Embed Size (px)
Citation preview
Physiotherapy Programmes (BSc Hons and MSc Pre-registration)
1 | P a g e
MMU
2011- 2012
Practice Educator’s Handbook 2011-2012 Physiotherapy ProgrammesFaculty of Health, Psychology and Social CareDepartment of Health Professions
Physiotherapy Programmes (BSc Hons and MSc Pre-registration)
Content Page Number
Telephone Numbers and contacts 4-5
University Background Information 6-8
Programme Design and Organisation 9-13
Practice Education 14-15
Accreditation of Clinical Placement 16-17
Organisation of Clinical Placements 18-19
Practice Placements BSc (Hons) and MSc Pre Registration Programmes
19-22
Monitoring and evaluation of placements 22-29
Complaints Procedure 30-31
Health and Safety 32-34
Procedures for Sickness Reporting 35-38
Procedure for supporting disabled students on practice placement
39-40
Professional Dress 41-42
Development of Clinical Practice 43
Role of the Student 43-44
Role of the Practice Educator 44-45
Role of the Visiting Lecturer 45
Learning from Practice 46-47
Assessment of Clinical Practice 47-48
Appendix I Clinical Observation Documentation
49-54
Appendix II Practice Education Record Book
55-75
2 | P a g e

Physiotherapy Programmes (BSc Hons and MSc Pre-registration)
Appendix III BSc Common Assessment Tool (Level 5)
76-112
Appendix IV MSc Common Assessment Tool (Level 6)
113-148
Appendix V Elective Placement Documentation
149-164
Appendix VII Case Review Guidance 165-167
Appendix VIII Assignment specification BSc practice placement 4
168-178
Appendix IX Assignment specification BSc practice placement 5
179-190
Appendix 10 Practice placement proforma
191-192
Appendix 11 New placement proforma 193
Appendix 12 MSc pre registration units and structure
194-210
Addendum 1 2009-2012 cohort course Structure BSc (Hons)
Addendum 2 2010-1013 course structure
BSc (Hons)Addendum 3 2011-2014 course structure
BSc (Hons)
3 | P a g e

Physiotherapy Programmes (BSc Hons and MSc Pre-registration)
Telephone Numbers / ContactsGeneral Enquiries via
Louise Taylor 0161 247 2457Placements Administrator Fax: 0161 247 6571Email: [email protected]
Clinical Education Team
Sophie Taylor 0161 247 2930Senior LecturerBSc (Hons) Practice Placement Co-ordinatorEmail: [email protected]
Jo Nicholson 0161 247 3057Senior LecturerBSc (Hons) Practice Placement [email protected]
Jackie Hindle 0161 247 3055Senior LecturerMSc Pre-registration Practice Placement Coordinator Email: [email protected]
Deborah O’Connor 0161 247 2598Senior LecturerEmail: [email protected]
Rachel Stockley 0161 247 2971Senior LecturerEmail: [email protected]
4 | P a g e

Physiotherapy Programmes (BSc Hons and MSc Pre-registration)
Visiting tutors
Jo Ashman 0161 247 2928
Jill Bailey 0161 247 3556
Jenny Caunt 0161 247 2967
Jenny Crampton 0161 247 2939
Daphne Dawson 0161 247 2919
Glenis Donaldson 0161 247 2908
Lynley Eason 0161 247 2579
Francis Fatoye 0161 247 2963
Peter Goodwin 0161 247 2941
Suzanne Gough 0161 247 2942
Claire Hamshire 0161 247 2940
Sally Hartley 0161 247 2946
Sandra Hartley 0161 247 2901
Kathryn Heathcote 0161 247 3056
Joyce Hughes 0161 247 2883
Kay Hurst 0161 247 2028
Ruth MacDonald 0161 247 2024
Lesley McLoughlin 0161 247 2956
Smarak Mishra 0161 247 2902
Janet Morrison 0161 247 2928
Jo Nicholson 0161 247 3057
Narayan Prabhu 0161 247 2954
Janet Rooney 0161 247 3575
Rajiv Sighamoney 0161 247 2916
Rachel Spearing 0161 247 2881
Sophie Taylor 0161 247 2930
Julie Wright 0161 247 2953
Gill Yeowell 0161 247 2961
Abebaw Yohannes 0161 247 2943
5 | P a g e
Physiotherapy Programmes (BSc Hons and MSc Pre-registration)
6 | P a g e

Manchester Metropolitan University
The Manchester Metropolitan University
The UniversityThe Manchester Metropolitan University was established in 1992 when the then Manchester Polytechnic was granted University status. Established in 1970, Manchester Polytechnic was formed from the Manchester College of Art and Design, the Manchester College of Commerce and the John Dalton College of Technology. In 1977 it was enlarged by mergers with Didsbury College of Education and Hollings College. In 1983 it incorporated the former City of Manchester College of Higher Education. In 1992 it further incorporated Crewe and Alsager College of Higher Education which was re-branded as MMU Cheshire in 2003.
The University occupies five sites in Manchester and two at Crewe and Alsager in Cheshire. It is presently organised into seven faculties:Faculty of Art and DesignBusiness SchoolFaculty of Health, Psychology and Social CareFaculty of Food, Clothing and Hospitality ManagementFaculty of Humanities, Law and Social ScienceFaculty of Science and EngineeringMMU Cheshire
In the current session, the University has over 30,000 students attending some 400 programmes in approximately 50 different subject areas. Its central campus stands to the South of Manchester’s City Centre alongside The Victoria University of Manchester, Manchester Business School, UMIST and the Royal Northern College of Music. This complex makes up the largest University campus in Western Europe. There are a further four campus locations situated in other parts of the City, together with a campus at Crewe and one at Alsager - both of which are in Cheshire.
The University employs approximately 3,500 staff, comprising almost 1,100 full-time teaching staff, 600 part-time teaching staff, 700 manual staff and 1,048 administrative, professional, clerical and technical staff.
The Vice-Chancellor of the University is Professor John Brooks. Reporting to him are twelve Directorate members. Seven of these are Deans of Faculty and five are responsible for support functions, comprising a Deputy Vice-Chancellor, an External Relations Director, a Financial Director, a Human Resources Director, and a Services Director.
The University has a Board of Governors of twenty one members made up of well known senior executives and regional figures, together with elected members from the academics and non-academic staff and the student body. The Board of Governors is responsible for broad policy and the Vice-Chancellor discharges responsibility for its implementation and for the organisation, direction and management of the University.
7 | P a g e

Manchester Metropolitan University
The Faculty of Health, Psychology and Social CareThe Faculty of Health, Psychology and Social Care consists of a School of Health, Psychology and Social Care. It is one of the largest faculties within MMU offering a broad spectrum of undergraduate, postgraduate and professional programmes which prepare students for their future professional lives. These programmes span a range of academic disciplines within the caring and enabling professions, including physiotherapy, speech and language therapy, psychology, nursing, social work and other health related subjects.
The Faculty operates on 2 campuses. Health related and psychology programmes are based at the Elizabeth Gaskell campus and Social Care is located at Didsbury campus.
The Faculty administration and the Dean are located at on the Elizabeth Gaskell site. Full library, computing support and audio-visual support is available on all sites, as are other student amenities.
Although the disciplines within the Faculty cover a wide spectrum, they are linked by an ethos of participation in community services. All programmes place emphasis on the applied nature of the subject. The aim of the Faculty is to enable students to achieve their ambition by helping them to develop the knowledge, skills and values that will ensure their eligibility for professional registration and practice or to secure employment in related fields or access to other undergraduate/postgraduate professional education programmes, thus placing them on the first step of their professional career. A key feature of the Faculty’s philosophy is the recognition of the dynamic interface between theory and practice and the value of learning from sustained experience in practice settings.
Physiotherapy constitutes a programme area in the Department of Health Professions a part of the Faculty of Health, Psychology and Social Care. Originally the Physiotherapy Programme area was called the Department of Physiotherapy which joined the University on 01 September 2003, having previously been part of the Central Manchester and Manchester Children’s University Hospitals NHS Trust.
This Programme area is one of the largest and most successful of the UK providers of undergraduate and postgraduate physiotherapy education. It runs a range of programmes, including a three year undergraduate degree, the BSc (Hons) Physiotherapy and a two year MSc Physiotherapy (Pre-registration), which confer eligibility to apply for registration with the Health Professions Council, and membership of the Chartered Society of Physiotherapy. In addition, the Continuing Professional Development and Postgraduate Studies Division offers two other Masters programmes; the MSc Physiotherapy (Post-registration) and the MSc Manual Therapy (Post-registration).
The quality of the educational programmes is overseen by a number of external agencies, including the Quality Assurance Agency, the professional body (the Chartered Society of Physiotherapy) and the statutory body (the Health Professions Council).
8 | P a g e

Manchester Metropolitan University
The NHS Northwest (Strategic Health Authority) has a contract with the University for educational provision approved by the HPC and CSP which thus confers eligibility to apply for registration on the HPC and membership of CSP. It is the body which pays for the NHS bursary places for students.
9 | P a g e

Programme Design and Organisation
Programme Design and Organisation
Programme Philosophy
Physiotherapy is a changing and evolving profession which encompasses the concepts of health promotion and prophylaxis, the restoration of function and the achievement of optimal rehabilitation.
The physiotherapist works within complex environments ranging from the community, industry, schools, hospitals and private practice. This work takes place against a climate of changing health needs and health care provision.
The ultimate goal of physiotherapy education is to produce a competent practitioner with skills which will enable him/her to go on learning and developing throughout their professional career.
A competent practitioner is someone who is able to demonstrate that they have reached the required level of ability which encompasses three main areas:
the award of either an MSc Physiotherapy (Pre-registration) or BSc (Hons) which fulfils the academic and professional requirements of the University, the HPC and the CSP.
the possession of a range and level of skills which enable them to carry out evaluative clinical practice appropriate to current health care needs.
the flexibility and capability to respond to changing health and service needs in the current clinical climate, this being one of the requirements of the service commissioners.
The skills required to achieve this include the ability to critically analyse and evaluate his/her own practice and to adopt a research approach to current and future physiotherapy practice.
Programme Structure
MSc Pre-registrationThe Programme is a two year qualifying Masters Degree with a license to practise for candidates with first degrees in subjects other than Physiotherapy. Having been educated to degree level, students will be expected to have developed the ability to recognise and address their own learning needs, and have pre-learned core intellectual skills, such as problem solving, critical thinking and research skills, and co-operative and independent learning skills. An accelerated programme of study allows such candidates to work academically at Masters Level, whilst attaining the skills and knowledge necessary to fulfil the standards set by professional and statutory bodies. Such entrants to the profession are expected to become confident
10 | P a g e

Programme Design and Organisation
to challenge practices, and through research, initiate change where appropriate, thus contributing to the development of the profession (CSP, 2003).
BSc(Hons) The BSc (Hons) Physiotherapy programme is provided on a full time basis over a period of three academic years. The structure, content and sequencing of the units including practice placements were designed to ensure that the student was able to acquire and develop the graduate skills, underpinning professional knowledge and practical skills that are a requirement of the university and the professional and statutory bodies.
Programme DeliveryIn order to achieve the aims of the programmes, a number of different teaching and learning strategies will be used. Programme delivery will incorporate student centred learning and a problem solving case-based approach. The selection of the different methods will be determined by various factors such as the aims of the session, the content of the session, the stage that the students are at within the programmes and the fact that within any group of students there will be a variety of preferred learning styles.
Teaching and Learning StrategiesThroughout the programmes there will be a strong emphasis on learning through reflection. Students will be encouraged to reflect on their experiences through the use of reflective logs/diaries and reflective writing assignments. These skills will also be used in the development of a Professional Development Portfolio.Evidence based practice (EBP) will be integrated throughout the units and students will be encouraged to explore and analyse how EBP underpins practice.
Lead lecturesLead lectures will normally be delivered to the whole cohort. They will be used for a variety of purposes:
To introduce major/new topics To summarise topics. As an information resource. To challenge thinking.
Workbooks, directed and self directed studyStudy may be facilitated with the use of workbooks and self-study packages, or by the students being set a specific study task or problem to explore. The specific nature of study tasks may be discussed and defined with facilitation from a member of teaching staff, for example in a tutorial. It is, however anticipated that early in the programmes, students will be expected to generate their own study objectives, with reference to the appropriate learning outcomes; students will also be expected to read widely around the subject areas covered.
TutorialsStudents will participate in small group tutorials, where they will normally be required to have completed some independent or directed study prior to the session and then
11 | P a g e

Programme Design and Organisation
use the information in a different way to meet the specific session learning outcomes. The use of a problem-solving, case based approach will promote clinical reasoning.
Practical skills sessionsAs a reflection of the learning outcomes there will be a large number of practical skills sessions. These will normally involve demonstration of skills by the tutor followed by opportunities for supervised practice of the skill with plentiful formative feedback.Underpinning knowledge and problem solving clinical reasoning activities will also be included in these sessions. With facilitation, students will be encouraged to peer assess each other’s performances.
WorkshopsWorkshops will be used for a variety of purposes:
As a terminal activity in a unit to review and integrate a cross section of aspects of the unit.
To provide a structured opportunity to cover a range of practical or theoretical components, promoting clinical reasoning and often involving input from other disciplines.
As a formative assessment opportunity prior to undertaking summative assessment components.
Case Based/Problem Based LearningCase based learning offers an opportunity for students to contextualise their knowledge and understanding and promotes clinical reasoning. The use of clinical cases will be central to each unit and provide the focus for learning about specific pathologies/conditions as well as related psycho-social issues. Cases will be developed and updated with the support of practitioners to ensure these core components reflect current practice. In some units the cases will be used to support a problem based approach and in others they will be used to draw together learning from the unit.
Shared LearningShared learning may be used to bring together students from different professional groups to achieve common learning outcomes for example in communication skills, or in exploring legal, moral and ethical issues. It will also be used to enable students from a variety of professions to share approaches to the management of patients with particular clinical problems for example, following Stroke.
Reflective logs and diariesLearning logs will be used to enable students to record their own learning experiences. These logs will ensure that all students have records that they can utilise to engage in reflection activity. Students will produce examples of reflective writing throughout the programme that will be used to compile a Professional Development Portfolio. The nature of reflective writing, particularly when related to clinical experiences, promotes critical practice and clinical reasoning.
12 | P a g e

Programme Design and Organisation
Project workWill be used to promote team working skills, independent study skills and clinical reasoning. Small projects will also be undertaken as part of the delivery of the curriculum. These will provide opportunities for formative feedback.
PresentationsPresentations will be used throughout the programme. They will usually be linked to directed study periods and incorporated into tutorials, practical skills or workshop situations. Students will be expected to present (in groups or individually) information to their peers. Peer assessment opportunities will arise from these activities and the use of presentations in the programme will allow communication skills to be developed, enhanced and refined thereby supporting the development of key skills.
Distance learning/ e-learningDistance learning / e-learning materials using WebCT will be used to allow flexibility in delivery of the programme therefore supporting the needs of the diverse student population. The flexibility offered by e-learning means that students are not constrained in their learning by time and place. E-learning also encourages active, self-directed learning and peer support through a virtual community.
Practice Based LearningPractice based learning will be central to the programme delivery. Students will normally spend at least 1,000 hours in clinical practice during the programmes. Practice placements are skills based to facilitate the transfer of skills across clinical areas. The skills will be related to those covered in the preceding units. The range of practice settings/placements covered will offer students the opportunity to meet the learning outcomes. Application of skills and knowledge in a range of practice environments demands clinical reasoning.
Placements will be supported by practice based clinical staff and visiting academic staff. These will provide unique learning opportunities and will be arranged to reflect current practice. Progression of learning across placements will be demonstrated by the increasing complexity and unpredictability of students’ caseloads.
Case Reviews
In the second year of the MSc pre-registration programme, students have to complete a project based on a case review. Students will be required to carry out a case review in all of the first three Practice Placements. The case review will then form the basis of an oral presentation plus a written project of 16,000 words, which may be:
An extended research proposal A reliability / validity study of outcome measures used in the case review, or A critical literature review of outcome measures or interventions referred to in
the case review.
A detailed specification for the Case Review can be found in appendices
13 | P a g e
Programme Design and Organisation
Both Pre Registration Physiotherapy Programmes and proformas that identify the learning outcomes for each section of the programme.
14 | P a g e

Practice Education
Practice Education
Philosophy
The ultimate goal of physiotherapy education is the development of a competent practitioner complete with skills which will enable him/her to continue learning and developing throughout their professional career.
Students are introduced early in the programmes to theories of learning and are aware of concepts of learning styles. They are encouraged to apply these in their own personal development throughout the programmes.
A competent practitioner is one who is able to adapt physiotherapy skills to meet the needs of patients in a variety of settings. The challenge to the student during clinical education is the development of this adaptability in the management of patients each with unique problems. Experiential learning is facilitated by clinical practice which provides the concrete experience and allows for reflection to deepen understanding. The testing of hypotheses developed leads the student into the ascending spiral of learning through reflective practice.
Clinical practice
Development of hypotheses Reflection and understanding
Testing of hypotheses(Adapted from Kolb (1984))
The elements of professional practice include knowledge, skills and professional attitudes. It is important that students possess a sound knowledge base upon which they may reflect their new experiences in developing physiotherapy practice. This will include basic sciences and interpersonal skills. The integrated units of both programmes will equip the student with the necessary knowledge base and skills prior to clinical practice. The ability to perform psychomotor skills and interact with others in a clinical environment will consolidate learning which took place in an academic setting. Clinical education is acknowledged as a vital element of both programmes leading to successful qualification as a physiotherapy practitioner.
15
Previous knowledge
Tutorials

Practice Education
Support for CliniciansBoth physiotherapy programmes recognise the contribution and commitment made by clinicians to the Physiotherapists of the future. Without the highly valued resource that Practice Educators provide, our students would not gain the valuable clinical experience that they require. We seek to inform and support our Clinicians in several ways:
Practice Educators CourseThe Department of Health Professions hosts two Practice Educators’ courses per year. Each course is four days in total, spread over a period of 6 months.
Issues addressed during the course include theories of learning, expectations of clinicians and students, placement planning, facilitation of learning, teaching skills, assessment and educational issues that may help clinicians to plan, implement and evaluate periods of clinical education for undergraduate physiotherapists.
The course can form part of the ‘Health Professional as an Educator’ unit of the MSc Physiotherapy (Post-registration) awarded by the Manchester Metropolitan University.
On-Site Support / Update Practice Educators CourseThe Department of Health Professions undertake to provide support for clinicians at their place of work in two ways:
(1) The role of the Visiting Lecturer includes discussion with the Practice Educator. This time can be spent in identifying training needs for the educator and incorporating such needs in its planning for future courses.
(2) The Practice Placement Co-ordinators and members of the programme teams visit placement sites upon request, both to deliver new and relevant information and to discuss problems and needs.
An update (one day) Practice Educators’ course can be delivered on site for a group of experienced Practice Educators as requested.
The LibraryThe library is available for reference for all our Practice Educators. Unfortunately, resources will not usually allow for loans but we would encourage our colleagues to share our facilities.
16 | P a g e

Practice Education
Accreditation of Clinical PlacementsNew initiatives in the Government White Paper, “The new NHS Modern, Dependable” provide a renewed focus for consideration of quality in the delivery of Health Care Services. A Joint initiative by Manchester Metropolitan University, the University of Salford and the University of Liverpool, has endeavoured to translate the same principles to pertain to the provision of clinical education to physiotherapy undergraduates. This has led to the development of a system of accreditation in the North West. Standards have been developed based on those generated by the CSP, by a working group consisting of service managers and clinical physiotherapy lecturers. Evidence of achievement of these standards is to be contained within a portfolio. (This evidence could also prove to be useful for the Continuous Professional Development diaries). Our scheme is a recognised route for the CSP ACE Award. Anyone who wishes to pursue this option can contact any of the clinical education team.
The steps needed to be taken to achieve accreditation can be seen in the flow chart on the following page.
17 | P a g e

Practice Education
THE ACCREDITATION PROCESSClinician notifies manager that they would like to become involved in the
accreditation process. (This could be identified during appraisal).
The manager informs practice placement co-ordinator at one of the three education providers.
The education provider sends out an accreditation pack with a named mentor.
Existing standards already being achieved are identified by both parties.
Existing documentation, policies, and information that can be used as evidence are identified.
Assistance and support needed are negotiated.
Plan of action identified to provide evidence.
Representatives from the education providers and another accredited service will meet to evaluate the portfolio.
Accredited status awarded Action plan with review date if all standards are not met
Accreditation
18 | P a g e

Practice Education
Organisation of Clinical Practice
Approval of Practice Placements
Approval of a new placement site
1. Preliminary communication between Practice Placement Co-ordinators and placement provider is made to ascertain feasibility.
2. Placement visit is arranged if placements are judged to be feasible from the discussion.
3. Facilities are viewed and learning opportunities/ learning resources discussed with manager and clinicians.
4. Roles and responsibilities are discussed e.g. placement provider, Practice Educators, students, visiting academic staff.
5. Provider completes Placement Profile Proforma (see appendices)6. Placement staff are identified as Practice Educators and if they have not
completed a Practice Educators course within the last three years, attendance on the next course is arranged.
7. Practice Placement Co-ordinators make professional judgement regarding approval of the placement site based on:
a. quality of learning opportunities;b. evidence that the organisation fulfils their responsibilities under health
and safety legislation in the workplace (complete MMU Health and Safety proforma);
c. evidence of an Equal Opportunities Policy for the organisation (complete MMU Equal Opportunity proforma);
d. their ability to support students on placement.8. If the placement fails to comply with the above, the placement will be deemed
unsuitable until the placement reaches an adequate standard and satisfies points 7a – 7d as above.
9. If the placement is approved, placement site receives copy(ies) of Practice Educators Handbook.
10.Placement profile is added to Master file which is housed in Elizabeth Gaskell Library and available online via the MMU website.
Approval of a new placement in an existing approved site
1. Initial discussion is made with manager or Practice Educator from placement site.
2. Discussion takes place regarding learning opportunities for that particular placement.
3. Practice staff are identified for training if required and attendance on the next course is arranged.
4. Practice Placement Co-ordinators make a professional judgement regarding approval of placement.
5. Placement Profile is amended to include the placement.
19 | P a g e

Practice Education
Preparation of Students for Practice Placements Placement preparation sessions are incorporated throughout the first year,
prior to practice placement. Debrief and planning sessions occur after placements once the students are
back in the university. Student Practice Education Handbook. Placement Profiles
Preparation of Practice Educators / Practice Placements Four day Multiprofessional Practice Educator Course (taught) A Multi-professional WebCT course (on line) One day Update (advanced) Practice Educator Course One to one sessions with Practice Educators by arrangement Group sessions with Practice Educators by arrangement Practice Educators Handbook ACE Accreditation Process for Practice Educators Production of Placement Profiles (in line with CSP guidelines and QAA bench
marks)
Preparation of Academic Staff to Visit Practice Placements Induction of new academic staff into the role of Visiting Lecturer (including
shadowing visits) Staff development sessions for academic staff Academic staff attend Practice Educators Course
Practice Placement Co-ordinators (MMU Academic staff) Members of CSP National Network of Clinical Education Co-ordinators Members of NW Clinical Education Co-ordinators Forum Members of NW Physiotherapy Accreditation Consortia Liaison with practice placement co-ordinators of pre-qualifying programmes
within the Faculty Liaison with Principal Lecturer- Practice Placement and Learning for guidance
and support on strategic development.
All the above occurs in reference to external benchmarks/standards (e.g. CSP, HPC and QAA). Additionally, all placements are governed internally by the Universities Institutional Code of Practice for Practice Placement learning, which can be accessed via the following link:http://www.mmu.ac.uk/academic/asu/Academic_Policies_Regulations_&_ICPs/Placement_and_Work-based_Learning_ICP.pdf
Practice PlacementsMSc Pre-registration:The student will be introduced to the clinical environment via 5 days of participant observation with a Physiotherapist at the end of the first term.
20 | P a g e

Practice Education
Practice placements commence in the third term of the MSc Pre-registration programme and are sequenced throughout the rest of the first and second years. Placements 1 to 5 will be assessed using the Common Assessment Tool. For students on the MSc Physiotherapy (Pre-registration) programme, all practice placements will be assessed at Level 6. However the marking criteria will only be used to ascertain that the student has achieved a satisfactory level of performance and whilst completion of the document will give students valuable formative feedback, a numerical value will not be associated with this and the placement outcome will be described as PASS / FAIL.
BSc (Hons):The student will be introduced to the clinical environment via 4 days of participant observation with a Physiotherapist at the end of the first year. Students arrange this participant observation placement themselves.Practice placements commence in the second year of the programme and are sequenced throughout the rest of the programme. Placements 1 to 5 will be assessed using the Common Assessment Tool (CAT) and will be expected to meet the criteria for level 5 for placements 1 to 3 and level 6 for placements 4 and 5.
Students will spend 5 week blocks of time on a work based experience placement. The placement philosophy is that of flexibility within a structure which reflects current physiotherapy service provision. The placements are skills based, to encourage the transfer of skills across the placements. When allocating student placements, the Practice Placement coordinators aim to give the students a wide range of experiences. Consideration is given to the location of the placement, for example whether the placement is hospital or community based; whether the placement is acute or rehabilitation, the age of the patients (children or the elderly); together with the specific skills that the student is likely to experience. Traditionally, the placements were divided into 4 different categories by speciality, however, the placement team now recognise that our students need to develop skills in core clinical areas but also within a range of placement settings.
Clinical Environment Clinical Speciality ExamplesAcute Respiratory
Neurology
Elderly
MSK
Acute stroke Unit
ITU
In-patient orthopaedics
Medical Admissions unit
Rehabilitation Respiratory
Neurology
Elderly
MSK
Intermediate care
Spinal Injuries unit
Elderly rehab
Community Respiratory
Neurology
Paediatric schools
Learning disabilities
21 | P a g e

Practice Education
Elderly
MSK
GP surgeries
Community neuro rehab
Rapid response team
A student will complete a total of 5 of these, 2 being musculoskeletal. The student will also complete an elective placement (see Appendix IV) of normally 4 weeks duration following successful completion of the 5 placements.
In order that all students complete the required range of placements, there will be differences in the sequence in which they gain their experience. Students are encouraged to keep a record of experience gained as they progress through the placements.
Reflective practice is facilitated by the provision of Professional Development Diaries, learning development plans, debriefing tutorials, Practice Education Record Book, self-evaluation and reflective logs / diaries. (See Appendix II for Practice Education Record Book).
It is vital that we have sufficient information about each placement setting to allow the clinical education team to allocate placements that represent the diversity of clinical skills and environments reflective of modern health service delivery.
Clinical HoursAll clinical placements are compulsory in order to satisfy the requirements of the programme and also to satisfy the required number of hours as recommended by the Chartered Society of Physiotherapy. The weekly hours vary dependent on the physiotherapy programme:
MSc Pre-registration:A minimum of 37 clinical hours per week and a maximum of 37.5 hours per week
BSc Hons:A minimum of 36 hours per week and a maximum of 37.5 hours per week
This will enable students to complete the 1000 hours of clinical practice required, in order to complete the course and to be able to apply to the HPC for registration . This not only includes patient contact hours, but also time for ward rounds, case conferences, team briefing meetings and in-service training sessions. This does not include study time in the evenings.
Practice Educators are responsible for recording the number of hours the student has completed on the final page of the Common Assessment Tool (Appendix III).
22 | P a g e

Practice Education
It is the policy of the programme team to cap clinical hours credited to the student for each practice placement. The cap is calculated by considering the number of hours possible should a student's attendance match that of a clinical colleague on a contract that requires them to work a maximum 37.5 hour working week. The maximum number of hours that can be credited for a normal 5 week placement is 187.5. This amount may decrease if a placement includes a Statutory Holiday.The programme team cannot sanction claims for clinical hours completed if it is implicit in the number of hours claimed that the student has worked without a break.The programme team cannot sanction claims for clinical hours that exceed 37.5 in any one week without prior negotiation with the practice placement coordinators.Students may not claim hours that are spent in preparation for practice placement outside the normal working day as clinical hours.
Learning Outcomes for Practice PlacementsOn completion of all the clinical placements the student will be at a satisfactory level of competence to practice physiotherapy.
See Practice Placement Proformas for more detail of learning outcomes.
Each Practice Educator is encouraged to discuss the objectives of their placement with each student. In addition, the Practice Educator and student must negotiate a learning development plan for each individual student. This highlights the student’s personal learning objectives.
Learning Outcomes for each clinical placement are given to students via their Programme and Year Handbooks.
Monitoring and Evaluation of PlacementsThe process used to monitor and evaluate practice placements is documented in the subsequent section. All evaluation forms are located at the end of the CAT booklet and should be completed by all parties concerned at the end of the clinical placement. All evaluations should be returned with the CAT booklet in order to maintain quality assurance.
23 | P a g e

Practice Education
Processes for Evaluation of Practice Placements.
24 | P a g e
Practice placements
Student evaluation of Practice Educator
Annual quality data sent to all placement
sites
Staff student forum
Practice Placement Forum
Feedback & appropriate action
Student evaluation of Visiting Lecturer
Practice Educator evaluation of Visiting Lecturer
Visiting Lecturer evaluation of Practice Educator
Communication with practice education co-
ordinators, Visiting Lecturers and Practice
Placement Team
Practice Education
Management and Quality Monitoring in Practice Education.
25 | P a g e
Department Management Team
Programme Management Team
Practice Education Co-ordinators& Practice Education Team
Pre-registration Programme Teams
Practice Placement Forum(Clinical managers & academic staff)
Students (directly)
Staff/student forum(including clinicians)
Practice Educators
Personal Tutors
Post placement debrief sessions (formal evaluations)
Principal Lecturer for placement
learning
Faculty Executive Group

Practice Education
Placement No: Clinical Debrief – Student Evaluation of Practice EducatorName of Practice Educator:Type of PlacementHospital/Unit/TrustPlacement dates From: To:
Yes No CommentsWere you made to feel part of the team?
Were you provided with a variety of learning experiences?
Did you feel able to ask questions and seek clarification?
Did you feel able to acknowledge your own weaknesses?
Were you given the opportunity to discuss or work with other disciplines?
Was you practice educator willing to demonstrate/teach/observe?
Was your practice educator willing to negotiate your L.D.P.?
Were you given regular constructive feedback?
Were you given adequate recommendations and guidance during you mid-term assessment?
26 | P a g e

Practice Education
Did you receive sufficient preparatory information prior to your placement?Did the practice educator understand how your placement related to the broader requirements of your course?
Please write any additional comments relating to your placement below:
Print name: Signature: Date:
27 | P a g e

Practice Education
Placement No: Student Evaluation of Visiting LecturerType of placement Musculoskeletal Medical Surgical Neurology CombinedHospital/UnitPlacement dates From: To: Placement Number:Name of Visiting Teacher:
Yes No CommentsDid you feel that your Visiting Lecturer provided you with guidance and support when you needed it?
Did you feel that your Visiting Lecturer helped your individual development?
Did you receive feedback from your Visiting Lecturer that helped you to progress from your placement?How many visits did you receive from your Visiting Lecturer? 2 1
If > or < 2 visits, please comment
Any additional comments
Signature Print name Date
28 | P a g e

Practice Education
Visiting Teacher Evaluation of Practice Educator
Name of Practice Educator
Placement Site
Date
Yes No CommentsDid there appear to be a variety of learning experiences?
Did you feel the Practice Educator provided a positive commitment to student education?
Was the Practice Educator up to date with all the issues/procedures regarding clinical education?
If not, did the Practice Educator request training to develop such skills?
Did the Practice Educator promote a learning environment that encouraged a problem-solving approach?
Was the Practice Educator willing to discuss student progress and give feedback regarding performance?
Were the procedures for assessment of students followed?
Any additional comments
Signature Date
Practice Educator Evaluation of Visiting Teacher
29 | P a g e

Practice Education
Name of Visiting TutorPlacement SiteDate
Yes No CommentsDid you find the Visiting Lecturer reliable, and kept to specific times given?Did the Visiting Lecturer arrange to visit the student at least twice during the placement?Was the Visiting Lecturer willing to spend time to discuss the student’s progress?Did you feel that the Visiting Lecturer would help you to develop your skills and knowledge in areas of clinical education if it was requested?Did the feel that the Visiting Lecturer provided you with help and support when you needed it?Was the Visiting Lecturer willing to provide feedback on your performance and placement management??Did you feel that the Visiting Lecturer monitored the student’s progress and gave appropriate constructive feedback?
Any additional comments
Signature Date
30 | P a g e

Practice Education
Complaints Procedure for Practice Placements
Complaints Procedure for Students
1.1 Any complaint should normally be resolved with the Practice Educator and/or Visiting Lecturer
1.2 Students should approach their personal tutor for additional support
Complaints Procedure for Practice Educators
2.1Any complaint should normally be resolved with the student and/or Visiting Lecturer
2.2 If it cannot be resolved, the Practice Educator should liaise with the Practice Education Co-ordinators who will document the details of the complaint and any agreed action. The Programme Leader will be informed as appropriate.
2.3 If the complaint remains unresolved, the Practice Educator should liaise with the Physiotherapy Programme Lead.
Complaints Procedure for Third Parties i.e. patients/members of the public
3.1 If a complaint arises from a student interaction with a patient/member of the public whilst the student is on clinical placement, local policies and procedures of the placement site must be followed.
3.2Any complaint should normally be resolved with the student and/or Visiting Lecturer
3.3The placement site must inform the Practice Education Co-ordinators that a complaint has arisen and local policy is being followed.
The Practice Education Co-ordinators will document the details of the complaint and inform the Programme Leader.
For further details on regulations, refer to:Practice Placement Complaints Procedure for Pre-Registration Programmes found on the following web page:http://www.hpsc.mmu.ac.uk/ppl/
31 | P a g e

Practice Education
Faculty of Health, Psychology and Social CareDepartment of Health Professions
Form for recording all complaints arising from clinical placement
Name
Please delete as appropriate Student / Practice Educator / Patient / Member of Public
Contact details of complainant
Nature of complaint(further details may be attached)
Immediate action
Response to complainant including any agreed action
Name of staff who received the complaintSignatureDate
32 | P a g e

Unit descriptions, aims, student activity and assessment
Bullying GuidanceBullying is defined as any action taken which makes another feel intimidated, excluded, or unsafe. All individuals should be treated fairly and consistently, and with dignity and respect, wherever they study or undertake clinical placements.Placements should also be free from undue stress, anxiety, fear and intimidation (CSP, 2009).
Support is in place for individuals who feel that they are not being treated in an equitable way. Any issues regarding bullying should be reported to the visiting tutor in the first instance. Additionally, you are reminded that the CSP has produced draft guidance for individuals. Please see the following link: http://www.csp.org.uk/uploads/documents/Dealing_with_Bullying_PD046.pdf
Practice Educators are also advised to consult their Trust Policies on Bulling and Harassment.
Health and SafetyAll students undergo a medical examination prior to their acceptance at the School of Health, Psychology and Social Care.
Should the student experience periods of ill-health which result in absence from clinical placement, the Division requires that they produce a self-certificate (SC1) for absences in excess of three days and a Doctors certificate for absences in excess of one week.
We ask the students to inform the department in which they are placed of absence due to sickness by 9 am (or by the time specified in the Placement Profile) to minimise disruption to the department. Practice Educators should then document the number of hours of illness on the Common Assessment Tool (Appendix III).
During the course of clinical placements, staff and students are responsible for reading the Health and Safety Policy pertaining to the area in which they are situated. On each new clinical locality the student shall sign to say they have familiarised themselves with the policy and this is documented in their Clinical Experience Record Book. Students living in hospital residencies should consult the Health & Safety Policy in their specific location. All students receive training in:
i. Moving and handling operations
ii. Cardio-pulmonary resuscitation
iii. Fire prevention – records of attendance of these sessions are kept by the School.
iv. Infection Control
33 | P a g e

Unit descriptions, aims, student activity and assessment
Infection ControlPlacements take place in clinical environments. It is therefore possible that some patients may have conditions that are potentially infectious.It is essential that students work closely under the guidance of qualified staff, who will assess the health of each patient in order to reduce the potential risk to students as much as possible.
Assessment will take a number of factors into consideration: the type of treatment, the nature of any infectious disease that the patient may have had and the ability and level of the student. This will determine the suitability of the student’s contact with the patient – i.e. hands on treatment or observation only.
Intact skin is the best way to reduce the risk of becoming infected with or spreading infectious disease. Therefore it is important that any cuts, especially on hands, are covered with waterproof dressings. Students with eczema/dermatitis must ensure that their skin remains in good condition.
Any deterioration in skin condition must be reported immediately to the Department of Occupational Health & Safety, Central Manchester and Manchester Children’s University Hospitals Trust, or local Occupational Health Department if on placement and ‘hands on’ patient contact must be suspended pending further advice.
Hepatitis B/HIV/Hepatitis C/Other Blood Borne Viral InfectionsStudents will be offered immunisation against Hepatitis B at pre-placement health assessment.
A card with dates of vaccinations will be given to each student. It is important that this card is kept safely, especially when on placement in the event that subsequent doses of vaccine are required, when the student is not at Central Manchester and Manchester Children’s University Hospitals Trust
Immunisation is not available for other blood borne infections and therefore adherence to Infection Control Policies and careful work practice is essential.
If accidental contamination with blood/other body fluids occurs (e.g. needle stick injury) the student/staff member must report the incident to their supervisor and be referred immediately to the Department of Occupational Health & Safety (CMMC or local if on placement) or Accident & Emergency for advice. The Division must be notified.
Students may only treat patients with the above conditions under the very close supervision of their Practice Educator and whilst wearing appropriate protective clothing (e.g. gloves). If the Practice Educator perceives the risk to the student to be high, the student should observe only (e.g. no ‘hands on’ treatment).
TuberculosisAll students will be assessed / advised regarding immunity to Tuberculosis at pre-placement Health assessment. It is the policy of the Division that students should not treat patients with active TB.
Methicillin Resistant Staphylococcus Aureus (MRSA)If a patient is known to be MRSA positive, students can have hands on treatment as long as infection control procedures are properly followed. Once the gloves and apron are removed hands should be disinfected with alcohol hand rub or gel prior to
34 | P a g e

Unit descriptions, aims, student activity and assessment
leaving the clinical area and before contact with other patients. Whenever possible, MRSA patients should be seen at the end of a session.
It is advisable that students with eczema or psoriasis on their hands should not care for MRSA patients if these lesions are inflamed.
If the student is inadvertently exposed to MRSA the Division should be informed immediately where a risk assessment for screening will be undertaken in the Department of Occupational Health and Safety at CMMC or elsewhere if on placement to ensure that the student is not ‘carrying’ the bacteria prior to continuing clinical work.
Swine FluThere is MMU guidance available on the following webpage http://www.mmu.ac.uk/swine-flu.php. The University should be informed if the diagnosis is confirmed using the following procedure:http://www.mmu.ac.uk/academic/asu/Regulations_for_UG_or_PG_Programmes/Appendix_9_%20Student_sickness_procedures.pdf . Students should inform the Programmes Office on 0161 247 4671. Students should identify a “flu buddy” to drop off the completed form. If it is determined that the student has contracted something other than Swine flu, and still needs to take time off, then MMU should still be informed using the same procedure regardless of the diagnosis. Students on placement should inform their placement first and as soon as possible, and then inform the Physiotherapy Programmes office immediately afterwards. Students on placement should follow the guidance provided by the NHS Trust or PCT hosting their placement with regard to the length of their sickness absence. Students with absences of >5 working days will need to provide a medical certificate. Below is the link to the National Pandemic Flu service – https://www.pandemicflu.direct.gov.uk/
35 | P a g e

Unit descriptions, aims, student activity and assessment
Procedures for sickness reporting on practice placement
The university has a procedure for reporting Absences from course and related activities (other than examinations or assessments). This is contained in an appendix to the regulations which can be found using the following link: http://www.mmu.ac.uk/academic/asu/Regulations_for_UG_or_PG_Programmes/Appendix_9_%20Student_sickness_procedures.pdf . For the purposes of the practice placement component the regulation should be interpreted as follows:
If you are absent due to illness from your practice placement, you must:1. Inform your practice placement educator immediately. It will be useful to them
if you could also indicate when you are likely to be able to return to practice placement.
2. Inform the practice placement administrator as soon as possible on the first day of absence. This can be done by telephone, email, or by a written message delivered by a third party.
If your absence is for less than seven days duration (inclusive of any non-working days) you must, upon resumption of your practice placement, complete and submit form SSC1 (obtainable from a link on WebCT) to Louise Taylor. You should do this even if you have had only one day off.
If your absence is, or is expected to be, for seven or more days duration (inclusive of any non-working days) you should submit a Medical Certificate signed by your Doctor to the practice placement administrator. The Medical Certificate should be mailed or otherwise delivered as soon as possible after you have obtained it from your Doctor.
A specimen medical certificate is attached.
You should note that if you require a medical certificate, your Doctor has three choices. He can
Complete a section to advise you, when you have recovered, that you are fit to return to work/practice placement or where appropriate, that your condition need not require you to refrain from work. He may suggest, under ‘Doctors remarks’, possible Work/practice placement restrictions or adjustments.
If a doctor suggests work restrictions or adjustments these must be discussed with the practice placement coordinators
Provide an Open certificate – this indicates the likely period of incapacity up to 6months during first 6 months of incapacity, then for clinically appropriate period up to indefinite.
If a Doctor completes this section it may be necessary to return for a further visit so that it can be confirmed that you are fit for practice placement. If your Doctor provides an open certificate you should discuss your return to placement with the practice placement coordinators
Provide a Closed certificate. This gives a date to return to work in the next 2 weeks. If your Doctor has completed this section then you may return to
36 | P a g e

Unit descriptions, aims, student activity and assessment
work/practice placement without seeking a further certificate to indicate that you are now recovered.
However, if you feel that you could return to work before the date indicated on the certificate, you should discuss this with the practice placement coordinators.Please note: you must additionally comply with any sickness procedure required by your placement provider. Remember to telephone your placement as soon as possible on the first day of absence.
Remember to contact the Practice placement administrator (Louise Taylor) once you return to practice placement. If you fail do this you may be recorded as being absent without authorisation.
At time of publication, the practice placement administrator is Louise Taylor located in the Placements office on 0161 247 2457 or email [email protected]
37 | P a g e

Unit descriptions, aims, student activity and assessment
specimen SSC1 (available through link on Webct)THE MANCHESTER METROPOLITAN UNIVERSITYSTUDENT SELF CERTIFICATE FOR ABSENCE DUE TO ILLNESS(FORM SSC 1)
Name _____________________________ Department ____________________________Course_______________________________________ Course Year __________________Date and time illness began: ___________________________________________________(including non-working days)First Notification to: ____________________________ On _________________________(give name of person notified and method by which this was done and date done)
Reason for absence: (e.g. nature of illness or description of accident)
Please describe symptoms (or give details of any accidental injuries)
Did you attend: (delete as appropriate) Hospital Clinic Doctor
Did you receive medication from: Hospital Clinic Doctor or: Self prescribed from chemist
Name(s) of medication ___________________________________ ___________________________________If you are still absent due to illness when are you likely to return? ____________________Give details of any course related work adversely affected by your illness or accident(use additional paper if necessary and staple to this form)
I understand that if I provide inaccurate or false information about my absence, it may be treated as misconduct under the University's Student Disciplinary Procedure. I undertake to inform my Head of Department of my resumption of course related work.
Signature: Date:__________________________________________________________________________Any departmental notes should be made on the reverse of this form
38 | P a g e

Unit descriptions, aims, student activity and assessment
specimen medical certificate
39 | P a g e
Open certificatePeriod of incapacity up to 6months during first 6 months of incapacity, then for clinically appropriate period up to indefinite. If the Doctor completes this section it may be necessary to return for a further visit so that it can be confirmed that you are fit for practice placement. If your Doctor provides an open certificate you should discuss your return to placement with the practice placement
Closed certificateDate to return to work in the next2 weeks. If your Doctor has completed this section then you may return to work/practice placement without seeking a further certificate to indicate that you are now
This section is completed to advise you that you are fit to return to work/practice placement or where appropriate, that your condition need not require you to refrain from work - in which case the Doctor may suggest, under ‘Doctors remarks’, possible Work/practice placement restrictions or adjustments. If a doctor suggests work restrictions or adjustments these must be discussed with the practice placement coordinators

Practice Education
Procedure for Supporting Disabled students on Practice Placement
1) A student’s disability is considered by the Practice Placement Team when allocating practice placements in order to allow for effective pre-placement planning/allocation of an appropriate placement.
2) Following the allocation of practice placements, personal tutors should arrange to meet with their students to discuss their Personal Learning Plans (PLP) in relation to practice placements. A copy of the pre-placement proforma and guidelines should be emailed to the student prior to this meeting so that they are able to consider their potential needs in advance. A copy of the definitive procedure should also be sent to inform the students of the processes in place and also to highlight their responsibilities within this procedure.
3) The pre-placement proforma should be completed at this meeting and then saved to the shared drive (with agreement from the student) to sit alongside their individual PLP. The importance/implications of disclosure should be discussed at this meeting and the outcome of this discussion should be documented within the relevant paperwork. A hard copy of the pre-placement proforma (signed by both the student and the personal tutor) should be kept in their personal tutee file.
4) The personal tutor and the student should then agree who is to instigate any agreed actions arising from their meeting including any arrangements for a pre-placement meeting if appropriate. Normally the expectation would be for the student to instigate any agreed actions however in some cases it may be necessary for the Personal Tutor/Visiting tutor/University Link Lecturer or Disability tutor to do so. This process ensures that any necessary reasonable adjustments can be set up following discussion with their Practice Educator and implemented prior to the start of the placement if appropriate. Any outstanding issues/concerns should be discussed with the programme Disability tutor/ Learning Support Unit/Practice Placement Team as appropriate and any further action taken as necessary. Please note it is the student’s responsibility to liase with their relevant tutor and Practice Educator if adjustments need to be amended.
5) Following allocation of the visiting tutors/University Link Lecturers (ULL) to their respective students, visiting tutors/ULL should review any relevant information on the shared drive (PLP and pre-placement proforma). This ensures they have up to date information regarding any disabled students they may be visiting and hence any reasonable adjustments that should have been put in place. Please note that for those students with a PLP in place their name on the visiting tutor list will be followed by PLP in brackets eg Jo Bloggs (PLP). This visiting tutor list will only be distributed to academics.
6) On visiting their students on placement the visiting tutor/ULL should ensure that any appropriate adjustments have been implemented and that the
40

Practice Education
student and Practice Educator are fully supported (this information should also inform the visiting tutor/ULL if the student has chosen not to disclose). Any outstanding issues/concerns should be addressed with the Practice Educator in the first instance and the Programme disability tutor and/or Practice Education Team if appropriate. The visiting tutor (on their second visit to the student) should encourage the student to contact their next placement (if appropriate) to organise any necessary reasonable adjustments in advance.
7) On completion of the placement the visiting tutor/ULL (in agreement with the student) should note down any disability specific issues onto the student’s initial pre-placement disability proforma. This should relate to for example, the successful implementation of any reasonable adjustments and any suggested recommendations for future placements.
8) Steps 4→7 should be completed for placements 2 and 3. Please note that the personal tutor will not have had the opportunity to meet up with the student whilst they are on practice placement 1 therefore the student and/or the visiting tutor/ULL on practice placement 1 should be encouraged to arrange/set up any necessary reasonable adjustments for the forthcoming placements. The visiting tutor/ULL is responsible for liaising with the student’s personal tutor and the student’s next visiting tutor as appropriate. In some circumstances it may be necessary for the student to meet up with their personal tutor in the break between P2 and P3. Should the student wish to do so it is their responsibility to arrange this meeting with their personal tutor.
9) Prior to the commencement of placement 4 in the 3rd year the student’s personal tutor should again review the student’s PLP and modify the pre-placement proforma accordingly setting new action plans if appropriate for placements 4, 5 and their forthcoming elective. In exceptional circumstances this pre-placement meeting could take place earlier (for example in the summer) if appropriate, in order for any reasonable adjustments to be implemented in time for the start of their practice placement.
Please noteStudent’s should be encouraged to take responsibility for their own learning on practice placement for example in the setting up of any agreed reasonable adjustments however academic staff (personal tutors/visiting tutors/ULL) should also be prepared to assist and support their students where appropriate as an integral part of their role.
Revised by JN/KB 23/12/08
41

Practice Education
Professional DressProfessional dress standards are strictly adhered to. Normally dress must not be mixed i.e. part casual/part uniform. These guidelines are issued to ensure the safety of the student and the patient/model.
The following guidelines relating to ‘CLINICAL UNIFORM’ apply to clinical placements, ward/department tutorials and visits, clinical observation and practical examinations.
CLINICAL UNIFORM
Manchester Metropolitan University identity badges and Trust identity badges (if supplied) must be worn at all times.
Male Students
White tunic/ Polo Shirt } Clean and ironed/pressedPlain navy (dark blue) trousers }Plain white shirt with plain dark coloured tieDark coloured, rubber soled shoes or predominantly white training shoesBlack/navy (dark blue) socksAll footwear must be CLEAN
Female Students
White tunic } Clean and ironed/pressedPlain navy (dark blue) trousers }Dark coloured, rubber soled shoes or predominantly white training shoesBlack/navy (dark blue) socks or neutral coloured tightsAll footwear must be CLEAN
Dark blue sweatshirts/cardigans (approved style) may be worn between locations; THEY MUST NOT BE WORN WHILE TREATING PATIENTS
As above or:
Navy track suit trousers } Clean and ironed/pressedWhite polo shirt }Predominantly white (clean) training shoesWhite socks
42

Practice Education
Students should not leave placement premises in uniform unless going on an official visit.
Hair
Should be kept neat and tidy and back from the faceHair accessories should be plain and discreet
Make-up
Should be subtle
Nails
Should be short, long nails prevent the effective application of some techniques and may place patients at risk during moving and handling
Nail Polish/Acrylic Nails
Nail polish should NOT be worn (including clear). Acrylic nails or nail extensions are inappropriate.
Jewellery
NO JEWELLERY other than a wedding ringA wristwatch may be worn but must be removed whilst treating/handling patientsEarrings – stud type onlyA small discreet nose stud (if appropriate)
See Rule 8 of the Rules of Professional Conduct.
NB: IF ANY DEPARTMENT/UNIT HAS DIFFERING REQUIREMENTS TO THESE PLEASE INFORM THE SCHOOL OF HEALTH, PSYCHOLOGY AND SOCIAL CARE, MMU, IN WRITING. THIS INFORMATION WILL THEN BE INCLUDED IN THE PLACEMENT PROFILE, HOUSED IN THE ELIZABETH GASKELL LIBRARY. THIS ENSURES THAT THE STUDENTS RECEIVE THE CORRECT INFORMATION ABOUT YOUR PLACEMENT.
43

Practice Education
Development of Clinical PracticeStudents will be introduced to the elements of physiotherapy practice during preceding units.
Before commencing a clinical placement the student should have:
1. Knowledge of the hospital/department and any other information relevant to clinical placement. This is provided in the Placement Profile written by the placement and is housed in the Elizabeth Gaskell library, MMU and also found on the physiotherapy intranet and on Web CT.
2. Attended a compulsory practical session on manual handling and cardiopulmonary resuscitation.
3. Attended a fire lecture.
4. Acquired a limited range of core clinical skills.
5. Attended the Clinical Education Preparation sessions, which include the philosophy of clinical education; learning outcomes for placements; assessment procedures; practice of core skills; role play of clinical situations.
Students should bring with them: Common Assessment Tool. Practice Education Record Book which includes their LDP (This is to be
completed in negotiation with the Practice Educator within the first week on placement and not before).
Student Practice Education Handbook.
Role of the StudentEach student has the right to:1. A safe placement environment conducive to learning.2. Be treated in accordance with all applicable legislation e.g. The Special
Educational Needs and Disability Act 2001, Race Relations Act and Equal Opportunities.
3. Be treated in accordance with the draft CSP guidance regarding bullying (CSP, 2009).
4. Be treated in accordance with local Trust Policies on Bulling and Harassment.
Each student must be aware of their own responsibilities.
Each student:1. Is a representative of Manchester Metropolitan University.2. Has a responsibility to the placement provider, its patients, clients and staff.3. Must manage their own learning and professional relationships.
44

