Embed Size (px)
Citation preview

Journal of Pediatric Neurology 7 (2009) 25–43 25DOI 10.3233/JPN-2009-0272IOS Press
Review Article
EEG and the newborn
Maria Roberta Cilio∗Division of Neurology, Bambino Gesu Children’s Hospital, Rome, Italy
Received 22 December 2008
Accepted 24 December 2008
Abstract. Despite the evolution of new technologies for assessing neonatal brain function, electroencephalography (EEG) remainsa powerful tool for neurological diagnosis and prognosis in neonates. It is considered the gold standard for distinguishing epilepticseizures from non-epileptic paroxysmal events and for detecting subclinical seizure activity in high-risk babies. In those babiesseverely ill, EEG is even more efficient as predictive test than the neurological examination. The prognostic value of neonatalEEG has been long recognized in term as well as in preterm infants. Background patterns, more that patterns of ictal discharges,correlate significantly with the long-term outcome. Although most abnormalities on the neonatal EEG are nonspecific, certainpatterns can be highly suggestive for diagnosis. Prognostic value can be increased by obtaining early recordings, possibly withinthe first 48 hr of life, prolonged recordings to include samples of different activity states, and serial EEGs at short intervals to assessrapid changes that are likely to occur in high-risk infants. It is important to distinguish neonatal seizures from neonatal-onsetepilepsies and epilepsy syndromes. Both benign and malignant neonatal epilepsy syndromes exist. While benign familial neonatalseizures represents a neonatal syndrome with benign outcome, early myoclonic encephalopathy and Ohtahara syndrome are theearliest form of age-dependent severe epilepsy syndromes. Early myoclonic encephalopathy and Ohtahara syndrome are bothcharacterized by the presence of a burst-suppression EEG pattern. This pattern is usually associated with a poor prognosis andis considered the electroencephalographic correlate of a complete disconnection within the thalamocortical systems. Migratingpartial seizures in infancy is a newly recognized epilepsy syndrome whose onset can be in the neonatal period. It is characterizedby multifocal intractable seizures associated with psychomotor impairment. No etiology has been found so far. Different drugscurrently used in neonatal intensive care unit, especially if in the toxic range, can alter the EEG background. Those effects needto be taken in account in the interpretation of neonatal EEG.
Keywords: EEG, newborn, epilepsy, seizures
1. Introduction
Electroencephalography (EEG) is one of the oldest,yet most valuable, diagnostic and prognostic test inneonates. It has been used for decades to objectivelyassess the neurological status of critically ill neonatesand may provide objective evidence for abnormal cere-bral functioning following perinatal depression. It rep-resents an important component of the clinical assess-ment of newborns with neurologic disorders, since it
∗Correspondence: Dr. Maria Roberta Cilio, Division of Neurolo-gy, Bambino Gesu Children’s Hospital, Piazza S. Onofrio 4, 00165Rome, Italy. E-mail: [email protected].
can provide an important extension to the clinical eval-uation and should always be interpreted with the aware-ness of the gestational age of the child. It is consideredthe gold standard for seizures detection and quantifi-cation and for assessment of cortical activity. In crit-ically ill newborns, EEG is even preferable to neuro-logical examination, as their clinical repertoire is nar-row, making the neurodevelopmental examination ofrather limited value [1,2]. While brain-imaging tech-niques developed over the last decades have revolution-ized the diagnosis of major structural disorders of theneonatal brain, neurophysiologic studies provide con-tinuous documentation of brain function, with or with-out demonstrable structural correlates. EEG recording
1304-2580/09/$17.00 2009 – IOS Press and the authors. All rights reserved

26 M.R. Cilio / Neonatal electroencephalography
can detect seizures, with or without clinical manifes-tations, and especially if combined with video moni-toring, it can differentiate them from paroxysmal non-epileptic events in order to avoid unnecessary treatmentand to institute the correct treatment when required [3,4]. However, in the pediatric setting, this tool is notalways available, as it requires interpretation by a neu-rologist with expertise in neonatal EEG. These reasonshave led to the development of complementary typesof cerebral function monitoring, such as amplitude-integrated EEG, which is intended to be applied andinterpreted independently by neonatologists in order toallow a real-time interpretation of results. Neverthe-less, EEG is necessary if precise classification into nor-mal or mildly, moderately, or markedly abnormal back-grounds is desired, and it can be particularly helpful inthe newborn intensive care unite in identifying infantssuitable for neuroprotective strategies and allowing ac-curate diagnosis and stratification of encephalopathy, aprerequisite for the evaluation of results of neuropro-tective strategies [5,6].
2. Technique
For the proper assessment of neonatal EEGs, it ismandatory to record at least a phase of active sleep andquiet sleep. In infants less than 30 weeks of concep-tional age who spend most of their time in indetermi-nate sleep, a record of approximately 40 min durationcomprising the most continuous and the most discon-tinuous pattern may be practically sufficient [7]. TheEEG in the neonatal period should be performed allow-ing some stimulations and in an environment as quietas possible.
There are several technical considerations whenrecording from a neonatal scalp. High skin resistanceimpedes low-resistance scalp-to-electrode contact. Theminimum standard required includes at least ten scalpelectrodes placed following the 10–20 InternationalSystem of Electrode Placement, modified for neonates(Fig. 1) as well as non-cerebral channels. Whereasthe classification of sleep states was developed mainlyon the EEG patterns in adults, poligraphic recordingbecame the gold standard for state classification anddevelopmental physiology in the newborn. Therefore,the EEG recording in the newborn should always bea poligraphy that means a continuous and simultane-ous recording of cerebral electrical activity, eye move-ments’ electrooculogram, muscle activity [electromyo-graphy (EMG)], heart activity (electrocardiogram) and
Fig. 1. Electrodes placement according to the 10-20 InternationalSystem modified for neonates.
respiratory activity. Respiratory monitoring should in-clude two respiratory monitors: a thoracic strain gaugeor motion transducer to detect chest wall movementsin one channel, and a thermistor to detect airflow inthe other channel. EMG should include a submen-tal EMG activity monitor. Such monitoring assistsin the identification of specific segments of the EEGsleep cycle and, especially if used together with high-synchronized video, facilitates the characterization ofseizures by correlating the clinical manifestations withthe ictal electrical discharge. Concordance betweenelectrographic and polygraphic signals marks the matu-ration of the central nervous system (CNS), as reflectedin EEG sleep development. Non-cerebral physiologicparameters may also be relevant to the clinical problemthat prompted the request for the EEG study, such asapnea. Important sources of artifact can be identifiedmore readily or eliminated by using non-cerebral mon-itors. As with adults, physiologic and non-physiologicartifacts must be properly identified in neonatal record-ings because the may interfere with the interpretation ofcerebral activity. The technologist should not only tryto identify the source of the artifact but eliminate suchartifacts during the recording. Accurate description bythe technologist may help the neurologist in the diag-nosis of a neurologic disorder in the neonate. It is im-portant to annotate the tracing with particular attentionto the state of activity (awake or asleep), to the pres-ence and type of eye movements, facial movements,sucking, crying, and any other events [7].

M.R. Cilio / Neonatal electroencephalography 27
3. Indications
There are no indications for systematical recordingof every newborn in the intensive care unit. However,an EEG should be considered when questions arise re-garding the baby’s abnormal neurological status or thepossibility of seizures. For instance, EEG will be re-quired for diagnosis of abnormal movements,autonom-ic signs (i.e. unexplained apnea, flushing of the face),abnormal neurological status (i.e. lethargy or hyperac-tivity), or reported fetal distress. In those cases, EEGmay allow recognition of patterns suggestive of spe-cific conditions such as inherited errors of metabolismor herpetic encephalitis, to detect focal abnormalitieslike in hemorrhagic or ischemic stroke or abscess, orto identify ictal discharges [8]. Serial studies more ac-curately document normal ontogeny or the evolutionof encephalopathic changes than do single recordings.The continuous changes that occur during early braindevelopment are often associated with striking changesin EEG pattern over short periods. Indeed, EEG pat-terns are expected to change according to the gesta-tional age. A trained interpreter of neonatal EEG canestimate the electrical maturity of the neonatal brainwith an accuracy of 2 weeks of the gestational age forpreterm infants and 1 week for full term infant [8,9]. Infact, CNS development of the immature brain in post-natal environment proceeds at about the same rate asduring fetal development and evolving electrical pat-terns reflect the conceptional age of the infant indepen-dently of his birth weight. Concordance between elec-trographic and polygraphic components of EEG sleepbegins as early as 30 weeks of estimated gestationalage and is complete after 36 weeks of estimated ges-tational age. The EEG also changes with behavioralstate cycles that show an increasing organization withadvancing conceptional age [10].
4. Prognostic value
It is generally accepted that the background EEG isa good prognostic tool in preterm infants as well asterm infants [11–16]. The EEG features used for prog-nostic purposes differ among authors. For prognosticpurposes, serial EEG recordings are more useful thana single recording [17]. Usually, various features aregrouped into different severity grades and correlatedwith outcome [13]. Some authors use some selectedfeatures such as discontinuity measures [18,19], matu-rational features [20,21], or sharp waves transient [22].
In the newborn with an acute hypoxic insult, the prog-nostic value of the EEG strongly depends on the dayof recording [17]. The longer the time between thehypoxic event and the pathologic tracing, the worst theprognosis. Conversely, EEGs obtained shortly after theinsult must be viewed with caution and a follow-upstudy is highly recommended.
The relationship between neonatal EEG findings andneurological outcome has been investigated in preterminfants younger than 33 weeks of gestation by Watan-abe et al. [15]. These authors defined changes in con-tinuity, frequency, and amplitude as acute stage abnor-malities, and changes in maturity and waves forms aschronic stage abnormalities. They also used the EEGto assess the timing of brain insult suggesting that acutestage abnormalities in EEG immediately after birth mayhave originated from insults occurring just before birth.In their study, the absence of chronic stages abnormal-ities was associated with a favorable outcome in 88%,while dysmature pattern was associated with mentalretardation or borderline outcome in 68%. Whereasmildly disorganized patterns were associate with nor-mal outcome in 52%, severely disorganized patternswere associated with moderate or severe CP in 79%of cases [15]. Also, serial EEG recordings beginningimmediately after birth demonstrated to be particular-ly useful to assess the timing and the degree of braininjuries and to elucidate their pathogenesis in youngpreterm infants [15].
The potential of neuroprotective therapies, such ashypothermia, has raised the importance of accurate pre-diction of outcome in the first 6 hr of life [6,23,24].EEG remains our best method of predicting neurologicoutcome in hypoxic ischemic encephalopathy [11,12,14]. A normal or mildly abnormal EEG in the first 24 hrof life has a positive predictive value of 94% in predict-ing a normal neurologic outcome. In contrast, a severe-ly abnormal or inactive EEG predicts death or severedisability in the great majority of cases. Moderate ab-normalities will be associated with neurologic disabili-ty in 60% of cases. Sarnat scoring has a good predictivevalue, but cannot be assessed until 24 hr of age, too latefor benefiting from currently available neuroprotectivetherapies. In contrast, EEG grading can be assignedsoon after delivery and offers more reliable prognosisthan the Sarnat score alone [12,25] Early amplitude-integrated EEG has been shown to accurately predictthe severity of encephalopathy and long-term neuro-logic outcome [26]. For this reason, this tool has beenused in the recruitment of infants with moderate andsevere encephalopathy to clinical trials of neuroprotec-

