Embed Size (px)
DESCRIPTION
Johns Hopkins University Department of Biomedical Engineering. Education and Promotion of Translational Biomedical Engineering I Entrepreneurship and Product Development Programs: Emerging Best Practices CBID: A New Model for Academic-Based Medtech Innovation and Global Health Innovation - PowerPoint PPT Presentation
Citation preview

Education and Promotion of Translational Biomedical Engineering IEntrepreneurship and Product Development Programs:
Emerging Best Practices
CBID: A New Model for Academic-Based Medtech Innovation and Global Health Innovation
Youseph YazdiExecutive Director
BMES Annual MeetingHartford ~ October 13, 2011
Johns Hopkins UniversityDepartment of
Biomedical Engineering

the education and development of
the next generation of leaders in healthcare innovation
and
the creation and early-stage development of
healthcare solutions that have a transformational impact
on human health around the world.
~
Our key measure of success is the positive impact
our students and our technologies
have on the quality and accessibility of healthcare.
CBID’s Mission,2 Key Elements

=+
Industry and Government Partners+
talented leaders and high impact innovations

not bench to bedside
bedside to bench to bedside
Our Approach
not tech transfer
inno
vatio
n pa
rtne
rshi
ps

Undergraduate Design Teams Program is 10 years old12 Teams x 5-8 students / team hand-picked team leaders and teams
New 1-Year Biodesign MSEfirst class graduated May 2010121516 students4 teams of 4 “Developed World” Innovation4 teams of 4 “Global Health” Innovation
Synergistic Undergraduate and Graduate Programs

IMPLEMENT
IDENTIFY
INVENT
o Objective: Ensure every Design Team project has high potential
o Over Summer and Early Fallo Identification and Validation of Medical Need
Intensive clinical rotations Clinical immersion, observations, interviews
o Assessment of Commercial Viabilityo Input from internal and external expertso From ~ 900 potential projects one per teamo Team Formed, including Clinician Mentor
Three Key Stages of 1-Year CBID MSE Program

Cardiology Gastroenterology General Surgery Interventional Radiology Neurosurgery
Orthopedic Surgery Obstetrics & Gynecology Ophthalmology Otolaryngology Urology
Clinical Immersions: Observation, Needs Identification
At Johns Hopkins School of Medicine (June, July)
International Rotations (August) India, Nepal, Tanzania, Ethiopia 3 weeks, 1 site per team Rural clinics and hospitals
new Global Health Innovation Program

CBID Clinical Immersion Program educates both students and clinicians generates clinical intuition in engineers develops collaborative skills essential to
successful design teams identifies and assesses medtech
innovation opportunities launches partnerships creates goodwill and working model for
future MSE classes

~900 raw needs
observations
48
2416 in-depth opportunity briefs
1 project per team
Clinician feedback/ Screening
Clinical Impact Analysis & Validation
Prelim Technical FeasibilityAssessment
Prelim. Commercial & Market Assessments
Careful filtering process with early stakeholder input
Clinician Immersion
June - July September

Design Team:Core + Support
4 Students2 Clinicians
1 Faculty
Regulators Mock 513g sessions Mock IDE reviews 8-wk summer
course
Non-core Clinicans: access to pts and labs reviews VoC
Industry Experts mentorship of team access to corp resources
(mkt data, prototyping, funds)
follow-on development
Startup Experts mentorship on startup
issues and strategy access to prof investors follow-on funding
Legal Experts: IP legal startup legal Regulatory strategy Reimbursement strat
Prof Engineering: design reviews DfM
Hosts teams in country Deployment and testing
Academics sci and tech suppl
coursework
Design Team

IMPLEMENT
IDENTIFY
INVENT
o Objective: Create and Develop a Solutiono High Clinical and Commercial Relevanceo Fall and Springo Team members research and brainstorm on a wide
range of potential solutionso Considerable input from clinician on team, plus
faculty and other advisorso Free to choose the best technology domain, not
constrained by the focus of a particular labo IP generation and reporting
Stage 2: Invent!

