Embed Size (px)
Citation preview
Issue 17 - Winter 2013
EDUCATION
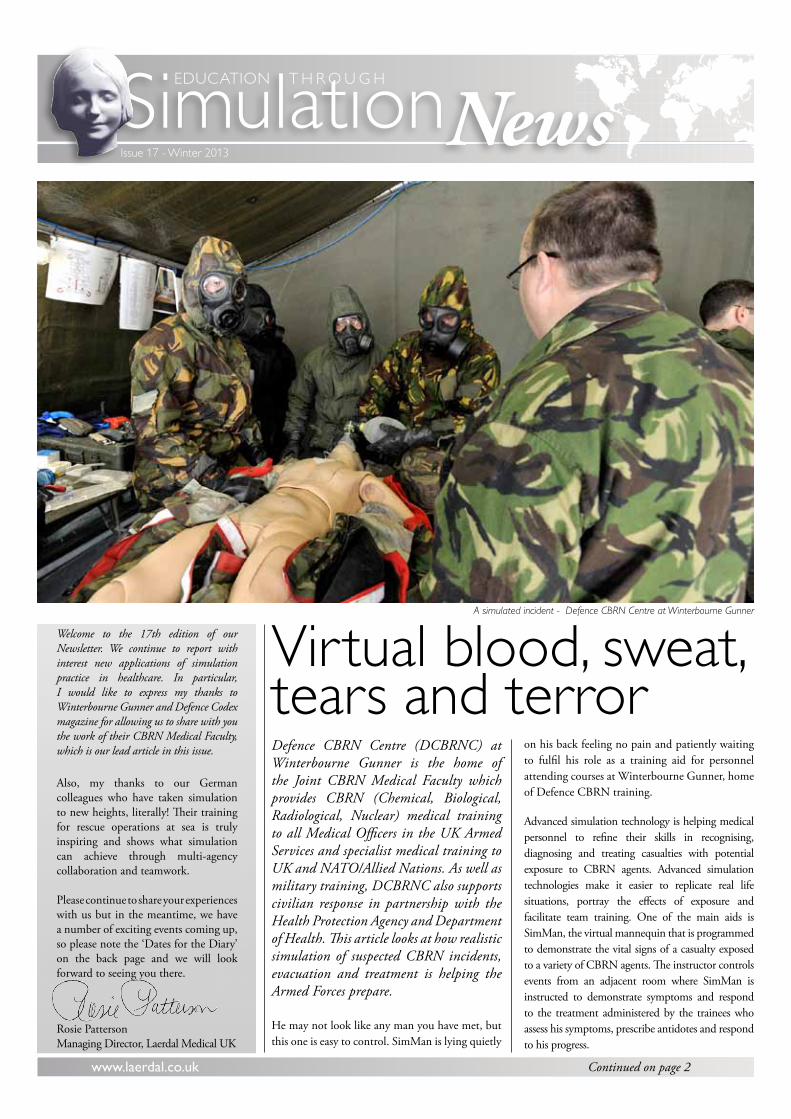
Virtual blood, sweat,tears and terrorDefence CBRN Centre (DCBRNC) at Winterbourne Gunner is the home of the Joint CBRN Medical Faculty which provides CBRN (Chemical, Biological, Radiological, Nuclear) medical training to all Medical Officers in the UK Armed Services and specialist medical training to UK and NATO/Allied Nations. As well as military training, DCBRNC also supports civilian response in partnership with the Health Protection Agency and Department of Health. This article looks at how realistic simulation of suspected CBRN incidents, evacuation and treatment is helping the Armed Forces prepare.
He may not look like any man you have met, but this one is easy to control. SimMan is lying quietly
on his back feeling no pain and patiently waiting to fulfil his role as a training aid for personnel attending courses at Winterbourne Gunner, home of Defence CBRN training.
Advanced simulation technology is helping medical personnel to refine their skills in recognising, diagnosing and treating casualties with potential exposure to CBRN agents. Advanced simulation technologies make it easier to replicate real life situations, portray the effects of exposure and facilitate team training. One of the main aids is SimMan, the virtual mannequin that is programmed to demonstrate the vital signs of a casualty exposed to a variety of CBRN agents. The instructor controls events from an adjacent room where SimMan is instructed to demonstrate symptoms and respond to the treatment administered by the trainees who assess his symptoms, prescribe antidotes and respond to his progress.
www.laerdal.co.uk Continued on page 2
T H R O U G H
Welcome to the 17th edition of our Newsletter. We continue to report with interest new applications of simulation practice in healthcare. In particular, I would like to express my thanks to Winterbourne Gunner and Defence Codex magazine for allowing us to share with you the work of their CBRN Medical Faculty, which is our lead article in this issue.
Also, my thanks to our German colleagues who have taken simulation to new heights, literally! Their training for rescue operations at sea is truly inspiring and shows what simulation can achieve through multi-agency collaboration and teamwork.
Please continue to share your experiences with us but in the meantime, we have a number of exciting events coming up, so please note the ‘Dates for the Diary’ on the back page and we will look forward to seeing you there.