Practice Education
4. Has a responsibility to record their progress and achievements.5. Has a responsibility to inform the placement and the University regarding
problems with placements that might prevent completion of the placement (including personal and health issues).
Role of the Practice EducatorPractice Educators are normally Senior Physiotherapists who have been recommended by their Manager as skilful and interested in education.
The Practice Educator has the right to:
1. Be treated in accordance with all applicable legislation e.g. The Special Educational Needs and Disability Act 2001, Race Relations Act and Equal Opportunities.
2. Be treated in accordance with their Trust Policies on Bullying and Harassment
The Practice Educator has a responsibility to:
Plan a period of clinical education including placement orientation.
3. Negotiate with the student a mutually agreeable learning development plan with reference to the specific learning outcomes for that area and to the individual needs of the student.
4. Facilitate clinical reasoning to emphasise the problem-solving approach in the clinical setting by discussion of the examination/assessment of the patient to:
interpret clinical findings identify main problems requiring attention to develop and justify a suitable plan of treatment
This process encourages reflective practice to identify the knowledge base, strengths and weaknesses and therefore motivate the student to become an active learner.
5. Facilitate clinical reasoning to emphasise the problem solving approach in the clinical setting by discussion of the effectiveness of the chosen treatment modalities and modifications in treatment to:
monitor the effectiveness evaluate the outcome
6. Provide demonstrations of appropriate clinical skills or allow the student to observe practice.
7. Observe the student in the clinical situation to ascertain the effectiveness of clinical professional practice and provide the student with constructive feedback on their progress and development.
8. Monitor the records kept by the student.9. Provide where appropriate, opportunity to attend multi-disciplinary case
conferences, ward rounds, theatre and other relevant areas.10.Liaise with the Visiting Lecturer with respect to the student’s and Practice
Educator’s needs.
45

Practice Education
11.Assess the student’s progress midway giving written feedback and plan of action for development. Assess the student’s progress at the end of the clinical placement. Liaise with Visiting Lecturer throughout placement.
12.Treat each student in accordance with the appropriate legislation
The Role of the Visiting LecturerThe academic staff have an important role to play in the clinical education component of the programme.
They are committed to making visits to all sites where students are gaining clinical experience.
The Visiting Lecturer has the right to:
13.Be treated in accordance with all applicable legislation e.g. The Special Educational Needs and Disability Act 2001, Race Relations Act and Equal Opportunities.
14.Be treated in accordance with the appropriate Trust of University policy on Bullying ands Harassment.
The Visiting Lecturer has the responsibility to:
provide a regular link with the School
support the student and facilitate their active learning
support the Practice Educator in their role as facilitator of student learning
facilitate clinical reasoning to emphasise the problem-solving approach in the clinical setting
provide the student and Practice Educator with constructive feedback from the visit and action planning for the following visits/placements.
Support the Practice Educator in their role as assessor of student performance and to act as internal moderator of the assessment procedure.
The Visiting Lecturer will normally make 2 visits however; additional visits can be arranged depending on the needs of students and Practice Educators.
NB. For insurance purposes:
It is recommended that academic Visiting Lecturers do not get directly involved in the management of patients. Their role is to facilitate the learning process in the clinical setting.
46

Practice Education
Learning from Practice
Learning Development Plans / Learning AgreementThe CSP states in its Clinical Education Placement Guidelines (2003):
“Within the first week, a learning agreement is negotiated between the student(s), and Practice Educator which takes into account the individual student needs within the parameters of the clinical education placement”.
This is a very important tool which facilitates learning. It is a way for the students and Practice Educators to recognise preferred learning styles and enable both to maximise the learning opportunities available on the placement.
In its simplistic form a learning development plan should be considered as a:
“..Document drawn up by the student and the clinician and identifies what the student wants to learn, how they will work to achieve this, and what the criteria for evaluation will be”.
Bouchard and Steele (1980, Cited by Gibson (1989) p226)
The students are strongly encouraged to take responsibility for their own learning and are asked to prepare for the placement by referring to the appropriate learning outcomes featured on practice placement proformas and the performance and assessment criteria as stated in the Common Assessment Tool (Appendix III), as well as familiarising themselves with the Placement Profiles. By a process of mutual negotiation and discussion early in the placement the student should then be able to identify specific learning needs and set personal goals and objectives in negotiation with you, as Practice Educator.
Although the outcome of the learning development plan is important you should consider the process of negotiation of equal value, in that, by analysing learning needs, giving constructive criticism and feedback you are encouraging reflective practice and a mutual commitment to continuing personal and professional development.
By the end of the first week the negotiating process should result in the drawing up of the written document and this is the sole responsibility of the student.
The student is also responsible for the monitoring of their progress by recording “Highs” and “Lows” of the placement, new skills acquired or any specific key incidents from which they have learned.
To assist with this monitoring, the student will be encouraged to keep a record of reflective practice, the contents of which may then be transferred to a personal portfolio. This can then be used to evidence their commitment to continuing professional development.
47

Practice Education
Through the learning development plans the student should be able to critically analyse his/her performance and draw professional conclusions which may then be carried forward to future clinical placements. It will also help the student’s Personal Tutor to lead a more structured discussion in the de-briefing tutorial on the student’s return to the University.
(A Learning Development Plan can found in the Practice Education Record Book, Appendix II)
Assessment of Clinical Practice
Clinical ObservationMSc Pre-registration:Students arrange five days (37 hours) in total of participant observation of clinical practice.
BSc Hons:Students arrange four days (24 hours) in total of participant observation of clinical practice.
Students then inform the University of the details of the placement (see Appendix I). Before commencing PPO, students are required to have undertaken a occupational health check and CRB check. There is also a minimum attendance requirement for both programmes that must be fulfilled in order to attend clinical placement.
All students must successfully complete the period of clinical observation prior to commencing subsequent practice placements.
As students are normally members of the Chartered Society of Physiotherapy they are subject to the rules of Professional Conduct. Students are therefore assessed on their competency to practice safely during this placement together with their ability to be professional at all times. The assessment forms are found in the Student Practice Placement 0 Handbook which is required for post clinical debrief sessions.
Practice Placement 1 to 5
These placements are arranged by the clinical education team.
During First Week
1. The student and Practice Educator will meet to negotiate the Learning Development Plan.
2. At this meeting the date for mid-placement grading will be agreed (normally this will be a date half way through the placement).
One Day Prior to Agreed Date for Mid-Placement Grading
48
Practice Education
1. The student will undertake and document a self evaluation, using the Common Assessment Tool.
At Mid-Placement Grading (normally half way through placement)
1. The Practice Educator will assign the student a grade for each category in each section, and will discuss with the student the grades allocated.
2. Grades will be recorded in the Common Assessment Tool.
3. The Practice Educator will document his/her comments and recommendations for the students continuing development throughout the remainder of the placement in the appropriate sections of the Practice Placement Assessment document.
Final Grading (normally on final day of placement )
1. The Practice Educator will assign the student a grade for each section.
2. The final grades will be presented to the student by the Practice Educator.
3. The Practice Educator will document Final Comments/Recommendations in the Common Assessment Tool
4. The student will document their final comments in the practice placement assessment document.
5. The Common Assessment Tool should be signed by the Practice Educator and the Student after the final grading discussion has taken place.
6. The Common Assessment Tool is returned to the student.
7. The Feedback given will contribute to the development of the student, whilst the assessment outcome for the Practice Placement is PASS / FAIL on the Pre registration MSc programme. For students on the BSc Hons programme, the assessment outcome contributes to the final degree award.
Elective PlacementStudents will arrange an Elective placement of four weeks (normally 125) duration to be completed at the end of the programme prior to graduation. Students are expected to demonstrate an acceptable level of clinical skills and underpinning knowledge; an acceptable level of professional behaviour and safe practice.
49
Practice Education
Appendix Ia: Clinical Observation Documentation MSc Pre-registration Programme
Faculty of Health, Social Care & EducationDepartment of Health Professions
CLINICAL EDUCATION
TO ALL FIRST YEAR STUDENTS
PARTICIPANT OBSERVATION
Prior to undertaking your practice placements you are required to complete successfully a total of 5 days of participant observation with a qualified physiotherapist. These five days may take place in one or two clinical environments. They must take place before Patient Management 2.
It is your responsibility as a student to organise these days.
The objective of this participant observation is to introduce you to the clinical environment.
The specific learning outcomes are that you will have:-
- developed basic interpersonal skills in a clinical setting.- had an opportunity to observe physiotherapists working in a
variety of Health Care settings.- reflected upon learning experiences.
A workbook will be supplied which, when completed, will form the foundation for debrief tutorials which will be held on your return to University.
This element of the programme is COMPULSORY and forms part of the total clinical education leading to your professional qualification. Please download copies of the appropriate letter and form from webCT and return the completed forms and letters on headed notepaper indicating the clinical locations and permission from managers to the Physiotherapy Placement Administrator at the Placement office, 4th Floor Tower Block by the date indicated in your Year Handbook.
These hours contribute to the total hours required for qualification for membership of the Chartered Society of Physiotherapy.
50

Practice Education
Appendix Ib: Clinical Observation Documentation BSc Hons Programme
Faculty of Health, Social Care & EducationDepartment of Health Professions
PRACTICE EDUCATION
TO ALL FIRST YEAR STUDENTS
PARTICIPANT OBSERVATION STUDY
Prior to undertaking clinical education in the 2nd year of the course you are required to complete successfully a total of 4 separate days of participant observation with a qualified physiotherapist.
It is your responsibility as a student to organise these days.
The objective of this participant observation is to introduce the student to the clinical environment.
The specific learning outcomes are: that the student will have:-
- developed basic interpersonal skills in a clinical setting.- had an opportunity to observe physiotherapists working in a
variety of Health Care settings.- begun to develop skills of Self-evaluation with respect to
learning
A workbook will be supplied which, when completed, will form the foundation for debrief tutorials which will be held on your return to the School.
This element of the course is COMPULSORY and forms part of the total clinical education leading to your professional qualification. Please download copies of the letter and form from Web CT and return the completed forms and letters on headed paper indicating the clinical locations and permission from managers to the Physiotherapy Placement Administrator at the Placement office, 4 th Floor Tower Block. These hours contribute to the total hours required for qualification for membership of the Chartered Society of Physiotherapy.
51

Practice Education
Appendix 1c: Practice Placement 0 Letter from Practice Educator (MSc Pre-reg)
Faculty of Health, Social Care & Education
Department of Health ProfessionsManchester Metropolitan UniversityElizabeth Gaskell CampusHathersage RoadMANCHESTERM13 0JA
Tel/Fax: 44 [0] 161 247 2457Email [email protected]
Date as postmark
Dear Colleague
Re: CLINICAL EDUCATION: PARTICIPANT OBSERVATIONAs an introduction to physiotherapy practice, 1st Year students are required to undertake a total of 5 days of participant observation, which is to be arranged by the student. The School would be pleased if you could offer: ……………………………………………………….... (Name of student)
the opportunity to shadow a member of your staff during the following period:
………………………………………………………………..
The objective of this participant observation is to introduce the student to the clinical environment.
The specific learning outcomes are that the student will have:-
- developed basic interpersonal skills in a clinical setting.- had an opportunity to observe physiotherapists working in a variety of
Health Care settings.- reflected upon their learning experiences.
Students will be given a workbook to complete during their visit which will involve enquiry, but should not involve the clinician in any extra paperwork. The workbook will form the basis of tutorials which will be held when the student returns to University.
If you feel that you could offer this valuable experience would you please complete the attached form together with written permission on separate headed paper from the Physiotherapy Manager for the Participant Observation and return it to the student who will then return it to the University. The student must submit both the form and the letter for their observation study to be accepted by the university.
Appendix 1d: Practice Placement 0 letter from Practice Educator (BSc Hons)
52

Practice Education
Faculty of Health, Psychology and Social CareDepartment of Health ProfessionsElizabeth Gaskell CampusHathersage RoadMANCHESTERM13 0JA
Tel: 44 [0] 161 247 2457Email [email protected]
Dear Colleague,
Re: PRACTICE EDUCATION: PARTICIPANT OBSERVATION
As an introduction to physiotherapy practice, 1st Year students are required to undertake a total of 4 separate days of 6 hours each (ie 24 hours in total), of participant observation at the end of their 1st Year, which is to be arranged by the student.
The School would be pleased if you could offer
……………………………………………………….... (name of student)
the opportunity to shadow a member of your staff for 4 days.
The objective of this participant observation is to introduce the student to the clinical environment.
The specific learning outcomes are: that the student will have:-
- developed basic interpersonal skills in a clinical setting.- had an opportunity to observe physiotherapists working in a variety of
Health Care settings.- begun to develop skills of Self-evaluation with respect to learning
Students will be given a workbook to complete during their visit which will involve enquiry, but should not involve the clinician in any extra paperwork. The workbook will form the basis of tutorials which will be held when the student returns to the School.
If you feel that you could offer this valuable experience would you please complete the attached form together with written permission on separate headed paper from the Physiotherapy Manager for the Participant Observation Study and return it to the student who will then return it to the School. The student must submit both the form and the letter for their observation study to be accepted by the university.Appendix 1e: Practice Placement 0 confirmation letter (both Programmes)
53

Practice Education
Faculty of Health, Psychology and Social CareDepartment of Health Professions
CLINICAL EDUCATIONPARTICIPANT OBSERVATION
Permission is granted for:
NAME OF STUDENT: ………………………………………………………….
to undertake participant observation on (date/s):…………………………………(and state number of days)
NAME AND FULL ADDRESS OF HOSPITAL/UNIT:
…………………………………………………………………………………………..
…………………………………………………………………………………………..
…………………………………………………………………………………………..
TEL NO: …………………………………………………………………………..
FAX NO: …………………………………………………………………………..
NAME OF SUPERVISING CLINICIAN:
…………………………………………………………………………………………..
CLINICAL AREA: …………………………………………………………………..
SIGNATURE OF PHYSIOTHERAPY MANAGER:………………………………..
DATE: …………………………………………………………………………..
Please return (via the student) to Physiotherapy Placement Administrator, Placement Office, 4th Floor Tower Block, by the date stated in your Year Handbook.
54

Practice Education
Apendix 1f: Declaration of attendance letter (both Programmes)
Faculty of Health, Psychology Social Care
Department of Health ProfessionsManchester Metropolitan UniversityElizabeth Gaskell CampusHathersage RoadMANCHESTERM13 0JA
Tel/Fax: 44 [0] 161 247 2457Email [email protected]
CLINICAL EDUCATION
PARTICIPANT OBSERVATION
Name of Student:…..………………………Name of Personal Tutor: ………………..
Supervising Clinician: ………………………………………………………….………….
Clinical Location: ………………………………………………………..………………….
Location Address:………………………………………………………….……………….
……………………………………………………………………………………………….….
Thank you for accepting one of our MSc Physiotherapy (Pre-registration) students for a period of participant observation.
I should be pleased if you will sign the declaration of attendance.
Thank you for your support.
Clinical Education Team
DECLARATION OF ATTENDANCE
I certify that ………………………………………………………. has completed …………. hours of
participant observation on this unit.
Signed: …………………………………Designation:……………………………….…..
Date: …………………………………………………………………………………………..
Please return this to: student life by the date indicated in your Year Handbook.
55

Practice Education
Appendix 2Practice Education Record Book
Name ………………………………………………………………………..
Personal Tutor ………………………………………………………………………..
Visiting Tutor ………………………………………………………………………..
Placement number 1 2 3 4 5 Elective
Dates of Placement From …./…./20…. to …./…./20….
The purpose of the Practice Education Record book is to provide you with guidance on the variety of ways you are able to document your clinical experiences and hence assist you in providing relevant evidence to support your learning and development within this environment. This record book encourages you to link your experiences and learning gained on this placement to the current standards you are expected to be working towards in order to gain registration with the Health Professions Council (HPC) on qualification (HPC, 08) (page 7). All members of the Chartered Society of Physiotherapy (CSP) are also required to adhere to the Core Standards of Physiotherapy Practice (CSP, 2005) together with the Rules of Professional Conduct (CSP, 2002) (page 9). On page 11 and 12 examples are given of a NHS KSF Broad Post Outline: Band 5 Physiotherapist and a Person Specification for a Band 5 Physiotherapy rotational post. These examples will assist you in mapping your learning to the relevant skills, knowledge base, experiences, qualities and attributes, etc that are required in a newly qualified Physiotherapist. These documents may also assist you in highlighting any deficits in these areas which may help to inform your Learning development Plan whilst on placement.The gathering of this evidence will link into your CPD file and will be invaluable when applying for that first junior physiotherapist position. Any evidence gathered will enhance both your job application form and also the interview process. Use the following guidelines and headings to list/note down your experiences gained on this placement. In order to demonstrate what you have learnt from these experiences you will need to provide a more detailed account/reflection on what you have learnt (see page 14 for a list of possible ways to document/evidence your learning).
56

Practice Education
List:
Patient problems/diagnosis if appropriate
57

Practice Education
General skills I have developed on this placement;
These could include communication skills, time management skills, caseload management, clinical reasoning, dealing with conflict, team working or presentation skills.
58

Practice Education
Specific treatments/skills:
These could include, for example, manual handling skills, exercise prescription, electrotherapy skills, chest clearance technique.
59

Practice Education
Other learning experiences: These could include, for example, ward rounds, consultant clinics, case conferences, interprofessional working/learning, theatre visits, home visits.
60

Practice Education
Learning Development Plan
Learning Objective(What is it I want to be able to do - these must be SMART goals)
Resources/Methods (What do I need to do to achieve my learning objectives).
Evaluation Criteria (How will I know I have achieved my learning objectives? What is it I can do differently?)
Outcome (Have I achieved my learning outcome? How well did I do this?)
61

Practice Education
Standards, codes of practice and performance criteriaIn the following pages you will find information outlining:
The Health Professions Council (HPC) Standards of conduct, performance and ethics (HPC, 2008)
The Core Standards of Physiotherapy Practice (CSP,2005) The Rules of Professional Conduct (CSP, 2005) The NHS KSF (Knowledge and Skills Framework) Broad Post Outline: Band 5
Physiotherapist Person specification for a Band 5 Physiotherapy Rotational Post A table suggesting ways of evidencing your experiences/learning on placement
Using the experiences you have listed/noted in the preceding pages (including the objectives in your LDP which you set yourself for this placement) try and link your experiences to the HPC and CSP standards, the KSF core dimensions and the essential/desirable criteria as noted in the person specification. Once you have completed this choose 2, 3 or more different experiences that you have identified as linking to the outlined standards/dimensions/criteria that you would specifically like to provide evidence for (you may find that one piece of evidence will cover/link into more than one standard/dimension/criteria).Once you have chosen your specific experiences, you need to consider the type of evidence you could provide and link this to the appropriate standard/dimension/criteria etc by writing a short reflective dialogue to demonstrate your learning. This evidence can also be linked to your placement document within your CPD file.
HPC (Health professions council) The HPC Standards of conduct, performance and ethics have recently been revised (HPC, 2008). They provide guidance for Health Professionals who are registered with them as well as those applying to become registered. They set out the expectations that they expect of their registrants with regards to professional behavior and help them make decisions about their practice. The HPC (2007) have also published Standards of proficiency that ensure all the professions they regulate work safely and effectively. Health Professionals must therefore also meet these standards to become registered (see reference list for a link to these standards).
Standards of conduct, performance and ethics Your duties as a registrantThe standards of conduct, performance and ethics you must keep to
1. You must act in the best interests of service users.
2. You must respect the confidentiality of service users.
3. You must keep high standards of personal conduct.
4. You must provide (to us and any other relevant regulators) any
5. important information about your conduct and competence.
62

Practice Education
6. You must keep your professional knowledge and skills up to date.
7. You must act within the limits of your knowledge, skills and
8. experience and, if necessary, refer the matter to another practitioner.
9. You must communicate properly and effectively with service users
10. and other practitioners.
11. You must effectively supervise tasks that you have asked other
12. people to carry out.
13. You must get informed consent to give treatment (except in
14. an emergency).
15. You must keep accurate records.
16. You must deal fairly and safely with the risks of infection.
17. You must limit your work or stop practicing if your performance or
18. judgement is affected by your health.
19. You must behave with honesty and integrity and make sure that
20. your behaviour does not damage the public’s confidence in you or your
21. profession.
22. You must make sure that any advertising you do is accurate.
63
Practice Education
Chartered Society of physiotherapy (CSP) Both qualified and student members of the Chartered Society of Physiotherapy are expected to adhere to the Core Standards of Physiotherapy (CSP, 2005) and the Rules of Professional Conduct (CSP, 2002). They link very closely to the HPC Standards of conduct, performance and ethics and to the NHS KSF dimensions.
The Core Standards of PhysiotherapyPatient PartnershipStandard 1 Individualised approachStandard 2 ConsentStandard 3 ConfidentialityAssessment and Treatment CycleStandards 4 – 6 AssessmentStandard 7 AnalysisStandard 8 Treatment planningStandard 9 ImplementationStandard 10 EvaluationStandard 11 Transfer of care/dischargeCommunicationStandard 12 Communication with patients and carersStandard 13 Communication with other professionalsDocumentationStandard 14 Record keepingStandard 15 Storage of recordsPromoting a Safe Working/Treatment EnvironmentStandard 16 Patient and physiotherapist safetyStandard 17 Physiotherapists working aloneStandard 18 Equipment safety
64

Practice Education
Continuing Professional Development (CPD)Standard 19 Assessment of CPDStandard 20 Planning of CPDStandard 21 Implementation of CPDStandard 22 Evaluation of CPD
65

Practice Education
Knowledge and skills framework (KSF)With the implementation of Agenda for Change (AFC) within the NHS came the implementation of the KSF. This framework together with the Development review process will assist both personal and service development. The framework includes 6 core dimensions which are common to all NHS workers. These Core dimensions include: Communication, Personal & People Development, Health, Safety & Security, Service improvement, Quality and Equality & Diversity. These core dimensions apply to all posts within the NHS hence all physiotherapy staff have them in their post outlines including newly qualified physiotherapists. Each dimension has 4 levels (level 1- level 4). The level within their post outline will be dependent on their role (CSP, 2006). Staff will be expected to provide evidence that they are achieving these post outline level descriptors. An example of a NHS KSF Broad Post Outline for a Band 5 Physiotherapy post is shown below overleaf.
66

Practice Education
NHS KSF Broad Post Outline: Band 5 Physiotherapy
Reporting to Clinical Lead Physiotherapist
Job Purpose Assess, treat and manage own caseload of patients as an autonomous practitioner in a variety of clinical settings on a rotational basis
No Dimension Level KSF Post outline set: Level descriptor Level Foundation subset: Level descriptor
C1 Communication 2 Communicate with a range of people on a range of matters
2 Communicate with a range of people on a range of matters
C2 Personal & People Development
2 Develop own knowledge & skills & provide information to others to help their development
2 Develop own knowledge & skills & provide information to others to help their development
C3 Health, Safety & Security
2 Monitor and maintain health, safety 7 security of self and others
2 Monitor and maintain health, safety 7 security of self and others
C4 Service improvement
2 Contribute to the implementation of services
2 Contribute to the implementation of services
C5 Quality 2 Maintain quality in own work and encourage others to do so
2 Maintain quality in own work and encourage others to do so
C6 Equality & Diversity 2 Support equality and value diversity 2 Support equality and value diversity
HWB6 Assessment and 3 Assess physiological and/or psychological 3 Assess physiological and/or
67

Practice Education
Treatment Planning functioning and develop, monitor and review related treatment plans
psychological functioning and develop, monitor and review related treatment plans
HWB7 Interventions and Treatments
3 Plan, deliver & evaluate interventions &/or treatments
3 Plan, deliver & evaluate interventions &/or treatments
68
Practice Education
Qualities and attributes required for a Band 5 Physiotherapy post When applying for a Band 5 Physiotherapy post you will be provided with a job description and a person specification. The person specification will set out a list of essential criteria that they expect the applicant to have and a list of desirable criteria that they would like the applicant to have. It is therefore important that you are able to provide evidence that you meet these criteria when applying for a particular post. Any evidence gathered will inform and enhance both the application and interview process. Below is an example of a person specification for a Band 5 Physiotherapy Rotational Post:
Person Specification
Job Title – Physiotherapist - Rotational
Specification Essential/Desirable How can I demonstrate that I
have this quality
QualificationsEssential:
Physiotherapy degree or equivalent professional qualification
Registered with the UK HPC
Desirable:
Membership of the CSP
ExperienceEssential:
Undergraduate placements in core Physiotherapy areas
Desirable:
Experience of multi-disciplinary team working
69
Practice Education
Specification Essential/Desirable How can I demonstrate that I
have this quality
Skills and abilities
Essential:
Good time management skills Ability to prioritise appropriately.
Timely management of patient medical records.
Written & verbal communication skills.
Practice Evidence Based therapy.
Ability to be aware of clinical & non-clinical complications & risks.
Ability to thrive in a multidisciplinary environment.
Enthusiasm for IST including presentation of IST & cases .
Basic management skills-to be able to help organise caseload & others.
Recognition of need for timely and accurate data.
Desirable:
Understanding of audit & outcome measurement.
IT literacy / presentation.
KnowledgeEssential:
Awareness of NHS & Trust systems, policies, procedures & current changes.
Sound therapeutic & clinical knowledge.
Personal Qualities
Essential:
Self motivated and self directed.
70

Practice Education
Specification Essential/Desirable How can I demonstrate that I
have this quality Excellent communication skills.
Excellent interpersonal skills.
Teamworker.
Able to work under pressure – flexible.
Motivational
Lateral thinker.
Below is a list of evidence you could provide to demonstrate your adherence to the HPC/CSP standards, NHS KSF core dimensions or to demonstrate that you meet the essential/desirable criteria in the person specification however it is not exhaustive. Any of these suggestions should then be linked to that particular standard, dimension, criteria etc with a short reflective piece to link your evidence to your learning.
Type of evidence Case study Reflective account (short reflective piece ~250 - 500 words/reflective assignment) Clinical supervision records if appropriate (ensure you gain permission for this and also
ensure patient and trust confidentiality) Literature search and critical review iCSP report Presentations Assessment sheets In service training/structured tutorials Patient information leaflets/exercise programmes Department policy documents/procedures Peer review sheets Reflective proforma (see overleaf for an example of a Reflective Practice Proforma)
71

Practice Education
Reflective Practice Proforma
72

Practice Education
Describe the experience (what happened)
What did you do and why did you do it?
What worked well? (what was good about it)
What could have been better? (what was not so good about it)
What did you learn from this experience?
73
Practice Education
How will you apply this learning in the future?
What would you do differently in a similar situation?/How could you apply what you have learned to other situations?
74

Practice Education
Summary of meeting with Visiting tutor
Name ………………………………………………………………………..
Personal Tutor ………………………………………………………………………..
Visiting Tutor ………………………………………………………………………..
Placement number 1 2 3 4 5 Elective
Dates of Placement From …./…./20…. to …./…./20….
Content
Remarks and Recommendations
Action Plan
Date of next visit
Date/signature of Visiting tutor Date/signature of student Summary of meeting with Visiting tutorName ………………………………………………………………………..
Personal Tutor ………………………………………………………………………..
Visiting Tutor ………………………………………………………………………..
Placement number 1 2 3 4 5 Elective
Dates of Placement From …./…./20…. to …./…./20….
Content
75

Practice Education
Remarks and Recommendations
Action Plan
Date of next visit
Date/signature of Visiting tutor Date/signature of student
76

Practice Education
ReferencesChartered Society of Physiotherapy (CSP) (2005) Core Standards of Physiotherapy, London, Chartered Society of Physiotherapy. Available from the World Wide Web at <http://www.csp.org.uk/uploads/documents/csp_core_standards_2005.pdf>
Chartered Society of Physiotherapy (CSP) (2005) Learning in the practice environment in qualifying programmes of Physiotherapy. CSP Information Paper: QA 05 [cited 24th July 08). Available from the World Wide Web at < http://www.csp.org.uk/uploads/documents/csp_quality_qa05.pdf>
Chartered Society of Physiotherapy (CSP) (2006) Guidance Paper; Equality and Diversity: Addressing core dimension 6 of the NHS Knowledge and Skills Framework Reference MOS/KSF/V3 [cited 18th July 2008) . Available from the world wide web at< www.csp.org.uk>
Chartered Society of Physiotherapy (CSP) Rules of Professional Conduct (2002), London; Chartered Society of Physiotherapy. Available from the World Wide Web at <http://www.csp.org.uk/uploads/documents/csp_rules_conduct.pdf>
Department of Health (2004) The NHS Knowledge and Skills Framework and the Development Review Process [online]. Available from the World Wide Web: <http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4090843>
Health Professions Council (HPC) (2007), Standards of proficiency [online] [cited 23rd
September 2008] Available from the World Wide Web at <http://www.hpc-uk.org/assets/documents/10000DBCStandards_of_Proficiency_Physiotherapists.pdf>
Health Professions Council (HPC) (2008) Standards of conduct, performance and ethics [online] [cited 23rd September 2008] Available from the World Wide Web at <http://www.hpc-uk.org/assets/documents/10002367FINALcopyofSCPEJuly2008.pdf>
77

Practice Education
Appendix 3: Example common assessment tool level 5 BSc Hons
PHYSIOTHERAPYPRACTICE PLACEMENT ASSESSMENT
LEVEL 5(I)
STUDENT NAME
YEAR OF STUDY
DATES OF PLACEMENT
PLACEMENT NUMBER
PLACEMENT SITE
PLACEMENT AREA/TYPE OF PLACEMENT
PLACEMENT EDUCATOR
VISITING TUTOR
FOR UNIVERSITY USE ONLY
MARK AWARDED %
Contact HOURS
78

Practice Education
Submission of practice placement bookletsPractice placement booklets should be submitted to the Student Life Office according to their document ‘Coursework submission guidance’ available from the internet at <http://www.did.stu.mmu.ac.uk/studentinfo/other_information.php>
Late submission of practice placement bookletsMarks for practice placement booklets submitted after the deadline for submission without prior written agreement from the Examinations Officers will be subject to penalty. Students are advised to consult the Revised Regulations for Programmes of Study 2008/09, appendix 9 relating to late submission of coursework (available from the internet at <http://www.mmu.ac.uk/academic/asu/Regulations_for_UG_or_PG_Programmes/Appendix_1_Submission_of_coursework.pdf >
Practice placement 1 Unit code 28150011. Unit leaders J Nicholson/s Taylor
Placement booklet submission *
Written component submission *
Late submission deadline (both elements) *
Marks normally released
(Subject to confirmation by the board of examiners)
*
Practice Placement 2 Unit code 28150012. Unit leaders J Nicholson/s Taylor
Placement booklet submission *
Written component submission *
Late submission deadline (both elements) *
Marks normally released
(Subject to confirmation by the board of examiners)
*
79

Practice Education
Practice Placement 3 Unit code 28150013. Unit leaders J Nicholson/s Taylor
Placement booklet submission *
Written component submission *
Late submission deadline (both elements) *
Marks normally released
(Subject to confirmation by the board of examiners)
By post, within 5 working days of the meeting of the Board of examiners.
PLEASE NOTE THAT LATE SUBMISSION OF THE PRACTICE
PLACEMENT BOOKLET OR THE WRITTEN ASSIGNMENT WITHOUT
PRIOR ARRANGEMENT FOR PRACTICE PLACEMENT 3 MAY
PREVENT YEAR TWO RESULTS BEING TAKEN TO THE JUNE BOARD
OF EXAMINERS AS IT CANNOT BE GUARANTEED THAT MARKING
AND INTERNAL MODERATION WOULD BE FEASIBLE IN ADVANCE
OF THE MEETING OF THE BOARD OF EXAMINERS. DECISIONS
REGARDING PROGRESSION INTO YEAR 2 OF THE PROGRAMME
MAY HAVE TO BE DEFERRED TO THE SEPTEMBER MEETING OF
THE BOARD OF EXAMINERS.
Health & Safety Declaration
I certify that I have read the Health & Safety Policies of the appropriate clinical area/s noting particularly the procedure in the event of fire and cardiac arrest, local policies for Moving and Handling of loads and any other specific procedure limitations.
THIS MUST BE COMPLETED BY THE END OF THE FIRST WEEK OF
PLACEMENT AS PART OF THE PLACEMENT INDUCTION PROCESS.
Signature of student Date
80

Practice Education
INFORMATION ABOUT THE FORMThe assessment of the student performance is divided into two parts.Part 1 comprises ten aspects of practice that will contribute to the overall assessment of the student’s performance. These are based on the Standards of Proficiency (SoP) of the Health Professions Council and play a central role in admission to the Register. They are also linked to the KSF Dimensions (Core 1-6, and HWB 6 & 7). They have been grouped into four areas:
INTERPERSONAL SKILLS (SoP 1b) (KSF dimensions C1, C2, C6)The student will:1 Demonstrate effective and appropriate skills in communication
2 Contribute effectively to work undertaken as part of a team
MANAGEMENT OF SELF (SoP 1a & SoP 3) (KSF dimensions C2, C4, C5)The student will:3 Demonstrate effective self-management of workload
4 Know the limits of their own practice and when to seek advice
5 Independently manage their own learning
MANAGEMENT OF PATIENT (SoP 2a, 2b, 2c & SoP 3) (KSF dimensions C1, C3, C4, C6, HWB6, HWB7)The student will:6 Gather appropriate information relating to patient
7 Plan and carry out an appropriate objective examination
8 Analyse examination findings and formulate a written treatment plan in partnership with the patient
9 Implement and critically evaluate impact of, or response to, treatment interventions
DOCUMENTATION (SoP 2b) (KSF dimensions C1, C3, C5, HWB6)The student will:10 Maintain accurate patient records.
81

Practice Education
For each aspect of practice, performance criteria have been identified and assessment criteria have been given. These are intended to provide a framework of reference for the judgment made by the practice placement educator in determining the student’s overall achievement on placement. In the table below we have provided the degree classifications alongside their corresponding assessment criteria.
Assessment Criteria Degree ClassificationOutstanding 1st *Excellent 1st
Very good 2.1Good 2.2Acceptable 3rdFail Fail
PART 2 of the student assessment relates to SAFETY and PROFESSIONAL BEHAVIOUR. These areas are assessed using a pass/fail judgment against a set of criteria.
FAILURE OF EITHER SECTION IN PART 2 WILL NORMALLY
OVERRIDE PART 1 OF THE ASSESSMENT AND CAUSE THE
STUDENT TO FAIL THE PLACEMENT.
82

Practice Education
HOW TO COMPLETE THE PLACEMENT ASSESSMENT DOCUMENT – PART 1Clinical Placement marks contribute to a student’s final degree classification. It is therefore very important that you are objective when completing this document. Please follow the guidance below when assessing the students.
For each aspect of practice within Part 1: Read the performance criteria and ensure that you consider ALL points before
referring to the assessment criteria
Read the assessment criteria thoroughly, referring to the glossary of terms on page 8
In order to mark a student in a particular box, all aspects of the assessment criteria within that box must be met
Please consider ALL levels of assessment criteria for all students. Students should be able to achieve any grade for the placement if their performance objectively meets the assessment criteria for that grade. This is applicable to all placements.
At midway: Ensure that the student has completed their self evaluation using the
assessment criteria, and also completed their midway comments
Complete your midway assessment of the student using the assessment criteria and complete your feedback, linking your comments to the performance criteria
Good practice would be to discuss the midway assessment and comments with the visiting tutor before discussing with the student. Ideally the sharing of the document with the student at this point should be a tripartite meeting, of clinical educator, student and tutor. However, this may vary between Universities since we all have different visiting practices.
Set and document an action plan for each aspect of practice in negotiation with the student, to demonstrate areas for development during the second half of the placement. This may be done at the tripartite meeting
Please be aware that students failing any of the following aspects of practice (1, 3, 4, 6, 7, 9, 10) at midway should be referred to Part 2 of the document and given appropriate warnings. An action plan should be formulated.
83

Practice Education
At the final assessment: Complete your final assessment of the student using the assessment criteria
and complete your feedback, linking your comments to the performance criteria
Your grading of the student should be based on the student’s performance in the final week of their placement
Good practice would be to discuss the final placement marks with the visiting tutor before being given to the student, in order for the University to moderate between different educators. The timing of this may vary between Universities since we all have different visiting practices.
Ensure that your cross is within a box not on the line between two boxes
Please cross a box in every aspect of practice. Please seek guidance from the visiting tutor if you are unsure how any particular aspect can be applied to your placement setting
Please be aware that students failing any of the following aspects of practice (1, 3, 4, 6, 7, 9, 10) will automatically fail the placement for unsafe/unprofessional behaviour, and this should be documented in Part 2. Please see the note below regarding notification of poor performance.
IF YOU CONSIDER THAT YOUR STUDENT IS LIKELY TO FAIL ANY
SECTION OF PART 1 OF THE DOCUMENT AT ANY POINT IN THE
PLACEMENT, THE STUDENT AND THE VISITING TUTOR SHOULD BE
MADE AWARE OF THIS AT THE EARLIEST OPPORTUNITY IN ORDER
TO ALLOW MAXIMUM TIME FOR THE STUDENT TO IMPROVE
THEIR PERFORMANCE TO AN ACCEPTABLE LEVEL AND RECEIVE
APPROPRIATE SUPPORT FROM THE UNIVERSITY.
84

Practice Education
HOW TO COMPLETE THE PLACEMENT ASSESSMENT DOCUMENT – PART 2If you are concerned about the student’s safety and/or professional behaviour at any time during the placement you should refer to Part 2 of the Assessment document. Please follow the guidance below when completing this section of the form:
Read the fail descriptors within the relevant section(s) of Part 2
Students should be given a verbal warning regarding any unsafe practice and/or unprofessional behaviour at the time of the incident, in the first instance. This should then be documented in Part 2, and signed and dated by the clinical educator and the student, and if appropriate the visiting tutor
Repeated poor practice and/or behaviour warrant a written warning using the relevant section(s) of Part 2, which should be signed and dated by the clinical educator and the student. The visiting tutor must be informed at this stage
Repeated poor practice and/or behaviour may be the same or different aspects of practice (e.g. repeated poor time management, or a range of errors relating to unsafe practice)
An action plan should be formulated and documented in order to maximise the student’s ability to reach an acceptable standard of performance
At the end of the placement (or earlier if appropriate) the outcome section should be completed with appropriate comments relating to the outcome of the action plan. Examples are given below to assist with this
o If the action plan has been complied with and there have been no further incidents of unsafe practice and/or unprofessional behaviour then the student should pass the placement.
o If there have been further incidents of unsafe practice and/or unprofessional behaviour this should be documented in the comment section as the reason for the student failing the placement.
o The decision as to whether a student should pass or fail therefore depends on the number of incidents, and a student should not fail on one incident alone.
o A clear identification of whether the student has passed or failed must be given by placing a cross in the appropriate box.
PLEASE DO NOT DELAY DISCUSSING POOR PERFORMANCE WITH
THE STUDENT IN THE HOPE THAT THEY WILL IMPROVE AS THIS
REDUCES THE TIME THAT IS AVAILABLE FOR THEM TO REACH AN
ACCEPTABLE LEVEL
Please note that repeated incidents of unsafe practice and/or professional behaviour leading to more than 1 written warning could result in the student being removed from the placement at any stage – i.e. the decision to fail may not only happen at the end of the placement.
85

Practice Education
GLOSSARY of terms
Prompting Used to describe a situation where the clinical educator
provides input to the student by the use of a key word, indirect
or open questioning to facilitate learning
Professionalism
Used to describe the attitudes and manner of the physiotherapy
student and does not take into account issues around safety,
work environment or the application of skills.
Consistently Used to describe a situation where a student meets the
requirements of the criteria >90% of the time.
Most … Used to describe a situation where a student meets the
requirements of the criteria >60% but <90% of the time.
Some … Used to describe a situation where a student meets the
requirements of the criteria >30% but <60% of the time.
Occasional… Used to describe a situation where a student meets the
requirements of the criteria <30% of the time.
Complex and unpredictable
Events which would not normally occur within the normal day-
to-day running of a unit, or which would provide particular
challenge to the student
86

Practice Education
PART 1 INTERPERSONAL SKILLS1. Effective and appropriate skills in communication
Performance criteria initiates communication and actively seeks participation and collaboration when interacting
with patients, staff and others. chooses appropriate communication strategies when interacting with patients, staff and
others. uses appropriate language and body language when interacting with patients, staff and others. shows ability in listening skills. shows ability in questioning skills. deals with questions appropriately, considering own level of knowledge and understanding,
own level of authority/responsibility is responsive and adapts communication to suit individuals involved can prepare written information/instruction for patient, staff and others
Assessment criteria(applied in relation to performance criteria above)
Self-Eval
½way
Final
Outstanding–Consistently selects and uses communication strategies effectively, adapting communication to individual situations, including some complex and unpredictable circumstances. Excellent –Consistently selects and uses effective communication strategies, adapting communication to individual patient’s needs. Very good –Effective verbal communication. Uses appropriate non verbal communication. Written information is clear and well-presented. Student requires minimal prompting with communication skills. Good – Verbal communication is good. Uses appropriate non-verbal communication with some prompting. Written information/instruction for patient, staff and others is appropriate. Satisfactory – Verbal communication is satisfactory but needs prompting to adapt communication in most situations. Requires prompting to use appropriate non-verbal communication. Written information/instruction for patient, staff and others is satisfactory in most situations.Fail – Verbal and non-verbal communication is poor or inappropriate. Unacceptable written information/instruction for patient/staff and others. Cannot adapt communication to suit individuals involved. Insufficient improvement despite feedback, leading to unsatisfactory professional conduct (see Part 2).
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
87

Practice Education
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
88

Practice Education
2. Contribute effectively to work undertaken as part of a team
Performance criteria integrates into and interacts in the day to day routine of the unit. identifies other team members and recognises their role. recognises own role, and its limitations, as a member of the team. adapts own practice to the requirements/procedures of the team. respects and values the skills, opinions and beliefs of other team members. develops effective working relationships with other team members. shows ability to respond to different personalities within the team. makes a meaningful contribution to the team through participating in e.g. discussions,
team/case meetings, joint documentation
Assessment criteria(applied in relation to performance criteria above)
Self-Eval
½way
Final
Outstanding –Readily integrates into the team, demonstrating an excellent level of awareness and acceptance of their own role and those of others. Makes an effective contribution to the team. Excellent –Readily integrates into the team, demonstrating a high level of awareness and acceptance of their own role and those of others. Readily contributes to the team without prompting. Very good – Integrates into the team, demonstrating an appropriate level of awareness and respect for their own role and those of others. Makes a contribution to the team with minimal prompting Good – Integrates into the team, demonstrating an appropriate level of awareness of their role and the roles of others. Contributes to the team with occasional prompting.Satisfactory – Integrates into the team with prompting. Demonstrates limited awareness of the individual roles within the team. Requires prompting to contribute to the team.Fail – Demonstrates very limited awareness of the purpose of the team, and the individual roles within the team. Contribution to the team is poor or inappropriate. Insufficient improvement despite feedback.
89

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
90

Practice Education
MANAGEMENT OF SELF3. Demonstrate ability in effective self-management of workload
Performance criteria Plans own working day, as applicable. Shows ability to prioritise workload. Recognises need to modify workload in response to changes in working environment
Assessment criteria(applied in relation to performance criteria above)
Self-Eval
½way
Final
Outstanding – Effectively plans, prioritises and modifies their own workload independently in all situations, including some complex and unpredictable circumstancesExcellent – Effectively plans, prioritises and modifies their own workload independently Very good – Plans, prioritises and modifies their own workload with minimal prompting Good – Plans, prioritises and modifies their own workload with some promptingSatisfactory – Plans their own workload but requires support to prioritise and modify. Fail – Planning, prioritising and modification of their workload is poor or inappropriate. Insufficient improvement despite regular feedback
91

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
92

Practice Education
4. Awareness of limits of own practice and when to seek advice
Performance criteria identifies their own strengths and weaknesses. recognises the limitations of their own clinical practice. seeks advice, as necessary.
Assessment criteria(applied in relation to performance criteria above)
Self-Eval
½way
Final
Outstanding – Shows an exceptional awareness of the limits of their own practice including some complex and unpredictable circumstances. Independently identifies their own strengths and weaknesses. Seeks advice at the appropriate time.Excellent - Aware of own limitations. Able to identify strengths and weaknesses without prompting. Seeks advice at the appropriate time.Very good – Aware of own limitations. Able to identify strengths and weaknesses with minimal guidance. Mostly seeks advice at the appropriate time.Good – Has an awareness of own limitations and is able to identify strengths and weaknesses with guidance. Seeks advice but not always at the appropriate time.Satisfactory Has some awareness of own limitations with guidance. Able to identify strengths and weaknesses only with prompting. Seeks advice but not always at the appropriate time.Fail – unaware of own limitations. Unable to identify strengths and weaknesses despite regular feedback. Fails to seek advice when required , leading to unsafe practice (see Part 2)
93

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
94

Practice Education
5. Independently manage own learning
Performance criteria develops, negotiates and uses a learning contract/development plan. takes responsibility for own learning and initiates ways to facilitate own learning. responds positively to constructive feedback. uses reflection as an aid to personal and professional development. actively seeks guidance and feedback to assist own development.
Assessment criteria(applied in relation to performance criteria above)
Self-eval
½way
Final
Outstanding- Takes responsibility for own learning and independently suggests ways to further their own development. Responds appropriately to constructive feedback. Excellent - Reflects on their experiences to assist own development. Responds appropriately to constructive feedback. Negotiates, develops and uses the learning contract. Actively seeks and uses guidance to assist their learning.Very good -Reflects on their experiences to assist own development. Responds appropriately to constructive feedback. Develops and uses the learning contract without prompting. Actively seeks guidance to assist their learning most of the time.Good- Reflects on their experiences to assist own development. Responds appropriately to constructive feedback. Uses the learning contract with some prompting.Satisfactory – Reflects on their experiences to assist own development only with prompting. Responds appropriately to constructive feedback most of the time. Needs prompting to use learning contract.Fail- Fails to take responsibility for own learning. Responds inappropriately to constructive feedback. Does not use learning contract/LDP despite regular feedback.
95

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
96

Practice Education
MANAGEMENT OF PATIENT 6. Gather appropriate information relating to patient
Performance criteria offer a clear explanation of process to patient throughout and gain consent. extract relevant information from a range of sources. uses appropriate and selective questioning to gather relevant information. uses logical and systematic questioning. identifies patient’s perceptions of their needs. considers patient’s psychosocial, cultural and religious issues.
Assessment criteria(applied in relation to performance criteria above)
Self-eval
½way
Final
Outstanding- Uses effective questioning in a logical and sequential manner to gather relevant information from a range of sources. Matches questioning to consider the patient’s psychosocial, cultural and religious needs and takes account of the patient’s perceptions of their needs. Gives appropriate explanation of the assessment process to the patient to gain consentExcellent - Uses appropriate and selective questioning in a logical and sequential manner to gather relevant information from a range of sources. Matches questioning to patient’s needs and takes account of the patient’s perceptions of their needs. Gives appropriate explanation of the assessment process to the patient to gain consentVery good- Uses appropriate and selective questioning, to gather relevant information. Matches questioning to patient’s needs and takes account of the patient’s perceptions of their needs with occasional prompting. Gives appropriate explanation of the assessment process to the patient to gain consentGood- Uses appropriate and selective questioning to gather relevant information with some prompting. Matches questioning to patient’s needs with some prompting. Gives appropriate explanation of the assessment process to the patient to gain consent. Satisfactory-Uses appropriate and selective questioning to gather relevant information only with prompting. Needs prompting to match questioning to patient’s needs. Gives basic explanation of the assessment process to the patient to gain consent. Fail- Unable to gather appropriate information relating to the patient despite regular feedback. Inadequate explanation to patient and failure to gain consent which has led to unsafe practice (see Part 2)
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
97
Practice Education
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
98

Practice Education
7. Plan and carry out an appropriate objective examination
Performance criteria uses information gathered from the subjective examination to plan the objective
examination. selects and effectively performs appropriate assessment techniques. recognises potential adverse effects of any procedure used. completes examination within an appropriate time. reasons through all actions/decisions used in the examination.
Assessment criteria(applied in relation to performance criteria above)
Self-eval
½way
Final
Outstanding- Consistently uses the subjective information gained to select and effectively perform an appropriate objective assessment within a relevant/agreed time. Consistently justifies all actions and recognises potential adverse events. Excellent - Uses the subjective information gained to select and effectively perform an appropriate objective assessment within a relevant/agreed time. Justifies the majority of actions and recognises potential adverse events in most circumstances.Very good- Uses the subjective information gained to select and effectively perform an appropriate objective assessment within a relevant/agreed time. In most circumstances justifies the majority of actions with minimal prompting and recognises many potential adverse events.Good- Requires minimal guidance to use the subjective information gained to select and perform an appropriate objective assessment within a relevant/agreed time. Attempts to justify actions. Recognises potential adverse events in most circumstances with prompting. Satisfactory –Requires guidance to uses the subjective information gained to select and effectively perform an appropriate objective assessment within a relevant/agreed time. Not always able to justify actions .Needs prompting to recognise any potential adverse events.Fail- Does not use the subjective information gained to guide objective assessment. Unable to perform an appropriate objective assessment within a relevant/agreed time. Unable to justify actions to recognise any potential adverse events despite regular feedback, which has led to unsafe practice (see Part 2).
99

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
100

Practice Education
8. Analyse examination findings and formulate a written treatment plan in partnership with the patient
Performance criteria identifies key abnormal findings. set specific, measurable, appropriate, realistic, and timed (SMART) goals in partnership with
the patient (whenever possible.) demonstrates evidence of clinical reasoning and critically evaluating treatment options from a
variety of sources in order to plan treatment. selects appropriate treatment techniques. treatment plan demonstrates due consideration of patient’s needs within their social context
and reflect cultural and religious beliefs. identifies appropriate outcome measures.
Assessment criteria(applied in relation to performance criteria above)
Self eval
½way
Final
Outstanding – Consistently and independently identifies key findings to set specific, measurable, appropriate, realistic and timed goals in partnership with the patient. Treatment plan indicates consideration of the wider context of the patient’s needs. Independently critically evaluates evidence to inform treatment plan. Excellent- Consistently identifies key findings to set goals in partnership with the patient. Evaluates evidence to inform treatment plan.Very good-Identifies key findings to set goals in partnership with the patient with occasional prompting . Able to use evidence to inform treatment plan.Good- Identifies key findings to set goals in partnership with the patient with some prompting. Needs some prompting to use evidence to inform treatment plan.Satisfactory- Identifies key findings to set goals in partnership with the patient only with prompting. Able to use evidence to inform treatment plan with prompting.Fail- Unable to- identify key findings to set goals in partnership with the patient. Unable to use evidence to inform treatment plan despite regular feedback.
101

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
102

Practice Education
9. Implement and critically evaluate impact of, or response to, treatment intervention
Performance criteria implements all interventions according to treatment plan. applies techniques safely and effectively. adapts treatment within a treatment session to meet patient’s needs. evaluates treatment plan to ensure effectiveness. recognises when to discontinue treatment and discharge patients appropriately.
Assessment criteria(applied in relation to performance criteria above)
Self-eval
½way
Final
Outstanding – Consistently and independently applies the planned interventions safely and effectively to meet the patient’s needs. Critically evaluates the treatment to ensure clinical effectiveness and adapts readily to unpredictable circumstances. Recognises when to discontinue treatment and discharge appropriately. Excellent –Applies the planned interventions safely and effectively to meet the patient’s needs. Critically evaluates and adapts the treatment to ensure clinical effectiveness. Recognises when to discontinue treatment and discharge appropriately.Very good – Applies the planned interventions safely and effectively to meet the patient’s needs. Evaluates and adapts the treatment to ensure clinical effectiveness. Recognises when to discontinue treatment and discharge appropriately with occasional prompting.Good -Applies the planned interventions safely and effectively. Evaluates and adapts the treatment to ensure clinical effectiveness most of the time. Recognises when to discontinue treatment and discharge appropriately with some prompting.Satisfactory- Applies planned interventions safely and effectively only with prompting. Needs prompting to evaluate and adapt treatment to ensure effectiveness. Recognises when to discontinue treatment and discharge patient only with prompting. Fail- Unable to apply planned interventions safely and effectively. Does not adapt treatment to ensure effectiveness. Fails to recognize when to discontinue treatment. Despite regular feedback, which has led to unsafe practice (see Part 2).
103

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
104

Practice Education
DOCUMENTATION10. Maintain accurate patient records
Performance criteria accurately records patient database obtained from patient details and examination findings.
accurately records identified patient problems/needs and treatment plans. accurately records progress notes and treatment summaries. completes all patient records by the end of the working day. maintains concise, legible, logical and dated patient records, signed by both student and
educator. adheres to local policies and procedures-including use of locally agreed
abbreviations/glossary.
Assessment criteria(applied in relation to performance criteria above)
Self-eval
½way
Final
Outstanding- Independently documents concise, logical and accurate patient records using POMR Always adheres to local policies and procedures. Always completes records by the end of each working day and ensures all records are signed and countersigned. Excellent- Documents concise, logical and accurate patient records using POMR. Adheres to local policies and procedures. Always completes records by the end of each working day and ensures all records are signed and countersigned.Very good - Documents accurate patient records using POMR. Always completes records by the end of each working day and ensures all records are signed and countersigned.Good – Documents accurate patient records using POMR, occasionally lacking in detail. Always completes records by the end of each working day and ensures all records are signed and countersigned.Satisfactory - Documents patient records using POMR but may lacks detail. Always completes records by the end of each working day and ensures all records are signed and countersigned. Fail - Fails to correctly document patient information despite regular feedback,. Fails to complete documentation by the end of the working day despite regular feedback. Fails to comply with local policies and procedures, which has led to unsafe practice (see Part 2).
105

