Embed Size (px)
Citation preview
ONLINE ONLY
Effect of 2 jaw exercises on occlusal function inpatients with obstructive sleep apnea during oralappliance therapy: A randomized controlled trial
Hiroshi Ueda,a Fernanda R. Almeida,b Hui Chen,c and Alan A. Lowed
Vancouver, British Columbia, Canada
Introduction: The aim of this study was to compare the effects on objective occlusal function of 2 types of jawexercises during oral appliance therapy in patients with obstructive sleep apnea (OSA). Methods: Sixteen con-secutive subjects with snoring or OSA undergoing oral appliance therapy were included in this study; the re-sults were based on 10 patients who completed it. The patients were randomized to start with either a jigexercise or stretching movements for 1 month; after 1 month without exercise, they crossed over to the otherexercise for 1 month. An occlusal diagnostic system that consisted of a pressure-sensitive sheet and an imagescanner was used to evaluate occlusal contact area and bite force. Results: Both exercises produced signif-icant increases in occlusal contact area and bite force in the morning compared with the period of no exercise.At night, the molar region had significant improvements in occlusal contact area and bite force only duringstretching movements. We found no significant differences between the 2 exercises, but stretching move-ments tended to be more effective in the molar region, whereas the jig exercise tended to be more effectivein the anterior region. Conclusions: Jaw exercises might help relieve masticatory muscle stiffness and accel-erate the repositioning of the mandible to the normal position, in addition to inhibiting or minimizing the occlu-sal functional changes in predisposed patients. (Am J Orthod Dentofacial Orthop 2009;135:430.e1–430.e7)
Oral appliances (OAs) have been established asa lifelong treatment for patients with mild tomoderate obstructive sleep apnea (OSA) and
those with severe OSAwho refuse nasal continuous pos-itive airway pressure therapy.1,2 The aim of OA therapyis to enlarge the pharyngeal airway by repositioning themandible forward.3-5 OSA is characterized by periodicreduction or cessation of breathing due to narrowingof the upper pharyngeal airway during sleep. It is a com-mon condition with major consequences for public
From the Faculty of Dentistry, University of British Columbia, Vancouver,
British Columbia, Canada.a Postdoctoral research fellow, Division of Orthodontics, Department of Oral
Health Sciences.b Clinical assistant professor, Department of Oral Biological and Medical
Sciences.c Visiting scholar, Division of Orthodontics, Department of Oral Health Sciences.d Professor and chair, Division of Orthodontics, Department of Oral Health
Sciences.
Klearway was invented by Alan A. Lowe at the University of British Columbia.
International patents have been obtained by the University of British Columbia,
and specific licensees are assigned the rights to manufacture and distribute the
appliance worldwide.The other authors report no commercial, proprietary, or fi-
nancial interest in the products or companies described in this article.
Reprint requests to: Hiroshi Ueda, Department of Orthodontics and Craniofacial
Developmental Biology, Hiroshima University Graduate School of Biomedical
Sciences, 1-2-3 Kasumi Minami-ku, Hiroshima, Japan 734-8553; e-mail,
Submitted, March 2007; revised and accepted, November 2007.
0889-5406/$36.00
Copyright � 2009 by the American Association of Orthodontists.
doi:10.1016/j.ajodo.2007.11.027
health because of its association with morbidity6 andmortality.7
Recent studies of patients with OSA have reportedthat long-term use of OAs was accompanied by jaw dis-comfort with difficulty chewing in the morning and oc-clusal changes such as reductions in both overbite andoverjet and mesial shift of the mandibular molars.8-13
Moreover, Rose et al14 reported that a temporary bitechange in the morning after removal of the OA occursin most patients, and, in some, permanent occlusalchanges have been observed after long-term treatmentperiods. Otsuka et al15 demonstrated a significant de-crease in occlusal contact area (OCA) and bite force(BF) in posttitration OA users when compared withtheir pretreatment measurements. During OA therapy,OCA and BF were also found to be significantly smallerin the morning than in the evening.
Jaw exercise therapy has long been used to treat mas-ticatory functional disorders in dental and temporoman-dibular joint disorder clinics.16-21 However, objectivedata evaluating the effectiveness of jaw exercises onmasticatory function in OSA patients have not been col-lected. Thus, it is important to clarify the potential ef-fects of jaw exercise on occlusal function as a potentialclinical tool in OSA patients during OA therapy.
A prospective randomized crossover study was de-signed to test the hypothesis that some jaw exercisesthat can stretch and relax masticatory muscles could
430.e1

430.e2 Ueda et al American Journal of Orthodontics and Dentofacial Orthopedics
April 2009
improve occlusal function in OSA patients. Our aim wasto objectively compare the effect on occlusal function of2 types of jaw exercises during OA therapy by recordingOCA and BF with pressure-sensitive sheets.
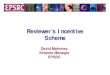
Fig 1. A titratable oral appliance (Klearway): the palatalscrew enables 44 advancements of the mandible in0.25-mm increments.
MATERIAL AND METHODS
Sixteen patients (9 men, 7 women) diagnosed with ei-ther OSA or snoring and undergoing OA therapy were re-cruited for this prospective randomized crossover study.All were referred by a physician to the Sleep Apnea Den-tal Clinic at the University of British Columbia. Patientswith inadequate dentition, periodontal disease, or tempo-romandibular joint dysfunction were excluded. Each pa-tient gave informed written consent, and the studyprotocol was approved by the Clinical Research EthicsBoard of the University of British Columbia.
