Embed Size (px)
Citation preview

P1: ZBU
Metabolic Brain Disease [mebr] pp712-mebr-457401 December 19, 2002 15:30 Style file version Nov. 19th, 1999
Metabolic Brain Disease, Vol. 18, No. 1, March 2003 (C© 2003)
Effect of Blood Ammonia Elevation following OralGlutamine Load on the Psychometric Performanceof Cirrhotic Patients
Andrea Masini,1 Cesare Efrati,1 Manuela Merli, 1 Francesca Nicolao,1
Piero Amodio,2 Franco Del Piccolo,2 and Oliviero Riggio1,3
Received April 2, 2002; accepted July 10, 2002
Oral glutamine challenge is a method to increase blood ammonia and may be used to studythe ammonia lowering effect of drugs potentially useful in hepatic encephalopathy (HE).We tested its influence on the psychometric performance of 18 cirrhotic patients withoutHE. Twelve nonencephalopatic cirrhotic patients were studied before and after glutamineload (20 g in 100 mL tap water) and six patients before and after placebo (100 mL tap water)by using the Number Connection Test (NCT), the Covert Visual Attention Orienting Test(CVAOT), and the Scan Test (SCT). Blood ammonia increased significantly after glutamine(from 79± 34 to 211± 66µg/dL) but not after placebo (from 94± 41 to 88± 26). Nodifference in the NCT was found before and after glutamine load or placebo. The CVAOTwas similar after glutamine challenge and placebo, nor any interaction between Loads(glutamine or placebo)× Cue position was found, suggesting that glutamine load did notinfluence attention-orienting. SCT results were also similar after glutamine and placebo,suggesting a lack of influence on the working memory. Glutamine challenge is a safe methodto induce hyperammonemia in nonencephalopatic cirrhotic patients and, therefore, to studythe efficacy of ammonia lowering treatments.
Key words: Ammonia; cirrhosis; glutamine challenge; minimal encephalopathy; psychometric performance.
INTRODUCTION
Although the mechanisms involved in the pathogenesis of hepatic encephalopathy (HE)are not completely clear as yet, alterations in the nitrogen metabolism leading to an increaseof blood ammonia are important factors (Butterworth, 2000). Ammonia reaching the liverby the portal vein may derive from the small intestine, mainly as a result of the conversion ofdietary glutamine, and from the large intestine, where ammonia is produced by the bacterialmetabolism of urea and other nitrogen compounds. (Vinceet al., 1973). In patients withcirrhosis, the detoxification of ammonia by the liver is reduced as a consequence of theimpaired capacity of both urea and glutamine synthesis (Gerok and Haussinger, 1984).Thus, blood ammonia levels increase and become available to the central nervous systemwhere may exert toxic effects (Butterworth, 2000).
1Department of Clinical Medicine, University of Rome “La Sapienza,” Rome, Italy.2Department of Clinical and Experimental Medicine, University of Padua, Italy.3To whom correspondence should be addressed at Via Costantino Maes, 68, 00162 Rome, Italy. E-mail:[email protected]
270885-7490/03/0300-0027/0C© 2003Plenum Publishing Corporation
P1: ZBU
Metabolic Brain Disease [mebr] pp712-mebr-457401 December 19, 2002 15:30 Style file version Nov. 19th, 1999
28 Masini, Efrati, Merli, Nicolao, Amodio, Del Piccolo, and Riggio
Oral glutamine (GLN) challenge is a method for inducing a blood ammonia rise,similarly to what happens after a protein meal. Following an oral load of 20 g of GLN,the blood ammonia rises in cirrhotic patients, but not in controls or in post-liver transplantsubjects (Opponget al., 1997). Ammonia concentration peaks between 30 and 60 minafter the GLN load. This time span suggests that the rise in blood ammonia is due to themetabolism of GLN in the small intestine. GLN challenge may therefore be used to observethe ammonia lowering effect of those drugs potentially useful in the treatment of HE. Werecently published examples of these approaches by studying the effect of lactitol. (Masiniet al., 1999) and sodium benzoate. (Efratiet al., 2000) on the rise of ammonia after GLN load.
The effects of short rises of plasma ammonia levels on the brain functioning are notclear yet. According to Stahl (1963) no behavioral effect is to be expected, whereas Opponget al. (1997) detected a prolongation of the choice reaction time to light (and an increasedEEG amplitude of unclear meaning) by oral GLN challenge. More recently, Douglass et al.(2001) were able to induce psychometric and EEG slowings in cirrhotic patients with severeliver failure and minimal HE by increasing the plasma ammonia with an oral amino acidload, thus simulating a gastrointestinal bleeding.