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
106

Practice Education
PART 2
FAILURE OF EITHER SECTION IN PART 2 WILL NORMALLY
OVERRIDE PART 1 OF THE ASSESSMENT AND CAUSE THE
STUDENT TO FAIL THE PLACEMENT.
SAFETY
Fail: Consistently fails to apply knowledge of departmental health and safety policy to specific
patient groups/conditions (e.g. Infection control, moving and handling policy, operation of medical devices).
Is unaware of, or disregards the contraindications of treatment.
Persistently applies treatment techniques and handling skills in a way that puts patient and/or self at risk.
Is unreliable in reporting and consistently fails to inform the educator about adverse findings and/or patient complaints.
Demonstrates consistently inappropriate verbal, non-verbal or written communication.
Persists in unsafe practice despite verbal instruction and / or warnings.
PROFESSIONAL BEHAVIOUR
STUDENT MEMBERS OF THE CHARTERED SOCIETY OF
PHYSIOTHERAPY ARE SUBJECT TO THE RULES OF PROFESSIONAL
CONDUCT.
ALL STUDENTS MUST COMPLY WITH THE HPC STANDARDS FOR
CONDUCT, PERFORMANCE AND ETHICS
Fail: Fails to comply with, and has inadequate knowledge of, the rules of professional conduct.
Persistently poor punctuality and time keeping.
Fails to implement arrangements and agreed procedures.
Does not respect patient confidentiality.
Poor or inappropriate standards of dress and /or hygiene in relation to departmental policy.
Exploits the mutual trust and respect inherent within a therapeutic relationship.
Persists in unprofessional behaviour despite verbal instructions and / or warnings.
Student members of the Chartered Society of Physiotherapy are subject to the Rules of Professional Conduct.
107

Practice Education
SAFETY - Record of warnings given:Any entries must be dated and signed by both the student and clinical educator. The
visiting tutor must be notified by telephone or email of any warnings given.
VE R BAL W AR NIN G:
Reason for verbal warning
Action Taken:
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
W R ITTE N W AR NI NG:
Reason for written warning
Action Taken:
108

Practice Education
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
Outcome Safety(PLEASE PLACE A CROSS IN THE APPROPRIATE BOX): IF THE OUTCOME IS A FAIL
FOR THE PLACEMENT, THE VISITING TUTOR MUST BE PRESENT TO SUPPORT THE
STUDENT AND CLINICAL EDUCATOR AND CHECK THAT THE PROCESS IS CARRIED
OUT FAIRLY
Pass Fail
109

Practice Education
CO MM E NTS :
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
PROFESSIONALISM - Record of warnings given:Any entries must be dated and signed by both the student and clinical educator. The
visiting tutor must be notified by telephone or email of any warnings given.
110

Practice Education
VE R BAL W AR NIN G:
Reason for verbal warning
Action Taken:
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
W R ITTE N W AR NI NG:
Reason for written warning:
Action Taken:
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
111

Practice Education
Outcome- professional behaviour (PLEASE PLACE A CROSS IN THE APPROPRIATE BOX): IF THE OUTCOME IS A FAIL
FOR THE PLACEMENT, THE VISITING TUTOR MUST BE PRESENT TO SUPPORT THE
STUDENT AND CLINICAL EDUCATOR AND CHECK THAT THE PROCESS IS CARRIED
OUT FAIRLY
Pass FailCO MM E NTS :
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
112

Practice Education
FINAL PLACEMENT COMMENTS
Clinical Educator’s Comments
Signature (Educator)…………………………… Date: …………………………….I confirm that I have received feedback from this placement and have had the opportunity to discuss it with my placement educatorSignature (Student)…………………………… Date: ……………………………….Student’s comments
Signature (Student)…………………………… Date: …………………………….I confirm that I have received feedback from this placement and have had the opportunity to discuss it with the studentSignature (Educator)…………………………… Date: ……………………………….
113

Practice Education
RECORD OF CLINICAL HOURS COMPLETED and ABSENCESDate Hours
completedDates of absence and reasons for absence
WEEK 1 / / WEEK 2 / / WEEK 3 / / WEEK 4 / / WEEK 5 / /FINAL TOTAL TOTAL ABSENCE
I confirm that this is an accurate record of the hours completed by the student
Placement Educator Name ……………………………………………..Signature …………………………………………..
Student Name ……………………………………………..Students should aim to achieve a minimum of 36 hours per working week (180 hours per 5 week practice placement) to ensure achieving the 1,000 clinical hours required for graduation from the BSc (Hons) Physiotherapy programme, eligibility for registration as a physiotherapist with the Health Professions Council and eligibility for membership of the Chartered Society of Physiotherapy.
STUDENTS WHO ANTICIPATE A POTENTIAL SHORTFALL IN
PRACTICE PLACEMENT HOURS ARE ADVISED TO DISCUSS THIS AS
SOON AS POSSIBLE WITH JO NICHOLSON OR SOPHIE TAYLOR.
114

Practice Education
Appendix 4: Example Common Assessment Tool Level 6 MSc Pre-registration
PHYSIOTHERAPYPRACTICE PLACEMENT ASSESSMENT
LEVEL 6(H)
STUDENT NAME
YEAR OF STUDY
DATES OF PLACEMENT
PLACEMENT NUMBER
PLACEMENT SITE
PLACEMENT AREA/TYPE OF PLACEMENT
PLACEMENT EDUCATOR
VISITING TUTOR
FOR UNIVERSITY USE ONLY
MARK AWARDED %
Contact HOURS
115

Practice Education
Submission of practice placement bookletsPractice placement booklets should be submitted to the Student Life Office according to their document ‘Coursework submission guidance’ available from the internet at <http://www.did.stu.mmu.ac.uk/studentinfo/other_information.php>
Practice Placement 2– Unit code 28050006 Unit leaders J hindle
Placement booklet submission ************2009 4.00pm
Health & Safety Declaration
I certify that I have read the Health & Safety Policies of the appropriate clinical area/s noting particularly the procedure in the event of fire and cardiac arrest, local policies for Moving and Handling of loads and any other specific procedure limitations.
THIS MUST BE COMPLETED BY THE END OF THE FIRST WEEK OF
PLACEMENT AS PART OF THE PLACEMENT INDUCTION PROCESS.
Signature of student Date
116

Practice Education
INFORMATION ABOUT THE FORMThe assessment of the student performance is divided into two parts.Part 1 comprises ten aspects of practice that will contribute to the overall assessment of the student’s performance. These are based on the Standards of Proficiency (SoP) of the Health Professions Council and play a central role in admission to the Register. They are also linked to the KSF Dimensions (Core 1-6, and HWB 6 & 7). They have been grouped into four areas:
INTERPERSONAL SKILLS (SoP 1b) (KSF dimensions C1, C2, C6)The student will:9 Demonstrate effective and appropriate skills in communication
10 Contribute effectively to work undertaken as part of a team
MANAGEMENT OF SELF (SoP 1a & SoP 3) (KSF dimensions C2, C4, C5)The student will:11 Demonstrate effective self-management of workload
12 Know the limits of their own practice and when to seek advice
13 Independently manage their own learning
MANAGEMENT OF PATIENT (SoP 2a, 2b, 2c & SoP 3) (KSF dimensions C1, C3, C4, C6, HWB6, HWB7)The student will:14 Gather appropriate information relating to patient
15 Plan and carry out an appropriate objective examination
16 Analyse examination findings and formulate a written treatment plan in partnership with the patient
9 Implement and critically evaluate impact of, or response to, treatment interventions
DOCUMENTATION (SoP 2b) (KSF dimensions C1, C3, C5, HWB6)The student will:10 Maintain accurate patient records.
117

Practice Education
HOW TO COMPLETE THE PLACEMENT ASSESSMENT DOCUMENT – PART 1Clinical Placement marks contribute to a student’s final degree classification. It is therefore very important that you are objective when completing this document. Please follow the guidance below when assessing the students.
For each aspect of practice within Part 1: Read the performance criteria and ensure that you consider ALL points before
referring to the assessment criteria
Read the assessment criteria thoroughly, referring to the glossary of terms on page 8
In order to mark a student in a particular box, all aspects of the assessment criteria within that box must be met
Please consider ALL levels of assessment criteria for all students. Students should be able to achieve any grade for the placement if their performance objectively meets the assessment criteria for that grade. This is applicable to all placements.
At midway: Ensure that the student has completed their self evaluation using the
assessment criteria, and also completed their midway comments
Complete your midway assessment of the student using the assessment criteria and complete your feedback, linking your comments to the performance criteria
Good practice would be to discuss the midway assessment and comments with the visiting tutor before discussing with the student. Ideally the sharing of the document with the student at this point should be a tripartite meeting, of clinical educator, student and tutor. However, this may vary between Universities since we all have different visiting practices.
Set and document an action plan for each aspect of practice in negotiation with the student, to demonstrate areas for development during the second half of the placement. This may be done at the tripartite meeting
Please be aware that students failing any of the following aspects of practice (1, 3, 4, 6, 7, 9, 10) at midway should be referred to Part 2 of the document and given appropriate warnings. An action plan should be formulated.
118

Practice Education
At the final assessment: Complete your final assessment of the student using the assessment criteria
and complete your feedback, linking your comments to the performance criteria
Your grading of the student should be based on the student’s performance in the final week of their placement
Good practice would be to discuss the final placement marks with the visiting tutor before being given to the student, in order for the University to moderate between different educators. The timing of this may vary between Universities since we all have different visiting practices.
Ensure that your cross is within a box not on the line between two boxes
Please cross a box in every aspect of practice. Please seek guidance from the visiting tutor if you are unsure how any particular aspect can be applied to your placement setting
Please be aware that students failing any of the following aspects of practice (1, 3, 4, 6, 7, 9, 10) will automatically fail the placement for unsafe/unprofessional behaviour, and this should be documented in Part 2. Please see the note below regarding notification of poor performance.
IF YOU CONSIDER THAT YOUR STUDENT IS LIKELY TO FAIL ANY
SECTION OF PART 1 OF THE DOCUMENT AT ANY POINT IN THE
PLACEMENT, THE STUDENT AND THE VISITING TUTOR SHOULD BE
MADE AWARE OF THIS AT THE EARLIEST OPPORTUNITY IN ORDER
TO ALLOW MAXIMUM TIME FOR THE STUDENT TO IMPROVE
THEIR PERFORMANCE TO AN ACCEPTABLE LEVEL AND RECEIVE
APPROPRIATE SUPPORT FROM THE UNIVERSITY.
119

Practice Education
HOW TO COMPLETE THE PLACEMENT ASSESSMENT DOCUMENT – PART 2If you are concerned about the student’s safety and/or professional behaviour at any time during the placement you should refer to Part 2 of the Assessment document. Please follow the guidance below when completing this section of the form:
Read the fail descriptors within the relevant section(s) of Part 2
Students should be given a verbal warning regarding any unsafe practice and/or unprofessional behaviour at the time of the incident, in the first instance. This should then be documented in Part 2, and signed and dated by the clinical educator and the student, and if appropriate the visiting tutor
Repeated poor practice and/or behaviour warrant a written warning using the relevant section(s) of Part 2, which should be signed and dated by the clinical educator and the student. The visiting tutor must be informed at this stage
Repeated poor practice and/or behaviour may be the same or different aspects of practice (e.g. repeated poor time management, or a range of errors relating to unsafe practice)
An action plan should be formulated and documented in order to maximise the student’s ability to reach an acceptable standard of performance
At the end of the placement (or earlier if appropriate) the outcome section should be completed with appropriate comments relating to the outcome of the action plan. Examples are given below to assist with this
o If the action plan has been complied with and there have been no further incidents of unsafe practice and/or unprofessional behaviour then the student should pass the placement.
o If there have been further incidents of unsafe practice and/or unprofessional behaviour this should be documented in the comment section as the reason for the student failing the placement.
o The decision as to whether a student should pass or fail therefore depends on the number of incidents, and a student should not fail on one incident alone.
o A clear identification of whether the student has passed or failed must be given by placing a cross in the appropriate box.
PLEASE DO NOT DELAY DISCUSSING POOR PERFORMANCE WITH
THE STUDENT IN THE HOPE THAT THEY WILL IMPROVE AS THIS
REDUCES THE TIME THAT IS AVAILABLE FOR THEM TO REACH AN
ACCEPTABLE LEVEL
Please note that repeated incidents of unsafe practice and/or professional behaviour leading to more than 1 written warning could result in the student being removed from the placement at any stage – i.e. the decision to fail may not only happen at the end of the placement.
120

Practice Education
GLOSSARY of terms
Prompting Used to describe a situation where the clinical educator
provides input to the student by the use of a key word, indirect
or open questioning to facilitate learning
Professionalism
Used to describe the attitudes and manner of the physiotherapy
student and does not take into account issues around safety,
work environment or the application of skills.
Consistently Used to describe a situation where a student meets the
requirements of the criteria >90% of the time.
Most … Used to describe a situation where a student meets the
requirements of the criteria >60% but <90% of the time.
Some … Used to describe a situation where a student meets the
requirements of the criteria >30% but <60% of the time.
Occasional… Used to describe a situation where a student meets the
requirements of the criteria <30% of the time.
Complex and unpredictable
Events which would not normally occur within the normal day-
to-day running of a unit, or which would provide particular
challenge to the student
121
Practice Education
PART 1 - INTERPERSONAL SKILLS1. Effective and appropriate skills in communication
Performance criteria initiates communication and actively seeks participation and collaboration
when interacting with patients, staff and others. chooses appropriate communication strategies when interacting with
patients, staff and others. uses appropriate language and body language when interacting with patients,
staff and others. shows ability in listening skills. shows ability in questioning skills. deals with questions appropriately, considering own level of knowledge and
understanding, own level of authority/responsibility is responsive and adapts communication to suit individuals involved can prepare written information/instruction for patient, staff and others
Assessment criteria(applied in relation to performance criteria above)
Self-Eval
½ way
Final
Outstanding–Consistently selects and uses all communication strategies effectively, adapting communication to individual situations, including complex and unpredictable circumstances. Excellent –Consistently selects and uses effective communication strategies, adapting communication to individual patient’s needs, including some complex and unpredictable circumstances. Very good –Effective verbal communication. Uses appropriate non-verbal communication. Written information is clear and well presented. No prompting is required with communication skills. Good – Verbal communication is good. Uses appropriate non-verbal communication with occasional prompting. Written information/instruction for patient, staff and others is appropriate. Satisfactory – Verbal communication is satisfactory but needs prompting to adapt communication in some situations. Requires prompting to use appropriate non-verbal communication. Written information/instruction for patient, staff and others is satisfactory in most situations.Fail – Verbal and non-verbal communication is very poor or inappropriate. Unacceptable written information/instruction for patient/staff and others. Unable to adapt communication to suit individuals involved. Insufficient improvement despite feedback, which has led to unsatisfactory professional conduct(see Part 2).
122

Practice Education
1. Effective and appropriate skills in communication
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
123

Practice Education
2. Contribute effectively to work undertaken as part of a team
Performance criteria integrates into and interacts in the day to day routine of the unit. identifies other team members and recognises their role. recognises own role, and its limitations, as a member of the team. adapts own practice to the requirements/procedures of the team. respects and values the skills, opinions and beliefs of other team members. develops effective working relationships with other team members. shows ability to respond to different personalities within the team. makes a meaningful contribution to the team through participating in e.g. discussions,
team/case meetings, joint documentation
Assessment criteria(applied in relation to performance criteria above)
Self-Eval
½ way
Final
Outstanding –Readily integrates into the team, demonstrating an outstanding level of awareness and acceptance of their-own role and those of others. Makes an exceptional contribution to the team. Excellent –Readily integrates into the team, demonstrating a high level of awareness and acceptance of their-own role and those of others. Makes an effective contribution to the team. Very good – Integrates into the team, demonstrating an appropriate level of awareness and respect for their own role and those of others. Makes a contribution to the team without prompting. Good – Integrates into the team, demonstrating an appropriate level of awareness of their role and the roles of others. Contributes to the team with occasional prompting.Satisfactory – Integrates into the team with prompting. Demonstrates limited awareness of the individual roles within the team. Requires prompting to contribute to the team.Fail – Demonstrates very limited awareness of the purpose of the team and the individual roles within the team. Contribution to the team is poor or inappropriate. Insufficient improvement despite feedback.
124

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
125
Practice Education
MANAGEMENT OF SELF3. Demonstrate ability in effective self-management of workload
Performance criteria Plans own working day, as applicable. Shows ability to prioritise workload. Recognises need to modify workload in response to changes in working environment
Assessment criteria(applied in relation to performance criteria above)
Self-Eval
½ way
Final
Outstanding – Effectively plans, prioritises and modifies own workload independently in all situations, including complex and unpredictable circumstancesExcellent – Effectively plans, prioritises and modifies own workload independently, including some complex and unpredictable circumstances. Very good – Plans, prioritises and modifies own workload independentlyGood – Plans, prioritises and modifies own workload with minimal prompting.Satisfactory – Plans own workload but requires support to prioritise and modify. Fail – Planning, prioritising and modification of their workload is very poor or inappropriate. Insufficient improvement despite regular feedback which has led to unsafe practice (see Part 2)
126

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
127

Practice Education
4. Awareness of limits of own practice and when to seek advice
Performance criteria identifies their own strengths and weaknesses. recognises the limitations of their own clinical practice. seeks advice, as necessary.
Assessment criteria(applied in relation to performance criteria above)
Self-Eval
½way
Final
Outstanding – Shows an exceptional awareness of the limits of their own practice within the wider healthcare setting including complex and unpredictable circumstances. Independently identifies their own strengths and weaknesses. Seeks advice at the appropriate time.Excellent - Aware of own limitations. Independently identifies their own strengths and weaknesses. Seeks advice at the appropriate time.Very good – Aware of own limitations. Able to identify strengths and weaknesses without prompting. Mostly seeks advice at the appropriate time.Good – Aware of own limitations and is able to identify strengths and weaknesses with occasional prompting. Seeks advice but not always at the appropriate time.Satisfactory- Some awareness of own limitations. Able to identify strengths and weaknesses with prompting. Seeks advice but not always at the appropriate time.Fail – unaware of own limitations. Unable to identify strengths and weaknesses despite regular feedback. Fails to seek advice when required, which has led to unsafe practice (see Part 2)
128

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
129

Practice Education
5. Independently manage own learning
Performance criteria develops, negotiates and uses a learning contract/development plan. takes responsibility for own learning and initiates ways to facilitate own learning. responds positively to constructive feedback. uses reflection as an aid to personal and professional development. actively seeks guidance and feedback to assist own development.
Assessment criteria(applied in relation to performance criteria above)
Self-eval
½way
Final
Outstanding- Takes responsibility for own learning and independently initiates ways to further their own development. Responds appropriately to constructive feedback. Excellent - Reflects on their experiences to assist own development. Responds appropriately to constructive feedback. Negotiates, develops and regularly uses the learning contract. Actively seeks and uses guidance to confirm their learning.Very good -Reflects on their experiences to assist own development. Responds appropriately to constructive feedback. Develops and uses the learning contract without prompting. Actively seeks guidance to assist their learning most of the time.Good- Reflects on their experiences to assist own development. Responds appropriately to constructive feedback. Uses the learning contract with occasional prompting.Satisfactory – Reflects on their experiences to assist own development only with prompting. Responds appropriately to constructive feedback most of the time. Needs prompting to use learning contract.Fail- Fails to take responsibility for their own learning. Responds inappropriately to constructive feedback. Does not use learning contract/LDP despite regular feedback.
130

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
131

Practice Education
MANAGEMENT OF PATIENT6. Gather appropriate information relating to patient
Performance criteria offer a clear explanation of process to patient throughout and gain consent. extract relevant information from a range of sources. uses appropriate and selective questioning to gather relevant information. uses logical and systematic questioning. identifies patient’s perceptions of their needs. considers patient’s psychosocial, cultural and religious issues.
Assessment criteria(applied in relation to performance criteria above)
Self-eval
½ way
Final
Outstanding- Uses highly effective questioning in a logical and sequential manner to gather relevant information from a range of sources. Matches questioning to consider the patient’s psychosocial, cultural and religious needs and takes account of the patient’s perceptions of their needs. Gives appropriate explanation of the assessment process to the patient to gain consentExcellent - Uses effective questioning in a logical and sequential manner to gather relevant information from a range of sources. Matches questioning to patient’s needs and takes account of the patient’s perceptions of their needs. Gives appropriate explanation of the assessment process to the patient to gain consentVery good- Uses appropriate and selective questioning in a logical and sequential manner to gather relevant information. Matches questioning to patient’s needs and takes account of the patient’s perceptions of their needs. Gives appropriate explanation of the assessment process to the patient to gain consentGood- Uses appropriate and selective questioning to gather relevant information with occasional prompting. Matches questioning to patient’s needs with occasional prompting. Gives appropriate explanation of the assessment process to the patient to gain consent. Satisfactory-Uses appropriate and selective questioning to gather relevant information with prompting. Needs occasional prompting to match questioning to patient’s needs. Gives basic explanation of the assessment process to the patient to gain consent. Fail- Unable to gather appropriate information relating to the patient despite regular feedback. Inadequate explanation to patient and failure to gain consent, which has led to unsatisfactory professional conduct and/or unsafe practice (see Part 2).
132

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
133

Practice Education
7. Plan and carry out an appropriate objective examination
Performance criteria uses information gathered from the subjective examination to plan the objective examination. selects and effectively performs appropriate assessment techniques. recognises potential adverse effects of any procedure used. completes examination within an appropriate time. reasons through all actions/decisions used in the examination.
Assessment criteria(applied in relation to performance criteria above)
Self-eval
½way
Final
Outstanding- Consistently uses the subjective information gained to select and effectively perform an appropriate objective assessment within a relevant/agreed time. Consistently justifies all actions and recognises any potential adverse event, including complex and unpredictable circumstances.Excellent - Consistently uses the subjective information gained to select and effectively perform an appropriate objective assessment within a relevant/agreed time. Consistently justifies all actions and recognise any potential adverse events.Very good- Uses the subjective information gained to select and effectively perform an appropriate objective assessment within a relevant/agreed time. Justifies the majority of actions and recognises potential adverse events in most circumstances.Good- Uses the subjective information gained with occasional prompting to select and effectively perform an appropriate objective assessment within a relevant/agreed time. Attempts to justify actions to recognise potential adverse events in most circumstances. Satisfactory –Uses the subjective information gained with prompting to select and effectively perform an appropriate objective assessment within a relevant/agreed time. Needs prompting to justify actions and to recognise any potential adverse events.Fail- Does not use the subjective information gained to guide objective assessment. Unable to perform an appropriate objective assessment within a relevant/agreed time. Unable to justify actions to recognise any potential adverse events despite regular feedback, which has led to unsafe practice (see Part 2).
134

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
135

Practice Education
8. Analyse examination findings and formulate a written treatment plan in partnership with the patient
Performance criteria identifies key abnormal findings. set specific, measurable, appropriate, realistic and timed (SMART) goals in partnership
with the patient whenever possible demonstrates evidence of clinical reasoning and critically evaluating treatment options
from a variety of sources in order to plan treatment. selects appropriate treatment techniques. treatment plan demonstrates due consideration of patient’s needs within their social
context and reflect cultural and religious beliefs. identifies appropriate outcome measures.
Assessment criteria(applied in relation to performance criteria above)
Self eval
½way
Final
Outstanding – Consistently and independently identifies key findings to set specific, measurable, appropriate, realistic and timed goals in partnership with the patient/including complex and challenging situations. Treatment plan indicates consideration of the wider context of the patient’s needs. Independently critically evaluates evidence to inform treatment plan. Excellent- Consistently and independently identifies key findings to set goals in partnership with the patient. Treatment plan indicates consideration of the wider context of the patients needs. Critically evaluates evidence to inform treatment plan.Very good-Identifies key findings to set goals in partnership with the patient. Treatment plan is appropriate to patients needs. Evaluates evidence to inform treatment plan.Good- Identifies key findings to set goals in partnership with the patient with occasional prompting. Uses evidence to inform treatment plan.Satisfactory- Identifies key findings to set goals in partnership with the patient with prompting. Uses evidence to inform treatment plan only with prompting.Fail- Unable to- identify key findings to set goals in partnership with the patient. Unable to use evidence to inform treatment plan despite regular feedback.
136

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
137

Practice Education
9. Implement and critically evaluate impact of, or response to, treatment intervention
Performance criteria implements all interventions according to treatment plan. applies techniques safely and effectively. adapts treatment within a treatment session to meet patient’s needs. evaluates treatment plan to ensure effectiveness.
recognises when to discontinue treatment and discharge patient appropriately.
Assessment criteria(applied in relation to performance criteria above)
Self-eval
½way
Final
Outstanding – Consistently and independently applies the planned interventions safely and effectively to meet the patient’s needs. Independently critically evaluates the treatment to ensure clinical effectiveness and adapts readily to complex and unpredictable circumstances. Recognises when to discontinue treatment and discharge appropriately. Excellent – Independently applies the planned interventions safely and effectively to meet the patient’s needs. Critically evaluates and adapts the treatment to ensure clinical effectiveness. Recognises when to discontinue treatment and discharge appropriately.Very good – Applies the planned interventions safely and effectively to meet the patient’s needs. Evaluates and adapts the treatment to ensure clinical effectiveness. Recognises when to discontinue treatment and discharge appropriately.Good -Applies the planned interventions safely and effectively. Evaluates and adapts the treatment to ensure clinical effectiveness most of the time. Recognises when to discontinue treatment and discharge appropriately with occasional prompting.Satisfactory- Applies planned interventions safely and effectively with prompting. Needs prompting to evaluate and adapt treatment to ensure effectiveness. Recognises when to discontinue treatment and discharge patient with prompting. Fail- Unable to apply planned interventions safely and effectively. Does not adapt treatment to ensure effectiveness. Fails to recognize when to discontinue treatment. Despite regular feedback, which has led to unsafe practice (see Part 2).
138

Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
139

Practice Education
DOCUMENTATION10. Maintain accurate patient records
Performance criteria accurately records patient database obtained from patient details and examination findings.
accurately records identified patient problems/needs and treatment plans. accurately records progress notes and treatment summaries. completes all patient records by the end of the working day. maintains concise, legible, logical and dated patient records, signed by both student and educator. adheres to local policies and procedures-including use of locally agreed abbreviations/glossary.
Assessment criteria(applied in relation to performance criteria above)
Self-eval
½way
Final
Outstanding- Independently documents concise, logical and accurate patient records using POMR Always adheres to local policies and procedures. Always completes records by the end of each working day and ensures all records are signed and countersigned. Excellent- Documents concise, logical and accurate patient records using POMR. Adheres to local policies and procedures. Always completes records by the end of each working day and ensures all records are signed and countersigned.Very good - Documents concise and accurate patient records using POMR. Always completes records by the end of each working day and ensures all records are signed and countersigned.Good – Documents accurate patient records using POMR, occasionally lacking in detail. Always completes records by the end of each working day and ensures all records are signed and countersigned.Satisfactory - Documents patient records using POMR but may lack detail. Always completes records by the end of each working day and ensures all records are signed and countersigned. Fail - Fails to correctly document patient information despite regular feedback,. Fails to complete documentation by the end of the working day despite regular feedback. Fails to comply with local policies and procedures, which has led to unsafe practice (see Part 2)
140
Practice Education
Clinical Educator - Half way comments (these should reflect the student’s progress to date)
Student - Half way comments (these should reflect your progress to date)
Action Plan
Clinical Educator - Final comments (reflecting students performance in final week of placement)
Student – final comments (reflecting your performance in final week of placement)
141

Practice Education
PART 2
FAILURE OF EITHER SECTION IN PART 2 WILL NORMALLY
OVERRIDE PART 1 OF THE ASSESSMENT AND CAUSE THE
STUDENT TO FAIL THE PLACEMENT.
SAFETY
Fail: Consistently fails to apply knowledge of departmental health and safety policy to specific
patient groups/conditions (e.g. Infection control, moving and handling policy, operation of medical devices).
Is unaware of, or disregards the contraindications of treatment.
Persistently applies treatment techniques and handling skills in a way that puts patient and/or self at risk.
Is unreliable in reporting and consistently fails to inform the educator about adverse findings and/or patient complaints.
Demonstrates consistently inappropriate verbal, non-verbal or written communication.
Persists in unsafe practice despite verbal instruction and / or warnings.
PROFESSIONAL BEHAVIOUR
STUDENT MEMBERS OF THE CHARTERED SOCIETY OF
PHYSIOTHERAPY ARE SUBJECT TO THE RULES OF PROFESSIONAL
CONDUCT.
ALL STUDENTS MUST COMPLY WITH THE HPC STANDARDS FOR
CONDUCT, PERFORMANCE AND ETHICS
Fail: Fails to comply with, and has inadequate knowledge of, the rules of professional conduct.
Persistently poor punctuality and time keeping.
Fails to implement arrangements and agreed procedures.
Does not respect patient confidentiality.
Poor or inappropriate standards of dress and /or hygiene in relation to departmental policy.
Exploits the mutual trust and respect inherent within a therapeutic relationship.
Persists in unprofessional behaviour despite verbal instructions and / or warnings.
Student members of the Chartered Society of Physiotherapy are subject to the Rules of Professional Conduct.
142

Practice Education
SAFETY - Record of warnings given:Any entries must be dated and signed by both the student and clinical educator. The
visiting tutor must be notified by telephone or email of any warnings given.
VE R BAL W AR NIN G:
Reason for verbal warning
Action Taken:
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
W R ITTE N W AR NI NG:
Reason for written warning:
143

Practice Education
Action Taken:
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
O UTC O ME
(PLEASE PLACE A CROSS IN THE APPROPRIATE BOX): IF THE OUTCOME IS A FAIL
FOR THE PLACEMENT, THE VISITING TUTOR MUST BE PRESENT TO SUPPORT THE
STUDENT AND CLINICAL EDUCATOR AND CHECK THAT THE PROCESS IS CARRIED
OUT FAIRLY
Pass Fail
144

Practice Education
CO MM E NTS :
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
145

Practice Education
146

Practice Education
PROFESSIONALISM - Record of warnings given:Any entries must be dated and signed by both the student and clinical educator. The
visiting tutor must be notified by telephone or email of any warnings given.
VE R BAL W AR NIN G:
Reason for verbal warning
Action Taken:
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
W R ITTE N W AR NI NG:
Reason for written warning:
147

Practice Education
Action Taken:
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
O UTC O ME
(PLEASE PLACE A CROSS IN THE APPROPRIATE BOX): IF THE OUTCOME IS A FAIL
FOR THE PLACEMENT, THE VISITING TUTOR MUST BE PRESENT TO SUPPORT THE
STUDENT AND CLINICAL EDUCATOR AND CHECK THAT THE PROCESS IS CARRIED
OUT FAIRLY
Pass Fail
148

Practice Education
CO MM E NTS :
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
149

Practice Education
FINAL PLACEMENT COMMENTS
Clinical Educator’s Comments
Signature (Educator)…………………………… Date: …………………………….I confirm that I have received feedback from this placement and have had the opportunity to discuss it with my placement educatorSignature (Student)…………………………… Date: ……………………………….Student’s comments
Signature (Student)…………………………… Date: …………………………….I confirm that I have received feedback from this placement and have had the opportunity to discuss it with the studentSignature (Educator)…………………………… Date: ……………………………….
150

Practice Education
RECORD OF CLINICAL HOURS COMPLETED and ABSENCESDate Hours
completedDates of absence and reasons for absence
WEEK 1 / / WEEK 2 / / WEEK 3 / / WEEK 4 / / WEEK 5 / /FINAL TOTAL TOTAL ABSENCE
I confirm that this is an accurate record of the hours completed by the student
Placement Educator Name ……………………………………………..Signature …………………………………………..
Student Name ……………………………………………..Students should aim to achieve a minimum of 37 hours per working week (185 hours per practice placement) to ensure achieving the 1,000 clinical hours required for graduation from the MSc Pre reg (Hons) Physiotherapy programme, eligibility for registration as a physiotherapist with the Health Professions Council and eligibility for membership of the Chartered Society of Physiotherapy.
STUDENTS WHO HAVE BEEN INFORMED OF A POTENTIAL
SHORTFALL IN PRACTICE PLACEMENT HOURS ARE ADVISED TO
DISCUSS REQUIREMENTS WITH JACKIE HINDLE
151

Practice Education
Appendix 5a: Elective Placement letter
Faculty of Health, Psychology and Social Care
Department of Health ProfessionsManchester Metropolitan UniversityElizabeth Gaskell CampusHathersage RoadMANCHESTERM13 0JA
Tel/Fax: 44 [0] 161 247 2457Email [email protected]
Date as postmark
Dear Colleague
Re: ELECTIVE PLACEMENT OF 4 WEEKS DURATION
As part of the MSc Physiotherapy (Pre-registration) programme students must complete an elective placement. This placement is organised by the student and approved by the University. The elective placement is a compulsory component of the programme at Manchester Metropolitan University and must be completed to a satisfactory standard. The student completes a placement having demonstrated:
An acceptable level of clinical skills and underpinning knowledge An acceptable level of professional behaviour Safe practice of physiotherapy skills.
We require the supervising clinician to complete the student’s elective assessment form with details of clinical hours completed and any other relevant comments. We also require you to complete a separate written letter on headed notepaper confirming your agreement to this placement. Students MUST complete 125 hours minimum on this placement to satisfy programme and professional requirements. Students will not be allowed to graduate if they have not completed this placement.
Normally students are registered with the Chartered Society of Physiotherapy which confers Professional Liability Insurance. This covers all countries throughout the world except Canada, Australia, New Zealand and USA .The key condition of the policy is that the student is supervised by a qualified physiotherapist. Students that are not registered with the CSP are aware that they must make alternative arrangements.
In addition, I must inform you that the University offers no remuneration for elective placements.
Thank you.
152

Practice Education
Appendix 5b: Elective placement details
Faculty of Health, Psychology and Social CareDepartment of Health Professions
E-mail: [email protected]
ELECTIVE CLINICAL EDUCATION PLACEMENT (TOTAL MINIMUM OF 125 HOURS)
PROPOSED ELECTIVE CLINICAL PLACEMENT
Name of Student………………………………………………………….…………….……
Dates of Placement:………………………………………………………….…………….…
Number of hours per week: …………………………………………………….……………(students need to complete a MINIMUM of 125 hours in total for elective placement)
Name of Supervising Clinician:………………………………………………………….……
Grade of Supervising Clinician:………………………………………………………….……
Physiotherapy Manager:………………………………………………………….……………
Signature of Manager:………………………………………………………….………………
Telephone Number:……………………………………………………………….……………
Name and Full Address of Hospital:……………………………………………………………………….………………………………………………………………………………………
Student Please return this form to the Placement administrator for Physiotherapy - 4 th Floor administration office by ***********r 2009 together with written permission on separate headed paper from the Physiotherapy Manager for the clinical placement . You must submit both the form and the letter for your elective placement to be accepted by the university.
If the elective is in the United Kingdom, the clinician must be registered as a physiotherapist with the Health Professions Council. If the elective is not in the United Kingdom, the clinician must be recognised by the authority of their country of practice as a “Physiotherapist” in order that they may supervise students under the terms of the corporate student insurance scheme operated by the Chartered Society of Physiotherapy and able to provide evidence of such if required (for example, letter on headed note paper or official stamp of organisation).
153

Practice Education
Appendix 5c: Practice Placement Equal Opportunities Checklist
Name of Employer ………………………………………………………..Address ………………………………………………………..
………………………………………………………..………………………………………………………..………………………………………………………..
154

Practice Education
Telephone ……………………………………Fax ……………………………………Email ………………………………………………………..
Please tick as appropriate, adding any relevant details: Yes No
1. Do you have a written Equal Opportunities Policy?
2. Are students made aware of your Equal opportunities policies during induction?
3. Do these policies extend to students onplacements within your organisation?
4. Do you have procedures in place to deal with breaches of Equal Opportunities policies for placement students?
5. Will breaches of Equal Opportunities policies and procedures experienced by the placement students be reported to the University?
6. Where can your policies and procedures regarding Equal Opportunities be accessed?
……………………………………………………………………………………………………………………………………………………………………
Signature ……………………………………….Position ……………………………………….
Please return to: Physiotherapy placement administrator Placement Office4th Floor Tower BlockManchester Metropolitan UniversityElizabeth Gaskell Campus
Hathersage RoadManchester M13 0JA
Appendix 5d Placement Health & Safety Checklist
Name of Employer: ............................................Address: ……………………………….……………………………….……………………………….Telephone: ……………………………….Fax: ……………………………….
155

Practice Education
The Health And Safety Executive
The LocalAuthority
EnvironmentalHealth
Department
1. Is your organisation registered with:
Yes No
2. Do you have a written Health and Safety Policy?
3. Will you provide induction training and any other relevant training and instruction for the placement student?
4. Do you hold Employer and Public Liability Insurance?
5. Are placement students covered by the above or any other insurance?
6. Do you have accident reporting procedures in accordance with RIDDOR?
7. Have you undertaken Risk Assessments of your significant hazards?
8. Will you report to the University any recorded accident or work related sickness experienced by the placement student?
9. Have you any emergency procedures to deal with imminent dangers e.g. fires?
Signed: …………………………………Please return to:
Physiotherapy Placement Administrator Placement OfficeManchester Metropolitan University
4th Floor Tower BlockElizabeth Gaskell Campus
Position: ………………………………… Hathersage Road M13 0JA
156

Practice Education
Appendix 6: Example elective placement assessment booklet (MSc Pre-reg)
ELECTIVE PRACTICE PLACEMENT ASSESSMENT
LEVEL 6(H)
STUDENT NAME
YEAR OF STUDY
157

Practice Education
DATES OF PLACEMENT
PLACEMENT NUMBER
PLACEMENT SITE
PLACEMENT AREA/TYPE OF PLACEMENT
VISITING TUTOR
UNIT CODE
FOR UNIVERSITY USE ONLY
MARK AWARDED %
Contact HOURS
158

Practice Education
Submission of practice placement bookletsPractice placement booklets should be submitted to the Student Life Office according to their document ‘Coursework submission guidance’ available from the internet at <http://www.did.stu.mmu.ac.uk/studentinfo/other_information.php>
Elective Placement– Unit code 28050015 Unit leaders J Hindle
Placement booklet submission
Health & Safety Declaration
I certify that I have read the Health & Safety Policies of the appropriate clinical area/s noting particularly the procedure in the event of fire and cardiac arrest, local policies for Moving and Handling of loads and any other specific procedure limitations.
THIS MUST BE COMPLETED BY THE END OF THE FIRST WEEK OF
PLACEMENT AS PART OF THE PLACEMENT INDUCTION PROCESS.
Signature of student Date
159

Practice Education
Elective placement – safety and professional behaviourFAIL UR E OF E IT H ER S EC TI ON W IL L C AUS E T HE S TUD E NT TO FAI L TH E E L EC TIV E
PLAC E ME NT.
SAFETY
Fail: Consistently fails to apply knowledge of departmental health and safety policy to specific
patient groups/conditions (e.g. Infection control, moving and handling policy, operation of medical devices).
Is unaware of, or disregards the contraindications of treatment.
Persistently applies treatment techniques and handling skills in a way that puts patient and/or self at risk.
Is unreliable in reporting and consistently fails to inform the educator about adverse findings and/or patient complaints.
Demonstrates consistently inappropriate verbal, non-verbal or written communication.
Persists in unsafe practice despite verbal instruction and / or warnings.
PROFESSIONAL BEHAVIOUR ST UD EN T ME MBE R S O F T H E C H AR TE R ED SO C IE TY O F PH YS IO TH E R APY AR E SU BJE C T TO TH E
R ULE S OF PR OF ES S IO NAL C ON DU CT . ALL S TU DE NTS MU ST C O MPL Y W ITH TH E HPC ST AND AR DS FO R CO ND UC T, PE R FO R MAN CE AND ET H ICS
Fail: Fails to comply with, and has inadequate knowledge of, the rules of professional conduct.
Persistently poor punctuality and time keeping.
Fails to implement arrangements and agreed procedures.
Does not respect patient confidentiality.
Poor or inappropriate standards of dress and /or hygiene in relation to departmental policy.
Exploits the mutual trust and respect inherent within a therapeutic relationship.
Persists in unprofessional behaviour despite verbal instructions and / or warnings.
Student members of the Chartered Society of Physiotherapy are subject to the Rules of Professional Conduct.
160

Practice Education
SAFETY - Record of warnings given:Any entries must be dated and signed by both the student and clinical educator. The
visiting tutor must be notified by telephone or email of any warnings given.
VE R BAL W AR NIN G:
Reason for verbal warning
Action Taken:
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
W R ITTE N W AR NI NG:
Reason for written warning:
161

Practice Education
Action Taken:
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
O UTC O ME
(PLEASE PLACE A CROSS IN THE APPROPRIATE BOX): IF THE OUTCOME IS A FAIL
FOR THE PLACEMENT, THE VISITING TUTOR MUST BE PRESENT TO SUPPORT THE
STUDENT AND CLINICAL EDUCATOR AND CHECK THAT THE PROCESS IS CARRIED
OUT FAIRLY
Pass Fail
162

Practice Education
CO MM E NTS :
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
163

Practice Education
PROFESSIONALISM - Record of warnings given:Any entries must be dated and signed by both the student and clinical educator. The
visiting tutor must be notified by telephone or email of any warnings given.
VE R BAL W AR NIN G:
Reason for verbal warning
Action Taken:
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
W R ITTE N W AR NI NG:
Reason for written warning:
164

Practice Education
Action Taken:
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
O UTC O ME
(PLEASE PLACE A CROSS IN THE APPROPRIATE BOX): IF THE OUTCOME IS A FAIL
FOR THE PLACEMENT, THE VISITING TUTOR MUST BE PRESENT TO SUPPORT THE
STUDENT AND CLINICAL EDUCATOR AND CHECK THAT THE PROCESS IS CARRIED
OUT FAIRLY
Pass Fail
165

Practice Education
CO MM E NTS :
Signed (Clinical Educator)………………………………… Date
…………………………………………..
Signed (Student)………………………………………… Date
…………………………………………..
Signed (Visiting Tutor, if appropriate)……………………… Date …………………………………………
166

Practice Education
FACULTY OF HEALTH, PSYCHOLOGY AND SOCIAL CAREDepartment of Health Professions
Elective placement assessment form part 1 (physiotherapy practice)I confirm that this student has: Attended an elective placement and has completed
clinical hours (125 hours minimum).
Had opportunity to participate in the physiotherapy management of patients/clients and in doing so has:
o Demonstrated effective communication skillso Demonstrated ability to work as part of a teamo Demonstrated ability to manage and organise caseloado Demonstrated awareness of own limitations in practice (knowledge,
understanding and skills)o Acted constructively to independently manage own learningo Collected information relating to patiento Planned and carried out appropriate objective examinationso Analysed findings and formulated written treatment plans in partnership
with the patiento Implemented and evaluated treatment planso Demonstrated ability to keep and maintain patient records
At a level and to a standard that is considered to be competent given the students experience to date.
PHYSIOTHERAPY PRACTICE PASS FAIL
Signature clinical educator…………………………………… Date …………………
Please return this form to Student Life by 4.00 pm Friday ***********
.
Student namePlacement LocationStart date Finish date
167

Practice Education
Appendix 7: Case Review Guidance MSc Pre-registration
CASE REVIEW GUIDANCE
One each to be written on Practice Placements 1, 2 and 3 Guidance on preparation of case review and its links to the Critical Thinking /Project UnitThis document should be read with reference to:
Case Review Feedback 1 form Case Review Feedback 2 form Project Idea Proposal form Critical Thinking / Project unit proforma
Introduction
The case review is a piece of work that you will be expected to carry out on each of
your first three practice placements. It will form the basis of the project component of
the MSc Physiotherapy (Pre-registration) programme. The staff: student contact
allocated for the Critical Thinking /Project Unit is ten hours. Time in addition to these
will be available for you to reflect on the case reviews carried out after Practice
Placements 1 and 2 with your personal tutor. A breakdown of the allocation of hours
can be seen at the end of this document.
The expected learning outcomes for the Critical Thinking / Project unit are:
The student will be able to:
Apply and integrate relevant aspects of knowledge, understanding, skills and
experiences developed in previous units of the programme.
Systematically search for, analyse and critically appraise the findings and
writing of others relevant to the research being undertaken. Select, synthesise
and manage information in order to undertake their research task.
Use logical and reasoned argument to support their project and discuss the
diversity of arguments and contradictions in the evidence base.
Design and discuss an appropriate and realistic research methodology to
effectively address the objectives of their project.
Discuss the importance of ethical issues related to the proposed research.
168

Practice Education
Discuss and apply appropriate statistical methods.
Produce a scholarly piece of work.
Assessment criteria for the Critical Thinking / Project unit are:
The students will produce a detailed project that demonstrates their ability to:
search for, select, critically evaluate and synthesise the current evidence
underpinning physiotherapy practice related to their chosen topic
develop and clearly formulate a justified research question
develop an appropriate and realistic methodology / strategy to achieve their
objectives
demonstrate an understanding of the relevant ethical issues
use logical, reasoned, coherent and evaluative arguments
present the project in an appropriate academic format
demonstrate some originality in the application of their knowledge.
Possible project formats:
A reliability study, using normal subjects to ascertain the reliability of a particular
monitoring tool or outcome measure that you have used in practice.
A critical and systematic literature review that explores in detail the evidence
base for a monitoring tool, outcome measure, management approach or
treatment intervention that you have used.
An extended research proposal that demonstrates a gap in the literature and
details an evidence based methodology to answer a question about a monitoring
tool, outcome measure, management approach or treatment intervention that you
have used.
Introductory session for the Critical Thinking /Project Unit:
This session will constitute one hour of the allocated ten hours contact time.
This session will take place towards the end of the Health Care Delivery unit and will
give further information about how the Case Reviews and the Case Review
Presentation will form the foundation of the Project. Tips on the setting of interim
169

Practice Education
deadlines and best use of time will be generated and assessment criteria will be
introduced and discussed. In this session, you will be provided with a Project
Handbook.
Format of the case review.The case review should be of a patient you have managed on practice placement.
The patient details should be anonymised to protect the patient’s identity. The
format in which you present the case review is up to you (it may be in narrative or
tabular form for example), but it should describe a journey or process and not a one-
off encounter. You should document the following aspects:
Examination:
a. What were your first impressions of the patient? What was the source of the
first impressions eg information from a referral, the patient themselves, other
health professionals, carers, relatives or your own observations about the
patient’s demeanour, appearance etc.
b. Use the standard headings (PC, HPC, PMH etc) to document the subjective
examination of the patient. Also include information about the patient’s
gender and age.
c. Hypothesise about the possible causes of the patient’s main presenting
problems – were you able to hypothesise about a possible diagnosis before
you started your objective examination? Reflect on why this was or wasn’t the
case.
d. Document the objective examination carried out. Reflect on why you carried
out the tests / examination procedures you did, and why you may have left out
others. If you were able to hypothesise about a possible diagnosis during
your subjective examination, did your tests confirm or refute your diagnosis?
Refer to the literature to find out about the psychometric properties of the tests
you used with particular reference to the context in which you were working.
e. List the patient’s clinical features and suggest possible diagnoses. Relate the
presenting clinical features to the underlying pathology for the diagnoses you
have suggested.
170

Practice Education
Appendix 8
Manchester Metropolitan UniversityFaculty of Health, Psychology and Social CareDepartment of Health ProfessionsPractice placement 4 – written element
AS SIGN ME NT S PE CIF ICA TIO N [2 0 0 9 - 10 ]
Assessment Specification
Practice placement 4This assignment is designed to test the 17 Unit learning Outcomes documented in the Students’ Practice Placement Handbook (2008:13) and the following key skills:
Key skills: The student will be able to:1. Reflect on and analyse clinical experience to facilitate continuous professional
development (CPD).
2. Produce pieces of reflective writing that demonstrate self awareness and provide evidence for CPD.
Note: Not all of the learning outcomes will be tested in all of the assignments.
Assessment – A case review with a focus on the outcome measures usedFor this piece of work you are expected to present the reasoning and justification for your choice of outcome measures in the assessment and treatment of a patient you have treated on practice placement 4.To do this you will need to:
o Describe the relevant clinical background, diagnosis and patho-physiology relevant to the patient’s condition.
o Explain and justify your choice of outcome measures used in the subjective & objective assessment procedures and in the evaluation of the patient’s progress.
o Present appropriate evidence to support your choice of outcome measures.
o Demonstrate that you have taken a critical approach to reviewing the evidence base related to your case review.
o Articulate how this experience has lead to professional development or has changed your clinical practice
o Present your case review in an appropriate academic / reflective style including a bibliography.
The topic chosen for the practice placement 4 case review will be marked using level 6 marking criteria which are attached to this document.
171

Practice Education
The marking of this assignment will be undertaken using software that enables markers to generate consistently formatted and individualised feedback. The feedback will assist you in that it will relate to the criteria for each section. The feedback will also indicate the mark that you were allocated for the section, the highest mark allocated by all markers for this section, the lowest mark allocated by all markers for this section and the average mark awarded.This feedback will be delivered to you through your student email account on the date of publication of results indicated in the year handbook.
Submission date
Practice Placement 4 – Unit code 28150015.
Unit leaders J Nicholson/s Taylor
Written component submission Wednesday 18th November 2009
Late submission deadline (both elements) Wednesday 2nd December 2009
Marks normally released
(Subject to confirmation by the board of examiners)
Wednesday 13th January 2010
Assessed coursework (practice placement booklet and the corresponding assignment) should be submitted to the Student Life Office according to their document ‘Coursework submission guidance’ available from the internet at: <http://www.hpsc.mmu.ac.uk/students/other_information.php>
Late submission of practice placement booklets and corresponding assignmentsMarks for assessed coursework (practice placement booklets and corresponding assignments) submitted after the deadline for submission without prior written agreement from the Examinations Officers will be subject to penalty. Students are advised to consult the Regulations for Undergraduate and Taught Postgraduate Programmes of Study 2008/09, Appendix 1 relating to penalties late submission of coursework (available from the internet at http://www.mmu.ac.uk/academic/grad_regulations.phpAssignments that are submitted after the late submission deadline without prior arrangement with the examinations officer will score zero marks.
Assignment Format RegulationsALL AS S IGNM EN TS M US T BE T YPE D U SI NG TH E F OL LO W ING LAY O UT AND R EGU LAT ION S: -
1. Margins (Left 1.5"(4 cm); Right 1.0"(2.5 cm); Top 1.0" (2.5 cm); Bottom 1.0" (2.5 cm)
2. Font size. Minimum 12pt/12 c.p.i. Good examples, which are easy to read, are Times New Roman and Ariel.
172

Practice Education
IT IS NOT ACCEPTABLE TO USE NARROW FONT, TO CONDENSE
THE FONT OR TO MODIFY KERNELLING AND STUDENTS MAY BE
PENALISED IF THIS OCCURS.
3. Pages should be numbered throughout (including bibliography) at the centre/bottom of the page.
4. Personal student identification number should be included in the header/footer of each page
5. Referencing, citations and bibliography construction should be constructed in line with the instructions that can be accessed via the library and WebCT.
6. Double spacing must be used throughout the text and the text must be on one side of the paper only.
MAXIMUM ASSIGNMENT LENGTH DOES NOT INCLUDE
BIBLIOGRAPHY OR TITLE PAGE OR ANY APPENDICES
The page limit for this assignment is 6 sides of A4 (MAXIMUM). Assignments that exceed this limit are subject to a penalty up to a maximum of 15 marks (see table).
WORD PENALTY SCALE
>6 sides A4 < 6 ½ sides of A4 5 marks deducted
> 6 ½ sides A4 < 7 sides of A4 10 marks deducted
> 7 sides of A4 15 marks deducted
173