IMPLEMENT
IDENTIFY
INVENT
o Objective: Build! Solution + Path to Marketo Completed by May Graduationo Teams build multiple iterations of looks-like and
works-like prototypeso Refined and focused by input from wide range of
stakeholder perspectives: investment, regulatory, reimbursement, technical
o Construct business plan for a startup based on their project
Stage Three: Implement

Selected Spinouts & StartupsFrom MSE Classes of 2010 & 2011
Class of 2012: sinusitis, biofilm, joints, stenting

• Instability of the spine may require surgical interventiono Standard of Care in Lumbar Spine is Posterior Fusion with Fixationo During Fixation, Screws are Placed in Pedicles of Vertebra
• Osteoporosis causes the bones to become softo Contraindication to pedicle screw fixation systemso Pedicle screw pullout = Catastrophic Failureo Hardware failure in osteoporotic bone: 10-25%
Clinical Background

15 Hsu Komanski Luxon Martinez
Commercial Opportunity
Target Market Patients with low bone quality
undergoing spinal fusion
Annual Market Growth Osteoporosis : 1.7% increase Spinal Fusions: 7% increase
Total Market Osteoporotic spinal fusions: 90,000
(~25% of all fusions)* Total of 720,000 pedicle screws at
risk of failure Potential Revenue: $300M
1993 1996 1999 2002 20050
100000
200000
300000
400000
Spinal Fusions in the United States
YearN
umbe
r of P
roce
dure
s
*Chin et al. “Prevalence of osteoporosis in patients requiring spine surgery: incidence and significance of osteoporosis in spine disease.” Osteoporosis Int (2007) 18:1219-1224.

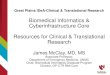
Analogous to a drywall anchor for the spine
Major Components1. Shaft – a cylindrically shaped component that
connects the other four design features.2. Lumen – an open space that provides room for
the pedicle screw to be inserted.3. Cap – a slotted head that is held in place with a
hemostat as the screw is placed.4. Hooks – projections that bridge the strong
cortical bone to the center of the pedicle.5. Wings – mechanisms that reconstruct the pedicle
by bridging the strong cortical shoulder to the center of the pedicle.
16 Hsu Komanski Luxon Martinez
Solution: The Cortical Anchor

Increases fixation by relying on hard bone instead of soft bone
Universally compatible with standard pedicles screws
Lower cost with respect to alternatives
Safer than alternatives
Designed for “on-the fly” use
Grows the spinal fusion market
17 Hsu Komanski Luxon Martinez
Competitive Advantages

Manufacturing ≈ $0.45 per anchor Pricing Points
Discussion with Experienced VC (Chris Shen) • $125 per unit ( $1,000 per procedure)
Comparables
Current Sales Price: $400 per cortical anchor
Pricing Strategy And Rationale
18 Hsu Komanski Luxon Martinez
Device or Method for Improving Spinal Fusion in Osteoporotic Bone
EstimatedCost
Kyphoplasty Kit (Bone Cement) $3500 per level
Expandable Screws $4200 per level
Extend the Fusion (Additional Hardware) $2000 per add’l level
Laminar Hooks, Clasps, etc. $1600 per level
Average Cost $2825 per level"FAQs." Parallax Medical - Devices for Spine Procedures, Vertebroplasty, Bone Biopsy Needles, Bone Cement, Acrylic Resin with Opacifiers . Web. <http://www.parallax-medical.com/index.php?pageId=49>.“; Interview with Alphatec Engineer at NASS Conference." Personal interview. 13 Nov. 2009. ; E. Cuartas et al. “Use of All-pedicle-screw Constructs in the Treatment of Adolescent Idiopathic Scoliosis.“ J Am Acad Orthop Surg. 2009 Sep;17(9):550-61.

