Embed Size (px)
Citation preview


Editor in chief
M.Y.Taher
Founder Editors
Hilmy Abaza
Seham Abdel Reheem
Co-Editors
Ahmed Shawky
FathAlla Sidkey
Maher Osman
Mohamed Sharaf De Din
International Advisory Board
JP Galmiche France
A Sandeberg Sweden
X Rogiers Belgium
S Jensen Denmark
Des Verrannes France
Antonio Ascione Italy
S Brauno Italy
P Almasio Italy
National Advisory Board
Moustafa El Henawi
Amira Shams Eldin
Nabil Abdel Baki
Hoda E-Aggan
M Essam Moussa
Ahmed Bassioni
Saeid Elkyal
Abdel Fataah Hano
Khaled Madboli
Ezzat Aly
Contents Alexandria Journal of Hepatogastroenterology, Volume XIV ( III ), December 2014
------------------------------------------- Manuscript Submission: For information and to submit
manuscripts please contact the editors by e-mail at :
Disclaimer: The Publisher, the Egyptian Society of
Hepatology Gastroenterology and Infectious Diseases in
Alexandria, and Editors cannot be held responsible for errors
or any consequences arising from the use of information
contained in this journal; the views and opinions expressed
do not necessarily reflect the those of the Publisher, The
Egyptian Society of Hepatology Gastroenterology &
Infectious Diseases in Alexandria, Editors, neither dose the
publication of advertisements constitute any endorsement by
the Publisher, society, and editors of the products advertised.
Original Article:
Assessment of Health-Related Knowledge and Practices of
Patients with Peptic Ulcer
Maha Adel Salem1, Amal Samir Ahmed1, Doaa Abdelnaby
Abdelfatah1, Mohammed Mohammed Shamseya2 and Ayman
Mohammed Shamseya3 1 Department of Medical-Surgical Nursing; Faculty of Nursing, 2
Department of Clinical and Experimental Internal Medicine;
Medical Research Institute, 3 Department of Internal Medicine; Faculty of Medicine, Alexandria University.
-------------------------------------------
Original Article:
Diagnostic Potential of Osteopontin Biomarker in
Irritable Bowel Syndrome
Gihane I Khalil1 ,Hanan M. Mostafa2 &Fatma I. Dwidar3
Chemical Pathology1 &Internal Medicine2 departments, Medical
Research Institute,Biochemistry department3, Faculty of Medicine, Alexandria University
-------------------------------------------
Original Article:
Fecal Calprotectin as a Screening Parameter for Hepatic
Encephalopathy and Spontaneous Bacterial Peritonitis in
HCV Related Hepatic Cirrhosis
Mohamed Y. El Hasafy1, MD, Ahmed H. Yosry2, MD., Amany
S. Elyamany1, Eman E. Hemimi1 1Department of Medicine (Hepatobiliary Unit), Faculty of
Medicine, University of Alexandria, Alexandria, Egypt. 2Department of Clinical Pathology, Institute of Medical Research,
University of Alexandria, Alexandria, Egypt.
-------------------------------------------
Original Article:
Impact of Minimal Histological Changes in Donor Liver
on the Outcome of Living Donor Liver Transplantation
Naglaa Allam1, Wael Abdel-Razek1, Nermine Ehsan2, Asmaa
Gomaa1, Dina El-Azab2, Imam Waked1
1. Hepatology, National Liver Institute, Menoufiya University, Shebeen ElKom, Egypt.
2. Pathology, National Liver Institute, Menoufiya University,
Shebeen ElKom, Egypt
------------------------------------------- Original Article:
Study of Nosocomial Infections in Cirrhotic Patients in
Minoufiya University Hospital
Nooh M A, EL-lehleh A M,Anees S E, Zaher E M and Teima .A. * M.D Tropical medicine ** M.D Clinical pathology
-------------------------------------------
Original Article:
The Role of Serum Alpha Feto Protein Isoform 3(L3) and
Magnetic Reosonance Imaging in the Assessment of
Management of Hepatocellular Carcinoma
Mohamad Kassem1, Akram Deghady2, Nasser Abd Allah1,
Hossam Abo El Kheir1, Mohamed El Shafei3, Marwa Ibrahim1
Tropical Medicine1, Clinical and Chemical Pathology2 and
Radiodiagnosis Departments3, Faculty of Medicine, Alexandria
University.
-------------------------------------------
2
21
32
41
53
62

Original Article
Assessment of Health-Related Knowledge and Practices of Patients with Peptic
Ulcer
Maha Adel Salem1, Amal Samir Ahmed1, Doaa Abdelnaby Abdelfatah1, Mohammed Mohammed Shamseya2 and
Ayman Mohammed Shamseya3 1 Department of Medical-Surgical Nursing; Faculty of Nursing, 2 Department of Clinical and Experimental Internal
Medicine; Medical Research Institute, 3 Department of Internal Medicine; Faculty of Medicine, Alexandria University.
ABSTRACT
Peptic ulcer disease had a tremendous effect on morbidity and mortality until the last decades of the 20th century, when
epidemiological trends started to point to an impressive fall in its incidence. Two important developments were
associated with the decrease in rates of peptic ulcer disease: the discovery of effective and potent acid suppressants, and
of Helicobacter pylori. With the discovery of H pylori infection, the causes, pathogenesis, and treatment of peptic ulcer
disease have been rewritten. Despite substantial advances, this disease remains an important clinical problem, largely
because of the increasingly widespread use of non-steroidal anti-inflammatory drugs (NSAIDs), low-dose aspirin and
poor health related practices among general populations. Aim of the study: The present study aimed to, assess health
related knowledge and practice of peptic ulcer patients. This study was conducted at the Gastroenterology &
Endoscopic units, Outpatient gastroenterology clinics, and Medical gastroenterology wards at both the Main University
Hospital of Alexandria and Medical Research Institute of Alexandria.
Main Results
Epigastric pain was reported to be the commonest
beginning symptoms among peptic ulcer patients.
Description of epigastric pain was reported to be
in the form of heartburn for 65.3% of patients,
while pain was increased by eating in 42.0% of
patients and awaken patients from sleep 26.7%.
As regards patients’ knowledge related to peptic
ulcer disease, the majority of the subjects 81.3%
had poor total knowledge scores. Statistically
significant differences were found between the
patient’s level of knowledge score and their
socioeconomic characteristics related to age; for
the favor of patients whose age ranged between
20-30 years old. Statistically significant
differences were found between the patient’s level
of knowledge score and their socioeconomic
characteristic occupation; for the favor of patients
who were students and office worker. Statistically
significant differences were found between the
patient’s level of knowledge score and their
socioeconomic characteristic area of residence;
for the favor of patients who were resident at
urban area. Statistically significant differences
were found between the patient’s level of
knowledge score and their socioeconomic
characteristic education degree; for the favor of
patients with high or secondary education. In
relation to patients’ health related practices,
regarding nutrition, more than half of the studied
patients were complaining of loss of appetite, also
more than half of them preferred fatty foods,
added salt to make food tasty, preferred frying and
foundry way of cooking. 52 % of the patients
followed low salt and low fat diet for peptic ulcer
disease, while 20.0% of them avoid any food
contains (fat, spices, acidic foods, soft drink, and
caffeine) because of peptic ulcer. In addition, it
was found that nearly one third of the studied
patients had or sometimes had sleeping problems.
The majority of them were having disturbed
sleeping. For the majority of patients, the main
cause for sleeping problems was epigastric pain.
For managing epigastric pain, more than one third
of the studied patients did nothing, while more
than one-fifth of them were drinking cold milk
and more than one fifth were taking analgesic,
while 9.5% of patients were taking antacid drugs.
As for exercise and daily physical activities,
46.0% of the studied patients reported 6-10hrs of
working daily, 42.4 of them reported muscular
work, and 66.9% of the subjects reported a
negative impact of peptic ulcer on their work.
Also, it was found that, the majority of the studied
patients were not practicing any type of exercise.
The majority of subjects 82.0% were drinking
(tea, coffee); actually 66.7% of them reported a
negative impact of these drinks on pain incidence.

Regarding smoking, 58.7% of the studied patients
were not smoking while 29.3% of them were
smoking and 12% of them were previous
smokers. In addition, more than half of the studied
patients mentioned that they were complaining of
psychological stress, 22.7% of them were
resorting to smoking for managing this problem,
while 19.3% of them isolate themselves. On the
other hand 14.0%, 14.7% of patients were taking
enough sleep & rest and were communicating
with a close relative, respectively. While, 21.3%
of the studied patients were doing nothing. In
relation to prescribed medications, 47.3% of the
studied patients knew the medication they take by
name, more than half of them were taking the
medication on its time; it was obvious that slightly
less than half of patients were feeling better when
they took prescribed medications. Concerning non
prescribed medications, results indicated that,
16.7% of the studied patients were taking
medication without doctor prescription, the
highest proportion, for this non prescribed
medication was mainly for pain relievers such as
aspirin, ibuprofen, and diclofenac. Concerning
compliance with therapeutic regimen, the majority
of the studied patients did not go to a doctor on a
regular base, while 10% of them were sometimes
doing it and only 14.7% who did on a regular
base. Concerning to compliance with the regimen
prescribed by a doctor, 60.0% of the studied
patients were supposed to comply with the
regimen prescribed by a doctor while 40.0
weren’t.
Introduction
Peptic ulcer disease (PUD) is one of the most
common disorders in the world, accounting for a
significant portion of visits to medical providers.(1)
Over the last two decades, significant advances
have been made in understanding the
pathophysiology of PUD.(2) Peptic ulcer disease
represented a major threat to the world’s
population over the past two centuries, with a high
morbidity and substantial mortality.(3) It is defects
in the gastric or duodenal mucosa that extend
through the muscularis mucosa. It has a
significant change in its incidence, detection,
treatment, and mortality.(4). Peptic ulcers are a
very common condition worldwide. (5)
Approximately 500,000 to 850,000 new cases are
reported each year, with 5 million people affected
in the United States alone.(6-8) In Egypt, the
incidence rate of PUD is approximately 1 million
people annually(6), with 1077 deaths per year.(9)
The incidence rate of PUD in other countries is
variable and is determined primarily by
association with the major causes of PUD:
Helicobacter pylori (H pylori) infection and non
steroidal anti inflammatory drugs (NSAIDs).(10).
The prevalence of PUD has shifted from
predominance in males, to similar occurrences in
males and females. Lifetime prevalence is
approximately 11-14% in men and 8-11% in
women. In relation to age PUD occurrence
researches reveal declining rates in younger men,
particularly for duodenal ulcer, and increasing
rates in older women.(5)The most common
etiologies of peptic ulcer disease are Helicobacter
pylori infection and non-steroidal anti-
inflammatory drugs usage. Other more obscure
etiologies include hypersecretory states, such as
Zollinger-Ellison syndrome, G-cell hyperplasia,
mastocytosis, and basophilic leukemia.(10). The
pathogenesis of peptic ulcer results from an
imbalance of aggressive gastric luminal factors
acid and pepsin and defensive mucosal barrier
function. Several causes and risk factors
contribute to ulcer formation by increasing gastric
acid secretion or weakening the mucosal
barrier.(11-13). The risk factors for PUD include
both modifiable and non modifiable risk factors.
Modifiable risk factors for PUD include smoking,
excessive alcohol intake and drug use as
NSAID.(14) Emotional stress and psychosocial
factors are frequently identified as important
contributors to ulcer pathogenesis, although stress
cannot be neglected as a contributing factor,
convincing evidence for it as the sole cause of
duodenal ulcer is scarce (15), while non modifiable
risk factors as age, sex and blood group.(14). Peptic
ulcer may be asymptomatic or symptomatic
disease. In particular, the absence of symptoms is
seen in NSAIDs-induced ulcers, for which upper
gastrointestinal bleeding or perforation might be
the first clinical manifestation of disease.(16)
However the predominant symptom of
symptomatic peptic ulcer is epigastric pain, which
can be accompanied by other dyspeptic symptoms
such as fullness, bloating, early satiety, and
nausea. In patients with duodenal ulcer, epigastric
pain occurs typically during the fasting state or
even during the night and is usually relieved by
food intake or acid-neutralizing agents, while a
third of these patients also have heartburn and
mostly without erosive esophagitis.(17).
Complications of PUD include: bleeding,

perforation, penetration and gastric outlet
obstruction. The major and severe complications
of peptic ulcer is bleeding, which is reported in
50-170 per 100, 000 patients. (18) On the other
hand perforation is less frequent than bleeding,
with an incidence of around 7-10 per 100,000
patients.(19) Penetration of retroperitoneal organs is
characterized by constant severe pain but
fortunately it is rare. Gastric outlet obstruction
due to ulcer-induced fibrosis is also rare, and
should raise suspicion of underlying malignant
disease. Management of peptic ulcers is aimed at,
restoring the balance between acid secretion and
mucosal protection and modifying risk factors,
e.g. NSAIDs use, dietary modification….
etc.(20)The management can be classified into
medical management through administering
prescribed medications as of histamine 2 blockers,
proton-pump inhibitors, and mucosal protectants
or surgical management, which is rare e.g. in case
of severe complications and nursing management
through health education and modifying patients’
health related practices.(21). Health-related
practices are one of the most important elements
in people's health and well-being which help in
the prevention, treatment, and management of
illness and the preservation of mental and physical
well-being.(22) Good health practices are defined
as activities and practices performed by people to
maintain a high level of wellness, improve their
health, and prevent disease complications.(23).
Poor health practices and poor socioeconomic
status are an important risk factor for developing
PUD.(24) Therefore, increasing attention has been
paid to health promotion and disease prevention
activities in the PUD because of its economic,
medical, nursing and social concerns with
increasing life expectancy. Also, by focusing on
preventive measures to decrease morbidity and
improve quality of life in patients with PUD.
Therefore, health related practices and lifestyle
have become important areas of concern over the
last 20 years.
Aim of the Study
Assess health-related knowledge and practices of
patients with peptic ulcer. Operational definition
of health related practices: For the purpose of this
study, health related practices will be
operationally defined as: Practices undertaken by
patients with peptic ulcer, in order to maintain
their health status and prevent complications.
Materials and Methods
1-Materials: Research Design: A descriptive
design was used to achieve the aim of this study.
Setting: This study was conducted at the
Gastroenterology & Endoscopic units, Outpatient
gastroenterology clinics, and Medical
gastroenterology wards at both the Main
University Hospital of Alexandria & the Medical
Research Institute of Alexandria. Subjects: A
convenience sample of 150 adult patients
diagnosed with peptic ulcer disease, admitted or
who have attended the above mentioned settings
according the following criteria: 1. Adult of both
sexes. 2. Patients diagnosed with peptic ulcer
(gastric or duodenal or esophageal) more than 3
months from diagnosis. 3. Age group 20 - 60
years old. 4. Being psychologically and physically
willing to participate. 5. Patients were excluded if
they had carcinoma of the stomach. Tool of data
collection: one tool was utilized for the purpose of
data collection. An Arabic Health – Related
Knowledge And Practices Structured Interview
Schedule was the tool to collect data about health
related knowledge and practices of patient with
peptic ulcer disease. - It was developed by the
researcher based on a review of relevant
literatures to assess the patients’ health-related
knowledge and practices related to peptic ulcer
disease (1, 9, 25). It was composed of three parts: Part
I: Socio-demographic characteristics and clinical
data: a) Socio-demographic data. b) Clinical data.
Part II: Peptic ulcer patients’ knowledge related to
peptic ulcer disease. Part III: Peptic ulcer patients’
health related practices.
2- Methods: This study was accomplished as
follows: 1- Written official approval to carry out
the study was obtained from: the ethical
committee in addition; required permission for
data collection was obtained from the responsible
authorities at the previously mentioned research
settings after explanation of the study purpose. 2-
Development of the tool: the health related
knowledge and practices questionnaire used to
collect data about heath related knowledge and
practices among peptic ulcer patients was
developed by the researcher after reviewing of
relevant literatures and translated in Arabic
language. 3- Content validity of the tool was
tested by five members in the field of medical-
surgical nursing , Faculty of Nursing - University
of Alexandria, to assure the content validity,
completeness and clarity of items and appropriate

translation. Modifications, correction and
clarifying of the items were done accordingly. 4-
Patient’s consent: informed oral consent of
patients in this study was obtained, after the
researcher introduced herself to every patient
agreed to participate in the study, explained the
purpose of the study for them, and confidentiality
and privacy was assured. 5- Reliability of the tool
was done using Cronbach Coefficient Alpha test
to measure the internal consistency of the tool.
The tool of the study was tested by 15 adult
patients with peptic ulcer disease. The data were
analyzed; the correlation coefficient for the tool
was (α =0. 80). 1. Pilot study: after the tool was
reconstructed a pilot study was applied on 15
patients diagnosed with peptic ulcer disease who
were excluded from the studied sample to test the
clarity and the applicability of the tool, to identify
the difficulties that may be faced during the
application of the tool and to estimate the time
needed to complete the interview schedule. 2.
Data collection: - The final draft of the structured
interview schedule was used to collect data in
order to achieve the objective of this study. The
data were collected by the researcher with each
patient’s on individualized interview from the
previous mentioned setting, where 92 patients of
the studied subjects were taken from the Main
University Hospital of Alexandria while, 58
patients of the studied subjects were taken from
the Medical Research Institute of Alexandria. -
The interview ranged from 20-45 minute on
individual basis depending on the degree of
understanding and patient’s response. Data
collection was conducted over a period of 10
months, from July 2012 to April 2013. 1.
Statistical analysis. 2. Data processing. 3. Data
analysis: - Data analysis was performed using
SPSS version 18.0. Regarding scoring system, the
item scores for each question were summed
together, then the total score was calculated by
summing the scores given for its responses. The
scores then transformed into score percent as the
following: Score % = (the observed score / the
maximum score) x 100. Then score % was
transferred into categories as follow: Poor: For
those who had a score % < 50.0%. Fair: For those
who had a score % 50.0 % - < 75.0%. Good
score: For those who had a score % ≥75%.
Results
The present study assessed the health-related
knowledge and practice of 150 adult patients with
peptic ulcer disease from the Main University
Hospital and the Medical Research Institute in
Alexandria. Personal characteristics of the sample.
The study shows that, (34%) of the studied
patients their age ranged from 20 to > 30 years,
(27.3%) of the patients were in the age group 30
to > 40 years, while about (19%) of them were in
the age group of 40 to >50 years and 50 to 60
years ,respectively. Also, it can be noticed that,
male patients represented a higher percentage
(52.0%), than female patients who represented
(48.0%) of the studied patients. Concerning
residence area, it was observed that, rural
residents constituted the higher percentage of the
studied patients (67.3%). In relation to marital
status, it was noticed that, more than half of the
studied patients (60%) were married. On the other
hand, (2.7%) of the studied patients were
divorced, (31.3%) of them were single and (6.0%)
of them were widows. Regarding the educational
level, it was evident that, illiterate patients formed
nearly (38%) of the subjects, while (22.7%) had
secondary education. In addition (19.3%) had a
bachelor degree. In relation to occupation, it was
found that, (34.7%) of the studied patients were
housewives, (32.7%) of them were manual
workers, and (22.7%) of them were office worker,
while (6.7%) of them were students and only,
(3.3%) of them were retired. Considering blood
group type, the table also reveals that, (26.7%) of
the studied patients were O blood group, while
(24.7%) of them were A blood group, (14.7%)
were B blood group, (10.7%) were AB blood
group and (23.3%) of the studied patients didn’t
know their blood group type. Table (1)

Table 1: Distribution of the studied patients according to their sociodemographic characteristics:
Sociodemographic data
Studied patients (n=150)
No %
Age (in years)
20- > 30 51 34.0
30-> 40 41 27.3
40-> 50 29 19.3
50- 60 29 19.3
Gender
Male 78 52.0
Female 72 48.0
ABO Blood group
A 37 24.7
B 22 14.7
AB 16 10.7
O 40 26.7
Don't know 35 23.3
Occupation
Office work 34 22.7
Manual work 49 32.7
Retired 5 3.3
Housewife 52 34.7
Student 10 6.7
Area of residence
Rural 101 67.3
Urban 49 32.7
Marital Status
Single 47 31.3
Married 90 60.0
Divorced 4 2.7
Widower 9 6.0
Education degree
Illiterate 57 38.0
Read and write 23 15.3
Basic education
completed
7 4.7
Secondary 34 22.7
University 29 19.3
Health history, peptic ulcer disease-related
variables of the subjects. (Table 2, figures 1 & 2).
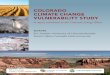
This table shows that, more than half of the
studied patients (57.3%) had duodenal ulcer,
while (36.7%) of them had gastric ulcer. Only,
(1.3%) of them had esophageal ulcer, while
(4.7%) of the studied patients stated that, they did
not know their type of ulcer. Also, the table
reveals that, almost half of the studied patients
(49.3%) had a free medical history, while (29.3%)
of them had a history of other associated
gastrointestinal disease as inflammatory bowel
disease and the minority of them (8.3%, 7.3%,
6.7%, and 2%) had endocrine disease as diabetes,
cardiovascular disease, rheumatoid arthritis and
hepatic disease, respectively. Regarding patients’
previous hospitalization, it was found that, more
than half of the studied patients (60%) had no
previous hospitalization with previously
mentioned diseases, while (40%) of patients were
previously hospitalized with one or more of the
previously mentioned diseases. In relation to
previous infection with H. pylori bacteria, it was
observed that, the majority of the studied patients
(70%) had been previously infected with H. pylori
bacteria, while (30%) of them had no infection or
didn’t know if they had been previously infected
with it. Concerning the family history of peptic
ulcer disease, it was obvious that, more than half
of the studied patients (53.3%) reported negative
family history of peptic ulcer disease, while
(46.7%) of them reported a positive family
history. The same table also displays that, more
than half of the studied patients (62.0%) had no
previous surgical history. Table (2)

Table 2: Distribution of the studied patients in relation to their medical history: Medical history No %
Type of ulcer
Gastric ulcer 55 36.7
Duodenal ulcer 86 57.3
Esophageal ulcer 2 1.3
Don't know 7 4.7
* Co morbid disease
Free medical history 74 49.3
Inflammatory bowel disease 44 29.3
Cardiovascular disease 11 7.3
Endocrine diseases such as diabetes 13 8.7
Renal diseases 5 3.3
Rheumatoid arthritis 10 6.7
Hepatic disease 3 2.0
Previous hospitalization
No 90 60.0
Yes 60 40.0
Previous H pylori bacteria infection
No / don't know 45 30.0
Yes 105 70.0
Surgical history
No 93 62.0
Cholecystectomy 20 13.3
Appendectomy 17 11.3
Eradication of part of the stomach 2 1.3
Tonsillectomy 5 3.3
Hysterectomy 6 4.0
Hernia 7 4.7
of peptic ulcer Family history
No / don't know 80 53.3
Father 20 13.3
Mother 21 14.0
Siblings 6 4.0
Relatives 23 15.3
* More than one answer was allowed
36.70%
57.30%
1.30%
4.70%
Type of ulcer Gastric ulcer
Duodenal ulcer
Esophageal ulcer
Don't know
Fig (1): Distribution of the studied patients according to type of ulcer.

30%
70%
Previous H pylori bacteria infection
No / don't knowYes
Fig (2): Distribution of the studied patients according to H. pylori infection.
Table 3: Distribution of the studied patients in
relation to their current symptoms: The table
demonstrates that, the majority of the studied
patients (88 %) complained of epigastric pain,
while more than half of the studied patients (60.7
%, and 56 %) complained of acidity and had
weight loss in their clinical manifestation,
respectively, more than one third of the studied
patients complained from loss of appetite
,vomiting ,indigestion and heart burn (39.3%,
42%, 36.0%, and 39.3%), respectively, while the
minority of the studied patients (20 %, 19.3%, 14
%, and 8 %) complained from esophageal reflux,
nausea, melena and hematemesis, respectively.
Regarding to the onset of current symptom,
findings showed that, (15.3%, and 34.7%) of the
studied patients began to complain of these
symptoms within 6 to> 9 months, 9 to > 12
months, respectively. While (29.3%) of the
studied patients began to complain of these
symptoms within 1 to >5 years, and (20.7%) of
them reported their complaints within 5 to >
10years. (figure 3).
Table 3: Distribution of the studied patients in relation to their current symptoms:
Current symptoms No (150) %
Acidity 91 60.7
Epigastric pain 132 88.0
Loss of appetite 59 39.3
Esophageal reflux 30 20.0
Nausea 29 19.3
Vomiting 63 42.0
Indigestion 54 36.0
Weight loss 84 56.0
Hematemesis 12 8.0
Melena 21 14.0
Heartburn 59 39.3
Onset of symptoms
(6 <9) months 23 15.3
(9 <12) months 52 34.7
(1<5) years 44 29.3
(5<10) years 31 20.7

60.70%
88%
39.3%
20% 19.3%
42%36%
56%
8%14%
39.3%
Current Symptoms
Fig (3): Distribution of the studied patients in relation to current symptoms.
Distribution of the studied patients in relation to
their beginning symptoms: The result shows that,
epigastric pain, heartburn, acidity and vomiting
were mentioned as beginning symptoms of peptic
ulcer disease by (45%, 25.3%, 24.7%, and 20%)
of the studied patients, respectively. In addition,
it was observed that, (10%) of the studied patients
started their symptoms with esophageal reflux,
(9.3%) with severe anemia, while (8.7%) of them
started their symptoms with weight loss, (8%) of
them with indigestion and vomiting of blood,
(4.7%) of them with headache, (4%) of them with
black tarry stool and abdominal distention, while
the other symptoms as constipation stated in
(2.7%) of patients, anorexia stated in (2%) of
patients and nausea was present among (1.3%) of
patients. In relation to epigastric pain description,
more than half of the studied patients (65.3%)
described their pain experience as pain in the form
of heartburn, (42%) of them described that pain is
increased by eating ,while for (8.7) of studied
patients pain usually appears with empty stomach
, and (13.3%) of studied patients described that,
pain diminished immediately after eating , while
(26.7%)of them reported that, pain awakens them
from sleep, and (14%) of them mentioned that,
pain can be diminished immediately after antacid
drugs. As regards to seeking medical advice,
results showed that, (29.3%) of the studied
patients sought medical advice after the onset of
the symptoms, while (42%) did after the
symptoms became more severe, while (28.7%) of
them did not seek medical advice until they
became unable to tolerate these symptoms.
Considering complications faced by the patients
from peptic ulcer disease, it was found that,
(42.7%) of patients had loss of appetite,
haematemesis occurred in 13.3% of patients,
melena in 18.7% of patients, while no
complications encountered was reported by 45.3%
of our patients.

