Embed Size (px)
Citation preview
5/22/2009
1
EEG in Status Epilepticus
Paul A. Garcia, M.D.
For discussion today
• Recognizing Seizures
• Recognizing Status
• Assessing Treatment
…hard to define, but "I know it when I see it "
Potter Stewart on pornography
Inter-observer Agreement
• Experienced: Kappa= 0.5
• Inexperienced: Kappa= 0.29
• Agreement also dependent upon pattern
Ronner HE et al, Seizure. in press
5/22/2009
2
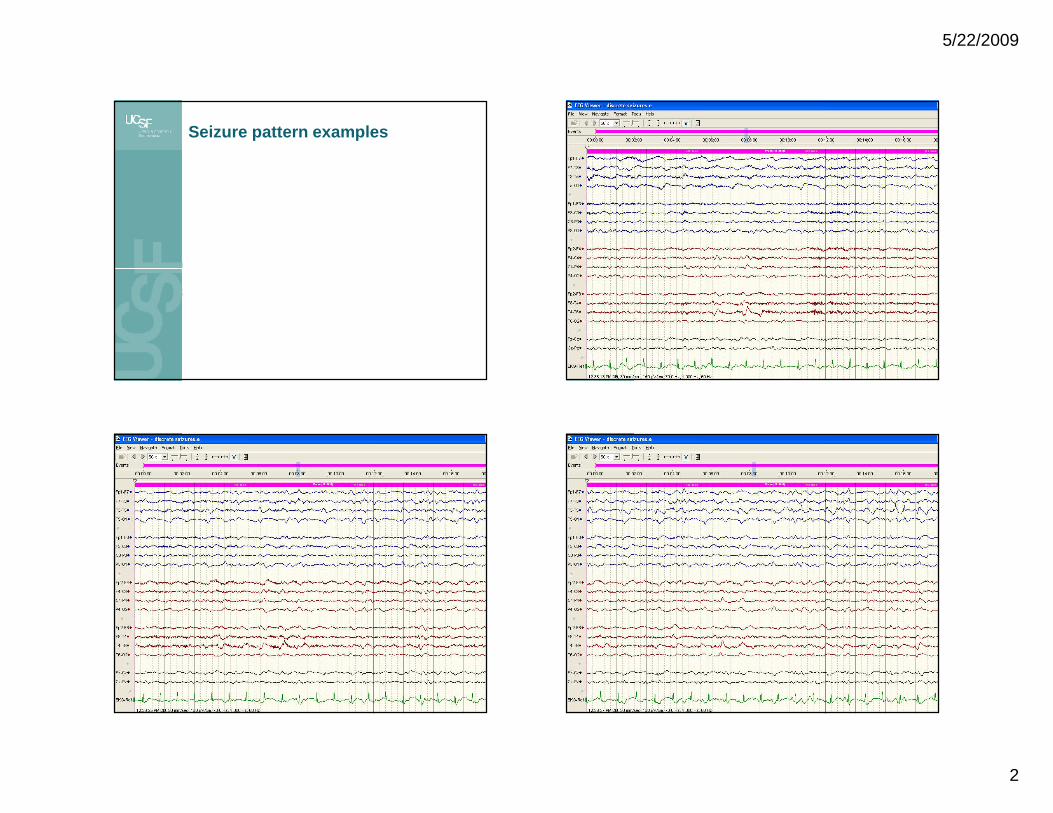
Seizure pattern examples

5/22/2009
3

5/22/2009
4
Less agreement

5/22/2009
5

5/22/2009
6
Recognizing Status
• Clinical
• EEG
22
Status Epilepticus: Definition
• Traditionally, >30 minutes continuous
• Current practice
– Tonic-Clonic seizures rarely greater than 2 minutes
– CPS rarely longer than 10 mins
When is EEG needed?
Clinical seizures don’t stop with initial treatment s
Clinical seizures stop but patient doesn’t improve as expected
Clinical seizures stop and there is no expectation of clinical improvement
Pharmacological paralysis
Baseline encephalopathy
Clinical information not diagnostic
24

5/22/2009
7
EEG patterns of status epilepticus
• Most clear when the patterns approach what we recognize as “ictal” based on experience with discrete seizures
• Some EEG patterns are common to seizures, normal physiological function and encephalopathy
• EEG patterns in rodent status
Discrete seizures
Merging seizures

5/22/2009
8
Continuous Discharges
FP1-C3FP1-C3
C3-O1C3-O1
FP1-T3FP1-T3
T3-O1T3-O1
FP2-C4FP2-C4
C4-O2C4-O2
FP2-T4FP2-T4
T4-O2T4-O2
CommentComment
TimeTime 0:01:01:080:01:01:08 0:01:01:100:01:01:10 0:01:01:120:01:01:12 0:01:01:140:01:01:14 0:01:01:160:01:01:16
FP1-C3
C3-O1
FP1-T3
T3-O1
FP2-C4
C4-O2
FP2-T4
T4-O2
Comment
Time 0:01:01:08 0:01:01:10 0:01:01:12 0:01:01:14 0:01:01:16
Continuous discharges with periods of attenuation Periodic discharges

5/22/2009
9
PLEDs
• Non-specific pattern suggesting focal injury superimposed on diffuse dysfunction
• Ictal EEG pattern with focal seizures
• EEG pattern following seizures
Status?
Approach to assessing PEDs
• Clinical context
• Benzodiazepine trial
– EEG response
– Clinical response
• The company that they keep
• Observation over time
Diagnosing “occult” status
• 18-34% with unexplained encephalopathy have seizures
• ~10% with unexplained encephalopathy have non-convulsive status epilepticus

5/22/2009
10
Risk factors for occult seizures
• Convulsive seizures
• Remote history of seizures/epilepsy
• Periodic discharges
Treating Refractory Status Epilepticus: EEG titration of anesthesia
38
Monitoring status epilepticus
• Continuous EEG
• Experienced ICU staff
• With the exception of HIE, outcomes are unpredictable—some do well after prolonged anesthesia
39
EEG in Status Epilepticus: Conclusions
Attention to common ictal EEG patterns will lead to recognition of status epilepticus in most cases
EEG is needed to guide treatment if initial medications fail to control status
• EEG is important to exclude ongoing seizures if clinical information doesn’t do so
• EEG is needed to diagnose “occult” status in patients with otherwise unexplained mental status changes
40



![Focal hemodynamic patterns of status epilepticus detected ... · epilepticus or subtle status epilepticus [4]. Electroenceph-alogram (EEG), the diagnostic gold standard, may not be](https://img.pdfslide.us/doc/110x75/6074493ed430437ef144c30f/focal-hemodynamic-patterns-of-status-epilepticus-detected-epilepticus-or-subtle.jpg)