Practice Education
General guidance Your notes from the research methods sessions delivered throughout your first
and second year units will provide you with essential guidance on writing your assignment.
There are many other useful resources on outcome measures and research methodology. Start with the resources recommended below;
Chartered Society of Physiotherapy (2001) ‘Outcome Measures’ [Online] [Accessed 22 September 2009] Available from: http://www.csp.org.uk/uploads/documents/csp_outcomemeasures_clef03.pdf
Sim, J. & Wright, C. (2000) ‘Research in health care - concepts, designs and methods.’ Nelson Thornes: Cheltenham
Wade, D. (1992) ‘Measurement in neurological rehabilitation.’ Oxford University Press: Oxford.
These represent an introduction to the use and justification of certain outcome measures. Read these before you search more widely as searching the internet or library website is likely to leave you initially overwhelmed.
Even though the page limit is 6 pages you will not be penalised if you write less as long as you meet the learning outcomes.
Unlike previous assignments reflective writing is always done in the 1st person e.g. “I think ……”, “I feel ……..”.
A bibliography is necessary as you need to support your reasoning with references from the evidence base related to your case review and the outcome measures chosen. Referencing in the text and the bibliography must be done in accordance with MMU policy (see referencing guide – WebCT). The Harvard method is the preferred method and no other method is acceptable. You will be penalised if other methods are used. See further information in the library about how Internet sites should be referenced.
Members of staff and clinical educators will not read drafts of your assignment nor discuss specific details about your assignment. Some support may be sought from your visiting teacher or personal tutor on the process of clinical reasoning and reflective writing.
Producing a well reasoned case review will require you to write a draft and reflect on this draft several times until you generate the necessary depth of explanation and justification for your choice of outcome measures with regard to your patient and as required by the marking criteria.
174

Practice Education
Thorough self evaluation of your practice is difficult and requires you to be honest with yourself. The more you practice it the better you become at it so begin early on in your placement.
For this assignment you are asked to concentrate on the outcome measures you have used with your patient and so consideration of the reasons why certain measures have been used would be a helpful topic for discussion between you and your fellow students, clinical educator and visiting teacher.
Ensure that you maintain anonymity and confidentiality of any persons or places you describe or discuss during your reflection. Failure to do so could constitute a breach of confidentiality under the Rules of Professional Conduct.
If you include a copy of the patient’s physiotherapy records in an appendix to your assignment, please ensure that you have the permission of your practice educator to make such a copy. In addition, ensure that those records have been anonymised; The reader should not be able to identify the patient, the practice setting or any of the other personnel involved with the patient. Again, failure to do so could constitute a breach of confidentiality under the Rules of Professional Conduct.
Ensure that any reflections you make are objective and could not offend, harm or infer a lack of competence in any of the persons discussed (see Rule 4: Rules of Professional Conduct. CSP).
175

Practice Education
Manchester Metropolitan UniversityFaculty of Health, Psychology & Social CareDepartment Of Health Professions BSc [Hons] PhysiotherapyMarking criteria 2009-2010
PR ACT IC E PL ACE ME NT 4 – W R ITT EN E L EM EN T
Each criterion will be marked out of 100 and weighted according to the following percentages;
Assessment criteria % Description 10Explanation of the outcome measures used in the assessment and monitoring procedures
20
Justification of the outcome measures used in the assessment and monitoring procedures
20
Use and critique of the evidence base 20Evidence of learning / professional development 20Presentation including bibliography 10
Total 100
Evidence of characteristicFirst (1) (70+) Extensive /Very StrongUpper Second (2.1) (60-69) Widespread / StrongLower Second (2.2) (50-59) Some / GoodThird (3) (40-49) Intermittent / AdequateFail (Marginal) (Fc) (35-39) Insufficient /WeakFail (F) (0-34) None, minimal / Very Weak
176

Practice Education
Marking criteria
Describe the relevant clinical background, including patho-physiology and the clinical diagnosis for the patient’s condition
0
No serious attempt has been made to describe the relevant clinical background, including patho-physiology and clinical diagnosis for the patient’s condition/your description is largely irrelevant .The scene is not set /the information provided does not support the process of clinical reasoning.
20
The description of the relevant clinical background/patho-physiology/clinical diagnosis is minimal. The information that you have provided is minimal. The scene that you have set and information provided only minimally supports the process of clinical reasoning.
35
The description of the relevant clinical background/patho-physiology/clinical diagnosis is lacking in detail. The information that you have provided is only weakly relevant. The scene is inadequately set/the information provided only partially supports the process of clinical reasoning.
40
The description of the relevant clinical background/patho-physiology/clinical diagnosis is adequate. The information that you have provided has adequate relevance. The scene is adequately set/the information provided supports the process of clinical reasoning.
50The description of the relevant clinical background/patho-physiology/clinical diagnosis is good. The information that you have provided has some relevance/scene setting is good. The information provided supports the process of clinical reasoning well.
60
The description of the relevant clinical background/patho-physiology/clinical diagnosis is very good. The information that you have provided has widespread relevance/scene setting is very good. The information provided supports the process of clinical reasoning very well.
70
The description of the relevant clinical background/patho-physiology/clinical diagnosis is excellent. The information that you have provided is extensively relevant/scene setting is excellent. The information provided to support the process of clinical reasoning is excellent.
85
The description of the relevant clinical background/patho-physiology/clinical diagnosis is outstanding. The information that you have provided has outstanding relevance/scene setting is outstanding. The information provided to support the process of clinical reasoning is outstanding.
Explanation of the outcome measures used in the assessment and monitoring procedures
0 There is no evidence of explanation of the outcome measures used to
177

Practice Education
address the needs of the patient in a holistic manner.
20 There is inadequate evidence of explanation of the outcome measures used to address the needs of the patient in a holistic manner.
35 There is intermittent evidence of explanation of the outcome measures used to address the needs of the patient in a holistic manner.
40 There is adequate evidence of explanation of the outcome measures used to address the needs of the patient in a holistic manner.
50 There is good evidence of explanation of the outcome measures used to address the needs of the patient in a holistic manner.
60 There is widespread evidence of explanation of the outcome measures used to address the needs of the patient in a holistic manner.
70 There is excellent evidence of explanation of the outcome measures used to address the needs of the patient in a holistic manner.
85 There is outstanding evidence of explanation of the outcome measures used to address the needs of the patient in a holistic manner.
Justification of the outcome measures used in the assessment and monitoring procedures
0 There is no evidence of justification of the outcome measures chosen and modification (or not) in light of clinical findings.
20 There is inadequate evidence of justification of the outcome measures chosen and modification (or not) in light of clinical findings.
35 There is intermittent evidence of justification of the outcome measures chosen and modification (or not) in light of clinical findings.
40 There is adequate evidence of justification of the outcome measures chosen and modification (or not) in light of clinical findings.
50 There is good evidence of justification of the outcome measures chosen and modification (or not) in light of clinical findings.
60 There is widespread evidence of justification of the outcome measures chosen and modification (or not) in light of clinical findings.
70 There is excellent evidence of justification of the outcome measures chosen and modification (or not) in light of clinical findings.
85 There is outstanding evidence of justification of the outcome measures chosen and modification (or not) in light of clinical findings.
178
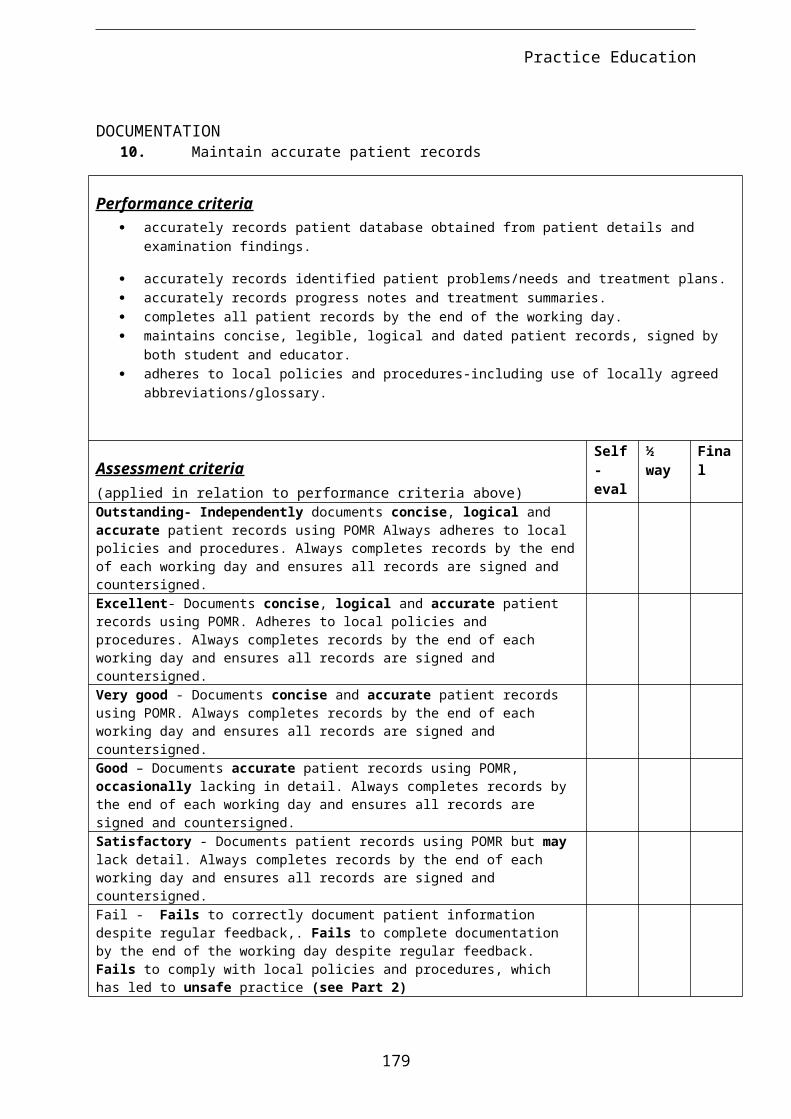
Practice Education
Present appropriate evidence to support your reasoning and demonstrate that you have taken a critical approach to reviewing the evidence base related to your case review
0There is no evidence that the assignment has been supported by relevant and current evidence and consequently no evidence of critical analysis of the literature
20There is inadequate evidence that the assignment has been supported by relevant and current evidence. There is inadequate critical analysis of the literature.
35There is intermittent evidence that the assignment has been supported by relevant and current evidence. There is intermittent critical analysis of the literature.
40There is adequate evidence that the assignment has been supported by relevant and current evidence. There is adequate critical analysis of the literature.
50There is good evidence that the assignment has been supported by relevant and current evidence. There is good critical analysis of the literature.
60There is widespread evidence that the assignment has been supported by relevant and current evidence. There is widespread critical analysis of the literature.
70There is excellent evidence that the assignment has been supported by relevant and current evidence. There is excellent critical analysis of the literature.
85There is outstanding evidence that the assignment has been supported by relevant and current evidence. There is outstanding critical analysis of the literature.
179

Practice Education
Evidence of learning professional Development and / or a change in clinical PRACTICE 0 There is no evidence that conclusions have been reached. There is no
evidence of planning for future action. There is no evidence of consideration of how reflection and clinical reasoning can contribute to professional or personal development
20 There is inadequate evidence that conclusions have been reached. There is inadequate evidence of planning for future action. There is inadequate evidence of consideration of how reflection and clinical reasoning can contribute to professional or personal development
35 There is intermittent evidence that conclusions have been reached. There is intermittent evidence of planning for future action. There is intermittent evidence of consideration of how reflection and clinical reasoning can contribute to professional or personal development
40 There is adequate evidence that conclusions have been reached. There is adequate evidence of planning for future action. There is adequate evidence of consideration of how reflection and clinical reasoning can contribute to professional or personal development
50 There is good evidence that conclusions have been reached. There is good evidence of planning for future action. There is good evidence of consideration of how reflection and clinical reasoning can contribute to professional or personal development
60 There is widespread evidence that conclusions have been reached. There is widespread evidence of planning for future action. There is widespread evidence of consideration of how reflection and clinical reasoning can contribute to professional or personal development
70 There is excellent evidence that conclusions have been reached. There is excellent evidence of planning for future action. There is excellent evidence of consideration of how reflection and clinical reasoning can contribute to professional or personal development
85 There is outstanding evidence that conclusions have been reached. There is outstanding evidence of planning for future action. There is outstanding evidence of consideration of how reflection and clinical reasoning can contribute to professional or personal development
180
Practice Education
Presentation
0The account has no obvious structure or focus. The account is illogical and incoherent. There are many grammatical, spelling or punctuation errors, which are so frequent that the meaning of sentences is unclear. Citations and bibliography entirely incorrect.
20The account has little obvious structure or focus. There is little logic or coherency to this account. There are many grammatical, spelling or punctuation errors. There are many major errors in citations and bibliography.
35The account has insufficient structure or focus. There is insufficient logic or coherency to this account. There are some grammatical, spelling or punctuation errors. There are some major errors in citations and bibliography.
40The account has adequate structure or focus. There is intermittent logic or coherency to this account. There are minor grammatical, spelling or punctuation errors. There are some minor errors in citations and bibliography.
50The account has good structure or focus. There is some logic or coherency to this account. Grammar, spelling and punctuation are mostly correct. Citations and bibliography is mostly correct.
60
The structure and focus of the account is very good. A very logical and coherent account. Rules of grammar and spelling are consistently applied using an appropriate academic style. Citations and bibliography are correct throughout and support the process of reflection and clinical reasoning.
70
The structure and focus of the account is excellent. A highly logical and coherent account. Rules of grammar and spelling consistently applied using an appropriate academic style. Citations and bibliography entirely correct throughout and support the process of reflection and clinical reasoning to a great extent.
85
The structure and focus of the account is outstanding. A highly logical and coherent account. Rules of grammar and spelling consistently applied using an appropriate academic style. Citations and bibliography entirely correct throughout and support the process of reflection and clinical reasoning to a very great extent.
181

Practice Education
Appendix 9
Manchester Metropolitan UniversityFaculty of Health, Psychology and Social CareDepartment of Health ProfessionsManchester Metropolitan UniversityFaculty of Health, Psychology and Social CareDepartment of Health ProfessionsPractice placement 5 – written element
AS SIGN ME NT S PE CIF ICA TIO N [2 0 0 9 - 10 ]
Assessment Specification
Practice placement 5This assignment is designed to test the 17 Unit learning Outcomes documented in the Students’ Practice Placement Handbook (2008:13) and the following key skills:
Key skills: The student will be able to:3. Reflect on and analyse clinical experience to facilitate continuous professional
development (CPD).
4. Produce pieces of reflective writing that demonstrate self awareness and provide evidence for CPD.
Note: Not all of the learning outcomes will be tested in all of the assignments.
Assessmento Students are required to submit a piece of reflective writing following practice
placement 5. The reflective writing should explore an experience that they have had during this practice placement and should articulate how this experience has lead to professional development or has changed their clinical practice.
o Reflective writing is largely concerned with looking back - but with a view to development in the future. To be useful and developmental, reflective writing must go beyond description of events and associated feelings. It is necessary to:
step back, explore and analyse your own role in the experience consider the different perspectives of other people involved make connections with relevant theories, supporting your ideas by reference to
literature and research where this is appropriate and most importantly show what you have learned from the process
o Students will choose the experience that will be the subject of their reflective writing. The topic chosen should be relevant to the placement that they have experienced. It is expected that a different experience will be chosen for each piece of reflective writing.
182

Practice Education
o Topics chosen for practice placement 5 will be marked using level 6 marking criteria which are attached to this document.
Submission
Practice Placement 5 – Unit code 28150016
Unit leaders J Nicholson/s Taylor
Placement booklet submission Wednesday 13th January 2010
Written component submission Wednesday 13th January 2010
Late submission deadline (both elements) Wednesday 27th January 2010
Marks normally released
(Subject to confirmation by the board of examiners)
Thursday 26th February 2010
Assessed coursework (reflective writing assignment) should be submitted to the Student Life Office according to their document ‘Coursework submission guidance’ available from the internet at: http://www.hpsc.mmu.ac.uk/students/other_information.php
Late submission of practice placement booklets and Reflective writing assignmentMarks for assessed coursework (practice placement booklets and corresponding assignments) submitted after the deadline for submission without prior written agreement from the Examinations Officers will be subject to penalty. Students are advised to consult the Regulations for Undergraduate and Taught Postgraduate Programmes of Study 2008/09, Appendix 1 relating to penalties late submission of coursework (available from the internet at http://www.mmu.ac.uk/academic/grad_regulations.phpAssignments that are submitted after the late submission deadline without prior arrangement with the examinations officer will score zero marks.
submitting your work to TurnitinUK [submit.ac.uk]You will find ‘Turnitin link: Reflective writing 5’ in your ‘Practice placement –Level 6’ WebCT area under the assessment folder. You need to submit your assignment using this link. If you have any problems with submitting to TurnitinUK, please contact Narayan Prabhu ([email protected])In order to help you improve the standard of your work, e.g. detecting whether you have quoted and referenced others’ work properly, you are required to submit your assignment through TurntinUK as part of the Reflective writing assessment process.TurnitinUK will provide you with an Originality Report. This provides a percentage relating to the amount of your work that is similar to that of others’. Use this like a
183

Practice Education
spell checker to see whether you have forgotten to reference or quote correctly the work of others’. Submit your work as many times as you like until you are happy that no plagiarism exists and that you have referenced and quoted correctly. Failure to reference or quote the work of others properly maybe seen as an attempt to pass their work off as your own; this is plagiarism.Details of how to login and submit work are also provided in ‘Student guide to TurnitinUK’ on WebCT. Submission to Turnitin is seen as part of your assessment, therefore, failure to upload you work will be seen as failure to submit your assignment. Your assignment will not be marked until the report has been submitted.
Avoiding plagiarism Make sure you understand what plagiarism is. The University views plagiarism as a serious matter. You are advised to read Appendix 5 for the information on plagiarism in the Assessment Regulations for Undergraduate and Taught Postgraduate Programmes of Study using the link given below. Penalties will be applied if plagiarism occurs. http://www.mmu.ac.uk/academic/grad_regulations.phpBeware the dangers of working too closely with your colleagues. Remember that the submission must be your own work. If you work too closely with others and you could find yourselves being penalised for plagiarising each other’s work.
All assignments must be typed using the following layout and regulations:-7. Margins (Left 1.5"(4 cm); Right 1.0"(2.5 cm); Top 1.0" (2.5 cm); Bottom 1.0" (2.5
cm)8. Font: Arial, 12pt no font substitution is acceptable.
IT IS NOT ACCEPTABLE TO USE NARROW FONT, TO CONDENSE THE FONT OR TO
MODIFY KERNELLING AND STUDENTS MAY BE SUBJECT TO PENALTY IF THIS OCCURS.
9. Pages should be numbered throughout (including bibliography) at the bottom of the page.
10. Personal student identification number should be included in the header/footer of each page
11. Referencing, citations and bibliography construction should be constructed in line with the instructions in the assignment specification. Guidance can be accessed via the library and WebCT.
12. Double spacing must be used throughout the text and the text must be on one side of the paper only.
The page limit for this assignment is 6 sides of A4 (MAXIMUM). Assignments that exceed this limit are subject to a penalty up to a maximum of 15 marks (see table).
WORD PENALTY SCALE
>6 sides A4 < 6 ½ sides of A4 5 marks deducted
184

Practice Education
> 6 ½ sides A4 < 7 sides of A4 10 marks deducted
> 7 sides of A4 15 marks deducted
General guidance The lecture notes from the theatre event on reflective writing in the FiPP Unit will
provide you with essential guidance on writing your assignment.
There are many other useful resources on reflective writing. Start with the two resources recommended in the theatre event.
Moon , J, (n.d.) Reflective writing: guidance notes for students.[online]. Available from: http://services.exeter.ac.uk/cas/employability/students/reflective.htm [accessed 22/01/09]
Bolton, G. (2001) Reflective Practice Writing for Professional Development. London: Sage (15 copies in Elizabeth Gaskell Library)
These represent a simple but concise introduction to reflective writing. Read these before you search more widely as searching the internet or library website is likely to leave you initially overwhelmed.
Even though the page limit is 6 pages you will not be penalized if you write less as long as you meet the learning outcomes.
Unlike previous assignments reflective writing is always done in the 1st person e.g. “I think ……”, “I feel ……..” .
A bibliography is not necessary but you may support your ideas with references from literature if appropriate. Referencing in the text and the bibliography must be done in accordance with MMU policy (see referencing guide– WebCT). The Harvard method is the preferred method and no other method is acceptable. You will be penalized if other methods are used. See further information in the library about how Internet sites should be referenced.
Members of staff and clinical educators will not read drafts of your assignment nor discuss specific details about your assignment. Some support may be sought from your visiting teacher or personal tutor on the process of reflective writing.
Reflective writing will require you to write a draft and reflect on this draft several times until you generate the necessary depth of reflection required by the marking criteria.
The process of deep reflection is difficult and requires you to be honest with yourself. The more you practice it the better you become at it so begin early on in your placement.
185

Practice Education
Get into the habit of talking through your reflections with your clinical educator, visiting teacher or fellow students.
Ensure that you maintain anonymity and confidentiality of any persons or places you describe or discuss during your reflection. Failure to do so could constitute a breach of confidentiality under the Rules of Professional Conduct.
Ensure that any reflections you make are objective and could not offend, harm or infer a lack of competence in any of the persons discussed (see Rule 4: Rules of Professional Conduct. CSP).
186

Practice Education
Manchester Metropolitan UniversityFaculty of Health, Psychology & Social CareDepartment Of Health Professions BSc [Hons] PhysiotherapyMarking criteria 2009-2010
PR ACT IC E PL ACE ME NT 5 – W R ITT EN E L EM EN T
Each criterion will be marked out of 100 and weighted according to the following percentages;
Assessment criteria %Description 20Depth of reflection 20Scope 20Evidence of learning 20Presentation including bibliography 20Total 100
Evidence of characteristicFirst (1) (70+) Extensive /Very StrongUpper Second (2.1) (60-69) Widespread / StrongLower Second (2.2) (50-59) Some / GoodThird (3) (40-49) Intermittent / AdequateFail (Marginal) (Fm) (35-39) Insufficient /WeakFail (F) (0-34) None, minimal / Very Weak
187

Practice Education
Marking criteria
Description Marks Criteria0 No serious attempt has been made to describe the learning experience. The
information that you have provided is largely irrelevant/the scene is not set/the information provided does not support the process of reflection. There is no consideration of the behaviour/reactions/feelings of relevant actors within the context.
20 The description of the learning experience is minimal. The information that you have provided is of minimal relevance/the scene is unclear/the information provided minimally supports the process of reflection. There is no consideration of the behaviour/reactions/feelings of relevant actors within the context.
35 The description of the learning experience is lacking in detail. The information that you have provided is only weakly relevant/the scene is inadequately set/the information provided only partially supports the process of reflection. There is insufficient consideration of the behaviour/reactions/feelings of relevant actors within the context.
40 The description of the learning experience is adequate. The information that you have provided has adequate relevance/the scene is adequately set/the information provided supports the process of reflection. There is intermittent consideration of the behaviour/reactions/feelings of relevant actors within the context.
50 The description of the learning experience is good. The information that you have provided has some relevance/scene setting is good/the information provided supports the process of reflection well. There is some consideration of the behaviour/reactions/feelings of relevant actors within the context.
60 The description of the learning experience is very good. The information that you have provided has widespread relevance/scene setting is very good/the information provided supports the process of reflection very well. There is widespread consideration of the behaviour/reactions/feelings of relevant actors within the context.
70 The description of the learning experience is excellent. The information that you have provided has very strong relevance/scene setting is extensive/the information provided to support the process of reflection is excellent. There is extensive consideration of the behaviour/reactions/feelings of relevant actors within the context.
85 The description of the learning experience is outstanding. The information that you have provided has outstanding relevance/scene setting is outstanding/the information provided to support the process of reflection is outstanding. There is extensive consideration of the behaviour/reactions/feelings of relevant actors within the context.
188
Practice Education
Depth of reflection Marks Criteria0 There is no evidence of self-analysis/exploring or testing of alternate
explanations/interpretation. Ideas are not reconsidered from different standpoints.
20 There is inadequate evidence of self-analysis/exploring or testing of alternate explanations/interpretation. Ideas are not reconsidered from different standpoints.
35 There is intermittent evidence of self-analysis/exploring or testing of alternate explanations/interpretation. Ideas are insufficiently reconsidered from different standpoints.
40 There is adequate evidence of self-analysis/exploring or testing of alternate explanations/interpretation. Ideas are intermittently reconsidered from different standpoints
50 There is good evidence of self-analysis/exploring or testing of alternate explanations/interpretation. Ideas are reconsidered from different standpoints well.
60 There is widespread evidence of self-analysis/exploring or testing of alternate explanations/interpretation. Ideas are reconsidered from different standpoints very well.
70 There is excellent evidence of self-analysis/outstanding exploring or testing of alternate explanations/interpretations. Ideas are deconstructed and are considered from different standpoints excellently.
85 There is outstanding evidence of self-analysis/outstanding evidence of exploring or testing of alternate explanations/interpretations. Ideas are deconstructed and reconsidered extensively from many different standpoints outstandingly.
189

Practice Education
Scope Marks Criteria0 There is no evidence that you have considered the perspectives of other
people or other factors involved in the situation. There is no evidence of standing back to gain a new perspective, or consideration of the wider professional context of the situation.
20 There is inadequate evidence that you have considered the perspectives of other people or other factors involved in the situation. There is inadequate evidence of standing back to gain a new perspective, or consideration of the wider professional context of the situation.
35 There is intermittent evidence that you have considered the perspectives of other people or other factors involved in the situation. There is intermittent evidence of standing back to gain a new perspective, or consideration of the wider professional context of the situation.
40 There is adequate evidence that you have considered the perspectives of other people or other factors involved in the situation. There is adequate evidence of standing back to gain a new perspective, or consideration of the wider professional context of the situation.
50 There is good evidence that you have considered the perspectives of other people or other factors involved in the situation. There is good evidence of standing back to gain a new perspective, or consideration of the wider professional context of the situation.
60 There is widespread evidence that you have considered the perspectives of other people or other factors involved in the situation. There is widespread evidence of standing back to gain a new perspective, or consideration of the wider professional context of the situation.
70 There is excellent evidence that you have considered the perspectives of other people or other factors involved in the situation. There is excellent evidence of standing back to gain a new perspective, or consideration of the wider professional context of the situation.
85 There is outstanding evidence that you have considered the perspectives of other people or other factors involved in the situation. There is outstanding evidence of standing back to gain a new perspective, or consideration of the wider professional context of the situation
190

Practice Education
Evidence of learning Marks Criteria0 There is no evidence of new learning, a change in attitude, or professional
practice. There is no evidence that conclusions have been reached. There is no evidence of planning for future action. There is no evidence of consideration of how reflection can contribute to professional or personal development
20 There is minimal evidence of new learning, a change in attitude, or professional practice. There is inadequate evidence that conclusions have been reached. There is inadequate evidence of planning for future action. There is inadequate evidence of consideration of how reflection can contribute to professional or personal development
35 There is insufficient evidence of new learning, a change in attitude, or professional practice. There is intermittent evidence that conclusions have been reached. There is intermittent evidence of planning for future action. There is intermittent evidence of consideration of how reflection can contribute to professional or personal development
40 There is some evidence of new learning, a change in attitude, or professional practice. There is adequate evidence that conclusions have been reached. There is adequate evidence of planning for future action. There is adequate evidence of consideration of how reflection can contribute to professional or personal development
50 There is some good evidence of new learning, a change in attitude, or professional practice. There is good evidence that conclusions have been reached. There is good evidence of planning for future action. There is good evidence of consideration of how reflection can contribute to professional or personal development
60 There is strong evidence of new learning, a change in attitude, or professional practice. There is widespread evidence that conclusions have been reached. There is widespread evidence of planning for future action. There is widespread evidence of consideration of how reflection can contribute to professional or personal development
70 There is very strong evidence of new learning, a change in attitude, or professional practice. There is excellent evidence that conclusions have been reached. There is excellent evidence of planning for future action. There is excellent evidence of consideration of how reflection can contribute to professional or personal development
85 There is extensive evidence of new learning, a change in attitude, or professional practice. There is outstanding evidence that conclusions have been reached. There is outstanding evidence of planning for future action. There is outstanding evidence of consideration of how reflection can contribute to professional or personal development
191

Practice Education
Presentation Marks Criteria0 The account has no obvious structure or focus. The account is illogical and
incoherent. There are many grammatical, spelling or punctuation errors, which are so frequent that the meaning of sentences is unclear. Citations (if used) and bibliography entirely incorrect.
20 The account has little obvious structure or focus. There is little logic or coherency to this account. There are many grammatical, spelling or punctuation errors. There are many major errors in citations (if used) and bibliography.
35 The account has insufficient structure or focus. There is insufficient logic or coherency to this account. There are some grammatical, spelling or punctuation errors. There are some major errors in citations (if used) and bibliography.
40 The account has adequate structure or focus. There is intermittent logic or coherency to this account. There are minor grammatical, spelling or punctuation errors. There are some minor errors in citations (if used) and bibliography.
50 The account has good structure or focus. There is some logic or coherency to this account. Grammar, spelling and punctuation are mostly correct. Citations (if used) and bibliography is mostly correct.
60 The structure and focus of the account is very good. A very logical and coherent account. Rules of grammar and spelling are consistently applied using an appropriate academic style. Citations (if used) and bibliography are correct throughout and support the process of reflection.
70 The structure and focus of the account is excellent. A highly logical and coherent account. Rules of grammar and spelling consistently applied using an appropriate academic style. Citations (if used) and bibliography entirely correct throughout and support the process of reflection to a great extent.
85 The structure and focus of the account is outstanding. A highly logical and coherent account. Rules of grammar and spelling consistently applied using an appropriate academic style. Citations (if used) and bibliography entirely correct throughout and support the process of reflection to a very great extent.
192

Practice Education
Title pageManchester Metropolitan UniversityFaculty of Health, Psychology and Social CareDepartment of Health Professions
Student ID No.
Unit Assessment: Practice placement 5 – written element
Unit Code: 28150016
Total number of pages submitted
Student Check List:
Student ID in header □Pages are numbered □Submitted to Turnitin □
Appendix 10: Placement Profile Proforma
193

Practice Education
Advance Information
PLACEMENT LOCATION
PLACEMENT LOCATION WEBSITE, (IF AVAILABLE)
CLINICAL AREA
FIELDWORK/PRACTICE EDUCATOR/S
CONTACT TELEPHONE NUMBER
SKILLS/PRE-READING REQUIRED BY STUDENT BEFORE BEGINNING THE PLACEMENTMAXIMUM NUMBER OF STUDENTS ON THIS PLACEMENT
SPECIFIC UNIFORM REQUIREMENTS
CHANGING/LOCKER FACILITIES
ADDITIONAL OCCUPATIONAL HEALTH SCREENING NEEDED (YES/NO + DETAILS)ACCOMMODATION INFORMATION(IF REQUIRED)NORMAL WORKING HOURS/LUNCH TIMES
PARKING
PUBLIC TRANSPORT
NEAREST LOCAL SHOPS
NEAREST CASH POINT
On Arrival
PLACE TO REPORT TO ON DAY 1
TIME TO REPORT ON DAY 1
Sickness
194

Practice Education
PERSON TO REPORT SICKNESS TO
BY WHAT TIME
WILL CLINICIANS INFORM SCHOOL OF ABSENCE IF VISIT FROM TEACHER IS SCHEDULED
Facilities and Resources
STAFF ROOM FACILITIES
CANTEEN FACILITIES
STUDENT SUPPORT ON PLACEMENT
LEARNING FACILITIES ON PLACEMENTINCLUDING ACCESS TO A COMPUTERDETAILS OF OPPORTUNITIES/TIME FOR STUDENT ACCESS TO LEARNING RESOURCES
LEARNING OPPORTUNITIES AVAILABLE ON PLACEMENT (INCLUDING OPPORTUNITIES FOR MULTI-PROFESSIONAL LEARNING)LEARNING OUTCOMES EXPECTED FROM PLACEMENT
NHS LIBRARY DETAILS(Please check to find out if you have access)
Library name –Telephone number – Opening hours – E mail -Web site –Intranet site – (Can only be accessed within the Trust)
Appendix 11
195

Practice Education
Faculty of Health, Psychology and Social CareDepartment of Health Professions
New Placement Provider Proforma Location
Date of Visit
Clinical Area
Clinical Educators
Health and Safety Check List
Equal Opportunity’s check list
Ability to meet the learning outcomes
Information Provided
Areas Discussed
Attendance of Clinical Educators Course
DateSignature
196

Practice Education
Sequencing of Units MSc Pre RegistrationThe curriculum for the MSc Pre Registration physiotherapy programme is structured around the theme of rehabilitation and various approaches are considered: preventative, maintenance, restorative and palliative, all within case-based clinical scenarios. Units have been sequenced to enable students to apply learning from one unit to another and / or to allow students to build on knowledge gained in earlier units by tackling similar but more complex themes at later stages. For example, Health Care Delivery includes research methods, which will be essential in ensuring that students acquire critical appraisal skills and are able to evaluate research findings. These skills are essential at Masters Level and will be integral to the teaching and learning within all programme units, preparing students for the project phase of the programme. Health Care Delivery and Patient Management 1 and 2 are sequenced so that all students will have studied the management of patients with a range of conditions from all three core areas of practice (musculoskeletal, cardio-respiratory and neurological), and will have considered the implications of clinical contexts and the legal and professional requirements of practice prior to Practice Placement 1. Health Care Delivery and Patient Management 1 and 2 will also include sessions to prepare students for Practice Placements:
Health Care Delivery will include sessions on: the philosophy of placements; roles and responsibilities of all parties; placement learning outcomes and assessment procedures; discussions with more experienced pre-registration students about their placement experiences; an introduction to Learning Development Plans and development of a Professional Development Portfolio. The unit also includes the mandatory training of CPR, fire lecture, infectious control and manual handling
Patient Management 1 and 2 will include role plays to explore issues of conflict; skills sessions linked to simulated practice scenarios; a meeting with the Visiting Lecturer to discuss roles and responsibilities of all parties and plan the Visiting Lecturer’s first clinical visit.
In order to ensure students are fully prepared for the clinical environment, students will not be allowed to commence Practice Placement 1 until they have successfully completed the assessments for Patient Management 1 and 2. They will thus be prepared to practice, apply and develop appropriate physiotherapy theory and practice in a variety of practice locations, and develop interpersonal and management skills. Patient Management 3 and 4 will build on the knowledge gained in Patient Management 1 and 2 by using case studies that are more complex and less predictable than those seen in the earlier units. Debrief sessions will be incorporated into the Health Care Delivery and Autonomous Practitioner units, to encourage reflection, conclusion and planning for future clinical experiences.
197

Programme Design and Organisation
198

Programme Design and Organisation
UNIT TITLE MSc Pre Registration Health Care Delivery
SUBJECT AREA Theme 1 – Introduction to ‘M’ LevelTheme 2 – Health and Social Care
UNIT LEARNING OUTCOMES
Unless stated otherwise all the following learning outcomes apply to all the unit themes.
The student will be able to:
Knowledge and Understanding Demonstrate an in-depth understanding of how
professional, statutory and regulatory body requirements impact on their learning experience (Theme 1).
Critically evaluate models of reflection and justify the need for reflective practice (Theme 1).
Critically analyse the factors that contribute to evidence-based practice (Theme 1).
Demonstrate a comprehensive understanding of the range of environments in which health & social care is delivered.
Demonstrate a comprehensive understanding of the organisation of health and social care services in the United Kingdom (UK) (Theme 2).
Demonstrate a critical awareness of the key drivers of health and social care policy in the UK.
Cognitive/Intellectual Skills Justify the importance of lifelong learning and continuing
professional development (Theme 1). Justify the need for equity of healthcare provision to a
diverse population. Critique a variety of approaches to rehabilitation and apply
their relevance to health (Theme 1). Critically evaluate different models of health & social care. Demonstrate a critical awareness of the relationship
between healthcare services and social care services (Theme 3).
Apply their knowledge of teamwork to the delivery of healthcare provision.
Key/transferable skills Communicate effectively in a variety of settings to both
specialist and non-specialist audiences. Demonstrate the application of research skills in order to
initiate and carry out projects (Theme 1). Work effectively with others as a member or a leader of a
group and meet obligations to others. Demonstrate the application of clinical reasoning skills in
order to make decisions for patient management.
199

Practice Education
Use appropriate study skills / information skills/ research methods skills / learning resources to support independent learning, including:- Undertake a systematic search of the literature.- Critically appraise and evaluate research literature.- Critically analyse a range of research designs and
methodologies appropriate to the health care field.- Identify and evaluate some of the available tools for
measuring aspects of health and health care.- Within different research approaches, evaluate issues
of validity and reliability or credibility and trustworthiness.
- Examine ethical issues arising in research situations and clinical contexts (Theme 1).
Preparation for Practice Placements including:- Appreciation of the Philosophy of placements and the
roles and responsibilities of all parties.- Exploration of practice placement learning outcomes
and assessment procedures.- Reflection on clinical observation.- Gain insight into the experiences of other students’ first
placements.
UNIT TITLE Patient Management 1
SUBJECT AREA
Physiotherapy Rehabilitation:Theme 1 – Foundations in Physiotherapy Management Theme 2 – Neurology
UNIT LEARNING OUTCOMES
Unless otherwise stated all the following learning outcomes apply to both unit themes. The student will be able to:
Knowledge and Understanding Demonstrate a comprehensive and systematic
understanding of how the structure and function of the major systems of the body contribute to human movement (Theme 1).
Explain the neuromuscular control of normal movement, the structure and function of the nervous system and apply these to explain the clinical features of selected predictable neurological deficits (Theme 2).
Interpret, reflect upon and evaluate the evidence base behind rehabilitation approaches for patients with neurological dysfunction (Theme 2).
Cognitive/intellectual skills Apply in depth knowledge of biomechanics to analyse normal
human movement (Theme 1). Discuss and evaluate the contribution of the major systems
of the body to normal human movement (Theme 1). Systematically apply an in-depth knowledge of histology and
200

Practice Education
physiology to explain soft tissue damage and repair (Theme 1).
Apply understanding of the principles of normal movement and the structure and function of the nervous system to select, plan, justify and discuss appropriate assessment and treatment techniques for patients with predictable neurological deficits (Theme 2).
Critically appraise the evidence base for treatment approaches to movement control (Theme 2).
Evaluate and select appropriate outcome measures for patients with predictable neurological deficits (Theme 2).
Key/transferable skills Apply knowledge of biomechanics and current legislation in
order to demonstrate safe and effective moving and handling in line with current legislation.
Use clinical reasoning and problem solving to plan and discuss assessment and treatment approaches for patients with predictable neurological deficits (Theme 2).
Access and critically appraise a comprehensive range of available evidence that underpins possible assessment and patient management choices (Theme 2).
Demonstrate an ability to reflect and be self-critical in the identification of appropriate learning needs and independently take responsibility for academic action planning.
Assist others in the identification of their learning needs. Communicate their learning through a variety of media and
engage confidently in academic and professional communication with others.
Work as part of a team to discuss plans for patient focused, achievable and realistic treatment goals that take into account patients’ psychological and socio-economic needs (Theme 2).
Discuss the role of members of the multi-disciplinary team involved in the management of patients with selected predictable neurological deficits and the role of the physiotherapist in this team (Theme 2).
Practical skills Demonstrate and document appropriate, safe and accurate
assessment and physiotherapy management techniques suitable for patients with predictable neurological deficits (Theme 2).
Apply a specified range of inclusive, non-discriminatory rehabilitation approaches in order to deliver holistic, patient focused care to a specified population suffering from predictable neurological deficits (Theme 2).
201
Practice Education
202

Programme Design and Organisation
UNIT TITLE Patient Management 2SUBJECT AREA
Physiotherapy Rehabilitation:Theme 1 – Musculoskeletal Theme 2 – Cardio-Respiratory
UNIT LEARNING OUTCOMES
Unless stated all the following Learning Outcomes apply to both themes. The student will be able to:
Knowledge and Understanding Demonstrate a comprehensive and systematic understanding
of the structure and functions of the lower quadrant and of the changes that occur due to pathology (Theme 1).
Demonstrate a comprehensive and systematic understanding of normal respiration and the cardiac cycle and of the changes that occur due to pathology (Theme 2).
Analyse the role of the physiotherapist within the health care team related to a range of musculoskeletal and cardio-respiratory conditions.
Cognitive/Intellectual Skills Analyse the pathology and clinical features of selected,
predictable pathologies and relate these to the structure and function of the lower quadrant (Theme 1).
Analyse the pathology and clinical features of selected, predictable pathologies of the cardio-respiratory system and relate these to the structure and function of the cardio-respiratory system (Theme 2).
Critically apply and synthesise their knowledge in order to select, plan, explain and evaluate appropriate assessment techniques for patients with selected, predictable pathologies of the lower quadrant and for patients with selected, predictable pathologies of the cardio-respiratory system and use clinical reasoning in order to interpret the findings.
Apply knowledge, problem solving and clinical reasoning skills in order to select, plan, explain, evaluate and apply a range of appropriate physiotherapy management techniques for patients with selected, predictable pathologies of the upper quadrant and for patients with selected, predictable pathologies of the cardio-respiratory system.
Critically evaluate and justify a range of outcome measures for used to monitor patients with pathologies of the lower quadrant and the cardio-respiratory system.
Work effectively as part of a team to suggest patient focused, achievable and realistic goals of treatment that take into account patients’ psychological and socio-economic needs.
Key/transferable skills Use clinical reasoning and problem solving to select, plan,
explain and evaluate the assessment and treatment of patients with selected, predictable pathologies of the lower
203

Practice Education
quadrant and for patients with selected, predictable pathologies of the cardio-respiratory system.
Critically apply knowledge learnt in previous units to selected, predictable pathologies of the upper quadrant and the cardio-respiratory system.
Access, critically appraise and evaluate a range of evidence that underpins their assessment and patient management choices.
Demonstrate an ability to reflect and be self-critical in the identification of appropriate learning needs and independently take responsibility for academic action planning.
Assist others in the identification of learning needs.
Practical Skills Demonstrate and document appropriate, safe and accurate
assessment and physiotherapy management techniques suitable for patients with selected, predictable pathologies of the lower quadrant and for patients with selected, predictable pathologies of the cardio-respiratory system.
Apply a range of inclusive, non-discriminatory rehabilitation approaches in order to plan holistic, patient focused care to patients presenting with selected, predictable pathologies of the lower quadrant and for patients with selected, predictable pathologies of the cardio-respiratory system.
Demonstrate and practise teaching self-management techniques for selected, predictable pathologies of the lower quadrant and the cardio-respiratory system.
204

Programme Design and Organisation
UNIT TITLE Patient Management 3
SUBJECT AREA
Physiotherapy Rehabilitation – Musculoskeletal (Upper quadrant)
UNIT LEARNING OUTCOMES
Unless otherwise stated all the following learning outcomes apply to both unit themes. The student will be able t
Knowledge and Understanding Explain the structure and functions of the upper quadrant Explain the pathophysiology, aetiology and clinical features
of complex, less predictable pathologies of the upper quadrant and.
Discuss the role of physiotherapy and work effectively as part of a team to suggest patient focused, achievable and realistic goals of treatment that take into account patients with complex psychological and socio-economic needs.
Cognitive/Intellectual Skills Analyse the pathology and clinical features of patients with
selected complex, less predictable pathologies of the upper quadrant and relate this to the relevant structure and function.
Critically apply and synthesise their knowledge in order to select, plan, explain and evaluate appropriate assessment techniques for patients with complex, less predictable pathologies of the upper quadrant and use clinical reasoning in order to interpret the findings.
Apply their knowledge in order to enable a high level of clinical reasoning and problem solving in order to select, plan, justify and evaluate a range of appropriate physiotherapy management techniques for patients with complex, less predictable pathologies of the upper quadrant.
Critically evaluate a range of outcome measures and select and justify appropriate outcome measures for patients with complex, less predictable pathologies of the upper quadrant.
Key/transferable skills Use clinical reasoning and problem solving to select, plan,
explain and evaluate the assessment and treatment of patients with complex, less predictable pathologies of the upper quadrant.
Critically apply knowledge learnt in previous units to complex, less predictable pathologies of the upper quadrant.
Access, critically appraise and evaluate a range of evidence that underpins their assessment and patient management choices.
Demonstrate an ability to reflect and be self-critical in the identification of appropriate learning needs and
205

Practice Education
independently take responsibility for academic action planning and manage own requirements for continuing professional development.
Assist others in the identification of their learning needs.
Practical Skills Demonstrate and document appropriate, safe and accurate
assessment and physiotherapy management techniques for patients with complex, less predictable pathologies of the upper quadrant.
Apply a range of inclusive, non-discriminatory rehabilitation approaches in order to deliver holistic, patient focused care to a patients presenting with complex, less predictable pathologies of the upper quadrant
206

Practice Education
UNIT TITLE The Autonomous Practitioner
SUBJECT AREA Professional Practice
UNIT LEARNING OUTCOMES
The student will be able to:
Cognitive/intellectual skills Demonstrate a systematic understanding and critical
awareness of factors underpinning professional autonomy and accountability.
Demonstrate a systematic understanding and critical awareness of factors underpinning effective professional relationships.
Demonstrate a systematic understanding and critical awareness of factors that contribute to the development of effective personal and professional skills.
Articulate the responsibilities of a registered professional within the wider health and social care context.
Critically reflect upon previous experience of practice placements using a variety of methods.
Demonstrate the ability to use clinical reasoning and systematic evaluation of evidence-based practice in order to justify all decision making in practice.
Critically appraise the relevance of professional, statutory and government requirements on their practice
Key transferable skills Reflect on their own and others working in order to prioritise
learning needs and develop future practice. Work effectively with others, as a member or a leader of a
group, towards a common goal and meet obligations to others.
UNIT TITLE Critical Thinking / Project
207

Practice Education
SUBJECT AREA Research
UNIT LEARNING OUTCOMES
The student will be able to:
Apply and integrate relevant aspects of knowledge, understanding, skills and experiences developed in previous units of the programme.
Systematically search for, analyse and critically appraise the findings and writing of others relevant to the research being undertaken. Select, synthesise and manage information in order to undertake their research task.
Use logical and reasoned argument to support their project and discuss the diversity of arguments and contradictions in the evidence base.
Design and discuss an appropriate and realistic research methodology to effectively address the objectives of their project.
Discuss the importance of ethical issues related to the proposed research.
Discuss and apply appropriate statistical methods. Produce a scholarly piece of work.
UNIT TITLE Patient Management 4SUBJECT AREA
Physiotherapy Rehabilitation: Theme 1 – NeurologyTheme 2 – Cardio-respiratory
UNIT LEARNING OUTCOMES
Unless otherwise stated all the following learning outcomes apply to both unit themes. The student will be able to:Knowledge and Understanding Explain the pathophysiology, aetiology and clinical features of
complex, less predictable pathologies the cardio-respiratory system.
Discuss the structure of the cardio-respiratory system in relation to its function and analyse how dysfunction in this system influences others, specifically the renal and pulmonary systems (Theme 2).
Demonstrate an in depth understanding of exercise physiology in order to prescribe, justify and evaluate prescription for the respiratory patient (Theme 2).
Discuss the role of physiotherapy and work effectively as part of a team to suggest patient focused, achievable and realistic goals of treatment that take into account patients with complex psychological and socio-economic needs.
Critically apply their knowledge of the neuromuscular control of normal movement and the structure and function of the nervous system to explain the clinical features of complex and
208

Practice Education
less predictable neurological deficits.
Cognitive/Intellectual Skills Analyse the pathology and clinical features of patients with
selected complex, less predictable pathologies of patients with selected complex, less predictable pathologies of the cardio-respiratory system and relate this to the relevant structure and function.
Critically apply and synthesise their knowledge in order to select, plan, explain and evaluate appropriate assessment techniques for patients with complex, less predictable pathologies of the cardio-respiratory system and use clinical reasoning in order to interpret the findings.
Apply their knowledge in order to enable a high level of clinical reasoning and problem solving in order to select, plan, justify and evaluate a range of appropriate physiotherapy management techniques for patients with complex, less predictable pathologies of the cardio-respiratory system.
Critically evaluate a range of outcome measures and select and justify appropriate outcome measures for patients with complex, less predictable pathologies of the cardio-respiratory system.
Apply their understanding of the principles of normal movement and the structure and function of the nervous system to select, plan, justify and evaluate appropriate assessment and treatment techniques for patients with complex and less predictable neurological deficits.
Evaluate, critically appraise and select appropriate outcome measures from a range of outcome measures suitable for patients with complex and less predictable neurological deficits.
Key/transferable skills Use clinical reasoning and problem solving to select, plan, explain
and evaluate the assessment and treatment of patients with complex, less predictable pathologies of the cardio-respiratory system.
Critically apply knowledge learnt in previous units to complex, less predictable pathologies of cardio-respiratory system.
Access, critically appraise and evaluate a range of evidence that underpins their assessment and patient management choices.
Demonstrate an ability to reflect and be self-critical in the identification of appropriate learning needs and independently take responsibility for academic action planning and manage own requirements for continuing professional development.
Assist others in the identification of their learning needs. Discuss the roles of multi-disciplinary team members in the delivery
and implementation of patient focused, specific, measurable, achievable and timed goals that take into account the patients psychological and socio-economic needs.
Independently clinically reason and problem solve to select, plan, justify and evaluate the assessment and treatment of patients with
209
Practice Education
complex and less predictable neurological deficits in a variety of clinical settings.
Apply knowledge learnt in previous units to complex and less predictable neurological deficits
Access and critically appraise a range of evidence that underpins their assessment and patient management choices
Demonstrate an ability to reflect and be self-critical in the identification of appropriate learning needs and independently take responsibility for academic action planning and manage own requirements for continuing professional development.
Assist others in the identification of learning needs. Communicate their learning through a variety of media and engage
confidently in academic and professional communication with others.
Practical Skills Demonstrate and document appropriate, safe and accurate
assessment and physiotherapy management techniques for patients with complex, less predictable pathologies of the cardio-respiratory system.
Apply a range of inclusive, non-discriminatory rehabilitation approaches in order to deliver holistic, patient focused care to a patients presenting with complex, less predictable pathologies of the cardio-respiratory system.
Use their knowledge of patients with complex and less predictable neurological deficits to execute and document a range of safe, accurate assessment and treatment techniques that are appropriate for this group of patients.
Apply a range of inclusive, non-discriminatory rehabilitation approaches (including restorative, supportive and palliative) in order to deliver holistic, patient focused care to a diverse population with complex and less predictable neurological deficits.
UNIT TITLE Evidence Based Practice
SUBJECT AREA Evidence based practice in physiotherapy
UNIT LEARNING OUTCOMES
The student will reflect on prior learning in order to select topics for further study from a range of topics offered.
The student will be able to apply existing knowledge in order to: Systematically and critically evaluate relevant literature to
include Government policy initiatives underpinning evidence-based practice.
Synthesise and analyse research findings in order to make value judgements about their contribution to the clinical evidence base.
Develop reasoned arguments in order to evaluate clinical
210

Practice Education
decisions. Engage effectively in debate, arguing and evaluating a variety
of viewpoints in a professional manner to produce detailed and coherent arguments.
Critically examine and reflect on their own practice and their own implementation of best available evidence and develop an understanding of some of the problems of implementing research findings into clinical practice.
UNIT TITLE Clinical Observation
SUBJECT AREA
Professional Practice
UNIT LEARNING OUTCOMES
The student will have:
developed basic interpersonal skills in a clinical setting; had an opportunity to observe physiotherapists working in a
variety of health care settings; reflected upon their learning experiences.
UNIT TITLE Practice Placements 1 to 5
SUBJECT AREA
Professional Practice
UNIT LEARNING OUTCOMES
There are 17 learning outcomes, which are divided into 5 categories. These reflect the aspects of practice that are assessed in the Practice Placement Common Assessment Tool, and were formulated with reference to the HPC Standards of Proficiency:
Interpersonal skillsThe student will:
1. demonstrate effective and appropriate skills in communication in order to collaborate and work effectively in partnership with others (professionals, support staff, patients/clients, carers, relatives and
211

Practice Education
external agencies) to the benefit of the client/patient and maximise health outcomes.
2. contribute effectively to work undertaken as part of a team.
3. recognise the scope of practice of other professionals.4. acknowledge cross professional boundaries.5. make appropriate referrals to others.
Management of selfThe student will:
6. demonstrate effective self management of workload.7. know the limits of their own practice and when to seek
advice.8. independently manage their own learning.
Management of patientThe student will:
9. gather appropriate information relating to the patient.10. plan and carry out an appropriate objective examination.11. analyse examination findings and formulate a written
treatment plan in partnership with the patient.12. implement and critically evaluate the impact of, or
response to, treatment interventions.
DocumentationThe student will:
13.maintain accurate patient records.
Professional practiceThe student will
14.promote patient centred care.15.comply with the CSP Rules of Professional Conduct.16.practise in line with relevant health and safety policy.17.work independently and as part of a team as appropriate.
UNIT TITLE Practice Placement 6 (Elective)
SUBJECT AREA Professional Practice
UNIT LEARNING OUTCOMES
The learning outcomes were formulated with reference to the HPC Standards of Proficiency, CSP Core Standards of Physiotherapy Practice and CSP Rules of Professional Conduct. The student will: demonstrate effective and appropriate skills in
communication in order to collaborate and work effectively in partnership with others (professionals, support staff, patients/clients, carers, relatives and external agencies) to the benefit of the client/patient and to maximise health outcomes.
212