Table 4: Distribution of the studied patients in relation to their beginning symptoms: Beginning symptoms No %
*Beginning symptoms
Acidity 37 24.7
Epigastric pain 68 45.3
Vomiting 30 20.0
Indigestion 12 8.0
Anorexia 3 2.0
Nausea lack stools heart burn 2 1.3
Weight loss 13 8.7
Reflux esophagus 15 10.0
Vomiting blood 12 8.0
Heart burn 38 25.3
Black stool 6 4.0
Severe anemia 14 9.3
Headache 7 4.7
Abdominal distension 6 4.0
Constipation 4 2.7
*Epigastric pain
No pain 2 1.3
Often the pain in the form of heartburn 98 65.3
Usually pain appears companion with empty stomach 13 8.7
Pain diminished immediately after eating 20 13.3
Pain diminished immediately after antacid drugs 21 14.0
Pain awakens you from sleep 40 26.7
Pain is increased by eating 63 42.0
First doctor visit
In the onset of symptoms 44 29.3
When symptoms increased 63 42.0
When you became unable to tolerate 43 28.7
*Complications
No 68 45.3
Bloody vomiting 20 13.3
Black stool 28 18.7
Loss of appetite 64 42.7
* More than one answer was allowed.
This part provided data about patient’s knowledge
regarding peptic ulcer disease. (Table 5, figure 4).
It can be seen that, more than half of the subjects
(54.0% and 56.7 %.) respectively didn’t know the
definition, and methods used for treatment of
peptic ulcer disease correctly and completely.
Regarding reasons of peptic ulcer disease, it was
found that, more than one-third of the study
participants (40%) did not know the reasons
related to peptic ulcer disease, and more than half
of patients (50.7%) knew the reasons related to
peptic ulcer disease partially while only (9.3%) of
the studied patients who knew the reasons related
to peptic ulcer completely and correctly.
Concerning signs and symptoms of peptic ulcer
disease, the table shows that, the minority of the
studied patients (10.0%) knew signs and
symptoms related to peptic ulcer disease
completely and correctly, while the majority of
them (77.3%) knew the signs and symptoms
partially correct, while (12.7%) of them did not
know any of the signs and symptoms related to
peptic ulcer disease. In relation to risk factors of
peptic ulcer disease, it was found that, the
minority of studied patients (10.7%) knew risk
factors related to peptic ulcer disease completely
and correctly, while more than half of the studied
patients (51.3%) didn’t know risk factors related
to peptic ulcer disease, and (38.0%) of them knew
risk factors related to peptic ulcer disease partially
correct. Regarding methods of treatment, the table
represents that, more than half of the subjects
(56.7%) didn’t know the methods of treatment at
all, and only (6.7%) of them knew the method of
treatment completely and correctly. Also the table
shows that, only (6.7%) of the studied patients
knew the drugs used in treatment of peptic ulcer
disease while the majority (74%) of them partially
knew the drugs used in treatment of peptic ulcer
disease and (19.3%) of the patient did not know
the drugs used in the treatment. Concerning
complications, only, (7.3%) of patients who knew

the complications related to peptic ulcer disease
completely while more than the half (54.7%)
knew them partially. Also, it was found that,
(38.0%) of the studied patients didn’t know any of
the complications related to peptic ulcer disease.
The Findings also reveal that, (44.0%) of the
studied patients had their information about peptic
ulcer disease from their own experience with the
disease, while (26.0%) of them had their
information from another patient, the minority of
them (1.3%, 3.3%, 5.3% and 10.7%),
respectively, had their information from (nurse,
friends & relatives, doctors and reading), while
(9.3%) of them did not receive any information
about peptic ulcer disease.
Table 5: Distribution of the studied patients according to their knowledge regarding peptic ulcer disease:
Knowledge items
Adult patients with Peptic Ulcer Disease
(n =150)
Completely
&
Correctly Know
Partially
&
Correctly know
Do not
Know/incorrect
answer
No. % No. % No. %
Definition 7 4.7 62 41.3 81 54.0
Causes 14 9.3 76 50.7 60 40.0
Signs and symptoms 15 10.0 116 77.3 19 12.7
Risk factors 16 10.7 57 38.0 77 51.3
Methods of treatment 10 6.7 55 36.7 85 56.7
Drugs used for treatment 10 6.7 111 74.0 29 19.3
Complications 11 7.3 82 54.7 57 38.0
*Source of information No. %
No source 14 9.3
Doctor 8 5.3
Nurse 2 1.3
Friends and relatives 5 3.3
Another patient 39 26.0
Reading 16 10.7
Patient’s experience with disease 66 44.0
* More than one answer was allowed n = number of studied patients
Figure 4: Distribution of the subjects according to their total health-related knowledge percent scores.
The Figure reveals that, the majority of the
studied patients (81.3%) had a poor knowledge
level, while 11.3% of them had a fair knowledge
level and only 7.3% had good knowledge level.
Poor Fair Good
81.30%
11.30%7.30%
Knowledge score
Poor
Fair
Good
This part provides data about health-related practices of subjects.

Table 6: Distribution of the studied patients in relation to their health-related practices regarding eating habits: Right Right but not complete Wrong
No % No % No %
Health practice related to eating habits 68 45.3 22 14.7 60 40.0
Health practice related to soft drinks, stimulants, and alcohol intake 68 45.3 15 10.0 67 44.7
Smoking habit 75 50 18 12 57 38
Health practice related to exercise and daily living activity 62 41.3 16 10.7 72 48
Health practice related to sleep and rest 58 38.7 45 30 47 31.3
Health practice related to mood and psychological status 69 46 52 34.7 29 19.3
Health practice related to medications 70 46.7 36 24 44 29.3
Health–related practices regarding Compliance with therapeutic regimen 63 42 36 24 51 34
Relationship between the scores of patients’ health-
related knowledge and their personal characteristics:
Table 7: Relationship between the patients’ health-
related knowledge score and their personal
characteristics: The findings reveal that, statistically
significant differences were found between the
patients’ health-related knowledge scores level and
patients’ age, where the highest score for good
knowledge were among young age (20- < 30 years). In
addition, statistically significant differences were
detected between the patients’ health-related
knowledge scores and patients’ occupation where, the
highest score for good knowledge were for students
and office workers (60.0%, 14.7%), respectively.
Moreover, statistically significant differences between
the patients’ health-related knowledge scores level and
area of residence were found with the highest
knowledge score for those coming from urban areas.
Finally, statistically significant differences were found
among the patients’ health-related knowledge scores
and patient educational level where, the highest
knowledge score was for high and secondary education
(24.1%, 11.8%), respectively.
Table 7: Relationship between the patients’ health-related knowledge score and their personal characteristics:
Sociodemographic data
Knowledge 2X P
Poor Fair Good
No % No % No %
Age
21.4 0.002*^
20- 40 78.4 5 9.8 6 11.8
30- 26 63.4 11 26.8 4 9.8
40- 28 96.6 0 0.0 1 3.4
50-60 28 96.6 1 3.4 0 0.0
Gender
1.1 0.574 Male 61 78.2 10 12.8 7 9.0
Female 61 84.7 7 9.7 4 5.6
Blood Type
13.1 0.108
A 34 91.9 2 5.4 1 2.7
B 18 81.8 2 9.1 2 9.1
AB 11 68.8 3 18.8 2 12.5
O 27 67.5 9 22.5 4 10.0
Don't know 32 91.4 1 2.9 2 5.7
Occupation
84.3 0.000*^
Office work 18 52.9 11 32.4 5 14.7
Manual work 47 95.9 2 4.1 0 0.0
Retired 5 100.0 0 0.0 0 0.0
Housewife 51 98.1 1 1.9 0 0.0
Student 1 10.0 3 30.0 6 60.0
Area of residence
15.9 0.000* Rural 90 89.1 9 8.9 2 2.0
Urban 32 65.3 8 16.3 9 18.4
Marital status
6.6 0.346^
Married 76 84.4 9 10.0 5 5.6
Not married 34 72.3 7 14.9 6 12.8
Divorced 3 75.0 1 25.0 0 0.0
Widower 9 100.0 0 0.0 0 0.0
Educational degree
54.2 0.000*^
Illiterate 57 100.0 0 0.0 0 0.0
Read and write 23 100.0 0 0.0 0 0.0
Primary 3 100.0 0 0.0 0 0.0
Preparatory 4 100.0 0 0.0 0 0.0
Secondary 23 67.6 7 20.6 4 11.8
University 12 41.4 10 34.5 7 24.1
^ P value based on Mont Carlo exact probability * P < 0.05 (significant)

Relationship between type of ulcer and patient’s
age, sex, blood group and H. pylori infection:
Table 8: Relationship between type of ulcer and
patient’s age, sex, blood group and H. pylori
infection: The findings reveal that, statistically
significant differences were found between the
patients’ blood group and type of ulcer in both
duodenal ulcer and gastric ulcer, where, the
highest percentage of those patients with gastric
ulcer (43.6%) were A blood group and the highest
percentage of those patients with duodenal ulcer
(33.7%) were O blood group. Finally, no
statistically significant differences were found
between the type of ulcer and the patient’s age,
sex or H.pylori infection.
Table 8: Relationship between type of ulcer and patient’s age, sex, blood group and H. pylori infection:
Type of ulcer
MCP Gastric ulcer Duodenal ulcer Esophageal ulcer Don't know
No
55 %
No
86 %
No
2 %
No
7 %
Age in years
0.163
20- 17 30.9 31 36.0 0 0.0 3 42.8
30- 15 27.3 25 29.1 0 0.0 1 14.4
40- 12 21.8 17 19.8 0 0.0 0 0.0
50 ≥ 60 11 20 13 15.1 2 100 3 42.8
Gender
0.206 Male 32 58.2 42 48.8 2 100 2 28.6
Female 23 41.8 44 51.2 0 0.0 5 71.4
Blood Type
0.017*
A 24 43.6 13 15.1 0 0.0 0 0.0
B 7 12.7 15 17.4 0 0.0 0 0.0
AB 5 9.1 10 11.6 0 0.0 1 14.3
O 10 18.2 29 33.7 1 50.0 0 0.0
Don't know 9 16.4 19 22.1 1 50.0 6 85.7
H pylori infection
0.641 No/don't know 15 27.3 27 31.4 0 0.0 3 42.8
Yes 40 72.7 59 68.6 2 100 4 57.1
MCP: P value based on Mont Carlo exact probability * P < 0.05 (significant)
Discussion Based on the current results and work experience,
the present study was carried out in order to assess
health related knowledge and practices of peptic
ulcer patients. Regarding age, the results of the
present study revealed that, the greater percentage
of the patients' ages were between 20-39 years
old. This finding agrees with Brunner and
Suddarth(26) and was nearly similar to that found
by Mohamed et al (27) who reported that, greater
percentage of the patients' ages were between 31-
35 years, and duodenal ulcer incidence at age
between 30-39 years, while in gastric ulcer
incidence is usually 50 years and older. These
findings may be related to the strong correlation
between age and chronicity of peptic ulcer
disease. In contrast with Niazy(28) who
emphasized that, the peak age for ulcer prevalence
is different among different studies and in
different populations and times. In his study,
ulcers were most frequent above the age of 60
years, rare in subjects under 20 years, attributed to
the low incidence of H. pylori in younger subjects
as a result of improved socioeconomic conditions
in the country in recent years. These results were
in accordance with other studies showing a shift
in ulcer prevalence towards older age groups, due
to increased prevalence of H. pylori infection and
increased NSAIDs use with age, with a peak in
ulcer incidence noted in above the age of 60
years.(29,30). Moreover, this study indicated that,
more than half of the studied patients had
duodenal ulcer , in age 20-40 years and is nearly
equal in men and women which agrees with Serra
and Jani(31) who suggested that, eighty percent of
peptic ulcers patients were diagnosed with
duodenal ulcers which were most common in
younger individuals aged 20-50, and was equally
common in men and women, while, the highest
percentage in gastric ulcers were in age 40-60
years ,were more common in men which agrees
with another study which suggests 15% of peptic
ulcers patients were diagnosed with gastric ulcers
which were more prevalent in older individuals

aged 50-70, were more common in men. This
finding was matched with Singh et al (32) who
stated that, duodenal to gastric ulcer ratio was
12:1 and peptic ulcer was more common in
elderly and dyspeptic individuals. Concerning
gender, the results of this study showed that,
about more than half of the studied patients were
males. In agreement with several studies(28,29,33)
and in accordance with Gerard and Lawrence, (34)
who reported that peptic ulcers were appearing in
men more often than women. This finding also
was supported by Barazandeh et al(35) and
Mohamadi et al(36) who indicated that, relative to
patients’ gender, more than half of the study
sample were males. The interpretation may be
related to the presence of more risk factors in
men, especially smoking and psychological
stresses, which is declining recently in western
countries with a changing pattern of smoking and
increased stress in working women in these
communities.(28). As regard blood group and
family history, this study showed that, more than
one quarter of the studied patients were blood
group O while nearly one quarter was blood group
A, which indicate that, the higher percentage in
the patient’s blood group was accounted for O
blood group which was supported with another
study of epidemiology of peptic ulcer disease that,
genetic factors play a role in both duodenal
and gastric ulcer. The results in this study support
the concept that DUs are more prevalent in
patients with blood group O, that GUs are more in
patients with blood group A.(28,37,38) The
interpretation may be related to increase
availability of H.pylori receptors in the gastric
mucosa of patients with blood group O as
compared with other blood groups,(37) while
another study showed no effect for blood group in
the prevalence of DUs.(39) . Furthermore, the
results of the current study showed that, the
highest percentage of the studied patients did not
have another family member with peptic ulcer
disease. These findings were in contrast with
Kohlstadt(40) who stated that, the first-degree
relatives of patients with duodenal ulcer have a
two- to threefold increase in risk of
getting duodenal ulcer and relatives of gastric
ulcer patients had a similarly increased risk of
getting a gastric ulcer and with another study
showed that, 62.2% of the patients had a family
history of PUD in their first degree relatives.
Moreover the results of the current study also,
contradicted with Niazy(28) who found that, family
history of ulcers was seen more in the ulcer group
and, had a history of ulcers in first degree
relatives . Regarding occupation, It was observed
that, housewives and manual work represented the
highest percentage of the studied patients. These
results may be justified by spreading of unhealthy
habits among rural housewives. These findings
were emphasized by Ronald(41) who conducted a
study on peptic ulcer among workers in the
engineering and chemical industries, in the United
State; he reported that, peptic ulcer was more
often diagnosed among manual work than in
office work and its incidence can be associated
with work conditions and lifestyle. These findings
were consistent with Sonnenberg and Everhart,(42)
who reported that, occupational workload was one
exogenous risk factor leading to increased acid
secretion and favoring male predominance with
respect to peptic ulcer. As regards patients’ area
of residence, the findings of this study showed
that, the highest percentage of the studied patients
came from rural areas, where rural residents
constituted the majority of the sample, due to
increased colonization of H. pylori among them as
result of low socioeconomic status.(28,43) These
results may be related to increased poverty, water
pollutions , unemployment and low
socioeconomic status in Egypt and especially in
rural regions. As regards marital status, the study
revealed that, the highest percentage of the
studied patients was married. This may be due to
that, married individuals hold wide
responsibilities and tasks which increase their
stress. These finding were matched with another
study that, 20.2% of the studied patients were
single, 70.6% were married and 9.2% were
divorced.(36) Furthermore, marital status has an
impact on patients' quality of life. These findings
also, were in disagreement with Minocha et al,(44)
who reported that race, marital status, and number
of persons in the household had no statistically
significant predictors of quality of life for patients
with peptic ulcer disease. As regards educational
level, the present study findings revealed that,
illiterate patients formed the greatest proportion of
the study sample, while more than one fifth of the
studied patients had a secondary educational level,
and nearly one fifth had a bachelor degree.
Similar findings were reported by Patrick,(45) and
Laaksonen et al,(46) who mentioned that lower
levels of educational attainment have been
associated with many diseases, including peptic
ulcer disease, other health-compromising

behaviors, and lower levels of treatment
adherence. Therefore, university graduated
patients had a good level of knowledge which is
significantly more than those who had a basic
education certificate or illiterate patients. These
findings can be rationalized by educated patients
who have health insurance, which facilitate,
health follow up and hence receive health
education and instructions. In addition, the study
findings may be related to the association between
illiteracy and many false traditional habits and
poor health related practices. This is in line with
Johnsen et al,(47) who reported that, low
educational level shared risk factors for peptic
ulcer in both men and women. The increased risks
associated with a low educational background
indicate that social strains, comprising lifestyle
and diet habits, are part of the multifactorial
etiology of peptic ulcer disease. This may be due
to that rural residence constitutes the majority of
the studied patients. Conversely, with Lafi(48) who
indicated that the majority of peptic ulcer patients
were Bachelor's degree or higher. The current
result was also supported by Nazi (28) who
indicated that ulcers were found to be increased in
illiterates and in subjects with lower educational
levels compared to those with higher education.
According to Rosenstock et al,(49) both family
income and level of education had an effect on
ulcer prevalence, reflecting the impact of stress
due to poverty and low income with an inability to
meet the life expenses on the prevalence of ulcers.
In addition, illiteracy is genuinely associated with
increased poor health related practices. In the
present study, it was also observed that,
individuals with PUD (72.7% for gastric ulcer and
68.6% for duodenal ulcer) were infected with
H.pylori. This finding was justified by spreading
of unhealthy habits, bad sanitation or unhealthy
environment through contaminated food or/and
contaminated groundwater with high prevalence
in third world countries as among the Egyptian
people.(50) Therefore, environmental, host-related
or factors related to the organism affect the
outcome of H.pylori infection. The highest
prevalence of H.pylori infection in PUD was in
accordance with Chinese endoscopic studies,(51,52)
and in contrast with European studies.(53,54,35) This
finding was matched with Snowden(50) and Li et
al,(52) who reported that 60% of gastric ulcers and
up to 90% of duodenal ulcers were caused by
chronic inflammation due to H. pylori infection.
This result was also supported by Galmiche and
Gournay(55) who proved that, there were
significant relationship between peptic ulcer and
H. Pylori. Moreover, Centers for Disease Control
and Prevention (2010), indicated that H. pylori
causes more than 90% of duodenal ulcers and up
to 80% of gastric ulcers and that approximately
two-thirds of the world’s populations are infected
with H. pylori.(56, 57) . In relation to patients’
current symptoms, the findings indicated that, the
majority of the studied patient complained of
epigastric pain. More than half of them
complained of acidity, had weight loss and less
than half of patients had loss of appetite Similarly
to Anand and Julian,(58) who stated that epigastric
pain is the commonest symptom of both gastric
and duodenal ulcers. The study also showed that,
most of the patients’ symptoms onset was within
9> 12 months and the results reflected also that,
the highest percentage of patients didn’t seek
medical help unless symptoms were increased
which may be due to lack of knowledge in the
highest proportion of illiterate patients. Moreover,
in the present study epigastric pain, heartburn,
acidity and vomiting were mentioned as
beginning symptoms of peptic ulcer disease for
the majority of the patients. These findings were
in agreement with Barkun and Leontiadis,(57) who
indicated that common ulcer symptoms include: A
burning, aching pain-or a pain that feels
like hunger. Pain sometimes extends to the back,
can last from a few minutes to a few hours and
usually goes away for a while after taking antacid
drugs. The results were also supported by Mayo
Foundation for Medical Education and Research
(MFMER),(59) which indicated that, epigastric
pain was the commonest symptom of peptic ulcer
disease. This finding also, in line with the
National Digestive Diseases Information
Clearinghouse (NDDIC),(60) which stated that, the
most common symptom of a peptic ulcer was a
gnawing or burning epigastric pain. On the other
hand, this finding was conversely with Aro et
al,(61) who conducted a study to explore the
prevalence, symptomatology, and risk factors for
peptic ulcer in a general adult population, the
results showed that, nausea and gastro esophageal
reflux were significant predictors of peptic ulcer
disease, but epigastric pain/discomfort was not. In
relation to patients’ knowledge related to peptic
ulcer disease, in the current study, data about
patients’ knowledge scores regarding peptic ulcer
disease proved that, the highest proportion of the
studied patients were scored as poor health-related

knowledge. This result may be related to that,
high proportion of studied patients were illiterate
and from rural areas or that, the majority didn’t
receive adequate information from health care
personnel. In addition to that, this finding matched
completely with a study conducted about peptic
ulcer disease and Jamaican patient awareness on
2007,(62) which showed that, awareness of
Jamaican patients about peptic ulcer disease were
inadequate. Therefore, the study suggests that,
there is a need for more physician education of
their patients as well as public health promotion
about peptic ulcer disease. As regard to health
related practices of the subjects, in relation to
dietary habits, the present study revealed that, the
highest percentage of the studied patients took
their food in fixed time and chew food well which
was considered as a healthy life style practice
however results also indicated loss of appetite for
the majority of patients and that, the majority of
patients preferred both spicy and fatty foods,
added salt and black pepper to made their food
tasty and more than half of the subjects cooked
their food by frying or use margarine in cooking
,which is considered as a poor healthy lifestyle
practice. This finding was supported by James et
al,(63) who showed that, a higher percentage of
subjects consumes fruits and vegetables were
associated with lower risk of duodenal ulcer. The
interpretation may be related to that; the Egyptian
diet contains high amounts of saturated fat. In
addition to that, Folklore has incriminated dietary
indiscretion as a cause for ulcers and dietary
factors had been hypothesized to account for some
of the regional variations of ulcer disease, but,
controversies surround this hypothesis due to
difficulties in having randomized, controlled
studies. Missing one of the 3 daily meals was a
common phenomenon, but some habitually skip
breakfast or other meals most of the days of the
week. This was found to be associated with
increased ulcerations especially in subjects who
skip breakfast or more than one meal daily.(63, 64).
This may be explained by the effects of prolonged
unneutralized gastric acidity, in addition, missing
meals leads usually to increased consumption of
coffee, and cigarettes, both of them increases
gastric acidity and decrease defensive
mechanisms of the gastric mucosa for
ulceration.(46) In relation to milk intake, the
highest percentage of subjects didn’t drink milk or
milk product to avoid discomfort which
contradicts with another study that indicated high
intake of milk products was associated with
decreased risk for ulcer, whereas increased risk
was noted for low milk intake.(65). As regards
smoking, soft drinks, stimulants, and alcohol
intake, the effect of smoking and coffee intake on
ulcer incidence was the subject of many studies
with different results. Smoking is well known to
have a number of adverse effects on mucosal
aggressive and protective factors.(64) The present
study shows that, the majority of studied patients
reported that, they were drinking caffeine,
stimulant namely coffee, tea and Nescafe as well
as , the majority of male subjects reported that,
they were smokers. Similar findings were reported
by another study, which supposed strong
association between cigarette smoking &
stimulants (coffee) and prevalence of DUs, and
this prevalence increases linearly with increase in
the number of cigarettes smoked, irrespective of
the duration of smoking and increases with an
increase in the number of cups of coffee ingested
daily.(66) Therefore, an improvement in
socioeconomic status, dietary instructions,
moderation of coffee intake and cessation of
cigarette smoking, all may help to decrease the
prevalence of ulcer in the community and its
impact on health and the economy. On the other
hand, these findings contradicted with
Mukhopadh et al,(64) who conducted a study of
smoking habits among slum dweller and the
impact on health among the population of West
Bengal. The study proved that, there was a low
effect of smoking on ulcer incidences. Concerning
physical activity, the study revealed that, nearly
half of the studied patients work from 6 to 10
hours per day while, more than one third of them
work more than 10 hours per day and that, the
highest proportion of the subjects did muscular
efforts in their work, Regarding the impact of
peptic ulcer disease at work, the findings also
revealed that, more than half of the subjects were
affected by peptic ulcer disease as had a negative
impact on their work. The majority of them were
unable to complete the work assigned to them. As
for exercises, it was clear that those who practiced
exercises were the minority of subjects, while the
majority of them didn’t practice exercise
anymore. This may be due to fatigue and
weakness related to peptic ulcer disease which
may be a risk for ulcer disease as suggested by
another study that moderate leisure time physical
activity protected against PUD, and that exercise
has a role in the treatment and prevention of more