Rosie PattersonManaging Director, Laerdal Medical UK
News
A simulated incident - Defence CBRN Centre at Winterbourne Gunner
2
Education through Simulation News - Issue 17 - Winter 2013
Continued from page 1
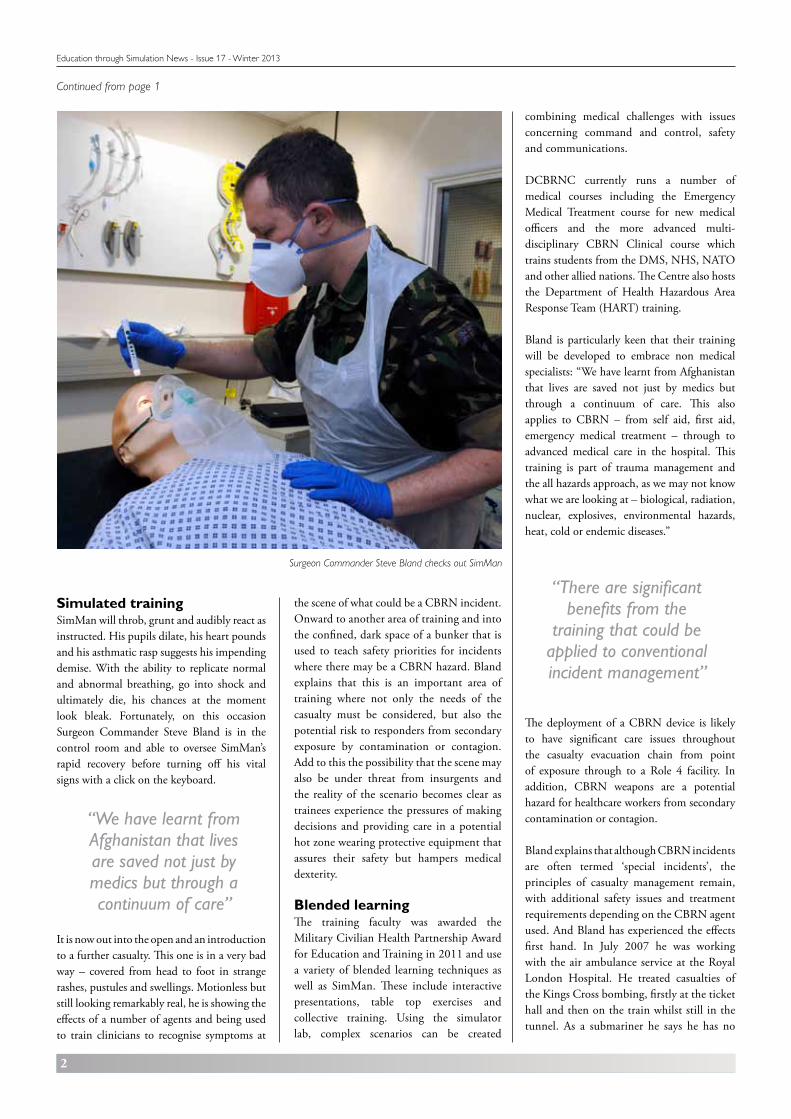
Simulated training SimMan will throb, grunt and audibly react as instructed. His pupils dilate, his heart pounds and his asthmatic rasp suggests his impending demise. With the ability to replicate normal and abnormal breathing, go into shock and ultimately die, his chances at the moment look bleak. Fortunately, on this occasion Surgeon Commander Steve Bland is in the control room and able to oversee SimMan’s rapid recovery before turning off his vital signs with a click on the keyboard.
It is now out into the open and an introduction to a further casualty. This one is in a very bad way – covered from head to foot in strange rashes, pustules and swellings. Motionless but still looking remarkably real, he is showing the effects of a number of agents and being used to train clinicians to recognise symptoms at
combining medical challenges with issues concerning command and control, safety and communications.
DCBRNC currently runs a number of medical courses including the Emergency Medical Treatment course for new medical officers and the more advanced multi-disciplinary CBRN Clinical course which trains students from the DMS, NHS, NATO and other allied nations. The Centre also hosts the Department of Health Hazardous Area Response Team (HART) training.
Bland is particularly keen that their training will be developed to embrace non medical specialists: “We have learnt from Afghanistan that lives are saved not just by medics but through a continuum of care. This also applies to CBRN – from self aid, first aid, emergency medical treatment – through to advanced medical care in the hospital. This training is part of trauma management and the all hazards approach, as we may not know what we are looking at – biological, radiation, nuclear, explosives, environmental hazards, heat, cold or endemic diseases.”
The deployment of a CBRN device is likely to have significant care issues throughout the casualty evacuation chain from point of exposure through to a Role 4 facility. In addition, CBRN weapons are a potential hazard for healthcare workers from secondary contamination or contagion.
Bland explains that although CBRN incidents are often termed ‘special incidents’, the principles of casualty management remain, with additional safety issues and treatment requirements depending on the CBRN agent used. And Bland has experienced the effects first hand. In July 2007 he was working with the air ambulance service at the Royal London Hospital. He treated casualties of the Kings Cross bombing, firstly at the ticket hall and then on the train whilst still in the tunnel. As a submariner he says he has no
“We have learnt from Afghanistan that lives are saved not just by medics but through a continuum of care”
“There are significant benefits from the
training that could be applied to conventional incident management”
the scene of what could be a CBRN incident. Onward to another area of training and into the confined, dark space of a bunker that is used to teach safety priorities for incidents where there may be a CBRN hazard. Bland explains that this is an important area of training where not only the needs of the casualty must be considered, but also the potential risk to responders from secondary exposure by contamination or contagion. Add to this the possibility that the scene may also be under threat from insurgents and the reality of the scenario becomes clear as trainees experience the pressures of making decisions and providing care in a potential hot zone wearing protective equipment that assures their safety but hampers medical dexterity.
Blended learning The training faculty was awarded the Military Civilian Health Partnership Award for Education and Training in 2011 and use a variety of blended learning techniques as well as SimMan. These include interactive presentations, table top exercises and collective training. Using the simulator lab, complex scenarios can be created
Surgeon Commander Steve Bland checks out SimMan
3
Education through Simulation News - Issue 17 - Winter 2013
fear of confined spaces, but it is more likely that his professional training and personal bravery contributed to his ability to respond.
At the time the reason for the catastrophe had not been determined, but Bland says that his training and personal interest in CBRN influenced his initial assessment: “One of the things I was looking at was whether the casualty had pinpoint pupils. The fire service was also able to provide advice using their radiation monitor. With military training you understand the mechanism of blast injuries and what to expect from an explosive device. Understanding the risks of CBRN enhances that knowledge.”
Bland is keen to share his knowledge and experience with his military and NHS colleagues: “One of the reasons I went into CBRN training initially was to make sure that others can recognise and know how to do a dynamic risk assessment on CBRN hazards. We use an underground recognition scenario to look at what CBRN agents may have been released, how these can be assessed, mitigated and any limitations that might affect our actions.”
and hazardous materials, DCBRNC will continue to train those who will be at the forefront in the event of a CBRN event. Future challenges for Bland include developing training as the Armed Forces changes focus from operations in Afghanistan: “I think the next challenge will be making sure that frontline commands are aware of the training that is available and developing this to meet contingencies and future threats.” For Bland this means exciting and challenging times and perhaps a few more near death experiences for SimMan.
Article re-produced by kind permission of MOD Defence Codex, The Magazine for Defence Engineering and Science. www.science.mod.uk
Contaminating agents The physical properties of CBRN agents are very important and divided into two categories: non-persistent gases and volatile liquids (which are unlikely to remain for a significant period of time) and persistent (which require deeper decontamination). Knowledge of the contaminating agent and hazard management priorities include how to extract casualties from the hot zone, treatment of the area and life saving interventions.