Practice Education
contribute effectively to work undertaken as part of a team.
acknowledge cross professional boundaries. make appropriate referrals to others. demonstrate effective self management of workload. demonstrate knowledge and understanding of the limits
of their own practice and work within their own scope of practice.
recognise the scope of practice of other professionals. independently manage their own learning. gather appropriate information relating to the patient. plan and carry out appropriate objective examinations. analyse examination findings and formulate written
treatment plans in partnership with the client/patient. implement and critically evaluate the impact of, or
response to, treatment interventions. maintain accurate patient records. promote patient centred care. comply with the CSP Rules of Professional Conduct. practice in line with relevant health and safety policy.
213

Practice Education
Sequencing of Units BSc (Hons)The curriculum for the BSc (Hons) physiotherapy programme is also structured around the theme of rehabilitation and various approaches are considered: preventative, maintenance, restorative and palliative, all within case-based clinical scenarios. Units have been sequenced to enable students to apply learning from one unit to another and / or to allow students to build on knowledge gained in earlier units by tackling similar but more complex themes at later stages.
In both the first and second year units the students are prepared for their clinical placements by covering areas such as : the philosophy of placements; roles and responsibilities of all parties; placement learning outcomes and assessment procedures; discussions with more experienced pre-registration students about their placement experiences; an introduction to Learning Development Plans and development of a Professional Development Portfolio. The units also include the mandatory training of CPR, fire lecture, infectious control and manual handling
Additional sessions include role plays to explore issues of conflict; skills sessions linked to simulated practice scenarios; a meeting with the Visiting Lecturer to discuss roles and responsibilities of all parties and plan the Visiting Lecturer’s first clinical visit.
In order to ensure students are fully prepared for the clinical environment, students will not be allowed to commence Practice Placement 1 until they have successfully passed all units in their second year. They will thus be prepared to practice, apply and develop appropriate physiotherapy theory and practice in a variety of practice locations, and develop interpersonal and management skills. Debrief sessions are incorporated in the third year units to encourage reflection, conclusion and planning for future clinical experiences.
Structure of the BSc (Hons) Physiotherapy ProgrammeThe BSc (Hons) Programme is undergoing a significant transition following two major events which has resulted in the restructure of all 3 years. These events include the review in 2009 and an initiative introduced by the MMU in 2010 known as EQUAL (Enhancing Quality and Assessment for Learning). This has resulted in a different structure and a change in title for a number of units for all 3 cohorts although the content delivered has remained relatively unchanged .
The structure therefore for all 3 years have been included with the third year (2009-2012 cohort) in addendum 1, second years (2010-2013 cohort) in addendum 2 and the structure the first years (2011-2014) in addendum 3 together with the curriculum content for all three programmes..
214

Programme Design and Organisation
215

Practice EducationUNIT TITLE Foundations in Professional Practice
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Physiotherapy
UNIT LEADER(S) Janet Morrison
CREDIT VALUE 20 CREDITS AT LEVEL: 4
AMOUNT OF STUDENT EFFORT (HOURS) 200
CLASS CONTACT TIME (HOURS) 65
UNIT STATUS Mandatory Core
PRE-REQUISITES None
CO-REQUISITES None
UNIT LEARNING OUTCOMES The student will be able toKnowledge and Understanding Describe how professional, statutory and regulatory body requirements impact on
their learning experience. Describe models of reflection and explain the need for reflective practice Explain with guidance the factors that contribute to evidence-based practice.Cognitive/Intellectual Skills Demonstrate an awareness of the importance of lifelong learning and continuing
professional development. Demonstrate an awareness of the need for equity of healthcare provision to a
diverse population. Describe a variety of approaches to rehabilitation and explain their relevance to
health.Key/transferable skills Communicate effectively using methods appropriate to physiotherapy practice. Demonstrate the application of research skills Work effectively with others as a member of a group and meet obligations to
others. Use appropriate study skills / information skills to support and enhance their
learning.
CURRICULUM OUTLINE Study skills – information skills (retrieval & analytical skills), reading, writing, note taking, etc.Roles and functions of professional, statutory and regulatory bodies. Rules of Professional ConductContinuing professional development, life long learning agenda.Diversity & cultural competence, promoting equality & people’s rights / responsibilitiesRehabilitation – social, medical models; preventative (including introduction to health promotion), restorative, maintenance, palliative approaches of rehabilitation, major approaches to psychology and their relevance to health; psychological factors affecting health.Evidence based practice, guidelines, protocols, and integrated care pathways.Research skills – critical appraisal, reliability, validity, research questions/hypotheses, qualitative and quantitative research methods, statistical analysis, the research process. Outcome measures.Introduction to research & practice ethics, patient confidentiality. Research / audit and how it underpins practice.Reflective practice, models of reflection, reflective writing and introduction to portfolio development.
TEACHING & LEARNING STRATEGIES
A variety of approaches will be used including lead lectures, self & directed study, tutorials, seminars, presentations, e-learning. Ref part time route
ASSESSMENT STRATEGIES Info Skills Workbook – formative but compulsory completionReflective log/diary – formativeReflective writing evidencing intended learning outcomes (2000 words – summative).
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate: an understanding of the unit content an ability to use and record in a written format simple reflection on a topic/situation
216
Practice Education a basic understanding of the models of reflection and the need to include reflection
in professional practice an ability to recognise the role of reflection in the development of lifelong learning
skills
217

Practice EducationUNIT TITLE Human Movement
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Physiotherapy – Human Movement
UNIT LEADER Glenis Donaldson
CREDIT VALUE 20 CREDITS AT LEVEL: 4
AMOUNT OF STUDENT EFFORT (HOURS) 200
CLASS CONTACT TIME (HOURS) 65
UNIT STATUS Mandatory Core
PRE-REQUISITES None
CO-REQUISITES None
UNIT LEARNING OUTCOMES The student will be able to:Knowledge and Understanding Explain the basic structure and function of the cardiovascular, musculoskeletal and
nervous systemsCognitive/Intellectual Skills Apply a knowledge of biomechanics to the analysis of normal human movement Explain how the major systems of the body contribute to normal human movement Use a knowledge of histology and physiology to explain soft tissue damage and
repairPractical Skills Demonstrate safe and effective moving and handling in line with current legislation
CURRICULUM OUTLINE The students will explore the structure and function of major systems of the body and relate their structure and function to human movement.This unit will cover biomechanics, histology and tissue repair and physiology. The specific systems for consideration will be the cardio-vascular system, the musculo-skeletal system and the nervous system.
TEACHING AND LEARNING STRATEGIES Makes strong use of student centred learning strategies with tutors creating both a
challenging and supportive environment using a variety of delivery methods in conjunction with both indicative reading and material accessed by the students themselves. A variety of strategies are used including theatre events, practical demonstrations, group work, skills sessions and tutorials.Tutors will be drawn from both academic and clinical backgrounds.The teaching and learning will be case-based and will use a problem solving approach.
ASSESSMENT STRATEGIES Analysis of movement workshops - Formative Analysis of movement 2000 word written report – summative
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate: an understanding of how the structure and function of the major systems of the
body contribute to human movement an understanding of the principles of movement analysis an ability to carry out a basic analysis of movement an ability to record an analysis of movement in a written report an ability to write in an appropriate academic format
Formative assessment procedures will be assessed by peer assessment using self evaluation checklists linked to the unit learning outcomes with personal tutor support/academic action planning.
218

Practice EducationUNIT TITLE Physiotherapy Management 1
UNIT CODE NUMBER
HOME PROGRAMME BSc. (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Physiotherapy Rehabilitation - Neurological
UNIT LEADER Rachel Stockley
CREDIT VALUE 20CREDITS AT LEVEL:
4
AMOUNT OF STUDENT EFFORT (HOURS)
200CLASS CONTACT TIME (HOURS)
65
UNIT STATUS Mandatory Core
PRE-REQUISITES Human Movement
CO-REQUISITES Foundations in Professional Practice
UNIT LEARNING OUTCOMESThe student will be able to:
Development of Knowledge and Understanding Use their knowledge of the neuromuscular control of normal movement and the
structure and function of the nervous system to explain the clinical features of selected predictable neurological deficits
Work as part of a team to suggest patient focussed, achievable and realistic goals of treatment that take into account the patients psycho-socio-economic needs
Identify the members of the multi-disciplinary team involved in the management of selected predictable neurological deficits and the role of the physiotherapist in this team
Cognitive/Intellectual Skills Apply their knowledge of the principles of normal movement and the structure
and function of the nervous system to select, plan, explain and with guidance evaluate appropriate assessment and treatment techniques for patients with predictable neurological deficits
Evaluate, with guidance, appropriate outcome measures for patients with predictable neurological deficits
Key/transferable skills Use basic clinical reasoning and problem solving to plan, explain and with
guidance evaluate the assessment and treatment of patients with predictable neurological deficits
Apply knowledge learnt in previous units to predictable neurological deficits Access and with guidance appraise the available evidence that underpins their
assessment and patient management choices Demonstrate an ability to identify appropriate learning needs and with
guidance take responsibility for academic action planning. Communicate their learning in a written format that fulfils the requirements of
academic writingPractical Skills Use their knowledge of patients with predictable neurological deficits to
execute and document safe, accurate assessment and treatment techniques that are appropriate for this group of patients.
Apply a specified range of inclusive, non-discriminatory rehabilitation approaches in order to deliver holistic, patient focussed care to a specified population suffering from predictable neurological deficits.
CURRICULUM OUTLINE This unit is intended to develop the student’s attitudes, skills and knowledge related to the physiotherapy assessment and management of the patient with the neurological deficits considered during the unit. Principles will be based on the Bobath concept, Carr and Shepherd’s Motor relearning approach and the application of anatomical and physiological knowledge of the CNS Functional outcome measures.
The structure of the unit will allow the student to develop the clinical reasoning skills that will underpin physiotherapy practice
219
Practice Education
TEACHING AND LEARNING STRATEGIES
Makes strong use of student centred learning strategies with tutors creating both a challenging and supportive environment using a variety of delivery methods in conjunction with indicative reading. A variety of strategies are used including theatre events, practical demonstrations, group work/role play, skills sessions and tutorials.Tutors will be drawn from both academic and clinical backgrounds.The teaching and learning will be case-based and use a problem solving approach.
ASSESSMENT STRATEGIES Self evaluation questionnaire linked to unit and session learning outcomes -
Formative Case based pathology and physiotherapy management 2000 word written
assignment – summative
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate:
an ability to relate the structure and function of the nervous system to the pathology and clinical features of selected neurological deficits and their physiotherapy management
basic clinical reasoning and problem solving skills an ability to select relevant information and use appropriately to support their
answers an ability to structure their ideas in a logical and organized manner an ability to present their answer in an appropriate academic formatFormative assessment procedures will be assessed by self evaluation questionnaire linked to the unit/session learning outcomes with personal tutor support/academic action planning.
Summative assessment procedures will be assessed through generic level 1 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
220

Practice Education
UNIT TITLE Physiotherapy Management 2
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Physiotherapy Rehabilitation - musculoskeletal
UNIT LEADER(S) Sally Hartley
CREDIT VALUE 20 credits CREDITS AT LEVEL: 4
AMOUNT OF STUDENT EFFORT (HOURS)
200 CLASS CONTACT TIME (HOURS)
65 hours
UNIT STATUS Mandatory Core
PRE-REQUISITES Human Movement
CO-REQUISITES Foundations in Professional Practice
UNIT LEARNING OUTCOMES The student will be able to:
Development of Knowledge and Understanding Describe and explain the structure and function of the upper quadrant Work as part of a team to suggest patient focussed, achievable and realistic goals
of treatment that take into account the patients psycho-socio-economic needsCognitive/Intellectual Skills Relate the pathology and clinical features of selected, predictable pathologies to
the structure and function of the upper quadrant Apply their knowledge in order to select, plan, explain and with guidance evaluate
appropriate assessment techniques for patients with predictable pathologies of the upper quadrant and with guidance interpret the findings.
Apply their knowledge in order to select, plan, explain and with guidance evaluate appropriate physiotherapy management techniques for patients with predictable pathologies of the upper quadrant
Evaluate, with guidance appropriate outcome measures for patients with predictable pathologies of the upper quadrant
Key/transferable skills Use basic clinical reasoning and problem solving to select, plan, explain and with
guidance evaluate the assessment and treatment of patients with predictable pathologies of the upper quadrant
Apply knowledge learnt in previous units to predictable pathologies of the upper quadrant
Access and with guidance appraise the available evidence that underpins their assessment and patient management choices
Demonstrate an ability to identify appropriate learning needs and with guidance take responsibility for academic action planning.
Practical Skills Demonstrate and document appropriate, safe and accurate assessment and
physiotherapy management techniques for patients with predictable pathologies of the upper quadrant
Apply a specified range of inclusive, non-discriminatory rehabilitation approaches in order to deliver holistic, patient focussed care to a specified population suffering from predictable pathologies of the upper quadrant
CURRICULUM OUTLINE This unit is intended to develop both cognitive and psychomotor skills in the undergraduate physiotherapist. The main principles are the integration and application of anatomical knowledge to selected pathologies of the upper quadrant which will enable the student to clinically reason and explain their clinical decisions. This unit covers functional anatomy, biomechanics, surface marking, differential diagnosis and treatment of pathologies in the following regions;Cervical spine, thoracic spine, shoulder, elbow, forearm, wrist and hand.
TEACHING AND LEARNING STRATEGIES
Makes strong use of student centred learning strategies with lecturers creating both a challenging and supportive learning environment using a variety of delivery methods in conjunction with indicative reading. A variety of strategies are used including; illustrated lectures, practical demonstrations, tutorials, e-learning, group work, role play and case based problem solving.
221

Practice Education
ASSESSMENT STRATEGIES Oral practical workshops / group work assessment /treatment skills - Formative Oral practical Examination (assessment and treatment skills) 30 minutes –
summative
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate: an ability to relate the structure and function of the upper quadrant to the pathology
and clinical features of selected musculoskeletal pathologies and their physiotherapy management
an ability to plan, discuss and explain the assessment, treatment and rehabilitation approach for patients with selected musculoskeletal pathologies
an ability to safely and accurately demonstrate physiotherapy assessment and management techniques for the selected pathologies
an ability to practice within the rules of professional conduct an ability to communicate clearly, coherently and using appropriate terminology
with both patients and colleagues.
Formative assessment procedures will assessed by peer/self evaluation checklists linked to the unit/session learning outcomes with personal tutor support/academic action planning.
Summative assessment procedures will be assessed through generic level 1 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
222

Practice EducationUNIT TITLE Health & Social Care
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Health and Social Care
UNIT LEADER(S) Jill Bailey
CREDIT VALUE 20 credits CREDITS AT LEVEL: 4
AMOUNT OF STUDENT EFFORT (HOURS)
200 CLASS CONTACT TIME (HOURS)
65 hours
UNIT STATUS Mandatory Core
PRE-REQUISITES None
CO-REQUISITES Foundations in Professional Practice
UNIT LEARNING OUTCOMES The student will be able toKnowledge and Understanding Describe the range of environments in which health & social care is delivered. Describe the organisation of health and social care services in the UK. Identify the key drivers of health and social care policy in the UK.Cognitive/Intellectual Skills Compare different models of health & social care. Identify the relationship between healthcare services and social care services. Apply their knowledge of teamwork to the delivery of healthcare provision.
CURRICULUM OUTLINE Key characteristics of primary care, secondary care, intermediate care, tertiary care, residential care, private health care, voluntary care, respite care, non traditional healthcare environments, educational & occupational settings.The multi-agency perspective including the role of carersCurrent health, social & educational policy relevant to the delivery of physiotherapy services – NSF’s, evidence based practice, clinical governance, guidelines, protocols, inclusion, reducing inequalities, making a difference in schools, Health inequalitiesDiversityPerson centred / patient centred / patient focussed careTeamwork – inter disciplinary, uni-disciplinary, skills of team workingEthical practice
TEACHING AND LEARNING STRATEGIES
A variety of approaches will be used including lead lectures, self & directed study, tutorials, seminars, presentations, e learning, group discussion.
ASSESSMENT STRATEGIES Group presentation & peer evaluation of group work - Formative Group presentation followed by group question & answers (70% of unit) –
summative 750 word written reflection on the group activity (30% of unit) - summative
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate:
an understanding of the unit content an ability to work within a group to develop and deliver an oral presentation an ability to communicate information both visually and orally an ability to answer questions related to information presented an ability to analyse their own and the contribution of others to a team task an ability to give and receive peer feedback an ability to use and record in a written format a reflection on group activity
Formative assessment procedures will assessed by : formative written feedback from academic staff related to presentation skills oral peer evaluation of presentation skills and teamwork
223

Practice EducationUNIT TITLE Physiotherapy Management 3
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Physiotherapy Rehabilitation - Cardiorespiratory
UNIT LEADER(S) Daphne Dawson
CREDIT VALUE 20 CREDITS AT LEVEL: Level 4
AMOUNT OF STUDENT EFFORT (HOURS)
200 CLASS CONTACT TIME (HOURS)
65
UNIT STATUS Mandatory Core
PRE-REQUISITES Human Movement Physiotherapy management units 1 & 2
CO-REQUISITES Foundations in Professional Practice Health and Social Care
UNIT LEARNING OUTCOMES The student will able to:Development of Knowledge and Understanding Identify and explain normal respiration and the changes that occur as a result of
disease Identify and explain normal cardiac function and the changes that occur as a result
of disease Work as part of a team to suggest patient focussed, achievable and realistic goals
of treatment that take into account the patients psycho-socio-economic needs Identify the members of the multi-disciplinary team involved in the management of
predictable cardio-respiratory pathology and the role of the physiotherapist in this team
Cognitive/Intellectual Skills Apply their knowledge of predictable cardio-respiratory patho-physiology to select,
plan, explain and with guidance evaluate appropriate assessment and physiotherapy management techniques for patients with uncomplicated, predictable cardio-respiratory pathology.
Evaluate, with guidance, appropriate outcome measures for monitoring patients with uncomplicated, predictable cardio-respiratory pathology.
Key/transferable skills Use basic clinical reasoning and problem solving to select, plan, explain and
with guidance evaluate the assessment and treatment of patients with uncomplicated, predictable cardio-respiratory pathology
Apply knowledge learnt in previous units to uncomplicated, predictable cardio-respiratory pathology
Access and with guidance appraise the available evidence that underpins their assessment and patient management choices
Demonstrate an ability to identify appropriate learning needs and with guidance take responsibility for academic action planning.
Practical Skills Demonstrate and document appropriate, safe and accurate assessment and
physiotherapy management techniques for patients with uncomplicated, predictable cardio-respiratory pathology
Demonstrate and teach appropriate self management techniques for patients with uncomplicated, predictable cardio-respiratory pathology
Apply a specified range of inclusive, non-discriminatory rehabilitation approaches in order to deliver holistic, patient focussed care to a specified population with uncomplicated, predictable cardio-respiratory pathology
CURRICULUM OUTLINE This unit is intended to develop both cognitive and psychomotor skills of the student in the assessment and treatment of uncomplicated cardiorespiratory conditions in primary and secondary healthcare settings. The unit covers basic cardio-respiratory physiology, functional and applied anatomy, biomechanics, examination and management of the above conditions.
TEACHING AND LEARNING STRATEGIES
Strong use will be made of student centred, case based problem solving learning strategies. Tutors create a challenging and supportive environment using a variety of learning and tutor methods in conjunction with directed study. This will include lectures, tutorials, group work and practical skills workshops.
224

Practice Education
ASSESSMENT STRATEGIES Self evaluation questionnaire linked to unit and session learning outcomes –
Formative Case based clinical reasoning examination (pre-released case) 2 hours –
summative
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
basic knowledge of the unit content a deeper understanding of unit content and a the ability to relate the
knowledge to the case study patients presentation and treatment apply their knowledge of cardio respiratory physiology to explain either
pathology clinical features assessment treatment
of the case study patient.
select and use appropriate information relevant to the topic and the case study patient.
Formative - assessed by self evaluation questionnaire linked to the unit/session learning outcomes with personal tutor support/academic action planning.
Summative assessment procedures will be assessed through generic level 1 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
225

Practice EducationUNIT TITLE Physiotherapy Management 4
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA PhysiotherapyRehabilitation - Neurological
UNIT LEADER Deborah O’Connor
CREDIT VALUE 20CREDITS AT LEVEL:
5
AMOUNT OF STUDENT EFFORT (HOURS)
200CLASS CONTACT TIME (HOURS)
50
UNIT STATUS Mandatory Core
PRE-REQUISITES All Level 1 Units
CO-REQUISITES
UNIT LEARNING OUTCOMES The student will be able to:Development of Knowledge and Understanding Critically apply their knowledge of the neuromuscular control of normal movement
and the structure and function of the nervous system to explain the clinical features of complex and less predictable neurological deficits
Develop the ability to collaborate with both patients and the multi-disciplinary team to suggest patient focussed, specific, measurable, achievable and timed goals that take into account the patients psycho-socio-economic needs
Collaborate with and suggest the referral of patients to the appropriate member of the MDT and identify how each professional can contribute to the delivery of holistic, patient focussed care for patients with complex and less predictable neurological deficits
Cognitive/Intellectual Skills Apply their knowledge of the principles of normal movement and the structure
and function of the nervous system to select, plan, justify and evaluate appropriate assessment and treatment techniques for patients with complex and less predictable neurological deficits
Evaluate and select appropriate outcome measures from a range of outcome measures suitable for patients with complex and less predictable neurological deficits
Key/Transferable Skills Use clinical reasoning and problem solving to select, plan, justify and evaluate
the assessment and treatment of patients with complex and less predictable neurological deficits in a variety of clinical settings
Apply knowledge learnt in previous units to complex and less predictable neurological deficits
Access and critically appraise the available evidence that underpins their assessment and patient management choices
Demonstrate an ability to evaluate appropriate learning needs and with guidance take responsibility for academic action planning
Practical Skills Use their knowledge of patients with complex and less predictable
neurological deficits to execute and document a range of safe, accurate assessment and treatment techniques that are appropriate for this group of patients.
Apply a range of inclusive, non-discriminatory rehabilitation approaches (including restorative, supportive and palliative) in order to deliver holistic, patient focussed care to a diverse population suffering from complex and less predictable neurological deficits
CURRICULUM OUTLINE This unit is intended to develop the student’s attitudes, skills and knowledge related to the physiotherapy assessment and management of patients with complex neurological deficits considered during the unit. Principles will be based on the Bobath concept, Carr and Shepherd’s Motor relearning approach and the application of anatomical and physiological knowledge. The students will consider neurological impairment in different age groups and also consider the role of the physiotherapist in restorative, supportive and palliative care.A range of outcome measures relevant to patients with complex neurological deficits
226

Practice Education
TEACHING AND LEARNING STRATEGIES
Makes extensive use of student centred learning strategies with tutors creating both a challenging and supportive environment using a variety of delivery methods in conjunction with both indicative reading and material accessed by the students themselves. A variety of strategies are used including theatre events, practical demonstrations, group work/role play, skills sessions and tutorials.Tutors will be drawn from both academic and clinical backgrounds.The teaching and learning will be case-based and use a problem solving approach. Greater complexity of the patient scenarios will promote clinical reasoning skills
ASSESSMENT STRATEGIES Group poster presentation - Formative Oral practical examination (video analysis/skills) 30 minutes – summative
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate:
An ability to use their knowledge of the neuromuscular control of normal movement and the structure and function of the nervous system to explain the clinical features and management of patients with more complex neurological deficits.
An ability to select, plan, justify and evaluate the most appropriate assessment, physiotherapy management and range of rehabilitation approaches for a described patient.
An ability to demonstrate a range of safe, appropriate, accurate and effective assessment skills, physiotherapy management skills and rehabilitation approaches for a described patient.
An ability to demonstrate holistic and patient focussed care An ability to practice within the rules of professional conduct An ability to communicate appropriately, clearly and coherently with
patients and colleagues
Formative assessment procedures will be assessed by peer assessment linked to the unit/session learning outcomes with personal tutor support/academic action planning.Summative assessment procedures will be assessed through generic level 2 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
227

Practice EducationUNIT TITLE Physiotherapy Management 5
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Physiotherapy Rehabilitation - Musculoskeletal
UNIT LEADER(S) Gillian Yeowell
CREDIT VALUE 20 credits CREDITS AT LEVEL: 5
AMOUNT OF STUDENT EFFORT (HOURS)
200 hours CLASS CONTACT TIME (HOURS)
50 hours
UNIT STATUS Mandatory Core
PRE-REQUISITES All Level 1 units
CO-REQUISITES
UNIT LEARNING OUTCOMES The student will be able to:
Development of Knowledge and Understanding Describe and explain the structure and function of the lower quadrant. Work as part of a team to suggest patient focussed, achievable and realistic goals
of treatment that take into account the patients psycho-socio-economic needs.Cognitive/Intellectual Skills Relate the pathology and clinical features of selected pathologies of the lower
quadrant to its structure and function. Apply their knowledge in order to select, plan, explain and evaluate appropriate
assessment procedures for patients with selected pathologies of the lower quadrant and interpret the findings.
Evaluate appropriate outcome measures for patients with selected pathologies of the lower quadrant
Key/transferable skills Clinically reason with reference to relevant literature appropriate management in
the rehabilitation of selected conditions in the lower quadrant including bio psychosocial factors.
Apply knowledge learnt in previous units to pathologies of the lower quadrant Access and appraise the available evidence that underpins their assessment
and patient management choices Demonstrate an ability to identify appropriate learning needs and take
responsibility for academic action planning.Practical Skills Plan, safely demonstrate and justify with reference to relevant literature
appropriate physiotherapy management strategies for specific pathological conditions in the lower quadrant
Apply a specified range of inclusive, non-discriminatory rehabilitation approaches in order to deliver holistic, patient focussed care to a specified population with selected pathologies of the lower quadrant
CURRICULUM OUTLINE This unit is intended to develop both cognitive and psychomotor skills in the undergraduate physiotherapist. The main principles are the integration and application of anatomical knowledge in conjunction with relevant biopsychosocial factors to selected pathologies of the lower quadrant which will enable the student to clinically reason, explain and justify their clinical decisions. This unit covers functional anatomy, biomechanics, surface marking, differential diagnosis and treatment of pathologies in the following regions;Lumbar spine, sacroiliac joint, hip, knee and ankle, and incorporates a range of rehab approaches
TEACHING AND LEARNING STRATEGIES
Makes strong use of student centred learning strategies with lecturers creating both a challenging and supportive learning environment using a variety of delivery methods in conjunction with indicative reading. A variety of strategies are used including; illustrated lectures, practical demonstrations, tutorials, critical appraisal, e-learning, group work and role play.
228

Practice Education
ASSESSMENT STRATEGIES Oral practical workshop - Formative 2000 word clinical pathology and physiotherapy management clinical reasoning
written assignment – summative
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The student will demonstrate:
An understanding of the unit content An ability to use clinical reasoning to explain the relationship between
pathology/clinical features and the physiotherapy management of patients with more complex lower quadrant pathologies
An ability to select, plan and justify appropriate physiotherapy management for a described patient
An ability to access, select and evaluate appropriate evidence to justify there physiotherapy management and rehabilitation approach
An ability to present written information in a logical, coherent and reasoned manner An ability to present their answer in an appropriate written academic style and
format
Formative assessment - peer assessment using self evaluation checklists linked to the unit/session learning outcomes with personal tutor support/academic action planning.
Summative assessment procedures will be assessed through generic level 2 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
229

Practice EducationUNIT TITLE Physiotherapy Management 6
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Physiotherapy Rehabilitation - Cardiorespiratory
UNIT LEADER(S) Daphne Dawson
CREDIT VALUE 20 CREDITS AT LEVEL: 5
AMOUNT OF STUDENT EFFORT (HOURS)
200 CLASS CONTACT TIME (HOURS)
50
UNIT STATUS Mandatory Core
PRE-REQUISITES All level 1 Units
CO-REQUISITES
UNIT LEARNING OUTCOMES The student will be able to:Development of Knowledge and Understanding Critically apply and explain their knowledge of normal respiration and the changes
that occur as a result of complex and less predictable disease, deformity or malformation
Critically apply and explain their knowledge of normal cardiac function and the changes that occur as a result of complex and less predictable disease, deformity or malformation
Explain the psycho-socio-economic issues for patients suffering from complex less predictable cardio-respiratory pathology and adapt the patients’ goals and management appropriately in order to deliver holistic, patient focussed care.
Develop the ability to collaborate with and refer to other members of the multi-disciplinary team involved in the management of complex and less predictable cardio-respiratory pathology and the explain role of the physiotherapist and other professionals in this team
Cognitive/Intellectual Skills Apply their knowledge of predictable cardio-respiratory patho-physiology to
select, plan, justify and evaluate a range of appropriate assessment and physiotherapy management techniques for patients with complex and less predictable cardio-respiratory pathology.
Evaluate a range of appropriate outcome measures for monitoring patients with complex and less predictable cardio-respiratory pathology.
Key/transferable skills Apply clinical reasoning and problem solving to select, plan, justify and
evaluate the assessment and treatment of patients with uncomplicated, predictable cardio-respiratory pathology in a variety of clinical settings
Apply knowledge learnt in previous units to complex and less predictable cardio-respiratory pathology
Access and critically appraise the available evidence that underpins their assessment and patient management choices
Demonstrate an ability to evaluate appropriate learning needs and with guidance take responsibility for academic action planning.
Practical Skills Demonstrate and document a range of appropriate, safe and accurate
assessment and physiotherapy management techniques for patients with complex and less predictable cardio-respiratory pathology
Demonstrate and teach a range of appropriate self management techniques for patients with complex and less predictable cardio-respiratory pathology
Apply a range of inclusive, non-discriminatory rehabilitation approaches (including restorative, supportive and palliative) in order to deliver holistic, patient focussed care to a range of patients suffering from complex and less predictable cardio-respiratory population pathology
CURRICULUM OUTLINE This unit is intended to further develop both cognitive and psychomotor skills of the student in assessment and treatment of a range of cardiorespiratory conditions. The unit covers cardio-respiratory physiology, functional and applied anatomy, biomechanics, examination and management of the above conditions in primary and secondary health care settings. A variety of rehabilitation approaches will be considered and clinical reasoning skills will be further developed through the use of more complex clinical scenarios.
230

Practice EducationTEACHING AND LEARNING STRATEGIES
Strong use will be made of student centred, case based problem solving learning strategies. Tutors create a challenging and supportive environment using a variety of learning and tutor methods in conjunction with directed study. This will include lectures, tutorials, group work and practical skills workshops. There will be an increased use of evidence based literature.
231
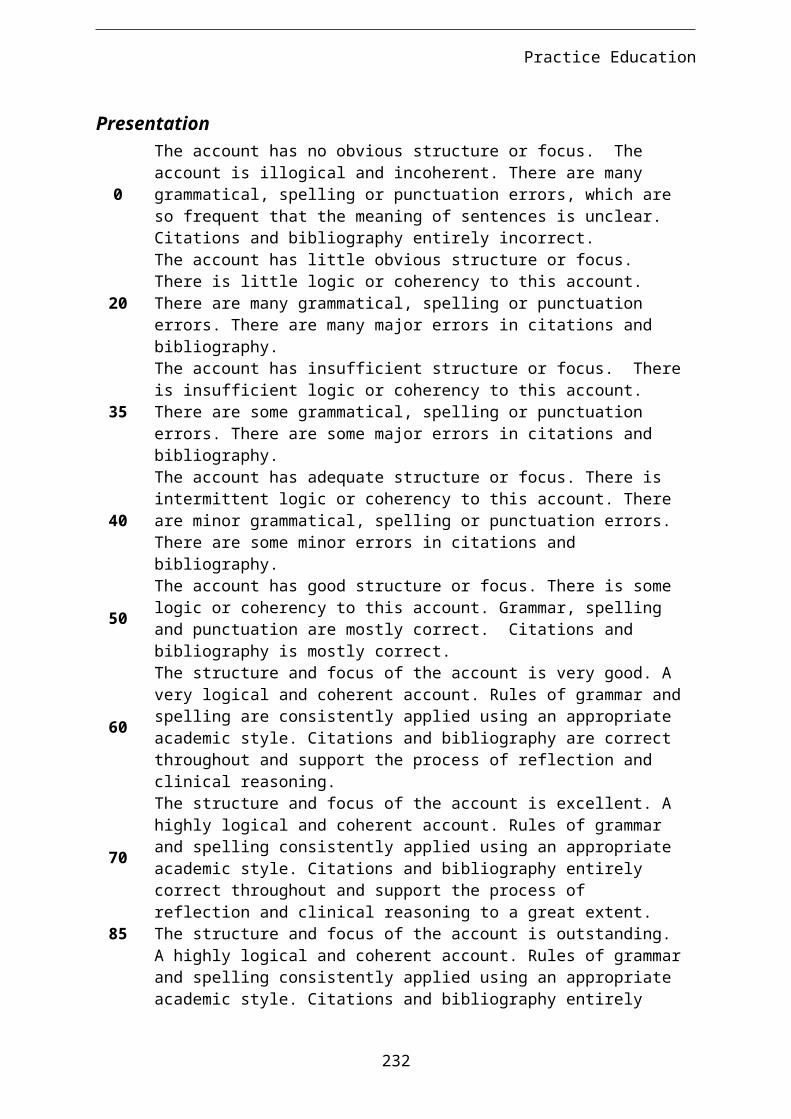
Practice Education
ASSESSMENT STRATEGIES Oral practical skills workshop - Formative Case based clinical reasoning oral practical examination – summative
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The student will demonstrate:
An understanding of the unit content An ability to use clinical reasoning in order to select, plan and justify
appropriate physiotherapy management techniques for a case study patient Safe, accurate and effective patient assessment and management techniques
that are clinically appropriate for the case study patient Demonstrate a patient focussed and holistic approach to patient care An ability to practice within the rules of professional conduct An ability communicate clearly, appropriately and coherently with both
patients and colleagues
Formative assessment procedures will assessed by peer assessment using self evaluation checklists linked to the unit/session learning outcomes with personal tutor support/academic action planning.
Summative assessment procedures will be assessed through generic level 2 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
232

Practice Education
UNIT TITLE Practice Placement 1, 2 and 3
UNIT CODE NUMBER
HOME PROGRAMMEBSc (Hons) Physiotherapy
HOME DEPARTMENTPhysiotherapy
SUBJECT AREAProfessional practice
UNIT LEADERJo Nicholson / Sophie Taylor
CREDIT VALUE20 for each placement
CREDITS AT LEVEL: 5
AMOUNT OF STUDENT EFFORT (HOURS)
200 for each placementCLASS CONTACT TIME (HOURS)
17
UNIT STATUSMandatory Core
PRE-REQUISITESBecoming a physiotherapistHuman movementHealth and social carePhysiotherapy management 1-6Clinical observation (level 1)
CO-REQUISITESNone
UNIT LEARNING OUTCOMES
There are 17 learning outcomes, which are divided into 5 categories:Interpersonal skillsThe student will:
1. demonstrate effective and appropriate skills in communication in order to collaborate and work effectively in partnership with others (professionals, support staff, patients/clients, carers, relatives and external agencies) to the benefit of the client/patient and maximise health outcomes.
2. contribute effectively to work undertaken as part of a team.3. recognise the scope of practice of other professionals.4. acknowledge cross professional boundaries.5. make appropriate referrals to others.6.
Management of selfthe student will
7. demonstrate effective self management of workload.8. know the limits of their own practice and when to seek advice.9. independently manage their own learning.10.
Management of patientthe student will:
11. gather appropriate information relating to the patient.12. plan and carry out an appropriate objective examination.13. analyse examination findings and formulate a written treatment plan in
partnership with the patient.14. implement and critically evaluate the impact of, or response to,
treatment interventions.15.
Documentationthe student will:
16. maintain accurate patient records.17.
Professional practicethe student will
18. promote patient centred care.19. comply with the CSP Rules of Professional Conduct.20. practice in line with relevant health and safety policy.21. work independently and as part of a team as appropriate.
CURRICULUM OUTLINE The student will be able to achieve the learning outcomes by managing an uncomplicated caseload of predictable patients. If the caseload is more complex, the student’s achievement must be adjusted to take this into account.The student should be able to apply and relate theory to practice. They should be able to evaluate the appropriateness of different approaches to solve
233

Practice Educationuncomplicated problems.
TEACHING AND LEARNING STRATEGIES
Assessment and treatment of patients under the supervision of a State Registered Physiotherapist.Experiential learning with reflective practice in the clinical settingUse of a Learning Development Plan/ContractSelf-directed studySelf-evaluation at mid-way and end of placement.Peer learningClinical staff development/in-service training sessionsAttendance at team meetings/case conference.WorkshopsTutorialsLecturesLearning will take place in a variety of clinical settings
ASSESSMENT STRATEGIES
These units will be assessed by a combination of placement performance (graded by practice placement staff) and pieces of reflective writing (graded by academic staff).Reflective log/diary - formativeAll clinical educators will be provided with the level 2 practice placement assessment documentation. This documentation is to be used for placement 1, 2 & 3 only. The student’s performance will be judged against a set of criteria generated in collaboration with other HEIs in the region.
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
General programme written and practical assessment criteria will apply.
Specific Assessment criteria for Level 2 practice placements.
Specific assessment criteria will be related to the written assignment.
234

Practice EducationUNIT TITLE Reflective Practice and Clinical Reasoning
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Reflective Practice and Clinical Reasoning
UNIT LEADER(S) Lesley McLoughlin
CREDIT VALUE 20 CREDITS AT LEVEL: 6
AMOUNT OF STUDENT EFFORT (HOURS)
200 CLASS CONTACT TIME (HOURS)
40
UNIT STATUS Mandatory Core
PRE-REQUISITES All Level 1 and Level 2 Units
CO-REQUISITES None
UNIT LEARNING OUTCOMES
The student will be able to:Cognitive/Intellectual Skills Critically reflect upon previous individual experiences of practice placement
using a variety of methods Demonstrate the ability to use clinical reasoning and evidence based
practice to justify all decision making in practice Critically appraise the relevance of professional, statutory and government
requirements on their practiceKey/transferable skills Use reflection and feedback to prioritise their learning needs in order to
support their professional development Interact effectively within a group and work with peers towards a common
goal
CURRICULUM OUTLINE This unit is intended to enable the student to: Continue to develop skills of both informal and formal reflective practice Use different methods of reflection and how these may inform practice Use reflection and clinical reasoning in order to make informed judgements,
decisions and prioritise actions taken Recognise the significance and implications of professional, statutory and
government requirements on practice.
TEACHING AND LEARNING STRATEGIES
Make strong use of student centred learning strategies with tutors creating a challenging and supportive environment.A variety of teaching strategies will be used including group work, tutorials, peer supported presentations, lectures.
ASSESSMENT STRATEGIES
Group case poster presentation – summative Self/ Peer appraisal of contribution to groupwork - Formative
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The student will demonstrate:
An ability to work effectively within a group of peers to develop, produce and present a poster
An ability to use/discuss the relevance of different models of reflection in reflecting on their practice and developing their future practice
The use of clinical reasoning and evidence based practice in order to justify their practice
An ability to present information in an appropriately constructed poster Access and critically evaluate appropriate evidence and select and justify
its inclusions in the poster. Discuss and answer questions related to the poster content and evidence
used with reference to the unit content
Formative assessment - written reflection on own contribution to a group activity and peer assessment of contribution to a group activity followed by discussion with personal tutor and academic action planning.Summative assessment procedures will be assessed through generic level 3 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
235

Practice Education
UNIT TITLE Practice Placement 4 and 5
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Professional practice
UNIT LEADER Jo Nicholson / Sophie Taylor
CREDIT VALUE 20 for each placement
CREDITS AT LEVEL: 6
AMOUNT OF STUDENT EFFORT (HOURS)
200 for each placement
CLASS CONTACT TIME (HOURS)
17
UNIT STATUS Mandatory Core
PRE-REQUISITES Foundations in Professional PracticeHuman movementHealth and social carePhysiotherapy management 1-6Clinical observation (level 1)Practice placements 1, 2 and 3
CO-REQUISITES None
UNIT LEARNING OUTCOMES
There are 17 learning outcomes, which are divided into 5 categories:Interpersonal skillsThe student will:
1. demonstrate effective and appropriate skills in communication in order to collaborate and work effectively in partnership with others (professionals, support staff, patients/clients, carers, relatives and external agencies) to the benefit of the client/patient and maximise health outcomes.
2. contribute effectively to work undertaken as part of a team.3. recognise the scope of practice of other professionals.4. acknowledge cross professional boundaries.5. make appropriate referrals to others.
Management of selfthe student will
6. demonstrate effective self management of workload.7. know the limits of their own practice and when to seek advice.8. independently manage their own learning.
Management of patient.the student will:
9. gather appropriate information relating to the patient.10. plan and carry out an appropriate objective examination.11. analyse examination findings and formulate a written treatment plan in
partnership with the patient.12. implement and critically evaluate the impact of, or response to,
treatment interventions.
Documentationthe student will:
13. maintain accurate patient records.
Professional practice.the student will
14. promote patient centred care.15. comply with the CSP Rules of Professional Conduct.
236

Practice Education16. practice in line with relevant health and safety policy.17. work independently and as part of a team as appropriate.
CURRICULUM OUTLINE
The student will be able to achieve the learning outcomes by managing a mixed caseload which may include complex patient conditions that do not respond in a predictable way.The student should be able to apply and relate theory to practice in greater detail than level 2. They should demonstrate an understanding of a complex body of knowledge and be able to apply problem solving skills to more complex situations and unpredictable circumstances.They should be able to evaluate evidence, arguments and assumptions to reach sound decisions.
TEACHING AND LEARNING STRATEGIES
Assessment and treatment of patients under the supervision of a State Registered Physiotherapist.Experiential learning with reflective practice in the clinical settingUse of a Learning Development Plan/ContractSelf-directed studySelf-evaluation at mid-way and end of placement.Clinical staff development/in-service training sessionsAttendance at team meetings/case conference.WorkshopsTutorialsLecturesLearning will take place in a variety of clinical settings
ASSESSMENT STRATEGIES
These units will be assessed by a combination of placement performance (graded by practice placement staff) and pieces of reflective writing (graded by academic staff).Reflective log/diary - formativeAll clinical educators will be provided with the level 3 practice placement assessment documentation. This documentation is to be used for placement 4 &5 only. The student’s performance will be judged against a set of criteria generated in collaboration with other HEIs in the region.
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
General programme written and practical assessment criteria will apply.
Specific assessment criteria for Level 3 practice placements.
Specific assessment criteria will be related to the written assignment.
237

Practice EducationUNIT TITLE Transition to Professional Practice
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Professional Practice
UNIT LEADER(S) Kathryn Heathcote
CREDIT VALUE 20 CREDITS AT LEVEL: 6
AMOUNT OF STUDENT EFFORT (HOURS)
200 CLASS CONTACT TIME (HOURS)
40
UNIT STATUS Mandatory Core
PRE-REQUISITES All Level 1 and 2 Units. Reflective Practice and Clinical Reasoning, Practice PlacementsHealth and Safety
CO-REQUISITES None
UNIT LEARNING OUTCOMES
The student will be able to:Cognitive/Intellectual Demonstrate critical awareness and knowledge of factors underpinning
professional autonomy and accountability Demonstrate critical awareness and understanding of factors underpinning
effective professional relationships Demonstrate critical awareness of the factors that contribute to the
development of effective personal and professional skills Articulate the responsibilities of a registered professional within health and
social care services
CURRICULUM OUTLINE This unit is intended to articulate expectations of a registered professional within health and social care services. It will enable the student to develop as an autonomous and accountable practitioner.The unit will cover;Standards and requirements of professional and statutory regulatory bodies.Legal and ethical responsibilitiesThe principles and practice of patient confidentialityFitness for practice and the need for CPDClinical governanceInterprofessional workingEffective team workingCommunication skillsTime management/prioritisation skillsAnti-discriminatory/anti-oppressive practiceWorking within scope of practiceMaintenance of health and well being
This unit will also address preparation of the student for their first clinical post. It will include CV development, interview practice, job applications.
TEACHING AND LEARNING STRATEGIES
Strong use of student –centred learning strategies. Based on a main Case study with self- directed study and tutorials. Other teaching strategies to include lectures, role play and mock interviews.
ASSESSMENT STRATEGIES
2000 word written assignment related to current professional issues – summative
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate: A critical awareness and understanding of the current key issues affecting
professional physiotherapy practice. An ability to access, select, evaluate and synthesise information related to
complex issues in order to produce an logical, coherent and evaluative piece of writing
An ability to present a written assignment in the appropriate academic style and format
Assessed through generic level 3 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
238

Practice Education
UNIT TITLE Evidence Based Practice Option1
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Physiotherapy
UNIT LEADER(S) Sally Hartley / Jenny Crampton / Jenny Caunt
CREDIT VALUE 10 CREDITS AT LEVEL: 6
AMOUNT OF STUDENT
EFFORT (HOURS)
100 CLASS CONTACT TIME
(HOURS)
20
UNIT STATUS Core
UNIT LEARNING OUTCOMES
The student will reflect on prior learning in order to select topics for further study from a range of topics offered.
The student will be able to build on existing knowledge to:
Critically evaluate relevant literature. Synthesise and analyse findings to influence the clinical reasoning process. Develop reasoned arguments in order to justify clinical decisions. Engage effectively in debate in a professional manner and produce detailed
and coherent arguments
CURRICULUM OUTLINE The student will have a choice of one topic from a minimum of three. The topics may include for example pain, exercise prescription, psychosocial model of rehabilitation.The topics available will be influenced by National guidelines and policies related to health care provision.
TEACHING AND LEARNING STRATEGIES
Lectures, small group tutorials, seminars, practical sessions and presentations
ASSESSMENT STRATEGIES
Open Book written examination (1.5 hours)
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate:
An in-depth understanding of the topic selected An ability to critically evaluate, apply, analyse and synthesise relevant
literature An ability to develop reasoned and coherent arguments in order to justify
conclusions and clinical decisions An ability to select and use appropriate literature and unit material
Assessed through generic level 3 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
INDICATIVE STUDENT LEARNING RESOURCES
The reading list will be based on current literature available particularly research activities and relevant government, professional body documents/publications
ADDITIONAL NOTES AND COMMENTS
Topics offered will be reviewed regularly in order to ensure their relevance and currency with reference to healthcare delivery and professional practice.
239

Practice Education
UNIT TITLE Evidence based Practice Option2
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Physiotherapy
UNIT LEADER(S) Deborah O’Connor / Francis Fatoye / Suzanne Gough
CREDIT VALUE 10 CREDITS AT LEVEL: 6
AMOUNT OF STUDENT
EFFORT (HOURS)
100 CLASS CONTACT TIME
(HOURS)
20
UNIT STATUS Core
PRE-REQUISITES
CO-REQUISITES
UNIT LEARNING OUTCOMES
The student will reflect on prior learning in order to select topics for further study from a range of topics offered.
The student will be able to build on existing knowledge to:
Critically evaluate relevant literature. Synthesise and analyse findings to influence the clinical reasoning process. Develop reasoned arguments in order to justify clinical decisions. Engage effectively in debate in a professional manner and produce detailed
and coherent arguments
CURRICULUM OUTLINE The student will have a choice of one topic from a minimum of three. The topics may include for example pain, exercise prescription, psychosocial model of rehabilitation.The topics available will be influenced by National guidelines and policies related to health care provision.
TEACHING AND LEARNING STRATEGIES
Lectures, small group tutorials, seminars, practical sessions and presentations
ASSESSMENT STRATEGIES
Open Book written examination (1.5 hours)
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate:
An in-depth understanding of the topic selected An ability to critically evaluate, apply, analyse and synthesise relevant
literature An ability to develop reasoned and coherent arguments in order to justify
conclusions and clinical decisions An ability to select and use appropriate literature and unit material
Assessed through generic level 3 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
240
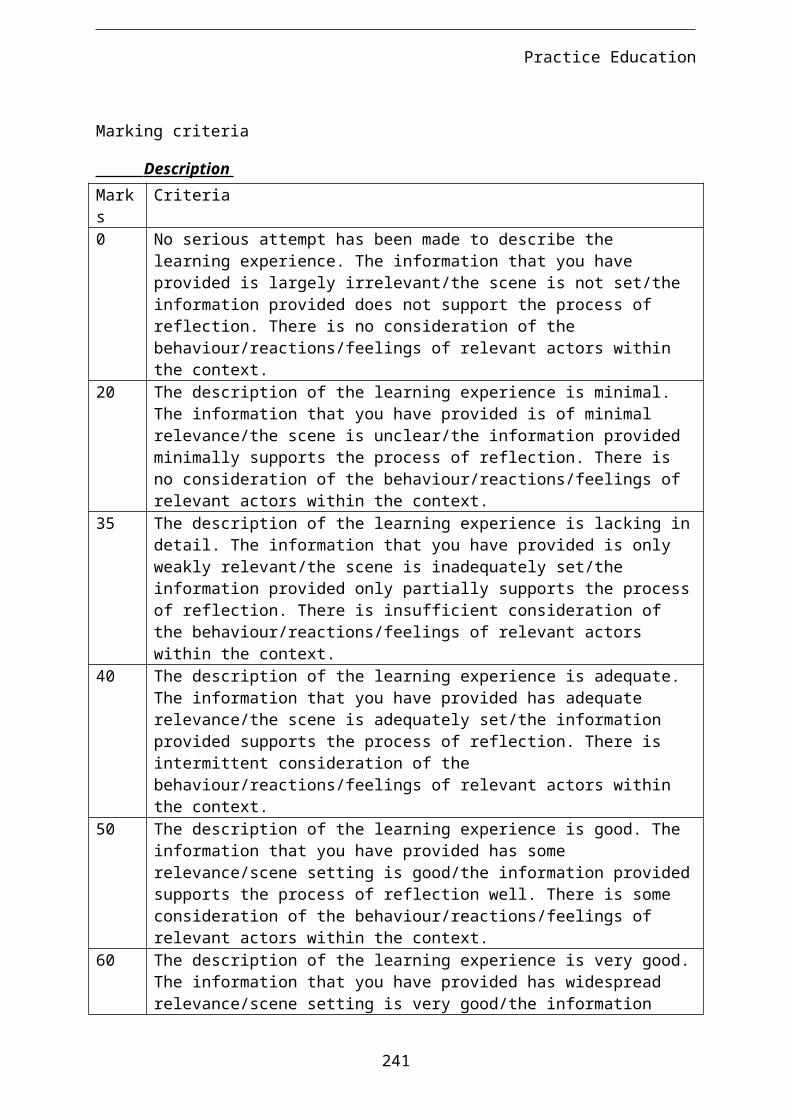
Practice Education
UNIT TITLE Critical Thinking/Enquiry
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Research Skills
UNIT LEADER(S) Janet Rooney
CREDIT VALUE 20 CREDITS AT LEVEL: 6
AMOUNT OF STUDENT EFFORT
(HOURS)
200 CLASS CONTACT TIME
(HOURS)
10
UNIT STATUS Mandatory Core
PRE-REQUISITES All Level 1 and 2 Units
CO-REQUISITES
UNIT LEARNING OUTCOMESThe student will be able to:Cognitive/Intellectual Skills Search for and critically evaluate the evidence underpinning current
physiotherapy practice or education Select, synthesise and manage information in order to undertake their
research task Use logical and reasoned argument to support their research study Develop and justify an appropriate and realistic research methodology to
investigate or explore their research question Demonstrate an understanding of the importance of ethical issues related
to the proposed research. Select and justify appropriate statistical methods
CURRICULUM OUTLINE Further develop skills in: critical thinking, literature searching, logical reasoning. developing logical and reasoned argument academic writing
TEACHING AND LEARNING STRATEGIES
Student centred learning with dedicated supervisor support.Lectures and tutorialsGroup discussionsPeer support
ASSESSMENT STRATEGIES Written submission of initial idea for research proposal (max 500 words) –
formative Written extended research proposal (4000 words) with academic
supervisory support.
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will produce a detailed research proposal that demonstrates their ability to: Search for, select, critically evaluate and synthesis the current evidence
underpinning physiotherapy practice related to their chosen topic develop and clearly formulate a justified research question develop an appropriate and realistic methodology demonstrate an understanding of the relevant ethical issues and an ability
to apply them to their study
241

Practice Education use logical, reasoned, coherent and evaluative arguments present the proposal in an appropriate academic format
Formative assessment procedure will be assessed by project management group consisting of academic staff and formative written feedback will be given related to the feasibility of the study and the ethical considerations.Summative assessment procedures will be assessed through generic level 3 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
242

Practice Education
UNIT TITLE Practice Placement 6
UNIT CODE NUMBER
HOME PROGRAMME BSc (Hons) Physiotherapy
HOME DEPARTMENT Physiotherapy
SUBJECT AREA Professional practice
UNIT LEADER Jo Nicholson / Sophie Taylor
CREDIT VALUE 10 Practice Credits
CREDITS AT LEVEL: 6
AMOUNT OF STUDENT EFFORT (HOURS)
100 CLASS CONTACT TIME (HOURS)
UNIT STATUS Mandatory Core
PRE-REQUISITES All preceding units – Levels 1, 2 and 3
CO-REQUISITES None
UNIT LEARNING OUTCOMESThere are 17 learning outcomes, which are divided into 5 categories:
Interpersonal skillsThe student will:
1. demonstrate effective and appropriate skills in communication in order to collaborate and work effectively in partnership with others (professionals, support staff, patients/clients, carers, relatives and external agencies) to the benefit of the client/patient and maximise health outcomes.
2. contribute effectively to work undertaken as part of a team.3. recognise the scope of practice of other professionals.4. acknowledge cross professional boundaries.5. make appropriate referrals to others.
Management of selfthe student will
6. demonstrate effective self management of workload.7. know the limits of their own practice and when to seek advice.8. independently manage their own learning.
Management of patient.the student will:
9. gather appropriate information relating to the patient.10. plan and carry out an appropriate objective examination.11. analyse examination findings and formulate a written treatment plan in
partnership with the patient.12. implement and critically evaluate the impact of, or response to,
treatment interventions.
Documentationthe student will:
13. maintain accurate patient records.
Professional practice.the student will
14. promote patient centred care.15. comply with the CSP Rules of Professional Conduct.

