Embed Size (px)
Citation preview
EDUCATION NEWSNina Turcato, CRNA DNP
Cliff Roberson. CRNA MSKarl Covert, PhD
Simulation-Based Education: What's in it for NurseAnesthesia Educators?
This column presents an overview of the current stateof the art of simulation-based training. It shares theresults of a recent national survey, describing the current use of simulation technology among nurse anesthesia programs. It reviews the theoretical advantagesof simulation-based instruction. Barriers to the development of simulation in nurse anesthesia programs are
discussed, as well as strategies educators can use toovercome these challenges.
Keywords: Crisis resource management, experientiallearning, nurse anesthesia education, simulation-basedtraining.
Simulationmode Examples
low fidelity Patient actors
Simulated interViews
Table 1. Simulation Modalitiesa laerdal Medical Corporation, WappingersFalls, New Yorkb Medical Education Technologies, Inc,Sarasota, Florida
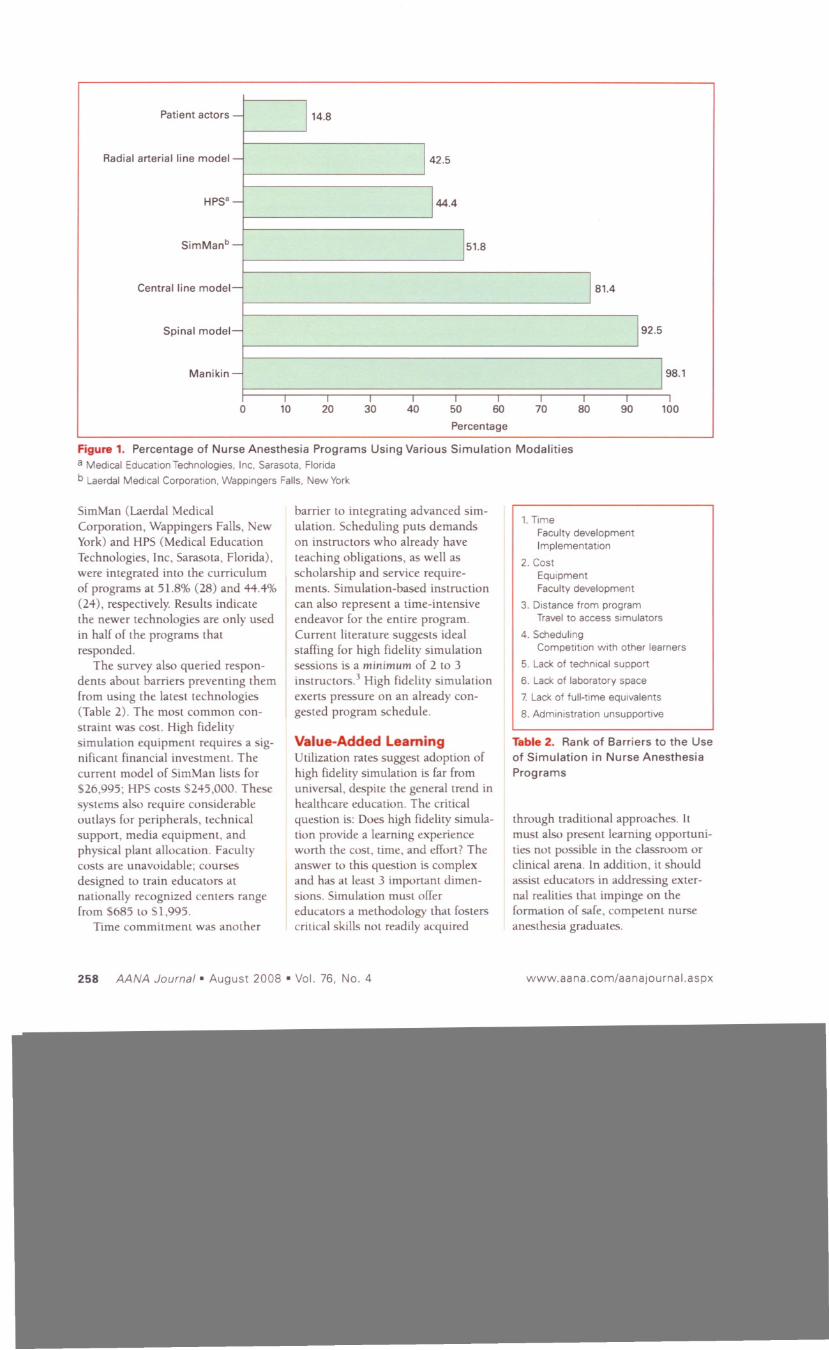
95 directors invited to participate, 52responded. Ninety-six percent (91)indicated they use some form of simulation in their curriculum. Task
trainers are frequently used acrossprograms; the most common areintubation manikins (98.1 %,52) and
spinal models (92.5%, 50). In thearea of high fidelity simulation, thereis a significant drop in program utilization rates. The 2 most widelyavailable simulation systems,
New technologies are revolutionizinghealthcare education across manydisciplines. "High fidelity" simulation now allows students to learn in
an environment representative ofactual operational conditions. Thesetools are engendering an importantparadigm shift that presents uniquechallenges to nurse anesthesia educators. This column presents anoverview of the current state of the
art of simulation-based training,results of a national survey about useof simulation technology amongnurse anesthesia programs, and abrief summary of the advantages ofsimulation as a pedagogic strategy.Barriers and strategies to overcomethem are identified, with the goal ofpromoting this tool in the educationof safe, competent nurse anesthetists.
Simulation DefinedSimulation is defined as any activitythat reproduces a task environmentwith sufficient realism to serve a
desired pedagogic goal. I The outcome for high-skill professions is toimprove student competence in both
technical and nontechnical
domains.I•2 Modalities vary fromrole-playing scenarios, to task trainers, and to high fidelity, roboticsimulation systems (Table 1).2Simulation is not new to healthcare