Bland believes that there are significant benefits from the training that could be applied to conventional incident management: “One of the first lectures that we give is to highlight that CBRN, (with the exception of nuclear incidents which would get in the way of our response) is that by being able to understand the threats, hazards and risks we are able to do more for the casualty in what was originally thought to be a non permissive environment. We know from our training and UK and NATO exercises that there are points in the casualty chain where we can maximise our medical treatment. These include antidote administration using intraosseous infusion (bone injection and other interventions) which we have learned from trauma management in Afghanistan, Iraq and responding to terrorist events in the UK and internationally. Clinicians realise we can do more whether it is diagnosis, treatment or advising on the hazard management of casualties.”
Whilst the Government focuses on critical programmes to build security in the UK and overseas, prioritising the security of nuclear, biological and chemical materials
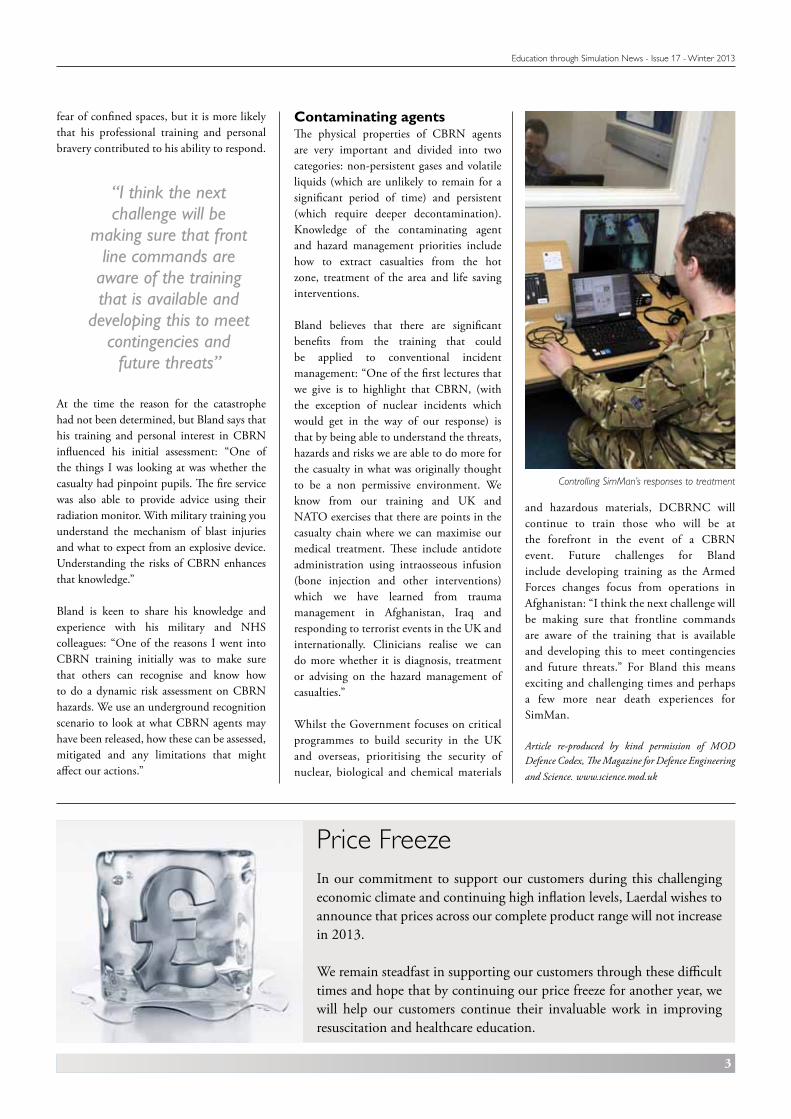
Controlling SimMan’s responses to treatment
“I think the next challenge will be
making sure that front line commands are
aware of the training that is available and
developing this to meet contingencies and
future threats”
Price FreezeIn our commitment to support our customers during this challenging economic climate and continuing high inflation levels, Laerdal wishes to announce that prices across our complete product range will not increase in 2013.
We remain steadfast in supporting our customers through these difficult times and hope that by continuing our price freeze for another year, we will help our customers continue their invaluable work in improving resuscitation and healthcare education.

4
Education through Simulation News - Issue 17 - Winter 2013
The third annual Association for Simulated Practice in Healthcare (ASPiH) conference took place in Oxford on 6th-8th November. Drawing over 350 professionals from all disciplines of medical practice and training from around the country, the diverse programme of seminars and master classes clearly demonstrated the support and the growing maturity of the UK simulation community.
This year, following investment from the Higher Education Academy into an ASPiH national simulation project, the engagement of educators, practitioners, researchers, students and associated suppliers is particularly key to the long-term growth of simulation training in and assessment of clinical and non-clinical skills. With major sponsorship from Laerdal, the aim of the event, which was co-hosted by the University of Oxford and Oxford University Hospitals NHS Trust, was to share new experiences and knowledge about the benefits of simulation, to communicate best practice and to act as a vital hub for inter-professional networking.