28 M.R. Cilio / Neonatal electroencephalography
tive hypothermia, giving promising results [23]. How-ever, amplitude integrated EEG shows poor reliabilitycompared with continuous EEG when reported by in-experienced personnel, and does not allow localizationof pathology or seizure activity [27].
While most neonatal EEG patterns are nonspecific,the EEG may be the first test to guide the clinician inreaching an unsuspected diagnosis. For example, aninterhemispheric or regional asymmetry of backgroundpattern is often the first clue for underlying lesion, suchas a prenatal ischemic event, unsuspected by history orexamination. Several EEG features may suggest dys-genetic brain anomalies, inborn errors of metabolism,such as non-ketotic hyperglycinemia and pyridoxinedependency, CNS infections like herpes simplex virusencephalitis. In the context of ictal disorders, the EEGhas been shown to be an excellent predictor of outcomeby the vast majority of prospective or retrospective in-vestigations performed during three decades. Manyauthors reached the conclusion that, for prognostic pur-poses, the background EEG patterns are more signif-icant that the patterns of EEG discharge. In a studyof 137 full-term infants with neonatal seizures, Roseand Lombroso [28] found that neonates with seizureswho had a normal EEG had an 86% chance of nor-mal development at age 4 yr. Conversely, in neonateswith low amplitude, periodic or multifocal spikes in theinterictal EEG background had only a 7% chance fornormal development. Monod et al. [29] found simi-lar correlations. for neonates presenting with seizures.In a review of 691 EEGs performed in 270 mostlyterm-born neonates recorded in the first month of age,they showed that normal EEGs were highly correlatedwith favorable outcome, while low-voltage, inactive,or burst-suppression EEGs were highly prognostic ofpoor outcome both in preterm and full-term infants. Inanother study, Rowe et al. [30] supported these findingsin 74 full-term and preterm neonates with seizures, em-phasizing that EEG background was more predictive ofoutcome than interictal sharp waves.
Normalization of a previously abnormal pattern mayindicate a minimal impact of a brain insult on matu-ration. Conversely, progressive deterioration of pre-viously normal or moderately abnormal patterns fa-vors the possibility of long-term neurological sequelae.Repeated recordings provide the clinician with greaterpredictive information than those derived from a singleEEG [31]. However, some EEG patterns are so severe-ly abnormal that they are considered sufficient for theformulation of the prognosis, without the need for seri-al tests. Some authors feel that predictions can be accu-
rately be advanced when the initial EEG shows an inac-tive or isoelectric pattern or a burst-suppression pattern,even if the test is obtained shortly after birth [11,28,29].In order to diagnose an isoelectric pattern, most authorsrequire the absence of all discernible cerebral electricalactivity recording at a sensitivity of 2 µV/mm [32]. Thetechnical requirements for the diagnosis of isoelectricrecordings in neonates are the same as in adults, name-ly, using the highest gains, long time constants, andlong interelectrodes distances, and meticulous attentionto artifacts. An isoelectric pattern is most commonlyseen following severe asphyxia, circulatory collapse,and massive intracerebral hemorrhages. It can alsobeen seen in severe malformation of the brain, such ashydranencephaly or massive hydrocephalus. In the ab-sence of drug intoxication, acute hypoxemia, hypother-mia, and postictal state, this EEG pattern carries a poorprognosis: most neonates with isoelectric EEG eitherdie in the neonatal period or suffer severe neurologicdeficits [11]. Very rarely in the newborn, EEG activitymay return normal after an isoelectric EEG recordedin the first 24 hr following an acute hypoxic-ischemicevent. Usually, in the survivors, the isoelectric EEG isfollowed by other abnormal patterns, particularly low-amplitude or burst-suppression backgrounds [33].
Burst suppression pattern on the neonatal EEG isusually associated with a poor outcome. This patternis characterized by burst of high voltage activity (75–200 µV) lasting 1 to 10 sec with mixed features (spikes,sharp waves, theta, delta) but no age-appropriate ac-tivity, alternating with periods of marked backgroundattenuation (voltage < 10 µV) lasting 2 to 45 sec. Thisperiodic pattern is persistent throughout awake andasleep states, unreactive and unaltered by exogenousstimuli (Fig. 2).
Steriade et al. [34] have investigated the cellularcorrelates of EEG burst-suppression patterns in ani-mals. In this study, burst-suppression was elicitedby the administration of an anesthetic agent. About95% of cortical cells entered burst-suppression, in closetime-relation with EEG activity, displaying sequencesof phasic depolarizing events associated with burstsof EEG waves and an electrical silence of the neu-ronal membrane during flat EEG periods. In contrastwith cortical neurons, only 60–70% of thalamic cellsceased firing before overt EEG burst-suppression andwas completely silent during flat periods of EEG ac-tivity, while the remaining 30–40% showed intrinsicpacemaking properties discharging rhythmic (1–4 Hz)spike bursts during periods of EEG silence. However,with the deepening of burst-suppression, when silent

M.R. Cilio / Neonatal electroencephalography 29
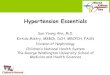
Fig. 2. Burst-suppression pattern in a 3-day-old full-term newborn. An alternating pattern of high-voltage mixed frequency activity and voltageattenuation indicates severe diffuse cerebral dysfunction. The bursts contain no age-appropriate activity. The muscle activity over the deltoidsand the irregular respiratory pattern differentiate the awake (A) from the sleep (B) state, while the cortical activity with the burst-suppressionpattern is invariant.

30 M.R. Cilio / Neonatal electroencephalography
Fig. 3. Trace alternant during quiet sleep in a 10 days old full-term infant. This pattern is reactive to stimuli, and alternate with the continuouspattern of the active sleep. It can be distinguished from the burst-suppression by the presence of high-voltage slow wave activity that alternatewith period of low voltage activity. The low voltage activity of the trace alternant is higher compared with the interburst activity of theburst-suppression pattern.
EEG periods became longer than 30 sec, thalamic cellsalso ceased firing. The assumption that full-blownburst-suppression is achieved through virtually com-plete disconnection in brain circuits implicated in thegenesis of the EEG is corroborated by the revival ofnormal cellular and EEG activities after volleys settinginto action thalamic and cortical networks. A recentstudy demonstrated that a predominant interburst inter-val duration of more than 30 sec correlated with the oc-currence of both unfavorable neurologic outcome andsubsequent epilepsy, suggesting that the interburst du-ration, an easily quantitated EEG parameter, could bevaluable for the early estimation of neurologic progno-sis in those patients [35]. According to this study, aninfant whose EEG contains a predominant interburstinterval duration of more than 30 sec has a 100% prob-ability of experiencing severe neurologic disabilities ordeath and an 86% chance of developing subsequentepilepsy. Burst-suppression pattern has been observedin individuals with cerebral conditions disconnectingthe cortex from deep structures. Highly discontinu-ous pattern as seen in burst-suppression can result frombrain immaturity, extensive brain damage or dysfunc-tion. Such dysfunction may be only temporary or belong lasting when structural lesions or diffuse changesof metabolic origin have taken place. Transient EEG
burst-suppression is seen in barbiturate anesthesia andhypoxic-ischemic encephalopathy, while a persistentburst-suppression is observed in deep brain tumors, se-vere congenital metabolic disorders such as non-ketotichyperglycinemia, or extensive brain malformation suchas hemimegalencephaly [36].
The burst-suppression pattern is easy to differentiatefrom the discontinuous features normally seen duringnon-rapidly eye moved or quite sleep in infants above34–36 weeks corrected age, when trace alternant be-gins to emerge clearly. The discontinuous pattern oftrace alternant is distinguished from burst-suppressionby the presence of its interburst activity, by being reac-tive to stimulations, and by the presence of normal EEGfeatures for corrected ages (i.e., delta brushes, tempo-ral theta, or frontal sharp transient), whereas there isalso cycling of the discontinuous pattern with the con-tinuous one of the rapid eye movement sleep (Fig. 3).Problems may arise in diagnosing burst-suppression inpreterm infants less than 33–32 weeks, because of thetrace discontinue that normally occurs at ages that aremore immature. The most reliable clue to distinguishthe pathological pattern of burst-suppression from thenormal pattern of trace discontinue is the clear knowl-edge of the infant’s conceptional age. Therefore, tracealternant and trace discontinue are two patterns of dis-

M.R. Cilio / Neonatal electroencephalography 31
Fig. 4. Status epilepticus in a 2 days old full term infant with hypoxic ischemic encephalopathy. The background activity is low voltage.Electrographic continuous seizures shift from an area to another, with one seizure starting from the fronto-central region of the left hemisphere(A) and spreading in the occipital region of the same hemisphere (B), then affecting the frontal region of the contralateral hemisphere (C), andspreading to the occipital region of the right hemisphere (D).
continuity that are normal for some conceptional agesbut may be abnormal for others, while burst- suppres-sion is usually invariant and lack other features charac-teristic for the EEGs of neonates of various conception-al ages. Testing for reactivity, usually absent in burst-suppression, is also helpful. Nonetheless, in youngpreterm infants, serial recording are advisable beforeformulating the poor prognosis associated with burst-suppression. If such activity is persistent through re-peated recordings, invariant and unresponsive to stim-ulation, with prolonged interburst intervals, then such a
pattern may be considered equivalent to the pathologicburst-suppression seen at term, as suggested by Tharpet al. [37] in 1981.
5. Seizures
Normal neonates commonly exhibit a variety ofparoxysmal movements including nonconjugate eyemovements, sucking movements without associatedeye abnormalities, and sleep-related myoclonus. These

32 M.R. Cilio / Neonatal electroencephalography
Fig. 4, continued.
normal behaviors as well as pathologic conditions canbe difficult to distinguish from epileptic seizures, whichcan also have somewhat subtle manifestations. EEG isa necessary tool in distinguishing among these entities.In a study of EEG diagnosis of seizures in neonates,90% of abnormal movements suspicious for seizureswere found to be nonepileptic on EEG recording [1].The EEG should therefore be recorded at the begin-ning of the first symptoms, and, if possible, before anyseizure treatment. Epileptic seizures are most frequentin the neonatal period than in any other time of thelife [38,39]. A generally accepted definition of what
constitutes an ictal discharge has not been established,especially in the newborn. Most authors classify a dis-charge as ictal if it lasts at least 10 sec. However, doc-umented clinical and electrical seizures have been de-scribed in neonates as lasting only a few sec, while withincreasing age seizure activity becomes usually longerin duration. There are striking differences betweenseizures in neonates and those of older patient in ictalEEG patterns and their correlation with clinical symp-toms and pathology [13,40]. Neonates more often havebrief albeit recurrent seizures with a brief interictal in-terval, as opposed to a single prolonged ictal event as

M.R. Cilio / Neonatal electroencephalography 33
Fig. 5. Focal seizure in a 10 hr old full-term infant with right middle cerebral artery infarct. The focal ictal discharge begins in the rightcentro-parietal region and does not have a clinical correlate (uncoupling) (A). Four min after the onset of electroencephalography recording theinfants presents with left arm clonic movements (B) and the ictal discharge remains confined to the same region. Seven min later, the dischargeis still recorded from the same region (C).
observed in older infants. Seizures may have an erraticevolution, shifting from one area to another even in thepresence of a diffuse pathological process (Fig. 4). Justas seizures differ between neonates and older popula-tions, so does status epilepticus [41]. Data from Mor-
ton et al. [42] showed that, while neonates with statusepilepticus presented with brief, partial, serial seizureswith multiple foci, infants older than 2 months of agewere capable of having prolonged seizures with typi-cally one focus and possible secondary generalization.