Practice Education16. practice in line with relevant health and safety policy.17. work independently and as part of a team as appropriate.
CURRICULUM OUTLINE The student should be able to achieve the learning outcomes by managing a mixed caseload which may include complex patient conditions that do not respond in a predictable way.The student should be able to apply and relate theory to practice in greater detail than level 2. They should demonstrate an understanding of a complex body of knowledge and be able to apply problem solving skills to more complex situations and unpredictable circumstances.They should be able to evaluate evidence, arguments and assumptions to reach sound decisions.
TEACHING AND LEARNING STRATEGIES
Assessment and treatment of patients under the supervision of a State Registered Physiotherapist.Experiential learning with reflective practice in the clinical settingUse of a Learning Development Plan/ContractSelf-directed studySelf-evaluation at mid-way and end of placement.Attendance at team meetings/case conference.
ASSESSMENT STRATEGIES The student will be assessed against a set of criteria that will be made available to them and their practice placement supervisors that are applicable to the placement in hand.
In order to be successful the students practice must match the requirements of the criteria. However, the placement will be considered pass/fail.
Formative self-evaluation with guidance from experienced clinical colleagues.
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
Specific assessment criteria for Level 3 practice placement with pass/fail outcome
ADDITIONAL NOTES AND COMMENTS
The professional body requires the completion of 1000 clinical hours during undergraduate physiotherapy education. In order to meet this requirement the student will complete this elective placement. The student will be responsible for the organisation of the placement. The placement must match the following requirements:The student must be supervised by an individual who is registered to practice as a physiotherapist.Where the placement is non-UK the student must ensure that they have obtained appropriate visas or other statutory documentsWhere the placement is in the United States of America or Canada the student must secure additional student liability insurance. This can be organised with the cooperation of the Chartered Society of Physiotherapy,

Practice Education

Practice Education
1 UNIT TITLE BSc (Hons) Physiotherapy 2010-13: Foundations in Professional Practice
2 BRIEF SUMMARY
This unit has its focus on the development of a series of skills that are essential to the learner and future professional. It includes generic study skills and an introduction to the basics of research. It has a physiotherapy specific focus on skills for continuing professional development, evidence based practice, teamwork, cultural awareness and professionalism.
3 UNIT CODE NUMBER
28151001
4 HOME PROGRAMME
BSc (Hons) Physiotherapy
5 HOME DEPARTMENT
Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S)
Janet Morrison
8 CREDIT VALUE 20 CREDITS AT LEVEL:
4 (C)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
20065 hours classroom contact135 hours directed/self-directed study and assessment preparation
10
UNIT STATUS Mandatory Core
11
PRE-REQUISITES
None
12
CO-REQUISITES
None
13
UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to, have attained or demonstrated:Knowledge and understanding.
1. Describe the roles of Professional, Statutory and Regulatory Body requirements and how they impact on their learning experience
2. Describe and use models of reflection, reflecting on their personal development and explain the need for reflective practice
3. Explain the factors that contribute to evidence-based

Practice Educationpractice
Cognitive/intellectual skills4. Identify own learning needs5. Explain the importance of lifelong learning and continuing
professional development6. Explore factors relating to cultural awareness and
stereotyping 7. Identify the fundamental principles of professionalism in
the health professionsKey/transferable skills
8. Communicate accurately and reliably using structured coherent arguments
9. Support and develop arguments using reference to relevant/contemporary literature
10. reflect on ability to work effectively with others as a member of a group and meet obligations to others.
11. Use appropriate study skills/ information skills to support and enhance their learning
14
CURRICULUM OUTLINE
Study skills, for example reading, writing and note taking. Information skills (retrieval and analysis/appraisal) Roles and functions of Professional, Statutory and
regulatory bodies, Rules of Professional Conduct, Standards of Conduct and Ethics.
Continuing professional development, lifelong learning agenda.
Diversity and cultural competence, promoting equality and people’s rights/responsibilities.
Rehabilitation – social and medical models: preventative (including introduction to health promotion), restorative, maintenance and palliative approaches to rehabilitation, major approaches to psychology and their relevance to health; psychological factors affecting health.
Evidence based practice, guidelines, protocols and integrated care pathways.
Research skills – critical appraisal, reliability, validity, research questions/hypotheses, qualitative and quantitative research methods, statistical analysis, the research process; outcome measures.
Introduction to research and practice ethics, patient confidentiality.
Research/audit and how it underpins practice. Reflective practice, models of reflection, reflective writing
and introduction to portfolio development.
15
LEARNING & TEACHING ACTIVITIES
A variety of approaches will be used including lectures, self and directed study, tutorials, seminars, presentations, e-learning.
16
ASSESSMENT STRATEGIES
Completion of a research skills self-evaluation (LO3, 9 and 11 - formative)
Use of ‘sharing’ in PebblePad® e-portfolio to present self-generated materials to personal tutor for appraisal and feedback (CPD) portfolio (LO4, 5 and 11 - formative)
Self/peer and tutor feedback on contribution to inter-

Practice Educationprofessional online forum – (LO10 - formative)
Essay based assignment (reflection) (8 sides of A4 double spaced) (LO1-11- 100% summative)
17
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The student will demonstrate: An understanding of the unit content. A basic understanding of the models of reflection An ability to use and record in a written format simple
reflection on their personal and professional development An ability to recognise the role of reflection in the
development of lifelong learning
18
INDICATIVE STUDENT LEARNING RESOURCES
Berglund, C.A., (2007) Ethics for health care 3rd Edition, Oxford, South Melbourne, Vic: Oxford University Press.
Bolton, G.E. J, (2010) Reflective Practice Writing and Professional Development 3rd edition. London: Paul Chapman Publishing.
Chartered Society of Physiotherapy (2002) Rules of Professional Conduct 2nd Edition. London: Chartered Society of Physiotherapy
Chartered Society of Physiotherapy (2005) Core Standards of Physiotherapy Practice. London: Chartered Society of Physiotherapy. [Online] http://www.csp.org.uk/uploads/documents/csp_core_standards_2005.pdf
Common assessment tool (2003) Manchester Metropolitan University, University of Central Lancashire, University of Cumbria, University of Liverpool and University of Salford.
Cottrell, S. (2008) The study skills handbook 3rd edn.. Basingstoke: Palgrave Macmillan.
Health Professions Council (2010), Guidance on conduct and ethics for students. London: Health Professions Council.
Health Professions Council. (2007) Standards for Continuing Professional Development [Online] [Accessed 16 November 2009] http://www.hpc-uk.org/aboutregistration/standards/cpd/
Health Professions Council. (2007) Standards of Proficiency Physiotherapists [Online] [Accessed 16 November 2009] Available from: http://www.hpc-uk.org/publications/standards/index.asp?id=49
Health Professions Council. (2008) Standards of conduct, performance and ethics [Online] Accessed 16 November 2009] Available from:http://www.hpc-uk.org/publications/standards/index.asp?id=38
Hicks, C. (2009) Research Methods for Clinical Therapists Applied Project Design and Analysis 5th Edition. London: Churchill Livingston.
Jasper, M. (2003) Beginning reflective practice. Foundations in nursing and health care. Cheltenham, Nelson Thornes Ltd.
Johns, C. (2004) Becoming a reflective practitioner. 2nd edition.

Practice EducationOxford, Blackwell publishing.
Mundsack, A. et al. (2003) How to study: And other skills for success in college [Electronic resource] ebook.
Sim, J. Wright, C (2000) Research in health care: concepts, designs and methods Cheltenham : Nelson Thornes.
Taylor, J (2003) Study skills in healthcare. Cheltenham: Nelson Thornes.
19
ANY ADDITIONAL NOTES AND COMMENTS
20
DATE OF APPROVAL
11 & 12 February 2010
21
DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Human Movement
2 BRIEF SUMMARY This unit acts as an introduction to a variety of basic principles that underpin all physiotherapy practice. It includes consideration of cytology and histology and physiology in specialised human tissues, the interaction of different body systems to produce movement in addition to the study of basic biomechanics as they are applied to movement and physiotherapy.
3 UNIT CODE NUMBER 28151002
4 HOME PROGRAMME BSC (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: Physiotherapy
7 UNIT LEADER(S)
8 CREDIT VALUE 20 CREDITS AT LEVEL:
4 (C)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
20065 hours classroom contact135 hours directed/self-directed study and assessment preparation
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES None
12 CO-REQUISITES Clinical Science
13 UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to, have attained or demonstrated:
1. describe and explain the normal cytology, histology and physiology of the cardiorespiratory, musculoskeletal and nervous systems
2. describe and explain how these systems interact to produce normal human movement
3. undertake accurate movement analysis using a human model
4. access appropriate resources to support their learning to support and develop arguments using reference to relevant/contemporary literature
5. select and present appropriate information to others in a professional manner and in an appropriate academic style.
14 CURRICULUM OUTLINE
The students will explore the structure and function of major systems of the body and relate their structure and function to normal human movement.This unit will cover anatomy, physiology, biomechanics,

Practice Educationhistology, tissue damage and repair. The specific systems for consideration will be the cardiorespiratory, the musculoskeletal and the nervous systems.
15 LEARNING & TEACHING ACTIVITIES
Makes strong use of student centred learning strategies with tutors creating both a challenging and supportive environment. This will be achieved by using a variety of delivery methods, including:
E-learning resources Theatre Events Practical demonstration/skills practise Tutorials Peer learning Student led tutorials Self directed learning
All of the above will be in conjunction with both indicative reading and material accessed by the students.The teaching and learning will comprise a combination of directed and problem solving approaches.
16 ASSESSMENT STRATEGIES
Functional activity workshops with self and peer appraisal (Learning Outcomes 1-6 - formative)
Diagnostic written assignment, tutor marked (1 page A4 double spaced) (Learning outcome 1, 4 and 5 – formative)
Essay based assignment related to normal structure and function of the human body (to include movement analysis) – (8 pages of A4 double spaced) (Learning Outcomes 1-5 – 100% summative)
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate: understanding of how the structure and function of the
major systems of the body contribute to normal human movement
understanding of the principles of functional analysis. ability to carry out a basic analysis of function. ability to explain an analysis of function in a written
report. ability to write in an appropriate academic format.
18 INDICATIVE STUDENT LEARNING RESOURCES
Abrahams, P H., Hutchings, R. and Marks, S .C. (2008) McMinn's color atlas of human anatomy. 6th ed. London: Mosby.
Agur, A. M. R. (2005) Grant's atlas of anatomy.11th ed. London: Lippincott Williams and Wilkins.
Beil, A. R. (2005) Trail guide to the body: how to locate muscles, bones, and more. 3rd ed. Boulder, USA, Books of Discovery
Byfield, D. and Kinsinger, S. (2002) A manual therapist’s guide to surface anatomy and palpation skills. Oxford: Butterworth Heinemann
Clarkson, H. M. (2000) Musculoskeletal assessment: joint range of motion and manual muscle strength. 2nd ed. London: Lippincott Williams and Wilkins.

Practice EducationGuyton. A. C. (2005) Textbook of medical physiology. 11th ed. London: Saunders
Hall, S. J. (2007) Basic biomechanics. 5th Ed. Boston: McGraw-Hill.
Kendall, F. P. (2005) Muscles: testing and function with posture and pain. 5th ed. London: Lippincott Williams and Wilkins.
Kisner, C. and Colby, L .A. (2007) Therapeutic exercise: foundations and techniques. 5th ed. Philadelphia: F. A. Davis.
Levangie, P. K. and Norkin, C. C. (2005) Joint structure and function: a comprehensive analysis. 4th ed. Philadelphia : F. A .Davis Company
McArdle, W. D., Katch, F .I. and Katch, V. L. (2005) Essentials of exercise physiology. 3rd ed. London: Lippincott, Williams and Wilkins
Nordin, M. (2001) Basic biomechanics of the musculoskeletal system. 3rd ed. Philadelphia: Lippincott Williams and Wilkins.
Oliver, J. and Middleditch, A. (2005) Functional anatomy of the spine. 2nd ed. Oxford: Butterworth Heinemann.
Palastanga, N., Field, D. and Soames, R. (2006) Anatomy and human movement: structure and function. 5th ed. Oxford: Butterworth Heinemann
Soames, R. (2003) Joint Motion: clinical measurement and evaluation. Edinburgh: Churchill Livingstone
Spector, T. D. (1999) An introduction to general pathology. 4th ed. Edinburgh: Churchill Livingstone.
Trew, M. and Everett, T. (2005) Human movement: an introductory text. 5th ed. Edinburgh: Churchill Livingstone. Earlier edition also available
Other resources / recommended websitesAnatomy TV
www.csp.org.uk
www.electrotherapy.org
www.prodigy.nhs.uk/clinicalguidance
http://thebrain.mcgill.ca/
19 ANY ADDITIONAL NOTES AND COMMENTS
This unit is intended to provide students with information that will form a foundation for further units of study.
20 DATE OF APPROVAL 11 & 12 February 2010

Practice Education
21 DATE OF MOST RECENT CONSIDERATION:
1 UNIT TITLE Clinical Sciences
2 BRIEF SUMMARY
This unit has a particular focus on the anatomy of the human body. The musculoskeletal, cardiorespiratory and nervous systems will be considered in terms of their detailed structure with a focus on relating anatomical knowledge to normal human functioning.
3 UNIT CODE NUMBER 28151003
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Sally Hartley
8 CREDIT VALUE 10 CREDITS AT LEVEL: 4 (C)
9
TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
10033 hours classroom contact67 hours directed/self-directed study and assessment preparation
10 UNIT STATUS Mandatory core
11 PRE-REQUISITES None
12 CO-REQUISITES Human Movement
13
UNIT LEARNING OUTCOMES
On successful completion of this unit students will have attained or demonstrated:
1. describe, classify and locate the anatomical components of the cardiorespiratory, musculoskeletal and nervous systems
2. explain how these components produce normal human movement
3. demonstrate safe and effective therapeutic handling4. demonstrate safe and accurate anatomical palpation5. practically demonstrate structure and function on a
human mode6. access appropriate, relevant and contemporary
resources to support their learning

Practice Education7. select and present appropriate information to others
in a professional manner
14
CURRICULUM OUTLINE
The students will explore the structure of major systems of the body and relate this structure to human movement.
This unit will cover normal human anatomy of the three main systems.
The specific systems for consideration will be the cardiorespiratory system, the musculoskeletal system and the nervous system.
15
LEARNING & TEACHING ACTIVITIES
Makes strong use of student centred learning strategies with tutors creating both a challenging and supportive environment. This will be achieved by using a variety of delivery methods, including:
E-learning resources
Theatre Events
Practical demonstration/skills practise
Tutorials
Peer learning
Student led tutorials
Self directed learning
All of the above will be in conjunction with both indicative reading and material accessed by the students.
The teaching and learning will comprise a combination of directed and problem solving approaches.
16
ASSESSMENT STRATEGIES
Functional anatomy based practical skills workshop with self/peer and tutor feedback on performance (LO 1-7 – formative)
Study skills self-evaluation inventory (PebblePAD) (LO6 – formative)
Oral practical examination (anatomy viva) 30 minutes; (Learning Outcomes 1-7 – 100% summative)
17
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate ability to: describe and explain the anatomical components of
the cardiorespiratory, musculoskeletal and nervous systems
explain how the structure of these systems facilitates their normal function
demonstrate safe and effective therapeutic handling demonstrate safe and accurate anatomical palpation practically demonstrate structure and function on a
human model appropriately, clearly and coherently communicate
with all relevant parties. adhere to Rules of Professional Conduct/Standards
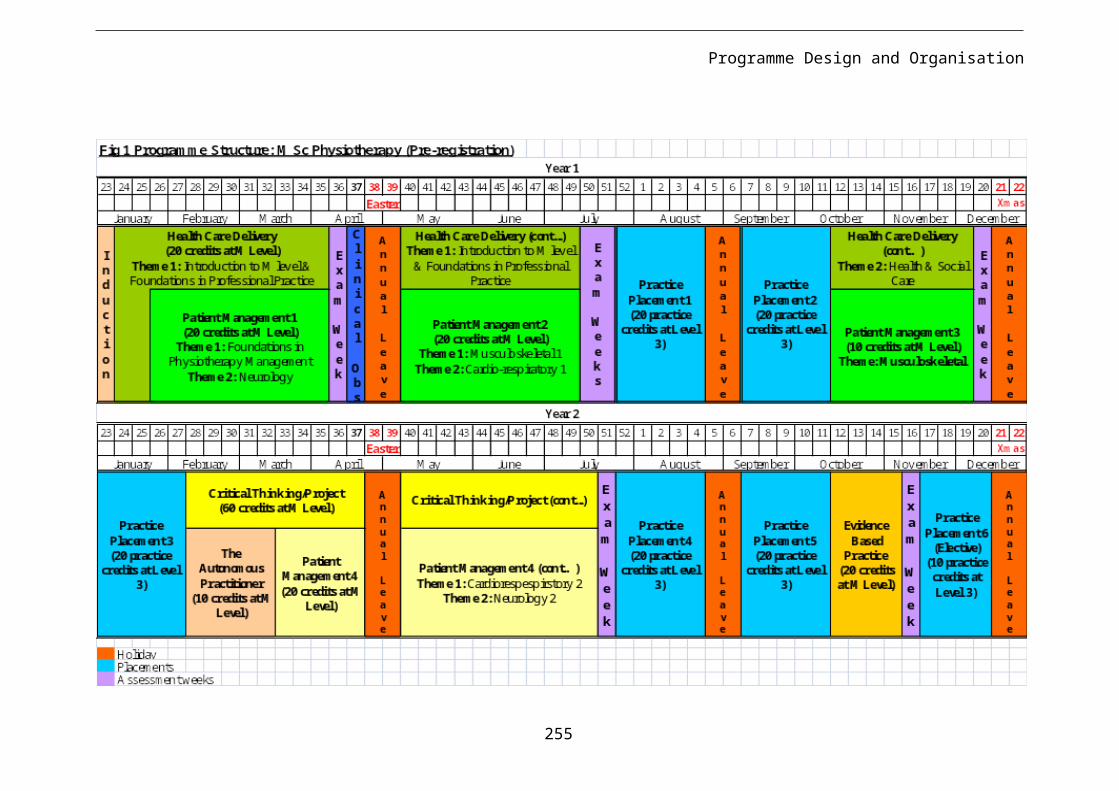
Practice Educationof Conduct and Ethics
use an organised, logical approach with effective use of equipment.
18
INDICATIVE STUDENT LEARNING RESOURCES
Abrahams, P. H., Hutchings, R. and Marks, S. C. (2008) McMinn's color atlas of human anatomy. 6th ed. London: Mosby.
Agur, A. M. R. (2005) Grant's atlas of anatomy. 11th ed. London: Lippincott Williams and Wilkins.
Anatomy.tv. [electronic resource]. Accessed via the MMU library website.
Beil, A. R. (2005) Trail guide to the body: how to locate muscles, bones, and more. Boulder Co. USA: Books of Discovery.
Byfield, D. and Kinsinger, S. (2002) A manual therapists guide to surface anatomy and palpation skills. Oxford: Butterworth Heinemann
Clarkson, H. M. (2000) Musculoskeletal assessment: joint range of motion and manual muscle strength. 2nd ed. London: Lippincott Williams and Wilkins.
Hess, S.A. (2000) ‘Functional stability of the glenohumeral joint.’ Manual Therapy. Vol. 5, no. 2, pp. 63-71
Levangie, P. K. and Norkin, C. C. (2005) Joint structure and function: a comprehensive analysis. 4th ed, Philadelphia : F. A Davis Company
Marieb, E. N. and Hoehn, K. (2009) Human anatomy and physiology. 8th ed, Redwood City, Ca: Pearson Education.
Middleditch, A. and Oliver, J. (2005) Functional anatomy of the spine. 2nd ed. Oxford: Butterworth-Heinemann.
Palastanga, N., Field, D. and Soames, R. (2006) Anatomy and human movement: structure and function.5th ed. Oxford: Butterworth Heinemann
19
ANY ADDITIONAL NOTES AND COMMENTS
This unit is intended to provide students with information that will form a foundation for further units of study.It is a professional body requirement that students will not be entitled to receive condoned passes for assessment that include practical skills. This unit must be passed with a mark ≥40.
20
DATE OF APPROVAL 11 & 12 February 2010
21
DATE OF MOST RECENT

Practice Education
CONSIDERATION:

Practice Education
1 UNIT TITLE Physiotherapy Management MSK 1
2 BRIEF SUMMARY This unit builds on knowledge gained in earlier units and has its focus on the upper quadrant. The unit allows students to consider trauma and other pathophysiology of the upper limb. Students will consider assessment, goal setting, treatment planning and evaluation for conditions of the upper quadrant. Students will consider how evidence informs practice and will learn to support clinical decision making with reference to research and evidence based guidelines.
3 UNIT CODE NUMBER 28151004
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Kay Hurst
8 CREDIT VALUE 20 CREDITS AT LEVEL:
4 (C)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
20065 hours classroom contact
135 hours directed/self-directed study and assessment preparation
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES
12 CO-REQUISITES
13 UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to,:
Knowledge and understanding1. apply knowledge of the structure and function of the
upper quadrant to explain the pathology and clinical features of selected pathologies of the upper quadrant.
2. suggest patient focused, achievable and realistic goals of treatment that take into account the patients’ psychosocioeconomic needs.
Cognitive/intellectual skills3. apply knowledge in order to selected, plan, explain
and evaluate (using basic methods) appropriate assessment techniques for patients with pathologies of the upper quadrant and with guidance interpret the findings.
4. apply knowledge in order to select, plan, explain and evaluate (using basic methods) appropriate

Practice Educationphysiotherapy management techniques for patients with pathologies of the upper quadrant.
5. evaluate appropriate basic outcome measures for patients with pathologies of the upper quadrant.
Key/transferable skills6. use basic clinical reasoning and problem solving to
select, plan, explain and with guidance evaluate the assessment and treatment of patients with pathologies of the upper quadrant.
7. apply knowledge learned in previous units to pathologies of the upper quadrant.
8. access and apply relevant and contemporary literature to support physiotherapy assessment and patient management choices.
9. Present information logically and coherently in an appropriate academic style
14 CURRICULUM OUTLINE
This unit is intended to develop both cognitive and psychomotor skills in the undergraduate physiotherapist. The main principles are the integration and application of anatomical knowledge to selected pathologies of the upper quadrant which will enable the student to clinically reason and explain their clinical decisions. This unit covers the application of functional anatomy, biomechanics, surface marking, differential diagnosis and treatment of pathologies in the following regions:
Cervical spine Thoracic spine Shoulder complex Elbow Forearm, wrist and hand.
15 LEARNING & TEACHING ACTIVITIES
Makes strong use of student centred learning strategies with lecturers creating both a challenging and supportive learning environment using a variety of delivery methods in conjunction with indicative reading. A variety of strategies are used including: illustrated lectures, practical demonstrations, practical skills sessions, tutorials, e-learning, group work, role play and case based problem solving.
16 ASSESSMENT STRATEGIES
Practical workshops (LO1-8 - formative). Comprehensive oral feedback will be provided by tutors and peers during the formative workshop.
Essay based assignment (eight sides of A4 double spaced) clinical pathology and physiotherapy management written assignment, demonstrating basic clinical reasoning (LO1-9– 100% summative)
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate: ability to relate the structure and function of the upper
quadrant to the pathology and clinical features of selected musculoskeletal pathologies and their physiotherapy management.
ability to use basic clinical reasoning to explain the relationship between pathology, clinical features and the physiotherapy management of upper quadrant

Practice Educationpathologies
ability to select, plan and explain appropriate physiotherapy management for a described patient.
ability to access, select and use appropriate evidence to support their chosen physiotherapy management approach.
ability to present written information in a logical, coherent and reasoned manner.
ability to present the answer in an appropriate written academic style and format.
Formative assessment – peer assessment using self-evaluation checklists linked to the unit/session learning outcomes.Summative assessment procedures will be assessed through generic level 4 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
18 INDICATIVE STUDENT LEARNING
RESOURCES
Abrahams, P. H., Hutchings, R. and Marks, S. C. (2008) McMinn's color atlas of human anatomy. 6th ed., London : Mosby.
Agur, A. M. R. (2009) Grant's atlas of anatomy. 12th ed., London: Lippincott Williams and Wilkins.
Biel, A. (2005) Trail guide to the body: how to locate muscles, bones and more. 3rd ed., Boulder, USA: Books of Discovery.
Boyling, J. D. and Jull, G. A. (2004) Grieves modern manual therapy: the vertebral column. 3rd ed., Edinburgh: Churchill Livingstone.
Byfield, D. and Kinsinger, S. (2002) A manual therapist’s guide to surface anatomy and palpation skills. Oxford: Butterworth Heinemann.
Clarkson, H. M. (2000) Musculoskeletal assessment: joint range of motion and manual muscle strength. 2nd ed., London: Lippincott Williams and Wilkins.
Cleland, J. and Durall, C. J. (2002) ‘Physical therapy for adhesive capsulitis: Systematic Review.’ Physiotherapy, Vol. 88, no. 8, pp. 450-457
Corrigan, B. and Maitland, G. D. (1998) Vertebral musculoskeletal disorders. Oxford: Butterworth-Heinemann.
Dandy, D. J. (2009) Essential Orthopaedics and Trauma. 5th ed., Edinburgh: Churchill Livingstone.
David, C. and Lloyd, J. (1999) Rheumatological physiotherapy. London: Mosby.
Elstrom, J. A., Virkus, W. W., Pankovich, A. M. (2005) Handbook of Fractures. 3rd ed., New York: McGraw-Hill.
French, S. and Sim, J. (2004) Physiotherapy : a Psychosocial Approach. 3rd ed., Oxford: Butterworth-Heinemann.
Hakim, A., Clunie, G. and Haq, I. (2006) Oxford handbook of

Practice Educationrheumatology. 2nd ed., Oxford: Oxford University Press.
Hengeveld, E. and Banks, K. (2005) Maitland’s Vertebral Manipulation, 7th ed., Oxford: Butterworth Heinemann.
Hess, S.A. (2000) ‘Functional stability of the glenohumeral joint.’ Manual Therapy, Vol. 5, no. 2, pp. 63-71
Holey, E. A. (2003) Evidence-based Therapeutic Massage: A Practical Guide for Therapists. 2nd ed., Edinburgh: Churchill Livingstone.
Janwantanakul, P. (2006) ‘Cold pack/skin interface temperature during ice treatment with various levels of compression.’ Physiotherapy, Vol. 92, pp. 254-259
Jones, M. and Rivett, D. (2003) Clinical reasoning for manual therapists. Oxford: Butterworth-Heinemann.
Kendall, F. P. (2005) Muscles: testing and function with posture and pain. 5th ed., London: Lippincott Williams and Wilkins. Earlier edition also available.
Kesson, M. and Atkins, E. (2005) Orthopaedic medicine: a practical approach. Oxford: Butterworth Heinemann
Kisner, C. and Colby, L. A. (2007) Therapeutic exercise: foundations and techniques. 5th ed., Philadelphia: F. A. Davis.
Levangie, P. K. and Norkin, C. C. (2005) Joint structure and function: a comprehensive analysis. 4th ed., Philadelphia: F. A. Davis Company.
Magarey, M. E, Rebbeck, T., Coughlan, B., Grimmer, K., Rivett, D. A. and Refhauge, K. (2004) ‘Pre-manipulative testing of the cervical spine review, revision and new clinical guidelines.’ Manual Therapy, Vol. 9, pp. 95-108
Main, C .J. and Watson, P. J. (1999) ‘Psychological aspects of pain.’ Manual Therapy, Vol. 4, pp. 203-215
McClune, T., Burton, A. K., Waddell, G. (2002) ‘Whiplash associated disorders: a review of the literature to guide patient information and advice.’ Emerg. Med. J, Vol. 19, pp. 499-506
McRae, R. and Esser, M. (2008) Practical fracture treatment. 5th ed. Edinburgh: Churchill Livingstone.
Norris, C. (2004) Sports injuries: diagnosis and management. 3rd ed., Oxford: Butterworth Heinemann.
Oliver, J. and Middleditch, A. (2005) Functional anatomy of the spine. 2nd ed., Oxford: Butterworth Heinemann.
Palastanga, N., Field, D. and Soames, R. (2006) Anatomy and Human Movement: Structure and Function. 5th ed., Oxford: Butterworth Heinemann.
Petty, N. J. and Moore, A. (2005) Neuromusculoskeletal examination and assessment: a handbook for therapists. 3rd

Practice Educationed., Edinburgh: Churchill Livingstone. Earlier edition also available
Robertson, V., Ward, A., Low, J. and Reed, A. (2006) Electrotherapy explained; principles and practice. 4th ed., Oxford: Butterworth Heinemann.
Snaith, M. L. (2004) ABC of rheumatology. 3rd ed., London: BMJ Publishing.
Soames, R. (2003) Joint Motion: clinical measurement and evaluation. Edinburgh: Churchill Livingstone.
Solomon, L. (2010) Apley's System of Orthopaedics and Fractures. 9th ed., London: Arnold.
Tugwell, P., Shea, B., Boers, M., Brooks, P., Simon, L., Strand, V. and Wells, G. (2004) Evidence Based Rheumatology. London: BMJ Publishing.
Vicenzino, B. (2003) ‘Lateral epicondylalgia: a musculoskeletal physiotherapy perspective.’ Manual Therapy, Vol. 8, no. 2, pp. 66-79
Watson, T. (2008) Electrotherapy: Evidence Based Practice. 12th ed., Edinburgh: Churchill Livingstone.
Wies, J. (2005) ‘Treatment of eight patients with frozen shoulder: a case study series.’ Journal of Bodywork and Movement Therapies, Vol. 9, pp. 58-64
www.csp.org.uk
www.electrotherapy.org
www.prodigy.nhs.uk/clinicalguidance
19 ANY ADDITIONAL NOTES AND COMMENTS
The content of this unit will support learning at level 4 and lay the necessary foundations for study at levels 5 and 6. The topics studied here will complement the content of parallel units and will be reinforced in other units throughout the programme..
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Health and Social Care
2 BRIEF SUMMARY This unit seeks to explore and promote understanding of the range of environments in which health and social care is delivered and how health and social care policy influences health care delivery. The unit includes consideration of contemporary issues in Health and Social Care and how this might influence physiotherapy practice.
3 UNIT CODE NUMBER 28151005
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Jill Bailey
8 CREDIT VALUE 10 CREDITS AT LEVEL:
4 (C)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
100 hours 33 hours classroom contact67 hours directed/self-directed study and assessment preparation
10
UNIT STATUS Mandatory Core
11
PRE-REQUISITES None required
12
CO-REQUISITES
13
UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to:Knowledge and understanding
1. describe how health and social care is delivered in the United Kingdom.
2. describe the organisation of health and social care services in the United Kingdom.
3. identify the key and contemporary drivers of health and social care policy in the United Kingdom.
Cognitive/intellectual skills4. Compare different models of health and social
care.5. identify the relationship between healthcare
services and social care services.6. apply knowledge of teamwork to the delivery of
healthcare provision.7. support and develop arguments using reference to
relevant/contemporary literature8. communicate learning accurately and reliably
using structured coherent arguments

Practice Education
14
CURRICULUM OUTLINE
The unit is intended to enable the student to: Have an ability to identify the current key health and
social care drivers that have influenced physiotherapy practice.
Have an ability to identify the range of environments in which physiotherapy practice is delivered.
Describe the multi-agency approach in patient/client care.
Have an awareness of their professional responsibility in delivering inclusive, non-discriminatory physiotherapy rehabilitation to a diverse population.
15
LEARNING & TEACHING ACTIVITIES
A variety of teaching strategies will be used including: Group discussions Lead lectures Expert panel Service user and carer involvement Peer review On-line resources Case based learning
16
ASSESSMENT STRATEGIES
Formative procedures will be assessed by Formative written and oral feedback from academic
staff related to a presentation (LO1-8 – formative) Oral peer evaluation of presentation skills and
teamwork (LO6 and 8 – formative). Group presentation followed by group question and
answers (Learning outcomes 1-8 100% summative)
17
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate. An understanding of the unit content An ability to work within a group to develop and deliver
an oral presentation. An ability to communicate information both visually
and orally. An ability to answer questions related to information
presented. An ability to give and receive peer feedback
18
INDICATIVE STUDENT LEARNING RESOURCES
Baker, M. R., (2000) Making sense of the NHS White Papers. 2nd edition. Abdingdon: Radcliffe Medical Press.
Bartley, M., (2004) Health Inequality: an introduction to theories, concepts and methods. Oxford: Polity
Department of Health (2000) The NHS Plan: a plan for investment, a plan for reform London: Department of Health [online] http://www.dh.gov.uk/assetRoot/04/05/57/83/04055783.pdf
Department of Health (2004) Making partnership work for patients, carers and service users: A strategic agreement between the Department of Health, the NHS and the voluntary and community sector. London: Department of Health [Online] http://www.dh.gov.uk/assetRoot/04/08/60/58/04086058.pdf
Department of Health (2004) The NHS Improvement Plan:

Practice EducationPutting people at the heart of public services London: Department of Health. [Online] http://www.dh.gov.uk/assetRoot/04/08/45/22/04084522.pdf
Department of Health (2008) High quality care for all: NHS Next Stage Review final report. [Online] http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_085825French, S. and Sim, J. (2004) Physiotherapy : a Psychosocial Approach. 3rd ed., Oxford: Butterworth-Heinemann
Ham, C. (2009) Health Policy in Britain: the politics and organisation of the National Health Service. 6th edition. Basingstoke: Palgrave Macmillan
Melnyk, B. M. and Fineout-Overholt, E (2010) Evidence-based practice in nursing and healthcare: a guide to best practice 2nd edn. London: Philadelphia, PA: Lippincott Williams and Wilkins
World Health Organisation (2001) International Classification of Functioning, Disability and Health. Geneva; World Health Organisation. [Online] http://www.who.int/classifications/icf/en/
19
ANY ADDITIONAL NOTES AND COMMENTS
The content of this unit will support learning at level 4 and lay the necessary foundations for study at levels 5 and 6. The topics studied here will complement the content of parallel units and will be reinforced in other units throughout the programme.
20
DATE OF APPROVAL 11 & 12 February 2010
21
DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Physiotherapy Management: Cardiorespiratory 1
2 BRIEF SUMMARY This unit is intended to develop both cognitive and psychomotor skills of the student in the assessment and treatment of uncomplicated cardiorespiratory conditions in primary and secondary healthcare settings. The unit covers basic cardiorespiratory physiology, functional and applied anatomy, examination and management of uncomplicated cardiorespiratory conditions
3 UNIT CODE NUMBER 28151006
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Daphne Dawson
8 CREDIT VALUE 20 CREDITS AT LEVEL:
4
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
20065 hours classroom contact
135 hours directed/self-directed study and assessment preparation
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES
12 CO-REQUISITES
13 UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to:Knowledge and understanding
1. identify and explain normal respiration and the changes that occur as a result of disease.
2. identify and explain normal cardiac function and the changes that occur as a result of disease.
3. suggest patient focused, achievable and realistic goals of treatment that take into account the patient’s psychosocioeconomic needs.
4. identify the members of the multidisciplinary team involved in the management of predictable cardiorespiratory pathology and the role of the physiotherapist in this team.
Cognitive/intellectual skills5. apply knowledge of predictable cardiorespiratory
pathophysiology to select, plan, explain and evaluate (using basic methods) appropriate assessment and

Practice Educationphysiotherapy management techniques for patients with uncomplicated, predictable cardiorespiratory pathology.
6. evaluate basic outcome measures for monitoring patients with uncomplicated, predictable cardiorespiratory pathology.
Key/transferable skills7. use basic clinical reasoning and problem solving to
select, plan, explain and evaluate (using basic methods) the assessment and treatment of patients with uncomplicated, predictable cardiorespiratory pathology.
8. apply knowledge learned in previous units to uncomplicated, predictable cardiorespiratory pathology.
10. access and appraise the available evidence that underpins their assessment and patient management choices to support and develop arguments using reference to relevant/contemporary literature
Practical skills11. demonstrate appropriate, safe and accurate
assessment and physiotherapy management techniques for patients with uncomplicated, predictable cardiorespiratory pathology.
12. demonstrate and teach appropriate self-management techniques for patients with uncomplicated, predictable cardiorespiratory pathology.
13. propose a specified range of inclusive, non- discriminatory rehabilitation approaches in order to deliver holistic, patient focused care to a specified population with uncomplicated, predictable cardiorespiratory pathology.
14 CURRICULUM OUTLINE
This unit is intended to develop both cognitive and psychomotor skills of the student in the assessment and treatment of uncomplicated cardiorespiratory conditions in primary and secondary healthcare settings. The unit covers basic cardiorespiratory physiology, functional and applied anatomy, examination and management of uncomplicated cardiorespiratory conditions, for example asthma and myocardial infarction. Students will be facilitated to consider how physiotherapy skills can be adapted to match the needs of patients with a variety of presentations. The role of the physiotherapist in preventative healthcare interventions will be considered.
15 LEARNING & TEACHING ACTIVITIES
Strong use will be made of student centred, case based, problem solving learning strategies. Tutors create a challenging and supportive environment using a variety of learning and teaching strategies in conjunction with directed study. This will include lectures, tutorials, group work and practical skills workshops.
16 ASSESSMENT STRATEGIES
Compulsory workshops with self/peer evaluation and tutor feedback – (LO1-13 - formative)

Practice Education Objective Structured Practical Examination (LO1-13
– 100% summative)
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The student will demonstrate Understanding of the unit content. Apply their knowledge of cardiorespiratory physiology
to explain:o Pathologyo Clinical featureso Assessmento Treatment
for a range of clinical scenariosFormative – assessed by skills workshopsSummative assessment procedures will be assessed through generic level 4 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
18 INDICATIVE STUDENT LEARNING RESOURCES
Bourke, S. J. (2007) Lecture Notes on Respiratory Disease,7th h ed. Oxford: Blackwell Scientific
Braunwald, E. and Goldman, L. (2003) Primary Cardiology. 2nd ed. London: W. B. Saunders
Department of Health (2004) National Service Framework for Children, Young People and Maternity Services: Asthma, [Online] http://www.dh.gov.uk/assetRoot/04/08/92/27/04089227.pdf
Ganong, W. F. (2009) Review of Medical Physiology. 23rd ed. Connecticut: Appleton and Lange
Gould, B. E. (2006) Pathophysiology for the Health Professions. 3rd ed. London: Saunders
Guyton, A. C. and Hall, J. E. (2005) Textbook of Medical Physiology. 11th ed. Oxford: Elsevier Saunders
Hampton, J. R. (2008) The ECG Made Easy. 7th ed. Edinburgh: Churchill Livingstone
Handler, C. E. (2004) Cardiology in Primary Care. Oxford: Radcliffe Publications
Hough, A. (2001) Physiotherapy in Respiratory Care – A Problem Solving Approach. 3rd ed. Cheltenham: Nelson Thornes
Klabunde, R. (2005) Cardiovascular Physiology Concepts. Philadelphia: Lippincott, Williams and Wilkins
McArdle, W. D., Katch, F. I. and Katch, V. L. (2010) Exercise Physiology. Nutrition, Energy and Human Performance. 7th ed. Baltimore: Lippincott Williams & Wilkins
Pryor, J. A. and Prasad, S. A. (2008) Physiotherapy for Respiratory and Cardiac Problems: Adults and Paediatrics. 4th ed. Edinburgh: Churchill Livingstone
Scottish Intercollegiate Guideline Network. (2000) SIGN No.

Practice Education97: Secondary Prevention of Coronary Heart Disease following Myocardial Infarction, [online] www.sign.ac.uk/guidelines
Scottish Intercollegiate Guideline Network. (2001) SIGN No. 55: Management of Diabetes, [online] www.sign.ac.uk/guidelines
Scottish Intercollegiate Guideline Network. (2002) SIGN No. 57: Cardiac Rehabilitation, [Online] www.sign.ac.uk/guidelines
Scottish Intercollegiate Guideline Network. (2004) SIGN No. 101: British Guideline on the Management of Asthma, [online] www.sign.ac.uk/guidelines
Spector, T. D. and Hall, P. (1999) An Introduction to General Pathology, 4th ed. Edinburgh: Churchill Livingstone
Sweetland, H. and Conway, K. (2004) Crash Course Surgery. Edinburgh: Mosby
Varjavand, N. (2000) The Interactive Oxyhemaglobin Dissociation Curve, [online] http://www.ventworld.com/resources/oxydisso/dissoc.html
Wasserman, K. (2005) Principles of Exercise Testing and Interpretation, including Pathophysiology and Clinical Applications. 4th ed. London: Lippincott, Williams and Wilkins.
Watkins, P. J (2003) ABC of Diabetes. (eBook) (Publication: London: BMJ Books)
Way, L. W. and Doherty, G. M. (2006) Current Surgical Diagnosis and Treatment. 12th ed. London: Lange Medical Books/McGraw Hill
19 ANY ADDITIONAL NOTES AND COMMENTS
The content of this unit will support learning at level 4 and lay the necessary foundations for study at levels 5 and 6. The topics studied here will complement the content of parallel units and will be reinforced in other units throughout the programme.It is a professional body requirement that students will not be entitled to receive condoned passes for assessment that include practical skills.
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Physiotherapy Management: Neurology 1
2 BRIEF SUMMARY This unit is concerned with the development of a knowledge base and skills set to enable the student to undertake reasoned assessment and treatment of patients with common and predictable neurological impairments for example stroke. Reference is made to evidence based guidelines that shape practice. Students will consider a range of widely used, outcome measures in preparation for the practice placement units of the programme.
3 UNIT CODE NUMBER 28151007
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Rachel Stockley
8 CREDIT VALUE 20 CREDITS AT LEVEL:
4(C)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
20065 hours classroom contact
135 hours directed/self-directed study and assessment preparation
10 UNIT STATUS Mandatory core
11 PRE-REQUISITES
12 CO-REQUISITES
13 UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to:Knowledge and understanding
1. apply knowledge of anatomy, neuromuscular control of normal movement and the structure and function of the nervous system to explain the clinical features of selected predictable neurological deficits.
2. suggest patient focused, achievable and realistic goals of treatment that take into account the patient’s psychosocioeconomic needs.
3. identify the members/roles of the multidisciplinary team involved in the management of selected, predictable neurological deficits and the role of the physiotherapist in this team.
Cognitive/intellectual skills4. apply knowledge of the principles of normal
movement and the structure and function of the

Practice Educationnervous system to select, plan, explain and evaluate (using basic methods) appropriate assessment and treatment techniques for patients with predictable neurological deficits.
5. evaluate, appropriate basic outcome measures for patients with predictable neurological deficits.
Key transferable skills6. use basic clinical reasoning and problem solving to
plan, explain and evaluate the assessment and treatment of patients with predictable neurological deficits.
7. apply knowledge learned in previous units to predictable neurological deficits.
8. access and apply the available evidence that underpins their assessment and patient management choices to support and develop arguments using reference to relevant/contemporary literature
9. communicate their learning in a written format that fulfils the requirements of academic writing.
Practical skills10. use their knowledge of patients with predictable
neurological deficits to explain their selection of safe, accurate assessment and treatment techniques that are appropriate for this group of patients.
11. propose a specified range of inclusive, non-discriminatory rehabilitation approaches in order to deliver holistic, patient focused care to a specified population with predictable neurological deficits.
12. Present information using an appropriate academic style.
14 CURRICULUM OUTLINE
This unit is intended to develop the student’s attitudes, skills and knowledge related to the physiotherapy assessment and management of the patient with the neurological deficits considered during the unit. Principles will be based on a variety of treatment approaches including the Bobath concept, and the Motor Relearning approach. Students will apply anatomical and physiological knowledge of the nervous system and select and utilise a range of functional outcome measures for people with predictable neurological deficits for example stroke.The structure of the unit will allow the student to develop the clinical reasoning skills that will underpin their physiotherapy practice.
15 LEARNING & TEACHING ACTIVITIES
Makes use of student centred learning strategies with tutors creating both a challenging and supportive environment using a variety of delivery methods in conjunction with indicative reading. A variety of strategies are used including lectures, practical demonstrations, group work/role play, skills sessions and tutorials.Tutors will be drawn from both academic and clinical backgrounds.The teaching and learning will be case-based and use a

Practice Educationproblem solving approach.
16 ASSESSMENT STRATEGIES
Self evaluation activities (paper and internet based) linked to unit and session learning outcomes (1, 3-10 - formative).
Skills based workshops with self/peer evaluation and tutor feedback (1, 4 - 11 - formative)
Essay based assignment (case based, clinical pathology, clinical reasoning, patient management) (1-12 – 100% summative)
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
Formative – assessed by skills revision sessions and e-learning self assessment quizzes.Summative assessment procedures will be assessed through generic level 4 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
18 INDICATIVE STUDENT LEARNING RESOURCES
Burnett, M. G., Zager, E. L. (2004), ‘Pathophysiology of peripheral nerve injury: a brief review.’ Neurosurg focus, vol. 16, no. 5, pp. 1-7 [online]. http://www.aans.org/education/journal/neurosurgical/may04/16-5-1.pdf
Carr, J. H. and Shepherd, R. B. (1998), Neurological Rehabilitation: optimizing motor performance, Oxford, Butterworth Heinemann
Edwards, S (2002) Neurological physiotherapy 2nd edn London: Churchill Livingstone
Greenberg, D. A., Aminoff, M. J., and Simon, R. P. (2009), Clinical Neurology, 7th edn, McGraw-Hill
Harvey, L. (2008) Management of spinal cord injuries: a guide for physiotherapists. London: Churchill Livingstone
Intercollegiate Working Party (2008), The National Clinical Guidelines on Stroke 3rd ed. London: Royal College of Physicians [online] http://www.rcplondon.ac.uk/pubs/contents/6ad05aab-8400-494c-8cf4-9772d1d5301b.pdf
Langhammer, B. and Stranhelle, J. K. (2000). Bobath or Motor Relearning Programme. ‘A comparison of two different approaches of physiotherapy in stroke rehabilitation: a randomised controlled. Clinical Rehabilitation, 14 (4) 361-369]
Lennon, S and Stokes, M. (2008) Pocketbook of Neurological Physiotherapy. Edinburgh: Churchill Livingstone
Pollock, A., Baer, G., Pomeroy, V. and Langhorne, P.