Three aspects of reimbursement: Coding, Coverage, Payment
Instrumentation for Spinal Fusion Lump Sum Reimbursement
Relevant Coding for Spinal Fusions
19 Hsu Komanski Luxon Martinez
Reimbursement Environment and Creating Incentives
MS-DRG MS-DRG Description EstimatedBase Payment (CMS)
459 Spinal Fusion Except Cervical with MCC $33,086
460 Spinal Fusion Except Cervical without MCC $19,771
Source: Reimbursement and Coding Reference Guide. Zimmer Spine. Zimmer, Inc., 1 Jan. 2009. Web. <http://www.zimmer.com/web/enUS/pdf/ Dynesys_Family_of_Products_Coding_Reference_Guide_080409.pdf>.
CPT CPT Code Description EstimatedBase Payment
22840 Posterior Non-Segmental Instrumentation $749
22942-22844 Posterior Multi-Segmental Instrumentation $750
Source: Vaught, Margie S., Blair C. Filler, and M. B. Henley. "Coding spinal procedures: Part II." AAOS Online Service. Web.. <http://www2.aaos.org/ aaos/archives/bulletin/oct04/code.htm>.

20 Hsu Komanski Luxon Martinez
Regulatory Environment: Substantial Equivalence Pathway
YES
YES
YES
YES
NO
NOYES

Global Health Innovation

Drivers for This New Program
Mission Critical • “Next generation of Leaders in Medtech Innovation”• How could we ignore the largest, fastest growing markets?
A Critical Skill• Frugal Design not a core skill in US-based engineers• HC costs unsustainable, skill will be in demand• A different kind of innovation challenge
Engagement and Passion• Seek impact, meaning, real value• Need is great, cries out for help• A worthy challenge
Global Health Innovation

Drivers for This New Program
Global Health Innovation
Labor Market Competition• Our graduates will be competing in a
global high-end design labor market Winning Combination:• Competence to succeed in both
advanced and lower-cost markets• Differential will loose geographic
context

Our Approach
Immersion in low-resource healthcare setting Simply cannot be appreciated back in Baltimore! Must be carefully managed to get real value just “being there” not sufficient
Training to identify and assess needs and opportunities market dynamics, and stakeholder analysis, in the local context
Field component: three weeks in duration: India, Nepal, Tanzania, Ethiopia
Experienced Partners, in Country Johns Hopkins School of Public Health, JHPIEGO, many more
Global Health Innovation

Our Approach
Development component: teams tasked develop market-appropriate novel technology solutionsproject selection by mid October, development thru May
Beyond product innovationnovel solutions + potential for significant impact + commercial
sustainability Integration into Design Mentality
Eliminate “us” vs “them” mentality bring Frugal, Value Driven, principles into mainstream design
Global Health Innovation

IMPLEMENT
IDENTIFY
INVENT Day of BirthAlliance

Global Health Innovation
AntenatalScreening Kit

Summary, CBID Practices…
Team Empowerment rigorous screening of participants so this is perceived as a high-quality endeavoro UG: hand-pick team leaders, then they choose their teamsoMSE: ability to contribute solidly technically, plus have the personality to succeed in
partnerships choose and own their projects manage their budgets, including travel keep their prize winnings, but not grants
Experienced Mentors ensures quality of content, if not delivery clinicians: Hopkins Medicine medtech VCs: Aberdare, Synergy LSP, NEA, others strategics: J&J, Medtronic, GE law firms: Hogan & Lovells, Womble Carlyle global health: Jhpiego, Laerdal Global Health technical & scientific expertise: JHU Faculty, external

Summary, CBID Practices…
Coursework Essentials regulatory reimbursement business of biomedical innovation ethics of biomed innovation (see poster) “insight informed innovation” leadership training through mentorship of UG teams, now fellows
Stakeholders on CBID Team a Medical Director a tech transfer guy external advisory board
Vision to Change Institution “skating to where the puck is going to be…” academic, healthcare, and medtech
business models are shifting should be a positive influence on the whole institution