than 40 chronic diseases including Alzheimer's
disease, diabetes, heart disease, obesity, peptic
ulcer and hypertension... etc.( 56,67) Also, Mustelin
L et al,(68) reported the positive effects of aerobic
activity while recovering from an ulcer and
suggested that, exercise had antidepressant effects
and that, regular exercises had a positive effect on
the general health of people and could lessen the
severity of emotional disorders by giving the
person a sense of greater control. As regards sleep
and rest, more than half of the studied patients
slept most frequently from 6 to 8 hrs per day
which is considered as a healthy sleeping hours.
In addition, it was found that, nearly one third of
the patients always or sometimes had sleeping
problems. The majority of them were having
disturbed sleeping. In accordance with Boonstra et
al,(69) who mentioned that, sleep disturbances may
be exacerbated by symptoms of gastrointestinal
(GI) alterations, pain, and fatigue. Peptic ulcer
disease, for example, was more common in shift
workers (a shift worker is anyone who follows a
work schedule that is outside of the typical "9am
to 5pm" business day). Also, in accordance to the
National Sleep Foundation's,(70) which indicated
that, sleeping problems and lack of sleep can
affect everything from personal and work
productivity to behavioral and relationship
problems. As regards mood and psychological
status, apparently more than half of the studied
patients were complaining of being nervous, these
findings may suggest that, psychological states
can be a risk factor for peptic ulcer disease. In
agreement with Mohamadi et al,(36) who reported
that, 60% of peptic ulcer patients believed PUD
was related to stress. This result was also, in
accordance with Goodwin,(71) who conducted a
study on the impact of stress on development of
peptic ulcer. He concluded that, person who
perceived their lives as stressful may be at
increased risk for the development of peptic ulcer
disease. Regarding medications, the result
revealed that, the highest percentage of patients
were taking or sometimes taking non prescribed
medications, which increase the risk for peptic
ulcer disease, which agrees with Chang et al,(72)
who revealed that, the drug use, especially
NSAIDs, and aspirin has become an important
cause of peptic ulcer bleeding in southern Taiwan.
Regarding compliance with therapeutic regimen,
the results revealed that, the majority of the
studied patients didn’t visit doctor on a regular
base. Patient compliance is paramount in the
effectiveness of therapeutic regimens .Without
compliance therapeutic goals cannot be achieved,
resulting in poorer patient health outcomes.(73)
This may be related to social and psychological
factors that, influence compliance as knowledge
and understanding including communication,
quality of the interaction including the patient–
provider relationship and patient satisfaction,
social isolation and social support including the
effect of the family, and factors associated with
the illness and the treatment including delay in
asking for medical help unless beginning of
symptoms of complications as severe pain,
bleeding or severe anemia. As regards the
correlation between knowledge scores and
personal characteristics of the studied patients, the
study illustrated that, there were statistically
significant differences between the patient’
health-related knowledge scores and patient age,
occupation, area of residence and level of
education. This significance was contradicted by
Sonnenberg, (75) who mentioned that, there were
no significant difference between the patients’
knowledge related to peptic ulcer disease and their
age, sex, area of residence, and occupation. As
regards the relationship between type of ulcer and
patient’s age, sex, blood group and H.pylori
infection, it was observed that, there were
statistically significant differences between the
patient’s blood group type, and type of ulcer in
both duodenal and gastric ulcer. This significance
was supported by Salih,(76) who mentioned that, O
blood group individuals were more susceptible
to H. pylori infection and its symptomatic
gastrointestinal complications. Also, in agreement
with Kanbay et al,(77) who mentioned that, patients
with blood groups A and O were more prone to H.
pylori infection and thus to peptic ulcer disease.
Recommendations From our study, we recommend the following: -
Nurses should receive advanced educational
programs about health-related practices of peptic
ulcer disease. -A colored illustrated booklet
should be available and distributed to each patient
with peptic ulcer disease about disease and health-
related practices. -The nurse should provide health
education to patients, taking into account the
questions and concerns of these patients. -Study
the factors involved in patient compliance and test
the effectiveness of compliance-enhancing
strategies.
References

1. Vakil N. Gastrointestinal and Liver Disease:
Pathophysiology, Diagnosis, Management. 9th ed.
Philadelphia, WB Saunders. 2010; 270.
2. Theodore W. Peptic Ulcer Disease. American
College of Gastroenterology 2012; 301 (1): 263-66.
3. Sonnenberg A. Causes Underlying the Birth-Cohort
Phenomenon of Peptic Ulcer: Analysis of Mortality
Data, England and Wales. International Journal of
Epidemiology 2006; 35 (15): 1090–7.
4. Everhart J. Peptic ulcer disease. The Burden of
Digestive Diseases in the United States. 2nd ed.
Washington, DC: US Government Printing Office.
2008; 280-83.
5. Michael W, Vignogna L. Peptic Ulcers Overview
2011. Available at http://www.emedicinehealth
.com/peptic_ulcers/article_em.htm#Peptic Ulcers
Overview. Retrieved on 6/2012
6. Right Diagnosis.com, Statistics by Country for
Peptic Ulcer, Health Grades, Inc, available at:
http://www.rightdiagnosis.com. Retrieved on,
6/2012.
7. ASHP commission for therapeutics. American
Society of Health Pharmacists, Therapeutic
Position Statement on the Identification and
Treatment of Helicobacter Pylori-Associated Peptic
Ulcer Disease in Adults. American Journal of
Health Systemic Pharma 2001; 58 (4): 331-7.
8. Johns H. Peptic Ulcer Disease, 2010. Available at:
http://www.hopkins-gi.org. Retrieved on, 6/ 2012.
9. Wolfram Alpha Computational Engine. Wolfram
Alpha knowledge base. DALY: Disability And
Peptic Ulcer Disease, Adjusted Life Years, 2011,
available at http://www.wolframalpha.com.
Retrieved on, 5/2012.
10. Papatheodoridis G, Sougioultzis S, Archimandritis
A. Effects of Helicobacter Pylori and Nonsteroidal
Anti-Inflammatory Drugs on Peptic Ulcer Disease:
A Systematic Review. Journal Clinical
Gastroenterology and Hepatology 2006; 4 (2): 130–
42.
11. Malfertheiner P, Francis K, Kenneth E, et al. Peptic
Ulcer Disease. 2009; Available at
www.thelancet.com.
12. Quan C, Talley N. Management of Peptic Ulcer
Disease Not Related to Helicobacter Pylori or
NSAIDs. American Journal of Gastroenterology
2002; 97 (4): 2950–61.
13. Streitparth F, Pech M, Bohmig M, et al. In Vivo
Assessment of the Gastric Mucosal Tolerance Dose
after Single Fraction, Small Volume Irradiation of
Liver Malignancies by Computed Tomography -
Guided, High – Dose - Rate Brachytherapy.
International Journal of Radiation Oncology,
Biology, Phys 2006; 65 (6): 1479–86
14. Rosenstock S, Jorgensen T, Bonnevie O, Andersen
L. Risk Factors for Peptic Ulcer Disease: A
Population Based Prospective Cohort Study
Comprising 2416 Danish Adults. Journal of British
Society of Gastroenterology 2003; 52 (4): 186–93.
15. Levenstein S. Upper Gastrointestinal Disorders in
Psychosomatic Medicine. Journal of Psychosomatic
Medicine 2002; 64 (2): 767–72.
16. Sung J, Tsoi K, Ma T, et al .Causes of mortality in
patients with peptic ulcer bleeding: a prospective
cohort study of 10,428 cases. American Journal of
Gastroenterology. 2010; 105(1):84-9.
17. Malfertheiner P, Dent J, Zeijlon L, et al. Impact of
Helicobacter Pylori Eradication on Heartburn in
Patients With Gastric or Duodenal Ulcer Disease—
Results from A Randomized Trial Program.
Aliment Pharmacology Therapy 2002; 16 (2):
1431–42.
18. Garcia Rodriguez L, Barreales T. Risk of Upper
Gastrointestinal Complications among Users of
Traditional NSAIDs and Coxibs in the General
Population. Gastroenterology 2007; 132 (2): 498–
506.
19. Gisbert J, Pajares J. Helicobacter Pylori Infection
and Perforated Peptic Ulcer Prevalence of the
Infection and Role of Antimicrobial Treatment.
Helicobacter 2003; 8 (3): 159–67.
20. Smoot D, Cryer B. Peptic Ulcer Disease. American
Journal of Gastroenterology. Primary Care 2001; 28
(3): 487-503.
21. Ford A, Delaney B, Forman D, et al. Eradication
Therapy For Peptic Ulcer Disease in Helicobacter
Pylori Positive Patients. Cochrane Database
Systemic Review; American Journal of
Gastroenterology 2006; (4):84-9
22. Green, L. W and Kreuter, M. (2002). Health
Promotion Planning: An Ecological and
Environmental Approach, 3rd ed. Mountain View,
CA: Mayfield Publishing Co. P 234
23. Rosenstock S, Jørgensen T and Bonnevie O, et
al .Does Helicobacter Pylori Infection Explain All
Socioeconomic Differences in Peptic Ulcer
Incidence? Genetic and Psychosocial Markers for
Incident Peptic Ulcer Disease in A Large Cohort of
Danish Adults. Scand Journal of
Gastroenterology. 2004; 39(9):823-9.
24. Lee R, Loke A. Health-Promoting Behaviors and
Psychosocial Well-Being of University Students in
Hong Kong. Public Health Nursing 2005; 66 (5):
271–2.
25. Leslie W, Shirley M, Jane H. Quality and Nursing:
Moving From a Concept to A Core Competency.
Alimentary Pharmacology Therapy. 2008 15;
19(10):1051-61.
26. Brunner L, Suddarth D. Medical Surgical Nursing.
11th ed, Lippincott, Philadelphia. 2008 p. p. 1209–
10,
27. Mohammad O, Yasin M. Mussa A, et al. Quality of
Life among Adult Patients with Peptic Ulcer in the
City of Sulaimani. Iraqi National Journal for
Nursing Specialties 2011; 24 (1): 81.

28. Niazy A. Risk Factors for Duodenal Ulcer Disease.
Jordan University of Science and Technology.
Saudi Medical Journal 2002; 23 (2): 38.
29. Lam S. Differences in Peptic Ulcers between East
and West. Baillieres Best Practice and Research.
Journal of Clinical Gastroenterology 2000; 14 (1):
41-52
30. Wang J, Liu S, Chen S, et al. Risk factors for Peptic
Ulcer in Shanghai. International Journal of
Epidemiology 1996; 25 (3): 638-43.
31. Serra S, Jani P. An approach to duodenal biopsies.
Journal of Clinical Pathology. 2006; 59(11): 1133–
1150.
32. Singh V, Trikha B, Nain CK , et al. Epidemiology
of Helicobacter pylori and peptic ulcer in India.
Journal of Gastroenterology and Hepatology. 2002;
17(6):659-65.
33. Ahmed M, Al-Knawy B, Al-Wabel A, et al.
Duodenal Ulcer and Helicobacter Pylori Infection
at High Altitude: Experience from Southern Saudi
Arabia. Canadian Journal Gastroenterology 1997;
11 (4): 313-16
34. Gerard M, Lawrence W. Current Surgical
Diagnosis and Treatment, 12th ed. Raw-Hill
Companies, New York. 2006; P.P: 513-515.
35. Barazandeh F, Yazdanbod A, PourfarziF, et al.
Epidemiology of Peptic Ulcer Disease: Endoscopic
Results of a Systematic Investigation in Iran.
Middle East Journal of Digestive Diseases2012; 4
(2): 90-6.
36. Mohamadi S, Baghian M, Falahi A, et al. In a study
of Survey on Quality Of Life Related Factors in
Patients with Peptic Ulcer Based on PRECEDE
Model in Yazd, Iran Journal of Medicine and Life
2011;4 (4): 407:11.
37. Boren T, Falk P, Larson G, et al. Attachment of
Helicobacter Pylori to Human Gastric Epithelium
Mediated by Blood Group Antigens. Science
1999;262 (5141): 1892-5
38. Sideebotham R, Baron J, Schrager J, et al.
Influence of Blood Group and Secretor Status on
Carbohydrate Structures in Human Gastric. Saudi
Medical Journal Clinical Science 2002; 89 (2): 405-
15.
39. Niv Y, Fraser G, Delpre G, etal. Helicobacter
Pylori Infection and Blood Groups. American
Journal Gastroenterology 1996; 91 (1): 101-4.
40. Kohlstadt I. Advancing Medicine with Food and
Nutrients, 2nd ed. CRC Press, 2012; 230.
41. Ronald J. Peptic ulcer among workers in the
engineering and chemical industries, in United
State. Journal of Gastroenterology and Hepatology
2002; 10 (6): 633-8.
42. Sonnenberg J, Everhart E. Prevalence of Self-
Reported Peptic Ulcer in the United States.
American Journal of Public Health 2000; 86 (2):
200-5.
43. Graham D, Malaty H, Evans D, et al. Epidemiology
of Helicobacter Pylori in an Asymptomatic
Population in the United States: Effect of Age, and
Socioeconomic Status. Journal of Gastroenterology
1999; 100 (1): 1495-501.
44. Minocha A, Wiginigton W, Johnson W. Detail
Characterization of Epidemiology of
Uninvestigated Dyspepsia and Its Impact on
Quality of Life among African American as
Compared to Caucaians. American Journal of
Gastroenterology 2006; 20 (101): 340.
45. Patrick E. Health and Behavior: The Interplay of
Biological, Behavioral, and Societal Influences.
Journal of Consulting and Clinical Psychology.
2011; 66(1):89–112.
46. Laaksonen M, Talala K, Martelin T, et al. Health
Behaviors as Explanations for Educational Level
Differences in Cardiovasculard All Community
Mortality: A follow Up of 600000 Men in Omen
Over 23years. European Public Health Journal
2008;18 (1): 38-43
47. Johnsen R, Forde O, Straume B. Etiology of
Peptic Ulcer: A Prospective Population Study in
Norway. Burhol Journal Epidemiology Community
Health 1997;48 (1): 156-60
48. Lafi, S. Life Style among Patients with Peptic
Ulcer. Iraqi National Journal for Nursing
Specialties, Bagdad 2004; 23 (1): 10-14.
49. Rosenstock S, Moller M , Larsson H et al.
Improving Quality of Care In Peptic Ulcer
Bleeding: nationwide cohort study of 13,498
consecutive patients in the Danish Clinical Register
of Emergency Surgery. American Journal
Gastroenterology 2013; 108 (9): 1449-57.
50. Snowden F. Emerging and Reemerging Diseases: A
Historical Perspective. Immunology Review 2008;
225 (1): 9–26.
51. Xia B, Ma C, Wong K, et al. Trends in the
Prevalence of Peptic Ulcer Disease and
Helicobacter Pylori Infection in Family Physician-
Referred Uninvestigated Dyspeptic Patients in
Hong Kong. Alimentary Pharmacology Therapy
2005; 22 (3): 243 – 9.
52. Li Z, Zou D, Ma X, et al. Epidemiology of Peptic
Ulcer Disease: Endoscopic Results of the
Systematic Investigation of Gastrointestinal
Disease in China. American Journal of
Gastroenterology 2010; 105 (1): 2570-7.
53. Aro P, Storskrubb T, Ronkainen J, et al. Peptic
Ulcer Disease in a General Adult Population: The
Kalixanda Study: A Random Population-Based
Study. American Journal of Epidemiology 2006;
163 (11): 1025 – 34.
54. Zagari R, Law G, Fuccio L, et al. Dyspeptic
Symptoms and Endoscopic Findings in The
Community: The Loiano-Monghidoro study.
American Journal of Gastroenterology 2010; 105
(3): 565 – 71.

55. Galmiche J, Gournay J. Role of Helicobacter
pylori in the Pathogenesis of Gastritis, Peptic Ulcer
and Gastric Cancer. Scand Journal
Gastroenterology 2003; 28 (196): 3-6.
56. Chan F, Leung W. Peptic-Ulcer Disease. Lancet
2002; 360 (9337); 933-41.
57. Barkun A and Leontiadis G. WebMD Medical
Reference from Healthwise. Peptic Ulcer Disease –
Symptoms.2010.Available at: http://www.
webmd.com/digestive-disorders/tc/peptic-ulcer-
disease-symptoms
58. Anand B, Julian K. Peptic Ulcer Disease.
Medscape: Drugs, Diseases and Procedures 2011.
Available at: http://emedicine.medscape.com/
article/181753-overview
59. Mayo Clinic staff. Peptic ulcer disease. Mayo
Foundation for Medical Education and Research
2013. Available at:
http://www.mayoclinic.com/health/peptic
ulcer/DS00242/DSECTION=symptoms.
60. National Digestive Diseases Information
Clearinghouse .Bethesda M. H.pylori and Peptic
Ulcer. 2007. NIH Publication No. 05–4225
www.gastro.org.
61. Aro P, Storskrubb T and Ronkainen J, et al .Peptic
Ulcer Disease in a General Adult Population.
American Journal of Epidemiology 2006;
163(11):1025-34.
62. Lee M, Soyibo K, Garro I, et al. Peptic Ulcer
Disease and Jamaican Patients' Awareness of Their
Disorders. West Indian Medical Journal 2007 Jun;
44 (2): 58-9.
63. James W, Pat B, Richard H, et al .Health benefits of
dietary fiber. International Life Sciences Institute
Nutrition Reviews 2009 ; 67 (4): 188–205
64. Mukhopadh S. Smoking Habits among Slum
Dweller and the Impact on Health among the
Population of West Bengal. Journal of
Gastroenterology and Hepatology 2007; 10 (6):
633-8.
65. Elmståhl S, Svensson U, Berglund G. Fermented
Milk Products are Associated with Ulcer Disease.
Results of a Cross-Sectional Population Study. US
National Library of Medicine. National Institutes of
European Journal of Clinical Nutrition. 1998;
52(9):668-74.
66. Chen T, Chang F, Lee S. Smoking and Male
Gender Rather than CagA Protein are Associated
with Increased Risk of Duodenal Ulcer in
Helicobacter pylori- Infected Patients in Taiwan.
Journal of Digestive Diseases and Sciences2000; 44
(2): 2076-80.
67. Rosenstock S, Jørgensen T, Bonnevie O, et al.
Risk Factors for Peptic Ulcer Disease: A Population
Based Prospective Cohort Study Comprising 2416
Danish adults. Journal of Gastroentrology 2003; 52
(1): 186-93.
68. Mustelin L, Silventoinen K, Pietil A, et al. Physical
Activity Reduces the Influence of Genetic Effects
on Body Mass Index and Waist Circumference: A
Study in Young Adult Twins. International Journal
of Obesity 2009; 33 (1): 29-36.
69. Boonstra L, Harden K, Jarvis S, et al. Sleep
Disturbance in Hospitalized Recipients of Stem
Cell Transplantation. Clinical Journal Oncology
Nursing 2011; 15 (3): 271-6.
70. The National Sleep Foundation. Sleep
Studies.2013.Available at:
http://www.sleepfoundation.org/article/sleep-
topics/sleep-studies
71. Goodwin R. Impact of Stress on Development of
Peptic Ulcer. Rajiv Gandhi University of Health
Sciences Bengaluru, Karnataka. 4th 'T' Block.2002.
Available at
:http://www.rguhs.ac.in/cdc/onlinecdc/uploads/05_
N145_14279.doc http://pre.docdat.com/docs/index-
185826.html
72. Chang C, Wu M, Lee C , et al. Prospective Survey
for the Etiology and Outcome of Peptic Ulcer
Bleeding: A Community Based Study in Southern
Taiwan. The Journal of the Formosan Medical
Association. 2011; 110 (4):223-9.
73. Panesar K. Patient Compliance and Health
Behavior Models. Journal of the United State
Pharmacology. 2012; 37(4):12-14.
74. Cameron C. Patient Compliance: Recognition of
Factors Involved and Suggestions for Promoting
Compliance with Therapeutic Regimens. Journal of
Advanced Nursing 2008; 24 (2): 244-50.
75. Sonnenberg A. Knowledge about Causes of Peptic
Ulcer Disease. Journal of Occupied Medicine 2002;
29 (1): 756-61
76. Salih M. Relationship between ABO blood group
and Helicobacter Pylori Infection in Symptomatic
Patients. Clinical Expression
Gastroenterology. 2011; 4: 221–6.
77. Kanbay M, Gur G, Arslan H, et al. The relationship
of ABO Blood Group, Age, Gender, Smoking, and
Helicobacter pyloriin Infection. Digestive Disease
Science. 2005; 50(7):1214-7.

Original Article
Diagnostic Potential of Osteopontin Biomarker in Irritable Bowel Syndrome
Gihane I Khalil1 ,Hanan M. Mostafa2 &Fatma I. Dwidar3
Chemical Pathology1 &Internal Medicine2 departments, Medical Research Institute,Biochemistry department3, Faculty
of Medicine, Alexandria University
ABSTRACT
Osteopontin (also known as early T lymphocyte activation Eta-1) ,a cytokine which promotes Th1 immune
responses.Several recent reports have suggested an important role for osteopontin in the pathogensis of inflammatory
bowel diseases as well as its possible use as a biomarker. Aim of the study: The aim of this work was to find out the
diagnostic potential of osteopontin biomarker in irritable bowel syndrome. Subjects and Methods: This study included:
Group I: included 40 patients who were fulfilling Rome III criteria for IBS. And Group II: included 20 healthy subjects
as controls.Informed consent were obtained from all subjects.All subjects were subjected to: medical history
taking,thorough physical examination and laboratory investigations which included:- Routine laboratory tests ,fecal
calprotectin assessment and serum osteopontin assessment.Colonoscopy and histopathological examination of biopsies
from the colon were done for patients only (Group I). Result: Out of 40 patients (group I); 20 were IBS-D (diarrhea
predominant), 14 IBS-C (constipation predominant) and 6 IBS-A (alternating diarrhea and constipation). Both group I
and group II were matched as regard age and sex. There were no statistical significant difference between the two
studied group as regard routine laboratory investigations. Stool analysis was normal in all subjects. No statistical
significant difference between the two groups as regard the mean erythrocytes sedimentation rate (ESR) at the frist and
second hour [p = 0.586& 0.194 respectively]. Also no statistical significant difference between the two groups as rgard
the mean C-reactive protein (CRP), the mean fecal calprotectin level and the mean serum osteopontin level [p = 0.432,
0.066 &0.086 respectively]. As regard colonoscopic findings in IBS patients:Hyperemia was found in 4 patients ,polyps
was found in 2 patients, diverticulae, ulcers and mass were not found in any patients . Regarding histopathological
findings of colonoscopic biopsies in IBS patients: Non specific colitis was found in 30 patients ,10 patients was normal.
Lymphocytic colitis was not found in any patient . Conclusion: Osteopontin has no role as a diagnostic biomarker in
IBS.Further work on a larger patients sample will be required to study the propabiltyle of the use of osteopontin as non
invasive biomarker in the differential diagnosis between functional and inflammatory gastrointesinal disorders.
Introduction
Irritable bowel syndrome (IBS) is a common
disorder that affects a heterogeneous group of
patients experiencing chronic and recurrent
abdominal pain usually associated with visceral
hypersensitivity and altered bowel habit.(1). The
Rome III criteria (2) (2006) for the diagnosis of
irritable bowel syndrome require that patients
must have recurrent abdominal pain or discomfort
at least 3 days per month during the previous 3
months that is associated with 2 or more of the
following; pain relieved by defecation, onset
associated with a change in stool frequency or
onset associated with a change in stool form or
appearance. Irritable bowel syndrome (IBS) is a
multifactorial disorder and a number of
pathophysiological mechanisms have been
proposed, including abnormalities of motility,
visceral sensation, and even alterations of gut
fermentation. In addition, psychological factors
are important in at least some patients. Small
bowel bacterial overgrowth has been heralded as a
unifying mechanism for the symptoms of bloating
and distention common to patients with irritable
bowel syndrome. This has led to proposed
treatments with probiotics and antibiotics. (3-6).
More recently, it has been proposed that
inflammation may play a role in IBS, based on
several lines of evidence. For instance, increased
numbers of mast cells have been found in the
terminal ileum of IBS patientsand some patients
with ulcerative colitis have IBS-like symptoms