education, yet new technology hasallowed simulators to replicatehuman physiology in an extraordinarily realistic manner. They cannow interface with actual monitoringequipment and anesthesia machines.Learners can manage uncommonclinical scenarios or be allowed tomake errors in routine decision mak
ing and have those errors reach theirnatural conclusions. The resultallows students to learn from deci
sions without the risk of harmingpatients. I
Simulation in NurseAnesthesia ProgramsTo what extent are nurse anesthesia
educators using simulation-basedinstruction? We disseminated a sur
vey 10 program directors asking themto describe simulation modalities
they currently use (Figure I). Of the
Task trainers
High fidelity
Written problems
Intubation manikins
Invasive monitoringand spinal trainers
SimManaHPSb
www.aana.com/aa najou rna I.aspx AANA Journal· August 2008 • Vol. 76, No.4 257
Patient actors 14.8
Radial arterial line model
42.5
HPS'
44.4
SimManb
51.8
Central line model
181.4
Spinal model-J
192.5
Manikin
I
II
IIIIIIIII0
102030405060708090100
Percentage
Figure 1. Percentage of Nurse Anesthesia Programs Using Various Simulation Modalities
a Medical Education Technologies. Inc, Sarasota, Florida
b Laerdal Medical Corporation, Wappingers Falls, New York
SimMan (Laerdal Medical
Corporation, Wappingers Falls, NewYork) and HPS (Medical Education
Technologies, Inc, SarasOla, Florida),were integrated into the curriculumof programs at 51.8% (28) and 44.4%(24), respectively. Results indicatethe newer technologies are only usedin half of the programs thatresponded.
The survey also queried respondents about barriers preventing themfrom using the latest technologies(Table 2). The most common constraint was cost. High fidelitysimulation equipment requires a significant financial investment. Thecurrent model of SimMan lists for526,995; HPS costs 5245,000. Thesesystems also require considerableoutlays for peripherals, technicalsupport, media equipment. andphysical plant allocation. Facultycosts are unavoidable; courses
designed to train educators atnationally recognized centers rangefrom 5685 to 51,995.
Time commitment was another
barrier to integrating advanced simulation. Scheduling puts demandson instructors who already haveteaching obligations, as well asscholarship and service requirements. Simulation-based instruction
can also represent a time-intensiveendeavor for the entire program.Current literature suggests idealstaffing for high fidelity simulationsessions is a minimum of 2 to 3
instructors.3 High fidelity simulationexerts pressure on an already congested program schedule.