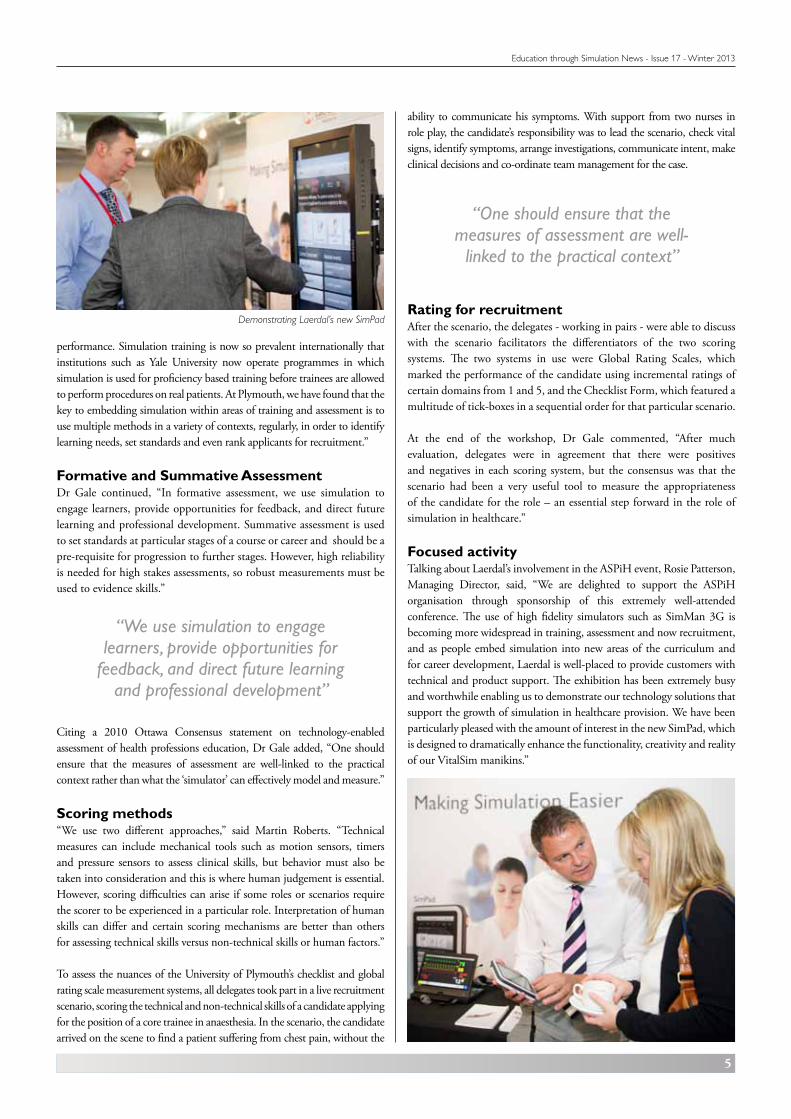
Using simulation for assessmentVibrant keynote presentations by Jonathan Wyatt, K. Anders Ericsson, Donald Clark and Tom Reader enhanced an engaging programme of special interest groups, exhibitions, poster sessions and workshops. One workshop that created huge interest was an interactive discussion that, featuring Laerdal’s SimMan 3G, explored processes involved in using simulation as an assessment tool.
The workshop, led by Dr Tom Gale and with support from Ian Anderson, Martin Roberts and Alex Mills from the Plymouth University Peninsula Schools of Medicine and Dentistry, and the Peninsula Simulation Network, focused mainly on the use of scoring metrics when using high fidelity patient simulators for assessment in training and career progression.
“A critical review of simulation-based literature by William C McGaghie et al between 2003 and 2009 outlined the importance of good quality assessment,” Dr Gale said. “The clinical profession recognises that formative and summative assessment using appropriate levels of simulation and clear scoring methods can help us assess knowledge, competence and
ASPiH Conference 2012- Leading the way
Dr Tom Dale and Ian Anderson explore simulation as an assessment tool
Demonstrating Laerdal’s new SimPad
5
Education through Simulation News - Issue 17 - Winter 2013
“We use simulation to engage learners, provide opportunities for
feedback, and direct future learning and professional development”
ability to communicate his symptoms. With support from two nurses in role play, the candidate’s responsibility was to lead the scenario, check vital signs, identify symptoms, arrange investigations, communicate intent, make clinical decisions and co-ordinate team management for the case.
Rating for recruitmentAfter the scenario, the delegates - working in pairs - were able to discuss with the scenario facilitators the differentiators of the two scoring systems. The two systems in use were Global Rating Scales, which marked the performance of the candidate using incremental ratings of certain domains from 1 and 5, and the Checklist Form, which featured a multitude of tick-boxes in a sequential order for that particular scenario.
At the end of the workshop, Dr Gale commented, “After much evaluation, delegates were in agreement that there were positives and negatives in each scoring system, but the consensus was that the scenario had been a very useful tool to measure the appropriateness of the candidate for the role – an essential step forward in the role of simulation in healthcare.”
Focused activityTalking about Laerdal’s involvement in the ASPiH event, Rosie Patterson, Managing Director, said, “We are delighted to support the ASPiH organisation through sponsorship of this extremely well-attended conference. The use of high fidelity simulators such as SimMan 3G is becoming more widespread in training, assessment and now recruitment, and as people embed simulation into new areas of the curriculum and for career development, Laerdal is well-placed to provide customers with technical and product support. The exhibition has been extremely busy and worthwhile enabling us to demonstrate our technology solutions that support the growth of simulation in healthcare provision. We have been particularly pleased with the amount of interest in the new SimPad, which is designed to dramatically enhance the functionality, creativity and reality of our VitalSim manikins.”
performance. Simulation training is now so prevalent internationally that institutions such as Yale University now operate programmes in which simulation is used for proficiency based training before trainees are allowed to perform procedures on real patients. At Plymouth, we have found that the key to embedding simulation within areas of training and assessment is to use multiple methods in a variety of contexts, regularly, in order to identify learning needs, set standards and even rank applicants for recruitment.”
Formative and Summative AssessmentDr Gale continued, “In formative assessment, we use simulation to engage learners, provide opportunities for feedback, and direct future learning and professional development. Summative assessment is used to set standards at particular stages of a course or career and should be a pre-requisite for progression to further stages. However, high reliability is needed for high stakes assessments, so robust measurements must be used to evidence skills.”
Citing a 2010 Ottawa Consensus statement on technology-enabled assessment of health professions education, Dr Gale added, “One should ensure that the measures of assessment are well-linked to the practical context rather than what the ‘simulator’ can effectively model and measure.”
Scoring methods“We use two different approaches,” said Martin Roberts. “Technical measures can include mechanical tools such as motion sensors, timers and pressure sensors to assess clinical skills, but behavior must also be taken into consideration and this is where human judgement is essential. However, scoring difficulties can arise if some roles or scenarios require the scorer to be experienced in a particular role. Interpretation of human skills can differ and certain scoring mechanisms are better than others for assessing technical skills versus non-technical skills or human factors.”
To assess the nuances of the University of Plymouth’s checklist and global rating scale measurement systems, all delegates took part in a live recruitment scenario, scoring the technical and non-technical skills of a candidate applying for the position of a core trainee in anaesthesia. In the scenario, the candidate arrived on the scene to find a patient suffering from chest pain, without the
“One should ensure that the measures of assessment are well-
linked to the practical context”
Demonstrating Laerdal’s new SimPad
6
Education through Simulation News - Issue 17 - Winter 2013
Registration Open A National Inter-Professional Paediatric Simulation Symposium
Friday 8th March 2013
Sponsored by:
This symposium continues to develop the close working relationship between ASPiH and Laerdal and their joint commitment to further develop
the effective use of simulation in paediatric healthcare simulation.