34 M.R. Cilio / Neonatal electroencephalography
Fig. 5, continued.
In the newborn, seizures are unique because the neona-tal brain differs in both structure and physiology fromthose of older children and adults. Although the basicorganization of the cortex is in place, dendritic growth,axonal-dendritic connections, and synaptic stabiliza-tion are not complete in the newborn [43,44]. Likewise,myelination is immature, preventing the rapid well-organized spread of epileptic discharges [45]. There-fore, newborns may present with focal ictal dischargesin metabolic disorders (i.e. in hypocalcemic or hypo-glycemic seizures) as well as structural lesions (i.e. is-chemic stroke). However, in localized structural le-sions, seizures tend to be more consistently confinedin the affected region even in the case of prolonged orrecurrent event (Fig. 5). From a clinical point of view,a seizure may be defined as a paroxysmal alterationin neurological function, i.e. behavioral, motor, and/orautonomic function, associated temporally with EEGseizure activity (electro-clinical seizure). In some occa-sions, this correlation is lacking (clinical seizures with-out EEG correlate) but it is not clear whether these latterphenomena are related to an epileptic condition [46–49]. Mizrahi and Kellaway [48] in 1987 suggestedclassifying as epileptic seizures only those paroxysmalevents associated with concurrent electrical seizure ac-tivity. However, the inconsistent electrographic captureon the scalp recordings may depend on seizures arisingfrom foci deep within the brain, only inconsistently dis-
charging through final anatomic pathway. Conversely,an electrical seizure without clinical correlate may bethe result of a discharge arising from an area of thecerebral cortex, which does not express itself overtlyin the newborn, such as a sensory, or language area.However, these considerations should not detract fromthe use of EEG as the standard means for determiningthe presence of seizures before consideration of drugtreatment. As it can be difficult to distinguish epilepticfrom non-epileptic seizures, EEG may provide a moreaccurate endpoint than clinical observation in assessingtreatment efficacy [4].
On the other hand, electrical seizures without clin-ical correlate are frequently recorded, particularly inseverely ill newborns, with severe brain damage, or inthose who are pharmacologically paralyzed [39]. Inone study, only 21% of neonates had a clinical corre-late during electrographic seizures [3]. Another reportfound that only 45% of preterm and 53% of full-termneonates demonstrated clinical signs coincident withtheir electrographic seizures [50]. This electroclinicaldissociation can also be seen after anti-epileptic drugs(AEDs) treatment, particularly phenobarbital. Recent-ly, Scher et al. [4] performed a prospective study on thephenomenon of uncoupling in 59 neonates with elec-trically confirmed seizures. Uncoupling EEG-clinicalseizures was defined as the persistence of electrograph-ic seizures despite the suppression of � 50% clinical

M.R. Cilio / Neonatal electroencephalography 35
seizures after phenobarbital or phenytoin administra-tion. The uncoupling was noted in 58% of the neonatalcohort. Phenobarbital and phenytoin resulted in equalrate of uncoupling. Therefore, continuous EEG mon-itoring during treatment of neonatal seizures is advis-able in order to assess the efficacy of the treatment [4].
6. Neonatal epilepsy syndromes
It is important to distinguish neonatal seizures fromneonatal-onset epilepsies and epilepsy syndromes [51].An epilepsy syndrome is defined by the combination ofage at onset, seizure types, interictal and ictal patternand, when known, etiology. This concept, developedfour decades ago by Gastaut [52] and the School ofMarseille, and established by the International LeagueAgainst Epilepsy (ILAE), remains the gold standardfor diagnosis in pediatric epileptology [53]. The recog-nition of epileptic syndromes allows an accurate diag-nosis and management of seizure disorders, and it isuseful for research regarding treatments and etiologies,including the genetic ones. The identification of newsyndromes is based mainly on clinical and EEG crite-ria, and advances in neuroimaging and genetics haveby no means contradicted this concept [54]. However,most neonatal seizures are provoked seizures, ratherthan a true epilepsy syndrome, and despite the highprevalence of neonatal seizures, epileptic syndromesin neonates are rare but often overlooked. Current-ly, four epilepsy syndromes with onset in the neonatalperiod are recognized by the ILAE [55]: benign fa-milial neonatal seizures (BNFS), early myoclonic en-cephalopathy (EME), Ohtahara syndrome (OS), alsoknown as early infantile epileptic encephalopathy, andthe newly recognized syndrome of migrating partialseizures in infancy (MPSI) [56].
BNFS is a benign neonatal epilepsy syndrome clas-sified among the autosomal dominant focal epilepsiesand characterized by onset of seizures during the neona-tal period, normal neurologic examination, and neg-ative evaluation for another etiology of the seizures,normal developmental and intellectual outcome, andpositive family history of newborn seizures with be-nign outcome [57–61]. Seizures usually occur usuallyin clusters for a few days and then stop after severalweeks or months. Seizures are generally brief, lastingfor approximately 1 to 2 min, but may occur as manyas 20 to 30 times a day. Although generalized seizureshave also been reported, seizures are often of a mixedtype, starting with tonic posture, apnea and other au-
tonomic features, and progressing to focal or multifo-cal clonic seizures. EEG and video-EEG recordingsshowed that seizures started with bilateral, symmetricalflattening of the EEG for 5 to 19 sec; simultaneouslythere was apnea and tonic motor activity [58–61]. TheEEG flattening was followed by a long (1–2 min) bi-lateral discharge of spikes and sharp waves; simulta-neously, there were vocalizations, chewing, and focalor generalized clonic activity. The prominence of EEGand motor abnormalities varied between the left and theright from one seizure to the next in any given child.The seizures stopped without EEG or clinical postic-tal depression. Interictal EEG is of little assistance inmaking the diagnosis of BNFS. It may or may not beabnormal interictally, and no diagnostic features havebeen described. The abnormalities reported includedspikes, sharp waves, “epileptiform” patterns, “general-ized periodicity”, and slowing, but abnormal findingsare mostly transient [58–61].
In many published case reports, EEG was not per-formed or the results were not described in sufficientdetail. This the only autosomal dominant epilepsy syn-drome where the molecular basis has essentially beendefined, the vast majority of families carrying muta-tions or deletions of the potassium channel subunitgenes KCNQ2 or KCNQ3 on chromosomes twenty andeight respectively [62,63].
MPSI is a newly recognized epileptic syndrome, la-beled as “syndrome in development” in the ILAE di-agnostic scheme [55]. It is characterized by the onsetin the first 6 months of age of nearly continuous mul-tifocal partial seizures arising independently and se-quentially from both hemispheres, progression througha period of intractable seizures, subsequent neurolog-ical deterioration or arrest with complete loss of bothcognitive and motor abilities, and decline of head cir-cumference percentile [56,64–66,68–70]. To date, noetiology has been found for this disorder. ConventionalAEDs have proven ineffective as well as trials with var-ious vitamins and ketogenic diet. Successful controlof seizures has been reported with potassium bromideand levetiracetam [65–67]. Approximately 50 cases ofthis unusual but easily overlooked epilepsy syndromehave been studied. Although the usual time of seizureonset is at 1 to 6 months, onset in the first days of lifehas been reported, and approximately one-half of caseshad onset in the first month of life. Neuroimaging isreported as normal at onset and, when abnormal, showprogressive atrophy on follow-up. At onset, interictalEEG background varies from normal to diffuse slow-ing [56,64,68] and epileptiform discharges may be rare,

36 M.R. Cilio / Neonatal electroencephalography
Fig. 6. Ictal recording of an infant with migrating partial seizures in infancy. (A) A seizure starts over the left frontal region; (B) Another seizurestarts over the right frontal region before the end of the first event; (C) Simultaneous ictal discharges involve two different area of the brain, theleft frontal region and the right frontal region; (D) The first event ends while the second over the right frontal region persists; (E) Another ictaldischarge arises from the left frontocentral region.
with a unifocal or multifocal interictal patterns. Themultifocal character of the seizures may become evi-dent only with prolonged video-EEG monitoring, sug-
gesting that long-term monitoring plays an importantrole in the diagnosis of this disease [70]. EEGs reflectthe escalation of seizure activity as no infant continues

M.R. Cilio / Neonatal electroencephalography 37
Fig. 6, continued.
to have a normal EEG. The location of the ictal onsetvaries not only from side to side but also within a hemi-sphere. Electrographically, the single ictal event canshift from one region to another and from one hemi-sphere to the other and additional seizures beginning in
other areas in either hemisphere could start before theend of the first event, or immediately follow it [56,64–70] (Fig. 6). The clinical semiology of seizures beginswith focal motor movements that can alternate fromone side of the body to another with lateral deviation of

38 M.R. Cilio / Neonatal electroencephalography
Fig. 6, continued.
the head and eyes and eye jerks, twitching of the eye-lids, limb myoclonic jerks, and increased tone of oneor both limbs. In addition, it is worth mentioning thatin very young patients motor and autonomic signs areoften the only clinically relevant symptoms of seizures.Focal motor components are often accompanied by au-tonomic signs including flushing of the face, salivationand apnea. Truly generalized tonic-clonic seizures arevery rare. Prolonged observation soon shows that bothsides are alternatively affected, which demonstrates theinvolvement of the whole brain cortex. In a few cas-es [56,65–67,69] seizures were eventually controlledand these children partly recovered motor and cognitiveabilities. In all series, developmental outcome appearsbetter in those with better seizure control, comparedwith those with continued intractable seizures. Somepatients die [56,66,67,70]. More recently, Marsh etal. [69] published a series of infants with MPSI and aslightly better outcome than previously reported. Giventhe unique clinical and EEG features exhibited by chil-dren with MPSI, it is extremely unlikely that this con-dition could be mistaken for one of the severe epilepticsyndromes of neonatal period,such EME and OS, as theabove entities do have a typical interictal EEG pattern,such as burst-suppression in EME and OS. Differentlyfrom OS, spasms are lacking in MPSI [56,64–70].
OS and EME represent the earliest forms of epilepticencephalopathy. The concept of epileptic encephalopa-
thy has been recently introduced and indicated a condi-tion in which the epileptiform abnormalities themselvesare believed to contribute to the progressive disturbancein cerebral function [55].
OS and EME are both characterized by a very ear-ly onset, mainly within 1 month and often within thefirst 10 days, and by a suppression-bursts pattern onEEG [71,72]. For those reasons, they are also knownas neonatal epileptic encephalopathy with suppression-burst pattern [36].
EME is characterized clinically by the onset of frag-mentary myoclonus appearing in the first month of life,often associated with erratic focal seizures [73,74]. On-set sometimes occurs as early as a few hours after birth,and postnatal movements are sometimes reported bythe mother to be of the same type as those felt at theend of pregnancy. Erratic myoclonias shift typicallyfrom one part of the body to another in a random andasynchronous fashion. They are often restricted in afinger, a toe, the eyebrows, eyelids, or lips, occurring inthe same muscle group and often migrating elsewhere(Fig. 7). The polygraphic EEG recording demonstratesthe presence of myoclonias that are brief, single orrepetitive, and can be very frequent or nearly continu-ous. Massive, usually bisynchronous, axial myoclonicjerks may start from the onset of the disease or occurlater, often interspersed with erratic myoclonias [75].Simple focal seizures are usually subtle with eye devi-

