In-troduction. New York: John Wiley & Sons; 1977.
17. Sokal RR, Rohlf RH. Biometry. San Francisco: WHFreeman and Co; 1969.
.18. Wali FA. Interactions of nifedipine and diltiazem withmuscle relaxants and reversal of neuromuscularblockade with endrophonium and neostigmine. JPharmacol. 1986; 17:244-253.
19. Meshul CK. Calcium channel blocker reverses anti-
cholinesterase-induced myopathy. Brain Res. 1989;497:142- 148.
20. Manning KA, Evinger C. Different forms of blinks andtheir two-stage control. Exp Brain Res. 1986; 64:579-588.
21. Lowitzsch K, Liider G. Habituation of the blink re-flex: computer assisted quantitative analysis. Electroen-cephalogr Clin Neurophysiol. 1985;60:525-531.
22. Rushworth G. Observations on blink reflexes. JNeurolNeurosurg Psychiatry. 1962;25:93-108.
23. Evinger C, Sibony PA, Manning KA, Fiero RA. A phar-macological distinction between the long and short la-tency pathways of the human blink reflex revealedwith tobacco. Exp Brain Res. 1988; 73:477-480.
24. Gonzalez-Serratos H, Valle-Aguilera R, Lathrop DA,del Carmen Garcia M. Slow inward calcium currentshave no obvious role in muscle excitation-contractioncoupling. Nature. 1982;298:292-294.
25. Walsh KB, Bryant SH, Schwartz A. Action of diltiazemon excitation-contraction coupling in bullfrog skeletalmuscle fibers, y Pharmacol Exp Ther. 1988; 245:531-536.
26. Vandenberg CA, Bezanilla F. Single-channel, macro-scopic, and gating currents from sodium channels inthe squid giant axon. BiophysJ. 1991;60:1499-1510.
27. Bhattacharya SK, Palmieri GMA, Bertorini TE, Nut-ting DF. The effects of diltiazem in dystrophic ham-sters. Muscle Nerve 1982;5:73-78.
28. Cavero I, Boudot J-P, Deauvray D. Diltiazem protectsthe isolated rabbit heart from the mechanical and ul-trastructural damage produced by transient hypoxia,low-flow ischemia and exposure to Ca++-free medium.J Pharmacol Exp Ther. 1983; 226:258-268.
29. Soza M, Karpati G, Carpenter S, Prescott S. Calcium-induced damage of skeletal muscle fibers is markedlyreduced by calcium channel blockers. Ada. Neuro-pathol. 1986; 71:70-75.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933396/ on 05/25/2018