Radisson Blu Hotel, Manchester Airport, Chicago Avenue, Manchester M90 3RA
8am – 6pm
Delegate Fees: ASPiH Member: £85 Non ASPiH Member: £115*
*to include membership of ASPiH for twelve months
Registration and Call for Abstracts Information Contact Christine Spencer by e-mail
Programme08.00 - 08.30 Registration & Coffee
08.30 - 08.45 Welcome Professor Ralph MacKinnon Royal Manchester Children’s Hospital
08.45 - 09.45 Simulation as a method for transforming the work environment Dr Chris Kennedy (MD) Director – Center for Excellence in Pediatric Resuscitation Children’s Mercy Hospital, Kansas City, Missouri, USA
09.45 - 10.45 Making it all worthwhile : regional, national and international collaboration targeted to direct patient outcomes Dr. Steve Hancock Transport Consultant (Paediatric Lead) Embrace Yorkshire & Humber Infant & Children’s Transport Service
10.45 - 11.15 Break for Coffee
11.15 - 12.45 Morning Workshops You may attend 2 workshops from the morning session which are 45 minutes long.
12.45 - 13.30 Poster Walks
13.30 - 14.15 Lunch
14.15 - 15.45 Afternoon Workshops You may attend 2 workshops from the afternoon session which are 45 minutes long.
15.45 - 16.30 Break for Coffee
16.30 - 17.30 Use of simulation as an educational tool to deliver bad news in paediatrics Dr. Thomas Baugnon - Medical Doctor (MD) Staff Anaesthesiologist Anaesthesiology and Paediatric Intensive Care Unit, Necker Hospital for Sick Children – Paris
17.30 - 18.00 Questions and Close
7
Education through Simulation News - Issue 17 - Winter 2013
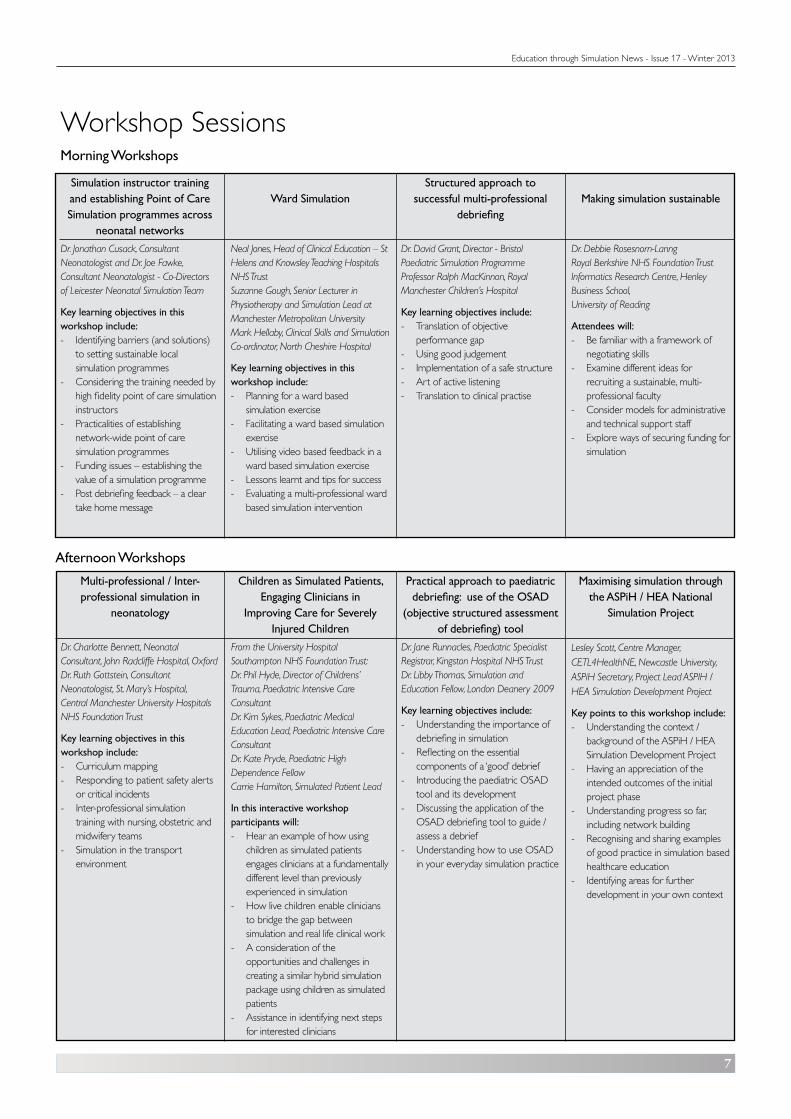
Simulation instructor training and establishing Point of Care Simulation programmes across
neonatal networksDr. Jonathan Cusack, Consultant Neonatologist and Dr. Joe Fawke, Consultant Neonatologist - Co-Directors of Leicester Neonatal Simulation Team
Key learning objectives in this workshop include:- Identifying barriers (and solutions)
to setting sustainable local simulation programmes
- Considering the training needed by high fidelity point of care simulation instructors
- Practicalities of establishing network-wide point of care simulation programmes
- Funding issues – establishing the value of a simulation programme
- Post debriefing feedback – a clear take home message
Ward Simulation
Neal Jones, Head of Clinical Education – St Helens and Knowsley Teaching Hospitals NHS TrustSuzanne Gough, Senior Lecturer in Physiotherapy and Simulation Lead at Manchester Metropolitan UniversityMark Hellaby, Clinical Skills and Simulation Co-ordinator, North Cheshire Hospital
Key learning objectives in this workshop include:- Planning for a ward based
simulation exercise- Facilitating a ward based simulation
exercise- Utilising video based feedback in a
ward based simulation exercise- Lessons learnt and tips for success- Evaluating a multi-professional ward
based simulation intervention
Structured approach to successful multi-professional
debriefing
Dr. David Grant, Director - Bristol Paediatric Simulation Programme Professor Ralph MacKinnon, Royal Manchester Children’s Hospital
Key learning objectives include:- Translation of objective
performance gap - Using good judgement - Implementation of a safe structure - Art of active listening - Translation to clinical practise
Making simulation sustainable
Dr. Debbie Rosesnorn-LanngRoyal Berkshire NHS Foundation TrustInformatics Research Centre, Henley Business School, University of Reading
Attendees will:- Be familiar with a framework of
negotiating skills- Examine different ideas for