All patients used the Klearway appliance (SpaceMaintainers Laboratories Canada Ltd, Vancouver, Brit-ish Columbia, Canada); the appliance design is shownin Figure 1. It is constructed of a thermoactive acrylicresin that becomes more compliant with heating. Theupper and lower portions of the appliance provide fullocclusive coverage of the teeth.22,23 Klearway also per-mits lateral and vertical jaw movements during sleep.The amount of mandibular advancement was initiallyset at two-thirds of maximum mandibular advancementand then progressively increased by a maximum of 2.0mm a month until the most effective and comfortableadvanced position was reached, snoring was reduced,or a significant reduction in symptoms was recorded.
An occlusal diagnostic system (Dental PrescaleOccluzer, Fuji Film, Tokyo, Japan), used to evaluatethe OCA and the BF, was described in previousstudies.24-28 The Dental Prescale is a horseshoe-shapedsheet with a thickness of 98 mm, wrapped with polyeth-ylene telephthalate film on both sides. Different micro-capsules in the sheets are designed to break and releasea color-forming material at various occlusal pressures.An image scanner (FPD-703, Fuji Film) can detectthe OCA indicated by the color-developing chemicalreaction. This computerized system also analyzedocclusal load quantitatively. For the occlusal functionaldata, each patient was asked to bite the sheets at thehabitual intercuspal position with maximum voluntaryclenching for 5 seconds. They were instructed andtrained by an investigator (H.U.) on how to place andclench a pressure-sensitive sheet every month. These pro-cedures were based on the method previously describedby Otsuka et al.15 The OCA and the BF were analyzedfor all maxillary teeth except the third molars. The meansand standard deviations in the total dental arch, and themolar, premolar, and anterior regions, were calculated
to evaluate occlusal function. The occlusal contact pointswere carefully verified on the dental casts.
Two types of exercises were each evaluated over a1-month period: jig exercise and stretching movements.Patients were randomized to start with either the jig ex-ercise or the stretching movements and then crossedover to the other exercise. For the jig exercise, patientswere instructed to bite on and hold a standard piece ofplastic (30 3 10 3 3 mm) between their anterior teethand slide their jaw with the largest amount of backwardand forward movement for 5 seconds each and to bitefirmly for 10 seconds at the relaxed jaw position.They were instructed to repeat these movements for 3minutes. The stretching movements exercise involvedboth vertical and lateral jaw excursions. The vertical ex-cursion had the patients opening the mandible as wideas possible and then closing it. The lateral excursionconsisted of the patients opening their jaw, sliding tothe right or left, and then returning the jaw in a circularpath to the closed position. The patients were instructedto do each exercise approximately 5 times, repeated for3 minutes.
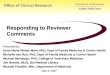
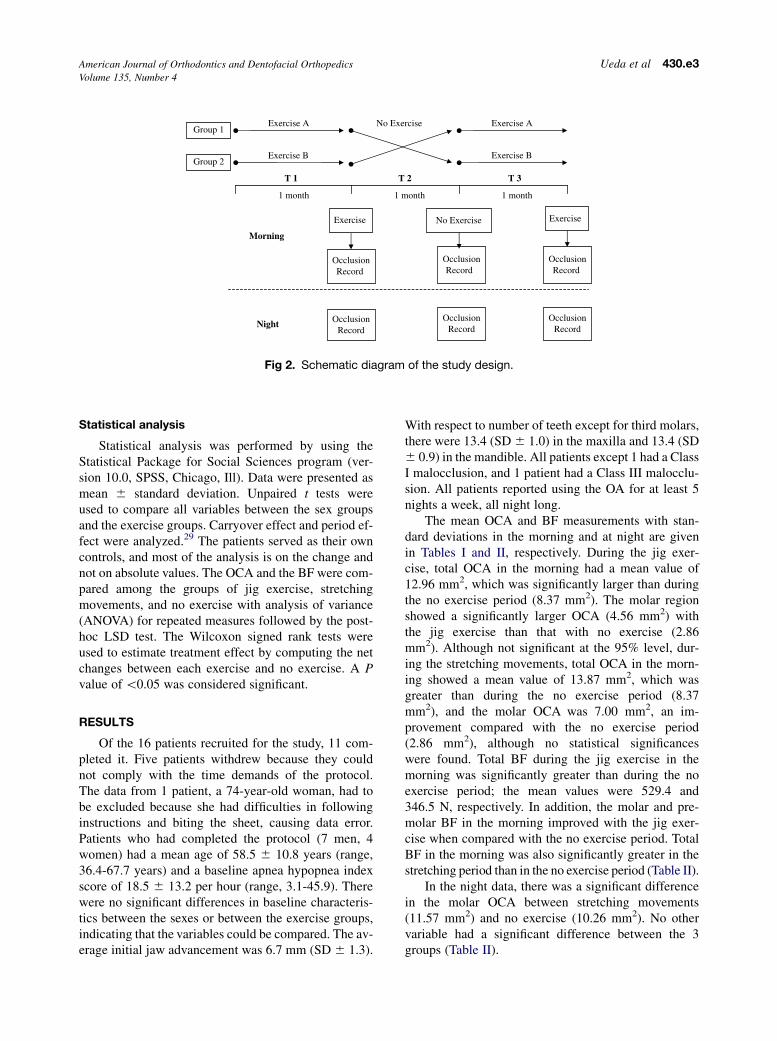
The first jaw exercise was repeated every morningfor a month (T1). Then, the patients had a 1-monthwashout period during which they were instructed notto do jaw exercises (T2). After that, they underwenta second 1-month exercise period with the other jaw ex-ercise (T3). They were seen monthly during the experi-mental period. After T1, T2, and T3, they were asked tobite a pressure-sensitive sheet in the morning after re-moving the OA and another in the evening before re-placing the OA for 3 consecutive days at home. Thesequence of treatments and evaluations is shown inFigure 2.