when in remission.(7&8) In addition, a substantial
proportion of cases are apparently precipitated by
gastrointestinal infection where a continuing
inflammatory response has been demonstrated.
Both colonic inflammation (increased numbers of
colonic mucosal lymphocytes ) and small bowel
inflammation have been discovered in a subset of
patients with irritable bowel syndrome as well as
in patients with inception of irritable bowel
syndrome after infectious enteritis (postinfectious
irritable bowel syndrome).(9). Calprotectin is a
cytoplasmic antimicrobial component prominent
in granulocytes, monocytes, and macrophages.(10)
It accounts for approximately 60% of the total
protein of the cytosol. The release of calprotectin
is most likely a consequence of cell disruption and
death.(11) Fecal calprotectin determination has been
demonstrated to be useful for diagnosing various
inflammatory diseases of the gastrointestinal
tract.(12). Osteopontin(also known as early T
lymphocyte activation Eta-1), a cytokine which
promotes Th1 immune responses.(13)Several recent
reports have suggested an important role for
osteopontin in the pathogensis of inflammatory
bowel disease (IBD) as well as its possible use as
a biomarker.(14) Osteopontin, is up-regulated in
relation to the severity of the disease.(15)
Moreover, since it is an adhesive glycoprotein
containing the peptide sequence glycine ±
arginine ± aspartate ± serine it promotes cell
attachment.(16,17)
Aim of the Work
The aim of this work was to find out the
diagnostic potential of osteopontin biomarker in
irritable bowel syndrome.
Subjects and Methods
This study was coducted on two groups: Group I:
included 40 patients who were fulfilling Rome III
criteria for IBS. Group II: included 20 healthy
subjects as controls. All patients and control were
matched as regard age and sex. Exclusion criteria
included: Patients with history of the use of drugs
such as nonsteroidal anti-inflammatory drugs
(NSAIDs), aspirin, and anticoagulants,
gastroenterological diseases such as inflammatory
bowel disease, infectious enterocolitis,
concomitant presence of other non-
gastroenterological diseases, in particular;
rheumatoid arthritis or other connective tissue
inflammatory diseases, or respiratory or urinary
tract inflammation/infection.Informed consents
were obtained from all patients. All patients and
controls were subjected to the followings: 1.
Medical history taking: Each patient were
evaluated by documentation of the ROME III
criteria,(2) which has been suggested as a guide for
the clinical diagnosis of irritable bowel syndrome.
2. Thorough physical examination to exclude
organic diseases. 3. Laboratory investigations
which included: A- Routine laboratory tests: Stool
analysis to exclude pus (as a sign of inflammation
or infection) and ova of parasites,complete blood
picture, blood urea, serum creatinine,fasting and
post prandial blood glucose levels,serum
transaminases, serum albumin, total serum
bilirubin,erythrocytes sedimentation rate, C-
reactive protein. B- Fecal calprotectin level
assessment using ELISA technique: (18)About 5
gm stool in a suitable container stored at – 20°C
until assayed for calprotectin. The sample of stool
was tested using the PhiCal ELISA test device,
produced by Nycomed Pharma AS. Essentially,
5g of faeces were mixed with 10 ml extraction
solution (Tris buffered isotonic saline with 10 mm
CaCl, pH 8.4) in a high speed homogeniser, the
homogenate was then centrifuged for 20 minutes
before the supernatant was harvested, and
calprotectin levels were measured. C- Serum
osteopontin assessment using ELISA technique: (19) The OPN protein content in serum was
measured using a commercial ELISA according to
the manufacturer's instructions (Assay Designs,
Inc., Ann Arbor, MI, USA). Briefly, serum
samples were diluted, 1 : 20 and were incubated at
37°C for 1 h in microtiter plates precoated with a
polyclonal N-terminal capture anti-OPN antibody.
Then, the plate was washed and incubated at 4°C
for 30 min with a horseradish peroxidase labeled
OPN-specific monoclonal antibody. After
washing, the wells were incubated with

tetramethylbenzidine-H2O2 solution for 30 min.
The color reaction was stopped by adding a
solution containing 1 N sulfuric acid. Optical
densities were measured at 450 nm with reference
wavelength set at 590 nm. The OPN
concentrations were calculated using a standard
curve of recombinant humanOPN provided by the
manufacturer. 4. Colonoscopy and
Histopathological examination:(20) Patients
presenting to our Gastroenterology Centre with
symptoms meeting the RomeIII criteria for
diagnosis of IBS were undergoing routine
diagnostic colonoscopy to exclude inflammatory
bowel disease . Multiple biopsies from different
regions of the colon were taken for
histopathological evaluation. 5. Data were
collected, revised and transferred into statistical
package for social science (SPSS/ version 20).
Results were expressed as means and standard
deviation. Statistical tests used in this study were
(t.test & chi.square). A level of 5% was
considered as the cutoff level of significance.
Results
This study was carried out on 40 patients (group I)
who were fulfilling Rome III criteria for irritable
bowel syndrome (IBS),20 of them are IBS-D
(diarrhea predominant), 14 IBS-C (constipation
predominant) and 6 IBS-A (alternating diarrhea
and constipation). Both the patients (group I) and
control group (group II) were matched as regard
age and sex.(Table 1) Also there were no
statistical significant difference between the two
studied group as regard routine laboratory
investigations.(Table 2) Stool analysis was normal
in all subjects.
Table (1): Comparison between the two studied groups according to demographic data
IBS patients
(n = 40)
Controls
(n = 20) Test of sig. p
No % No %
Sex
Male 12 30.0 6 30.0 = 0.0 1.000
Female 28 70.0 14 70.0
Age
Min.- Max. 21.0 - 48.0 20.0 - 52.0 t = 0.655 0.515
Mean ± SD 32.78 ± 8.17 31.25 ± 9.14
p: p value for comparing between the two studied groups 2: Chi square test
t: Student t-test

Table (2): Comparison between the two studied groups according to routine laboratory investigations.
IBS patients
(n = 40)
Controls
(n = 20) t p
Albumin )g/dl)
Range 4.40 - 5.20 4.40 - 5.0 0.285 0.777
Mean ± SD 4.59 ± 0.26 4.57 ± 0.24
AST (u/l)
Range 16.0 - 21.0 16.0 - 21.0 0.056 0.955
Mean ± SD 18.67 ± 1.65 18.70 ± 1.56
ALT (u/l)
Range 12.0 - 22.0 12.0 - 21.0 0.502 0.618
Mean ± SD 15.13 ± 3.28 15.60 ± 3.79
Total billirubin(mg/dl)
Range 0.40 - 0.60 0.40 - 0.60 0.481 0.632
Mean ± SD 0.44 ± 0.05 0.45 ± 0.06
WBCs(th/mm3)
Range 5.58 - 9.90 5.58 - 9.90 0.319 0.751
Mean ± SD 7.81 ± 1.32 7.92 ± 1.29
RBCs (mi/ mm3)
Range 3.70 - 4.86 3.70 - 4.86 0.849 0.399
Mean ± SD 4.32 ± 0.31 4.39 ± 0.29
Plateletes (th/mm3)
Range 201.0 - 444.0 201.0 - 444.0 0.518 0.606
Mean ± SD 297.40 ± 78.03 286.35 ± 77.61
BL urea(mg/dl)
Range 17.0 - 33.0 17.0 - 33.0 0.195 0.846
Mean ± SD 23.20 ± 3.76 23.40 ± 3.73
Serum creatinine(mg/dl)
Range 0.40 - 0.90 0.40 - 0.90 0.561 0.577
Mean ± SD 0.72 ± 0.15 0.74 ± 0.15
FBG(mg/dl)
Range 80.0 - 123.0 80.0 - 107.0 0.483 0.631
Mean ± SD 91.45 ± 11.39 90.05 ± 8.74
PPS(mg/dl)
Range 100.0 - 139.0 100.0 - 120.0 0.695 0.490
Mean ± SD 111.23 ± 9.45 109.60 ± 6.26
t: Student t-test for comparing between the two studied groups
th = thousand, mi = million

As regard the markers of inflammation (Table
3): The mean erythrocytes sedimentation rate
(ESR) at the frist and second hour showed no
statistical significant difference between the
patients group (12.13 ± 2.05and 24.55 ±
3.17mm/hr respectively) and control group (11.80
± 2.38 and 23.25 ± 4.38 mm/hr respectively), with
[p = 0.586] in the first hour and [p = 0.194] in the
second hour.(Figure 1) The mean C-reactive
protein (CRP) was 4.44 ± 1.53 mg/l in group I,
4.13 ± 1.10 mg/l in group II, with no statistical
significant difference between the two groups [p =
0.432].(Figure 2) The mean fecal calprotectin
level was28.60 ± 19.24 mg/kg in group I, 21.75 ±
9.08 mg/kg in group II, with no statistical
significant difference between the two groups [p =
0.066].(Figure 3) The mean serum osteopontin
level was 2.92 ± 0.91in group I and 2.50 ± 0.78 in
group II with no statistical significant difference
between the two groups [p =0.086].(Figure4)
Table (3): Comparison between the two studied groups according to the markers of inflammation
IBS Cases
(n = 40)
Control
(n = 20) t p
ESR at 1st hrs (mm/hr)
Min.- Max. 8.0 - 15.0 7.0 - 15.0
0.548 0.586 Mean ± SD 12.13 ± 2.05 11.80 ± 2.38
Median 13.0 13.0
ESR at 2nd hrs (mm/hr)
Min.- Max. 20.0 - 31.0 15.0 - 31.0
1.315 0.194 Mean ± SD 24.55 ± 3.17 23.25 ± 4.38
Median 25.0 23.0
CRP (mg/l)
Min.- Max. 2.60 - 8.0 2.60 - 6.0
0.791 0.432 Mean ± SD 4.44 ± 1.53 4.13 ± 1.10
Median 4.0 4.0
Calprotectin (mg/kg)
Min.- Max. 10.0 – 65.0 10.0 – 45.0
1.872 0.066 Mean ± SD 28.60 ± 19.24 21.75 ± 9.08
Median 19.0 20.0
Osteopontin
Min. – Max 2.0 – 7.0 1.50 – 4.0
Mean ± SD 2.92 ± 0.91 2.50 ± 0.78 1.748 0.086
Median 2.80 2.25
t: Student t-test for comparing between the two studied groups
*: Statistically significant at p ≤ 0.05
Figure (1): Comparison between the two studied groups according to ESR.
0
5
10
15
20
25
ESR at 1st hrs ESR at 2nd hrs
Mea
n
Cases
Control

Figure (2): Comparison between the two studied groups according to CRP.
Figure (3): Comparison between the two studied groups according to fecal calprotectin
Figure (4): Comparison between the two studied groups according to serum osteopontin
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Cases Control
Mea
n o
f C
RP
0
5
10
15
20
25
30
Cases Control
Mea
n o
f C
alp
rote
ctin
(m
g/k
g)
0.00.20.40.60.81.01.21.41.61.82.02.22.42.62.83.03.2
Cases Control
2.92
2.5
Mea
n

As regard colonoscopic findings in IBS patients
(groupI) :
Hyperemia was found in 4 patients (10 %) ,polyps
was found in 2 patients (5 %), diverticulae, ulcers
and mass were not found in any patients . (Figure
5). Regarding histopathological findings of
colonoscopic biopsies in IBS patients : (Figure 6).
Non specific colitis was found in 30 patients (75
%) (Figure 7),10 patients (25 %) was normal
(Figure 8).Lymphocytic colitis was not found in
any patient (0 %).
Figure (5): Colonoscopic finding in IBS patients group
Figure (6): Histopathological findings of colonoscopic
biopsies in IBS patients
Figure (7): Low and high power view of chronically inflammed colonic mucosa showing colonic glands surrounded by stroma
infiltrated by inflammatory cells forming lymphoid follicles (H and E) (X10 and X40)
Figure (8): Low and high power view of normal colonic mucosa showing normally oriented colonic glands
(H and E) (X10 and X40)
0
20
40
60
80
100
120
Hyperemia Polyps Diverticulae Ulcers Mass
Per
cen
tag
e
No Yes
Normal10
25%
Lmphocytic colitis0
0%
Non specific colitis
3075%

Discussion
Irritable bowel syndrome (IBS) is one of the most
common functional gastrointestinal disorders and
is that with the greatest socioeconomic impact
worldwide. Although mortality is not increased,
some individuals experience high morbidity with
a profound impact on their ability to work and
enjoy life.(3) Diagnosis of IBS is based on clinical
criteria that have been modified over time, the
Rome III criteria(2) being those that are currently
followed. Importantly, signs of micro-
inflammation are found in the bowels of patients
with IBS.(8) The use of inflammatory markers in
stools (such as calprotectin) may help to
distinguish between IBS and IBD.(21)Osteopontin,
a cytokine which promotes Th1 immune
responses, is overexpressed in the gut of patients
with inflammatory bowel diseases. The main
cellular source of this cytokine appears to be gut
plasma cells. (22) The aim of this work was to find
out the diagnostic potential of osteopontin
biomarker in irritable bowel syndrome.This study
was carried out on 40 patients (group I) who were
fulfilling Rome III criteria for irritable bowel
syndrome (IBS) and the control (group II)
involved 20 healthy subjects of age and sex
matched as patients. All patients and controls
were subjected to clinical and laboratory
evaluation. Patients only (group I) were subjected
to colonoscopic and histopathological evaluation
of colonoscopic biopsies. In The present study we
found that about(50%) of the patients were IBS-D
(diarrhea predominant), (35%) were IBS-C
(constipation predominant) and (15%) were IBS-
A (alternating diarrhea and constipation). In
agreement, Chadwick et al (23) found that55%
were diarrhea predominant, 14% were
constipation predominant, and the remainder had
alternating symptoms. Also, El-Salhy et al(24)
found that 60% IBS-D and 40% IBS-C.In contrast
to our finding, Hod et al(25) found that 62% were
IBS-A, 26% were IBS-D and 12% IBS-C. The
inflammation is an important component of the
bowel wall structure. The amount of inflammation
is gradually increased from normal state, to
functional bowel disorders and to inflammatory
bowel disease.
As regard the results of systemic inflammatory
markers:
The present work showed that, no statistical
significant difference between the two groups
(patients and controls) as regard the mean
erythrocytes sedimentation rate level in the first
and second hours (ESR). This finding goes with
Hauser G et al(26) who found that no significant
correlation was found between ESR and the
disease severity in IBS. Also, Chadwick et al(23)
founds that ESR results were normal in Their IBS
patients. No significant difference was found in
the present study between the two groups (IBS
patients and controls) as regards mean serum C-
reactive protein level (CRP). This result was
similar with Chadwick et al (23) who concluded
that the CRP results were normal in their IBS
patients. However, Hod et al (25) found that mean
serum CRP levels are higher in IBS patients than
controls, but still in the normal laboratory range.
Another finding by Poullis et al (27) who reported
that, no significant difference was observed
between IBS constipation-predominant and
control while significant difference was detected
between IBS diarrhea-predominant and control
group. This difference from our study may be due
to the use of Hs-CRP in their studies. Both of the
latter (ESR, CRP), when used in isolation, give
significant ORs for predicting inflammatory
disease but are inferior compared with fecal
calprotectin. When assessed by the multiple
logistic regression model, both ESR and CRP
provide no additional discriminatory value over
and above calprotectin and Rome III criteria in
distinguishing between patients with
inflammatory and functional gastrointestinal
disrases.(28). The potential strength of fecal
calprotectin assessment is that it is a direct
measure of mucosal inflammatory activity that
may be detected at a level insufficient to cause an
increase in ESR and CRP, and levels in the stool
seem to be unaffected by a variety of non

intestinal conditions, which may result in an
elevation of the systemic inflammatory
markers.(28). In the present work we found that, no
statistical significant difference between the two
groups (IBS patients and healthy controls) as
regard the mean level of fecal calprotectin level.
This result was similar to Tibble et al(28) who
concluded that fecal calprotectin, intestinal
permeability, and positive Rome I criteria provide
a safe and noninvasive means of helping
differentiate between patients with organic and
nonorganic intestinal disease. Also, Li et al(29)
concluded that fecal calprotectin as a non-invasive
screening biomarker can be used as a biomarker
in exclusion of organic diseases before diagnosis
of irritable bowel syndrome. This also goes with
Grad et al(30) who concluded that fecal
calprotectin is a test which can differentiate
between IBD and IBS patients. As regard the
result of serum osteopontin, the present study
showed no statistical significant difference in the
serum level of osteopontin between the patients
with IBS and the healthy control group. This
result was in agreement with the previous results
of systemic inflammatory markers (ESR&CRP)
and fecal calprotectin .This result could be
explained by the role of osteopontin as a cytokine
that is upgrading only in the presence of
inflammation and that IBS is a functional non
organic gastrointestinal disorder (31&32). No
previous study has discussed the role of this
cytokine in IBS. Further study will be needed to
discuss the role of this cytokine as non invasive
biomarker to differentiate between IBS and IBD.
The indication of colonoscopy in IBS patients is
the presence of alarm symptomes like: bleeding
per rectum, unexplained iron deficiency anemia
and weight loss in old patients and family history
of cancer rectum or colon. (6)No one in our IBS
patients showed alarm symptomes. Patients
presenting to our Gastroenterology Centre with
symptoms meeting the RomeIII criteria for
diagnosis of IBS were undergoing routine
diagnostic colonoscopy to exclude inflammatory
bowel disease . All patients reported abdominal
pain. Regarding the findings of colonoscopy, in
the present study, colonoscopy was normal in
most of our patients (85%), hyperemia was found
in (10 %) and polyps was found in (5 %). In
agreement, Chadwick et al(23)found that,
colonoscopy was normal in all cases.Also El-
Salhy et al(24) found that, the colon and rectum of
the IBS patients and control subjects were
macroscopically normal.And also, Hilmi et
al(33)found that, the colonoscopic findings in the
IBS-D patients were; normal in (78.4%),
diverticula disease in (6.8%), polyps in (12.2%)
and haemorrhoids in (2.7%). Since the first
descriptions of microscopic colitis syndromes
(collagenous colitis and Lymphocytic Colitis), the
importance of obtaining mucosal biopsy
specimens when the colon is endoscopically
normal in patients with diarrhea has been widely
recognized. We extended this practice to patients
meeting the Rome III criteria for IBS, including
patients with diarrhea, constipation, or both.
Perhaps it is not surprising that some of these
patients turned out to have milder forms of
collagenous colitis, granulomatous colitis, or
Lymphocytic Colitis, because the Rome criteria
simply define a symptom complex and a diagnosis
of IBS has not required intestinal biopsy.(25). In
the present research, the results of
histopathological picture were as follow; non
specific colitis was found in (75 %) and (25 %)
was normal.Lymphocytic colitis was not found in
any patient (0 %). Those findings were in
agreement with Chadwick et al(23),who concluded
that examination of colonoscopic biopsy
specimens from patients meeting the Rome
criteria for a clinical diagnosis of irritable bowel
syndrome showed subgroups with normal and
abnormalconventional histology. All groups
showed increased numbers of activated
immunocompetent cells in the intestinal mucosa
on quantitative immunohistology. Also,De Silva
et al(34) found that there was evidence of
subclinical intestinal mucosal inflammation in
patients with IBS-D. They concluded that
Low-grade inflammation may, however, play an
important role in the pathogenesis of a subset of
IBS, namely post-infectious IBS (PI-IBS). In

contrast ,El-Salhy et al(24) showed that the
mucosal density of leucocytes as a whole and
lymphocytes, monocytes, macrophages and mast
cells in the rectum in the sporadic IBS patients did
not differ from that of the controls. These findings
oppose low-grade inflammation as a pathogenic
factor in sporadic IBS. This difference from the
present study may be due to use of control group
their work (these subjects underwent colonoscopy
due to gastrointestinal bleeding, where the source
of the bleeding was identified as haemorrhoids or
angiodysplasia and others were examined due to
health worries caused by a diagnosis of colon
carcinoma in a relative).
Conclusion
Osteopontin has no role as a diagnostic biomarker
in IBS. Further work on a larger patients sample
will be required to study the propabiltyle of the
use of osteopontin as non invasive biomarker in
the differential diagnosis between functional and
inflammatory gastrointesinal disorders.
References
1. Sperber AD, Drossman DA. Review article: the
functional abdominal pain syndrome. Aliment
Pharmacol Ther 2011; 33: 514-24.
2. Drossman DA. The functional gastrointestinal
disorders and the Rome III process.
Gastroenterology 2006;130:1377-90.
3. Elsenbruch S. Abdominal pain in Irritable Bowel
Syndrome: A review of putative psychological,
neural and neuro-immune mechanisms. Brain
Behav Immun 2010;25:386-94.
4. Kassinen A, Krogius-Kurikka L, Mäkivuokko
H. The fecal microbiota of irritable bowel
syndrome patients differs significantly from that of
healthy subjects. Gastroenterology 2007;133(1):24-
33.
5. Longstreth GF, Thompson WG, Chey WD,
Houghton LA, Mearin F, Spiller RC. Functional
bowel disorders. Gastroenterology 2006;130:1480-
91.
6. Dizdar V, Gilja OH, Hausken T. Increased visceral
sensitivity in Giardia-induced postinfectious
irritable bowel syndrome and functional dyspepsia.
Effect of the 5HT3-antagonist ondansetron.
Neurogastroenterol Motil 2007;19:977-82.
7. Nobaek S, Johansson ML, Molin G, Ahrné S,
Jeppsson B. Alteration of intestinal microflora is
associated with reduction in abdominal bloating
and pain in patients with irritable bowel syndrome.
Am J Gastroenterol 2000;95:1231-8.
8. Ortiz-Lucas M, Saz-Peiró P, Sebastián-Domingo
JJ.Irritable bowel syndrome immune hypothesis.
Part one: the role of lymphocytes and mast
cells.Rev Esp Enferm Dig 2010;102:637-47.
9. Grover M, Herfarth H, Drossman DA. The
functional-organic dichotomy: post infectious
irritable bowel syndrome and inflammatory bowel
disease irritable bowel syndrome. Clin
Gastroenterol Hepatol 2009; 7:48-53.
10. Langhorst J, Elsenbruch S, Koelzer J, Rueffer A,
Michalsen A, Dobos GJ. Noninvasive markers in
the assessment of intestinal inflammation in
inflammatory bowel diseases: performance of fecal
lactoferrin, calprotectin, and PMN-elastase, CRP,
and clinical indices. Am J Gastroenterol
2008;103:162-9.
11. Otten CM, Kok L, Witteman BJ, Baumgarten R,
Kampman E, Moons KG, de Wit NJ. Diagnostic
performance of rapid tests for detection of fecal
calprotectin and lactoferrin and their ability to
discriminate inflammatory from irritable bowel
syndrome. Clin Chem Lab Med 2008; 46:1275-80.
12. Lasson A. Calprotectin in feces a well-documented
marker of gastrointestinal inflammation. Indicates
disease intensity--normalization of values predict
mucosal healing.Lakartidningen 2010; 107:2645-9.
13. Sun Y, Yin XS, Guo H, Han RK, Rui Dong He, Li
Jun Chi. Elevated osteopontin level in Mild
Cognitive Impairment and Alzaheimer's Diseases.
Mediator of inflammation 2013;2013:515745
14. Neuman MG.Osteopontin biomarker in
inflammatory bowel disease,animal models and
target for drug discovery. Dig Dis Sci
2012;57:1430-31
15. Ashkar S, Weber GF, Panoutsakopoulou V, et al.
Eta-1 (osteopontin): an early component of type-1
(cell-mediated) immunity. Science. 2000;287:860–
864
16. Gordon JN, MacDonald TT. Osteopontin: a new
addition to the constellation of cytokines which
drive T helper cell type 1responses in Crohn’s
disease. Gut 2005; 54:1213–5.
17. Glas J, Seiderer J, Bayrle C, et al. The role of
osteopontin (OPN/SPP1) haplotypes in the

susceptibility to Crohn’s disease. PLoS ONE.
2011;6:e29309.
18. Ton H, Brandsnes O, Dale S, et al. Improved assay
for fecal calprotectin, Clin Chim Acta.
2000;292:41-54.
19. Mishima R, Takeshima F, Sawai T, Ohba K, Ohnita
K,Isomoto H,Omagari K,Mizuta
Y,OzonoY,KohnoS.High plasma osteopontin levels
in patients with inflammatory bowel disease. J Clin
Gastroentrol.2007;41(2):67-72.
20. Lucak S. Diagnosing irritable bowel syndrome:
what's too much, what's enough? MedGenMed
2004;6(1):17.
21. Mearin F, Perelló A, Balboa A.Irritable bowel
syndrome and inflammatory bowel disease: Is there
a connection?Gastroenterol Hepatol. 2009 May 11.
22. Glas J, Seiderer J, Bayrle C, et al. The role of
osteopontin (OPN/SPP1) haplotypes in the
susceptibility to Crohn’s disease. PLo Sone
2011;6:e29309.
23. Chadwick VS, Chen W, Shu D, et al. Activation of
the mucosal immune system in irritable bowel
syndrome.Gastroenterol 2002;122:1778.
24. El-Salhy M, Gundersen D, Hatlebakk JG, Hausken
T. Low-grade inflammation in the rectum of
patients with sporadic irritable bowel syndrome.
Mol Med Rep 2013;7(4):1081-5.
25. Hod K, Dickman R, Sperber A, Melamed S, Dekel
R, Ron Y, et al. Assessment of high- sensitivity
CRP as a marker of micro-inflammation in irritable
bowel syndrome. NeurogastroentrolMotil
2011;23(12):1105-10.
26. Hauser G, Tkalcic M, PletikosticS,Grabar N,
StimacD.Erythrocyte sedimentation rate-possible
role in determining the existence of the low grade
inflammationin irritable bowel syndrome patients.
Med Hypotheses2012; 78(6):818-20.
27. Poullis A, Foster R, Mendall MA, Fagerhol MK.
Emerging role of calprotectin in gastroenterology. J
Gastroenterol Hepatol 2003, 18: 756.
28. Tibble JA, Sigthorsson G, Foster R, Forgacs I,
Bjarnason I. Use of surrogate markers of
inflammation and Rome criteria to distinguish
organic from non organic intestinal disease.
Gastroentrol 2002;123:450-60.
29. Li XG, Lu YM, Gu F, Yang XL. Fecal
calprotectinin differential diagnosis of irritable
bowel syndrome. Beijing Da XueXueBao
2006;38(3):310-3.
30. Grad C, David L, Portinacasa P, Dumitrascu DL.
Diagnostic value of calprotectin in irritable bowel
syndrome and inflammatory bowel diseases. Rom J
Intern Med 2012;50(1): 3-6.
31. MacDonald TT, Monteleone G. Immunity,
inflammation and allergy in the gut.
Science2005;307:1920–25.
32. Sato T, Nakai T, Tamura N, et al. Osteopontin/Eta-
1 upregulated in Crohn’s disease regulates the Th1
immune response. Gut2005;54:1254–62.
33. Hilmi I, Hartono JL, Pailoor J, Mahadeva S, Goh
KL. Low prevalence of 'classical' microscopic
colitis but evidence of microscopic inflammation in
Asian irritable bowel syndrome patients with
diarrhoea. BMC Gastroenterol.2013; 8;13:80.
34. De Silva AP, Nandasiri SD, Hewavisenthi J,
Manamperi A, Ariyasinghe MP, Dassanayake AS,
et al. Subclinical mucosal inflammation in diarrhea-
predominantirritable bowel syndrome (IBS) in a
tropical setting. Cand J Gastroenterol 2012;
47(6):619-24.

