Embed Size (px)
DESCRIPTION
Purpose To determine if the femtosecond laser be used to create reliable cuts under an irregular corneal surface.
Citation preview

Effect of an irregular anterior surface on a lamellar femtosecond
laser cut
Robert E. Fintelmann, MDMichele M. Bloomer, MD
Bennie H. Jeng, MD
Authors have no financial interest
Department of Ophthalmology University of California San Francisco

First femtosecond laser approved in 2000 to create lamellar cuts for LASIK
Now being used for Anterior and posterior lamellar keratoplastyCustomized trephination for penetrating
keratoplastyTunnel creation for intracorneal ring
segmentsAstigmatic keratotomy
Introduction

Purpose
To determine if the femtosecond laser be used to create reliable cuts under an irregular corneal surface.

Methods
Three types of defects createdRectangle at 210µmManual 2.5 mm punchManual triangular defect
Three corneas masked with hydroxypropylmethylcellulose
Three corneas without masking agent

Lamellar cuts created with femtosecond laser (300µm depth, 9mm Diameter, power 3mJ, IntraLase, Model FS60, software v 1.12 Abbott Medical optics, Abbott Park, IL)
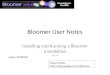
Corneas examined with ocular coherence tomography (RTVue SD-OCT with CAM-L lens) (Figure 1)
All corneas were then fixed in formaldehyde, cut through the created defect and examined under the microscope

Figure 1: OCT of Defects
En face OCT of rectangle
Transverse OCT of rectangle

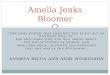
ResultsFemtosecond laser creates a smooth cut
under irregular surfaces (Figure 2)Irregularities on the surface can lead to
differences in thickness in the bed (Figure 3)
No difference in bed appearance between masked and unmasked corneas

Figure 2: OCT of bed
Thinning of bed under defect
Bed under punch
Bed under rectangle

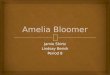
Figure 3:Histopathology of cornea under defect
Thicker bed outside area of defect
Thinner bed in area under defect

DiscussionFemtosecond lasers can help changing an
irregular surface into a smooth bed for a corneal transplant
Small study size insufficient to quantify the variability in the beds
Masking agent does not appear to be necessary for producing regular beds

A corneal graft with a regular surface placed into the now smoother bed may give a good clinical outcome

References Ratkay-Traub I, Juhasz T, Horvath C, et al. Ultra-short pulse (femtosecond) laser surgery:
initial use in LASIK flap creation. Ophthalmol Clin North Am. 2001; 14(2): 347-355, viii-ix. Harissi-Dagher M and Azar DT. Femtosecond laser astigmatic keratotomy for postkeratoplasty
astigmatism. Can J Ophthalmol. 2008; 43(3): 367-369. Ignacio TS, Nguyen TB, Chuck RS, Kurtz RM and Sarayba MA. Top hat wound configuration
for penetrating keratoplasty using the femtosecond laser: a laboratory model. Cornea. 2006; 25(3): 336-340.
Malta JB, Soong HK, Shtein R, et al. Femtosecond laser-assisted keratoplasty: laboratory studies in eye bank eyes. Curr Eye Res. 2009; 34(1): 18-25.
Rabinowitz YS, Li X, Ignacio TS and Maguen E. INTACS inserts using the femtosecond laser compared to the mechanical spreader in the treatment of keratoconus. J Refract Surg. 2006; 22(8): 764-771.
Seitz B, Langenbucher A, Hofmann-Rummelt C, Schlotzer-Schrehardt U and Naumann GO. Nonmechanical posterior lamellar keratoplasty using the femtosecond laser (femto-plak) for corneal endothelial decompensation. Am J Ophthalmol. 2003; 136(4): 769-772.
Yoo SH, Kymionis GD, Koreishi A, et al. Femtosecond laser-assisted sutureless anterior lamellar keratoplasty. Ophthalmology. 2008; 115(8): 1303-1307, 1307 e1301.