Value-Added LearningUtilization rates suggest adoption ofhigh fidelity simulation is far fromuniversal, despite the general trend inhealth care education. The critical
question is: Does high fidelity simulation provide a learning experienceworth the cost, time, and effort? The
answer to this question is complexand has at least 3 important dimensions. Simulation must offer
educators a methodology that fosterscritical skills not readily acquired
1.Time
Faculty developmentImplementation
2. Cost
EquipmentFaculty development
3. Distance from programTravel to access simulators
4. SchedulingCompetition with other learners
5. Lack of technical support
6. Lack of laboratory space
7. Lack of full-time equivalents
8. Administration unsupportive
Table 2. Rank of Barriers to the Use
of Simulation in Nurse Anesthesia
Programs
through traditional approaches. It
must also present learning opportunities not possible in the classroom orclinical arena. In addition, it shouldassist educators in addressing external realities that impinge on theformation of safe, competent nurseanesthesia graduates.
258 AANA Journal· August 2008 • Vol. 76, No.4 www.aana.com/aanajou rnal.aspx
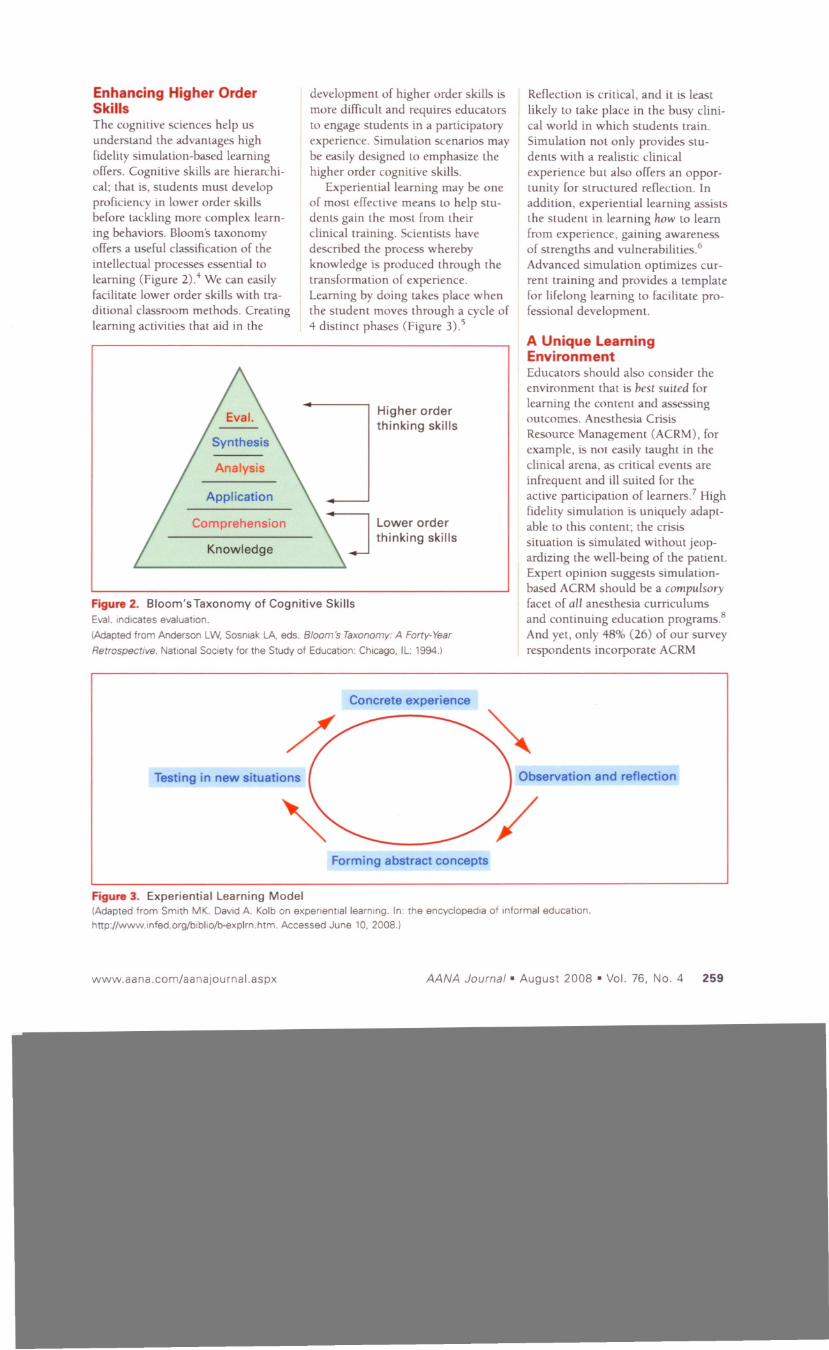
Figure 2. Bloom'sTaxonomy of Cognitive SkillsEva!. indicates evaluation.