Original Article
Fecal Calprotectin as a Screening Parameter for Hepatic Encephalopathy and
Spontaneous Bacterial Peritonitis in HCV Related Hepatic Cirrhosis
Mohamed Y. El Hasafy1, MD, Ahmed H. Yosry2, MD., Amany S. Elyamany1, Eman E. Hemimi1 1Department of Medicine (Hepatobiliary Unit), Faculty of Medicine, University of Alexandria, Alexandria, Egypt. 2Department of Clinical Pathology, Institute of Medical Research, University of Alexandria, Alexandria, Egypt.
ABSTRACT
Hepatitis C virus (HCV) continues to be a major health problem. The highest prevalence rate of HCV infection in the
world was recently reported among Egyptian blood donors, reaching about 15-20% in the general population.
Approximately one fifth of patients with chronic hepatitis C develop cirrhosis over a time period of 10-30 years. Once
cirrhosis has developed, complications including gastrointestinal bleeding, hepatic encephalopathy (HE), ascites,
spontaneous bacterial peritonitis (SBP) are common. Bacterial translocation (BT) is one of the most common path
physiological mechanisms of SBP and HE. Calprotectin is an interesting peptide, proposed as a biomarker for various
inflammatory diseases due to its potential role in the pathophysiology of inflammation associated with tissue
destruction, apoptosis and growth impairment. Aim of the study: Evaluation of the relationship between fecal
calprotectin, SBP and HE, and its potential role as screening parameter for them. Materials and Methods: This study
included fifty patients. They were classified into four groups. Group I: included 15 patients with HCV related hepatic
cirrhosis and SBP. Group II: included 15 patients with HCV related hepatic cirrhosis and HE. Group III: included 10
patients with HCV related hepatic cirrhosis without SBP, HE. Group IV: included 10 healthy individuals. Fecal
calprotectin level was measured in all subjects. Results: Fecal calprotectin level showed significantly higher level in
patients with SBP and in HE patients compared to cirrhotic patients and control group. The median level of fecal
calprotectin in group I, II, III was127, 115, and 32.5 respectively compared to control group, which was 18. There was a
significant increase in level of fecal calprotectin with the grade of HE. Also significant increase its level with advanced
Child-Pugh scoring. Conclusion: Fecal calprotectin can be used as screening parameter for SBP and HE in HCV
related liver cirrhosis.
Introduction
Hepatitis C virus is considered as a major health
problem. Egypt is the country with the highest
prevalence in the world based on a Demographic
Health Survey which was carried out in Egypt in
2008. (1, 2, 3, 4, 5). Approximately 20-30% of patients
with chronic hepatitis C develop cirrhosis over a
time period of 10-30 years. Once cirrhosis has
developed, complications including gastro-
intestinal bleeding, portosystemic encephalopathy
and ascites are common. (6, 7). Cirrhotic patients
are prone to develop bacterial infections, mainly
SBP. It is the most frequent and life-threatening
infection in patients with liver cirrhosis requiring
prompt recognition and treatment. SBP is present
in approximately 15% of patients with cirrhosis
and ascites. In-hospital mortality for the first
episode of SBP ranges from 10- 50 %.( 8, 9, 10) In
fact, the occurrence of SBP or other severe
bacterial infections markedly worsens the
prognosis in patients with cirrhosis, so-called
‘‘critically ill cirrhotic”. Patients at this late stage
have to be evaluated for the possibility of liver
transplantation. (11). Hepatic encephalopathy is a
neuropsychiatric syndrome seen in liver
dysfunction or in Porto-systemic shunting without
liver dysfunction. This potentially reversible
condition is associated with both acute and
chronic liver disease. (12). Pathological BT plays
an important role in the pathogenesis and
complications of cirrhosis as SBP and HE. Three
factors have been implicated in the development
of pathological BT in liver cirrhosis which are:
alterations in gut microbiota; increased intestinal

permeability; and impaired immunity. (13). Also
altered small bowel motility, delayed intestinal
transit, hypochlorhydria, decrease in intraluminal
immunoglobulin’s, and reduced secretion of IgA
in cirrhotic leads to bacterial overgrowth in the
small intestine, which worsens with increasing
severity of liver disease.(14). Fecal calprotectin is
an interesting peptide, proposed as a biomarker
for various inflammatory diseases. As acute phase
reactant, calprotectin increases more than 100
folds during inflammatory conditions.(15)
Neutrophils and monocytes are the first cells that
migrate to the inflammatory sites where they carry
out defense mechanisms like phagocytosis,
release of reactive oxygen species (ROS),
enzymes and antimicrobial peptides. Calprotectin
triggers degradation of endothelial cell tight
junction which induces the migration of
neutrophils and monocytes to the site of
inflammation. (16) Fecal calprotectin is a well-
established marker of inflammation and is used to
monitor inflammatory bowel disease. (17). As the
gastrointestinal tract of cirrhotic patients shows
various alterations of its mucosal barrier including
infiltrates of neutrophils, calprotectin might be a
promising diagnostic parameter to diagnose the
onset and course of HE and SBP. (18)
Aim of The Work
The aim of this work was to study the significance
of fecal calprotectin as a screening test for HE and
SBP in HCV related hepatic cirrhosis and
comparison of its level with that of normal
subjects. Also to test for correlation of fecal
calprotectin level with the grade of HE, role of
fecal calprotectin as a non invasive diagnostic
marker for of SBP.
Patients and Methods
The present study was conducted on 40 patients
diagnosed as HCV related hepatic cirrhosis; who
were referred to the Hepatobiliary Unit,
Department of Internal Medicine, The Main
University Hospital, Alexandria Faculty of
Medicine. They were 29 males and 11 females
and their ages ranged between 35 and 68 years
(mean ± SD = 42.2±15.5 years). All patients had
clinical, laboratory and radiological findings
consistent with hepatic cirrhosis and seropositivity
for circulating HCV antibodies. Exclusion criteria
included seropositivity for HBV infection; history
of alcohol consumption; known patients with
inflammatory bowel disease, patients with active
gastrointestinal bleeding, secondary peritonitis,
neurological and psychiatric diseases that might
be misdiagnosed as HE such as cerebral
hemorrhage and seizures, colorectal carcinoma,
cirrhotic patients with esophageal varices grade
IV or with sever portal hypertensive gastropathy
and chronic use of certain drugs as (NSAIDS,
anticoagulant, proton pump inhibitors). Also, 10
age- and sex-matched healthy subjects with no
evidence of liver disease were included in the
study as a control group to obtain normal ranges
of biochemical assays. They were 6 males and 4
females and their ages ranged between 22-68
years (mean ± SD = 42.2 ±15.5years). Subjects
were divided into four groups as follow: Group I:
Fifteen patients with HCV related hepatic
cirrhosis with proved diagnosis of SBP
(neutrophils in ascitic fluid > 250/mm³) and
ascetic fluid culture. Group II: Fifteen patients
with HCV related hepatic cirrhosis with HE.
Group III: Ten patients with HCV related hepatic
cirrhosis, with no evidence of HE or SBP. Group
IV: Ten age- and sex-matched healthy subjects
with no evidence of liver disease were included as
control group. After the approval of ethical
committee was taken. The study was conducted in
accordance with the provisions of the Declaration
of Helsinki and Good Clinical Practice guidelines.
An informed consent was obtained from all
subjects prior to procedures initiation. Once
admitted into the study, the base line assessment
included: age, gender, symptoms and signs of
chronic liver disease, liver and spleen size, serum
albumin, serum bilirubin, serum aspartate and
alanine aminotransferases (AST and ALT
respectively), serum gamma glutamyl
transpeptidase (GGT), prothrombin time,
international normalized ratio and serum
creatinine. HCV antibodies, hepatitis B surface

antigen and anti HBc Abs using enzyme linked
immunosorbent assay (ELISA). Abdominal
ultrasonographic examination was used to assess
of: liver echo pattern and size. Upper
gastrointestinal endoscopy was performed. Fecal
calprotectin is a quantitative enzyme-linked
immunoassay for the detection of calprotectin in
feces, which uses polyclonal antibody against
calprotectin. Calprotectin present in the diluted
sample is bound by the antibody adsorbed to the
surface of the plastic well. The enzyme
conjugated antibody binds to the captured antigen
and subsequently to a colored product. The
intensity of the color is proportional to the amount
of conjugate bound, and thus to the amount of
captured calprotectin in the samples which is
calculated using the provided standards.
Statistical Analysis:
Data were collected and entered into the personal
computer. Statistical analysis was done using the
Statistical Package for Social Sciences (SPSS/
version 11) software. Results were expressed as
percentages, means and standard deviations (SD).
The Student’s t test was used as a test of
significance for comparison between two
arithmetic means. The Pearson correlation
coefficient used to find the strength of correlation
("r" value) between continuous quantitative
variables. The Spearman rho correlation
coefficient used to find the strength of correlation
("r" value) between discontinuous quantitative
variables. The 5% level was chosen as the cut-off
level of significance.
Table (1): Statistical analysis
GI cirrhotic with
SBP
GII cirrhotic with
HE
GIII cirrhotic
without SBP or HE GIV control
Age(years) 50.4± 9.9 50.9± 7.7 49.5± 9.9 42.2 ±15.5
Gender:Male 73.3% 66.7% 80.0% 60.0%
Serum albumin
Mean ± SD 1.8 ±0.2 1.7 ±0.2 2.2 ±0.6 4.2±0.3
GGT
Mean ± SD 33.3±1.5 56.7±41.9 32.5±0.7 22±2
INR
Mean± SD 1.5±0.3 1.6±0.4 1.4±0.3 0.8±0.2
Fecal calprotectin
Mean ± SD 150.9±58.9 147.8±61.9 34.5±7.9 23.5±11.0
Results:
There was no correlation between age, gender and
level of fecal calprotectin in the studied groups.
The median value for fecal calprotectin (mg/kg) in
GI, GII, GIII, and G IV was 127,115, 32.5, and 18
respectively. There was a significant difference
between the studied groups as regard fecal
calprotectin, P < 0.05 (P= 0.000). Figure (1)

Figure (1): Comparison between studied groups as regard
fecal calprotectin.
GI: Group I, GII: Group II, GIII: Group III, GIV:
Group IV. The cut off value for fecal calprotectin level for
predicting SBP or HE in HCV related cirrhosis was 95
mg/kg with a sensitivity of 96.67% and specificity of
100%, area under the curve of 1 (fig 2) .
Figure (2): ROC curve for the diagnostic performance of
fecal calprotectin for SBP and HE
Table (2): Agreement for fecal calprotectin level with the diagnosis of SBP and HE in HCV related hepatic cirrhosis
No SBP
or H.E
SBP or
H.E
Sen
siti
vit
y
Sp
ecif
icit
y
PP
V
NP
V
Acc
ura
cy
Fecal calprotectin ≤95 10 1 96.
67
100
.0
100
.0
90.
91
97.5
0 >95 0 29
PPV: positive predictive value., NPV: negative predictive value.
A positive correlation was found between fecal
calprotectin level and advanced child- Pugh score.
There was significant difference between the studied
groups as regard Child-Pugh Scoring& fecal
calprotectin, P < 0.05 (P= 0.042). Figure (3)
Figure (3): Correlation between studied groups as regard fecal calprotectin and Child Pugh scoring.
Group IVGroup IIIGroup IIGroup I
Group
400.00
300.00
200.00
100.00
0.00
Fecal calp
rote
cti
n
25
32
24
0
20
40
60
80
100
120
140
160
180
200
B8 B9 C10 C11 C12 C13
Mea
n o
f fe
cal ca
lpro
tect
in
Child score
AUC p
Fecal
calprotectin 1.000* <0.001

A positive correlation was found between fecal
calprotectin level and HE grade, there was a
significant positive correlation between its levels with
increased grade of HE, P < 0.05 (P=0.009). Figure (4)
Figure (4): Correlation between levels of fecal
calprotectin with grade of HE.
HE: Hepatic encephalopathy, GI-II: Grade I-II hepatic
encephalopathy, GII: Grade II hepatic encephalopathy, GII-
III: Grade II-III hepatic encephalopathy, GIII: Grade III
hepatic encephalopathy.
There was a significant decrease in level of fecal
calprotectin after treatment of SBP. Figure (5)
Figure (5): Comparison between study phase and fecal
Calprotectin before and after treatment.
Fecal calprotectin level showed no significant difference in patients presented by both of SBP and HE in
comparison to patients in GI or GII, P= 0.930. Figure (6)
Figure (6): Comparison fecal calprotectin in patients with H.E&SBP and in patients with both.
SBP: Spontaneous bacterial peritonitis, HE: Hepatic encephalopathy, Combined: Having both Spontaneous bacterial
peritonitis and Hepatic encephalopathy.
Disscusion
In the present study, the median FCCs were
significantly higher in cirrhotic patients with SBP
compared with cirrhotic patients without SBP and
control group. Despite of a careful exclusion of other
causes of abnormal calprotectin results e.g. GI
bleeding. As the GI tract of cirrhotic patients shows
various alterations of its mucosal barrier including
infiltrates of neutrophils, In agreement with these
results, Gundling et al (2011) (18) found that fecal
calprotectin level was higher in cirrhotic with SBP
when compared with cirrhotic without SBP or
0
50
100
150
200
250
GI GI-II GII GII-III GIII
Mea
n o
f fe
cal
calp
rote
ctin
Grade0
20
40
60
80
100
120
140
Before treatment After treatmentM
ea
n o
f f
eca
l ca
lpro
tecti
n
0
20
40
60
80
100
120
140
160
SBP(GI) HE(GII) Combined
Mea
n o
f fe
cal ca
lpro
tect
in

control group. This finding suggests that calprotectin
in cirrhotic patients can be considered as a valid
marker of intestinal inflammation. This could be
explained that cirrhotic patients are in particular
susceptible to bacterial infections because of
increased migration of bacteria or bacterial products
from the intestinal lumen related to liver dysfunction
and reduced reticuloendothelial function (19). An
altered gut flora and BT are known to play an
important role in the pathogenesis of certain
complications of cirrhosis such as HE and SBP. (20).
The mucosal epithelium per se closely interacts with
antigen-presenting cells beneath and intraepithelial
lymphocytes (IEL) within the lamina propria to
maintain intestinal integrity. In human cirrhosis,
structural changes of the intestinal mucosa including
widening of intercellular spaces, vascular
congestion, edema, fibro muscular proliferation,
decreased villous to crypt ratio, and thickening of
the muscularis mucosa have been described (21,22).
Therefore, in cirrhotic conditions, loosening of tight
junctions (TJs) may result in an increased
accessibility of bacterial products to areas of ‘‘free’’
passage. However, most critical for the translocation
of living whole bacteria is the transcellular route.
e.g., for E. coli. (23). In this study culture ascitic fluid
was sterile in 73% of cases of patients with SBP ,
20% E.coli and 6.6% Klebsiella in accordance with
Wiest R et al. which proved that classical culture
techniques fail to grow bacteria in up to 65% of
neutrocytic ascites. Bedside inoculation of ascites
into blood culture bottles has been shown to increase
the sensitivity to nearly 80%. Handling processes
influence culture results and delay in transport
increases false negative results.(24) Also E.coli was
most common isolated organism in culture positive
ascites followed by Klebsiella in accordance with
Angeloni S et al. (25). In our study, a significant
correlation emerged between elevated FCCs and
HE grading as measured by West–Haven criteria
and FCC .This was in accordance with Gundling
et al (2011) (18) which demonstrated that not only
higher FCCs levels with cirrhotic with HE but
also increases with advanced grade of HE. This
explained by progression to severe HE is
associated with infection.(26)The exposition of
astrocytes to cytokines in cultures induces
astrocyte swelling, which is considered a
neuropathological hallmark of HE.(27) Also
enhanced production of reactive nitrogen species
(RNS) and reactive oxygen species (ROS) occurs
in cultured astrocytes that are exposed to
ammonia, inflammatory cytokines, hyponatremia
or benzodiazepines.(28) Increase the permeability
of the blood–brain barrier, which ultimately
promotes astrocyte swelling and cerebral
edema.(27). In the present study, median FCCs
were significantly higher with advanced liver
disease assessed by Child-Pugh scoring, In
accordance with Gundling et al. (2011) (18) that
document that FCCs are significantly elevated in
cirrhotic patients dependent on the severity of
liver disease. This may be explained that with
advanced cirrhosis associated with structural and
functional alterations in the intestinal mucosa that
increase permeability to bacteria and bacterial
products, Also Altered small bowel motility
favors small intestinal bacterial overgrowth and
impaired immunity with advanced liver disease
liver dysfunction and cirrhosis is accompanied by
deficits in innate and adaptive intrahepatic,
intestinal and systemic immunity. (29, 30, 31, 32, 33).
Rate and degree of pathological BT increase with
severity of liver disease. Pathological
translocation of vital bacteria to MLN is a
phenomenon of the decompensated stage. These
data are in accordance with studies in cirrhotic
patients demonstrating significant increases in
lipopolysaccharide-binding-protein (long-term
marker of gram negative pathological BT) and
intestinal permeability in ascitic cirrhotic but not
in patients without ascites as compared to healthy
controls. Also SIBO is observed in increasing
frequency with worsening of severity of liver
diseases, reaching incidences above 80% in
advanced cirrhotic patients with ascites.
Moreover, direct data on culturable BT to MLN
revealed a significantly higher rate in Child C
cirrhotic patients (30%) as compared to Child B or
A (8% and 3%, respectively) patients and Child-
Pugh score was the only independent predictor for
pathological BT(34, 35, 36, 37, 38, 39). Furthermore, the

present study demonstrated that a higher
prevalence of diabetes mellitus in the studied
groups with higher incidence of SBP and HE. In
accordance with Jamil S et al. (2011) which
demonstrated diabetus as one of the predicting
factors not only for SBP but also for its
recurrence. (40) The possible mechanism can be
altered immunity and deficiencies in complement
system with depressed functions of neutrophils
and macrophages in patients with cirrhosis. It has
been proven that cirrhotic patients with low level
of serum C3 and C4 are more prone to develop
BT. So that DM as co-morbid was a significant in
patients having recurrence of SBP. (40) . Patients
with HCV-related liver cirrhosis are associated
with a significantly higher prevalence of DM than
those cirrhotic patients with other etiologies.
Increasing prevalence of type 2 diabetus with
severity of sonographic stages in anti-HCV-
positive subjects implies that viral inflammatory
activity, time duration, insulin secretion, insulin
sensitivity, and the interaction with other well-
known diabetes risk factors appear to play an
important role in the development of T2D. In
accordance with Elhawary E et al. (2011) (41) that
demonstrated close relationship between HCV
infection and DM. may be explained that a more
severe inflammatory and fibrotic process were
associated with diabetes suggest that the
pathogenesis of DM in HCV infection may be
multifactorial- a precirrhotic state leading to an
abnormal glucose metabolism and insulin
resistance, acting in conjunction with undefined
pancreatic damage, occurring in genetically prone
patients is an explanation is that β-cell
responsiveness is impaired in patients with HCV,
possibly because of direct viral effects on β-cell
function. Thus for a given degree of liver
dysfunction-and presumably IR, diabetes would
be more likely to occur in patients with HCV.
Consistent with Ampuero J et al. (2013), HE was
more prevalent in diabetic patients. (42) This
explained by that the main cognitive dysfunction
in cirrhotic patients associated with impaired
prognosis. Hyper-ammonemia plus inflammatory
response do play a crucial role on HE. DM and
insulin resistance are characterized by releasing
and enhancing these pro-inflammatory cytokines
and, additionally, has been related to HE. Indeed,
patients with diabetes showed raised risk of overt
HE in comparison with non-cirrhotic. Type 2 DM
could worsen grade of HE by different
mechanisms that include: a) increasing
glutaminase activity; b) impairing gut motility
and promoting constipation, intestinal bacterial
overgrowth and BT. (42). Level of FCC was
assessed after treatment of five patients (one of
them had SBP and four had both SBP and HE)
and compared to the pre-treatment level. It
showed a significant decrease in post- treatment
FCC level. Median value of FCC before treatment
(114.00) compared by post treatment value
(31.50) (P= 0.052). Even though diagnostic
paracentesis is regarded as a safe procedure, there are
undoubtedly complications inherent with the test. These
include bleeding, visceral perforation, local infection and
persistent leak. (18) However, diagnostic alternatives are
sparse. The use of diagnostic tools such as leucocyte
esterase reagent strips, pH testing or analysis of
procalcitonin and lactoferrin of ascitic fluid is doubtful
.Therefore, a simple, non-invasive, rapid and cheap
screening test to make a presumptive diagnosis of HE and
SBP in cirrhotic patients would help to reach these
goals.(18)
Conclusion:
Fecal calprotectin can be used as a screening
parameter for SBP and HE.
References:
1. Guerra J, Garenne M, Mohamed MK, Fontanet A.
HCV burden of infection in Egypt: results from a
nationwide survey. J Viral Hepat 2012; 19(8):560-
7.
2. World Health Organization (WHO). World Health
Report 2002.Annex table 2: deaths by cause, sex
and mortality strarum in WHO regions, estimates
for 2001. Available from:
www.who.int/entity/whr/2002/en/whr/2002-
annex2.pdf. [Accessed On: 1 Jan, 2013].
3. Lai CL, Ratziu V, Yuen MF, Poynard T. Viral
hepatitis B. Lancet 2003; 362:2089-94.