M.R. Cilio / Neonatal electroencephalography 39
Fig. 7. Poligraphic electroencephalography recording in a 7-day-old full term infant with early myoclonic encephalopathy showing aburts-suppression pattern. The bursts last 2–3 sec and appear synchronously and asynchronously on the two hemispheres. The polygraphicrecording show an altered respiratory pattern with chest movements occurring almost exclusively during the bursts phase. The electromyographyallows to demonstrate fragmentary low amplitude myoclonic jerks involving both extremities and shifting randomly from one side to another.
ation or autonomic symptoms such as flushing of theface or apnea, but they can be focal clonic involvingany part of the body. Epileptic spasms are rare and gen-erally appear late in the course of the disease, usuallyat around 3–4 months of age. Neurological abnormali-ties are constant: very severe delay in psychomotor ac-quisitions, marked hypotonia, and disturbed alertness,sometimes with a vegetative state. Signs of peripheralneuropathy may also occur in rare cases. Although theetiology is mostly unknown, nonketotic hyperglycine-mia, pyridoxine or pyridoxal-phosphate deficiency ordependent, and congenital deficiency of the mitochon-drial glutamate transporter are known to produce a sim-
ilar clinical picture [75,76]. There is a high risk offamilial recurrence since in most cases the disease ap-pears to be inherited as an autosomal recessive trait.There is no effective treatment. The prognosis is poor:children with the condition survive in a persistent veg-etative state or die within the first or second year of life.OS shares with EME the age at onset, the suppression-bursts EEG, and, often, the poor prognosis [36].
The main differences are the seizure types, my-oclonic in EME and tonic spasms in OS. Therefore,in order to distinguish these disorders, in addition tothe usual recording, it is extremely useful to recordthe deltoid EMG to detect massive myoclonus or tonic

40 M.R. Cilio / Neonatal electroencephalography
spasms, and distal EMG (fingers, face) to detect errat-ic myoclonus. The distinction has a great importanceboth from a diagnostic point of view, as the search ofetiology can be best directed, and from a therapeuticpoint of view since vigabatrin might improve OS butnot EME [71,72]. Epileptic tonic spasms, the mainseizure type in OS, may occur in cluster or singly, bothin the awake or the sleep state. In addition, partial mo-tor seizures are observed in more than half of the cases.Brain imaging discloses gross structural abnormalitiesin most cases, such as Aicardi syndrome, hemimega-lencephaly, dento-olivary dysplasia, focal cortical dys-plasia. However, recently a de novo mutation in thegene encoding STXBP1 has been found in individualswith OS [77]. STXBP1 is involved in synaptic vesi-cles release, suggesting that the functionally impairedSTXBP1 may affect synaptic functions in the humanbrain. Psychomotor development is virtually absent ormarkedly retarded. Neurological examination showsvariable signs, depending on the brain malformation,and is frequently asymmetrical. Some patients mayshow an improvement after resection of the corticaldysgenesis [78].
7. Effect of drugs on neonatal EEG
Although there are few studies documenting the ef-fect of drugs on the neonatal EEG, it is evident that,as with older children, drugs, especially if in the toxicrange, can alter background activity. Prolonged peri-ods of inactivity on the EEG recording usually occurfollowing a loading dose of phenobarbital and may lastlonger than one hr following administration. Staudt etal. [79] argued that infants with phenobarbital plasmalevels above 6 mg/dL show significant background sup-pression. Other authors also reported the appearance ofisoelectric or invariant discontinuous record after treat-ment with phenobarbital [11,80]. Levels greater that25 µg/mL in neonates were reported to suppress EEGactivity [71]. In their study, Ashwal and Schneider [80]found discordance between EEG activity and radionu-clide uptake in infants with phenobarbital level between25 and 35 µg/mL. The lack of EEG activity with pres-ence of cerebral blood flood suggested that phenobarbi-tal suppressed EEG activity. In the same study, one in-fant who met the clinical criteria for brain death had ab-sent cerebral activity with level of 30 µg/mL. However,he developed some cerebral activity when the pheno-barbital level fell to zero [80]. These are important ob-servations that should be taken in account by electroen-
cephalographers, as phenobarbital therapy is frequent-ly administered to the neonate on a clinical basis, priorto the first EEG recording. However, this correlationwas not confirmed in preterm infants. Benda et al. [19]in studying 46 preterm infants found that a mean serumlevel of phenobarbital of 34.5 µg/mL with a range 14–64 µg/mL did not prolonged interburst intervals dur-ing trace discontinue in preterm infants. Among med-ication other than AEDs that may also affect the EEGtracing, morphine has been found to produce profound,largely reversible alteration of neonatal EEG as record-ed in preterm as well as full-term infants [81]. Con-versely, when Bye et al. [82] investigated the effectof morphine and midazolam on background EEG ofa group of neonates undergoing extracorporeal mem-brane oxygenation, they noted that despite midazolamand morphine serum levels were sufficient to produceadequate sedation, no patients had burst-suppressed orinactive EEG backgrounds. In addition, these authorspointed out that prolonged immobility due to sedationmay lead to scalp edema and subsequent artifactualattenuation of EEG background [82].
8. Conclusions
Despite being one of the oldest tests available, EEGremains the only neurodiagnostic procedure that pro-vides a continuous record of cerebral function over longperiods. Although other advanced methods of anatom-ic or functional investigations provide detailed snap-shots into cerebral pathophysiology, EEG provides avaluable assessment of cerebral functioning, and itsevolution and structure in time. However, after havingbeen in routine use for about half a century, EEG iscurrently facing unprecedented challenges in the new-born because of the survival of high-risk infants and thedevelopment of neuroprotective strategies. Therefore,its use should be extended to those centers that do notcurrently have access to either the equipment or exper-tise required for prompt neonatal EEG recording andinterpretation. Interictal EEG findings are particular-ly useful in predicting neurologic outcome in neonateswith seizures. Background EEG activity is an excellentindicator of outcome. The combination of age at onset,seizure types, interictal and ictal EEG patterns, definesan epilepsy syndrome. Delineating epilepsy syndromesin the newborn allows a greater precision in diagno-sis, prognosis and treatment than simply classifying theseizure types.

M.R. Cilio / Neonatal electroencephalography 41
References
[1] M.S. Scher, M.J. Painter, I. Bergman, M.A. Barmada andJ. Brunberg, EEG diagnoses of neonatal seizures: clinicalcorrelations and outcome, Pediatr Neurol 5 (1989), 17–24.
[2] G. Holmes, J. Rowe, J. Hafford, R. Schmidt, M. Testa and A.Zimmerman, Prognostic value of the electroencephalogram inneonatal asphyxia, Electroencephalogr Clin Neurophysiol 53(1982), 60–72.
[3] R.R. Clancy, A. Legido and D. Lewis, Occult neonatalseizures, Epilepsia 29 (1988), 256–261.
[4] M.S. Scher, J. Alvin, L. Gaus, B. Minnigh and M.J. Painter,Uncoupling of EEG-clinical neonatal seizures after antiepilep-tic drug use, Pediatr Neurol 28 (2003), 277–280.
[5] J.S. Wyatt, P.D. Gluckman, P.Y. Liu, D. Azzopardi, R. Ballard,A.D. Edwards, D.M. Ferriero, R.A. Polin, C.M. Robertson, M.Thoresen, A. Whitelaw and A.J. Gunn, CoolCap Study Group,Determinants of outcome after head cooling for neonatal en-cephalopathy, Pediatrics 119 (2007), 912–921.
[6] S. Sarkar, J.D. Barks and S.M. Donn, Should amplitude-integrated electroencephalogram be used to identify infantssuitable for hypothermic neuroprotection? J Perinatol 28(2008), 117–122.
[7] M.S. Sher, Electroencephalography of the newborn: normalfeatures, in: Clinical Neurophysiology of Infancy, Childhood,and Adolescence, (1st ed.), G.L. Holmes, S.L. Moshe and H.Royden Jones Jr., eds, Philadelphia: Butterworth HeinemannElsevier, 2006, pp. 46–69.
[8] C.T. Lombroso, Neonatal polygraphy in full-term and prema-ture infants: a review of normal and abnormal findings, J ClinNeurophysiol 2 (1985), 105–155.
[9] R.A. Hrachovy, E.M. Mizrahi and P. Kellaway, Electroen-cephalography of the newborn, in: Current Practice of Clini-cal Electroencephalography, D.D. Daly and T.A. Pedley, eds,New York: Raven Press, 1990, p. 201.
[10] F. Torres and C. Anderson, The normal EEG of the humannewborn, J Clin Neurophysiol 2 (1985), 89–103.
[11] C. Pezzani, M.F. Radvanyi-Bouvet, J.P. Relier and M. Monod,Neonatal electroencephalography during the first twenty-fourhr of life in full-term newborn infants, Neuropediatrics 17(1986), 11–18.
[12] H.B. van Lieshout, J.W. Jacobs, J.J. Rotteveel, W. Geven andM. v’t Hof, The prognostic value of the EEG in asphyxiatednewborns, Acta Neurol Scand 91 (1995), 203–207.
[13] G.L. Holmes and C.T. Lombroso, Prognostic value of back-ground patterns in the neonatal EEG, J Clin Neurophysiol 10(1993), 323–352.
[14] D. Selton and M. Andre, Prognosis of hypoxic-ischaemic en-cephalopathy in full-term newborns value of neonatal elec-troencephalography, Neuropediatrics 28 (1997), 276–280.
[15] K. Watanabe, F. Hayakawa and A. Okumura, Neonatal EEG:a powerful tool in the assessment of brain damage in preterminfants, Brain Dev 21 (1999), 361–372.
[16] S. Marret, D. Parain, J.F. Menard et al., Prognostic value ofneonatal electroencephalography in premature newborns lessthan 33 weeks of gestational age, Electroencephalogr ClinNeurophysiol 102 (1997), 178–185.
[17] T. Takeuchi and K. Watanabe, The EEG evolution and neu-rological prognosis of neonates with perinatal hypoxia, BrainDev 11 (1989), 115–120.
[18] J. Connell, L. de Vries, R. Oozer, R. Regev, L.M. Dubowitzand V. Dubowitz, Predictive value of early continuous elec-troencephalogram monitoring in ventilated preterm infants
with intraventricular hemorrhage, Pediatrics 82 (1988), 337–343.
[19] G.I. Benda, R.C. Engel and Y.P. Zhang, Prolonged inactivephases during the discontinuous pattern of prematurity in theelectroencephalogram of very-low-birthweight infants, Elec-troencephalogr Clin Neurophysiol 72 (1989), 189–197.
[20] J.S. Hanh and B.R. Tharp, The dysmature EEG pattern in in-fants with bronchopulmonary dysplasia and its prognostic im-plications, Electroencephalogr Clin Neurophysiol 76 (1990),106–113.
[21] E. Biagioni, L. Bartalena, P. Biver, R. Pieri and G. Cioni,Electroencephalographic dysmaturity in preterm infants: aprognostic tool in the early postnatal period, Neuropediatrics27 (1996), 311–316.
[22] E. Biagioni, A. Boldrini, U. Bottone, R. Pieri and G. Cioni,Prognostic value of abnormal EEG transients in preterm andfull-term neonates, Electroencephalogr Clin Neurophysiol 99(1996), 1–9.
[23] S.E. Jacobs, Selective head cooling with mild systemic hy-pothermia after neonatal encephalopathy: Multicentre ran-domised trial, Lancet 365 (2005), 663–670.
[24] S. Shankaran, A.R. Laptook, R.A. Ehrenkranz et al., Whole-body hypothermia for neonates with hypoxic-ischemic en-cephalopathy, N Engl J Med 353 (2005), 1574–1584
[25] D.M. Murray, C.A. Ryan, G.B. Boylan, A.P. Fitzgerald and S.Connolly, Prediction of seizures in asphyxiated neonates: cor-relation with continuous video-electroencephalographic mon-itoring, Pediatrics 118 (2006), 41–46.
[26] M.C. Toet, L. Hellstrom-Westas, F. Groenendaal, P. Eken andL.S. de Vries, Amplitude integrated EEG 3 and 6 hr after birthin full term neonates with hypoxic-ischaemic encephalopathy,Arch Dis Child Fetal Neonatal Ed 81 (1999), F19–F23.
[27] J.M. Rennie, G. Chorley, G.B. Boylan, R. Pressler, Y. Nguyenand R. Hooper, Non-expert use of the cerebral function moni-tor for neonatal seizure detection, Arch Dis Child Fetal Neona-tal Ed 89 (2004), F37–F40.
[28] A.L. Rose and C.T. Lombroso, A study of clinical, pathologi-cal, and electroencephalographic features in 137 full-term ba-bies with a long-term follow-up, Pediatrics 45 (1970), 404–425.
[29] N. Monod, N. Pajot and S. Guidasci, The neonatal EEG: statis-tical studies and prognostic value in full-term and pre-term ba-bies, Electroencephalogr Clin Neurophysiol 32 (1972), 529–544.
[30] J.C. Rowe, G.L. Holmes, J. Hafford et al., Prognostic value ofthe electroencephalogram in term and preterm infants follow-ing neonatal seizures, Electroencephalogr Clin Neurophysiol60 (1985), 183–196.
[31] R.L. Khan, M.L. Nunes, L.F. Garcias da Silva and J.C. daCosta, Predictive value of sequential electroencephalogram(EEG) in neonates with seizures and its relation to neurologicaloutcome, J Child Neurol 23 (2008), 144–150.
[32] K. Aso, M.S. Scher and M.A. Barmada, Neonatal electroen-cephalography and neuropathology, J Clin Neurophysiol 6(1989), 103–123.
[33] C.T. Lombroso, Some aspects of EEG polygraphy in newbornat risk for neurological disorders, Electroencephalogr ClinNeurophysiol Suppl 36 (1982), 652–663.
[34] M. Steriade, F. Amzica and D. Contreras, Corticaland thalamic cellular correlates of electroencephalographicburst-suppression, Electroencephalogr Clin Neurophysiol 90(1994), 1–16.