(Adapted from Anderson LW, Sosniak LA. eds. Bloom's Taxonomy: A Forty-Year
Retrospective. National Society for the Study of Education: Chicago, IL; 1994.)
Enhancing Higher OrderSkillsThe cognitive sciences help usunderstand the advantages highfidelity simulation-based learningoffers. Cognitive skills are hierarchical; that is, students must developproficiency in lower order skillsbefore tackling more complex learning behaviors. Bloom's taxonomyoffers a useful classification of the
intellectual processes essential tolearning (Figure 2).4 We can easilyfacilitate lower order skills with tra
ditional classroom methods. Creatinglearning activities that aid in the
Analysis
Application
Comprehension
Knowledge
development of higher order skills ismore difficult and requires educatorsto engage students in a participatoryexperience. Simulation scenarios maybe easily designed to emphasize thehigher order cognitive skills.
Experiential learning may be oneof most effective means to help students gain the most from theirclinical training. Scientists havedescribed the process wherebyknowledge is produced through thetransformation of experience.Learning by doing takes place whenthe student moves through a cycle of4 distinct phases (Figure 3).5
Higher orderthinking skills
Lower order
thinking skills
Reflection is critical, and it is least
likely to take place in the busy clinical world in which students train.
Simulation not only provides students with a realistic clinical
experience but also offers an opportunity for structured reflection. Inaddition, experiential learning assiststhe student in learning how to learnfrom experience, gaining awarenessof strengths and vulnerabilities.6Advanced simulation optimizes current training and provides a templatefor lifelong learning to facilitate professional development.
A Unique LearningEnvironmentEducators should also consider theenvironment that is hest suited for
learning the content and assessingoutcomes. Anesthesia Crisis
Resource Management (ACRM), forexample, is not easily taught in theclinical arena, as critical events areinfrequent and ill suited for theactive participation of learners.7 Highfidelity simulation is uniquely adaptable to this content; the crisissituation is simulated without jeopardizing the well-being of the patient.Expert opinion suggests simulationbased ACRM should be a compulsoryfacet of all anesthesia curriculums
and continuing education programs.sAnd yet, only 48% (26) of our surveyrespondents incorporate ACRM
Concrete experience
Testing in new situations
Forming abstract concepts
Observation and reflection
Figure 3. Experiential Learning Model(Adapted from Smith MK. David A. Kolb on experientiallearnmg. In: the encyclopedia of informal education.
hnp://www.infed.org/bibliolb-explrn.htm. Accessed June 10, 2008.)
www.aana.com/aa najou rna I.aspx AANA Journal· August 2008 • Vol. 76, No.4 259

t--Dedicated course
2.0
f--
Module in
7.3existing course -Workshop
9.2
- Incorporate in
29.6various courses -Do not incorporate
51.9in curriculum
10
I310I
510600 2040
Percentage
Figure 4. Nurse Anesthesia Programs and Crisis Resource ManagementTeaching
instruction in their curriculum
(Figure 4). Of these, a little morethan a third (39%, 21) use simula
tion to teach these principles. Whilestudents can be taught how to manage critical events in a classroomsetting, it has definite limitations.ACRM with simulation can illuminate errors in care and decision
making, which can identify furthereducational needs.1
Simulation is also well suited for
assessing student clinical performance. Problem behaviors can be
identified in a realistic setting so thestudent can gain insights in a meaningful way.9 A student whose clinicalevaluations indicate the learner rou
tinely fails to exhibit due vigilanceduring cases can be placed in a simulated situation. The student's
performance can be videotaped andreviewed during the debriefingprocess. This process promotes selfawareness, helps validate clinicalissues, and permits faculty to facilitate the student's active refiection on
problem behaviors. The student andfaculty can then create a meaningfulremediation plan.