Aim of the present study was to verify whether the rise in blood ammonia following anoral GLN load may cause alterations in the psychometric performance of nonencephalopaticcirrhotic patients.
PATIENTS AND METHODS
Eighteen male cirrhotic patients were included in the present study. Their characteristicsare reported in Table 1. None of them presented HE at the time of the study or prior to it.None were receiving lactulose, lactitol, or oral antibiotic treatments. All the patients wereunder a standard not protein-restricted hospital diet (protein content= 90 g/day) and werestudied the morning after an overnight fast. Twelve patients received 20 g of GLN in 100 mLtap water and six patients received a placebo (100 mL of tap water). Samples of free-flowingblood were taken in iced tubes and the whole blood venous ammonia (Ammonia Checker II,Menarini, Florence) was measured immediately before and 30 and 60 min after the load.Psychometric tests were administered the day before the GLN challenge or placebo, andrepeated immediately after the last blood sample (at 60 min). We selected those tests sensibleto a spectrum of cognitive alterations including psychomotor speed, attention, and workingmemory, which are expected to be altered in cirrhotic patients. (Amodioet al., 1999; McCrea
Table 1.Characteristics of the 18 Cirrhotic Patients
Treatment Glutamine (12) Placebo (6)
Age (years) 54± 13 60± 6Etiology Viral= 3; Crypto= 2; Alcohol=7 Viral = 5; Crypto= 1Sex Male= 12 Male= 6Child-Pugh’s class A= 3; B= 7; C= 2 B= 5; C= 1Child-Pugh’s score 7.7± 1.7 8.5± 1.0Bilirubin (mg/dL) 1.7± 1.6 1.3± 0.8Prothrombin activity (%) 67± 17 66± 19Albumin (g/dL) 3.0± 0.4 3.0± 0.2
P1: ZBU
Metabolic Brain Disease [mebr] pp712-mebr-457401 December 19, 2002 15:30 Style file version Nov. 19th, 1999
Oral Glutamine Challenge and Psychometric Tests 29
et al., 1996). A single investigator administered the following tests in a quiet and well-litenvironment:
• Number Connection Test (NCT) (Conn, 1977; Reitan, 1955, 1958). The NCT(Part A) measures the time needed to connect 25 circles containing numbers from1 to 25. It is a classical test to study HE and is considered to reflect an impairedvisuopractical capacity. The test was administered after an initial session of expla-nation. One of the four variants of equal difficulty was performed before and afterthe GLN challenge.• Covert Visual Attention Orienting Test (CVAOT) (Amodioet al., 1998a; Posner
et al., 1987; Posner and Petersen, 1990). According to Posner the test was per-formed as follows: the subjects sitting before a computer monitor were instructed tostare at a cross on the center of the screen. Ocular movements were ruled out by thedirect observation of the patient’s eyes. Two squares were displayed on the screenat approximately 5 degrees to the left and to the right of fixation point. The test wascomposed of 120 trials, preceded by 15 practice trials. In each trial, a stimulus (anasterisk) randomly appeared within the squares on the screen which could be eitherperipherally cued by an arrow appearing 200 ms before it (on the same side of thescreen in 80% of cases, “valid position”; on the opposite side in 20% of cases, “in-valid position”) or not cued (“neutral position”). In the latter case, a question markappeared in the middle of the screen 200 ms before the stimulus. The maximumintertrial interval was 2 s. The subject’s task was to press a button as quickly aspossible when the stimulus was displayed. The right index finger was used for thefirst 30 trials, the left index finger for the following 60, and the right index fingeronce again for the last 30. Mean reaction times in valid, invalid, and neutral positionswere measured, while reaction times above or below 2 standard deviations from themean were excluded, because of the poor informative value of such outliers. The dif-ference between the mean reaction times in the neutral position minus that of thevalid position (N–V interval) is considered theadvantage effect of the cue(Posnereffect), due to covert visual attention orienting where the stimulus is displayed. Thedifference between the mean reaction times in the invalid position minus that ofthe neutral position (I –N interval) is considered thecost effect of the cue, due tocovert visual attention orienting in the opposite side of the displayed stimulus. Thedifference between the mean reaction times in the invalid position minus that of thevalid position (I –V interval) was also measured because this index—-thevalidityeffectof the cue—-is considered a good measure of attention-orienting.• The Scan Test (SCT) (Amodioet al., 1998b, 1999; Sternberg, 1966, 1969). This test
is based on the Sternberg Paradigm and concerns memory scanning. This comput-erized digit recognizing test measures the mean reaction times and the percentageof errors in identifying whether there is at least a common digit in pairs of numbers(of 2–4 digits) subsequently displayed on the computer screen. The test was carriedout by displaying on the screen a series of 72 random, sorted pairs of numbers for3 s. Subjects were asked to tap “1” or “3” on the keyboard depending on whetherthey recognized a common digit in the pair of numbers. The reaction times wereweighted by the number of errors, as previously reported (Amodioet al., 1999).The SCT can be considered a test of working memory and sustained attention, and
P1: ZBU
Metabolic Brain Disease [mebr] pp712-mebr-457401 December 19, 2002 15:30 Style file version Nov. 19th, 1999
30 Masini, Efrati, Merli, Nicolao, Amodio, Del Piccolo, and Riggio
therefore a tool to assess the functions of prefrontal cortex. It was found to be asensitive tool to detect mild HE (Amodioet al., 1999).