Exercise A
T 1
Exercise B
Group 1
Group 2
1 month 1 month 1 month
T 3T 2
Exercise B
Exercise A
Exercise Exercise
No Exercise
OcclusionRecord
Morning
Night
OcclusionRecord
OcclusionRecord
OcclusionRecord
OcclusionRecord
OcclusionRecord
No Exercise
Fig 2. Schematic diagram of the study design.
American Journal of Orthodontics and Dentofacial Orthopedics Ueda et al 430.e3Volume 135, Number 4
Statistical analysis
Statistical analysis was performed by using theStatistical Package for Social Sciences program (ver-sion 10.0, SPSS, Chicago, Ill). Data were presented asmean 6 standard deviation. Unpaired t tests wereused to compare all variables between the sex groupsand the exercise groups. Carryover effect and period ef-fect were analyzed.29 The patients served as their owncontrols, and most of the analysis is on the change andnot on absolute values. The OCA and the BF were com-pared among the groups of jig exercise, stretchingmovements, and no exercise with analysis of variance(ANOVA) for repeated measures followed by the post-hoc LSD test. The Wilcoxon signed rank tests wereused to estimate treatment effect by computing the netchanges between each exercise and no exercise. A Pvalue of \0.05 was considered significant.
RESULTS
Of the 16 patients recruited for the study, 11 com-pleted it. Five patients withdrew because they couldnot comply with the time demands of the protocol.The data from 1 patient, a 74-year-old woman, had tobe excluded because she had difficulties in followinginstructions and biting the sheet, causing data error.Patients who had completed the protocol (7 men, 4women) had a mean age of 58.5 6 10.8 years (range,36.4-67.7 years) and a baseline apnea hypopnea indexscore of 18.5 6 13.2 per hour (range, 3.1-45.9). Therewere no significant differences in baseline characteris-tics between the sexes or between the exercise groups,indicating that the variables could be compared. The av-erage initial jaw advancement was 6.7 mm (SD 6 1.3).
With respect to number of teeth except for third molars,there were 13.4 (SD 6 1.0) in the maxilla and 13.4 (SD6 0.9) in the mandible. All patients except 1 had a ClassI malocclusion, and 1 patient had a Class III malocclu-sion. All patients reported using the OA for at least 5nights a week, all night long.
The mean OCA and BF measurements with stan-dard deviations in the morning and at night are givenin Tables I and II, respectively. During the jig exer-cise, total OCA in the morning had a mean value of12.96 mm2, which was significantly larger than duringthe no exercise period (8.37 mm2). The molar regionshowed a significantly larger OCA (4.56 mm2) withthe jig exercise than that with no exercise (2.86mm2). Although not significant at the 95% level, dur-ing the stretching