External ForcesSimulation-based teaching must support educators in addressing externalforces that have an impact on theirability to prepare graduates. One isthe shortage of nurse anesthetists. Itis estimated the demand for CRNAs
will exceed 35,000 by 2010, and thenumber of graduates may not satisfythis need.to The shortfall places pressure on educators to meet the
demand, without a correspondingincrease in the resources to do so.
Healthcare systems will have limitedpersonnel to support the clinicaltraining of students. The currentapprenticeship system has alreadybecome burdensome in the face of
newer standards of quality and efficiency in the 21st century operatingroom; a shortage of nurse anesthetists will only compound theproblem. Simulation can help educators meet some of these challenges. Itwill allow students to gain a considerable degree of mastery ofanesthesia skills befort: entering theclinical environment. High fidelitysimulation may, in fact, acceleratestudent learning. II This creates an
enormous advantage in a tight labormarket, by allowing preclinical training to promote a level of competencyunseen before and by preparing safeand competent graduates of a qualityunmatched by the current educational system.
Another external force is the
increasingly complex environment inwhich healthcare is delivered.
Perioperative services have become amore strategically important component of the financial and operationalwell-being of healthcare organizations. Clinical decision making notonly has an impact on the health andsafety of the patient but also on system function. A delayed emergence,for example, can echo throughoutthe organization in terms of cost andmanpower. The operating room staffhas evolved into a complex, multidisciplinary team that requires a highdegree of competency in interpersonal communication. Advanced
simulation-based teaching is ideal forthe instruction of the skill sets neces
sary to negotiate this environment.Scenarios may be designed to [ostersituational awareness, decision mak-
260 AANA Journal • August 2008 • Vol. 76. No.4 www.aana.com/aanajou rna I.aspx
Table 3. Goals and Strategies to Confront Barriers to High Fidelity Simulation
ing and team communication, andallow students to develop strategiesthey can apply to multiple situationsalong their professional practice continuum.12
Promotion of anesthesia safetyhas always been an important component of nurse anesthesiaeducation. In recent years it has alsobecome a significant external forcefrom an institutional and regulatoryperspective. The Institute ofMedicine has urged educators toconfront the problem of humanerror and strive to limit negativeoutcomes. 13 The Joint Commissionhas highlighted patient safety byasking providers to improve communication among caregivers. 14 Thekey question is: Does simulationbased teaching serve to reduce errorsand improve safety? The verdict isstill out, hut preliminary data arepromising. Procedural simulationstudies in surgery show intraoperative errors can be reduced with
simulation training.15 Many organizations are proceeding on theassumption that simulation doesindeed improve safety. Malpracticecarriers, recognizing the impact ofpoor team communication and crisismanagement on claims, are offeringsignificant reductions in insurancefor teams who undergo simulationbased training.16 Nurse anesthesiaeducators can make the same
assumptions in adopting simulationbased learning in their programs.
Confronting BarriersHow can educators confront the
barriers to integrating advanced simulation in their curriculum (Table
3)? Strategies begin with disseminating the merits of simulation-basededucation. Administrators must be
made aware of the growing body ofevidence suggesting simulation accelerates the speed and quality oflearning and may improve patientsafety and outcomes. Moreover, it ispoised to become a standard methodology by which programs will bejudged by prospective students and
Goal
Disseminate benefits to decision makers.
Generate enthusiasm among colleagues.
Pool resources with colleagues.
faculty, as well as accreditation agencies. Organizalions, such as theSociety of Simulation in Health Care,puhlish peer-reviewed research onthe utilization and effectiveness ofsimulation-based education across a
number of disciplines, which can bea useful source of information toshare with decision makers.
Strategies that can generateenthusiasm for simulation amongcolleagues are key. Faculty workshops can be used to educate andpersuade others to consider simulation in their curriculum. Interest can
be generated with presentations atlocal, state, regional, and nationalmeetings. While articles and casereports about simulation are anessential means of understandinghigh fidelity simulation, nothing candefine the methodology and sparkinterest better than viewing "liveclips" of simulation-based teachingscenarios. The ideal situation is to
entertain colleagues in a simulationlaboratory so they may see for themselves what it is like to be a learner.