All the patients performed the NCT and none of them had age and education-adjustedabnormal values. (Amodioet al., 2002). The patients who underwent GLN challenge werestudied by the CVAOT (six patients) or the SCT (six patients). The patients treated with theplacebo underwent both the CVAOT and the SCT. All patients were carefully monitoredduring and after the loads to check for modifications in their mental or neurological status(asterisks).
The study was conformed to the Helsinki II declaration.
STATISTICAL ANALYSIS
The results are expressed as mean± SD, unless specified.The effect of GLN load on ammonia or psychometric variables was assessed by repeated
measures analysis of variance.
RESULTS
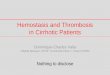
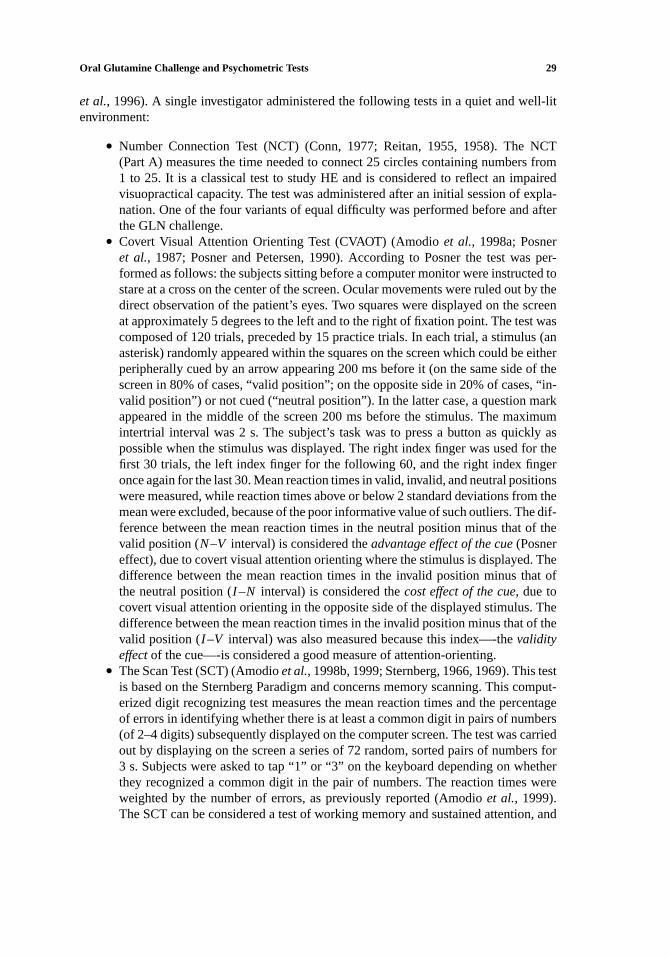
The oral GLN challenge test was well tolerated by all the patients. Venous plasmaammonia increased significantly in the GLN-treated patients (p = 0.006) 30 and 60 minafter the load (p < 0.001) with a significant Time× Treatment interaction (p < 0.001),due to the ammonia increase in the GLN-treated group only (Fig. 1).
In basal conditions, the performance of psychometric tests was comparable in thosepatients who underwent water load and in those who underwent GLN load: NCT (p = 0.8),CVAOT (p = 0.62), and SCT (p = 0.07). The data of patients who underwent water or GLNload were then pooled together.
Figure 1. Comparison of the variations of ammonia levels after placebo or GLN challenge test.Interaction treatment× Time: F(2, 30)= 17, p = 0.00001.