4. El-Serag HB. Hepatocellular carcinoma: an
epidemiologic view. J Clin Gastroenterol 2002;
35:S72-8.
5. NIH Consensus Statement on Management of Hepatitis
C. NIH Consens State Sci Statement 2002; 19(3):1-46.
6. Alter MJ. Epidemiology of hepatitis C in the West.
Semin Liver Dis 1995; 15:5-14.
7. Alazawi W, Cunningham M, Dearden J, Foster GR.
Systematic review: outcome of compensated
cirrhosis due to chronic hepatitis C infection.
Aliment Pharmacol Ther 2010; 32: 344-55.
8. Pinzello G, Simonetti RG, Craxì A, Di Piazza S,
Spanò C, Pagliaro L. Spontaneous bacterial
peritonitis: a prospective investigation in
predominantly nonalcoholic cirrhotic patients.
Hepatology 1983; 3:545-9.
9. Follo A, Llovet JM, Navasa M, Planas R, Forns X,
Francitorra A, et al. Renal impairment after
spontaneous bacterial peritonitis in cirrhosis:
incidence, clinical course, predictive factors and
prognosis. Hepatology 1994; 20:1495-501.
10. Toledo C, Salmerón JM, Rimola A, Navasa M,
Arroyo V, Llach J, et al. Spontaneous bacterial
peritonitis in cirrhosis: predictive factors of
infection resolution and survival in patients treated
with cefotaxime. Hepatology 1993; 17:251-7.
11. Arvaniti V, D’Amico G, Fede G, Manousou P,
Tsochatzis E, Pleguezuelo M. et al. Infections in
patients with cirrhosis increase mortality four-fold and
should be used in determining prognosis.
Gastroenterology 2010; 139:1246–56.
12. Ferenci P, Lockwood A, Mullen K, Tarter R,
Weissenborn K, Blei AT. Hepatic encephalopathy--
definition, nomenclature, diagnosis, and
quantification: final report of the working party at
the 11th World Congresses of Gastroenterology,
Vienna, 1998. Hepatology 2002; 35:716-21.
13. Wiest R, Garcia-Tsao G. Bacterial translocation
(BT) in cirrhosis. Hepatology 2005; 41:422-33.
14. Thalheimer U, Triantos CK, Samonakis DN, Patch
D, Burroughs AK. Infection, coagulation, and
variceal bleeding in cirrhosis. Gut 2005; 54(4):556-
63.
15. Golden BE, Clohessy PA, Russell G, Fagerhol MK.
Calprotectin as a marker of inflammation in cystic
fibrosis. Arch Dis Child 1996; 74:136-9.
16. Irving WL. Acute hepatitis C virus infection: a
neglected disease?. Gut 2006; 55:1075-7.
17. Wassell J, Wallage M, Brewer E. Evaluation of the
Quantum Blue® rapid test for faecal calprotectin.
Ann Clin Biochem 2012; 49: 55-8.
18. Gundling F, Schmidtler F, Hapfelmeier A, Schulte
B, Schmidt T, Pehl C, et al. Fecal calprotectin is a
useful screening parameter for hepatic
encephalopathy and spontaneous bacterial
peritonitis in cirrhosis. Liver Int 2011; 31:1406–15.
19. Garcia-Tsao G, Wiest R. Gut microflora in the
pathogenesis of the complications of cirrhosis. Best
Pract Res Clin Gastroenterol 2004; 18:353–72.
20. Wong F, Bernardi M, Balk R, Christman B, Moreau
R, Garcia-Tsao G, et al. Sepsis in cirrhosis: report
on the 7th meeting of the internatinal ascites club.
Gut 2005; 54: 718–25.
21. Astaldi G, Strosselli E. Peroral biopsy of the
intestinal mucosa in hepatic cirrhosis. Am J Dig Dis
1960;5: 603–12.
22. Misra V, Misra S, Dwivedi M, Gupta S.
Histomorphometric study of portal hypertensive
enteropathy. Am J Clin Pathol 1997;108:652–7.
23. Wiest R, Lawson M, Geuking M. Pathological
bacterial translocation in liver cirrhosis. J Hepatol
2013; S0168-8278(13): 602-8.
24. Wiest R, Krag A, Gerbes A. Spontaneous bacterial
peritonitis: recent guidelines and beyond. Gut 2012;
61(2):297-310.
25. Angeloni S, Leboffe C, Parente A, Venditti M,
Giordano A, Merli M,, et al. Efficacy of current
guidelines for the treatment of spontaneous
bacterial peritonitis in the clinical practice. World J
Gastroenterol 2008; 14:2757-62.
26. Vaquero J, Polson J, Chung C, Helenowski I,
Schiodt FV, Reisch J, et al. Infection and the
progression of hepatic encephalopathy in acute liver
failure. Gastroenterology 2003; 125:755-64.
27. Ha¨ussinger D, Schliess F. Astrocyte swelling and
protein tyrosine nitration in hepatic encephalopathy.
Neurochem Int 2005; 47 ;( 1–2):64–70.
28. Murthy CR, Rama-Rao KV, Bai G, Norenberg MD.
Ammonia-induced production of free radicals in
primary cultures of rat astrocytes. J Neurosci Res
2001; 66: 282–98.
29. Bauer TM, Steinbrückner B, Brinkmann FE, Ditzen
AK, Schwacha H, Aponte JJ, et al. Small intestinal
bacterial overgrowth in patients with cirrhosis:
prevalence andrelation with spontaneous bacterial
peritonitis. Am J Gastroenterol 2001; 96:2962-7.
30. Pardo A, Bartolí R, Lorenzo-Zúñiga V, Planas R,
Viñado B, Riba J, et al. Effect of cisapride on

intestinal bacterial overgrowth and bacterial
translocation in cirrhosis. Hepatology 2000;
31:858-63.
31. Chiva M, Guarner C, Peralta C, Llovet T, Gómez
G, Soriano G, et al. Intestinal mucosal oxidative
damage and bacterial translocation in cirrhotic rats.
Eur J Gastroenterol Hepatol 2003; 15:145-50.
32. Ramachandran A, Prabhu R, Thomas S, Reddy JB,
Pulimood A, Balasubramanian KA. Intestinal
mucosal alterations in experimental cirrhosis in the
rat: role of oxygen free radicals. Hepatology 2002;
35:622-9.
33. Altman C, Grangé JD, Amiot X, Pelletier G, Lacaine F,
Bodin F, et al. Survival after a first episode of
spontaneous bacterial peritonitis. Prognosis of potential
candidates for orthotopic liver transplantation. J
Gastroenterol Hepatol 1995; 10:47-50.
34. Wiest R, Das S, Cadelina G, Garcia-Tsao G,
Milstien S, Groszmann RJ. Bacterial translocation
in cirrhotic rats stimulates eNOS-derived NO
production and impairs mesenteric vascular
contractility. J Clin Invest 1999;104:1223–33.
35. Albillos A, DelaHera A, Gonzalez M, Moya J, Calleja J,
Monserrat J,
et al. Increased lipopolysaccharide binding protein in
cirrhotic patients with marked immune and
hemodynamic derangement. Hepatology 2003; 37:208–
17.
36. Kalaitzakis E, Johansson JE, Bjarnason I,
Bjornsson E. Intestinal permeability in cirrhotic
patients with and without ascites. Scand J
Gastroenterol 2006; 41:326–30.
37. Zuckerman MJ, Menzies IS, Ho H, Gregory GG,
Casner NA, Crane RS, et al. Assessment of
intestinal permeability and absorption in cirrhotic
patients with ascites using combined sugar probes.
Dig Dis Sci 2004;49:621–6.
38. Pande C, Kumar A, Sarin SK. Small-intestinal
bacterial overgrowth in cirrhosis is related to the
severity of liver disease. Aliment Pharmacol Ther
2009; 29:1273–81.
39. Jun DW, Kim KT, Lee OY, Chae JD, Son BK, Kim
SH, et al. Association between small intestinal
bacterial overgrowth and peripheral bacterial DNA
in cirrhotic patients. Dig Dis Sci 2010; 55:1465–71.
40. Jamil S, Ahmed S, Memon A, Masood S, Ali Shah
S, Hamid S, Jafri W. Factors Predicting the
Recurrence of Spontaneous Bacterial Peritonitis in
Patients with Cirrhosis. Journal of the College of
Physicians and Surgeons Pakistan 2011; 21(7): 407-
10.
41. Elhawary E, Mahmoud G, El-Daly M, Mekky F,
Esmat G , Abdel-Hamid M. Association of HCV
with diabetes mellitus: an Egyptian case-control
study. Virology J 2011; 8: 367.
42. Ampuero J , Ranchal I, del Mar Díaz-Herrero M,
del Campo JA, Bautista JD, Romero-Gómez M.
Role of diabetes mellitus on hepatic
encephalopathy. Metab Brain Dis 2013; 28(2):277-
9.

Original Article
Impact of Minimal Histological Changes in Donor Liver on the Outcome of
Living Donor Liver Transplantation
Naglaa Allam1, Wael Abdel-Razek1, Nermine Ehsan2, Asmaa Gomaa1, Dina El-Azab2, Imam Waked1
1. Hepatology, National Liver Institute, Menoufiya University, Shebeen ElKom, Egypt.
2. Pathology, National Liver Institute, Menoufiya University, Shebeen ElKom, Egypt
ABSTRACT
Apparently healthy individuals occasionally have minimal hepatic histological changes that do not alter liver tests. In
living donor liver transplantation (LDLT), limited donor availability often makes a donor with minimal histologic
changes the only available donor, and the only chance to save the patient, and is frequently accepted for donation. The
impact of donor minimal histological changes on donor and recipient outcome has not been extensively analyzed.
Methods: We analyzed unexpected histological changes in donors, and the effects of accepted minimal changes on the
outcome. Post-operatively, donors’ and recipients’ labs on postoperative days 1, 7, 14; length of hospital stay;
complications; recipients’ portal vein velocity and hepatic artery resistivity index and 3-year survival were correlated to
different minimal histologic changes. Results: Of 380 related donors, 252 (66.3%) were rejected because of abnormal
liver tests or imaging, unsuitable volumetry; only 128 (33.7%) underwent liver biopsy. Twenty donors (15.6%) were
rejected due to significant histopathological changes: expanded bilharzial portal fibrosis in 12 (60%), steatosis >30% in
6 (30%) and prominent lobular necroinflammation in 2 (10%). Of 108 accepted donors (77 males (71.3%), mean age
28.2±7 years; mean BMI 24±3.6), forty-two (38.9%) had minimal changes: 10-20% steatosis in 4; minimal portal
fibrosis in 24; mild hepatitic changes in 11; ductular proliferation in 2; minimal lobular hepatitis in 1. Thus 62 of the
128 potential donors with normal tests and imaging (48.4%) had histological changes (20 significant + 42 minimal),
which prevented donation in 15.6% (20 cases). Recipients were 96 males (88.9%) with mean age 47.3±7.5 years, mean
MELD score 16.5 (range 11-25). None of these changes had significant impact on donors’ or recipients’ parameters
including no effect on acute rejection and HCV recurrence, or on 3-year survival [donor steatosis (p=0.4), portal fibrosis
(p=0.26), hepatitic changes (p=0.8)]. Conclusion: Grafts with minimal histologic changes were the only available
option for 39% of the patients. Nevertheless, accepting these donors did not affect donor outcome, and had no negative
impact on recipient outcome and three-year survival, even for recipients with MELD score up to 25.
Introduction
With the shortage in deceased livers available for
transplantation, and the increase in adult living
donor liver transplantation (LDLT), controversies
about the inherent risks to the donor persist. This
is particularly important in areas where liver
transplants depend mainly on living donors and
deceased organs are unavailable or in short
supply. The ideal pre-transplant evaluation
process should be extensive to detect any
unapparent abnormalities that may affect the
potential graft function and increase the risk to the
donor and/or the recipient. Indeed some
individuals with “normal” livers have minimal
hepatic histological changes that do not alter liver
tests or imaging and are occasionally accepted as
donors for LDLT. The reported histopathological
abnormalities in “normal” livers include mild
steatosis, hepatitic changes, portal fibrosis,
granulomas of unknown etiology, chronic
hepatitis, and microabscessses (1). The donor with
these changes could be the only available option
for some patients. These changes are accepted for
donation if minimal, and their impact on the
outcome of the donors and recipients has not been
extensively studied. In this study we aimed to
review the different minimal histopathologic liver
findings among the accepted right lobe donors and
assess the effects of these changes on the outcome
of the donors and recipients.

Methods
The medical records of adult-to-adult LDLT
performed between January 2003 and January
2012 at the National Liver Institute, a tertiary
referral center for liver disease & transplantation,
were reviewed for this retrospective study. Donors
and recipients were followed till October 2014.
Donors
Three hundred and eighty related donors had
consented for right lobe liver donation. Of these,
252 (66.3%) had been rejected because of
abnormal liver tests or imaging, or unsuitable
volumetry, and only 128 (33.7%) had undergone
liver biopsy as part of the evaluation. Based on
biopsy results, 20 donors (15.6%) had been
rejected, due to expanded bilharzial portal fibrosis
in 12 (60%), steatohepatitis with steatosis >30%
in 6 (30%) (2 of whom were >60%), and
prominent lobular necroinflammation in 2 (10%).
One hundred and eight donors with “normal” liver
histology were accepted. “Minimal changes” not
preventing donation were accepted, and these are
the subject of this analysis. Direct relationship to
the recipient was necessary. Each donation had to
be approved by the Ethics Committee at the
National Liver Institute, and the central
Transplant Committee of the Ministry of Health
(MOH) and the ethics committee of the Egyptian
Physician’s syndicate. In all 108 donors, the right
lobe was harvested without the middle hepatic
vein and the remaining donor liver volume was
35-40%. The histologic findings of the liver of the
accepted 108 donors were re-evaluated by an
experienced liver pathologist, blinded to the
radiologic and surgical findings. Formalin-fixed,
paraffin embedded liver tissue from all the
accepted donors were retrieved from Archives of
pathology department at the National Liver
Institute. Serial sections 4 μm thick were cut and
placed on three different slides. They were stained
with hematoxylin and eosin to evaluate
pathological changes, Masson's trichrome that
stains collagen fibers to assess the state of fibrosis
and Perls stain which reveals iron deposits. Liver
pathological changes such as macrovesicular
steatosis, steatohepatitis, granulomatous reactions,
fibrosis, portal tract mononuclear inflammation,
interface hepatitis, iron deposition, focal lobular
necroinflammation, apoptotic bodies & lipofuscin
granules deposition were all reported. Special
emphasis on the presence and degree of steatosis,
hepatitic changes and portal and periportal
fibrosis was made. The degree of macrovesicular
steatosis was quantified on a percentage scale,
which estimated the amount of liver parenchyma
that had been replaced by macrovesicular steatotic
droplets. Macrovesicular steatosis was graded as
minimal (1%-10%), mild (>10%-20%), or not
accepted for donation at our center because of
higher amount of steatosis (>20%). Minimal
hepatitic changes describe occasional foci of
spotty necrosis in hepatic lobules 1-2
foci/10xHPF, no apoptotic bodies, no focal
confluent necrosis, no perivenular inflammation.
Mild hepatitic changes describe occasional foci of
spotty necrosis in hepatic lobules 1-2
foci/10xHPF, occasional apoptotic bodies 0-
1/10xHPF, occasional foci of confluent necrosis
0-1/10xHPF, lipofuscin granules in perivenular
region.
Recipients
The medical record of the 108 accepted recipients
were reviewed with emphasis on the aetiology of
liver cirrhosis, any pretransplant treatment offered
to cases with hepatitis C, hepatitis B and
hepatocellular carcinoma and the postoperative
course. Post-operatively, donors’ and recipients’
labs (ALT, AST, bilirubin, INR) on POD1, 7, 14,
30, and on ICU (intensive care unit) and hospital
discharge; the length of ICU and hospital stay;
complications and morbidities as well as donor
requirement for blood transfusion; and recipients’
portal vein velocity and hepatic artery resistivity
index on POD1 and 1-year survival were
recorded. The above-mentioned lab results and
parameters of both the recipients and donors were
correlated to the different changes in donor
histology. The study was approved by the
institutional review board (IRB number
IRB00003413).

Statistical Methods
Data were analyzed using SPSS (Statistical
Package for Social Science) program for
Windows, version 16.0 (SPSS Inc., Chicago, IL,
USA). Categorical data were compared using Chi-
square test. Fisher’s exact test was used if at least
one of the observed or expected values was less
than 5. The independent samples t-test and
analysis of variance (ANOVA) were used to
compare quantitative data in case of two variables
and more than two variables, respectively.
Histopathological changes were tested as
predictors of recipients’ mortality post-LDLT
using Kaplan-Meier method with the log-rank test
to verify the significance of difference between
the different categories. HCV recurrence post-
LDLT was estimated and analyzed in those
patients who were transplanted for HCV-related
liver disease as a subgroup analysis. Two-tailed p
values were considered statistically significant if
less than 0.05.
Results
The study included 108 donors and their related
recipients.
Donor
The demographic and pre-operative histological
data of the donors are shown in Table 1. All
donors had no history of liver diseases, normal
liver biochemistry and negative hepatitis B and C
markers. Preoperative abdominal ultrasonography
did not show any abnormal findings in 88 (81.5%)
donors while hepatomegaly and periportal fibrosis
were seen in 15 (13.9%) and 25 (23.1%) donors
respectively. CT volumetry showed that they had
sufficient liver volume to safely donate the right
lobe for their relatives. Some overlap occurred
among the donor histopathological findings
shown in Table 1. Donor surgery in all cases was
uneventful. None of the donors required blood
transfusion. The mean hospital stay was 13.4±6.3
days. Postoperative complications included bile
leak in 9 donors (8.3%), biliary stricture in 3
(2.8%), pleural effusion in 3 (2.8%), wound
infection in 2 (1.9%), and neuropraxia of ulnar
nerve in one donor (0.9%). Recipient
characteristics are shown in Table 2. Hepatitis C
was the underlying etiology of liver disease in 100
cases (92%). All patients did not receive
pretransplant antiviral treatment. In 29 of these
HCV cases, HCC was associated. not received ttt..
HCC All patients were within Milan criteria with
no vascular invasion or lymph node spread
detected by preoperative imaging. Only eight of
the HCC cases had received pretransplant therapy.
Four patients had undergone transarterial chemo
embolisation (TACE) before transplantation: one
with complete ablation and 3 without. Two
patients had had radiofrequency ablation (RFA).
Another 2 patients had undergone combined
TACE and RFA. In three cases, the underlying
aetiology was hepatitis B. All patients were on
lamivudine therapy pretransplant. After
transplantation, they received HBIG the dose
varying according to the HBV DNA: 2000 IU
intramuscular in the anhepatic phase if HBV DNA
negative and 4000 if positive followed by 800 IU
daily for 6 days and every week for 1 month. All
patients continued on lamivudine and the titre of
anti-HBs Ab was followed regularly with a
booster of 400 units of HBIG given if the level
dropped below 100. The mean hospital stay of the
recipients was 18.2±9.1. Postoperative
complications included biliary stricture in 7
patients (6.5%), bile leak in 4 (3.7%), hepatic
artery thrombosis in 1 (0.9%), cytomegalovirus
(CMV) infection in 1 (0.9%), splenic abscess in 1
(0.9%), post-transplant lymphoproliferative
disease (PTLD) in 1 (0.9%) and intestinal
obstruction in one (0.9%).
Impact of histopathological abnormalities on
donor and recipient outcome:
(A) Steatosis: Donors with 10-20% steatosis (S1)
were significantly older than those with <10%
steatosis (S0) (P=0.047). BMI was not
significantly different. Two donors had BMI ≤25,
yet their biopsies showed steatosis up to 20%. In
only two of the four cases with 10-20% steatosis,
ultrasound showed abnormal findings: a bright
liver denoting fatty infiltration in one case and

hepatomegaly in the other. MRI of the four cases
failed to detect any fatty infiltration. Postoperative
donor liver tests increased and reached maximum
levels on POD1. The levels of bilirubin, ALT and
INR on POD1, POD7 and POD14 in donors with
steatosis less or more than 10% are shown in
Figures 1-3. Neither bilirubin, AST, ALT nor INR
showed a statistically significant difference
between the two groups on POD1 (P=0.59, 0.70,
0.90, 0.82 respectively), POD7 (P=0.17, 0.35,
0.30, 0.16 respectively) or on POD14 (0.82, 0.90,
0.85, 0.52). Similarly, hospital stay was not
different (14.3±0.5 for donors with steatosis
<10%, and 13.4±6.4 days for donors with
steatosis 10-20%, P=0.79). Recipients who
received grafts from both groups were not
significantly different as regards age, gender,
MELD score or underlying liver disease. The
hepatic artery resistivity index and portal vein
velocity increased, reached their peak on POD1 in
both groups with no significant difference
between the two as shown in Figures 4 and 5
(P=0.62 and P=0.35 respectively). Steatosis did
not have a significant impact on the mean ICU
stay and overall hospital stay of the recipients
(8.5±4.4 vs. 9±4.1, P=0.83 and 18.1±9.2 vs.
22.3±5.4, P=0.37). In addition the incidence of
HCV recurrence and graft rejection were not
affected by the 10-20% steatosis as shown in
Table 3 (P=0.98, 0.99 respectively). The Kaplan-
Meier survival curve in Figure 6 (a) shows that
steatosis did not affect recipient 3-year survival
(P=0.4). The mean survival was 36 months in
those with S1 versus 30.7 months in those with
S0.
(B) Mild hepatitic changes: The demographics
of the 11 donors with mild hepatitic changes were
similar to those without. As regards the impact of
mild hepatitis changes on donors' labs and
hospital stay: there was no significant impact on
the donors' bilirubin on POD 1 and 14 [P=0.24,
0.63 respectively (Figure 1)] ; the donors' AST on
POD 7 and 14 (p=0.09, p=0.14 respectively) ; the
donors' ALT on POD 7 (p=0.16, 0.15) [Figure 2];
the INR on POD 1, 7 and 14 (P=0.07, 0.38, 0.98
respectively (Figure 3)],and the hospital stay
(13.7±6.4 vs. 10.9±4.2 respectively, P=0.16). In
fact, AST and ALT on POD1 and bilirubin on
POD7 were slightly higher in donors without
minimal hepatitic changes (Figures 1-3).
Recipients who received grafts with mild hepatitic
changes were similar in demographics, MELD
score and underlying etiology to those who
received grafts without. These changes did not
significantly affect the hepatic artery resistivity
index (P=0.87, Figure 4), portal vein velocity
(P=0.55, Figure 5), ICU stay (8.5±4.5 vs. 9.1±3.8
days, P=0.67), hospital stay (18.2±9.1 vs.
18.8±9.8 days, P=0.83), HCV recurrence
(P=0.96), graft rejection (P=0.59, Table 3) or 3-
year survival [P=0.8, Figure 6 (b)]. The mean
survival was 30.4 months in those with mild
hepatitic changes versus 31.2 months in those
without.
(C) Mild periportal fibrosis (PPF): Mild PPF
without Schistosoma granulomas was diagnosed
in 24/108 (22.2%). There was no difference in
age, gender or BMI between those with or without
PPF. Laboratory and imaging did not predict
accurately this histological finding. Two of the
donors had demonstrated positive serological
indirect hemaglutination test for schistosomiasis,
but had negative rectal biopsies and were
diagnosed as having past schistosomiasis, and
were accepted for donation. Pre-operative
ultrasound showed some degree of PPF in only 19
of the 24 patients. Transaminases were slightly
higher in the donors with PPF than those without
PPF (Figure 2). However the difference was not
significant and the levels almost normalized by
POD14 in both groups. There was no significant
difference in the bilirubin and INR levels between
the two groups and both parameters normalized
by POD14 (Figures 1 and 3). There was also no
significant impact on donor hospital stay
(13.6±6.6 vs. 12.8±4.8 days, P=0.57). As regards
recipients, PPF did not significantly affect the
recipients' portal vein velocity (Figure 4, P=0.50)
while the hepatic artery resistive index was higher
in recipients of grafts with minimal PPF (P=0.04).