movements, total OCA in the morn-ing showed a mean value of 13.87 mm2, which wasgreater than during the no exercise period (8.37mm2), and the molar OCA was 7.00 mm2, an im-provement compared with the no exercise period(2.86 mm2), although no statistical significanceswere found. Total BF during the jig exercise in themorning was significantly greater than during the noexercise period; the mean values were 529.4 and346.5 N, respectively. In addition, the molar and pre-molar BF in the morning improved with the jig exer-cise when compared with the no exercise period. TotalBF in the morning was also significantly greater in thestretching period than in the no exercise period (Table II).
In the night data, there was a significant differencein the molar OCA between stretching movements(11.57 mm2) and no exercise (10.26 mm2). No othervariable had a significant difference between the 3groups (Table II).
No.1 (Class III)
No.2 (Class I)
No.3 (Class I)
No.4 (Class I)
No.5 (Class I)
No.6 (Class I)
No.7 (Class I)
No.8 (Class I)
No.9 (Class I)
No.10 (Class I)
mean
Morning OCA
Night OCA
Morning BF
Night BF
0
10
20
30
40
50
60
0
500
1000
1500
2000
0
500
1000
1500
StretchingMovements
NoExercise
JigExercise
StretchingMovements
NoExercise
JigExercise
(A) (C)
(D)
(mm2 )
StretchingMovements
NoExercise
JigExercise
StretchingMovements
NoExercise
JigExercise
(N)
(N )
0
10
20
30
40
50
60
70
(B)
(mm2 )
††
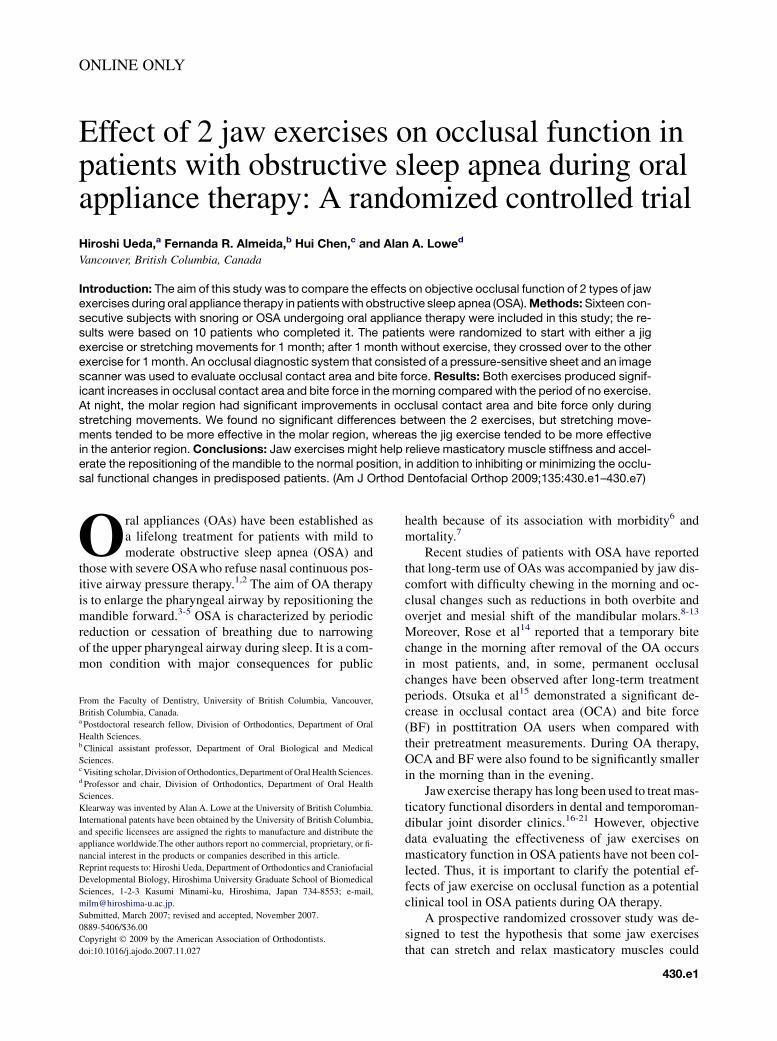
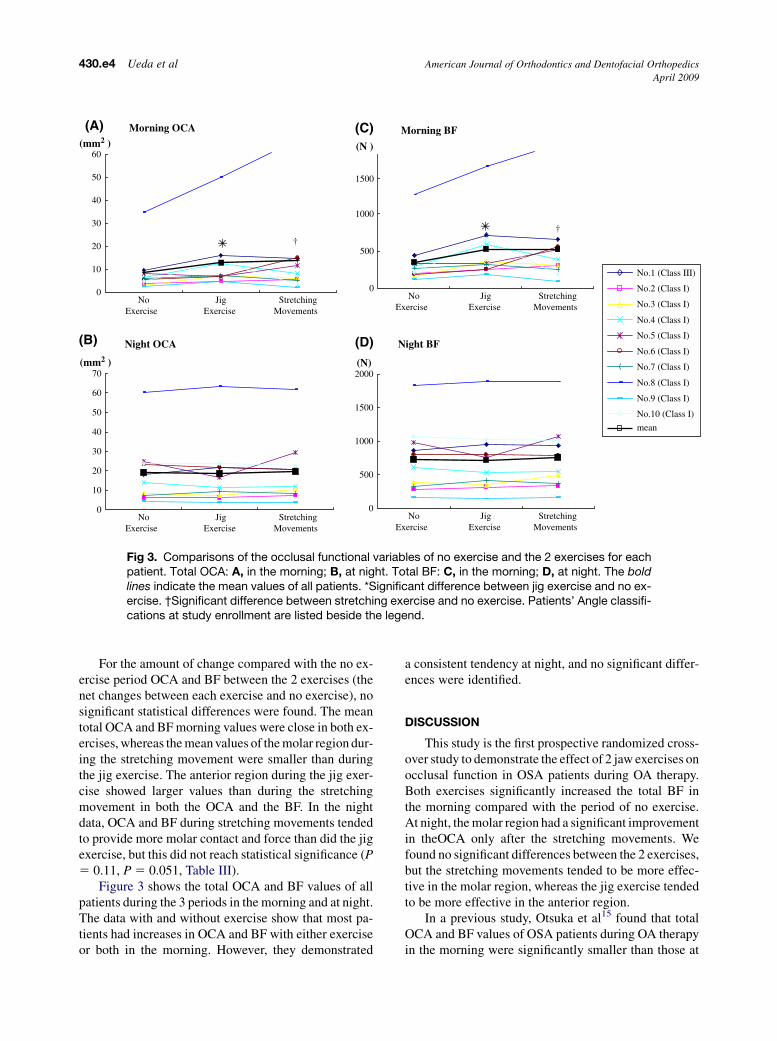
Fig 3. Comparisons of the occlusal functional variables of no exercise and the 2 exercises for eachpatient. Total OCA: A, in the morning; B, at night. Total BF: C, in the morning; D, at night. The boldlines indicate the mean values of all patients. *Significant difference between jig exercise and no ex-ercise. †Significant difference between stretching exercise and no exercise. Patients’ Angle classifi-cations at study enrollment are listed beside the legend.
430.e4 Ueda et al American Journal of Orthodontics and Dentofacial Orthopedics
April 2009
For the amount of change compared with the no ex-ercise period OCA and BF between the 2 exercises (thenet changes between each exercise and no exercise), nosignificant statistical differences were found. The meantotal OCA and BF morning values were close in both ex-ercises, whereas the mean values of the molar region dur-ing the stretching movement were smaller than duringthe jig exercise. The anterior region during the jig exer-cise showed larger values than during the stretchingmovement in both the OCA and the BF. In the nightdata, OCA and BF during stretching movements tendedto provide more molar contact and force than did the jigexercise, but this did not reach statistical significance (P5 0.11, P 5 0.051, Table III).