P1: ZBU
Metabolic Brain Disease [mebr] pp712-mebr-457401 December 19, 2002 15:30 Style file version Nov. 19th, 1999
Oral Glutamine Challenge and Psychometric Tests 31
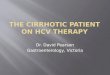
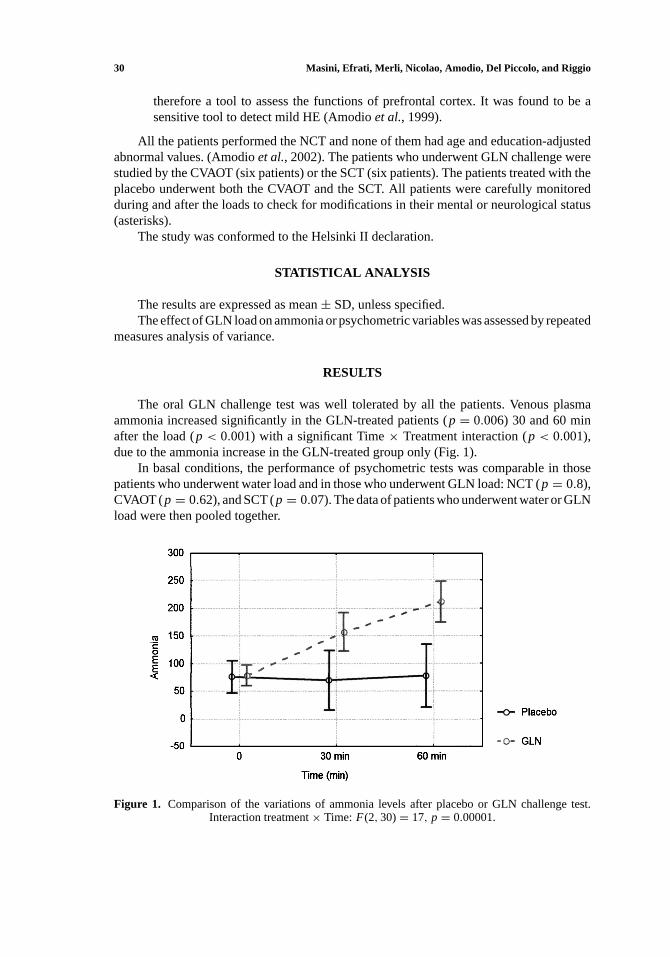
Figure 2. Comparison of the variations of the NCT in patients undergoing placebo or GLN oral load.
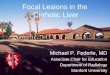
No difference in the NCT performance was found between patients who underwentGLN or water loads (p = 0.88): water basal 60± 15 s (mean± SEM.), postwater load56± 13 s, GLN basal 57± 5 s, and post-GLN load 55± 7.6 s (Fig. 2). The CVAOT showedthat covert attention orienting was detectable (p = 0.007). However, the reaction times didnot change after GLN load as compared with placebo (p = 0.63), nor any interaction wasfound between the Treatments (GLN or water)× Cue position (p = 0.12), thus showingthat GLN load did not influence attention-orienting (Fig. 3). The SCT improved in the
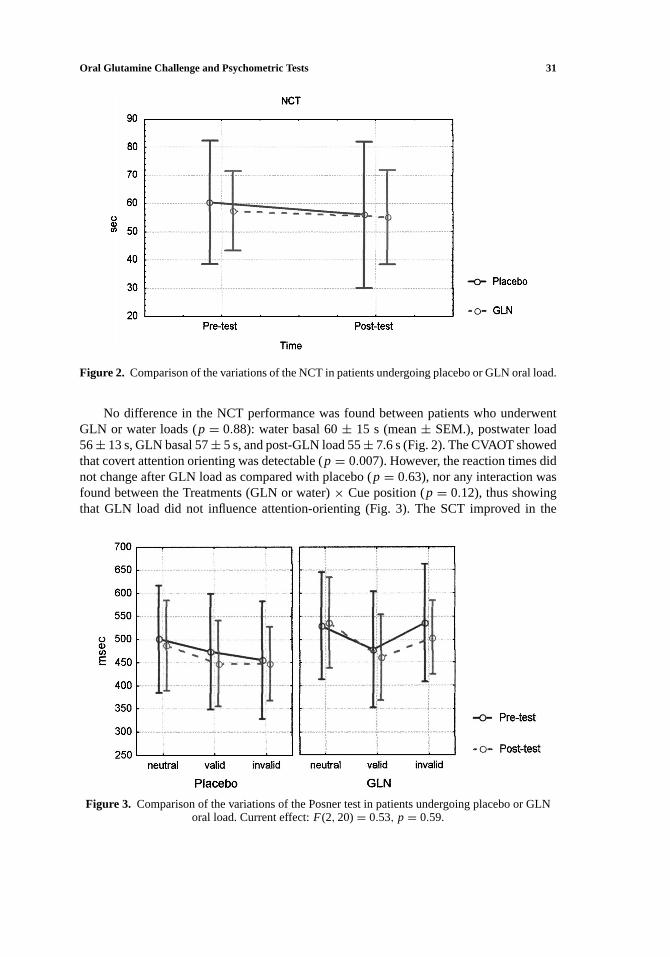
Figure 3. Comparison of the variations of the Posner test in patients undergoing placebo or GLNoral load. Current effect:F(2, 20)= 0.53, p = 0.59.