recruiting a sustainable, multi-professional faculty
- Consider models for administrative and technical support staff
- Explore ways of securing funding for simulation
Multi-professional / Inter-professional simulation in
neonatology
Dr. Charlotte Bennett, Neonatal Consultant, John Radcliffe Hospital, OxfordDr. Ruth Gottstein, Consultant Neonatologist, St. Mary’s Hospital, Central Manchester University Hospitals NHS Foundation Trust
Key learning objectives in this workshop include:- Curriculum mapping - Responding to patient safety alerts
or critical incidents- Inter-professional simulation
training with nursing, obstetric and midwifery teams
- Simulation in the transport environment
Children as Simulated Patients, Engaging Clinicians in
Improving Care for Severely Injured Children
From the University Hospital Southampton NHS Foundation Trust:Dr. Phil Hyde, Director of Childrens’ Trauma, Paediatric Intensive Care ConsultantDr. Kim Sykes, Paediatric Medical Education Lead, Paediatric Intensive Care ConsultantDr. Kate Pryde, Paediatric High Dependence FellowCarrie Hamilton, Simulated Patient Lead
In this interactive workshop participants will:- Hear an example of how using
children as simulated patients engages clinicians at a fundamentally different level than previously experienced in simulation
- How live children enable clinicians to bridge the gap between simulation and real life clinical work
- A consideration of the opportunities and challenges in creating a similar hybrid simulation package using children as simulated patients
- Assistance in identifying next steps for interested clinicians
Practical approach to paediatric debriefing: use of the OSAD
(objective structured assessment of debriefing) tool
Dr. Jane Runnacles, Paediatric Specialist Registrar, Kingston Hospital NHS TrustDr. Libby Thomas, Simulation and Education Fellow, London Deanery 2009
Key learning objectives include:- Understanding the importance of
debriefing in simulation- Reflecting on the essential
components of a ‘good’ debrief- Introducing the paediatric OSAD
tool and its development- Discussing the application of the
OSAD debriefing tool to guide / assess a debrief
- Understanding how to use OSAD in your everyday simulation practice
Maximising simulation through the ASPiH / HEA National
Simulation Project
Lesley Scott, Centre Manager, CETL4HealthNE, Newcastle University, ASPiH Secretary, Project Lead ASPIH / HEA Simulation Development Project
Key points to this workshop include:- Understanding the context /
background of the ASPiH / HEA Simulation Development Project
- Having an appreciation of the intended outcomes of the initial project phase
- Understanding progress so far, including network building
- Recognising and sharing examples of good practice in simulation based healthcare education
- Identifying areas for further development in your own context
Workshop SessionsMorning Workshops
Afternoon Workshops

8
Education through Simulation News - Issue 17 - Winter 2013
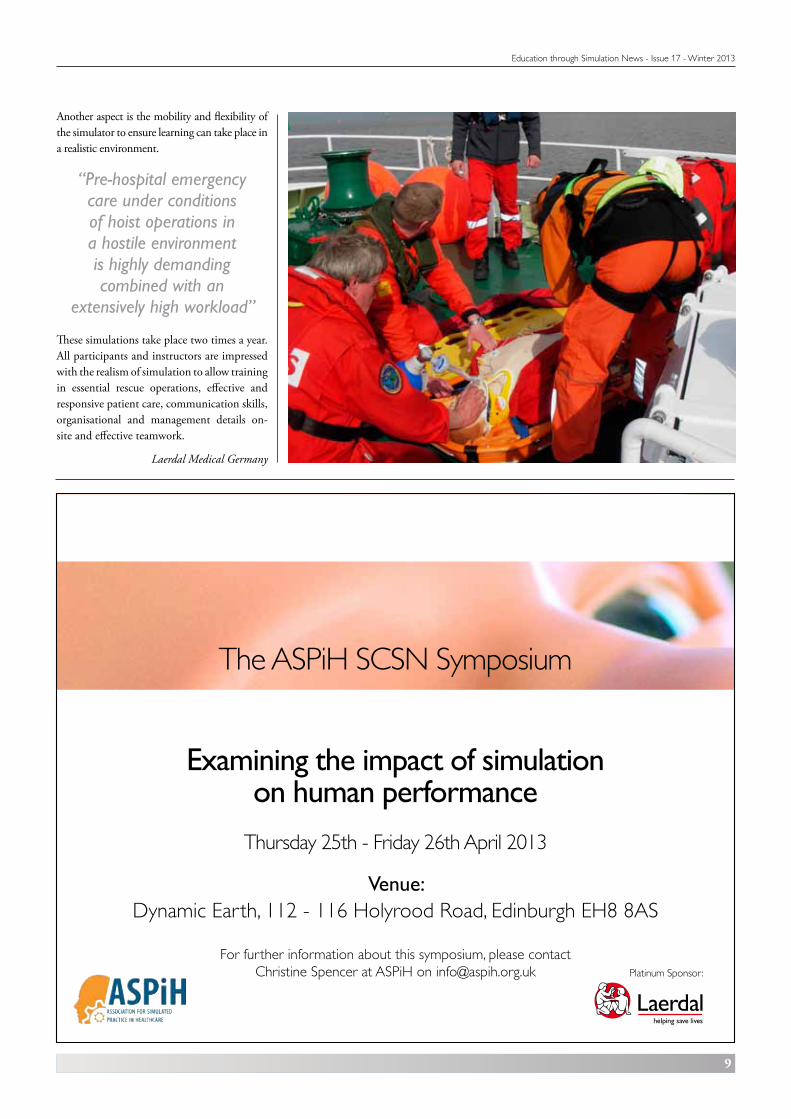
Rescue operations at sea East Frisia, GermanyPatient simulation and hoist operations (winch training) for pre-hospital emergency care
Five different aid organisations completed a successful training exercise with SimMan Essential at sea. The main objective of the training was to optimise communication skills and teamwork between different aid organisations: ADAC-Luftrettung GmbH, Deutsche Lebens-Rettungs-Gesellschaft e.V. (DLRG), Technische Hilfswerk (THW) and Deutsche Gesellschaft zur Rettung Schiffbrüchiger (DGzRS).