Collaboration between nurse
anesthesia programs is essential.Mechanisms to share resources can
be negotiated among programs withgeographic or institutional similarities. i\'urse anesthesia programs
StrategiesEducate administrators.
Impart peer-reviewed state of theeVidence.
Emphasize accreditation andcertification trends.
Organize faculty informationsessions.
Tour a Simulation center.
Report simulation specific outcomedata.
Share faculty training costs.
Negotiate contracts with preexistingcenters.
Codevelop scenarios.
Create user groups.
without access to advanced simulation can share resources with those
who do hy arranging fee-for-servicecontracts and sending students toengage in specific learning activities.These arrangements can be mutuallybeneficial as students from one insti
tution are afforded meaningfullearning experiences, while the othercan use external fees to offset the
often high maintenance costs associated with high fidelity simulation.This revenue source can be essential
to a simulation center's survival, asequipment often needs to beupdated or replaced after 5 years.17
Other mechanisms for promotionof advanced simulation may involverecruitment of staff from clinicalsites to serve as simulation instruc
tors. This collaboration can solidifythe link between the simulation curriculum and the clinical arena, as
well as improve faculty workloadproblems. Links may also beextended between programs by theformation of simulation task forces,
whose goal is collaboration andsharing of resources to promote simulation among member programs.The pooling of energies can be further enhanced with external fundinggrants to support collaborativeteaching enterprises.
www.aana.com/aa najou rnal. aspx AANA Journal· August 2008 • Vol. 76, No.4 261
Interdisciplinary collaboration canalso reduce simulation costs. Strengthin numbers keeps simulation on theradar screen of administrators anddecision makers. Areas of collabora
tion may include development ofresearch projects and case scenarios.Multidisciplinary simulation usergroups also offer an opportunity toupdate faculty on policies, equipment, software, and Internet
resources. Taped learning cases canbe presented at meetings to discussthe nuts-and-bolts of advanced simu
lation teaching and learning.Members may also cross disciplinesto participate as "actors" in eachother's clinical scenarios and as facili
tators in debriefings. Cross staffingoffsets the time and costs associatedwith simulation-based instruction
throughout the institution.
SummarySimulation-based instruction can
help educators meet the challengesof training nurse anesthetists in anincreasingly complex world. It isbased on sound pedagogy that fostersthe acquisition of critical skills.Simulation allows replication notonly of the complex interplaybetween patient physiology, anesthetics and equipment but also thedynamic clinical environment inwhich students must function.
Tentative but growing evidence suggests simulation accelerates the speedand quality of student learning andmay enhance our capacity to preventhuman error. Practice may indeedmake perfect, as deliherate learningexperiences allow students to honecritical skills in an authentic learningenvironment. The creation of collab
orative alliances may help surmountthe barriers to universal use ofadvanced simulation-hased instruc
tion in our programs. Curtailment of
time and financial constraints are
essential, so that more student nurseanesthetists can be exposed to thisvaluable teaching tool and theunique and important learning experience it offers.
REFERENCESI Jha AK. Dunkan B\V, Bates DW Simulator
based training and patient safely. In'Makini: Health Care Safer: A Critical
AnalYSIS of Pallcnl Safety PraCllCCS. 200 I:511- 518 Agency for Healthcare Researchand Qualny. RockvIlk. MD.
hltp:lA\ww.ahrq .j;e>v/chmc:lptsafety/.Accessed March 25. 2008.
2 Salas E. WIlson KA. 8urke CS. Priest HA.
USing slmulalion-based training toimprove pallent safely)l Camm) Quul
Patient Sar. 2005;31(7):363-371.
3 O'Donnell J. Fletcher J. Dixon B, Palmer
L. Planning and Implememing ananestheSia cnSlS resource managememcourse for studet1l nurse aneSlhellsts.
CRNA 1998;9(2):50-58.
4 8100m B. Taxonomy of Educallonal
Objectll'CS. New York. ~Y: Longmans.Green and Co; 1956.