P1: ZBU
Metabolic Brain Disease [mebr] pp712-mebr-457401 December 19, 2002 15:30 Style file version Nov. 19th, 1999
32 Masini, Efrati, Merli, Nicolao, Amodio, Del Piccolo, and Riggio
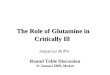
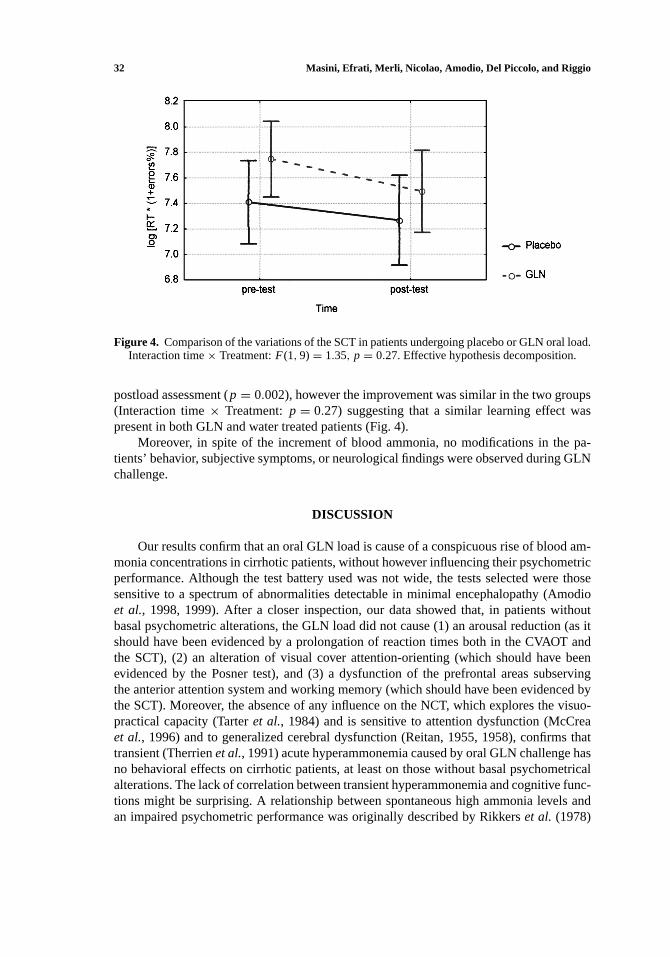
Figure 4. Comparison of the variations of the SCT in patients undergoing placebo or GLN oral load.Interaction time× Treatment:F(1, 9)= 1.35, p = 0.27. Effective hypothesis decomposition.
postload assessment (p = 0.002), however the improvement was similar in the two groups(Interaction time× Treatment:p = 0.27) suggesting that a similar learning effect waspresent in both GLN and water treated patients (Fig. 4).
Moreover, in spite of the increment of blood ammonia, no modifications in the pa-tients’ behavior, subjective symptoms, or neurological findings were observed during GLNchallenge.