Figure 3 shows the total OCA and BF values of allpatients during the 3 periods in the morning and at night.The data with and without exercise show that most pa-tients had increases in OCA and BF with either exerciseor both in the morning. However, they demonstrated
a consistent tendency at night, and no significant differ-ences were identified.
DISCUSSION
This study is the first prospective randomized cross-over study to demonstrate the effect of 2 jaw exercises onocclusal function in OSA patients during OA therapy.Both exercises significantly increased the total BF inthe morning compared with the period of no exercise.At night, the molar region had a significant improvementin theOCA only after the stretching movements. Wefound no significant differences between the 2 exercises,but the stretching movements tended to be more effec-tive in the molar region, whereas the jig exercise tendedto be more effective in the anterior region.
In a previous study, Otsuka et al15 found that totalOCA and BF values of OSA patients during OA therapyin the morning were significantly smaller than those at
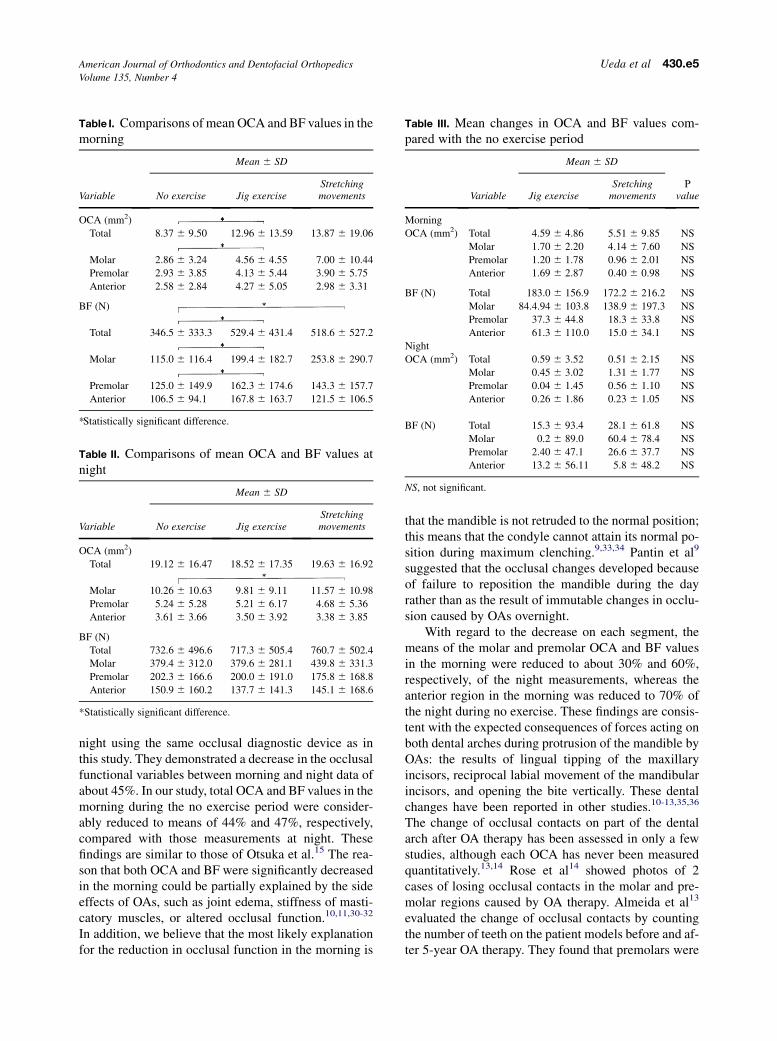
Table I. Comparisons of mean OCA and BF values in themorning
Mean 6 SD
Variable No exercise Jig exerciseStretchingmovements
OCA (mm2)
Total 8.37 6 9.50 12.96 6 13.59 13.87 6 19.06
Molar 2.86 6 3.24 4.56 6 4.55 7.00 6 10.44
Premolar 2.93 6 3.85 4.13 6 5.44 3.90 6 5.75
Anterior 2.58 6 2.84 4.27 6 5.05 2.98 6 3.31
BF (N)
Total 346.5 6 333.3 529.4 6 431.4 518.6 6 527.2
Molar 115.0 6 116.4 199.4 6 182.7 253.8 6 290.7
Premolar 125.0 6 149.9 162.3 6 174.6 143.3 6 157.7
Anterior 106.5 6 94.1 167.8 6 163.7 121.5 6 106.5
*Statistically significant difference.
Table II. Comparisons of mean OCA and BF values atnight
Mean 6 SD
Variable No exercise Jig exerciseStretchingmovements
OCA (mm2)
Total 19.12 6 16.47 18.52 6 17.35 19.63 6 16.92
Molar 10.26 6 10.63 9.81 6 9.11 11.57 6 10.98
Premolar 5.24 6 5.28 5.21 6 6.17 4.68 6 5.36
Anterior 3.61 6 3.66 3.50 6 3.92 3.38 6 3.85
BF (N)
Total 732.6 6 496.6 717.3 6 505.4 760.7 6 502.4
Molar 379.4 6 312.0 379.6 6 281.1 439.8 6 331.3
Premolar 202.3 6 166.6 200.0 6 191.0 175.8 6 168.8
Anterior 150.9 6 160.2 137.7 6 141.3 145.1 6 168.6
*Statistically significant difference.