42 M.R. Cilio / Neonatal electroencephalography
[35] C.C. Menache, B.F. Bourgeois and J.J. Volpe, Prognostic valueof neonatal discontinuous EEG, Pediatr Neurol 27 (2002),93–101.
[36] J. Aicardi and S. Ohtahara, Severe neonatal epilepsies withsuppression-burst pattern, in: Epileptic Syndromes in Infancy,Childhood and Adolescence J. Roger, P. Thomas, M. Bureau,E. Hirsch, C. Dravet, P. Genton, eds, London: John LibbeyEurotex, 2005, pp. 39–50.
[37] B.R. Tharp, F. Cukier and N. Monod, The prognostic valueof the electroencephalogram in premature infants, Electroen-cephalogr Clin Neurophysiol 51 (1981), 219–236.
[38] M.J. Lanska, D.J. Lanska, R.J. Baumann and R.J. Kryscio, Apopulation-based study of neonatal seizures in Fayette County,Kentucky, Neurology 45 (1995), 724–732.
[39] E.M. Mizrahi, P. Plouin and R.R. Clancy, Neonatal seizures,in: Epilepsy: A Comprehensive Textbook, J. Engel, A. Ped-ley, J. Aicardi, M.A. Dichter, S. Moshe, eds, Philadelphia:Lippincott-Raven Publishers, 2007, pp. 639–658.
[40] S. Patrizi, G.L. Holmes, M. Orzalesi and F. Allemand, Neona-tal seizures:characteristics of EEG ictal activity in preterm andfullterm infants, Brain Dev 25 (2003), 427–437.
[41] J.N. Gaitanis and J.J. Riviello, Status epilepticus in neonates,in: Current Clinical Neurology: Status Epilepticus, F.W. Dris-lane, ed., Totowa, NJ: Humana Press Inc, 2005, pp. 339–352.
[42] L.D. Morton, D.J. Leszczyszyn, L. Kopec-Garnett et al., Mat-urational changes in the EEG of status epilepticus in the firstsix months of life, Neurology 54 (2000), 248.
[43] J.J. Volpe, Neurology of the Newborn, (5th ed.), Philadelphia:WB Saunders, 2008.
[44] M.J. Litzinger, C.L. Mouritsen, B.B. Grover, M.S. Esplinand J.R. Abbott, Regional differences in the critical peri-od neurodevelopment in the mouse:implications for neonatalseizures, J Child Neurol 9 (1994), 77–80.
[45] C.G. Wasterlain, H. Hattori, C. Yang, P.H. Schwartz, D.G.Fujikawa, A.M. Morin, B.E. Dwyer, Selective vulnerabilityof neuronal subpopulations during ontogeny reflects discretemolecula events associated with normal brain development,in: Neonatal Seizures, C.G. Wasterlain and P. Vert, eds, NewYork: Raven Press, 1990, pp. 77–80.
[46] M. Mizrahi and P. Kellaway, Diagnosis and Management ofNeonatal Seizures, Philadelphia: Lippincott-Raven, 1998.
[47] J.J. Volpe, Neonatal seizures: current concepts and revisedclassification, Pediatrics 84 (1989), 422–428.
[48] E.M. Mizrahi and P. Kellaway, Characterization and classifi-cation of neonatal seizures, Neurology 37 (1987), 1837–1844.
[49] D.A. Shewmon, What is a neonatal seizure? Problems in defi-nition and quantification for investigative and clinical purpos-es, J Clin Neurophysiol 7 (1990), 315–368.
[50] M.S. Scher, K. Aso, M.E. Beggarly, M.Y. Hamid, D.A. Steppeand M.J. Painter, Electrographic seizures in preterm and full-term neonates: clinical correlates,associated brain lesions, andrisk for neurologic sequelae, Pediatrics 91 (1993), 128–134.
[51] M. Mastrangelo, A. Van Lierde, M. Bray, G. Pastorino, A.Marini and F. Mosca, Epileptic seizures, epilepsy and epilepticsyndromes in newborns: a nosological approach to 94 newcases by the 2001 proposed diagnostic scheme for people withepileptic seizures and with epilepsy, Seizure 14 (2005), 304–311.
[52] H. Gastaut, Clinical and electroencephalographical classifica-tion of epileptic seizures, Epilepsia 10 (1969), 2–13.
[53] Commission on classification and terminology of the Interna-tional League Against Epilepsy (No authors listed), Propos-al for revised classification of epilepsies and epileptic syn-dromes, Commission on Classification and Terminology of the
International League Against Epilepsy, Epilepsia 30 (1989),389–399.
[54] R. Nabbout and O. Dulac, Epileptic syndromes in infancy andchildhood, Curr Opin Neurol 21 (2008), 161–166.
[55] J. Engel Jr., International League Against Epilepsy. A pro-posed diagnostic scheme for people with epileptic seizures andwith epilepsy: report of the ILAE Task Force on Classificationand Terminology, Epilepsia 42 (2001), 796–803.
[56] G. Coppola, P. Plouin, C. Chiron, O. Robain and O. Dulac,Migrating partial seizures in infancy: a malignant disorderwith developmental arrest, Epilepsia 36 (1995), 1017–1024.
[57] M.R. Cilio, Benign familial neonatal seizures, Orphanet En-cyclopedia, March, 2004.
[58] G.M. Ronen, T.O. Rosales, M. Connolly, V.E. Anderson andM. Leppert, Seizure characteristics in chromosome 20 benignfamilial neonatal convulsions, Neurology 43 (1993), 1355–1360.
[59] E. Hirsch, A. Velez, F. Sellal et al., Electroclinical signs ofbenign neonatal familial convulsions, Ann Neurol 34 (1993),835–841.
[60] A.M. Bye, Neonate with benign familial neonatal convulsions:recorded generalized and focal seizures, Pediatr Neurol 10(1994), 164–165.
[61] P. Plouin, Benign familial neonatal seizures and benign id-iopathic neonatal seizures, in: Epilepsy: A ComprehensiveTextbook, J. Engel, A. Pedley, J. Aicardi, M.A. Dichter andS. Moshe, eds, Philadelphia: Lippincott-Raven Publishers,2007, pp. 2287–2296.
[62] S.E. Heron, K. Cox, B.E. Grinton et al., Deletions or duplica-tions in KCNQ2 can cause benign familial neonatal seizures,J Med Genet 44 (2007), 791–796.
[63] M.V. Soldovieri, M.R. Cilio, F. Miceli et al., Atypical gatingof M-type potassium channels conferred by mutations in un-charged residues in the S4 region of KCNQ2 causing benignfamilial neonatal convulsions, J Neurosci 27 (2007), 4919–4928.
[64] M.R. Cilio, O. Dulac, R. Guerrini and F. Vigevano, Migratingpartial seizures in infancy, in: Epilepsy: A ComprehensiveTextbook,J. Engel, A. Pedley, J. Aicardi, M.A. Dichter, S.Moshe, eds, Philadelphia: Lippincott-Raven, 2007, pp. 2323–2328.
[65] K. Okuda, A. Yasuhara, A. Kamei, A. Araki, N. Kitamuraand Y. Kobayashi, Successful control with bromide of twopatients with malignant migrating partial seizures in infancy,Brain Dev 22 (2000), 56–59.
[66] G. Hmaimess, H. Kadhim, M.C. Nassogne, C. Bonnier and K.van Rijckevorsel, Levetiracetam in a neonate with malignantmigrating partial seizures, Pediatr Neurol 34 (2006), 55–59.
[67] M.R. Cilio, R. Bianchi, C. Armelisasso et al., Intravenouslevetiracetam terminates refractory status epilepticus in mi-grating partial seizures in infancy, Epilepsia 49 (2008), 213,(abstract).
[68] R.H. Caraballo, E. Fontana, F. Darra et al., Migrating focalseizures in infancy: analysis of the electroclinical patterns in17 patients, J Child Neurol 23 (2008), 497–506.
[69] E. Marsh, S.E. Melamed, T. Barron and R.R. Clancy, Migrat-ing partial seizures in infancy: expanding the phenotype of arare seizure syndrome, Epilepsia 46 (2005), 568–572.
[70] J.M. Wilmshurst, D.B. Appleton and P.J. Grattan-Smith, Mi-grating partial seizures in infancy: two new cases, J ChildNeurol 15 (2000), 717–722.
[71] O. Dulac, Epileptic encephalopathy, Epilepsia 42 (2001), 23–26.

M.R. Cilio / Neonatal electroencephalography 43
[72] R. Nabbout and O. Dulac, Epileptic encephalopathies: a briefoverview, J Clin Neurophysiol 20 (2003), 393–397.
[73] B. Dalla Bernardina, O. Dulac, N. Fejerman et al., Early my-oclonic epileptic encephalopathy, Eur J Pediatr 140 (1983),248–252.
[74] R. Nabbout, Early infantile epileptic encephalopathy, Or-phaned Encyclopedia, July, 2004.
[75] M. Mastrangelo, L. Canafoglia, S. Franceschetti et al., High-frequency rhythmic cortical myoclonus in a long-surviving pa-tient with nonketotic hypergylcemia, J Child Neurol 23 (2008),321–324.
[76] D. Wang, J.M. Pascual, H. Yang et al., Glut-1 deficiency syn-drome: clinical, genetic, and therapeutic aspects, Ann Neurol57 (2005), 111–118.
[77] H. Saitsu, M. Kato, T. Mizuguchi et al., De novo mutations inthe gene encoding STXBP1 (MUNC18-1) cause early infantileepileptic encephalopathy, Nat Genet 40 (2008), 782–788.
[78] J.M. Pedespan, H. Loiseau, A. Vital, C. Marchal, D. Fontanand A. Rougier, Surgical treatment of an early epileptic en-cephalopathy with suppression-bursts and focal cortical dys-plasia, Epilepsia 36 (1995), 37–40.
[79] F. Staudt, M.L. Scholl, R.W. Coen and R.B. Bickford, Pheno-barbital therapy in neonatal seizures and the prognostic valueof the EEG, Neuropediatrics 13 (1982), 24–33.
[80] S. Ashwal and S. Schneider, Brain death in the newborn, Pe-diatrics 84 (1989), 429–437.
[81] G.B. Young and O.P. da Silva, Effects of morphine on the elec-troencephalograms of neonates: a prospective, observationalstudy, Clin Neurophysiol 111 (2000), 1955–1960.
[82] A.M. Bye, D. Lee, D. Naidoo and D. Flanagan, The effectsof morphine and midazolam on EEGs in neonates, J ClinNeurosci 4 (1997), 173–175.