DISCUSSION
Our results confirm that an oral GLN load is cause of a conspicuous rise of blood am-monia concentrations in cirrhotic patients, without however influencing their psychometricperformance. Although the test battery used was not wide, the tests selected were thosesensitive to a spectrum of abnormalities detectable in minimal encephalopathy (Amodioet al., 1998, 1999). After a closer inspection, our data showed that, in patients withoutbasal psychometric alterations, the GLN load did not cause (1) an arousal reduction (as itshould have been evidenced by a prolongation of reaction times both in the CVAOT andthe SCT), (2) an alteration of visual cover attention-orienting (which should have beenevidenced by the Posner test), and (3) a dysfunction of the prefrontal areas subservingthe anterior attention system and working memory (which should have been evidenced bythe SCT). Moreover, the absence of any influence on the NCT, which explores the visuo-practical capacity (Tarteret al., 1984) and is sensitive to attention dysfunction (McCreaet al., 1996) and to generalized cerebral dysfunction (Reitan, 1955, 1958), confirms thattransient (Therrienet al., 1991) acute hyperammonemia caused by oral GLN challenge hasno behavioral effects on cirrhotic patients, at least on those without basal psychometricalalterations. The lack of correlation between transient hyperammonemia and cognitive func-tions might be surprising. A relationship between spontaneous high ammonia levels andan impaired psychometric performance was originally described by Rikkerset al. (1978)

P1: ZBU
Metabolic Brain Disease [mebr] pp712-mebr-457401 December 19, 2002 15:30 Style file version Nov. 19th, 1999
Oral Glutamine Challenge and Psychometric Tests 33
but not confirmed by other authors (Marchesiniet al., 1980) or when, among other factors,ammonia levels were included in a multivariate analysis (Queroet al., 1996). On the otherhand, a clear relationship between ammonia plasma levels and a minimal HE assessed byneurophysiological techniques was repeatedly reported (Amodioet al., 1998b, 2001; Queroet al., 1996). The effect of a transient acute ammonia elevation (induced by different loads)on the psychometric performance is variably reported in the literature. In fact, while noeffect was observed after an ammonia tolerance test by Rikkerset al.(1978) and Loguercioet al.(1991) or after GLN challenge as in the present study, Douglasset al.(2001) were ableto induce psychometric and EEG slowings in cirrhotic patients with severe liver failure andminimal HE by increasing plasma ammonia with an oral amino acid load simulating a gas-trointestinal bleeding. Although differences in the various loads utilized cannot be excluded,these apparently conflicting results can probably be explained by a different brain sensitivityto similar plasma ammonia levels. This conclusion can be drawn by the observations ofDouglasset al. (2001), who did not find cognitive effects of transient induced hyperam-monemia in well-compensated cirrhotic patients, as well as by the observations of Rohmerand Kurtz (1961) that EEG alterations (and clinical symptoms) developed approximately30–45 min after the ingestion of 5 g of ammonium acetate, only in those cirrhotic patientswho already had EEG alterations (i.e., minimal encephalopathy). This finding suggests thatencephalopathy develops only if the brain is “sensitized” to ammonia toxicity. The natureof this sensitization is still obscure. It may be due to brain-barrier alterations (Lockwoodet al., 1984), to pH (Krameret al., 2000), to the presence of other toxic substances (Zieve,1981), or to the lack or excess of metabolites due to cerebral ammonia metabolism. In thisregard, it is worth recalling that acute ammonia toxicity can be prevented by methionine-sulphoximine, which blocks brain ammonia detoxification via glutamine synthesis (Bleiet al., 1994). In addition, it should be noted that one of the reasons of the beneficial effectof BCAA or ornithine aspartate (Fujiwaraet al., 1986; Kircheiset al., 1997; Stauchet al.,1998; Therrienet al., 1991; Vogelset al., 1997) on encephalopathy could be the increaseof precursors for brain ammonia detoxification (Roseet al., 1998, 1999). This increasemay prevent the dysfunction of the tricarboxylic acid cycle, demonstrated by the increasedlactate production in portacaval shunted rats (Therrienet al., 1991). Moreover, the hypoth-esis that brain ammonia toxicity might depend on the availability of precursors used in itsdisposal fits in quite well with early observations showing that similar ammonia loads mayor may not cause encephalopathy in the same patient at different times (Rohmer and Kurtz,1961). Variations in the sensitivity to ammonia load may explain why we did not detectany neuropsychological effect of GLN oral challenge test, whereas Opponget al. (1997)found a mild prolongation of choice reaction times in a wider number of patients with anapparently similar severity of liver disease.
In conclusion, transient hyperammonemia induced by the GLN oral challenge testdid not alter the psychometric performance in nonencephalopatic cirrhotic patients andwas therefore confirmed to be a safe method to study the efficacy of ammonia loweringtreatments.
REFERENCES
Amodio, P., Del Piccolo, F., Marchetti, P., Angeli, P., Iemmolo, R., Caregaro, L., Merkel, C., Gerunda, G., andGatta, A. (1999). Clinical features and survival of cirrhotic patients with subclinical cognitive alterations
P1: ZBU
Metabolic Brain Disease [mebr] pp712-mebr-457401 December 19, 2002 15:30 Style file version Nov. 19th, 1999
34 Masini, Efrati, Merli, Nicolao, Amodio, Del Piccolo, and Riggio
detected by the number connection test and computerized psychometric tests.Hepatology29:1662–1667.
Amodio, P., Del Piccolo, F., Petteno, E., Mapelli, D., Angeli, P., Iemmolo, R., Muraca, M., Musto, C.,Gerunda, G., Rizzo, C., Merkel, C., and Gatta, A. (2001). Prevalence and prognostic value of quantifiedelectroencephalogram (EEG) alterations in cirrhotic patientsJ. Hepatol.35:37–45.