Table III. Mean changes in OCA and BF values com-pared with the no exercise period
Mean 6 SD
Variable Jig exerciseSretching
movementsP
value
Morning
OCA (mm2) Total 4.59 6 4.86 5.51 6 9.85 NS
Molar 1.70 6 2.20 4.14 6 7.60 NS
Premolar 1.20 6 1.78 0.96 6 2.01 NS
Anterior 1.69 6 2.87 0.40 6 0.98 NS
BF (N) Total 183.0 6 156.9 172.2 6 216.2 NS
Molar 84.4.94 6 103.8 138.9 6 197.3 NS
Premolar 37.3 6 44.8 18.3 6 33.8 NS
Anterior 61.3 6 110.0 15.0 6 34.1 NS
Night
OCA (mm2) Total �0.59 6 3.52 0.51 6 2.15 NS
Molar �0.45 6 3.02 1.31 6 1.77 NS
Premolar �0.04 6 1.45 �0.56 6 1.10 NS
Anterior �0.26 6 1.86 �0.23 6 1.05 NS
BF (N) Total �15.3 6 93.4 28.1 6 61.8 NS
Molar 0.2 6 89.0 60.4 6 78.4 NS
Premolar �2.40 6 47.1 �26.6 6 37.7 NS
Anterior �13.2 6 56.11 �5.8 6 48.2 NS
NS, not significant.
American Journal of Orthodontics and Dentofacial Orthopedics Ueda et al 430.e5Volume 135, Number 4
night using the same occlusal diagnostic device as inthis study. They demonstrated a decrease in the occlusalfunctional variables between morning and night data ofabout 45%. In our study, total OCA and BF values in themorning during the no exercise period were consider-ably reduced to means of 44% and 47%, respectively,compared with those measurements at night. Thesefindings are similar to those of Otsuka et al.15 The rea-son that both OCA and BF were significantly decreasedin the morning could be partially explained by the sideeffects of OAs, such as joint edema, stiffness of masti-catory muscles, or altered occlusal function.10,11,30-32
In addition, we believe that the most likely explanationfor the reduction in occlusal function in the morning is
that the mandible is not retruded to the normal position;this means that the condyle cannot attain its normal po-sition during maximum clenching.9,33,34 Pantin et al9
suggested that the occlusal changes developed becauseof failure to reposition the mandible during the dayrather than as the result of immutable changes in occlu-sion caused by OAs overnight.
With regard to the decrease on each segment, themeans of the molar and premolar OCA and BF valuesin the morning were reduced to about 30% and 60%,respectively, of the night measurements, whereas theanterior region in the morning was reduced to 70% ofthe night during no exercise. These findings are consis-tent with the expected consequences of forces acting onboth dental arches during protrusion of the mandible byOAs: the results of lingual tipping of the maxillaryincisors, reciprocal labial movement of the mandibularincisors, and opening the bite vertically. These dentalchanges have been reported in other studies.10-13,35,36
The change of occlusal contacts on part of the dentalarch after OA therapy has been assessed in only a fewstudies, although each OCA has never been measuredquantitatively.13,14 Rose et al14 showed photos of 2cases of losing occlusal contacts in the molar and pre-molar regions caused by OA therapy. Almeida et al13
evaluated the change of occlusal contacts by countingthe number of teeth on the patient models before and af-ter 5-year OA therapy. They found that premolars were

430.e6 Ueda et al American Journal of Orthodontics and Dentofacial Orthopedics
April 2009
often in open-bite relationships. Our results of OCA canqualitatively support the significant dental changesdescribed in previous studies.
The effectiveness of remedial exercise has beenmentioned in a few previous studies, even though actualquantitative data were not provided. George33 advisedOA patients to clench their teeth isometrically 3 timesfor 6 seconds shortly after awakening. He speculatedthat the reason the bite did not feel right on awakeningmight be because the condyle was held forward by thepartially contracted inferior lateral pterygoid muscle,and firm chewing exercise could resolve the problem.In this study, we used 2 jaw exercises after the subjectsremoved the OA in the morning. Stretching movements,a well-known jaw exercise for patients with temporo-mandibular joint disorder, appears to be effective pri-marily by stretching and relaxing the masticatorymuscles and maintaining or increasing the jaw’s rangeof motion.37 In contrast, the jig exercise, by using the‘‘leaf gauge’’ technique of Williamson et al,16 wasused as a clinical procedure to position the mandibleto the maximum intercuspal position. Although we as-sumed that these 2 exercises might have some differencein effectiveness on the occlusal function in OA patients,no significant differences were found. However, ourdata demonstrated some interesting tendencies: stretch-ing movements tended to be more effective in the molarregion, and the jig exercise tended to be more effectivein the anterior region. In addition, for the night data,only the stretching movements showed a significant im-provement in the molar OCA; this could suggest a per-sistent efficacy of this type of jaw exercise. The patientdoes not need to bite firmly during the stretching move-ments, which is an easy exercise to relax the muscles.This exercise involves the dynamic movement of themandible and the masticatory muscles together. Suchdifferences could be attributed to a longer effect in themolar OCA. We speculated that the jig exercise couldplay a considerable role on the anterior teeth, becauseof holding the jig between the maxillary and mandibularincisors during the exercise, and have a fast-acting effecton the bite in the morning.