Participants of the simulation training exercise were pilots, air personnel and rescue workers. One essential learning goal was the recovery of a shipwrecked person with the ADAC flying ambulance near the port Hooksiel in East Frisia. The next challenge was to rescue SimMan Essential from a burning ship.
Providing pre-hospital emergency care under conditions of hoist operations in a hostile environment is highly demanding combined with an extensively high workload for all
Helicopter Emergency Medical Services (HEMS) team members. To enhance operational and patient safety under these conditions, ADAC air rescue performs combined hoist and patient simulation scenarios for rescue missions in alpine and maritime environments.
Dr. Matthias Ruppert (Medical Head of ADAC-Luftrettung GmbH München/ADAC Air Rescue Munich) is convinced of the positive training effects of simulation. He believes the wide application spectrum of SimMan Essential provides efficient training especially in Airway Management, tracheotomy, monitoring of vital parameters and inter-disciplinary training.
“The main objective of this training was to optimise
communications skills and the teamwork between
different aid organisations”
9
Education through Simulation News - Issue 17 - Winter 2013
Another aspect is the mobility and flexibility of the simulator to ensure learning can take place in a realistic environment.
These simulations take place two times a year. All participants and instructors are impressed with the realism of simulation to allow training in essential rescue operations, effective and responsive patient care, communication skills, organisational and management details on-site and effective teamwork.
Laerdal Medical Germany
The ASPiH SCSN Symposium
Examining the impact of simulation on human performance
Thursday 25th - Friday 26th April 2013
Venue: Dynamic Earth, 112 - 116 Holyrood Road, Edinburgh EH8 8AS
For further information about this symposium, please contact Christine Spencer at ASPiH on [email protected] Platinum Sponsor:
“Pre-hospital emergency care under conditions of hoist operations in a hostile environment is highly demanding combined with an
extensively high workload”
Education through Simulation News - Issue 17 - Winter 2013
10
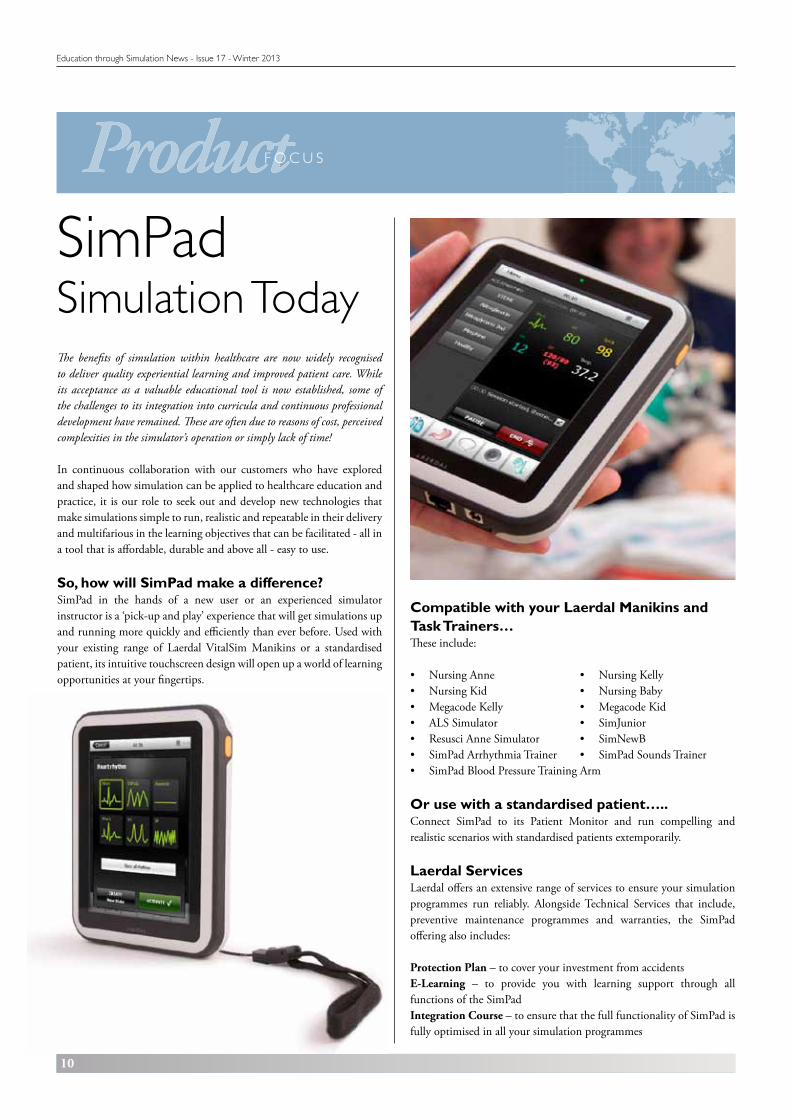
SimPadSimulation Today
Compatible with your Laerdal Manikins and Task Trainers…These include:
• NursingAnne • NursingKelly• NursingKid • NursingBaby• MegacodeKelly • MegacodeKid• ALSSimulator • SimJunior• ResusciAnneSimulator • SimNewB• SimPadArrhythmiaTrainer • SimPadSoundsTrainer• SimPadBloodPressureTrainingArm
Or use with a standardised patient…..Connect SimPad to its Patient Monitor and run compelling and realistic scenarios with standardised patients extemporarily.
Laerdal ServicesLaerdal offers an extensive range of services to ensure your simulation programmes run reliably. Alongside Technical Services that include, preventive maintenance programmes and warranties, the SimPad offering also includes:
Protection Plan – to cover your investment from accidentsE-Learning – to provide you with learning support through all functions of the SimPadIntegration Course – to ensure that the full functionality of SimPad is fully optimised in all your simulation programmes
The benefits of simulation within healthcare are now widely recognised to deliver quality experiential learning and improved patient care. While its acceptance as a valuable educational tool is now established, some of the challenges to its integration into curricula and continuous professional development have remained. These are often due to reasons of cost, perceived complexities in the simulator’s operation or simply lack of time!
In continuous collaboration with our customers who have explored and shaped how simulation can be applied to healthcare education and practice, it is our role to seek out and develop new technologies that make simulations simple to run, realistic and repeatable in their delivery and multifarious in the learning objectives that can be facilitated - all in a tool that is affordable, durable and above all - easy to use.
So, how will SimPad make a difference?SimPad in the hands of a new user or an experienced simulator instructor is a ‘pick-up and play’ experience that will get simulations up and running more quickly and efficiently than ever before. Used with your existing range of Laerdal VitalSim Manikins or a standardised patient, its intuitive touchscreen design will open up a world of learning opportunities at your fingertips.