Video-EEG monitoring in newborns withhypoxic-ischemic encephalopathy treatedwith hypothermia
K.B. Nash, MD*S.L. Bonifacio, MD*H.C. Glass, MDJ.E. Sullivan, MDA.J. Barkovich, MDD.M. Ferriero, MDM.R. Cilio, MD, PhD
ABSTRACT
Background: Therapeutic hypothermia (TH) is becoming standard of care in newborns withhypoxic-ischemic encephalopathy (HIE). The prognostic value of the EEG and the incidence ofseizures during TH are uncertain.
Objective: To describe evolution of EEG background and incidence of seizures during TH, and toidentify EEG patterns predictive for MRI brain injury.
Methods: A total of 41 newborns with HIE underwent TH. Continuous video-EEG was performedduring hypothermia and rewarming. EEG background and seizures were reported in a standard-ized manner. Newborns underwent MRI after rewarming. Sensitivity and specificity of EEG back-ground for moderate to severe MRI brain injury was assessed at 6-hour intervals during TH andrewarming.
Results: EEG background improved in 49%, remained the same in 38%, and worsened in 13%. Anormal EEG had a specificity of 100% upon initiation of monitoring and 93% at later time points.Burst suppression and extremely low voltage patterns held the greatest prognostic value onlyafter 24 hours of monitoring, with a specificity of 81% at the beginning of cooling and 100% atlater time points. A discontinuous pattern was not associated with adverse outcome in mostpatients (73%). Electrographic seizures occurred in 34% (14/41), and 10% (4/41) developedstatus epilepticus. Seizures had a clinical correlate in 57% (8/14) and were subclinical in 43%(6/14).
Conclusions: Continuous video-EEG monitoring in newborns with HIE undergoing TH providesprognostic information about early MRI outcome and accurately identifies electrographic sei-zures, nearly half of which are subclinical. Neurology® 2011;76:556–562
GLOSSARYAED � antiepileptic drug; BS � burst suppression; HIE � hypoxic-ischemic encephalopathy; ROC � receiver operatingcharacteristic; SE � status epilepticus; TH � therapeutic hypothermia; UCSF � University of California, San Francisco.
Hypoxic-ischemic encephalopathy (HIE) after perinatal asphyxia is an important cause ofmortality and neurologic morbidity.1,2 Randomized clinical trials have demonstrated that mod-erate hypothermia is associated with a reduction in death and neurologic impairment at 18 to22 months of age.3,4 As a result, many centers now offer therapeutic hypothermia (TH) as aneuroprotective strategy for neonatal HIE.
Reliable early predictors of neurologic outcome in newborns after acute hypoxic-ischemicinsult are important for counseling families and for making thoughtful treatment decisions.Clinical assessment can help with prognosis,5-7 although sedating medications and clinicalchanges with TH8 are complicating factors. Brain MRI is highly predictive of neurologicoutcome,9,10 including in the setting of hypothermia,11 although it does not provide functional
*These authors contributed equally to this work.
From the Departments of Neurology (K.B.N., H.C.G., J.E.S., D.M.F., M.R.C.), Pediatrics (K.B.N., S.L.B., H.C.G., D.M.F.), and Radiology andBiomedical Imaging (A.J.B.), and Newborn Brain Research Institute (K.B.N., S.L.B., H.C.G., J.E.S., A.J.B., D.M.F., M.R.C.), University ofCalifornia, San Francisco; and Division of Neurology (M.R.C.), Bambino Gesu Children’s Hospital, Rome, Italy.
Study funding: Supported by NIH/NCRR UCSF-CTSI UL1 RR024131 and NIH P50 NS035902-12. S.L.B. was supported by NIH5T32HD007162. H.C.G. was supported by NIH/NCRR/OD UCSF-CTSI KL2 RR024130. M.R.C. was supported by E-Rare grant JTC 2007EUROBFNS from the European Commission.
Disclosure: Author disclosures are provided at the end of the article.
Address correspondence andreprint requests to Dr. MariaRoberta Cilio, Division ofNeurology, Bambino GesuChildren’s Hospital, Piazza S.Onofrio 4, 00165 Rome, [email protected]
556 Copyright © 2011 by AAN Enterprises, Inc.

assessment and its sensitivity for hypoxic-ischemic injury in the first 48 hours of life islimited. A single EEG recording during thefirst week of life in noncooled infants withHIE,12-14 and in infants with HIE treated withTH,15 may help predict neurologic outcome.However, continuous video-EEG monitoringis the gold standard for evaluating brain func-tion and for recording electrographic seizuresin neonates with HIE16,17 and it has not yetbeen reported in neonates with HIE undergo-ing TH.
Our aim was to describe the evolution ofthe EEG background during TH and re-warming and to determine the incidence ofelectrographic seizures in newborns with HIEtreated with moderate hypothermia. We alsosought to determine the prognostic value ofEEG background during TH using brainMRI as an early outcome measure.
METHODS Consecutive newborns with HIE who underwentTH with whole-body cooling at University of California, SanFrancisco (UCSF), between November 2007 and July 2009 wereincluded in this cohort study. Our TH clinical protocol is basedon published trials.3,4 Selection for TH included 1) �36 weeksgestational age at birth, 2) any of the following: cord or first gaspH �7.0, cord or first gas base deficit �12, 10-minute Apgarscore �5, or prolonged resuscitation, and 3) moderate to severeencephalopathy within 6 hours of birth. Exclusion criteria in-cluded suspected or known congenital malformation and inbornerrors of metabolism. TH was initiated as soon as possible afterbirth at UCSF or at the time of referral from the outside hospitaland consisted of whole-body moderate hypothermia (CincinnatiSub-Zero Blanketrol III) (target temperature 33.5°C) for 72hours followed by rewarming over approximately 6 hours. Allpatients received morphine infusion throughout TH to preventdiscomfort and shivering (10 –25 �g/kg/h, with boluses asneeded). Clinical and electrographic seizures were treated withantiepileptic drugs (AEDs) including lorazepam, phenobarbital,fosphenytoin, and levetiracetam according to institutional guide-lines. Clinical data were extracted from medical records.
Standard protocol approvals, registrations, and patientconsents. The Committee on Human Research at UCSF ap-proved the retrospective review of the clinical, EEG, and imag-ing data for this study.
Video-EEG monitoring. Video-EEG was initiated as soon aspossible after admission to the nursery. As part of our clinicalprotocol, infants are continuously monitored with a NicoletOnevideo-EEG system throughout TH and rewarming. A trainedtechnician applied surface electrodes according to the interna-tional 10–20 system, modified for neonates. EEG recordingswere interpreted by a pediatric neurophysiologist (J.S.) for clini-cal use in the acute setting. Using stored files, full video-EEGrecordings were scored in a standardized fashion by a pediatricneurophysiologist (M.R.C.) blinded to all clinical factors exceptpatient age. Predominant background pattern and occurrence of
electrographic seizures and status epilepticus (SE), with or with-
out clinical manifestations, were reported in 6-hour intervals
with the initiation of recording as time “0.” Clinical seizures
without EEG correlates were not considered. For the analysis, we
used the initial 6-hour interval (beginning of cooling), the 24- to
30-hour interval (midcooling), the last interval prior to rewarm-
ing (end of cooling), and the first interval after rewarming (post-
cooling). A seizure was defined as a repetitive, evolving, and
stereotyped pattern, with a definite beginning and end, a mini-
mum duration of 10 seconds, and a minimal amplitude of 2
�V.18,19 SE was defined as continuous seizure activity for at least
30 minutes or recurrent seizures for over 50% of 1–3 hours of
recording time.20 EEG background was classified into 5 patterns
as previously described21,22: 1) normal pattern for gestational age,
including recordings with transient periods of discontinuous ac-
tivity occupying less than 50% of the recording, with presence of
distinct state changes; 2) excessively discontinuous, with persis-
tence of discontinuous activity occupying more than 50% of the
recording and consisting of bursts of normal activity separated
by abnormally long, interburst intervals of more than 6 seconds
duration, and amplitude �25 and �5 �V, with poor state
changes; 3) depressed and undifferentiated, with persistently
low-voltage background activity with amplitude between 5 and
15 �V and without normal features; 4) burst suppression (BS),
invariant and unreactive pattern of bursts of paroxysmal activity
with mixed features but no age-appropriate activity lasting less
than 10 seconds alternating with periods of marked voltage at-
tenuation with amplitude �5 �V; 5) extremely low voltage, in-
variant and unreactive pattern, with amplitude �5 �V or with
no discernible cerebral activity.
Brain MRI. Infants were imaged shortly after rewarming (me-
dian of 5 days of life) using a specialized neonatal head coil on a
1.5-Tesla Signa EchoSpeed system (GE Medical Systems). Imag-
ing sequences included T1- and T2-weighted MRI and
diffusion-weighted imaging. A pediatric neuroradiologist
(A.J.B.), blinded to the clinical history, evaluated all images. In-
jury was scored using a system strongly predictive of neurodevel-
opmental outcome following neonatal HIE.23 We defined
normal to mild MRI injury as basal ganglia/thalamus score �2
and watershed score �3 and moderate to severe MRI injury as
basal ganglia/thalamus score �2 (involving both the thalamus
and the lentiform nucleus) or watershed pattern �3 (involving
both watershed cortex and white matter). A similar classification
was highly predictive for neurologic disability at 18 months of
age in newborns with HIE treated with hypothermia.11
Statistical analysis. All analyses were performed with STATA
software (Stata 10.1, Stata Corporation, College Station, TX).
�2 and Fisher exact tests were used to compare dichotomous
variables, and t test was used for continuous variables. Wilcoxon
rank sum test (Mann-Whitney U) was used to compare nonpara-
metric data. Receiver operating characteristic (ROC) curves were
used to assess the prognostic value of EEG background patterns
at each time interval. We considered significant a p value � 0.05.
RESULTS Patient population. During the study pe-riod, 49 newborns were treated with hypothermiaand 46 had continuous video-EEG available for re-view. Of these, 41 were evaluated with MRI. Fiveinfants who were deceased following redirection ofcare and were not studied with MRI were excluded.Four of them had an initial extremely low voltage
Neurology 76 February 8, 2011 557