ICU stay (8.8±4.8 vs. 7.5±2.3 days), hospital stay
(18.8±9.5 vs. 16.5±7.5 days) were not
significantly affected (P=0.67, 0.83). HCV
recurrence and graft survival were not affected
significantly (Table 3, P=0.96, 0.59 respectively),
and 3-year survival was similar [P=0.26, Figure 6
(c)]. The mean survival was 29.4 months in those
with periportal fibrosis versus 31.8 months in
those without.
Discussion
Liver histological changes can occasionally
escape prediction by laboratory tests and imaging.
In this series, 62 of the 128 donors with normal
liver tests and imaging (48.4%) had histological
changes on biopsy, which were severe and
prevented donation in (15.6%). Occasionally, the
donor with “minimal” histological changes could
be the only available donor, and the only chance
the patient has to save his life. The data of the
present study showed that different forms of
unexpected histopathological abnormalities were
found in 38.8% of the liver biopsies of the
evaluated donors who had normal liver tests and
imaging, and were negative for hepatitis viruses.
Steatosis (10-20%) was detected in 4 (3.7%)
donors; periportal fibrosis without schistosomal
granuloma in 24 (22.2%); mild hepatitic changes
in 11 (10.3%); ductular proliferation in 2 (0.02%)
and chronic hepatitis in 1 (0.01%). In
comparison, a higher rate of abnormalities was
detected by Tran et al. who found that 67% had
unexpected abnormalities, of which steatosis was
the most common abnormality (38.5%). Other
histopathological abnormalities included
granulomas of unknown etiology (7%), chronic
hepatitis (6%) and a case of microabscess (1). On
the other hand, Nadalin et al. reported a lower rate
of abnormal findings (21%) with 14.6% being
liver steatosis of varying kinds and grades, and in
the other 5.4% non steatotitic hepatopathies in the
form of hepatitis of unknown origin, diffuse
granulomatosis as well as portal and periportal
fibrosis (2). Accurate quantification of the degree
of steatosis is important in calculating functional
graft mass in LDLT. However, there is no
standard grading of "mild" steatosis used in the
literature and this sometimes makes data
comparison difficult. Cho et al. classified as
follows: group 1, less than 5%; group 2, 5% to
15% and group 3, more than 15% (3). In a study
done by Soejima et al., they divided steatotic
groups into: none, 0%; mild, 0% to 20% and
moderate, 20% to 50% (4). In the present study, we
chose to classify the steatosis into: group S1
<10% and group S2, 10% to 20%. In the current
study, nearly all detected histological
abnormalities had not been suspected before the
biopsy despite the extensive investigations
conducted. The demographics of the cohort with
the histologic abnormalities were similar to those
without. BMI measurement could not eliminate
those with steatosis, where two donors had a BMI
of less than or equal to 25, yet their biopsies
showed steatosis up to 20%. In general, there was
no significant difference in BMI between those
with steatosis <10% or 10-20%. However, we did
not include individuals with BMI higher than 33
as this would contra-indicate living liver donation.
This was consistent with the findings from
another reported series (5). Hence, although high
BMI is generally indicative of a higher risk of
steatosis, normal BMI does not consistently
predict its absence. As regards imaging,
ultrasound of the four S2 cases had detected a
suspicion of fatty infiltration in only one case and
hepatomegaly in another. However, subsequent
MRI of all the cases failed to detect any fatty
infiltration. On the other hand, in one case with
S1, the ultrasonography was suggestive of fatty
infiltration. Similar to our results, Rinella et al.
reported that both MRI and CT scans were
negative in 30% and 24%, respectively, in
individuals despite >10% steatosis on biopsy (6).
Imaging did not predict the biopsy-detected
hepatitic changes either. And in periportal
fibrosis, there was a mismatch between the
ultrasound and the biopsy findings. Ultrasound
reports had revealed PPF in 19 of the 22 positive
biopsies. On the other hand, in 5 cases with
negative biopsies, ultrasound reports had showed

PPF. Hence we cannot rely on non-invasive
modalities in accurately screening for
histopathologic changes; liver biopsy stands out
as a necessity. In the presence of donor histologic
abnormalities, donor safety is of concern because
of the potential for reduced regeneration and the
higher operative risk. In the present study, the
three main mild histopathologic abnormalities did
not impact the immediate postoperative or long-
term outcome of the donors. The donors with 10-
20% steatosis demonstrated an insignificantly
higher transaminases, bilirubin and INR than the
S0 donors and the levels decreased by around
30% on POD7 and almost normalized by POD14.
This temporary effect corresponds to previous
studies which demonstrated an initially poor
function of steatotic livers that recovered within
the first week postoperatively hence suggesting a
high potential for post-transplant regeneration
despite mild steatosis (4, 7). The mean duration of
hospital stay was not significantly different either
(13 days). Similarly, Soejima et al. reported that
the mean length of hospital stay of the donors
with mild steatotic grafts (0%-20%) was 13.6
days (4) and Hayashi et al. concluded that in
general the hospital stay of those with/ without
steatosis was not significantly different (8).
Actually there is no wide agreement on the
percentage of steatosis that serves as cutoff value
for safe performance of living donor liver
transplantation; initially Ryan et al. set the level of
10% (5), but later Cho et al. and Fan et al. set the
limit of 30% steatosis for any impairment (3, 9). In
the present study all donors with less than 20%
demonstrated an uneventful postoperative
recovery and a good long-term outcome. We did
not accept donors with steatosis >20%. We found
that minimal histological changes in donor livers
had no deleterious effects on recipient outcome.
Donor steatosis has been identified as an
independent risk factor for postoperative
complications after liver transplantation. Adams
at al. showed that donor grafts with steatosis of
>30% increases the risk of primary-non-function
of the graft to 13%, as compared with 2.5% for
non-steatotic grafts (10), and others reported that
even mild hepatic steatosis <30% may have an
adverse effect on recipient outcome following
liver transplantation (11-13). In contrast, more recent
studies indicated that livers with even moderate
steatosis can be transplanted safely without
affecting patient outcome or organ survival (7, 14,
15), and Cho et al. reported that the degree of
preoperative mild steatosis is significantly
reduced to below 10% immediately after
successful LDLT (3). In the current study, we
found that 10-20% steatosis did not have a
significant impact on the early postoperative
recovery. It has been speculated that diminished
organ blood flow in steatotic livers grafts may
induce a state of chronic hypoxia that contributes
to impaired organ function following reperfusion (16, 17). In this regard, a decrease in sinusoidal
blood flow has been reported using laser Doppler
flow meters prior to organ explantation of
steatotic livers (16). However, the present study did
not identify impairment in portal vein velocity and
hepatic artery resistivity index for those receiving
grafts with 10-20% steatosis. The hospital stay
was similar to the other cohort receiving group S0
steatotic grafts. Actually Cho et al. reported that
the hepatic regeneration power of steatotic grafts
is not impaired versus non steatotic grafts and
they observed that the preoperative degree of mild
steatotic graft is significantly reduced to below
10% immediately after successful LDLT (3). We
also found no significant relation between
steatosis and HCV recurrence or 3-year survival.
Similarly, Botha et al. reported that mild/moderate
macrovesicular steatosis in the donor liver had no
impact on HCV recurrence after liver
transplantation (18).The prognosis of
macrovesicular steatosis appears to be impaired if
other risk factors coexist as prolonged ischemic
time (>10 hours) and donor age above 65 years (19,
20), and advanced donor age has been associated
with a higher degree of HCV recurrence and
faster progression (21, 22). In the current study, most
of the donors were younger than 35 years, and the
absence of higher risk of complications may be
explained by the exclusion of steatosis >20% and
the inclusion of only young donors. Several

studies have reported impaired organ survival of
steatotic organs (11, 12, 23, 24). In the current study,
there was no significant impact of mild steatosis
on 1-year patient survival. It seems that the
survival is related to the percentage of mild
steatosis. Patkowski et al. reported 1-year survival
of 89% when liver steatosis was <20% (as in the
present study) versus 75.5% in cases with liver
steatosis >20% (25). Actually a significantly
reduced 4-month survival rate was observed
comparing steatotic grafts (up to 30% steatosis)
with livers without fatty infiltration (12). However
Chui et al. reported that this difference in survival
rate was no longer evident at 1 year of follow-up (7), as in the present study. The second main
histologic abnormality we found in 22% of our
donors was "mild periportal fibrosis". This lesion
is characteristic of previous infection with
Schistosoma mansoni. In Egypt, schistosomiasisis
endemic, and the number of previously infected
individuals is high. In the present study, rectal
biopsy was negative in all cases implying no
active infection, and liver function was preserved.
The presence of mild periportal fibrosis thus
indicates past infection that has been cured. The
use of schistosomiasis infected liver grafts is
controversial. Some authors stated that the
histological findings of granulomatous reactions
of Schistosoma eggs in preoperative liver biopsy
samples was a contraindication for liver donation (1, 2). In contrast, Vincenzi et al. reported that
simple presence of Schistosoma eggs in liver
tissue may not be a contraindication for liver
donation, especially when treatment of
schistosomiasis is possible during the preoperative
donor evaluation (26). Andraus et al. reported good
2-year outcome of two donors; in one of them, the
donor liver biopsy had revealed epithelioid
granulomas with Schistosoma eggs and in the
other the donor had Schistosoma eggs in his feces
and was treated by praziquantel (27). In the present
study, the donor postoperative parameters were
not significantly affected by the periportal
fibrosis. Only the transaminases were slightly
higher than those without PPF. However the
difference was not significant and the levels
almost normalized by POD14 in both groups. As
regards recipient outcome few reports have
demonstrated the presence of Schistosoma ova
and granulomas in grafts from deceased donors
with no consequences for graft or recipient
survival. Up to two years follow up did not
demonstrate any evidence of schistosomiasis on
liver biopsy of the recipients (28, 29). In the present
study, hepatic artery resistivity index was the only
postoperative parameter which was significantly
different between both groups. Again as in mild
steatosis, there was no significant impact of PPF
on the ICU stay, hospital stay and 3-year survival.
Our results come in contrast to those of Ydreborg
et al. who reported that histopathological features,
especially portal inflammation and stage of
fibrosis, in the donor liver may deleteriously
affect graft and patient survival (30). The difference
in their observation may be explained by the older
donor age. In their study, most of the donors were
older than 60 years whereas in the current study
the mean age was 28 years. The presence of mild
hepatitic changes did not have a significant impact
on donor and recipient postoperative parameters
or the long-term outcome. In all 11 recipients who
received hepatitic grafts, the underlying etiology
was hepatitis C with/without HCC. The rate of
histologic HCV recurrence was slightly higher in
those who received hepatitic grafts (18% vs.
3.4%) and there was no difference in the
incidence of acute rejection, overall morbidity and
mean survival time. However the sample size was
small. In conclusion, our study showed that in
LDLT, preoperative liver biopsies showed donor
histologic abnormalities which had not been
detectable by serological, biochemical and
radiological methods. These grafts from living
donors with minimal histologic changes were the
only available option for 39% of the patients in
our program and these grafts did not affect the
survival of even the patients with MELD score
above 20. There are other potential implications to
our findings which suggest that many healthy
individuals have unsuspected mild abnormalities
on liver biopsy. These findings may also have
implications in the non-transplant setting as

changes ascribed to specific etiologies for liver
disease might include changes occurring in
apparently healthy individuals. We found that the
clinical outcome of grafts with steatosis <20%,
mild schistosomal periportal fibrosis and mild
hepatitic changes appears comparable to the other
cohort of donors and transplant patients. Hence, in
the absence of other confounding factors such as
old donor age, livers with these mild histologic
changes can be transplanted safely with good
results. It is true that our study has the following
limitations. The graft regeneration could have
been more accurately assessed in a prospective
design. Also a larger sample size could have
added to the significance of the analysis; however
it is noteworthy that donors included in this study
were all related donors who were not excluded by
the strict donor selection criteria or ethical
committees at the institute, MOH and physicians'
syndicate. The precise significance of the long-
term consequences of these histologic
observations on the donors and patients warrant
further study. Nevertheless in the meantime
judging from the data presented here, we support
the continued use of grafts with steatosis up to
20%, mild periportal fibrosis and mild hepatitic
changes in recipients even with MELD score up
to 25 and regardless of HCV status.
Table 1. Donor demographics and preoperative histopathological liver findings
Age (years), range (mean±SD) 18-47 (28.2±7.0)
Male : Female, n (%) 77 : 31 (71.3 : 28.7)
BMI, range (mean±SD) 18-33 (24.7±3.6)
Histological findings, n (%)
Steatosis <10% 104 (96.3)
Steatosis 10-20% 4 (3.7)
No hepatitic changes 97 (89.8)
Mild hepatitic changes 11 (10.3)
No PPF 84 (77.8)
Mild PPF 24 (22.2)
Chronic hepatitis (interface hepatitis) 1 (0.01)
Others (ductular proliferation) 2 (0.02)
Table 2. Characteristics of the recipients
Age (years), mean (range) 47.3 (24-61)
Male : Female, n (%) 96 : 12 (88.9 : 11.1)
MELD score, mean (range) 16.5 (11-25)
Indications for liver transplantation, n (%)
HCV-related cirrhosis 71 (65.7)
HBV-related cirrhosis 3 (2.8)
HCC associated with HCV 29 (26.8)
Budd-Chiari syndrome 1 (0.9)
Wilson's disease 1 (0.9)
Alcoholic cirrhosis 1 (0.9)
Cryptogenic 2 (1.9)

Table 3. Post LDLT recipients' complications according to the abnormal histologies in the donors' biopsies
Graft Rejection HCV recurrence
No Yes P Value No Yes P Value
Steatosis
<10% 96 (92.3) 8 (7.7) 1
91 (94.8) 5 (5.2) 1
10-20% 4 (100) 0 4 (100) 0
Hepatitic changes
Absent 90 (92.8) 7 (7.2) 0.59
86 (96.6) 3 (3.4) 0.09
Present 10 (90.9) 1 (9.1) 9 (81.8) 2 (18.2)
Periportal fibrosis
Absent 77 (91.7) 7 (8.3) 1
72 (93.5) 5 (6.5) 0.59
Present 23 (95.8) 1 (4.2) 23 (100) 0


References
1. Tran TT, Changsri C, Shackleton CR, Poordad FF,
Nissen NN, Colquhoun S, et al. Living donor liver
transplantation: histological abnormalities found on
liver biopsies of apparently healthy potential
donors. J Gastroenterol Hepatol. 2006;21(2):381-3.
2. Nadalin S, Malago M, Valentin-Gamazo C, Testa
G, Baba HA, Liu C, et al. Preoperative donor liver
biopsy for adult living donor liver transplantation:
risks and benefits. Liver Transpl. 2005;11(8):980-6.
3. Cho JY, Suh KS, Kwon CH, Yi NJ, Cho SY, Jang
JJ, et al. The hepatic regeneration power of mild
steatotic grafts is not impaired in living-donor liver
transplantation. Liver Transpl. 2005;11(2):210-7.
4. Soejima Y, Shimada M, Suehiro T, Kishikawa K,
Yoshizumi T, Hashimoto K, et al. Use of steatotic
graft in living-donor liver transplantation.
Transplantation. 2003;76(2):344-8.
5. Ryan CK, Johnson LA, Germin BI, Marcos A. One
hundred consecutive hepatic biopsies in the workup
of living donors for right lobe liver transplantation.
Liver transplantation. 2002;8(12):1114-22.
6. Rinella ME, Alonso E, Rao S, Whitington P, Fryer
J, Abecassis M, et al. Body mass index as a
predictor of hepatic steatosis in living liver donors.
Liver Transplantation. 2001;7(5):409-14.
7. Chui A, Shi L, Rao A, Anasuya A, Hagl C, Pillay
P, et al. Primary graft dysfunction after liver
transplantation. Transplantation proceedings; 2000:
Elsevier; 2000. p. 2219-20.
8. Hayashi M, Fujii K, Kiuchi T, Uryuhara K,
Kasahara M, Takatsuki M, et al. Effects of fatty
infiltration of the graft on the outcome of living-
related liver transplantation. Transplantation
proceedings; 1999: Elsevier; 1999. p. 403.
9. Fan S-T, Lo C-M, Liu C-L, Yong B-H, Chan JK-F,
Ng IO-L. Safety of donors in live donor liver
transplantation using right lobe grafts. Archives of
surgery. 2000;135(3):336-40.
10. Adam R, Bismuth H, Diamond T, Morino M,
Figure 6: Kaplan Meier curves of recipients' survival at 3 years post-LDLT according to histologic changes in donors'
biopsies in relation to (A) Steatosis (B) Hepatitic changes (C) Periportal Fibrosis

Astarcioglu I, Johann M, et al. Effect of extended
cold ischaemia with UW solution on graft function
after liver transplantation. The Lancet.
1992;340(8832):1373-6.
11. Todo S, Demetris AJ, Makowka L, Teperman L,
Podesta L, Shaver T, et al. Primary nonfunction of
hepatic allografts with preexisting fatty infiltration.
Transplantation. 1989;47(5):903-5.
12. Marsman WA, Wiesner RH, Rodriguez L, Batts
KP, Porayko MK, Hay JE, et al. Use of fatty donor
liver is associated with diminished early patient and
graft survival. Transplantation. 1996;62(9):1246-
51.
13. Imber CJ, St Peter SD, Lopez I, Guiver L, Friend
PJ. Current practice regarding the use of fatty
livers: a trans-Atlantic survey. Liver Transpl.
2002;8(6):545-9.
14. Selzner M, Clavien PA. Fatty liver in liver
transplantation and surgery. Semin Liver Dis.
2001;21(1):105-13.
15. Yoo HY, Molmenti E, Thuluvath PJ. The effect of
donor body mass index on primary graft
nonfunction, retransplantation rate, and early graft
and patient survival after liver transplantation.
Liver Transpl. 2003;9(1):72-8.
16. Seifalian AM, Piasecki C, Agarwal A, Davidson
BR. The effect of graded steatosis on flow in the
hepatic parenchymal microcirculation.
Transplantation. 1999;68(6):780-4.
17. Ijaz S, Yang W, Winslet MC, Seifalian AM.
Impairment of hepatic microcirculation in fatty
liver. Microcirculation. 2003;10(6):447-56.
18. Botha JF, Thompson E, Gilroy R, Grant WJ,
Mukherjee S, Lyden ER, et al. Mild donor liver
steatosis has no impact on hepatitis C virus fibrosis
progression following liver transplantation. Liver
Int. 2007;27(6):758-63.
19. Mutimer DJ, Gunson B, Chen J, Berenguer J,
Neuhaus P, Castaing D, et al. Impact of donor age
and year of transplantation on graft and patient
survival following liver transplantation for hepatitis
C virus. Transplantation. 2006;81(1):7-14.
20. Condron SL, Heneghan MA, Patel K, Dev A,
McHutchison JG, Muir AJ. Effect of donor age on
survival of liver transplant recipients with hepatitis
C virus infection. Transplantation. 2005;80(1):145-
8.
21. Wiesner RH, Sorrell M, Villamil F. Report of the
first International Liver Transplantation Society
expert panel consensus conference on liver
transplantation and hepatitis C. Liver Transpl.
2003;9(11):1-9.
22. Feray C. Steroid and azathoprine maintenance as
the best regimen during recurrent hepatitis C? Liver
Transpl. 2005;11(4):384-5.
23. Zamboni F, Franchello A, David E, Rocca G,
Ricchiuti A, Lavezzo B, et al. Effect of
macrovescicular steatosis and other donor and
recipient characteristics on the outcome of liver
transplantation. Clin Transplant. 2001;15(1):53-7.
24. Busquets J, Figueras J, Serrano T, Torras J, Ramos
E, Rafecas A, et al. Postreperfusion biopsy changes
predict biliary complications after liver
transplantation. Transplant Proc. 2002;34(1):256-8.
25. Patkowski W, Zieniewicz K, Skalski M, Krawczyk
M. Correlation between selected prognostic factors
and postoperative course in liver transplant
recipients. Transplantation proceedings; 2009:
Elsevier; 2009. p. 3091-102.
26. Vincenzi R, Neto JS, Fonseca EA, Pugliese V,
Leite KR, Benavides MR, et al. Schistosoma
mansoni infection in the liver graft: The impact on
donor and recipient outcomes after transplantation.
Liver Transplantation. 2011;17(11):1299-303.
27. Andraus W, Pugliese V, Pecora R, D'Albuquerque
LAC. Intentional use of Schistosoma mansoni-
infected grafts in living donor liver transplantation.
Liver Transpl. 2012;18(7):867-8.
28. Pungpapong S, Krishna M, Abraham SC, Keaveny
AP, Dickson RC, Nakhleh RE. Clinicopathologic
findings and outcomes of liver transplantation using
grafts from donors with unrecognized and unusual
diseases. Liver Transpl. 2006;12(2):310-5.
29. Pannegeon V, Masini J-P, Paye F, Chazouillères O,
Girard PM. Schistosoma mansoni infection and
liver graft. Transplantation. 2005;80(2):287.
30. Ydreborg M, Westin J, Lagging M, Castedal M,
Friman S. Impact of donor histology on survival
following liver transplantation for chronic hepatitis
C virus infection: a Scandinavian single-center
experience. Scand J Gastroenterol. 2012;47(6):710-
7.

Original Article
Study of Nosocomial Infections in Cirrhotic Patients in Minoufiya University
Hospital
Nooh M A, EL-lehleh A M,Anees S E, Zaher E M and Teima .A.
* M.D Tropical medicine ** M.D Clinical pathology
ABSTRACT
Nosocomial infections are infections which are results of treatment in a hospital or a health care service unit. Infections
are considered nosocomial if they first appear 48 hours or more after hospital admission or within 30 days after
discharge. Aim of the work: Study of nosocomial infections in cirrhotic patients in Minoufiya university hospital.
Patients and methods: This study was conducted on sixty patients admitted to Tropical Medicine department-
Menoufiya university hospital- they were divided in two main groups,the first group was the control one and included
15 patients without liver cirrhosis and the second cirrhotic group included 45 patients was subdivided in to three sub
groups according to child classification, each subgroup was included 15 patients and all patients were subjected to
,thorough history taking,full clincal and local examination and aseries of laboratory investigations including analysis
and culture of different body fluids and also serological tests of different infections as widal and brucella. Results: the
incidence of infections in hospitalized cirrhotic patients was 29%(13/45) and this was more statistically significant
different than infections in non cirrhotic patients6.7% (1/15), (P value<o.o5), In the present study the most common
acquired nosocomial infections among cirrhotic patients were chest infections 38.5%(5/13) followed by urinary tract
infections23%. Conclusions: from this study we concluded that, nosocomial infections were more common among
patients with liver cirrhosis especially Child c patients than other general hospital population, the most common type of
acquired infections were respiatory infections follwed by urological ,asceitic fluid infection and cellulitis and the most
common causative organisms were bacterial especially gram positive Cocci.
Introduction
Nosocomial infections are infections which are
results of treatment in a hospital or a health care
service unit. Infections are considered nosocomial
if they first appear 48 hours or more after hospital
admission or within 30 days after discharge. This
type of infection is also known as, a hospital-
acquired infection (or health care associated
infection) (1) . Nosocomial infections are caused
by bacterial, viral and fungal pathogens. The most
common pathogens are Staphylococci,
Pseudomonas, E-coli, Mycobacterium tuber-
culosis, Candida, Aspergillus, Fusibacterium,
Trichosporn and Malassezia (2) . Patients admitted
to intensive care units have been shown to be at
particular risk of acquiring nosocomial infections
with prevalence rate as high as 30% (3). Bacterial
infections specially with intestinal type flora is a
common complication in patients with
cirrhosis.Spontaneous bacterial peritonitis (SBP),
urinary tract infection, respiratory tract sepsis
(pneumonia and spontaneous bacterial empyema)
and bacteraemia are the most frequent infective
complications occurring in this group (2) . The
incidence of infection with gram positive cocci
has increased in recent years, with such flora, the
most frequent isolates in hospitalised cirrhotic
patients with nosocomial infection specially those
admitted to intensive care units presumably due to
the high rate of invasive procedures including
placement of indwelling vascular and bladder
catheters performed in this group (4). Between 15
% and 35% of cirrhotic patients admitted to
hospital develop nosocomial bacterial infections,
the rate of hospital-acquired infections is of 5% to
7% in the general hospital setting (5). Infection
may have severe adverse clinical consequences in
cirrhotic patients.The associated pro-
inflammatory response exacerbates hepatic
dysfunction, encephalopathy and the haemo-

dynamic disturbances that underlie the
development of portal hypertension and hepato
renal syndrome (6). Increasing evidence suggests
that, bacterial infection is a trigger for variceal
haemorrhage in patients with cirrhosis possibly as
a consequence of both activation of hepatic
stellate cells leading to increased intrahepatic
vascular resistance and prostacyclin-related
inhibition of platelets aggregation (7). The
mortality rate associated with bacterial infection
in this group of patients is more than twenty times
higher than that in the general population (8).
Aim of the work
The aim of this work was to study nosocomial
infections in cirrhotic patients in Minoufiya
university hospital.
Patients and methods
This study was conducted on sixty patients
admitted to Tropical Medicine department in
Menoufiya university hospital, fourty of them
were males and twenty were females. Their ages
ranged from 40 to 60 years. Patients were divided
into two main groups, the first group was the
control one included fifteen patients without liver
cirrhosis and the second group of cirrhotic
patients was subdivided into three subgroups
according to Child's Pugh classification and each
group of them include fifteen patients as
following: Group IIa: Child's Pugh grade A
patients. Group IIb: Child's Pugh grade B
patients. Group IIc: Child's Pugh grade C
patients. All Patients will be subjected to the
following: Thorough history taking, Full clinical
examination (general, abdominal and local
examination of the all body systems), abdominal
ultrasonography, chest X ray, laboratory
investigations(urine analysis and culture, Stool
analysis and culture, complete blood count ,
erythrocyte sedimentation rate, liver function
tests, kidney function tests, viral markers (HCV-
Ab, HBs-Ag and HIV-Ab), asceitic fluid sample
analysis and culture ,sputum clture and sensitivity,
widal test, Brucella agglutination test,
cerebrospinal fluid examination, upper endoscopy
and colonoscopy. Statistical analysis was done,
Quantitative data were expressed as mean and
standard deviation (X ±SD) and analyzed by
applying F test (One way Anova) for comparison
of more than two groups of normally distributed
variables and Kruskal Wallis test for non-
normally distributed ones. Qualitative data were
expressed as number and percentage (No & %)
and analyzed by applying chi-square test.
Results
This study was done on sixty patients- admitted to
Tropical Medicine department in Menoufiya
university hospital – Their ages ranged from 40 to
60 years and fourty of them were males(66.6%)
and twenty of them were females(33.3%) and
there was no statistically significant difference
between the studied groups as regards age and
sex. We found that ,the incidence of infections in
hospitalized cirrhotic patients (group II) was
29%(13/45) and in non cirrhotic patients (group I)
was 6.66%(1/15) and this difference was of
statistifically significant (P value <0.05). The
most common acquired nosocomial infections in
cirrhotic patients was chest infections
38.5%(5/13) followed by urinary tract infections
23%(3/13),SBP23%(3/13) and cellulitis
15.5%(2/13). *Regarding clinical presentations of
group IIb at admission and 48 hours after
admission,There was statistically significant
difference as regards fever at and after admission
as shown in table(1). *Regarding clinical
presentations of group IIc at admission and 48
hours after admission,There was statistically
significant difference as regards fever and toxic
look at and after admission as shown in table(2).
* Laboratory investigations of group IIb at
admission and 48 hours after admission was of
statistically significant difference as regards
leucocytosis at and after admission as shown in
table(3). * Laboratory investigations of group IIc
at admission and 48 hours after admission was of
statistically significant difference as regards
leucocytosis at and after admission as shown in
table(4). *Regarding prevalence of infections
among the studied groups at admission and 48

hours after admission, the prevalence of infections
after 48 hrs or more of hospitalization was
statistically significant higher among GIIc patients
than other studied groups of patients as shown in
table (5). *As regards the causetive organisms of
hospital acquired infections, the most common
isolated organisms were gram-ve organisms
including (E-coli and pseudomonas) and gram
+ve organisms including (strept pneumonia and
staph aureus) as shown in table (6).
Table (1) Shows comparison between the studied group IIb at admission
and after 48 hrs of hospitalization as regards clinical symptoms and signs:
parameters Group
IIb at
admission
N=15
Group IIb
after 48 hrs of
hospitalization
N=15
X2 P-
Value
No % No %
Dyspepsia 4 26.7 5 33.3 0.16 >0.05
Halitosis 5 33.3 5 33.3 - -
Heart burn 2 13.3 2 13.3 - -
Water brush 1 6.7 1 6.7 - -
Eructation 2 13.3 2 13.3 - -
Vomiting 1 6.7 1 6.7 - -
Abd-distension 4 26.7 5 33.3 0.16 >0.05
Abd-pain 2 13.3 3 20 0.24 >0.05
Constipation 4 26.7 4 26.7 - -
Melena 6 40 4 26.7 0.60 >0.05
Dyspnea 2 13.3 3 20 0.24 >0.05
Cough 2 13.3 4 26.7 0.83 >0.05
Expectoration 0 0 2 13.3 2.14 >0.05
Dysuria 0 0 1 6.7 1.03 >0.05
Frequency 0 0 1 6.7 1.03 >0.05
Suprapubic pain 0 0 1 6.7 1.03 >0.05
Fever 0 0 4 26.7 4.5 <0.05*
rigors 0 0 1 6.7 1.03 >0.05
Jaundice 6 40 6 40 - -
pallor 6 40 4 26.7 0.20 >0.05
Toxic look 0 0 3 20 3.33 >0.05
Working ala nasi 0 0 2 13.3 2.14 >0.05
clubbing 8 53.3 8 53.3 - -
Flapping tremors 4 26.7 3 20 0.19 >0.05
Lower limbs oedema 5 33.3 4 26.7 0.16 >0.05
Ascites 5 33.3 5 33.3 - -
hepatomegaly 1 6.7 1 6.7 - -
splenomegaly 9 60 10 66.7 0.14 >0.05
Diminished air entery 1 6.7 3 20 1.15 >0.05
crepitations 0 0 2 13.3 2.14 >0.05
Dullness 1 6.7 1 6.7 - -