11
Education through Simulation News - Issue 17 - Winter 2013
SimPadA tool that when attached to a Laerdal manikin or used with a standardised patient and patient monitor, can replicate and adjust the physiological parameters of a patient in multiple scenarios by a simple touch on the SimPad screen.
Run SimPad in Manual Mode and you can deviate the scenario instantly and capture those unique learning moments as they occur.
In Automatic Mode you can run standardised scenarios for consistent delivery of learning objectives and assessment, as well as reduce your workload in running the scenario.
SimPad is a complete solution. It will elevate the learning more than you could ever have experienced from your Laerdal manikins before , because quite simply - it can do more and do it more easily. And with the Log Viewer, reflective learning can be further maximised throughpost-event quality debriefing and evaluation.
Mobile simulationLearning becomes more profound if simulation takes place in real environments. Whether it’s in the back of an Ambulance, through the doors into A&E or in the lift to the patient wards, SimPad’s portability means that learning can take place where ever it needs to.
Scenario Design is now a simple process with SimPad’s supporting software solutions: Theme Editor and SimDesigner.
Theme Editor for use in Manual Mode will enable you to create patient conditions complete with states and trends that automatically improve or deteriorate in response to treatment.
SimDesigner is a comprehensive scenario design solution for simple application to your SimPad when used in Automatic Mode. By creating patient data, scenario outlines, learner briefs, learning objectives and equipment checklists you can build your own library of learning material ready to use when you need it.
Simulation at your fingertips!
Run scenarios by manuallyoperating the patient
simulator and registeringinterventions.
Find details on battery status,connection and clock.
Run pre-programmedscenarios by simply
registering interventions.
Select a log to facilitatedebriefing with the Log Viewer.
Register SimPad on SimStoreor synchronise with
SimStore and access ready made scenarios from a
growing library of validated content from many leading
international healthcare institutions.
Adjust display brightness,clock and more.
For complete details of the Simpad system and a demonstration, please contact our Inside sales team on 01689 876634 or email [email protected]
LAERDAL MEDICAL LTD. Laerdal House, Goodmead Road, Orpington, Kent BR6 0HXTel: +44 (0)1689 876634, E-mail: [email protected]
www.laerdal.co.uk
EDUCATION T H R O U G H
NewsDates for your diary15th - 17th January 2013Combat - Humanitarian - CivilianPark Plaza, Victoria, London
8th March 2013ASPiH Laerdal National Inter-professional Paediatric Simulation SymposiumRadisson Blue Hotel, Manchester AirportContact: [email protected] for details
21st - 25th April 2013RCN Congress Exhibition 2013Liverpool Arena and Convention Centre (ACC)
25th - 26th April 2013The ASPiH SCSN SymposiumDynamic Earth, 112-116 Holyrood Road, Edinburgh EH8 8AS
16th - 17th May 2013Life Connections 2013Kettering Conference Centrewww.lifeconnections.uk.com
For more information about these meetings, please contact our Customer Service Department on 01689 876634 or [email protected]
Reader contributions
If you would like to contribute articles to this newsletter that relate to simulation we would be pleased to hear from you. Please contact: [email protected]
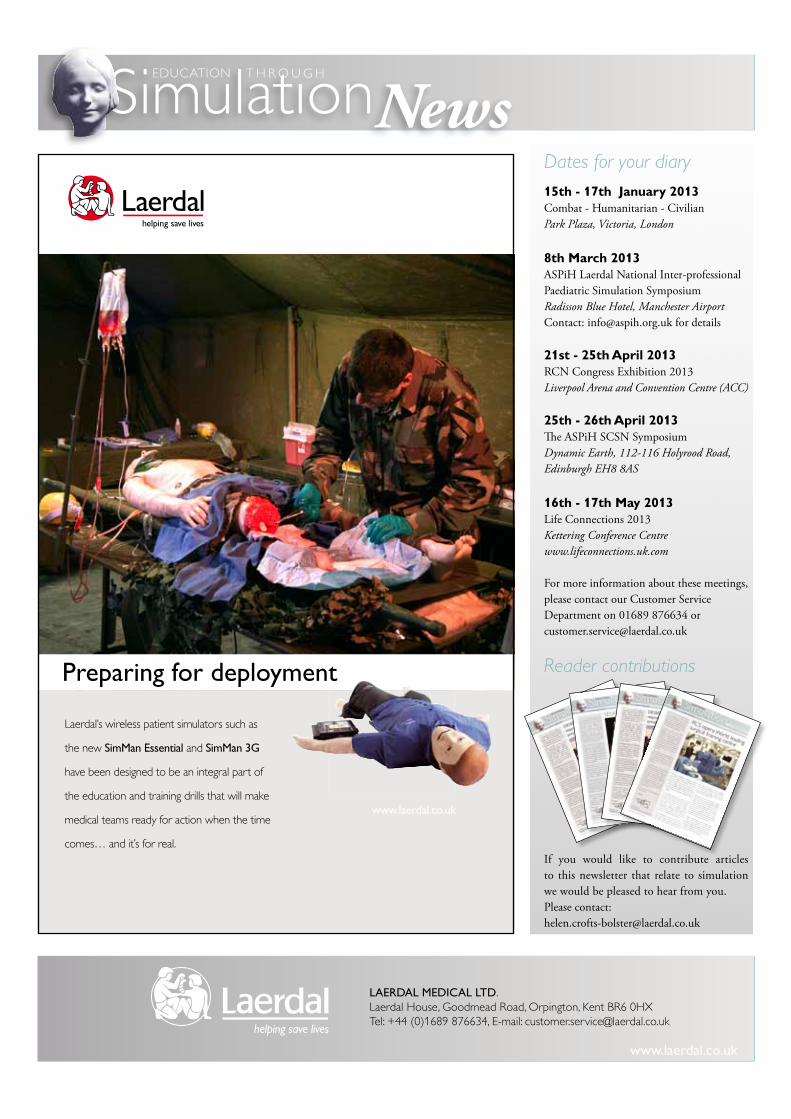
Laerdal’s wireless patient simulators such as
the new SimMan Essential and SimMan 3G
have been designed to be an integral part of
the education and training drills that will make
medical teams ready for action when the time
comes… and it’s for real.
www.laerdal.co.uk
Preparing for deployment