Practice Education
Physiotherapy treatment approaches for the recovery of postural control and lower limb function following stroke. Cochrane Database of Systematic Reviews 2007, Issue 1. Art. No.: CD001920. DOI: 10.1002/14651858.CD001920.pub2.
Saunders, D. H., Greig, C. A., Young, A. and Mead, G. E. Physical fitness training for stroke patients. Cochrane Database of Systematic Reviews 2004, Issue 1. Art. No.: CD003316. DOI: 10.1002/14651858.CD003316.pub2
Shumway Cook, A. and Woollacott, M. (2007) Motor control: translating research into clinical practice 3rd edn Philadelphia: Lippincott, Williams and Wilkins
Stokes, M. (2004), Neurological physiotherapy 2nd edn. London, Mosby
Teasell, R. (2003), Stroke recovery and rehabilitation, Stroke, vol. 34, pp. 365-366.
Trew, M. and Everett, T. (eds) (2005) Human Movement. An Introductory Text. 5th ed. Edinburgh: Churchill Livingstone.
World Health Organization (2001), International classification of functioning, disability and health World Health Organization
19 ANY ADDITIONAL NOTES AND COMMENTS
The content of this unit will support learning at level 4 and lay the necessary foundations for study at levels 5 and 6. The topics studied here will complement the content of parallel units and will be reinforced in other units throughout the programme.
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Practice Placement 0 – Participant Observation
2 BRIEF SUMMARY Students will have opportunity to observe and participate in physiotherapy management of patients in the locality that they choose. However, during this placement the student is not expected to be solely responsible for assessment/physiotherapy management/evaluation of the effectiveness of physiotherapy management for a caseload. They must be supervised during the placements by a physiotherapist whose name appears on the register maintained by the Health Professions Council. It may be possible for this placement to occur in an institution outside the United Kingdom. In all circumstances the placements must be deemed to be suitable and meet minimum standards relating to Health and Safety at Work and Equal Opportunities legislation.
3 UNIT CODE NUMBER 28151008
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Joanne Nicholson/Sophie Taylor
8 CREDIT VALUE CREDITS AT LEVEL:
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
24 hours clinical practice
10 UNIT STATUS Mandatory core
11 PRE-REQUISITES Students will have engaged with all level 4 units before this placement is undertaken.
12 CO-REQUISITES
13 UNIT LEARNING OUTCOMES
The student will have demonstrated or attained:1. The ability to match Standards relating to
professional behavioura. Apply their knowledge of departmental health
and safety policy to specific patient groups/conditions (e.g. Infection control, moving and handling policy, operation of medical devices.
b. Awareness of and regard to the contraindications of treatment.
c. Inform the practice placement educator about adverse findings and/or patient complaints

Practice Educationwhere relevant.
2. the ability to adhere to organisational policies and procedures that relate to Health and Safety at work
a. Comply with and has adequate knowledge of the Rules of Professional Conduct.
b. Demonstrate satisfactory punctuality and time keeping.
c. Implement local arrangements and agreed procedures
d. respect patient confidentiality. e. Appropriate standards of dress and /or
hygiene in relation to departmental policy. f. Facilitate the mutual trust and respect
inherent within a therapeutic relationship.
14 CURRICULUM OUTLINE
The student will be able to achieve the learning outcomes by adopting the role of a participant observer in a health care setting under the supervision of a physiotherapist
15 LEARNING & TEACHING ACTIVITIES
Depending upon the location of the placement that the student arranges for themselves:
Observation of the assessment and treatment of patients under the supervision of a physiotherapist
Experiential learning with reflective practice in the clinical setting
Self-directed study Attendance at meetings/case conferences
16 ASSESSMENT STRATEGIES
self/practice placement educator evaluation based on worksheets and checklists (formative)
Reflective log/diary to promote reflection on performance supported by practice placement educator (formative)
Individual debriefing following placement facilitated by personal tutor and group debriefing facilitated by academic staff (formative)
Evidence of performance on placement based on criteria related to unit learning outcomes that matches PSRB requirements for professional conduct (Summative, LO1 a-c)
Evidence of performance on placement based on criteria related to unit learning outcomes that demonstrates adherence to placement policies and procedures relating to Health and Safety at Work (Summative, LO2 a-f).
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The unit will be assessed as pass/fail in accordance with regulation D2.2 (Assessment Regulations for Undergraduate Programmes of Study 2009-2010). In order to be credited with the associated practice placement hours the student’s practice placement educator must confirm that the student’s practice has matched PSRB requirements as stated in the Rules of Professional Conduct of the CSP (2002b) and the Standards of Performance, Conduct and Ethics of the HPC (2008) articulated through unit specific criteria and that they have been able to demonstrate adherence to placement

Practice Educationpolicies and procedures as these relate to Health and Safety at Work.
The student will provide evidence of satisfactory completion of 24 hours of participant observation using standardised documentation provided by the programme team and validated by the supervising practice placement educator.
18 INDICATIVE STUDENT LEARNING RESOURCES
Chartered Society of Physiotherapy. (2002) Rules of professional conduct. 2nd ed. London: Chartered Society of Physiotherapy. [Online] [Accessed on 27 April 2009] http://www.csp.org.uk/uploads/documents/csp_rules_conduct.pdf
Health Professions Council (2010), Guidance on conduct and ethics for students. London: Health Professions Council.Health Professions Council. (2008) Standards of conduct, performance and ethics. London: Health Professions Council. [Online] [Accessed on 22 May 2009] http://www.hpc-uk.org/assets/documents/10002367FINALcopyofSCPEJuly2008.pdf
Moon, J. A. (2004) A handbook of reflective and experiential learning: theory and practice. London: Taylor and Francis.
19 ANY ADDITIONAL NOTES AND COMMENTS
While this unit is not associated with academic credit it must be successfully completed for the student to be eligible to proceed to the second year of the programme and is a prerequisite for units at level 5 within the programme. Students must provide evidence of satisfactory completion of 24 hours of participant observation using standardised documentation provided by the programme in order to progress to level 5.
Students who do not successfully complete this practice placement unit at first attempt will be entitled to subsequent attempts at the discretion of the Board of Examiners.
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Physiotherapy Management: MSK 2
2 BRIEF SUMMARY This unit considers the lumbar spine and lower limb. Skills developed during earlier units will be developed further and students will learn how to adapt these skills and apply them to the lower quadrant. There is a strong focus on enhancing clinical reasoning which will include exploration of biopsychosocial factors that can impact on physiotherapy management and treatment outcomes.
3 UNIT CODE NUMBER 28151009
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Gill Yeowell
8 CREDIT VALUE 20 CREDITS AT LEVEL:
5 (I)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
20050 hours classroom contact150 hours directed/self-directed study and assessment preparation
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES All units at level 4 (C)Practice Placement 0
12 CO-REQUISITES None
13 UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to:Knowledge and understanding
1. critically apply knowledge of the structure and function of the lower quadrant to explain the pathology and clinical features of selected pathologies of the lower quadrant.
2. propose and justify patient focused, achievable and realistic goals of treatment that take into account the patients’ psychosocioeconomic needs.
Cognitive/intellectual skills3. critically apply their knowledge in order to select,
plan, explain and evaluate appropriate assessment procedures for patients with selected pathologies of the lower quadrant and interpret the findings.
4. critically evaluate appropriate a wide range of outcome measures for patients with selected pathologies of the lower quadrant.
Key/transferable skills5. clinically reason with reference to relevant literature
appropriate management including biopsychosocial

Practice Educationfactors in the rehabilitation of selected conditions in the lower quadrant.
6. critically apply knowledge learned in previous units to pathologies of the lower quadrant.
7. access, critically appraise and apply the available evidence that underpins physiotherapy assessment and patient management choices.
Practical skills8. plan, safely/correctly demonstrate and justify with
reference to relevant literature appropriate physiotherapy management strategies for specific pathological conditions in the lower quadrant.
9. apply a specified range of inclusive, non-discriminatory rehabilitation approaches in order to deliver holistic, patient focused care to a specified population with selected pathologies of the lower quadrant.
10. Communicate complex information in a professionally and academically appropriate style.
CURRICULUM OUTLINE
This unit is intended to develop both cognitive and psychomotor skills in the undergraduate physiotherapist. The main principles are the integration and application of anatomical knowledge in conjunction with relevant biopsychosocial factors to selected pathologies of the lower quadrant which will enable the student to clinically reason, explain and justify their clinical decisions. This unit covers functional anatomy, biomechanics, surface marking, differential diagnosis and treatment of pathologies (for example inflammatory/degenerative arthropathies) in the following regions: lumbar spine, sacroiliac joint, hip, knee and ankle and incorporates a range of rehabilitation approaches.
15 LEARNING & TEACHING ACTIVITIES
Makes use of student centred learning strategies with lecturers creating both a challenging and supportive learning environment using a variety of delivery methods in conjunction with indicative reading and material accessed by students themselves. A variety of strategies are used including: illustrated lectures, practical demonstrations, practical skills sessions, tutorials, critical appraisal, e-learning, group work and role play.
16 ASSESSMENT STRATEGIES
Practical workshop (LO1-11 – formative). Students will receive comprehensive verbal feedback from tutors and peers.
Unstaffed peer assessment practical sessions – formative (LO1-11 - formative). Verbal feedback will be provided by peers, with guidance from resources including books and other literature.
Oral clinical reasoning examination (element 1 – 50% of unit mark – summative LO1 – 7 and 10) and practical skill examination (assessment and treatment skills 50% of unit mark – summative LO4 and 6 -10) (30 minutes)

Practice Education
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The student will demonstrate: An understanding of the unit content An ability to use clinical reasoning to explain the
relationship between pathology/clinical features and the physiotherapy management of lower quadrant pathologies.
An ability to select, plan and justify appropriate physiotherapy management for a described patient.
An ability to safely and accurately demonstrate physiotherapy assessment and management techniques for the selected pathologies.
An ability to communicate clearly, coherently and using appropriate terminology with both models and colleagues.
Formative assessment – peer assessment using self-evaluation checklists linked to the unit/session learning outcomes.Summative assessment procedures will be assessed through generic level 5 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
18 INDICATIVE STUDENT LEARNING RESOURCES
Adams, M. A., Burton, K., Dolan, P., Bogduk, N. (2006) The biomechanics of back pain. Edinburgh: Churchill Livingstone Elsevier.
Boyling, J. D. and Jull, G. A. (2004) Grieve’s modern manual therapy: the vertebral column. 3rd ed. Edinburgh: Churchill Livingstone Elsevier.
Chartered Society of Physiotherapy (2006) Clinical guidelines for the physiotherapy management of persistent low back pain: part 1: exercise. London: Chartered Society of Physiotherapy.
Chartered Society of Physiotherapy (2006) Clinical guidelines for the physiotherapy management of persistent low back pain: part 2: manual therapy. London: Chartered Society of Physiotherapy.
Hengeveld, E. and Banks, K. (2005) Maitland's vertebral manipulation. 7th ed. Oxford: Butterworth-Heinemann.
Main, C. J. and Spanswick, C. C. (2000) Pain management: an interdisciplinary approach. New York: Churchill Livingstone.
Maitland, G. D. (2002) Vertebral manipulation 6th ed. Oxford: Butterworth-Heinmann.
Mckenzie, R. (2003) The lumbar spine: mechanical diagnosis and therapy. New Zealand: Spinal Publications New Zealand Ltd.
Middleditch, A. and Oliver, J. (2005) Functional anatomy of the spine. 2nd ed. Oxford: Butterworth-Heinemann.
National Institute for Health and Clinical Excellence (2009)

Practice EducationLow back pain: Early management of persistent non-specific low back pain. [online] [cited 10th June 2009] http://guidance.nice.org.uk/CG88
Richardson, C., Hodges, P. W. and Hides, J. (2004) Therapeutic exercise for lumbopelvic stabilisation, a motor control approach for the treatment and prevention of low back pain. Edinburgh: Churchill Livingstone.
Shacklock, M. O. (2005) Clinical neurodynamics: a new system of musculoskeletal treatment. Edinburgh: Butterworth-Heinemann.
Violante, F. and Kilbom, A. (2000) Occupational ergonomics: work related musculoskeletal disorders. London: Taylor Francis.
Waddell, G. (2004) The back pain revolution. 2nd ed. Edinburgh: Churchill Livingstone.
Woby, S. R., Watson, P. J., Roach, N. K., Urmston, M. (2005) ‘Coping strategy use: does it predict adjustment to chronic back pain after controlling for catastrophic thinking and self efficacy for pain control?’ Journal of Rehabilitation Medicine. Vol. 37, pp. 100-107.
Osteoarthritis
Arthritis Care (2004) OA nation report. [Online] [cited 17/6/2009] http://www.arthritiscare.org.uk/PublicationsandResources/Forhealthprofessionals/OANation
Bennell, K; Hinman, R. S; Metcalf, B. R.; Crossley, K. M.; Buchbinder, M.; Smith, M.; and McColl, G. (2003) ‘Relationship of knee joint proprioception to pain and disability in individuals with knee osteoarthritis.’ Journal of Orthopaedic Research, vol. 21, no. 5, pp. 792-797.
Bijlsma, J. W. J.; Knahr, K. (2007) ‘Strategies for the prevention and management of osteoarthritis of the hip and knee.’ BEST PRACTICE AND RESEARCH CLINICAL RHEUMATOLOGY. Vol. 21, no. 1, pp. 59-76.
French, H. P. (2007)’ Physiotherapy management of osteoarthritis of the hip: a survey of current practice in acute hospitals and private practice in the Republic of Ireland.’ Physiotherapy, vol. 93, pp. 253-260.
Hinman, R. S.; Heywood, S. E. and Day, A. R. (2007) ‘Aquatic physical therapy for hip and knee osteoarthritis: Results of a single blind randomised controlled trial.’ Physical Therapy, vol. 87, no. 1, pp. 32-43.
McCarthy, C. J.; Mills, P. M.; Pullen, R.; Roberts, C.; Siman, A. and Oldham, J. A. (2004) ‘Supplementing a home exercise programme with a class based exercise programme is more effective than home exercise alone in the treatment

Practice Educationof knee osteoarthritis.’ Rheumatology. Vol. 43, pp. 880-886.
National Collaborating Centre for Chronic Conditions (2008) Osteoarthritis: national clinical guidelines for care and management in adults. London: Royal College of Physicians.
National Health Service. (2007) What is the evidence that muscle training matters in the management of OA? [Online] [cited 17/6/2009] http://www.library.nhs.uk/musculoskeletal/ViewResource.aspx?resID=267877
Van Baar, M. E.; Dekker, J.; Oostendorp, R. A. B.; Bijl, D.; Voorn, T. B.; and Bijlsma, J. W. J. (2001) ‘Effectiveness of exercise therapy in patients with osteoarthritis of the hip and knee; nine months follow up.’ Ann Rheum Dis. Vol. 60, pp. 1123-1130.
Walsh, NE; Mitchell, HL; Reeves, BC; and Hurley, MV. (2006) ‘Integrated exercise and self-management programs in osteoarthritis of the hip and knee: a systematic review of effectiveness.’ Physical Therapy Reviews. Vol. 11, pp. 289-297.
Yates, B. (ed) (2008) Merriman’s assessment of the lower limb. Edinburgh 3rd edn: Churchill Livingstone.
Further resources
Anatomy.tv. [electronic resource]. Accessed via the MMU library website.
Beil, A. R. (2005) Trail Guide to the Body: How to Locate Muscles, Bones, and More. 3rd ed. Boulder, USA, Books of Discovery.
Guyton, A. C and Hall, J. E. (2005) Textbook of medical physiology. 11th ed. Philadelphia, P.A.: Elsevier Saunders.
Jones, M. A. and Rivett, D. A (2003). Clinical reasoning for manual therapists. Edinburgh: Butterworth-Heinemann.
Kesson, M. and Atkins, E. (2005) Orthopaedic medicine: a practical approach. Oxford: Butterworth Heinemann.
Kisner, C. and Colby, L. A. (2007) Therapeutic exercise: foundations and techniques. 5th ed. Philadelphia, P. A.: F. A. Davis.
Levangie, P. K. (2005) Joint structure and function: a comprehensive analysis. 4th ed. Philadelphia, P.A.: F. A. Davis.
Magee D. J. (2008) Orthopaedic physical assessment. 5th ed. London: Saunders.
Palastanga, N., Field, D. and Soames, R. (2006) Anatomy and human movement: structure and function. 5th ed. Oxford: Butterworth Heinemann.
Petty, N.J. and Moore, A. (2005) Neuromusculoskeletal

Practice Educationexamination and assessment: a handbook for therapists. 3rd ed. Edinburgh: Churchill Livingstone.
Soames, R. (2003) Joint motion: clinical measurement and evaluation. Edinburgh: Churchill Livingstone.
19 ANY ADDITIONAL NOTES AND COMMENTS
The content of this unit will support learning at level 5 and 6. The topics studied here will complement the content of parallel units and will be reinforced in other units throughout the programme.It is a professional body requirement that students will not be entitled to receive condoned passes for assessment that include practical skills. Both elements of the unit assessment must be passed with a mark ≥40 and the unit must be passed with a mark ≥40.
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE
Physiotherapy Management: Cardiorespiratory 2
2 BRIEF SUMMARY
This unit builds on learning at level 5 and considers more complex and less predictable pathologies of the cardiorespiratory system including peripheral vascular disease. There is a strong emphasis on the evidence base that supports physiotherapy management. Students will consider issues that relate to care that has its focus on maintenance, support and palliation and the physiotherapy contribution to the provision of high quality care at the end of life.
3 UNIT CODE NUMBER
28151010
4 HOME PROGRAMME
BSc (Hons) Physiotherapy
5 HOME DEPARTMENT
Health Professions
6 SUBJECT AREA
B160: physiotherapy
7 UNIT LEADER(S)
Daphne Dawson
8 CREDIT VALUE
20 CREDITS AT LEVEL:
5 (I)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
20050 hours classroom contact
150 hours directed/self-directed study and assessment preparation
10
UNIT STATU
Mandatory Core

Practice Education
S
11
PRE-REQUISITES
All units at level 4 (C)Practice Placement 0
12
CO-REQUISITES
None
13
UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to,:Knowledge and understanding
1. critically apply and explain their knowledge of normal respiration and the changes that occur as a result of complex and less predictable disease, deformity or malformation.
2. critically apply and explain their knowledge of normal cardiac function and the changes that occur as a result of complex and less predictable disease, deformity or malformation.
3. explain the psycho-socio-economic issues for patients suffering from complex and less predictable cardiorespiratory pathology and adapt the patients’ goals and management appropriately in order to deliver holistic, patient focused care.
4. develop the ability to collaborate with and refer to other members of the multidisciplinary team involved in the management of complex and less predictable cardiorespiratory pathology and explain the role of the physiotherapist and other professionals in this team.
Cognitive/intellectual skills5. critically apply their knowledge of predictable cardiorespiratory
pathophysiology to select, plan, justify and evaluate a range of appropriate assessment and physiotherapy management techniques for patients with complex and less predictable cardiorespiratory pathology.
6. evaluate a wide range of appropriate outcome measures for monitoring patients with complex and less predictable cardiorespiratory pathology.
Key/transferable skills7. critically apply clinical reasoning and problem solving to select, plan,
justify and evaluate the assessment and treatment of patients with complex and less predictable cardiorespiratory pathology in a variety of clinical settings.
8. critically apply knowledge and skills learned in previous units to complex and less predictable cardiorespiratory pathology.
11. access, critically appraise and apply the available evidence that underpins physiotherapy assessment and patient management choices.
Practical skills9. select and justify a range of appropriate, safe and accurate
assessment and physiotherapy management techniques for patients with complex and less predictable cardiorespiratory pathology.
10. select and justify a range of appropriate self-management techniques for patients with complex and less predictable cardiorespiratory pathology.
11. select and justify range of inclusive, non discriminatory rehabilitation
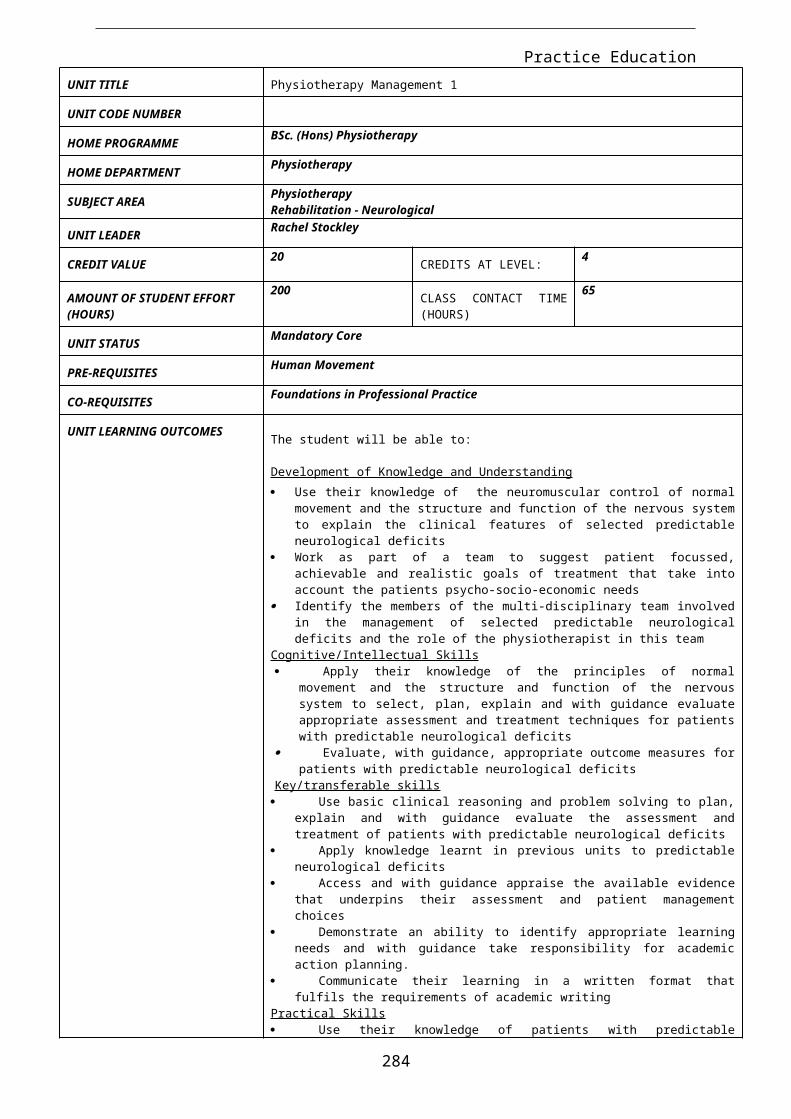
Practice Educationapproaches (including restorative, supportive and palliative) in order to deliver holistic, patient focused care to a range of patients suffering from complex and less predictable cardiorespiratory pathology.
12. Present information in an appropriate academic style.
14
CURRICULUM OUTLINE
This unit is intended to further develop both cognitive and psychomotor skills of the student in assessment and treatment of a range of more complex cardiorespiratory conditions (for example chronic obstructive pulmonary disease). The unit covers cardiorespiratory physiology, functional and applied anatomy, examination and management of the less predictable cardiorespiratory conditions in primary and secondary health care settings. A variety of rehabilitation approaches will be considered and clinical reasoning skills will be further developed through the use of more complex clinical scenarios.
15
LEARNING & TEACHING ACTIVITIES
Strong use will be made of student centred, case based problem solving learning strategies. Tutors create a challenging and supportive environment using a variety of learning and teaching strategies in conjunction with directed study. This will include lectures, tutorials, group work and practical skills workshops. There will be an increased use of the evidence base.
16
ASSESSMENT STRATEGIES
Practical skills workshops with self/peer and tutor evaluation and feedback (LO1-11 – formative)
Self assessment questions (paper and internet based)– (LO 1-11 – formative)
Essay based assignment (case based, clinical pathology, clinical reasoning and patient management) (8 sides A4 double spaced) – (Learning outcomes 1-12 - 100% summative)
17
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The student will demonstrate: An understanding of the unit content An ability to use clinical reasoning in order to select, plan and justify
appropriate physiotherapy management techniques for a case study patient
Select effective patient assessment and management techniques that are clinically appropriate for the case study patient
Demonstrate a patient focused and holistic approach to patient care An ability to present arguments in an appropriate academic style An ability to use the evidence base to generate and support
argumentsFormative assessment procedures will assessed by peer assessment using self evaluation checklists linked to the unit/session learning outcomes with personal tutor support/academic action planning.Summative assessment procedures will be assessed through generic level 5 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
18
INDICATIVE STUDENT LEARNING RESO
Baines, S, Garrod, R. and Morgan, M (2004) ‘Standards for outpatient Pulmonary Rehabilitation.’ Journal of the ACPRC, vol. 36, pp. 44-46
BBC News Channel (2008) Girl Wins Right to Refuse Heart, [Online] http://news.bbc.co.uk/1/hi/england/hereford/worcs/7721231.stm
Bourke, S. J. (2007) Respiratory medicine. 7th ed. Oxford: Blackwell
British Thoracic Society (2009) Concise BTS/ACPRC Guidelines.

Practice Education
URCES Physiotherapy Management of the Adult, Medical, Spontaneously Breathing Patient, [online] www.brit-thoracic.org.uk/Portals/0/Clinical%20Information/Physiotherapy/PhysiotherapyGuideline/PhysioConcise-web.pdf
Camp, P. G., Appleton, J. and Reid, W. D. (2000) ‘Quality of life after pulmonary rehabilitation: assessing change using quantitative and qualitative methods.’ Physical Therapy, vol. 80, no. 10, pp. 986-995
Chartered Society of Physiotherapy (2003) The effectiveness of pulmonary rehabilitation: evidence and implications for physiotherapists, [Online] http:// www.csp.org.uk/director/members/libraryandpublications/csppublicatio ns.cfm?item_id=74C873050E654C8CF266687968C0C097
Cystic Fibrosis Trust (2001) Standards for the Clinical care of Children and Adults with Cystic Fibrosis in the UK, [Online] http://www.cftrust.org.uk/scope/documentlibrary/CFTRust/Standards%20of%20Care.pdf
Department of Health (2005) National Service Framework for Long-term Conditions - Good Practice Guide, [Online] http://www.dh.gov.uk/PolicyAndGuidance/HealthAndSocialCareTopics/LongTermConditions/BestPractice/GoodPracticeGuide/fs/en?CONTENT_ID=4105451&chk=BRvkwN
Department of Health (2004) Report from the National Clinical Director for Children on the development of the National Service Framework for Children, Young People and Maternity Services, [Online] http://www.dh.gov.uk/PublicationsAndStatistics/Publications/PublicationsPolicyAndGuidance/PublicationsPolicyAndGuidanceArticle/fs/en?CONTENT_ID=4116394&chk=BQ05dx
Department of Health (2004) The NHS cancer plan and the new NHS: Providing a patient-centred service, [Online] http://www.dh.gov.uk/PublicationsAndStatistics/Publications/PublicationsPolicyAndGuidance/PublicationsPolicyAndGuidanceArticle/fs/en?CONTENT_ID=4092531&chk=2OgU1i
Department of Health (1999) A National Service Framework for mental health, [Online] http://www.dh.gov.uk/assetRoot/04/07/72/09/04077209.pdf
Everett, T., Donaghy, M. and Feaver, S. (2003) Interventions for Mental Health: An evidence-based approach for Physiotherapists and Occupational Therapists. Edinburgh: Butterworth-Heinemann
Faull, C., Carter, Y. H. and Daniels, L. (eds) (2005) Handbook of palliative care. 2nd ed. Oxford: Blackwell.
Glassey, N. (2004) Physiotherapy for Burns and Plastic Reconstruction of the Hand. London: Whurr
Harden, B. (2004) Emergency physiotherapy. Edinburgh: Churchill Livingstone
Hough, A. (2001) Physiotherapy in respiratory care – an evidence-based approach to respiratory and cardiac management. 3rd ed. Cheltenham: Nelson Thornes
Koike, A. K., Unützer, J. and Wells, K. B. (2002) ‘Improving the care for

Practice Educationdepression in and patients with comorbid medical illness’. American Journal of Psychiatry, vol. 159, pp 1738-1745
McGavin, C. R., Gupta, S .P. and McHardy, G. J. R. (1976) 12-minute walking test for assessing disability in chronic bronchitis. British Medical Journal Vol. 1, No. 6013, pp 822-823
National Institute for Clinical Excellence (2004) Guidelines for the management of COPD in adults in primary and secondary care, [Online] http://www.nice.org.uk/page.aspx?o=cg012&c=respiratory
National Institute for Clinical Excellence (2004) Depression: management of depression in primary and secondary care, [Online] http://www.nice.org.uk/page.aspx?o=cg023quickrefguide
Pryor, J. A. and Prasad, S. A. (2008) Physiotherapy for respiratory and cardiac problems: adults and paediatrics. 4th ed. Edinburgh: Churchill Livingstone
Singh, S. J., Morgan, M, D. L., Scott, S., Walters, D, and Hardman A. E. (1992): ‘Development of a shuttle walking test of disability in patients with chronic airways obstruction’. Thorax, vol. 47, no. 12, pp. 1019-1024
Stiller, K. (2000) ‘Physiotherapy in intensive care: towards an evidence-based practice.’ Chest, vol. 118, no. 6, pp. 1801-1813
Taylor-Piliae, R. (2002) ‘Review: several techniques optimise oxygenation during suctioning of patients.’ Evidence Based Nursing, vol. 5, p 51
Watson, M.S. (2008) Oxford handbook of palliative care 2nd edn. Oxford: Oxford University Press
West, J. B. (2008) Pulmonary Pathophysiology – the essentials. 7th ed. Baltimore: Lippincott, William and Wilkins
Yohannes, A. M., Baldwin, R. C. and Connolly, M. J. (2000) Depression in elderly outpatients with disabling chronic obstructive pulmonary disease. Age and Aging, vol. 27, pp 155-160
19
ANY ADDITIONAL NOTES AND COMMENTS
The content of this unit will support learning at level 5 and 6. The topics studied here will complement the content of parallel units and will be reinforced in other units throughout the programme.
20
DATE OF APPROVAL
11 & 12 February 2010
21
DATE OF

Practice Education
MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Physiotherapy Management: Neurology 2
2 BRIEF SUMMARY This unit builds on learning at level 5 to consider more complex and less predictable impairment in the neurological system for example multiple sclerosis. In addition it will facilitate consideration of the provision of physiotherapy treatment to the management of traumatic brain injury and cerebral palsy and in so doing requires the students to consider how treatment should be adapted to match the needs of patients across the age spectrum.
3 UNIT CODE NUMBER
28151011
5 HOME PROGRAMME
BSc (Hons) Physiotherapy
5 HOME DEPARTMENT
Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Peter Goodwin
8 CREDIT VALUE 20 CREDITS AT LEVEL:
5 (I)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
20050 hours classroom contact
150 hours directed/self-directed study and assessment preparation
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES All units at level 4 (C)Practice Placement 0
12 CO-REQUISITES
13 UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to have attained or demonstrated:Knowledge and understanding
1. critically apply their knowledge of the neuromuscular control of normal movement and the structure and function of the nervous system to explain the clinical features of complex and less predictably neurological deficits.
2. critically discuss collaboration with the multidisciplinary team to suggest patient focused, specific, measurable, achievable and timed goals that take into account the patients’ psychosocioeconomic needs.
3. critically discuss collaboration with and referral to members of the multidisciplinary team and identify how each profession can contribute to the delivery of holistic, patient focused care for patients with complex and less

Practice Educationpredictable neurological deficits.
Cognitive/intellectual skills4. critically apply their knowledge of the principles of
normal movement and the structure and function of the nervous system to select, plan, justify and evaluate appropriate assessment and treatment techniques for patients with complex and less predictable neurological deficits.
5. evaluate and select appropriate outcome measures from a range of outcome measures suitable for patients with complex and less predictable neurological deficits.
Key/transferable skills6. use clinical reasoning and problem solving to select,
plan, justify and evaluate the assessment and treatment of patients with complex and less predictable neurological deficits in a variety of clinical settings.
7. Critically apply knowledge learned in previous units to complex and less predictable neurological deficits.
8. access, critically appraise and apply the available evidence that underpins physiotherapy assessment and patient management choices.
Practical skills9. critically apply knowledge of patients with complex and
less predictable neurological deficits to execute and document a range of safe, accurate assessment and treatment techniques that are appropriate for this group of patients.
10. critically apply a range of inclusive, non-discriminatory rehabilitation approaches (including restorative, supportive and palliative) in order to deliver holistic, patient focused care to a diverse population suffering from complex and less predictable neurological deficits.
14 CURRICULUM OUTLINE
This unit is intended to develop the students’ attitudes, skills and knowledge related to the physiotherapy assessment and management of patients with complex neurological deficits considered during the unit. Principles will be based on the Bobath concept, Carr and Shepherd’s Motor Relearning approach and the application of anatomical and physiological knowledge. The students will consider neurological impairment in different age groups and also consider the role of the physiotherapist in restorative, supportive and palliative care.A range of outcome measures relevant to patients with complex neurological deficits will be evaluated to establish their utility, reliability and validity.
15 LEARNING & TEACHING ACTIVITIES
Makes extensive use of student centred learning strategies with tutors creating both a challenging and supportive environment using a variety of delivery methods in conjunction with both indicative reading and material accessed by the students themselves. A variety of strategies are used including theatre events, practical demonstrations, group work/role play, skills sessions and tutorials.

Practice EducationTutors will be drawn from both academic and clinical backgrounds.The teaching and learning will be case based and use a problem solving approach. Greater complexity of the patient scenarios will promote clinical reasoning skills.
16 ASSESSMENT STRATEGIES
Workshops with self/peer and tutor evaluation and feedback LO1-10 - formative)
Oral clinical reasoning examination (50% of unit mark – summative) practical skills examination (video analysis/skills) 30 minutes (50% of unit mark LO1-10 –summative)
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate: An ability to use their knowledge of the neuromuscular
control of normal movement and the structure and function of the nervous system to explain the clinical features and management of patients with more complex neurological deficits.
An ability to select, plan, justify and evaluate the most appropriate assessment, physiotherapy management and range of rehabilitation approaches for a described patient including involvement of the multidisciplinary team.
An ability to demonstrate a range of safe, appropriate, accurate and effective assessment skills, physiotherapy management skills and rehabilitation approaches for a described patient.
An ability to demonstrate holistic and patient focused care.
An ability to practice within the Rules of Professional Conduct of the Chartered Society of Physiotherapy/Standards of conduct, performance and Ethics of the Health Professions Council.
An ability to communicate appropriately, clearly and coherently with models and examiners.
An ability to construct and support arguments.Formative assessment procedures will be assessed by peer assessment linked to the unit/session learning outcomes with personal tutor support/academic action planning.Summative assessment procedures will be assessed through generic level 5 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
18 INDICATIVE STUDENT LEARNING RESOURCES
Burnett, M. G., Zager, E. L. (2004), ‘Pathophysiology of peripheral nerve injury: a brief review.’ Neurosurg focus, vol. 16, no. 5, pp. 1-7 [online]. http://www.aans.org/education/journal/neurosurgical/may04/16-5-1.pdf
Edwards, S (2002) Neurological physiotherapy 2nd edn London: Churchill Livingstone
Greenberg, D. A., Aminoff, M. J., and Simon, R. P. (2009), Clinical Neurology, 7th edn, McGraw-Hill

Practice EducationHarvey, L. (2008) Management of spinal cord injuries: a guide for physiotherapists. London: Churchill Livingstone
Intercollegiate Working Party (2008), The National Clinical Guidelines on Stroke 3rd ed. London: Royal College of Physicians [online] http://www.rcplondon.ac.uk/pubs/contents/6ad05aab-8400-494c-8cf4-9772d1d5301b.pdf
Langhammer, B. and Stranhelle, J. K. (2000). Bobath or Motor Relearning Programme. ‘A comparison of two different approaches of physiotherapy in stroke rehabilitation: a randomised controlled. Clinical Rehabilitation, 14 (4) 361-369]
Lennon, S and Stokes, M. (2008) Pocketbook of Neurological Physiotherapy. Edinburgh: Churchill Livingstone
Michael-Titus, A., Revest, P., Shortland, P. (2007) The nervous system: Basic science and clinical conditions Edinburgh: Churchill-Livingstone
Pollock, A., Baer, G., Pomeroy, V. and Langhorne, P. Physiotherapy treatment approaches for the recovery of postural control and lower limb function following stroke. Cochrane Database of Systematic Reviews 2007, Issue 1. Art. No.: CD001920. DOI: 10.1002/14651858.CD001920.pub2.
Price C. I. M., Pandyan, A. D. Electrical stimulation for preventing and treating post-stroke shoulder pain. Cochrane Database of Systematic Reviews 2000, Issue 4. Art. No.: CD001698. DOI: 10.1002/14651858.CD001698.
Saunders, D. H., Greig, C. A., Young, A. and Mead, G. E. Physical fitness training for stroke patients. Cochrane Database of Systematic Reviews 2004, Issue 1. Art. No.: CD003316. DOI: 10.1002/14651858.CD003316.pub2
Shumway Cook, A. and Woollacott, M. (2007) Motor control: translating research into clinical practice 3rd edn Philadelphia: Lippincott, Williams and Wilkins
Stokes, M. (2004), Neurological physiotherapy 2nd edn. London, Mosby
Teasell, R. (2003), Stroke recovery and rehabilitation, Stroke, vol. 34, pp. 365-366.
Trew, M. and Everett, T. (eds) (2005) Human Movement. An Introductory Text. 5th ed. Edinburgh: Churchill Livingstone.
World Health Organization (2001), International classification of functioning, disability and health World Health Organization, Geneva.
19 ANY ADDITIONAL NOTES AND COMMENTS
The content of this unit will support learning at level 5 and 6. The topics studied here will complement the content of parallel units and will be reinforced in other units throughout the

Practice Educationprogramme.It is a professional body requirement that students will not be entitled to receive condoned passes for assessment that include practical skills. Both elements of assessment must be passed with a mark ≥40. The unit must be passed with a mark ≥40
20 DATE OF APPROVAL
11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:
Practice Education
1 UNIT TITLE Practice Placement 1
2 BRIEF SUMMARY This practice placement is undertaken during the second year of the programme. Students will be allocated to a practice placement educator who will provide them with opportunities to apply knowledge and skills learned on campus to manage the needs of patients. Placements will occur in a variety of clinical settings to develop and consolidate the core skills of physiotherapy and professional skills to prepare them for employment.
3 UNIT CODE NUMBER 28151012
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Joanne Nicholson / Sophie Taylor
8 CREDIT VALUE 20 CREDITS AT LEVEL:
5 (I)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
200190 hours of clinical practice
10 hours directed/self-directed study and assessment preparation including tutorial support from visiting academic tutor.
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES All level 4 unitsPractice Placement 0Physiotherapy Management: MSK 2Physiotherapy Management: Cardiorespiratory 2Physiotherapy Management: Neurology 2
12 CO-REQUISITES None
13 UNIT LEARNING OUTCOMES
There are 18 learning outcomes, which are divided into 5 categories:Interpersonal skillsThe student will
1. Demonstrate effective and appropriate skills in communication in order to collaborate and work effectively in partnership with others (professionals, support staff, patients/clients, carers, relatives and external agencies) to the benefit of the client/patient and maximise health outcomes.
2. Contribute effectively to work undertaken as part of a team.

Practice Education3. Recognise the scope of practice of other
professionals.4. Acknowledge cross professional boundaries.5. Make appropriate referrals to others.
Management of patientThe student will
6. Demonstrate effective self management of workload.7. Know the limits of their own practice and when to
seek advice.8. Independently manage their own learning.
Management of patientThe student will
9. Gather appropriate information relating to the patient.10. Plan and carry out an appropriate objective
examination.11. Analyse examination findings and formulate a written
treatment plan in partnership with the patient.12. Implement and critically evaluate the impact of, or
response to treatment interventions.DocumentationThe student will
13. Maintain accurate patient recordsProfessional PracticeThe student will
1. Promote patient centred care2. Comply with the CSP Rules of Professional Conduct
and/or Standards of Conduct, Performance and Ethics
3. Practice in line with relevant health and safety policy4. Work independently and as part of a team as
appropriate.5. Reflect on and analyse clinical experience to
facilitate continuous professional development (CPD).
a. Knowledge and critical understanding of the value of reflection in continuing professional development.
b. Describe and appraise a clinical experience and use this appraisal to propose solutions to problems in clinical practice.
14 CURRICULUM OUTLINE
The student will be able to achieve the learning outcomes by taking responsibility for all aspects of the assessment/treatment and evaluation of treatment for a caseload of patients with guidance/support from a practice placement educator. The placements will take place in a wide variety of clinical specialities in a wide variety of clinical locations in order to ensure that the student is able to demonstrate achievement of competence in core skills of physiotherapy by the end of

Practice Educationthe programme.The student will be provided with opportunities to apply and relate theory to practice. They will be facilitated to evaluate the appropriateness of different approaches to solve uncomplicated problems.
15 LEARNING & TEACHING ACTIVITIES
Assessment and treatment of patients under the supervision of an individual who is registered as a physiotherapist with the Health Professions Council
Experiential learning with reflective practice in the clinical setting
Use of a learning development plan/contract Self directed study Self evaluation at mid-way and end of placement Peer learning Clinical staff development./in service training
sessions Attendance at team meetings/case conference. Workshops Tutorials Lectures
Learning will take place at a variety of clinical settings.
16 ASSESSMENT STRATEGIES
This unit will be assessed by a combination of placement performance (graded by practice placement staff, 75% of unit mark LO1-17 summative) and pieces of reflective writing (graded by academic staff, 25% of unit mark LO18a + b summative). Reflective log/diary (practice education record) (formative)Self/practice placement educator assessment at mid-placement using common assessment tool (formative)All clinical educators will be provided with level 5 (I) practice placement assessment documentation which includes performance/marking criteria (common assessment tool). This documentation will be used for placements 1, 2 and 3 only.The student’s performance for LO1-17 will be judged against these criteria which were generated in collaboration with other HEIs who provide qualifying programmes in physiotherapy in the region. These have been determined to be appropriate for the level.
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
Assignment specific criteria for the reflective writing component (LO18a + b – Summative, 25% of unit mark).
Specific assessment criteria for level 4 practice placement element (LO1-17 using common assessment tool –Summative 75%).
Failure to achieve the standard required for LO16 and 17 will constitute a fail overall
18 INDICATIVE STUDENT LEARNING RESOURCES
Chartered Society of Physiotherapy. (2002) Rules of professional conduct. 2nd ed. London: Chartered Society of Physiotherapy. [Online] [Accessed on 27 April 2009] http://www.csp.org.uk/uploads/documents/csp_rules_conduc

Practice Educationt.pdf
Chartered Society of Physiotherapy (2005) Core standards of Physiotherapy Practice. London: Chartered Society of Physiotherapy
Health Professions Council (2010), Guidance on conduct and ethics for students. London: Health Professions Council.
Health Professions Council. (2008) Standards of conduct, performance and ethics. London: Health Professions Council. [Online] [Accessed on 22 May 2009] http://www.hpc-uk.org/assets/documents/10002367FINALcopyofSCPEJuly2008.pdf
Moon, J. A. (2004) A handbook of reflective and experiential learning: theory and practice. London: Taylor and Francis.
19 ANY ADDITIONAL NOTES AND COMMENTS
Students who achieve an aggregate mark for this unit that is <40 are not entitled to a condoned pass.
The practice placement element of assessment must be passed with a mark ≥40. Students achieving a mark<40 for this element will be entitled to one reassessment attempt only.
Students achieving a mark for the reflective writing element of assessment in the marginal fail band (35 – 39) shall be entitled to receive a condoned pass for this element of assessment at the discretion of the Board of Examiners. Students achieving a mark of <35 will be entitled to one reassessment attempt only.
Students who are required to undertake reassessment and do not satisfactory achieve a unit mark ≥ 40 by achieving the conditions stated above after a first reassessment opportunity will not match the requirements for progression to the third year of the programme and will be withdrawn.
Subject to satisfactory completion the practice placement hours accrued will contribute toward the 1,000 hours of practice placement required by the Chartered Society of Physiotherapy in order to become eligible for membership.
Students are required to have satisfactorily completed occupational health assessment and enhanced CRB check prior to commencing this unit.
NOTE: failure to achieve the standard required for LO16 and 17 will constitute a fail overall
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST
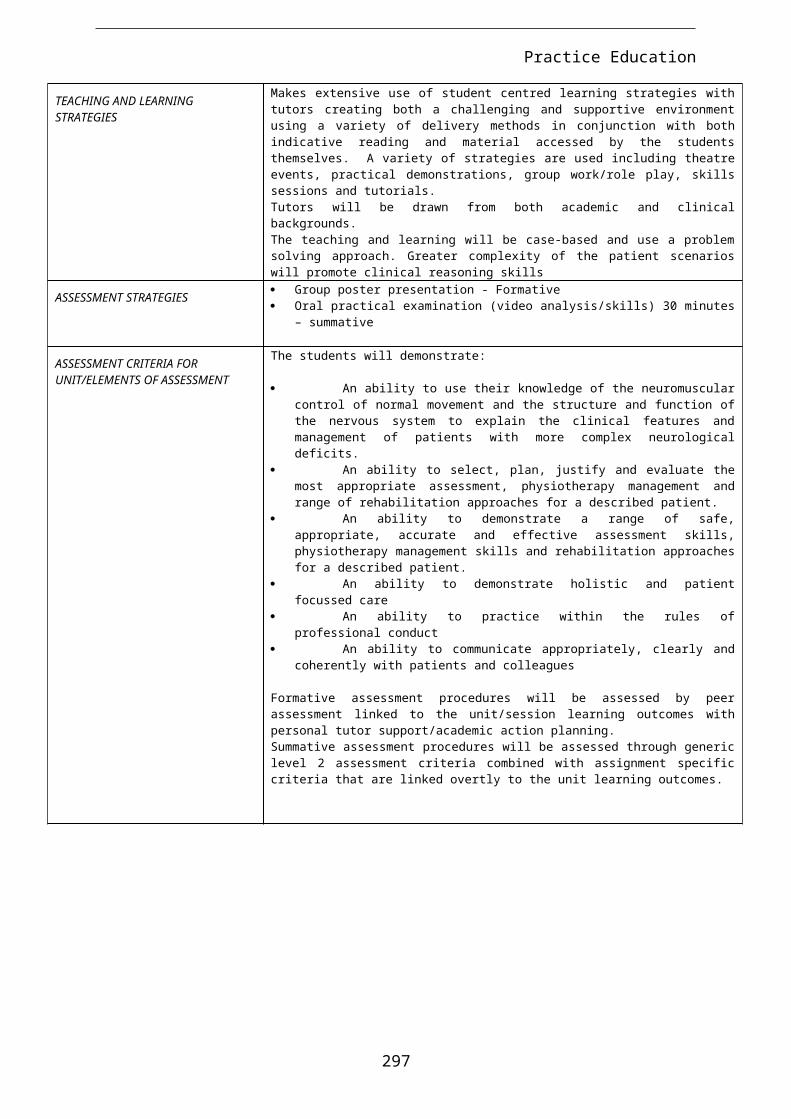
Practice Education
RECENT CONSIDERATION:
1 UNIT TITLE Practice Placement 2
2 BRIEF SUMMARY This practice placement is undertaken during the second year of the programme. Students will be allocated to a practice placement educator who will provide them with opportunities to apply knowledge and skills learned on campus to manage the needs of patients. Placements will occur in a variety of clinical settings to develop and consolidate the core skills of physiotherapy and professional skills to prepare them for employment.
3 UNIT CODE NUMBER 28151013
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Joanne Nicholson / Sophie Taylor
8 CREDIT VALUE 20 CREDITS AT LEVEL:
5 (I)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
200190 hours of clinical practice
10 hours directed/self-directed study and assessment preparation including tutorial support from visiting academic tutor
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES All level 4 unitsPractice Placement 0Physiotherapy Management: MSK 2Physiotherapy Management: Cardiorespiratory 2Physiotherapy Management: Neurology 2
12 CO-REQUISITES None
13 UNIT LEARNING OUTCOMES
There are 18 learning outcomes, which are divided into 5 categories:Interpersonal skillsThe student will
1. Demonstrate effective and appropriate skills in communication in order to collaborate and work effectively in partnership with others (professionals, support staff, patients/clients, carers, relatives and external agencies) to the benefit of the client/patient

Practice Educationand maximise health outcomes.
2. Contribute effectively to work undertaken as part of a team.
3. Recognise the scope of practice of other professionals.
4. Acknowledge cross professional boundaries.5. Make appropriate referrals to others.
Management of patientThe student will
6. Demonstrate effective self management of workload.7. Know the limits of their own practice and when to
seek advice.8. Independently manage their own learning.
Management of patientThe student will
9. Gather appropriate information relating to the patient.10. Plan and carry out an appropriate objective
examination.11. Analyse examination findings and formulate a written
treatment plan in partnership with the patient.12. Implement and critically evaluate the impact of, or
response to treatment interventions.DocumentationThe student will
13. Maintain accurate patient recordsProfessional PracticeThe student will
14. Promote patient centred care15. Comply with the CSP Rules of Professional Conduct
and/or Standards of Conduct, Performance and Ethics
16. Practice in line with relevant health and safety policy17. Work independently and as part of a team as
appropriate.18. Reflect on and analyse clinical experience to
facilitate continuous professional development (CPD).
a. Knowledge and critical understanding of the value of reflection in continuing professional development.
b. Describe and appraise a clinical experience and use this appraisal to propose solutions to problems in clinical practice.
14 CURRICULUM OUTLINE
The student will be able to achieve the learning outcomes by taking responsibility for all aspects of the assessment/treatment and evaluation of treatment for a caseload of patients with guidance/support from a practice placement educator. The placements will take place in a wide variety of clinical

Practice Educationspecialities in a wide variety of clinical locations in order to ensure that the student is able to demonstrate achievement of competence in core skills of physiotherapy by the end of the programme.The student will be provided with opportunities to apply and relate theory to practice. They will be facilitated to evaluate the appropriateness of different approaches to solve uncomplicated problems.
15 LEARNING & TEACHING ACTIVITIES
Assessment and treatment of patients under the supervision of an individual who is registered as a physiotherapist with the Health Professions Council
Experiential learning with reflective practice in the clinical setting
Use of a learning development plan/contract Self directed study Self evaluation at mid-way and end of placement Peer learning Clinical staff development./in service training
sessions Attendance at team meetings/case conference. Workshops Tutorials Lectures
Learning will take place at a variety of clinical settings.
16 ASSESSMENT STRATEGIES
This unit will be assessed by a combination of placement performance (graded by practice placement staff, 75% of unit mark LO1-17 summative) and pieces of reflective writing (graded by academic staff, 25% of unit mark LO18a + b summative). Reflective log/diary (practice education record) (formative)Self/practice placement educator assessment at mid-placement using common assessment tool (formative)All clinical educators will be provided with level 5 (I) practice placement assessment documentation which includes performance/marking criteria (common assessment tool). This documentation will be used for placements 1, 2 and 3 only.The student’s performance for LO1-17 will be judged against these criteria which were generated in collaboration with other HEIs who provide qualifying programmes in physiotherapy in the region. These have been determined to be appropriate for the level.
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
Assignment specific criteria for the reflective writing component (LO18a + b – Summative, 25% of unit mark).
Specific assessment criteria for level 4 practice placement element (LO1-17 using common assessment tool –Summative 75%).
Failure to achieve the standard required for LO16 and 17 will constitute a fail overall

Practice Education
18 INDICATIVE STUDENT LEARNING RESOURCES
Chartered Society of Physiotherapy. (2002) Rules of professional conduct. 2nd ed. London: Chartered Society of Physiotherapy. [Online] [Accessed on 27 April 2009] http://www.csp.org.uk/uploads/documents/csp_rules_conduct.pdf
Chartered Society of Physiotherapy (2005) Core standards of Physiotherapy Practice. London: Chartered Society of Physiotherapy
Health Professions Council (2010), Guidance on conduct and ethics for students. London: Health Professions Council.
Health Professions Council. (2008) Standards of conduct, performance and ethics. London: Health Professions Council. [Online] [Accessed on 22 May 2009] http://www.hpc-uk.org/assets/documents/10002367FINALcopyofSCPEJuly2008.pdf
Moon, J. A. (2004) A handbook of reflective and experiential learning: theory and practice. London: Taylor and Francis.
19 ANY ADDITIONAL NOTES AND COMMENTS
Students who achieve an aggregate mark for this unit that is <40 are not entitled to a condoned pass.
The practice placement element of assessment must be passed with a mark ≥40. Students achieving a mark<40 for this element will be entitled to one reassessment attempt only.
Students achieving a mark for the reflective writing element of assessment in the marginal fail band (35 – 39) shall be entitled to receive a condoned pass for this element of assessment at the discretion of the Board of Examiners. Students achieving a mark of <35 will be entitled to one reassessment attempt only.
Students who are required to undertake reassessment and do not satisfactory achieve a unit mark ≥ 40 by achieving the conditions stated above after a first reassessment opportunity will not match the requirements for progression to the third year of the programme and will be withdrawn.
Subject to satisfactory completion the practice placement hours accrued will contribute toward the 1,000 hours of practice placement required by the Chartered Society of Physiotherapy in order to become eligible for membership.
Students are required to have satisfactorily completed occupational health assessment and enhanced CRB check prior to commencing this unit.
NOTE: failure to achieve the standard required for LO16 and 17 will constitute a fail overall

Practice Education
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:
1 UNIT TITLE Practice Placement 3
2 BRIEF SUMMARY This practice placement is undertaken during the second year of the programme. Students will be allocated to a practice placement educator who will provide them with opportunities to apply knowledge and skills learned on campus to manage the needs of patients. Placements will occur in a variety of clinical settings to develop and consolidate the core skills of physiotherapy and professional skills to prepare them for employment.
3 UNIT CODE NUMBER 28151014
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Joanne Nicholson / Sophie Taylor
8 CREDIT VALUE 20 CREDITS AT LEVEL:
5 (I)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
200190 hours of clinical practice
10 hours directed/self-directed study and assessment preparation including tutorial support from visiting academic tutor
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES All level 4 unitsPractice Placement 0Physiotherapy Management: MSK 2Physiotherapy Management: Cardiorespiratory 2Physiotherapy Management: Neurology 2
12 CO-REQUISITES None
13 UNIT LEARNING OUTCOMES
There are 18 learning outcomes, which are divided into 5 categories:Interpersonal skillsThe student will
1. Demonstrate effective and appropriate skills in

Practice Educationcommunication in order to collaborate and work effectively in partnership with others (professionals, support staff, patients/clients, carers, relatives and external agencies) to the benefit of the client/patient and maximise health outcomes.
2. Contribute effectively to work undertaken as part of a team.
3. Recognise the scope of practice of other professionals.
4. Acknowledge cross professional boundaries.5. Make appropriate referrals to others.
Management of patientThe student will
6. Demonstrate effective self management of workload.
7. Know the limits of their own practice and when to seek advice.
8. Independently manage their own learning.Management of patientThe student will
9. Gather appropriate information relating to the patient.
10. Plan and carry out an appropriate objective examination.
11. Analyse examination findings and formulate a written treatment plan in partnership with the patient.
12. Implement and critically evaluate the impact of, or response to treatment interventions.
DocumentationThe student will
13. Maintain accurate patient recordsProfessional PracticeThe student will
14. Promote patient centred care15. Comply with the CSP Rules of Professional
Conduct and/or Standards of Conduct, Performance and Ethics
16. Practice in line with relevant health and safety policy
17. Work independently and as part of a team as appropriate.
18. Reflect on and analyse clinical experience to facilitate continuous professional development (CPD).
a. Knowledge and critical understanding of the value of reflection in continuing professional development.
b. Describe and appraise a clinical

Practice Educationexperience and use this appraisal to propose solutions to problems in clinical practice.
14 CURRICULUM OUTLINE
The student will be able to achieve the learning outcomes by taking responsibility for all aspects of the assessment/treatment and evaluation of treatment for a caseload of patients with guidance/support from a practice placement educator. The placements will take place in a wide variety of clinical specialities in a wide variety of clinical locations in order to ensure that the student is able to demonstrate achievement of competence in core skills of physiotherapy by the end of the programme.The student will be provided with opportunities to apply and relate theory to practice. They will be facilitated to evaluate the appropriateness of different approaches to solve uncomplicated problems.
15 LEARNING & TEACHING ACTIVITIES
Assessment and treatment of patients under the supervision of an individual who is registered as a physiotherapist with the Health Professions Council
Experiential learning with reflective practice in the clinical setting
Use of a learning development plan/contract Self directed study Self evaluation at mid-way and end of placement Peer learning Clinical staff development./in service training
sessions Attendance at team meetings/case conference. Workshops Tutorials Lectures
Learning will take place at a variety of clinical settings.
16 ASSESSMENT STRATEGIES
This unit will be assessed by a combination of placement performance (graded by practice placement staff, 75% of unit mark LO1-17 summative) and pieces of reflective writing (graded by academic staff, 25% of unit mark LO18a + b summative). Reflective log/diary (practice education record) (formative)Self/practice placement educator assessment at mid-placement using common assessment tool (formative)All clinical educators will be provided with level 5 (I) practice placement assessment documentation which includes performance/marking criteria (common assessment tool). This documentation will be used for placements 1, 2 and 3 only.The student’s performance for LO1-17 will be judged against these criteria which were generated in collaboration with other HEIs who provide qualifying programmes in physiotherapy in the region. These have