This study has certain limitations because the samplesize was relatively small, and not all patients completedthe study. One patient failed to bite the sheets as in-structed, and 4 patients dropped out. Interestingly, onewho had slight jaw stiffness after using an OA refusedthe no exercise period because his first exercise, the jigexercise relieved his jaw discomfort. Even in this smallsample, most patients had improved occlusal functionwith either jaw exercise or both in the morning. There-fore, we believe our hypothesis can be accepted basedon the results. A recently developed occlusal function
measurement system, consisting of a pressure-sensitivesheet and an image scanner, was used in this study.24-28
The OCA and the BF on the teeth were measured by us-ing a polyester sheet that was flexible, permitted naturalocclusion, and prevented mandibular displacement dur-ing clenching because of its 98-mm thickness. BF mea-surements have traditionally been limited byinstrumentation. Strain-gauge transducers have gener-ally been used for evaluating BF in most previous stud-ies.38-40 These devices open the interocclusal spacebecause of their thickness under the experimental condi-tion that never reproduced the true maximum intercuspalposition. Conversely, the bite sheet in this study was thin,and the patients could put both jaws together in a com-fortable position while biting it. Therefore, our findingsmore accurately compare differences in the samepatient. Since we prospectively studied the same patientand maximum intercuspation was easily achieved, anydifference should be minimal throughout the varioustesting events.
CONCLUSIONS
This prospective study, carried out among partici-pants of a randomized crossover trial, compared the ef-fectiveness of 2 jaw exercises on occlusal function inOSA patients during OA therapy. Despite the limita-tion of the small number of patients, it appears thatjaw exercises can help to relieve masticatory musclestiffness and accelerate the repositioning of the mandi-ble to the normal position, in addition to minimizingthe occlusal functional change in predisposed patients.Because the adverse events affecting occlusal functionwere considered minor compared with the positiveeffects on sleep-disordered breathing, the therapeuticeffects of OAs are well accepted. However, since treat-ment of OSA with OAs might be a lifelong process,possible dental side effects should be identified whenconsidering OA therapy. Consequently, a further inves-tigation focusing on preventing the decline in occlusalfunction and the long-term effects of the jaw exerciseshould be attempted.
We thank Ingrid Ellis for her editorial assistance,Mary Wong for her assistance with the statistical analy-sis, and Alan Hannam at the University of British Co-lumbia for his advice on the Dental Prescale Occluzer.
REFERENCES
1. American Sleep Disorders Association. Practice parameters for
the treatment of snoring and obstructive sleep apnea with oral ap-
pliances. An American Sleep Disorders Association report. Sleep
1995;18:511-3.
2. Mehta A, Qian J, Petocz P, Darendeliler MA, Cistulli PA. A ran-
domized, controlled study of a mandibular advancement splint for

American Journal of Orthodontics and Dentofacial Orthopedics Ueda et al 430.e7Volume 135, Number 4
obstructive sleep apnea. Am J Respir Crit Care Med 2001;163:
1457-61.
3. Ryan CF, Love LL, Peat D, Fleetham JA, Lowe AA. Mandibular
advancement oral appliance therapy for obstructive sleep apnoea:
effect on awake caliber of the velopharynx. Thorax 1999;54:972-7.
4. Kato J, Isono S, Tanaka A, Watanabe T, Araki D, Tanzawa H, et al.
Dose-dependent effects of mandibular advancement on pharyn-
geal mechanics and nocturnal oxygenation in patients with
sleep-disordered breathing. Chest 2000;117:1065-72.
5. Tsuiki S, Hiyama S, Ono T, Imamura N, Ishiwata Y, Kuroda T,
et al. Effects of a titratable oral appliance therapy on supine air-
way size in awake non-apneic individuals. Sleep 2001;24:554-60.
6. Strohl KP, Redline S. Recognition of obstructive sleep apnea. Am
J Respir Crit Care Med 1996;154:279-89.
7. He J, Kryger MH, Zorick FJ, Conway W, Roth T. Mortality and
apnea index in obstructive sleep apnea. Experience in 385 male
patients. Chest 1988;94:9-14.
8. Bondemark L. Does 2 years’ nocturnal treatment with a mandibu-
lar advancement splint in adult patients with snoring and OSAS
cause a change in the posture of the mandible? Am J Orthod Den-
tofacial Orthop 1999;116:621-8.
9. Pantin CC, Hillman DR, Tennant M. Dental side effects of an oral
device to treat snoring and obstructive sleep apnea. Sleep 1999;
22:237-40.
10. Fritsch KM, Iseli A, Russi EW, Bloch KE. Side effects of mandib-
ular advancement devices for sleep apnea treatment. Am J Respir
Crit Care Med 2001;164:813-8.
11. Marklund M, Franklin KA, Persson M. Orthodontic side-effects
of mandibular advancement devices during treatment of snoring
and sleep apnoea. Eur J Orthod 2001;23:135-44.
12. Almeida FR, Lowe AA, Sung JO, Tsuiki S, Otsuka R. Long-term
sequellae of oral appliance therapy in obstructive sleep apnea pa-
tients: part 1. Cephalometric analysis. Am J Orthod Dentofacial
Orthop 2006;129:195-204.
13. Almeida FR, Lowe AA, Otsuka R, Fastlicht S, Farbood M,
Tsuiki S. Long-term sequellae of oral appliance therapy in ob-
structive sleep apnea patients: part 2. Study-model analysis. Am
J Orthod Dentofacial Orthop 2006;129:205-13.
14. Rose EC, Schnegelsberg C, Staats R, Jonas IE. Occlusal side ef-
fects caused by a mandibular advancement appliance in patients
with obstructive sleep apnea. Angle Orthod 2001;71:452-60.
15. Otsuka R, Almeida FR, Lowe AA. The effects of oral appliance
therapy on occlusal function in patients with obstructive sleep
apnea: a short-term prospective study. Am J Orthod Dentofacial
Orthop 2007;131:176-83.