cerebral activity, and one had BS pattern, bothpersisting for more than 24 hours. Their clinicalseverity was similar to those with persistent BS orextremely low voltage activity and moderate to se-vere MRI injury. Clinical characteristics of new-borns with respect to brain injury are presented intable 1. Mean hour of life to reach target tempera-ture was 5.2 � 1.9.
Video-EEG monitoring. EEG monitoring was initi-ated at a mean of 10.2 � 2.9 hours of life. All infantsreached target temperature before or within 1 hourafter EEG initiation. Mean duration of monitoringwas 90.9 � 28.2 hours. Nine infants received AEDsprior to the onset of EEG monitoring, and one ofthem subsequently developed subclinical seizures. In2 newborns, monitoring was discontinued prior torewarming.
EEG background pattern. From the beginning ofcooling to rewarming, the background improved in19 newborns (49%), remained the same in 15(38%), and worsened in 5 (13%). EEG backgroundpattern and the burden of moderate to severe MRIinjury at each time interval are presented in table 2.The background pattern for newborns with moder-ate to severe injury was significantly worse than forthose with no or mild injury for all monitoring timepoints (table 3). The sensitivity and specificity of
EEG background at specified time intervals wasgreatest at midcooling and beyond (table 4).
Beginning of cooling. None of the newborns with anormal background at the beginning of cooling hadmoderate to severe injury. Of the 15 newborns withan excessively discontinuous pattern, 4 (27%) hadmoderate to severe injury, 5 had mild injury, and 6were normal. In contrast, of the 14 newborns withBS or extremely low voltage patterns, 9 (64%) hadmoderate to severe injury. Of these, 4 had maximalMRI injury scores. Interestingly, 5 newborns withBS or extremely low voltage patterns at the beginningof cooling had a normal MRI or only mild injury. Inall 5 cases, however, the EEG improved by 12–18hours of recording, and in 3 of them the backgroundnormalized by midcooling.
Midcooling. One newborn whose EEG had nor-malized by this interval from a discontinuous back-ground at the beginning of cooling had moderate tosevere MRI injury; none of the remaining 14 new-borns with a normal EEG during midcooling hadmoderate to severe injury. Of the 13 infants with adiscontinuous EEG, again about one-quarter (23%)had moderate to severe injury, accounting for 2 infantswhose background was unchanged from the beginningof cooling and an additional infant whose initial back-ground was depressed and undifferentiated. By thistime period, all newborns (7/7, 100%) with BS or ex-tremely low voltage patterns had moderate to severe in-jury, with 3 having maximal MRI injury scores.
End of cooling. Moderate to severe MRI injury waspresent in 1 of the 12 infants (8%) whose back-ground was normal and 3 of the 16 infants (19%)whose background was excessively discontinuous,compared with all 5 (100%) whose backgroundshowed BS or extremely low voltage.
Postcooling. During this interval, the same new-born with a normal background (6%) and the same 3newborns with a discontinuous background (27%)had moderate to severe injury. All 6 infants with BS
Table 1 Clinical characteristics and MRI outcome
Moderate to severeMRI injury(n � 15)
No or mildMRI injury(n � 26) p Value
Gestational age, wk, mean � SD 39.4 � 1.5 39.1 � 1.4 0.4
Sex ratio, M:F 1:1.5 1:1 0.5
Birth weight, g, mean � SD 3,234 � 552 3,381 � 760 0.5
10-min Apgar, median (range) 4 (0–7) 5 (1–8) 0.07
Cord or blood gas pH, mean � SD 6.86 � 0.19 6.98 � 0.21 0.08
Inborn neonates, n (%) 0 (0) 4 (15) 0.09
Table 2 Evolution of EEG background with hypothermia by severity of MRI injurya
EEG background
Phase of therapeutic hypothermia
Beginning Mid End Post
None/mildinjury
Moderate/severeinjury
None/mildinjury
Moderate/severeinjury
None/mildinjury
Moderate/severeinjury
None/mildinjury
Moderate/severeinjury
Normal 8 (100) 0 14 (93) 1 (7) 11 (92) 1 (8) 15 (94) 1 (6)
Excessively discontinuous 11 (73) 4 (27) 10 (77) 3 (23) 13 (81) 3 (19) 8 (73) 3 (27)
Depressed andundifferentiated
2 (50) 2 (50) 2 (40) 3 (60) 2 (29) 5 (71) 2 (33) 4 (67)
Burst suppression 2 (29) 5 (71) 0 4 (100) 0 2 (100) 0 4 (100)
Extremely low voltage 3 (43) 4 (57) 0 3 (100) 0 3 (100) 0 2 (100)
a Values are n (%).
558 Neurology 76 February 8, 2011

or extremely low voltage patterns after rewarminghad moderate to severe injury.
Electrographic seizures and SE. Electrographic sei-zures were identified in 14 newborns (34%), 4 ofwhom had SE. Among the 14 newborns with sei-zures, 13 (93%) had seizure onset within the first 18hours of recording, 8 in the first 6 hours. One infanthad seizure onset during rewarming. Recurrent sei-zures were recorded during midcooling in 2 patientsand during rewarming in 3. Six of 14 patients (43%)never showed a clinical correlate during seizures, in-cluding 3 with subclinical SE. All 4 infants with SEhad BS or extremely low voltage patterns at the be-ginning of cooling and never recovered better thandepressed and undifferentiated at last time point.Isolated or recurrent seizures were more frequent inpatients with moderate to severe MRI injury com-pared with those with no or mild injury (53% vs23%, p � 0.05), and SE was only seen in newbornswith moderate to severe injury (p � 0.01).
Nonsurviving infants. Among the 5 nonsurviving in-fants, 4 had persistent BS or extremely low voltage
backgrounds throughout the duration of monitoringand maximal MRI injury, and goals of care were re-directed to comfort measures. One infant had an ex-cessively discontinuous background at the initiationof monitoring, depressed and undifferentiated bymidcooling, with less severe MRI injury. Goals ofcare were redirected due to persistent multisystemfailure.
DISCUSSION This study demonstrates that contin-uous video-EEG recording is an important diagnos-tic and prognostic tool in newborns with HIEundergoing TH. In our cohort, EEG backgroundwas associated with early MRI findings throughoutthe treatment period. A normal EEG was associatedwith no or mild MRI brain injury at all time points,although a normal background at the beginning ofcooling was even more predictive of a favorable MRIoutcome (100% specific) than at later time points(93% specific), as the EEG background of one new-born with moderate to severe MRI injury improvedfrom excessively discontinuous to normal over thefirst 24 hours of monitoring. In contrast, the prog-nostic value of a BS pattern or extremely low voltagebackground for moderate to severe injury increasedfrom the beginning of cooling (81% specific) to mid-cooling and thereafter (100% specific), reflecting 5newborns with these concerning patterns at the onsetof monitoring who rapidly improved by midcoolingand were spared from moderate to severe MRI in-jury. The greatest prognostic value of EEG back-ground in this population for predicting moderate tosevere MRI brain injury was not achieved until mid-cooling, highlighting the importance of continuousmonitoring or sequential EEGs in this population.
Our findings are substantiated by prior studies innoncooled infants with HIE, which demonstratedthat a normal EEG within the first 2–7 days of life is
Table 3 EEG background evolution, seizures and status epilepticus, andMRI outcomea
Moderate to severeMRI injury(n � 15)
No or mildMRI injury(n � 26) p Value
EEG background pattern, median (range)
Beginning of cooling 4 (2–5) 2 (1–5) 0.003
Midcooling 3.5 (1–5) 1 (1–3) 0.0000
End of cooling 3 (1–5) 2 (1–3) 0.0001
Postcooling 3 (1–5) 1 (1–3) 0.0000
Seizures, n (%) 8 (53) 6 (23) 0.05
Status epilepticus, n (%) 4 (27) 0 (0) 0.01
a EEG background scoring: 1 � normal; 2 � excessively discontinuous; 3 � depressed andundifferentiated; 4 � burst suppression; 5 � extremely low voltage.
Table 4 Sensitivity and specificity of EEG background during hypothermia for moderate to severe MRI injury
EEG background cutpointa
Phase of therapeutic hypothermia
Beginning Mid End Post
Sensitivity,%b
Specificity,%c
Sensitivity,%b
Specificity,%c
Sensitivity,%b
Specificity,%c
Sensitivity,%b
Specificity,%c
1 vs 2, 3, 4, 5 100 31 93 54 93 42 93 60
1, 2 vs 3, 4, 5 73 73 71 92 71 92 71 92
1, 2, 3 vs 4, 5 60 81 50 100 36 100 43 100
1, 2, 3, 4 vs 5 27 88 21 100 21 100 14 100
Area under receiveroperating characteristiccurve
0.77 0.88 0.86 0.89
a 1 � normal, 2 � excessively discontinuous, 3 � depressed/undifferentiated, 4 � burst suppression, 5 � extremely low voltage.b Sensitivity: Given moderate to severe injury, % identified as positive by EEG.c Specificity: Given no moderate to severe injury, % identified as negative by EEG.
Neurology 76 February 8, 2011 559

associated with favorable developmental outcomeand a severely abnormal EEG (BS or extremely lowvoltage) on the second day of life or thereafter is asso-ciated with poor outcome.12-14,24 The few studies thatreported EEG background in this population withinthe first 24 hours of life17,25,26 showed a relativelypoor specificity for adverse developmental outcomefollowing a severely abnormal background duringthe first 12 hours of life because of EEG normaliza-tion by 12 to 24 hours of life in some infants withnormal outcome. Similarly, in our cohort, a BS orextremely low voltage EEG was not highly predictivefor moderate to severe MRI injury until the secondday of life, around the time of midcooling. This find-ing is supported by a prior study evaluating EEGduring hypothermia in neonatal HIE by a singlesample recorded sometimes in the first 48 hours oflife, which found that a background of �5 �V wasassociated with death or major neurologic disabil-ity.15 Similarly, a recent study evaluating the prognos-tic value of amplitude-integrated EEG in newbornswith HIE exposed to normothermia compared to thosetreated with TH showed that a severely abnormal back-ground pattern in the hypothermia-treated group wasnot specific for abnormal developmental outcome until48 hours of life.27
Our findings differ from prior studies of non-cooled newborns with HIE in 2 main ways. First,prior studies have shown that a discontinuous EEGin the first several days of life is often associated withpoor outcome,28-31 whereas the majority of newbornsin our cohort (73%) with an excessively discontinu-ous pattern after rewarming had no or only mildMRI injury. While it is difficult to directly compareour study to prior studies given the differences inmethodology and the wide range of definitions ofdiscontinuous background in the literature, the out-come of newborns with an excessively discontinuousbackground appears to be different in newbornstreated with hypothermia. Interestingly, clinical en-cephalopathy on the fourth day of life following THhas also been shown to be less predictive of outcomein cooled infants compared to noncooled infants.8
Second, in comparison to the single study of contin-uous EEG monitoring in noncooled newborns withHIE which showed improvement of the backgroundpattern over the first 3 days of life in all newborns,17
the background worsened over the course of moni-toring in 13% of newborns in our cohort. Whetherthe EEG differences seen in our cohort of infantswith HIE and cooling are attributed to hypothermiaitself or the evolution of injury in this population isuncertain.
Electrographic seizures were present in 34% ofnewborns during TH, and continuous video-EEG
revealed that almost 50% of newborns with seizures,including 3 with SE, had seizures without clinicalcorrelate. Although experimental studies showed apotent effect of hypothermia in controlling sei-zures,32,33 a high incidence of seizures has been re-ported in children during TH.34 This discrepancymay be related to the earlier and deeper cooling usedin animal models.32,33 Most studies rely on clinicalevaluation for seizure diagnosis and classification ofseizure severity in newborns.35,36 However, it isknown that the majority of seizures, especially in crit-ically ill infants, do not have a clinical correlate andwill not be recognized without continuousEEG.16,37,38 Moreover, it is often impossible to accu-rately differentiate between seizure-related and non-seizure movements in infants using clinicalevaluation alone.39 While isolated or recurrent sei-zures were recorded in more than 50% of infantswith moderate to severe brain injury, not all wereassociated with moderate to severe brain injury. Incontrast, all newborns with SE had severely abnormalMRI. These results are in keeping with a recent worksuggesting that a significantly worse outcome occursin newborns with SE compared to newborns withrecurrent seizures.20
There are several limitations to our study. First,due to the referral pattern at our institution, new-borns did not start monitoring at the exact same timein the first day of life. However, in most of our pa-tients, monitoring was initiated within the first 12hours of life. Second, an excessively discontinuousbackground by our system encompassed a broadrange of interburst intervals. Therefore, it is not sur-prising that a discontinuous pattern was a relativelypoor predictor of MRI brain injury. Third, we usedMRI as a short-term outcome measure and do notyet know the long-term outcome in this cohort. Ithas been reported that hypothermia does not af-fect the prognostic value of MRI in newborns withHIE.11 However, long-term developmentalfollow-up of this cohort is needed to confirm ourresults. Finally, as many patients with poor EEGbackgrounds and moderate to severe brain injurywere treated with AEDs, we were unable to assesswhether depressed background activity was an effectof medication or due to underlying brain injury.
EEG monitoring in newborns is noninvasive,provides data from the entire cortex, and can be eas-ily performed at the bedside. Our findings under-score the importance of continuous EEG monitoringin this population to assist with seizure managementand discussions regarding prognosis and goals ofcare. Even in the setting of hypothermia, EEG re-mains a strong predictive tool, and its routine usealongside clinical evaluation and MRI is warranted.
560 Neurology 76 February 8, 2011