Amodio, P., Marchetti, P., Del Piccolo, F., Campo, G., Rizzo, C., Iemmolo, R.M., Gerunda, G., Caregaro, L.,Merkel, C., and Gatta, A. (1998a). Visual attention in cirrhotic patients: A study on covert visual attentionorienting.Hepatology27:1517–1523.
Amodio, P., Marchetti, P., Del Piccolo, F., Rizzo, C., Iemmolo, R.M., Caregaro, L., Gerunda, G., and Gatta, A.(1998b). Study on the Sternberg paradigm in cirrhotic patients without overt hepatic encephalopathy.Metab.Brain Dis.13:159–172.
Amodio, P., Wenin, H., Del Piccolo, F., Mapelli, D., Montagnese, S., Pellegrini, A., Musto, C., Gatta, A., andUmilta, C. (2002). Variability of Trailmaking Tests, Symbol Digit Test and Line Trait Test in normal people.A normative study taking into account age-dependent decline and sociobiological variables.Aging Clin. Exp.Res.14:117–131.
Blei, A.T., Olafsson, S., Therrien, G., and Butterworth, R.F. (1994). Ammonia-induced brain edema and intracranialhypertension in rats after portacaval anastomosis.Hepatology19:1437–1444.
Butterworth, R.F. (2000). Complications of cirrhosis III. Hepatic encephalopathy.J. Hepatol.32:171–180.Conn, H.O. (1977). Trailmaking and number-connection tests in the assessment of mental state in portal systemic
encephalopathy.Am. J. Dig. Dis.22:541–550.Douglass, A., Al Mardini, H., and Record, C. (2001). Amino acid challenge in patients with cirrhosis: A model
for the assessment of treatments for hepatic encephalopathy.J. Hepatol.34:658–664.Efrati, C., Masini, A., Merli, M., Valeriano, V., and Riggio, O. (2000). Effect of sodium benzoate on blood
ammonia response to oral glutamine challenge in cirrhotic patients: A note of caution.Am. J. Gastroenterol.95:3574–3578.
Fujiwara, M., Watanabe, A., Hashimoto, M., Yamauchi, Y., Nakatsukasa, H., Kobayashi, M., Higashi, T., andNagashima, H. (1986). Prevention of ammonia-induced brain edema in dogs infused with a branched-chainamino acid solution.Biochem. Med. Metab. Biol.36:207–209.
Gerok, W., and Haussinger, D. (1984). Ammonia detoxification and glutamine metabolism in severe liver diseaseand its role in the pathogenesis of hepatic coma. In (D. Haussinger and H. Sies, eds.),Glutamine Metabolismin Mammalian Tissues, Springer, Heidelburg, Germany, pp. 257–277.
Kircheis, G., Nilius, R., Held, C., Berndt, H., Buchner, M., Gortelmeyer, R., Hendricks, R., Kruger, B., Kuklinski,B., Meister, H., Otto, H.J., Rink, C., Rosch, W., and Stauch, S. (1997). Therapeutic efficacy ofL-ornithine-L-aspartate infusions in patients with cirrhosis and hepatic encephalopathy: Results of a placebo- controlled,double-blind study.Hepatology25:1351–1360.
Kramer, L., Tribl, B., Gendo, A., Zauner, C., Schneider, B., Ferenci, P., and Madl, C. (2000). Partial pressure ofammonia versus ammonia in hepatic encephalopathy.Hepatology31:30–34.
Lockwood, A.H., Bolomey, L., and Napoleon, F. (1984). Blood–brain barrier to ammonia in humans.J. Cereb.Blood Flow Metab.4:516–522.
Loguercio, C., Del Vecchio Blanco, C., and Coltorti, M. (1991). Oral ammonia load in well compensated cirrhosis:Effect on psychometric tests. In (F. Bengtsson, B. Jepsson, T. Almdal, and H. Vilstrup, eds.),Progress inHepatic Encephalopathy and Metabolic Nitrogen Exchange, CRC Press, Boston, pp. 83–89.
Marchesini, G., Zoli, M., Dondi, C., Cecchini, L., Angiolini, A., Bianchi, F.B., and Pisi, E. (1980). Prevalence ofsubclinical hepatic encephalopathy in cirrhotics and relationship to plasma amino acid imbalance.Dig. Dis.Sci.25:763–768.
Masini, A., Efrati, C., Merli, M., Attili, A.F., Amodio, P., Ceccanti, M., and Riggio, O. (1999). Effect of lac-titol on blood ammonia response to oral glutamine challenge in cirrhotic patients: Evidence for an effectof nonabsorbable disaccharides on small intestine ammonia generation.Am. J. Gastroenterol.94:3323–3327.