16. Williamson EH, Steinke RM, Morse PK, Swift TR. Centric rela-
tion: a comparison of muscle-determined position and operator
guidance. Am J Orthod 1980;77:133-45.
17. Tegelberg A, Kopp S. Short-term effect of physical training on
temporomandibular joint disorder in individuals with rheumatoid
arthritis and ankylosing spondylitis. Acta Odontol Scand 1988;46:
49-56.
18. Hickman DM, Cramer R, Stauber WT. The effect of four jaw
relations on electromyographic activity in human masticatory
muscles. Arch Oral Biol 1993;38:261-4.
19. Braun S, Marcotte MR, Freudenthaler JW, Honigle K. An evalua-
tion of condyle position in centric relation obtained by manipula-
tion of the mandible with and without leaf gauge deprogramming.
Am J Orthod Dentofacial Orthop 1997;111:34-7.
20. Magnusson T, Syren M. Therapeutic jaw exercise and interocclusal
appliance therapy: a comparison between two common treatments
of temporomandibular disorders. Swed Dent 1999;23:27-37.
21. Nicolakis P, Erdogmus B, Kopf A, Nikolakis M, Piehslinger E.
Effectiveness of exercise therapy in patients with myofascial
pain dysfunction syndrome. J Oral Rehabil 2002;29:362-8.
22. Lowe AA, Sjoholm TT, Ryan CF, Fleetham JA, Ferguson KA,
Remmers JE. Treatment, airway and compliance effects of a titrat-
able oral appliance. Sleep 2000;23(Suppl 4):S172-8.
23. Lowe AA. Oral appliances for sleep breathing disorders. In:
Kryger MH, Roth T, Dement WC, editors. Principles and prac-
tice of sleep medicine. 3rd ed. Philadelphia: W.B. Saunders;
2000. p. 929-39.
24. Matsui Y, Ohno K, Michi K, Suzuki Y, Hirose K, Yamagata K. A
computerized method for evaluating balance of occlusal load. J
Oral Rehabil 1996;23:530-5.
25. Miura H, Araki Y, Hirai T, Isogai E, Hirose K, Umenai T. Evalu-
ation of chewing activity in the elderly person. J Oral Rehabil
1998;25:190-3.
26. Hidaka O, Iwasaki M, Saito M, Morimoto T. Influence of clench-
ing intensity on bite force balance, occlusal contact area, and
average bite pressure. J Dent Res 1999;78:1336-44.
27. Miura H, Watanabe S, Isogai E, Miura K. Comparison of maxi-
mum bite force and dentate status between healthy and frail
elderly persons. J Oral Rehabil 2001;28:592-5.
28. Sultana MH, Yamada K, Hanada K. Changes in occlusal force and
occlusal contact area after active orthodontic treatment: a pilot study
using pressure-sensitive sheets. J Oral Rehabil 2002;29:484-91.
29. Everitt BS. Statistical methods for medical investigations. New
York: Oxford University Press; 1994. p. 1-96.
30. Ferguson KA, Ono T, Lowe AA, Keenan SP, Fleetham JA. A ran-
domized crossover study of an oral appliance vs nasal-continuous
positive airway pressure in the treatment of mild-moderate
obstructive sleep apnea. Chest 1996;109:1269-75.
31. Rose EC, Staats R, Virchow C Jr., Jonas IE. Occlusal and skeletal
effects of an oral appliance in the treatment of obstructive apnea.
Chest 2002;122:871-7.
32. Ringqvist M, Walker-Engstrom ML, Tegelberg A, Ringqvist I. Dental
and skeletal changes after 4 years of obstructive sleep apnea treatment
with a mandibular advancement device: a prospective, randomized
study. Am J Orthod Dentofacial Orthop 2003;124:53-60.
33. George PT. Is adjustability advantageous in mandibular advance-
ment appliance in the treatment of sleep-disordered breathing?
Sleep Breath 2001;5:139-47.
34. Fransson AMC, Tegelberg A, Johansson A, Wenneberg B. Influ-
ence of the masticatory system in treatment of obstructive sleep
apnea and snoring with a mandibular protruding device: a 2-year
follow-up. Am J Orthod Dentofacial Orthop 2004;126:687-93.
35. Fransson AMC, Tegelberg A, Svenson BAH, Lennartsson B,
Isacsson G. Influence of mandibular protruding device on airway
passages and dentofacial characteristics in obstructive sleep apnea
and snoring. Am J Orthod Dentofacial Orthop 2002;122:371-9.
36. Robertson C, Herbison P, Harkness M. Dental and occlusal
changes during mandibular advancement splint therapy in sleep
disordered patients. Eur J Orthod 2003;25:371-6.
37. Wilk BR, McCain JP. Principles and practice of temporomandib-
ular joint arthroscopy. St Louis: Mosby; 1996. p. 286-92.
38. Gibbs CH, Mahan PE, Mauderli A, Lundeen HC, Walsh EK.
Limits of human bite strength. J Prosthet Dent 1986;56:226-9.
39. Kikuchi M, Korioth TWP, Hannam AG. The association among
occlusal contacts, clenching effort, and bite force distribution in
man. J Dent Res 1997;76:1316-25.
40. Raadsheer MC, Van Eijden TMGJ, Van Ginkel FC, Prahl-
Andersen B. Contribution of jaw muscle size and craniofacial mor-
phology to human bite force magnitude. J Dent Res 1999;78:31-42.