Establishing consensus on neonatal EEG nomencla-ture and classification will help future studies on theprognostic value of EEG during TH. Particularly,further analysis and revalidation of the excessivelydiscontinuous pattern in neonates being treated withHIE is warranted. Given emerging data suggestingthat seizures may be associated with increased braininjury following neonatal HIE,35,36,40 accurate seizuredetection is becoming an important issue in the con-text of neuroprotection. Future studies that evaluatewhether rapid and effective treatment of seizures willimprove neurologic outcome will rely on continuousEEG monitoring.
AUTHOR CONTRIBUTIONSStatistical analysis was conducted by Dr. H.C. Glass, Dr. S.L. Bonifacio,
and Dr. K.B. Nash.
ACKNOWLEDGMENTThe authors thank the neonatal research nurses of the Pediatric Clinical
Research Center at UCSF for their work on this study.
DISCLOSUREDr. Nash reports no disclosures. Dr. Bonifacio has received fellowship
support from the NIH. Dr. Glass has received research support from the
NIH. Dr. Sullivan has received research support from Pfizer Inc. and the
NIH. Dr. Barkovich serves on the editorial boards of the American Journal
of Neuroradiology, Neuroradiology, Brain and Development, and Neuropedi-
atrics; receives royalties from the publication of Pediatric Neuroimaging,
4th ed. (Lippincott Williams & Wilkins, 2005), Pediatric Neuroradiology
(Amirsys, 2008), and Neuroradiology, 2nd ed. (Amirsys, 2009); and re-
ceives research support from the NIH. Dr. Ferriero serves on a scientific
advisory board for the NIH/NINDS; serves as an Associate Editor for
Annals of Neurology and Pediatric Research; receives royalties from the pub-
lication of Principle and Practices of Pediatric Neurology (Elsevier, 2005);
and receives research support from the NIH. Dr. Cilio receives research
support from the European Commission.
Received June 7, 2010. Accepted in final form October 12, 2010.
REFERENCES1. Pierrat V, Haouari N, Liska A, Thomas D, Subtil D,
Truffert P. Prevalence, causes, and outcome at 2 years ofage of newborn encephalopathy: population based study.Arch Dis Child Fetal Neonatal Ed 2005;90:F257–F261.
2. Pin TW, Eldridge B, Galea MP. A review of developmen-tal outcomes of term infants with post-asphyxia neonatalencephalopathy. Eur J Paediatr Neurol 2009;13:224–234.
3. Shankaran S, Laptook AR, Ehrenkranz RA, et al. Whole-body hypothermia for neonates with hypoxic-ischemic en-cephalopathy. N Engl J Med 2005;353:1574–1584.
4. Azzopardi DV, Strohm B, Edwards AD, et al. Moderatehypothermia to treat perinatal asphyxial encephalopathy.N Engl J Med 2009;361:1349–1358.
5. Sarnat HB, Sarnat MS. Neonatal encephalopathy follow-ing fetal distress: a clinical and electroencephalographicstudy. Arch Neurol 1976;33:696–705.
6. Mercuri E, Guzzetta A, Haataja L, et al. Neonatal neurologi-cal examination in infants with hypoxic ischaemic encepha-lopathy: correlation with MRI findings. Neuropediatrics1999;30:83–89.
7. Miller SP, Latal B, Clark H, et al. Clinical signs predict
30-month neurodevelopmental outcome after neonatal en-
cephalopathy. Am J Obstet Gynecol 2004;190:93–99.
8. Gunn AJ, Wyatt JS, Whitelaw A, et al. Therapeutic hypo-
thermia changes the prognostic value of clinical evaluation
of neonatal encephalopathy. J Pediatr 2008;152:55–58.
9. Barnett A, Mercuri E, Rutherford M, et al. Neurological
and perceptual-motor outcome at 5–6 years of age in chil-
dren with neonatal encephalopathy: relationship with neo-
natal brain MRI. Neuropediatrics 2002;33:242–248.
10. Miller SP, Ramaswamy V, Michelson D, et al. Patterns of
brain injury in term neonatal encephalopathy. J Pediatr
2005;146:453–460.
11. Rutherford M, Ramenghi LA, Edwards AD, et al. Assess-
ment of brain tissue injury after moderate hypothermia in
neonates with hypoxic-ischaemic encephalopathy: a nested
substudy of a randomised controlled trial. Lancet Neurol
2010;9:39–45.
12. Monod N, Pajot N, Guidasci S. The neonatal EEG: statis-
tical studies and prognostic value in full-term and pre-term
babies. Electroencephalogr Clin Neurophysiol 1972;32:
529–544.
13. Watanabe K, Miyazaki S, Hara K, Hakamada S. Behav-
ioral state cycles, background EEGs and prognosis of new-
borns with perinatal hypoxia. Electroencephalogr Clin
Neurophysiol 1980;49:618–625.
14. Holmes G, Rowe J, Hafford J, Schmidt R, Testa M, Zim-
merman A. Prognostic value of the electroencephalogram
in neonatal asphyxia. Electroencephalogr Clin Neuro-
physiol 1982;53:60–72.
15. Mariani E, Scelsa B, Pogliani L, Introvini P, Lista G. Prog-
nostic value of electroencephalograms in asphyxiated new-
borns treated with hypothermia. Pediatr Neurol 2008;39:
317–324.
16. Murray DM, Ryan CA, Boylan GB, Fitzgerald AP, Con-
nolly S. Prediction of seizures in asphyxiated neonates: cor-
relation with continuous video-electroencephalographic
monitoring. Pediatrics 2006;118:41–46.
17. Murray DM, Boylan GB, Ryan CA, Connolly S. Early
EEG findings in hypoxic-ischemic encephalopathy predict
outcome at 2 years. Pediatrics 2009;124:e459–e467.
18. Clancy RR, Legido A. The exact ictal and interictal dura-
tion of electroencephalographic neonatal seizures. Epilep-
sia 1987;28:537–541.
19. Scher MS, Hamid MY, Steppe DA, Beggarly ME, Painter
MJ. Ictal and interictal electrographic seizure durations in
preterm and term neonates. Epilepsia 1993;34:284–288.
20. Pisani F, Cerminara C, Fusco C, Sisti L. Neonatal status
epilepticus vs recurrent neonatal seizures: clinical findings
and outcome. Neurology 2007;69:2177–2185.
21. Holmes GL, Lombroso CT. Prognostic value of back-
ground patterns in the neonatal EEG. J Clin Neurophysiol
1993;10:323–352.
22. Lamblin MD, Andre M, Challamel MJ, et al. Electroen-
cephalographie du nouveau-ne premature et a terme: as-
pects maturatifs et glossaire. Neurophysiol Clin 1999;29:
123–219.
23. Barkovich AJ, Hajnal BL, Vigneron D, et al. Prediction of
neuromotor outcome in perinatal asphyxia: evaluation of MR
scoring systems. AJNR Am J Neuroradiol 1998;19:143–149.
24. Selton D, Andre M. Prognosis of hypoxic-ischaemic enceph-
alopathy in full-term newborns–value of neonatal electroen-
cephalography. Neuropediatrics 1997;28:276–280.
Neurology 76 February 8, 2011 561

25. Pezzani C, Radvanyi-Bouvet MF, Relier JP, Monod N.Neonatal electroencephalography during the first twenty-four hours of life in full-term newborn infants. Neuropedi-atrics 1986;17:11–18.
26. Pressler RM, Boylan GB, Morton M, Binnie CD, RennieJM. Early serial EEG in hypoxic ischaemic encephalopa-thy. Clin Neurophysiol 2001;112:31–37.
27. Thoresen M, Hellstrom-Westas L, Liu X, de Vries LS. Effectof hypothermia on amplitude-integrated electroencephalogramin infants with asphyxia. Pediatrics 2010;126:131–139.
28. Biagioni E, Mercuri E, Rutherford M, et al. Combined useof electroencephalogram and magnetic resonance imagingin full-term neonates with acute encephalopathy. Pediat-rics 2001;107:461–468.
29. Wertheim D, Mercuri E, Faundez JC, Rutherford M, Aco-let D, Dubowitz L. Prognostic value of continuous electro-encephalographic recording in full term infants withhypoxic ischaemic encephalopathy. Arch Dis Child 1994;71:F97–F102.
30. van Lieshout HB, Jacobs JW, Rotteveel JJ, Geven W, v’tHof M. The prognostic value of the EEG in asphyxiatednewborns. Acta Neurol Scand 1995;91:203–207.
31. Menache CC, Bourgeois BF, Volpe JJ. Prognostic value ofneonatal discontinuous EEG. Pediatr Neurol 2002;27:93–101.
32. Liu Z, Gatt A, Mikati M, Holmes GL. Effect of tempera-ture on kainic acid seizures. Brain Res 1993;631:51–58.
33. Schmitt FC, Buchheim K, Meierkord H, Holtkamp M.Anticonvulsant properties of hypothermia in experimentalstatus epilepticus. Neurobiol Dis 2006;23:689–696.
34. Abend NS, Topjian A, Ichord R, et al. Electroencephalo-graphic monitoring during hypothermia after pediatriccardiac arrest. Neurology 2009;72:1931–1940.
35. Glass HC, Glidden D, Jeremy RJ, Barkovich AJ, FerrieroDM, Miller SP. Clinical neonatal seizures are indepen-dently associated with outcome in infants at risk forhypoxic-ischemic brain injury. J Pediatr 2009;155:318–323.
36. Miller SP, Weiss J, Barnwell A, et al. Seizure-associatedbrain injury in term newborns with perinatal asphyxia.Neurology 2002;58:542–548.
37. Murray DM, Boylan GB, Ryan CA, Connolly S. Earlycontinuous video-EEG in acute near-total intrauterine as-phyxia. Pediatr Neurol 2006;35:52–56.
38. Clancy RR, Legido D, Lewis D. Occult neonatal seizures.Epilepsia 1988;29:256–261.
39. Malone A, Ryan CA, Fitzgerald A, Burgoyne L, ConnollyS, Boylan GB. Interobserver agreement in neonatal seizureidentification. Epilepsia 2009;50:2097–2101.
40. Bjorkman ST, Miller SM, Rose SE, Burke C, Colditz PB.Seizures are associated with brain injury severity in a neo-natal model of hypoxia-ischemia. Neuroscience 2010;166:157–167.
Neurology® Launches Subspecialty Alerts by E-mail!Customize your online journal experience by signing up for e-mail alerts related to your subspecialtyor area of interest. Access this free service by visiting http://www.neurology.org/cgi/alerts/etoc.xhtml or click on the “E-mail Alerts” link on the home page. An extensive list of subspecialties,methods, and study design choices will be available for you to choose from—allowing you priorityalerts to cutting-edge research in your field!
562 Neurology 76 February 8, 2011