5 Kolb DA. Learmng and problem solVIngIn: Ke>lhDA, Ruhin 1M. McintyreJM, elal. Orgamzallonal Psych%!!;}'. 2nd edUpper Saddle RIver, NJ: Prentice-Halllnc;1974:27-42.
o F.lekmann P. Kolb A. Kolb O. ManagIng asDesigning: Creanng a New Vocahulary forManagement Educanon and Research.Cleveland, OH: Case Western Reserve
Umversity, OH. June 14-15.2002.7 (;aba OM, ftsh K), I!oward 5K. CriSIS
Management m Anesrhesl%K\'. New York,NY: ChurchIll Lis~ngstone; 1994.
8 Howard SK. Gaba DM, FIsh KJ, SarnqUlstFH. AnestheSia cnsls resource
management traInmg: teachmganestheSIOlogists to handle critical
incidents. Avtor Space Envtron Med.1992;63(9):763-770.
9 Issenberg SB. McGaghie WC. Pretrusa ER,lee Ge>rde>nD, Scalese R]. Features and
uses of hlgh-fidelny medical slmulallonsthat lead to effeCllve learnIng: a BEMEsystemane reView. /l.kd 1i'U( h.
2005;27(1): I0-28.
10. OueHene SM. Bruton-Maree N, Kohlenherg
E. Expansion of nurse anesthesia
educational programs: where are thebarners? AANAJ. 2002;70(0)-435-438
II. Ge>rde>nfA. Bmwn, DFM, Armstmng EG.Can a SImulated cnucal care encounter
accelerate basic science learning among
preclImcal medical students? A pilot study.Sunu/atlOn m Hea/rhcare. 2006;1:13-17.
12. Fletcher GC, McGeorge P. Fhn RH, GlaVInRJ, Maran NJ. The role of non-technicalskIlls in anaestheSia: a re\'lew of current
Inerature. Br) Anaesth. 2002;88(3):418429.
13. Kohn LT, Comgan JM, Donaldson MS,
eds. Commiltee on Qualny of Heahh Carein America, Institute of MediCIne. To Err is
HUnJun: Buildmg £I SuJt'r Hrulth Curt' Syslt'm
(Executive Summary). 1999. http://books.
nap edulopenbookphp?record_id=9728&page =I. Accessed January 6, 2008.
14. The Joint Commission. 2008 Nallonal
Panent Safety Goals, Hospital Program.http://wwwjOlntwmmlsslOn.orglPatientSaf
etylN anonal PatientSafet yGoalsl08 _ha p_n psg,.hlm. Acce,sed January 6, 2008.
15. Gallagher AG. Cates CU. Approval of
vinual reality trammg for carolld stenting:what this means for procedural-basedmediCIne. JAMA 2004;292(24 ):302of-1026.
16. ~cCarthy J. Cooper JB. MalpracnceInsurance Carner ProVIdes PremIUm
IncentIve for Simulation-8ased TramIngand Believes It lIas Made a DIfference.
Anesthesia Patient Safety Foundation
News/ella Spring 2007;22( 1).17.
17. Schaefer JJ III Cost of TechnologyDifferenceslSimulatie>n. Pre>ented at:
AANA Assembly of School Faculty,Orlando. FL. Fehruary 24, 2007.
AUTHORSNina TurcaLO, CR~A, D~P' IS director at theSchool of ~urse Aneslhesla, University of NewEngland. Portland. MaIne. Email: [email protected].
ClIff Roberson, CRNA, MS. IS assistantdirecLOr, School of Nurse Anesthesia, Universityof New England. Portland, MaIne. Ematl:[email protected].
Karl Covert, PhO, IS adjunct professl\r at theUmverslty of New England. Portland, MaIne.
ACKNOWLEDGMENTSWe thank the followmg: Margaret Fallt-Callahan, CRNA, DNSc, FAA~, Rush UmversJly College of NursIng Nurse Anesthesia Program, forher mentorshlp; the AANA f'"undation f,'rfundIng Nina TurcaLOs doctoral work on simulation-based education In the New Englandarea; James Botkin, PhD, Botkin Chemie, forassistance With data presentation.
262 AANA Journal· August 2008 • Vol. 76. NO.4 www.aana.com/aanajourna I,aspx

























![COMPUTER SIMULATION AND ARENA SOFTWARE - Benvenuti su [email protected]](https://img.pdfslide.us/doc/110x75/613d4b98736caf36b75ba337/computer-simulation-and-arena-software-benvenuti-su-emailprotected.jpg)