McCrea, M., Cordoba, J., Vessey, G., Blei, A.T., and Randolph, C. (1996). Neuropsychological characterizationand detection of subclinical hepatic encephalopathy.Arch. Neurol.53:758–763.
Oppong, K.N., Al Mardini, H., Thick, M., and Record, C.O. (1997) Oral glutamine challenge in cirrhotics pre-and post-liver transplantation: A psychometric and analyzed EEG study.Hepatology26:870–876.
Posner, M.I., and Petersen, S.E. (1990). The attention system of the human brain.Annu. Rev. Neurosci.13:25–42.Posner, M.I., Walker, J.A., Friedrich, F.A., and Rafal, R.D. (1987). How do the parietal lobes direct covert attention?
Neuropsychologia25:135–145.Quero, J.C., Hartmann, I.J., Meulstee, J., Hop, W.C., and Schalm, S.W. (1996). The diagnosis of subclinical hepatic
encephalopathy in patients with cirrhosis using neuropsychological tests and automated electroencephalogramanalysis.Hepatology24:556–560.
Reitan, R.M. (1955). The relation of the Trail Making Test to organic brain damage.J. Consult. Psychol.19:393–394.
P1: ZBU
Metabolic Brain Disease [mebr] pp712-mebr-457401 December 19, 2002 15:30 Style file version Nov. 19th, 1999
Oral Glutamine Challenge and Psychometric Tests 35
Reitan, R.M. (1958). Validity of the Trail Making Test as an indicator of organic brain damage.Percept. Mot.Skills8:271–276.
Rikkers, L., Jenko, P., Rudman, D., and Freides, D. (1978). Subclinical hepatic encephalopathy: Detection, preva-lence, and relationship to nitrogen metabolism.Gastroenterology75:462–469.
Rohmer, F., and Kurtz, D. (1996).E.E.G. et ammoniemie dans les troubles nerveux des affections hepatiques,Roma, Edizione per il Congresso. Atti del 7◦ Congresso Internazionale di Neurologia, pp. 115–163.
Rose, C., Michalak, A., Pannunzio, P., Therrien, G., Quack, G., Kircheis, G., and Butterworth, R.F. (1998).L-ornithine-L-aspartate in experimental portal-systemic encephalopathy: Therapeutic efficacy and mechanismof action.Metab. Brain Dis.13:147–157.
Rose, C., Michalak, A., Rao, K.V., Quack, G., Kircheis, G., and Butterworth, R.F. (1999).L-ornithine-L-aspartatelowers plasma and cerebrospinal fluid ammonia and prevents brain edema in rats with acute liver failure.Hepatology30:636–640.
Stahl, J. (1963). Studies of the blood ammonia in liver disease. Its diagnostic, prognostic, and therapeutic signifi-cance.Ann. Intern. Med.58:1–21.
Stauch, S., Kircheis, G., Adler, G., Beckh, K., Ditschuneit, H., Gortelmeyer, R., Hendricks, R., Heuser, A.,Karoff, C., Malfertheiner, P., Mayer, D., Rosch, W., and Steffens, J. (1998). OralL-ornithine-L-aspartatetherapy of chronic hepatic encephalopathy: Results of a placebo-controlled double-blind study.J. Hepatol.28:856–864.
Sternberg, S. (1966). High-speed scanning in human memory.Science153:652–654.Sternberg, S. (1969) Memory-scanning: Mental processes revealed by reaction-time experiments.Am. Sci.57:421–
457.Tarter, R.E., Hegedus, A.M., Van Thiel, D.H., Schade, R.R., Gavaler, J.S., and Starzl, T.E. (1984). Nonalco-
holic cirrhosis associated with neuropsychological dysfunction in the absence of overt evidence of hepaticencephalopathy.Gastroenterology86:1421–1427.
Therrien, G., Giguere, J.F., and Butterworth, R.F. (1991). Increased cerebrospinal fluid lactate reflects deteriorationof neurological status in experimental portal-systemic encephalopathy.Metab. Brain Dis.6:225–231.
Vince, A., Dawson, A.M., Park, N., and O’Grady, F. (1973). Ammonia production by intestinal bacteria.Gut14:171–177.
Vogels, B.A., Karlsen, O.T., Mass, M.A., Bovee, W.M., and Chamuleau, R.A. (1997).L-ornithine vsL-ornithine-L-aspartate as a treatment for hyperammonemia-induced encephalopathy in rats.J. Hepatol.26:174–182.
Zieve, L. (1981). The mechanism of hepatic coma.Hepatology1:360–365.