Practice Educationbeen determined to be appropriate for the level.
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
Assignment specific criteria for the reflective writing component (LO18a + b – Summative, 25% of unit mark).
Specific assessment criteria for level 4 practice placement element (LO1-17 using common assessment tool –Summative 75%).
Failure to achieve the standard required for LO16 and 17 will constitute a fail overall
18 INDICATIVE STUDENT LEARNING RESOURCES
Chartered Society of Physiotherapy. (2002) Rules of professional conduct. 2nd ed. London: Chartered Society of Physiotherapy. [Online] [Accessed on 27 April 2009] http://www.csp.org.uk/uploads/documents/csp_rules_conduct.pdf
Chartered Society of Physiotherapy (2005) Core standards of Physiotherapy Practice. London: Chartered Society of Physiotherapy
Health Professions Council (2010), Guidance on conduct and ethics for students. London: Health Professions Council.
Health Professions Council. (2008) Standards of conduct, performance and ethics. London: Health Professions Council. [Online] [Accessed on 22 May 2009] http://www.hpc-uk.org/assets/documents/10002367FINALcopyofSCPEJuly2008.pdf
Moon, J. A. (2004) A handbook of reflective and experiential learning: theory and practice. London: Taylor and Francis.
19 ANY ADDITIONAL NOTES AND COMMENTS
Students who achieve an aggregate mark for this unit that is <40 are not entitled to a condoned pass.
The practice placement element of assessment must be passed with a mark ≥40. Students achieving a mark<40 for this element will be entitled to one reassessment attempt only.
Students achieving a mark for the reflective writing element of assessment in the marginal fail band (35 – 39) shall be entitled to receive a condoned pass for this element of assessment at the discretion of the Board of Examiners. Students achieving a mark of <35 will be entitled to one reassessment attempt only.
Students who are required to undertake reassessment and do not satisfactory achieve a unit mark ≥ 40 by achieving the conditions stated above after a first reassessment opportunity will

Practice Education
not match the requirements for progression to the third year of the programme and will be withdrawn.
Subject to satisfactory completion the practice placement hours accrued will contribute toward the 1,000 hours of practice placement required by the Chartered Society of Physiotherapy in order to become eligible for membership.
Students are required to have satisfactorily completed occupational health assessment and enhanced CRB check prior to commencing this unit.
NOTE: failure to achieve the standard required for LO16 and 17 will constitute a fail overall
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Reflective Practice and Clinical Reasoning
2 BRIEF SUMMARY
This unit is intended to allow the student to enhance skills of reflective practice and clinical reasoning by using different methods of reflection and varied reasoning strategies.
3 UNIT CODE NUMBER
28151015
4 HOME PROGRAMME
BSc (Hons) Physiotherapy
5 HOME DEPARTMENT
Health Professions
6 SUBJECT AREA
B160: physiotherapy
7 UNIT LEADER(S)
Lesley McLoughlin / Janet Morrison
8 CREDIT VALUE
10 CREDITS AT LEVEL:
6(H)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
10020 hours of classroom contact
80 hours of directed/self-directed study and assessment preparation.
10
UNIT STATUS
Mandatory core
11
PRE-REQUISITES
All level 4(C)Practice Placement 0All level 5 (I) units
12
CO-REQUISITES
None
13
UNIT LEARNING OUTCOMES
On successful completion of this unit students will have attained or be able to demonstrate:Cognitive/intellectual skills
1. Critically reflect upon previous individual experiences of practice placement using a variety of methods.
2. Demonstrate the ability to use clinical reasoning and evidence based practice to justify all decision making in practice.
3. Critically appraise the relevance of professional,
Practice Educationstatutory and government requirements on their practice.
Key transferable skills4. Use reflection to prioritise their learning needs in
order to support their professional development.5. Interact effectively within a group and work with
peers towards a common goal.
14
CURRICULUM OUTLINE
This unit is intended to enable the student to: Continue to develop skills of both informal and formal
reflective practice. Use different methods of reflection and how these may
inform practice. Use reflection and clinical reasoning in order to make
informed judgements, decisions and prioritise actions taken.
Recognise the significance and implications of professional, statutory and government requirements on practice
15
LEARNING & TEACHING ACTIVITIES
Makes use of student centred learning strategies with tutors and creating a challenging, supportive environment. A variety of teaching strategies will be used including group work, tutorials, peer supported presentations and lectures.
16
ASSESSMENT STRATEGIES
Self/peer appraisal of professional development and peer/staff assessment of reflective and clinical reasoning skills LO1-5 - Formative).
Group case poster presentation (LO1- 5 – 100% Summative).
17
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will demonstrate: An ability to work effectively within a group of peers to
develop, produce and present a poster. An ability to use/discuss the relevance of different
models of reflection in reflecting on their practice and developing their future practice.
The use of clinical reasoning and evidence based practice in order to justify their practice.
Ability to present information in an appropriately constructed poster.
Access and critically evaluate appropriate evidence and select and justify its inclusion in the poster.
Discuss and answer questions related to the poster content and evidence used with reference to the unit content.
Formative assessment – self and peer evaluation of professional development with regard to reflective practice and clinical reasoning skills, followed by discussion with personal tutor and / or visiting tutor and clinical educator to facilitate further development both in practice and academically.Summative assessment procedures will be assessed through generic level 6 assessment criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
1 INDICATIVE Bolton, G. E. J. (2010) Reflective practice: writing and

Practice Education
8 STUDENT LEARNING RESOURCES
professional development. 3rd ed. London: Sage Publications Ltd.
Chartered Society of Physiotherapy. (2001) Developing a portfolio. A guide for CSP members. London: Chartered Society of Physiotherapy.
Chartered Society of Physiotherapy. (2002) Rules of professional conduct. 2nd ed. London: Chartered Society of Physiotherapy. [Online] [Accessed on 27 April 2009] http://www.csp.org.uk/uploads/documents/csp_rules_conduct.pdf
Chartered Society of Physiotherapy (2005) Core standards of physiotherapy practice. 2nd ed. London: Chartered Society of Physiotherapy. [Online] [Accessed on 27 April 2009] http://www.csp.org.uk/uploads/documents/csp_core_standards_2005.pdf
Fook, J. and Gardiner, F. (2007) Practising critical reflection. A resource handbook. Berkshire: Open University Press.
Health Professions Council. (2007) Standards of proficiency. London: Health Professions Council. [Online] [Accessed on 27 April 2009] http://www.hpc-uk.org/assets/documents/10000DBCStandards_of_Proficiency_Physiotherapists.pdf
Higgs, J. and Jones, M.A. (2008) Clinical reasoning in the health professions. 3rd ed. Oxford: Butterworth Heineman.
Manchester Metropolitan University. (2008) Clinical reasoning guidelines - Physiotherapy management 2.
Moon, J. A. (2004) A handbook of reflective and experiential learning: theory and practice. London: Taylor and Francis.
Redmond, B. (2006) Reflection in action. Developing reflective practice in health and social services. Aldershot: Ashgate Publishing Ltd.
Further resources
Chartered Society of Physiotherapy. (2008) PebblePAD: e-portfolio system. [Online] [Accessed on 27 April 2009) http://eportfolio.csp.org.uk/
Clinical educators
Level 4 practice placements
Level 5 practice placements
Personal and professional development plans
Study guides from specific placements
19
ANY ADDITIONAL
This unit is split – part of it will be delivered in between Practice Placement 3 and Practice placement 4 – this element of the
Practice Education
NOTES AND COMMENTS
unit is intended to enable students to make the transition from level 5 to level 6 practice.
The second half of the unit is delivered after Practice Placement 5 and complements the Transition to Professional Practice unit.
20
DATE OF APPROVAL
11 & 12 February 2010
21
DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Critical Thinking and Enquiry ‘A’
2 BRIEF SUMMARY
The unit will have a focus on the physiotherapist as a consumer of research to enhance service provision. Students will have opportunity to access and appraise contemporary literature to make reasoned judgements in terms of quality of published material. Students will consider processes to facilitate the application of new knowledge to enhance contemporary physiotherapy practice.
3 UNIT CODE NUMBER
28151016
4 HOME PROGRAMME
BSc (Hons) Physiotherapy
5 HOME DEPARTMENT
Health Professions
6 SUBJECT AREA
B160: physiotherapy
7 UNIT LEADER(S)
Francis Fatoye
8 CREDIT VALUE
10 CREDITS AT LEVEL:
6(H)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
10020 hours of classroom contact
80 hours of directed/self-directed study and assessment preparation
10
UNIT STATUS Mandatory Core
11
PRE-REQUISITES
All level 4(C)Practice Placement 0All level 5 (I) units
12
CO-REQUISITES
None
13
UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to, have attained or demonstrated an ability to:Cognitive and intellectual skills
1. generate comprehensive and discriminating strategies for searching the professional literature
2. develop and employ a systematic and reasoned approach to the selection of material for inclusion in a review of contemporary practice

Practice Education3. use a systematic and reasoned approach to the
appraisal of research material4. make reasoned judgements about the quality of
published material that are supported by use of other literature
5. make reasoned judgements about the impact of the findings of research/audit on physiotherapy practice
6. propose the role of the individual in facilitating service development secondary to research/audit findings to enhance physiotherapy practice
14
CURRICULUM OUTLINE
Build on achievement at level 4 and 5 to further develop skills in
Critical thinking Literature searching Appraising the quality of evidence Developing and supporting logical and reasoned
argument Academic writing Learning needs analysis Portfolio building
15
LEARNING & TEACHING ACTIVITIES
Makes use of student centred learning strategies with tutors and creating a challenging, supportive environment. Includes small group work, project work, purposeful interaction with online resources (databases) with tutor support, lectures, seminars/presentations.
16
ASSESSMENT STRATEGIES
Group presentation with peer evaluation (LO1-6 – Formative).
Peer/self appraisal (LO1-2 - Formative) Essay based assignment – critical appraisal and
evidence based practice (6 sides A4 double spaced) (LO1-6 – 100% Summative).
Will be assessed through generic criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
17
ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
Students will demonstrate the ability to: generate a rational, reproducible search strategy employ methods for selecting appropriate material for a
review of physiotherapy practice select and apply a purposeful, reasoned and systematic
approach to the critical appraisal of professional literature
Use the outcome of critical review to structure and support argument relating to the value/relevance of the findings of research/audit
Propose how research/audit findings should impact on clinical practice
18
INDICATIVE STUDENT LEARNING RESOURCES
Chartered Society of Physiotherapy (2005a), Core standards of physiotherapy practice London: Chartered Society of Physiotherapy.
Chartered Society of Physiotherapy (2005b) Internet Resources (1): Using the Internet, London: Chartered Society of Physiotherapy. [Online]

Practice Education<http://www.csp.org.uk/uploads/documents/csp_lis06_internet1.pdf
Chartered Society of Physiotherapy (2005c) Internet Resources (2): Finding published information, London, Chartered Society of Physiotherapy [Online] http://www.csp.org.uk/uploads/documents/csp_lis07_internet.pdf
Chartered Society of Physiotherapy (2005d) Internet resources (3): Assessing the quality of information and putting it into practice London: Chartered Society of Physiotherapy. [Online] http://www.csp.org.uk/uploads/documents/csp_lis08_internet.pdf
Chartered Society of Physiotherapy (2009) CSP guide to literature searching. London: Chartered Society of Physiotherapy [Online] http://www.csp.org.uk/uploads/documents/Literature_searching_PD051.pdf
Chartered Society of Physiotherapy and College of Occupational Therapy (2001) Audit pack: guideline for the collaborative, rehabilitative management of elderly people who have fallen. London: Chartered Society of Physiotherapy [Online] http://www.csp.org.uk/uploads/documents/csp_falls_audit2.pdf
Crombie, I. K. (1996), The pocket guide to critical appraisal: a handbook for health care professionals London: BMJ Publishing.
Health Professions Council (2007), Standards of proficiency: physiotherapists London: Health Professions Council.
Hicks, C. (2009), Research methods for clinical therapists: applied project design and analysis, 5th edn, Edinburgh: Churchill Livingstone.
Higgins, J. P. T. and Green, S. (2006). Cochrane Handbook for Systematic Reviews of Interventions 4.2.6. [Online]. The Cochrane Library. Issue 3 [Online] http://www.cochrane.org/resources/handbook/Handbook4.2.6Sep2006.pdf
Maxwell, J. (2005), Qualitative research design: an interactive approach London: Sage.
Mays, N. and Pope, C. (2000), Qualitative research in health care: assessing quality in qualitative research, British Medical Journal, 320 pp. 50-52.
McPherson, K. and Lord, S. (2000), Clinician's guide to research Part 2: matching the method to the question, New Zealand Journal of Physiotherapy, 28 (2), pp. 20-29
Public Health Resource Unit (2007) CASP: critical appraisal skills programme [Online]

Practice Educationhttp://www.phru.nhs.uk/Pages/PHD/CASP.htm
Wyatt, J. and Guly, H. (2002) Identifying the research question and planning the project. Emerg. Med. J. vol. 19, pp. 318-321
19
ANY ADDITIONAL NOTES AND COMMENTS
20
DATE OF APPROVAL
11 & 12 February 2010
21
DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Practice Placement 4
2 BRIEF SUMMARY This practice placement is undertaken during the third year of the programme. Students will be allocated to a practice placement educator who will provide them with opportunities to apply knowledge and skills learned on campus to manage the needs of patients. There is an expectation that students will demonstrate greater autonomy in their clinical practice during placements at level 6. There is an expectation that students will have the capacity to manage patients with increasing complexity and be able to respond to situations that are not predictable. Placements will occur in a variety of clinical settings to develop and consolidate the core skills of physiotherapy and professional skills to prepare them for employment.
3 UNIT CODE NUMBER 28151017
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Joanne Nicholson / Sophie Taylor
8 CREDIT VALUE 20 CREDITS AT LEVEL:
6 (H)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
200190 hours of clinical practice
10 hours directed/self-directed study and assessment preparation including tutorial support from visiting academic tutor
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES All level 4(C)Practice Placement 0All level 5 (I) units
12 CO-REQUISITES None
13 UNIT LEARNING OUTCOMES
There are 18 learning outcomes, which are divided into 5 categories:Interpersonal skillsThe student will
1. Demonstrate effective and appropriate skills in communication in order to collaborate and work effectively in partnership with others (professionals, support staff, patients/clients, carers, relatives and external agencies) to the benefit of the client/patient

Practice Educationand maximise health outcomes.
2. Contribute effectively to work undertaken as part of a team.
3. Recognise the scope of practice of other professionals.
4. Acknowledge cross professional boundaries.5. Make appropriate referrals to others.
Management of patientThe student will
6. Demonstrate effective self management of workload.7. Know the limits of their own practice and when to
seek advice.8. Independently manage their own learning.
Management of patientThe student will
9. Gather appropriate information relating to the patient.10. Plan and carry out an appropriate objective
examination.11. Analyse examination findings and formulate a written
treatment plan in partnership with the patient.12. Implement and critically evaluate the impact of, or
response to treatment interventions.DocumentationThe student will
13. Maintain accurate patient recordsProfessional PracticeThe student will
14. Promote patient centred care15. Comply with the CSP Rules of Professional
Conduct/Standards of Conduct, Performance and Ethics
16. Practice in line with relevant health and safety policy17.Work independently and as part of a team as
appropriate.18. Reflect on and analyse clinical experience to
facilitate continuous professional development (CPD).
a. Systematic understanding and critical awareness of the value of reflection in continuing professional development
b. Describe and appraise a clinical experience and use this appraisal to formulate and defend solutions to problems in clinical practice.
14 CURRICULUM OUTLINE
The student will be able to achieve the learning outcomes by taking responsibility for all aspects of the physiotherapy management of a mixed caseload with supervision from a practice placement educator. The caseload may include complex patient conditions that do not respond in a

Practice Educationpredictable wayThe student will have opportunity to relate theory to practice and will be able to generate multiple competing hypotheses to explain patient’s presenting signs and symptoms and systematically exclude those which do not apply to reach sound judgements. They will have opportunity to develop and apply an understanding of a complex body of knowledge and be able to apply problem solving skills to more complex situations and unpredictable circumstances.They will have opportunity to consolidate skills in the evaluation of evidence, the development and supporting of arguments in the context of clinical decision making and will be encouraged to question assumptions to reach sound decisions.
15 LEARNING & TEACHING ACTIVITIES
Assessment and treatment of patients under the supervision of an individual who is registered as a physiotherapist with the Health Professions Council
Experiential learning with reflective practice in the clinical setting
Use of a learning development plan/contract Self directed study Self evaluation at mid-way and end of placement Peer learning Clinical staff development./in service training
sessions Attendance at team meetings/case conference. Workshops Tutorials Lectures
Learning will take place at a variety of clinical settings.
16 ASSESSMENT STRATEGIES
This unit will be assessed by a combination of placement performance (graded by practice placement staff – 75% of unit mark – LO1-17 summative) and pieces of reflective writing (graded by academic staff – 25% of unit mark – LO18 - summative).
Reflective log/diary (practice education record) to promote reflective practice and to allow student self-evaluation of the sufficiency of their personal development portfolio – formative
Self/practice placement educator evaluation at Mid-placement using the common assessment tool as a framework to promote focused dialogue - formative
All clinical educators will be provided with level 6(H) placement assessment documentation that includes performance and marking criteria. This documentation will be used for placements 4 and 5 only.
The student’s performance will be judged against these criteria which were generated in collaboration with other HEIs who provide qualifying programmes in physiotherapy in the region. These have been determined to be appropriate for the level

Practice Education
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
General programme written and practical assessment criteria will apply. Specific assessment criteria for level 6(H) practice placements
Specific assessment criteria will be related to the written assignment.
18 INDICATIVE STUDENT LEARNING RESOURCES
Chartered Society of Physiotherapy. (2002) Rules of professional conduct. 2nd ed. London: Chartered Society of Physiotherapy. [Online] [Accessed on 27 April 2009] http://www.csp.org.uk/uploads/documents/csp_rules_conduct.pdf
Chartered Society of Physiotherapy (2005) Core standards of Physiotherapy Practice. London: Chartered Society of Physiotherapy
Health Professions Council (2010), Guidance on conduct and ethics for students. London: Health Professions Council.
Health Professions Council. (2008) Standards of conduct, performance and ethics. London: Health Professions Council. [Online] [Accessed on 22 May 2009] http://www.hpc-uk.org/assets/documents/10002367FINALcopyofSCPEJuly2008.pdf
Moon, J. A. (2004) A handbook of reflective and experiential learning: theory and practice. London: Taylor and Francis
19 ANY ADDITIONAL NOTES AND COMMENTS
Students who achieve an aggregate mark for this unit that is <40 are not entitled to a condoned pass.
The practice placement element of assessment must be passed with a mark ≥40. Students achieving a mark<40 for this element will be entitled to one reassessment attempt only.
Students achieving a mark for the reflective writing element of assessment in the marginal fail band (35 – 39) shall be entitled to receive a condoned pass for this element of assessment at the discretion of the Board of Examiners. Students achieving a mark of <35 will be entitled to one reassessment attempt only.
Students who are required to undertake reassessment and do not satisfactory achieve a unit mark ≥ 40 by achieving the conditions stated above after a first reassessment opportunity will not match the requirements for the award of BSc (Hons) Physiotherapy and will not be eligible to apply for registration as a physiotherapist with the HPC.
Subject to satisfactory completion the practice placement hours accrued will contribute toward the 1,000 hours of practice placement required by the Chartered Society of Physiotherapy in order to become eligible for membership.
Students are required to have satisfactorily

Practice Educationcompleted occupational health assessment and enhanced CRB check prior to commencing this unit.
NOTE: failure to achieve the standard required for LO16 and 17 will constitute a fail overall
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:
1 UNIT TITLE Practice Placement 5
2 BRIEF SUMMARY This practice placement is undertaken during the third year of the programme. Students will be allocated to a practice placement educator who will provide them with opportunities to apply knowledge and skills learned on campus to manage the needs of patients. There is an expectation that students will demonstrate greater autonomy in their clinical practice during placements at level 6. There is an expectation that students will have the capacity to manage patients with increasing complexity and be able to respond to situations that are not predictable. Placements will occur in a variety of clinical settings to develop and consolidate the core skills of physiotherapy and professional skills to prepare them for employment.
3 UNIT CODE NUMBER 28151018
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Joanne Nicholson / Sophie Taylor
8 CREDIT VALUE 20 CREDITS AT LEVEL:
6 (H)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
200190 hours of clinical practice
10 hours directed/self-directed study and assessment preparation including tutorial support from visiting academic tutor
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES All level 4(C)Practice Placement 0All level 5 (I) units
12 CO-REQUISITES None

Practice Education
13 UNIT LEARNING OUTCOMES
There are 18 learning outcomes, which are divided into 5 categories:Interpersonal skillsThe student will
1. Demonstrate effective and appropriate skills in communication in order to collaborate and work effectively in partnership with others (professionals, support staff, patients/clients, carers, relatives and external agencies) to the benefit of the client/patient and maximise health outcomes.
2. Contribute effectively to work undertaken as part of a team.
3. Recognise the scope of practice of other professionals.
4. Acknowledge cross professional boundaries.5. Make appropriate referrals to others.
Management of patientThe student will
6. Demonstrate effective self management of workload.7. Know the limits of their own practice and when to
seek advice.8. Independently manage their own learning.
Management of patientThe student will
9. Gather appropriate information relating to the patient.10. Plan and carry out an appropriate objective
examination.11. Analyse examination findings and formulate a written
treatment plan in partnership with the patient.12. Implement and critically evaluate the impact of, or
response to treatment interventions.DocumentationThe student will
13. Maintain accurate patient recordsProfessional PracticeThe student will
14. Promote patient centred care15. Comply with the CSP Rules of Professional
Conduct/Standards of Conduct, Performance and Ethics
16. Practice in line with relevant health and safety policy17.Work independently and as part of a team as
appropriate.18. Reflect on and analyse clinical experience to
facilitate continuous professional development (CPD).
a. Systematic understanding and critical awareness of the value of reflection in continuing professional development

Practice Educationb. Describe and appraise a clinical experience
and use this appraisal to formulate and defend solutions to problems in clinical practice.
14 CURRICULUM OUTLINE
The student will be able to achieve the learning outcomes by taking responsibility for all aspects of the physiotherapy management of a mixed caseload with supervision from a practice placement educator. The caseload may include complex patient conditions that do not respond in a predictable wayThe student will have opportunity to relate theory to practice and will be able to generate multiple competing hypotheses to explain patient’s presenting signs and symptoms and systematically exclude those which do not apply to reach sound judgements. They will have opportunity to develop and apply an understanding of a complex body of knowledge and be able to apply problem solving skills to more complex situations and unpredictable circumstances.They will have opportunity to consolidate skills in the evaluation of evidence, the development and supporting of arguments in the context of clinical decision making and will be encouraged to question assumptions to reach sound decisions.
15 LEARNING & TEACHING ACTIVITIES
Assessment and treatment of patients under the supervision of an individual who is registered as a physiotherapist with the Health Professions Council
Experiential learning with reflective practice in the clinical setting
Use of a learning development plan/contract Self directed study Self evaluation at mid-way and end of placement Peer learning Clinical staff development./in service training
sessions Attendance at team meetings/case conference. Workshops Tutorials Lectures
Learning will take place at a variety of clinical settings.
16 ASSESSMENT STRATEGIES
This unit will be assessed by a combination of placement performance (graded by practice placement staff – 75% of unit mark – LO1-17 summative) and pieces of reflective writing (graded by academic staff – 25% of unit mark – LO18 - summative).
Reflective log/diary (practice education record) to promote reflective practice and to allow student self-evaluation of the sufficiency of their personal development portfolio – formative
Self/practice placement educator evaluation at Mid-placement using the common assessment tool as a framework to promote focused dialogue - formative
All clinical educators will be provided with level 6(H)

Practice Educationplacement assessment documentation that includes performance and marking criteria. This documentation will be used for placements 4 and 5 only.
The student’s performance will be judged against these criteria which were generated in collaboration with other HEIs who provide qualifying programmes in physiotherapy in the region. These have been determined to be appropriate for the level
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
General programme written and practical assessment criteria will apply. Specific assessment criteria for level 6(H) practice placements
Specific assessment criteria will be related to the written assignment.
18 INDICATIVE STUDENT LEARNING RESOURCES
Chartered Society of Physiotherapy. (2002) Rules of professional conduct. 2nd ed. London: Chartered Society of Physiotherapy. [Online] [Accessed on 27 April 2009] http://www.csp.org.uk/uploads/documents/csp_rules_conduct.pdf
Chartered Society of Physiotherapy (2005) Core standards of Physiotherapy Practice. London: Chartered Society of Physiotherapy
Health Professions Council (2010), Guidance on conduct and ethics for students. London: Health Professions Council.Health Professions Council. (2008) Standards of conduct, performance and ethics. London: Health Professions Council. [Online] [Accessed on 22 May 2009] http://www.hpc-uk.org/assets/documents/10002367FINALcopyofSCPEJuly2008.pdf
Moon, J. A. (2004) A handbook of reflective and experiential learning: theory and practice. London: Taylor and Francis
19 ANY ADDITIONAL NOTES AND COMMENTS
Students who achieve an aggregate mark for this unit that is <40 are not entitled to a condoned pass.
The practice placement element of assessment must be passed with a mark ≥40. Students achieving a mark<40 for this element will be entitled to one reassessment attempt only.
Students achieving a mark for the reflective writing element of assessment in the marginal fail band (35 – 39) shall be entitled to receive a condoned pass for this element of assessment at the discretion of the Board of Examiners. Students achieving a mark of <35 will be entitled to one reassessment attempt only.
Students who are required to undertake first reassessment and do not satisfactory achieve a unit

Practice Education
mark ≥ 40 by achieving the conditions stated above after a first reassessment opportunity will not match the requirements for the award of BSc (Hons) Physiotherapy and will not be eligible to apply for registration as a physiotherapist with the HPC.
Subject to satisfactory completion the practice placement hours accrued will contribute toward the 1,000 hours of practice placement required by the Chartered Society of Physiotherapy in order to become eligible for membership.
Students are required to have satisfactorily completed occupational health assessment and enhanced CRB check prior to commencing this unit.
NOTE: failure to achieve the standard required for LO16 and 17 will constitute a fail overall
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Transition to Professional Practice2 BRIEF SUMMARY This unit is intended to assist the student as they
prepare to access their first post in physiotherapy. There is a strong focus on professionalism and the demonstration of competence through a variety of media.
3 UNIT CODE NUMBER 281510194 HOME PROGRAMME BSc (Hons) Physiotherapy5 HOME DEPARTMENT Health Professions6 SUBJECT AREA B160 physiotherapy7 UNIT LEADER(S) Kathryn Heathcote8 CREDIT VALUE 20 CREDITS AT
LEVEL:6 (H)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
200
40 hours of classroom contact160 hours of directed/self-directed study and assessment preparation
10 UNIT STATUS Mandatory core
11 PRE-REQUISITES All level 4(C) unitsPractice Placement 0All level 5 (I) units
12 CO-REQUISITES None
13 UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to, have attained or demonstrated:Cognitive and intellectual
1. relate critical awareness and knowledge of factors underpinning professional autonomy and accountability.
2. relate critical awareness and understanding of factors underpinning effective professional relationships
3. relate critical awareness of the factors that contribute to the development of effective personal and professional skills.
4. interpret the responsibilities of a registered professional in the context of health and social care services
5. critically reflect upon previous individual experiences of practice placement using a variety of methods
6. demonstrate application of clinical reasoning and evidence based practice to justify all decision making in practice

Practice Education14 CURRICULUM
OUTLINE
This unit is intended to articulate expectations of a registered professional within health and social care services. It will enable the student to develop as an autonomous and accountable practitioner.The unit will cover:
Standards and requirements of professional and statutory regulator bodies.
Legal and ethical responsibilities The principles and practice of patient confidentiality Fitness for practice and the need for CPD Clinical governance Interprofessional working Effective team working: with a work group and work
with peers towards a common goal Communication skills Time management/prioritisation skills Anti-discriminatory/anti-oppressive practice Working within scope of practice Maintenance of health and well being Formal and informal methods of reflection and how
they may inform practice Use of reflection and clinical reasoning in order to
make informed judgements, decisions and prioritise actions taken to support their professional development
The unit will also address preparation of the student for their first clinical post. It will include CV development, interview practice, job applications.
15 LEARNING & TEACHING ACTIVITIES
Use of student-centred learning strategies. Based on a main case study with self-directed study and tutorials. Other teaching strategies to include lectures, group work, tutorials, peer-supported presentations, role play and mock interviews.
16 ASSESSMENT STRATEGIES
essay based assignment (8 pages A4 double spaced) (LO1-6 – 100% summative).
mock interviews with peer and staff feedback, (formative)
peer review of personal statements, group presentations with peer and staff feedback, self analysis of learning development needs with action planning (formative).
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The student will demonstrate: A critical awareness and understanding of the current
key issues affecting professional physiotherapy practice and relate to the unit learning outcomes
An ability to access, select, evaluate and synthesise information related to complex issues on order to produce a logical, coherent and evaluative piece of writing
An ability to present a written assignment in the appropriate academic style and format.
Assessed through generic assessment criteria combined with

Practice Educationassignment specific criteria that are linked overtly to the unit learning outcomes.
18 INDICATIVE STUDENT LEARNING RESOURCES
Bolton, G. E. J. (2010) Reflective practice: writing and professional development. 3rd ed. London: Sage Publications Ltd.
Chartered Society of Physiotherapy. (2001) Developing a portfolio. A guide for C.S.P. members. London: Chartered Society of Physiotherapy.
Chartered Society of Physiotherapy. (2002) Rules of professional conduct. 2nd ed. London: Chartered Society of Physiotherapy. [Online] http://www.csp.org.uk/uploads/documents/csp_rules_conduct.pdf
Chartered Society of Physiotherapy (2006), The New Chartered Physiotherapist: Guidelines of good practice for new entrants to Physiotherapy. London: Chartered Society of Physiotherapy.
Chartered Society of Physiotherapy. (2005) Core standards of physiotherapy practice. 2nd ed. London: Chartered Society of Physiotherapy. [Online] http://www.csp.org.uk/uploads/documents/csp_core_standards_2005.pdf
Chartered Society of Physiotherapy (2005), Keeping a portfolio: getting started. London: Chartered Society of Physiotherapy.
Chartered Society of Physiotherapy (2005), Mentoring: A Review. London: Chartered Society of Physiotherapy.
Chartered Society of Physiotherapy (2008), Keeping a CPD Portfolio – Using your ePortfolio / CD. Guidance for Students. London: Chartered Society of Physiotherapy. [online] http://www.interactivecsp.org.uk/uploads/documents/PD013%20-%20Student%20portfolio%20guidance%20mixed.doc
Dainow, S. (1998), Working and surviving in organizations: A trainer’s guide to developing organisational skills. Chichester, Wiley and Sons Ltd.
Department of Health (2004), The NHS Knowledge and Skills Framework (NHS KSF) and Development Review Process. London: Department of Health. [online] http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4090843>
Fook, J. and Gardiner, F. (2007) Practising critical reflection. A resource handbook. Berkshire: Open University Press.
Health Professions Council. (2007) Standards of proficiency. London: Health Professions Council. [Online] http://www.hpc-uk.org/assets/documents/10000DBCStandards_of_Proficiency_Physiotherapists.pdf

Practice EducationHealth Professions Council (2008), Confidentiality – Guidance for Registrants. London: Health Professions Council.
Higgs, J. and Jones, M.A. (2008) Clinical reasoning in the health professions. 3rd ed. Oxford: Butterworth Heineman.
Manchester Metropolitan University. (2008) Clinical reasoning guidelines – Physiotherapy management 2
Molyneaux, J. (2001), Interprofessional teamworking: what makes teams work well? Journal of Interprofessional Care. Vol. 15, no. 1, pp. 29-35
Mullins, L. J. (2009), Management and organisational behaviour, 8th ed. Prentice Hall, Harlow.
Moon, J. A. (2004) A handbook of reflective and experiential learning: theory and practice. London: Taylor and Francis.
Redmond, B. (2006) Reflection in action. Developing reflective practice in health and social services. Aldershot: Ashgate Publishing Ltd.
Skjorshammer, M. (2001), ‘Co-operation and conflict in a hospital: interprofessional differences in perception and management of conflicts.’ Journal of Interprofessional Care. Vol. 15, no. 1, pp. 7-18
Waterworth, S. (2003), ‘Time management strategies in nursing practice.’ Journal of Advanced Nursing. Vol. 43, no. 5, pp. 432-440
Further resources
Chartered Society of Physiotherapy. (2008) PebblePAD: e-portfolio system. [Online] [Accessed on 27 April 2009) http://eportfolio.csp.org.uk/
19 ANY ADDITIONAL NOTES AND COMMENTS
20 DATE OF APPROVAL 11 & 12 February 201021 DATE OF MOST
RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Evidence Based Practice 1
2 BRIEF SUMMARY This unit (with evidence based practice 2) offers the students the opportunity to explore certain topics to greater depth. They will use skills learned during other third year units to critically examine evidence that supports physiotherapy management of a variety of conditions in depth and use this to support reasoned decision making.
3 UNIT CODE NUMBER 28151020
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160 physiotherapy
7 UNIT LEADER(S) Daphne Dawson/Deborah O’Connor/Sally Hartley/Narayan Prabhu/Jenny Crampton/Suzanne Gough
8 CREDIT VALUE 10 CREDITS AT LEVEL:
6(H)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
10020 hours of classroom contact
80 hours of directed/self-directed study and assessment preparation
10 UNIT STATUS Mandatory core
11 PRE-REQUISITES All level 4(C) unitsPractice Placement 0All level 5 (I) units
12 CO-REQUISITES
13 UNIT LEARNING OUTCOMES
The student will reflect on prior learning in order to select topics for further study from a range offered.The student will demonstrate
1. skill in the critical appraisal of relevant and contemporary literature
2. synthesis and analysis of findings to influence the clinical reasoning process
3. ability to construct, sustain and support arguments in order to make informed judgements
4. ability to engage effectively in debate in a professional manner and produce detailed and coherent arguments
5. presentation of arguments in an appropriate academic style.
14 CURRICULUM OUTLINE
The student will select one topic from a minimum of three offered. The topics will include clinical areas such as the

Practice Educationmanagement of pain, exercise prescription and psychosocial model of rehabilitation.The topics available will be influenced by contemporary National Guidelines and policies related to health care provision.
15 LEARNING & TEACHING ACTIVITIES
Lectures, small group tutorials, seminars and presentations.
16 ASSESSMENT STRATEGIES
Formative evaluation will be undertaken in a context appropriate to the topic selected
Open book examination (1.5 hours) (LO1-5 – 100% summative).
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The student will demonstrate An in-depth understanding of the topics selected An ability to critically evaluate, apply, analyse and
synthesise relevant literature An ability to develop, sustain and support reasoned
and coherent arguments in order to justify their conclusions and clinical decisions
An ability to select and use appropriate literature and unit material to support their arguments
An ability to present their arguments in an appropriate academic style.
Formative assessment procedures will be relevant to the topic selected.Summative assessment procedures will be assessed through generic criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
18 INDICATIVE STUDENT LEARNING RESOURCES
Reading lists will be based on current literature available that is related to the topic areas selected.Particular reference will be made to research based evidence, evidence based guidelines, professional body document/publications and National Service Frameworks.
19 ANY ADDITIONAL NOTES AND COMMENTS
Topics offered will be reviewed regularly to ensure their relevance to contemporary physiotherapy practice, healthcare delivery and service priorities.
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Evidence Based Practice 2
2 BRIEF SUMMARY This unit (with evidence based practice 1) offers the students the opportunity to explore certain topics to greater depth. They will use skills learned during other third year units to critically examine evidence that supports physiotherapy management of a variety of conditions in depth and use this to support reasoned decision making.
3 UNIT CODE NUMBER 28151021
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160 physiotherapy
7 UNIT LEADER(S) Daphne Dawson/Deborah O’Connor/Sally Hartley/Narayan Prabhu/Jenny Crampton/Suzanne Gough
8 CREDIT VALUE 10 CREDITS AT LEVEL:
6(H)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
10020 hours of classroom contact
80 hours of directed/self-directed study and assessment preparation
10 UNIT STATUS Mandatory core
11 PRE-REQUISITES All level 4(C)Practice Placement 0All level 5 (I) units
12 CO-REQUISITES
13 UNIT LEARNING OUTCOMES
The student will reflect on prior learning in order to select topics for further study from a range offered.The student will demonstrate
1. skill in the critical appraisal of relevant and contemporary literature
2. synthesis and analysis of findings to influence the clinical reasoning process
3. ability to construct, sustain and support arguments in order to make informed judgements
4. ability to engage effectively in debate in a professional manner and produce detailed and coherent arguments
5. presentation of arguments in an appropriate academic style.
14 CURRICULUM OUTLINE
The students will select one topic from a minimum of three offered. The topics may include clinical areas such as the

Practice Educationneuroplasticity and neurorehabilitation, management of the recently deteriorated patient and aspects of musculoskeletal rehabilitation.The topics available will be influenced by contemporary National Guidelines and policies related to health care provision
15 LEARNING & TEACHING ACTIVITIES
Lectures, small group tutorials, seminars and presentations.
16 ASSESSMENT STRATEGIES
Formative evaluation will be undertaken in a context appropriate to the topic selected
Open book examination (1.5 hours) (LO1-5 – 100% summative).
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The student will demonstrate An in-depth understanding of the topics selected An ability to critically evaluate, apply, analyse and
synthesise relevant literature An ability to develop, sustain and support reasoned
and coherent arguments in order to justify their conclusions and clinical decisions
An ability to select and use appropriate literature and unit material to support their arguments
An ability to present their arguments in an appropriate academic style.
Formative assessment procedures will be relevant to the topic selected.Summative assessment procedures will be assessed through generic criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
18 INDICATIVE STUDENT LEARNING RESOURCES
Reading lists will be based on current literature available that is related to the topic areas selected.Particular reference will be made to research based evidence, evidence based guidelines, professional body document/publications and National Service Frameworks.
19 ANY ADDITIONAL NOTES AND COMMENTS
Topics offered will be reviewed regularly to ensure their relevance to contemporary physiotherapy practice, healthcare delivery and service priorities.
20 DATE OF APPROVAL 11 & 12 February 2010
21 DATE OF MOST RECENT CONSIDERATION:

Practice Education

Practice Education
1 UNIT TITLE Critical Thinking and Enquiry ‘B’
2 BRIEF SUMMARY This unit provides students an opportunity to apply research skills gained during earlier units to develop an ethical and feasible research proposal that has the potential to enhance the evidence base for physiotherapy practice.
3 UNIT CODE NUMBER
28151022
4 HOME PROGRAMME
BSc (Hons) Physiotherapy
5 HOME DEPARTMENT
Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Janet Rooney
8 CREDIT VALUE 20 CREDITS AT LEVEL:
6(H)
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
20010 hours of classroom contact/academic tutorial support190 hours of directed/self-directed study and assessment preparation.
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES All level 4(C) unitsPractice Placement 0All level 5 (I) units
12 CO-REQUISITES None
13 UNIT LEARNING OUTCOMES
On successful completion of this unit students will be able to:Cognitive and intellectual skills
1. generate professionally relevant research problem and to develop a clearly defined research question that has potential for systematic investigation.
2. apply a range of established problem solving approaches in order to identify and critically evaluate the evidence base for physiotherapy practice.
3. generate logical and reasoned argument to define clear and relevant study aims and objectives/hypotheses.
4. Identify and justify a research design/methodology that matches the research question and develop an ethical research protocol to allow the question to be systematically and rigorously investigated.
5. Develop and justify an approach to the analysis and presentation of data that would allow conclusions to be drawn.

Practice Education6. Present the proposal in an appropriate academic style.
14 CURRICULUM OUTLINE
Build on achievement at level 4 and 5 to further develop skills in Critical thinking Literature searching Logical reasoning Developing logical and reasoned argument Academic writing Learning needs analysis Managing complex processes (to include time and
resources and professional relationships). The use of mentoring relationships to facilitate personal
development
15 LEARNING & TEACHING ACTIVITIES
Student centred learning with dedicated supervisor support.Lectures and tutorials, group discussions for peer support and the use of PebblePAD.
16 ASSESSMENT STRATEGIES
Written submission of initial idea for research proposal (500-1,000 words LO1-6 – formative)
Written extended research proposal (24 sides A4 double spaced with academic supervisory support – LO1-6 – 100% summative).
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
The students will produce a detailed research proposal that demonstrates their ability to:
Search for, select, critically evaluate and synthesise the current evidence underpinning physiotherapy practice related to their chosen topic to develop a clearly formulate a justified research question.
Develop an ethical, appropriate, realistic methodology with robust support from appropriate high quality literature.
Identify a clear strategy for the collection, analysis and presentation of relevant data.
Use logical, reasoned, coherent, evaluative and supported arguments.
Present the proposal in an appropriate academic format.Formative assessment procedures will be assessed by academic supervisors and constructive and developmental written feedback will be given related to the feasibility of the study and the ethical considerations and by peer evaluation of an abstract.Summative assessment procedures will be assessed through generic criteria combined with assignment specific criteria that are linked overtly to the unit learning outcomes.
18 INDICATIVE STUDENT LEARNING RESOURCES
Anderson, J. and Poole, M. (2001), Assignment and thesis writing, 4th edn, Chichester: Wiley.
Blackmer, J. (2003). The unique ethical challenges of conducting research in the rehabilitation medicine population BMC Medical Ethics [Online] http://www.biomedcentral.com/1472-6939/4/2
Bleakley, C. M., O’Connor, S., Tully, M. A., Rocke, L. G. MacAuley, D. C. and McDonugh, S. M. (2007), The PRICE study (Protection Rest Ice Compression Elevation): design of a randomized controlled trial comparing standard versus

Practice Educationcryokinetic ice applications in the management of acute ankle sprain [ISRCTBI3903946], BMC Musculoskeletal Disorders [Online] http://www.biomedcentral.com/content/pdf/1471-2474-8-125.pdf
Chartered Society of Physiotherapy (2005a), Core standards of physiotherapy practice London: Chartered Society of Physiotherapy.
Chartered Society of Physiotherapy (2005b) Internet Resources (1): Using the Internet, London: Chartered Society of Physiotherapy. [Online] <http://www.csp.org.uk/uploads/documents/csp_lis06_internet1.pdf
Chartered Society of Physiotherapy (2005c) Internet Resources (2): Finding published information, London, Chartered Society of Physiotherapy [Online] http://www.csp.org.uk/uploads/documents/csp_lis07_internet.pdf
Chartered Society of Physiotherapy (2005d) Internet resources (3): Assessing the quality of information and putting it into practice London: Chartered Society of Physiotherapy. [Online] http://www.csp.org.uk/uploads/documents/csp_lis08_internet.pdf
Chartered Society of Physiotherapy (2009) CSP guide to literature searching. London: Chartered Society of Physiotherapy [Online] http://www.csp.org.uk/uploads/documents/Literature_searching_PD051.pdf
Crombie, I. K. (1996), The pocket guide to critical appraisal: a handbook for health care professionals London: BMJ Publishing.
Delany, C. M. (2005), Respecting patient autonomy and obtaining their informed consent: ethical theory - missing in action, Physiotherapy, vol. 91, no. 4, pp. 197-203.
Department of Health (2005), Research governance framework for health and social care, 2nd edn, London: Department of Health [Online] http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4108962
Health Professions Council (2007), Standards of proficiency: physiotherapists London: Health Professions Council.
Hicks, C. (2009), Research methods for clinical therapists: applied project design and analysis, 5th edn, Edinburgh: Churchill Livingstone.
Higgins, J. P. T. and Green, S. (2006). Cochrane Handbook for Systematic Reviews of Interventions 4.2.6. [Online]. The Cochrane Library. Issue 3 [Online] http://www.cochrane.org/resources/handbook/Handbook4.2.6Sep2006.pdf

Practice EducationMaxwell, J. (2005), Qualitative research design: an interactive approach London: Sage.
Mays, N. and Pope, C. (2000), Qualitative research in health care: assessing quality in qualitative research, British Medical Journal, 320 pp. 50-52.
McPherson, K. and Lord, S. (2000), Clinician's guide to research Part 2: matching the method to the question, New Zealand Journal of Physiotherapy, 28 (2), pp. 20-29.
Medical Research Council (2000), Good research practice London: Medical Research Council.
National Research Ethics Service (2007). Information sheets & consent forms [online] http://www.nres.npsa.nhs.uk/EasySiteWeb/GatewayLink.aspx?alId=4757
National Patient Safety Agency (2008). Standard Operating Procedures for Research Ethics Committees [Online] http://www.nres.npsa.nhs.uk/EasySiteWeb/GatewayLink.aspx?alId=11364
Peat, J. (2002), Health science research; a handbook of quantitative methods London: Sage.
Pope, C., Ziebland, S., and Mays, N. (2000), Qualitative research in health care: analysing qualitative data, British Medical Journal, 320 pp. 114-116.
Sim, J. and Wright, C. (2000), Research in health care: concepts, designs and methods Cheltenham: Stanley Thornes (Publishers) Ltd.
Walker, J., Holloway, I., and Wheeler, S. (2005), Guidelines for the ethical review of qualitative research, Research Ethics Review, vol. 1, no. 3, pp. 90-96.
World Medical Association. (2002). Declaration of Helsinki: ethical principles for medical research involving human subjects < http://www.wma.net/e/policy/b3.htm
19 ANY ADDITIONAL NOTES AND COMMENTS
20 DATE OF APPROVAL
11 & 12 February 2010
21 DATE OF MOST

Practice Education
RECENT CONSIDERATION:

Practice Education
1 UNIT TITLE Practice Placement 6
2 BRIEF SUMMARY This practice placement is undertaken during the third year of the programme. This placement is normally arranged by the student in a clinical speciality and a placement location of their choice. The university requires that the placements selected match requirements related to provisions for Health and Safety at Work and undertakings related to Equality and Opportunity legislation. The university reserves the right to decline a student’s request to undertake practice placement 6 in a particular locality should these requirements not be met.The student must be supervised by an individual who is registered as a physiotherapist with the Health Professions Council or who is recognised as a physiotherapist by regulatory bodies in the relevant country where this placement occurs outside the United Kingdom.Students will have the opportunity to consolidate their core professional knowledge and skills in preparation for employment.
3 UNIT CODE NUMBER 28151023
4 HOME PROGRAMME BSc (Hons) Physiotherapy
5 HOME DEPARTMENT Health Professions
6 SUBJECT AREA B160: physiotherapy
7 UNIT LEADER(S) Joanne Nicholson / Sophie Taylor
8 CREDIT VALUE 10 practice credits CREDITS AT LEVEL:
9 TOTAL AMOUNT OF STUDENT LEARNING (NOTIONAL HOURS OF LEARNING)
125 (minimum) clinical practice
10 UNIT STATUS Mandatory Core
11 PRE-REQUISITES All level 4(C) unitsPractice Placement 0All level 5 (I) units Practice placement 4 Practice placement 5 – placement element.
12 CO-REQUISITES None
13 UNIT LEARNING OUTCOMES
There are 17 learning outcomes, which are divided into 5 categories:Interpersonal skillsThe student will
1. demonstrate effective and appropriate skills in
Practice Educationcommunication in order to collaborate and work effectively in partnership with others (professionals, support staff, patients/clients, carers, relatives and external agencies) to the benefit of the client/patient and maximise health outcomes.
2. contribute effectively to work undertaken as part of a team.
3. recognise the scope of practice of other professionals.
4. acknowledge cross professional boundaries.5. make appropriate referrals to others.
Management of patientThe student will
6. demonstrate effective self management of workload.7. know the limits of their own practice and when to
seek advice.8. independently manage their own learning.
Management of patientThe student will
9. gather appropriate information relating to the patient.10. plan and carry out an appropriate objective
examination.11. analyse examination findings and formulate a written
treatment plan in partnership with the patient.12. implement and critically evaluate the impact of, or
response to treatment interventions.DocumentationThe student will
13. maintain accurate patient recordsProfessional PracticeThe student will
14. promote patient centred care15. comply with the CSP Rules of Professional
Conduct/Standards of Conduct, Performance and Ethics
16. practice in line with relevant health and safety policy17. work independently and as part of a team as
appropriate.
14 CURRICULUM OUTLINE
The student will be able to achieve the learning outcomes by taking responsibility for all aspects of the physiotherapy management of a mixed caseload with supervision from a practice placement educator. The caseload will include complex patient conditions that do not respond in a predictable wayThe student will have opportunity to relate theory to practice and will be able to generate multiple competing hypotheses to explain patient’s presenting signs and symptoms and systematically exclude those which do not apply to reach sound judgements. They will have opportunity to develop and apply an understanding of a complex body of knowledge and be able to apply problem solving skills to more complex situations and unpredictable circumstances.

Practice EducationThey will have opportunity to consolidate skills in the evaluation of evidence, the development and supporting of arguments in the context of clinical decision making and will be encouraged to question assumptions to reach sound decisions.
15 LEARNING & TEACHING ACTIVITIES
Assessment and treatment of patients under the supervision of an individual who is registered as a physiotherapist with the Health Professions Council
Experiential learning with reflective practice in the clinical setting
Use of a learning development plan/contract Self directed study Self evaluation at mid-way and end of placement Peer learning Clinical staff development./in service training
sessions Attendance at team meetings/case conference. Workshops Tutorials Lectures
Learning will take place at a variety of clinical settings.
16 ASSESSMENT STRATEGIES
The supervising clinician will assess whether the student has demonstrated an acceptable level of clinical skills and underpinning knowledge, an acceptable level of professional behaviour and safe practice.
This placement is graded pass/fail based on satisfactory physiotherapy practice, adherence to Health and Safety arrangements and adherence to requirements for Professional Behaviour.
The CAT can be used to provide constructive and developmental feedback for students
17 ASSESSMENT CRITERIA FOR UNIT/ELEMENTS OF ASSESSMENT
Specific assessment criteria for level 6(H) practice placements will apply
The assessment criteria relate to safe clinical practice and professional behaviour as articulated in relevant PSRB documents (CSP 2002; 2005, HPC 2008; 2010)
Satisfactory clinical practice will be determined in terms of the students ability to match levels of performance articulated through the common assessment tool (level 6)
18 INDICATIVE STUDENT LEARNING RESOURCES
Chartered Society of Physiotherapy. (2002) Rules of professional conduct. 2nd ed. London: Chartered Society of Physiotherapy. [Online] [Accessed on 27 April 2009] http://www.csp.org.uk/uploads/documents/csp_rules_conduct.pdf
Chartered Society of Physiotherapy (2005) Core standards of Physiotherapy Practice. London: Chartered Society of Physiotherapy
Health Professions Council (2010), Guidance on conduct and ethics for students. London: Health Professions Council.

Practice EducationHealth Professions Council. (2008) Standards of conduct, performance and ethics. London: Health Professions Council. [Online] [Accessed on 22 May 2009] http://www.hpc-uk.org/assets/documents/10002367FINALcopyofSCPEJuly2008.pdf
Moon, J. A. (2004) A handbook of reflective and experiential learning: theory and practice. London: Taylor and Francis
19 ANY ADDITIONAL NOTES AND COMMENTS
This unit carries practice credits and is assessed pass/fail according to regulation D2.2
The unit (in addition to the other requirements for the award of an honours degree) must be successfully completed for a student to graduate with BSc (Hons) Physiotherapy
The practice placement hours accrued will contribute toward the 1,000 hours of practice placement required by the Chartered Society of Physiotherapy in order to become eligible for membership.
Students are required to have had occupational health and CRB clearance prior to commencing this unit.
Students who are unsuccessful at first attempt will be offered a reassessment opportunity at the discretion of the Board of Examiners. A further placement of a minimum of 125 hours duration will be arranged by the programme practice placement coordinators
Students who fail practice placement 6 after reassessment will not be eligible for the award of BSc (Hons) Physiotherapy and will exit the programme with a pass degree and will therefore be ineligible to apply for registration as a physiotherapist with the HPC.

Practice Education

Practice Education



![ACHC ACCREDITATION STANDARDS ACHC ACCREDITATION GUIDE …€¦ · ACHC ACCREDITATION STANDARDS ACHC ACCREDITATION . GUIDE TO SUCCESS WORKBOOK [ HOME HEALTH ] ÍÍÜÏÎÓÞËÞÓÙØ](https://img.pdfslide.us/doc/110x75/5eac162a083b4c0f86673c3a/achc-accreditation-standards-achc-accreditation-guide-achc-accreditation-standards.jpg)

