Table (2) Shows comparison between the studied group IIc at admission
and after 48 hrs of hospitalization as regards clinical symptoms and signs
Parameters Group IIc at
admission
N=15
Group IIc after 48 hrs
of hospitalization
N=15
X2 P-Value
No % No %
Dyspepsia 4 26.7 7 46.7 1.29 >0.05
Halitosis 2 13.3 2 13.3 - -
Heart burn 3 20 2 13.3 0.24 >0.05
Anorexia 2 13.3 1 6.7 0.37 >0.05
Vomiting 1 6.7 1 6.7 - -
Abd-distension 4 26.7 4 26.7 - -
Abd-pain 1 6.7 5 33.3 3.33 >0.05
Constipation 5 33.3 4 26.7 0.16 >0.05
Diarrhea 0 0 2 13.3 2,14 >0.05
Melena 6 40 3 20 1.43 >0.05
Dyspnea 4 26.7 2 13.3 0.38 >0.05
Cough 3 20 5 33.3 0.68 >0.05
Expectoration 0 0 2 13.3 2.14 >0.05
Dysuria 0 0 2 13.3 2.14 >0.05
Frequency 0 0 2 13.3 2.14 >0.05
Fever 0 0 7 46.7 8.1 <0.05*
Rigors 0 0 3 13.3 3.33 >0.05
Orthopnea 2 13.3 1 6.7 0.37 >0.05
Jaundice 11 73.3 7 46.7 2.22 >0.05
Pallor 6 40 3 20 1.43 >0.05
Toxic look 0 0 5 33.3 6.0 <0.05*
Working ala nasi 0 0 2 13.3 2.14 >0.05
Clubbing 7 46.7 6 40 0.14 >0.05
Flapping tremors 4 26.7 5 33.3 0.16 >0.05
Spider naevi 6 40 5 40 - -
Signs of
inflammation
(redness, hotness,
lymphadenitis
0 0 1 6.7 1.03 >0.05
Lower limbs
oedema
13 86.7 10 66.7 1.68 >0.05
Ascites 15 100 15 100 - -
hepatomegaly 2 13.3 2 13.3 - -
splenomegaly 7 46.7 7 46.7 - -
Diminished air
entery
5 33.3 6 40 0.14 >0.05
Crepitations 0 0 2 13.3 2.14 >0.05
Dullness 4 26.7 4 26.7 - -
Tender renal angle 0 0 1 6.7 1.03 >0.05
Suprapubic
tenderness
0 0 1 6.7 1.03 >0.05

Table (3) Shows comparison between the studied group IIb at admission
and 48hrs after hospitalization as regards laboratory investigations:
parameters Group IIb at
admission
N=15
Group IIb
after 48 hrs of
hospitalization
N=15
T test P-Value
X¯+ SD X¯+ SD
HB% 9.45+2.16 9.85+2.00 0.52 >0.05
WBCs 4.55+1.46 7.80+5.91 2.06 <0.05*
Platelets 129.86+77.86 129.33+78.18 0.01 >0.05
SGOT 68.26+16.12 74.86+18.27 1.04 >0.05
SGPT 69.33+21.21 79.20+23.82 1.19 >0.05
Serum albumin(gm) 2.89+0.66 2.87+0.62 0.08 >0.05
Seum bilirubin(mg) 1.66+0.79 2.13+0.95 1.47 >0.05
Prothrombin time (Seconds) 18.20+2.83 18.93+2.86 0.70 >0.05
Serum urea 29.13+3.20 31.73+5.56 1.56 >0.05
Serum creatinine 1.18+0.52 1.43+0.71 1.10 >0.05
ESR 45.80+39.10 46.13+38.39 0.02 >0.05
Random blood sugar(mg) 141.93+16.70 143.06+13.61 0.20 >0.05
Table (4) shows comparison between the studied group IIc at admission
and 48hrs after hospitalization as regards laboratory investigations:
parameters Group IIc at
admission
N=15
Group IIc
after 48 hrs of
hospitalization
N=15
T test P-Value
X¯+ SD X¯+ SD
HB% 9.60 + 2.27 10.24+1.78 0.80 >0.05
WBCs 3.53 + 0.91 9.40+6.29 3.57 <0.05*
PLT 76.73 + 24.34 77.20+20.88 0.05 >0.05
SGOT 66.13+ 17.26 69.06+ 18.16 0.45 >0.05
SGPT 75.40 + 30.54 81.60+30.38 0.55 >0.05
Serum albumin(gm) 1.82 + 0.30 1.84+0.29 0.18 >0.05
Seum bilirubin(mg) 5.52+2.93 5.67+2.75 0.14 >0.05
Prothrombin time(Seconds) 29.73+3.57 29.33+3.13 0.32 >0.05
Serum urea 31.00+3.25 30.93+3.45 0.54 >0.05
Serum creatinine 1.68+0.36 1.75+0.60 0.36 >0.05
ESR 42.53+29.93 42.53+29.93 0.00 >0.05
Random blood sugar(mg) 134.13+16.48 133.46+15.54 0.14 >0.05
Table(5) Shows the prevalence of infections among the studied groups 48hrs or more after hospitalization.:
Infections G1
(N=15)
GIIa
(N=15)
GIIb
(N=15)
GIIC
(N=15)
X2 P-Value
No % No % No % No %
At
admission:
0 0 0 0 0 0 0 0
After 48 h: 1 6.7 2 13.3 4 26.7 7 46.7 7.83 <0.05
Pneumonia 1 6.7 0 0 2 13.3 1 6.7 2.14 >0.05
Broncho
Pneumonia
0 0 1 6.7 0 0 1 6.7 2.07 >0.05
UTI 0 0 0 0 1 3.7 2 13.3 3.86 >0.05
SBP 0 0 0 0 1 6.7 2 13.3 6.86 >0.05
Cellulitis 0 0 1 6.7 0 0 1 6.7 2.07 >0.05

Table (6) shows comparison between the studied groups as regard type of organisms found
in different cultures and their antibiotic sensitivity 48hrs or more after hospitalization:
Parameters G1
(N=15)
GIIa
(N=15)
GIIb
(N=15)
GIIC
(N=15)
X2 P-Value
No % No % No % No %
B1ood culture:
Gm +ve
staph
aureus for
meronem
0 0 1 6.7 0 0 1 6.7 0.74 >0.05
Gm +ve
strept for
augmentin
0 0 0 0 1 6.7 0 0 3.0 >0.05
Urine culture:
Ecoli for
amikin
0 0 0 0 0 0 1 6.7 >0.05
Ecoli for
levofloxacin
0 0 0 0 0 0 1 6.7
Asceitic fluid culture:
Ecoli for
cefotaxime
0 0 0 0 1 6.7 0 0 3.0 >0.05
Ecoli for
ceftriaxone
0 0 0 0 0 0 1 6.7 3.0 >0.05
Sputum culture:
Strept
pneumonia
for
augmentin
1 6.7 0 0 0 0 0 2 13.3 >0.05
Strept
pneumonia
for
meronem
0 0 0 0 0 1 6.7 0 0 >0.05
Strept
pneumonia
for
zithromax
0 0 1 6.7 0 0 0 0 0 >0.05
Discussion
Bacterial infections in cirrhotic patients is regard
as an important cause of death in cirrhotics (9). it`s
estimated to cause up to 25% of deaths in cirrhotic
patients (10). This study was done on sixty patients-
admitted to Tropical Medicine department in
Menoufiya university hospital - Their ages ranged
from 40 to 60 years and fourty of them were
males (66.6%) and twenty of them were females
(33.3%). In the present study, the incidence of
infections in hospitalized cirrhotic patients was
29% (13/45). Prospective series from 1990s
described an incidence of bacterial infections in
hospitalized cirrhotic patients of 47% (4), 20% (12),
32% (13) and in one egyptian study it was 60% (14).
The present study clarified that, nosocomial
infections in non cirrhotic patients was 6.66% (1/15). Nosocomial infections may be also attributed
to frequent hospitalization and long hospital stays
of decompensated cirrhotic patients (15), In the
present study the prolonged hospital stay of
infected groups was attributed to drawback of
infectious episodes and not considered as arisk
factor for infection. Various risk factors for
nosocomial infections in patients with liver
cirrhosis have been studied and the present study
demonesterated that, the more advanced liver
disease, the higher is the propensity to infection as
susceptibility to infection was higher in patients
with child C than patients with child A and B

classes(P value < o.o5) and this result was also
reported by Toledo et al.,1999 (16), Yoshida et al.,
2003 (13) and Goulis et al., 2008 (7). In the present
study there was no statistically significant
difference among studied groups as regard age
and sex as risk factors for infection that is also
was in agreement with Follo et al., 1994 (18) and
Goulis et al., 2008 (7) while, this was disagreed by
Bac et al., 1994 (19) who reported that, increasing
age was a risk factor of acquiring infection among
immunocompromized patients. Bacterial
infections are not frequently presenting with full
clinical picture in cirrhotic patients (20). often
recognition of infection is made more difficulty
by the absence of the typical clinical features of
infection that is,fever, rigors,hypotension,other
symptoms according to the site of infection and
leucocytosis,in which case the only clues may be
deterioration of hepatic functions,precoma or
coma or impaired renal functions (17). In the
present study, the clinical manifestations of
infections were more significantly present among
child C patients such as, fever and toxic look and
this was also reported by Navas et al.,1999 (21)
who revealed that, fever, rigors & manifestations
of toxaemia are the most prevelant manifestations
among infected cirrhotic patients while, Kuo et
al.,2001 (22) revealed that, the deterioration of
clinical state of the patients such as, precoma or
coma was the main clue for diagnosing infection
in cirrhotic patients. In the present study the main
clue for diagnosing acquired infection in cirrhotic
patients as regards laboratory investigations which
were done at patients admission and repeated 48
hrs or more after hospitalization was leucocytosis
(TLC>11000) which was recorded in almost all
infected patients 100% and this result was in
agreement with Marilyn et al 2003(28) and Fiuza et
al.,2000(24) who was clarified that, the main
changes in studied investigations among infected
hospitalized patients especially immuno-
compromized patients were peripheral blood
leukoccytosis 90%,deterioration in liver function
tests and impairement of renal functions.while,
these results were disagreed by Angeloni et
al.,2008 (25) who reported that, the main clue for
diagnosing acquired infections among
hospitalized cirrhotic patients was the clinical
deterioration such as, precoma or coma as the
changes in laboratory investigations were not
significantly different among cirrhotic patients
before and after acquiring infection as
leucocytosis was reportrd in 20% of infected
patients. In the present study the most prevalent
aetiology of cirhhosis was chronic hepatitis C
which was significantly present among cirrhotic
patients and this was correlated with different
studies as regards the aetiologies of cirrhosis
which were revealed that, the chronic hepatits C is
one of the most important and prevelant cause of
cirrhosis worldwide(26), (27) and (8). In the present
study the most common acquired nosocomial
infections among cirrhotic patients was chest
infections 38.5% (5/13) followed by urinary tract
infection23%, this was attributed to invasive
procedures that are used such as, endotracheal
intubation,oxygen masks and urinary catheters
followed by spontaneous bacterial peritonitis23% (3/13) and soft tissue infections in the form of
cellulitis15.5% (2/13).These results were in
agreement with Borzio et al.,2001 (20) who was
reported that, chest infections especially bacterial
pneumonia is the most prevalent infection 41%
among immuno compromized patients especially
who were admitted in intensive care units while,
these results were in disagreement with Navasa et
al.,1999 (21) who reported that, the most common
infections in cirrhotic patients was spontaneous
bacterial peritonitis 32%, urinary tract infection
11% , chest infections 11% , bacteraemia 4% and
soft tissue infections 2%. Approximately, 75% of
nosocomial bacterial infections in cirrhotic
patients are caused by gram negative bacteria (E-
coli, Klebsiella pneumoniae, Aeromonas
hydrophila, Pseudomonas and Vibrio spp)
especially in spontaneous bacterial peritonitis and
urinary tract infections, whereas, gram positive
bacteria comprise 21.2% (Staphylococcus aureus,
Streptococcus pneumonia, Streptococcus viridans
and Anaerobes comprise only 3.5% (Bacteroids
and Peptostreptococcus spp) (30). In the present
study, the most common isolated organisms were

gram-ve organisms including (E-coli and
pseudomonas) in 46% (6/13) and gram +ve
organisms including (strept pneumonia and staph
aureus) in 54% (7/13). simillar results were also
documented by Deschenes and Villeneure 1999 (12) and Borzio et al., 2001 (20). The causative
organisms in chest infection and soft tissue
infection (cellulitis) was gram +ve cocci (Staph
aureus and Strept pneumonia) while, the causative
organisms of spontaneous bacterial peritonitis and
urinary tract infection were gram -ve bacilli (E-
coli and pseudomonas).
Conclusions
From this study we can conclude that,
Nosocomial infections are more common among
patients with liver cirrhosis especially Child c
patients than other general hospital populations,
the most common type of acquired infections
were respiatory infections follwed by urological,
ascitic fluid infection and cellulitis and the most
common causative organisms were bacterial
especially gram positive Cocci.
References
1. Mc bride ES:An investigation of contact
transmission of methicillin-resistant staphylococcus
aureus.Journal of Hospital Infection 2004, 58,104-
108.
2. Bernardi M: Clinical significance and outcome of
nosocomial acquisition of spontaneous bacterial
peritonitis in liver cirrhosis, Int. Emerg. Med 2010,
1, 37-44.
3. Carven DE, Kunches LM and Leitenberg DA :
Nosocomial infection and fatality in medical and
surgical intensive care unit patients.Arch intern
med 1998,148,5,1161-8.
4. Fernandez J, Navasa M and Gomez J: Bacterial
infections in cirrhosis: Epidemiological changes
with invasive procedures and norfloxacin
prophylaxis. Hepatology 2005, 35: 140-148.
5. Soriano G, Guarner C and Tomas A: Norfloxacin
prevents bacterial infection in cirrhotics with
gastrointestinal haemorrhage.
Gastroenterology;1992, 103: 1267-1272.
6. Riordan SM and Williams R: Mechanisms of
hepatocyte injury, multiorgan failure and
prognostic criteria in acute liver failure. Semin
Liver Dis 2003, 23: 203-215.
7. Goulis J, Patch D and Burroughs AK: Bacterial
infections in the pathogenesis of variceal bleeding.
Lancet 2008, 353: 139-142
8. Vilstrup H:Cirrhosis and bacterial infections. Rom J
Gastroenterol 2003,12: 297-302.
9. Rose C, Michalak A and Rama R: L-ornithine-L-
aspartate lowers plasma and cerebrospinal fluid
ammonia and prevents brain edema in rats with
acute liver failure. Hepatology 2006, 30: 636.
10. Kang CI, Song JH, Chung DR and Yong KG:
Liver cirrhosis as a risk factor for mortality in a
national cohort of patients with different underlying
diseases.J Infect 2011, 63,5,336-343.
11. Caly WR and Strauss E:Aprospective study of
bacterial infections in patients with cirrhosis,J
Hepatol 1993, 18,353-358.
12. Deschenes M and Villeneure JP:Risk factots for the
development of bacterial infections in hospitalized
patients with cirrhosis, Am J Gastroenterol 1999,
94,8,2193-2197.
13. Yoshida H, Hamada T, Inuzuka S, Ueno T and
14. Tanikawa K:Bacterial infections in cirrhosis with
and without hepatocellular carcinoma. Am J
Gastroenterol 2003, 88,12, 2067-2071.
15. Arafat MA and Awny G:Aprospective study of
bacterial infections in patients with liver
cirrhosis.The New Egyptian journal of Medicine
1994, 11, 2, 1123-1127.
16. Campillo B,Richardet JP and Kheo T:Nosocomial
Spontaneous bacterial peritonitis and bacteremia in
cirrhotic patients,impact of isolated type on
prognosis and characteristics of infection ,Clin
Infect Dis 2002, 35,1,1-10.
17. Toledo C, Flores C and Aaenz M :Bacterial
infections in hepatic cirrhosis. RevMed Chil 1999,
122,7, 788-794.
18. Kastlezan SB, Stomka M, Celinski K, Serwacki M,
Szczerbinski M and Cichoh H: Prevalance of
spontaneous bacterial peritonitis in asymptomatic
patients with liver cirrhosis. Adv Med Sci 2011,
56,1,13-17.
19. Follo A, Liovet JM and Navasa M: Renal
impairement after spontaneous bacterial peritonitis
in cirrhosis : Incidence, clinical course, predictive
factors and prognosis. Hepatology 1994, 20,1495-
1501.
20. Bac DJ ,De Marie S and Siersema PD: post
sclerotherapy bacterial peritonitis, complications of

sclerotherapy of variceal bleeding. AM J
Gastrenterol 1994, 89,859-862. 20-Borzio M,
Salerno F and Piantoni L:Bacterial infections in
patients with advanced cirrhosis, multicenter
prospective study.Dig Liver Dis 2001 ,33,4,41-48.
21. Navasa M, Fernandez J and Rhodes J: Bacterial
infections in liver cirrhosis. Ital J Gastroenterol
Hepatol 1999, 31,7,16-25.
22. Kuo CH, Changchien CS and Yang CY:
Bacteraemia in patients with cirrhosis of the
liver.Liver 2001,11,334-339.
23. Gomez F,Ruiz P and Scheiber AD:Impaired
functions of macrophages Fc-gamma receptors and
bacterial infections in alcoholic cirrhosis. N Eng
Med 1994, 331,1122-1128.
24. Fiuza C, Salcedo M and Clemente G:In vivo
neutrophil dysfunction. J Infect Dis 2000,
182,2,526-533.
25. Angeloni S,Leboffe C and Parente A :Efficacy of
current guidelines for the treatment of spontaneous
bacterial peritonitis in the clinical practice.World J
Gastroenterol 2008, (14), 2757-2762.
26. Brann OS :Infectious complications of cirrhosis.
Curr Gastroenterol 2001, 3,4,285-292.
27. Sherlock S and Dooley J: Diseases of the liver and
biliary system 11th edition. Black well scientific
publication, Oxford, London, Edinburgh., hepatic
encephalopathy 2002, 86-100.
28. Marilyn G, Foreman, David M and Marc Moss:
Cirrhosis is a risk factor for sepsis and
death;Analysis of the national hospital discharge
survey.Cest 2003, 124,3,1216-1250.
29. Navasa M and Rhodes J: Bacterial infections in
liver cirrhosis. Liver international 2004, 24,4,277-
280.
30. Horan TC, Andrus M and Dudeck MA:CDC/NHSN
surveillance definition of health care-associated
infections and criteria for specific types of
infections in the acute care setting.Am J Infect
Control 2008, 36,5,309-332.

Original Article
The Role of Serum Alpha Feto Protein Isoform 3(L3) and Magnetic Reosonance
Imaging in the Assessment of Management of Hepatocellular Carcinoma
Mohamad Kassem1, Akram Deghady2, Nasser Abd Allah1, Hossam Abo El Kheir1, Mohamed El Shafei3, Marwa
Ibrahim1
Tropical Medicine1, Clinical and Chemical Pathology2 and Radiodiagnosis Departments3, Faculty of Medicine,
Alexandria University.
ABSTRACT
The aim of this work was to study the serum level of Alpha feto protein iso form L3 in patients with HCC before and
after management (Radiofrequency Ablation, TACE) combined with contrast enhanced MRI, to diagnose early
recurrence. Subjects and Methods: Serum level of Alpha Feto Protein L3 was measured using an ELISA kit in 50
subjects divided into three groups; group I consisted of twenty patients with HCC before and after radiofrequency
ablation (RF), group II Twenty patients with HCC before and after TACE, group III Ten patients with cirrhosis without
HCC. Response to treatment was determined using contrast enhanced MRI. Results: Regarding serum Alpha Feto
Protein L3, There was a significant difference between the studied groups before intervention and controls but no
significant difference between groups after intervention and controls. There was no significant correlation between
alpha feto protein L1 and response to intervention, on the other hand a significant positive correlation was found
between the studied groups after intervention regarding Alpha feto protein L3 and response to intervention. In the
present study, a cutoff value of AFP-L3 was 26.0 IU was obtained to determine the respose to therapy. Values less than
or equal to 26.0 IU was associated with a complete response with a sensitivity of 87% and a specificity of 50%.
Conclusion: Combination of AFP-L3 and Contrast enhanced MRI could improve the diagnostic value for HCC
detection in patients with or without increased AFP levels. AFP-L3 study provides a clue in HCC detection in patients
with persistent elevation of AFP. The sensitivity of AFP-L3 from our study was generally around 87%, while the
specificity was around 50 %.
Introduction
Hepatocellular carcinoma (HCC) is one of the
most common cancers worldwide, and has a poor
prognosis unless treated. In patients with un-
resectable tumors, the median survival is less than
four months, whereas in patients with less-
advanced disease, survival is less than one year if
left untreated. (1) In many countries, the incidence,
recurrence and mortality rates of liver cancer
remain high. Clinical studies have shown that
there is a close relationship between the level of
serum AFP and HCC incidence, recurrence and
metastasis. Serum AFP level has been used as the
main index of prediction for HCC prognosis after
therapy. (2-4). Treatment options for patients with
un-resectable HCCs are transarterial
chemoembolization (TACE) or transarterial
radiembolization (using yttrium-90 microspheres).
These transarterial therapies are based on the idea
that HCC is supplied mainly by the hepatic artery.
TACE causes a cytotoxic effect on malignant
cells, as well as obliteration of the feeding arteries
of the tumor. (5) Ablative therapies are the second
choice for patients with liver tumors who are not
eligible for surgery (because of advanced liver
disease, or because of the location of the tumor).
Local ablation also may be used to control HCC
while awaiting transplantation. (6). These therapies
are known to have low morbidity and mortality, as
well as being less expensive than surgical
resection. Other advantages of ablative therapies
compared with surgery include the possibility of
real-time imaging guidance, and the ability to
perform these procedures on outpatients. (7).
Alpha-fetoprotein (AFP) and ultrasonography are
two important noninvasive modalities for early

detection of hepatocellular carcinoma (HCC). (8)
Cirrhotic nodules are found frequently with
increasing use of abdominal ultrasound. (9) AFP
elevation is not uncommon in such cases because
liver inflammation is generally coexistent in the
cirrhotic liver. (10. 11) AFP-L3 is a fucosylated
species of AFP that is the product of α1-6 fucosyl
transferase in the presence of GDP fucose. (12).
This enzyme activity was higher in HCC tissues
than in the surrounding non tumor tissue.
Therefore, AFP-L3 is considered more specific
than AFP in diagnosis of HCC. It has been used
for early detection of HCC and evaluation for
recurrent tumor after treatment. AFP-L3 dynamics
are largely related to the degree of biological
malignancy of hepatocellular carcinoma. (13).
Besides detecting and diagnosing the HCC
lesions, contrast enhanced computed tomography
(CT) and magnetic resonance imaging (MRI) are
widely used in the post-treatment follow-up of
these patients, for the detection of residual or
recurrent tumors after treatment, as well as for the
detection of post-treatment complications. The
early detection of residual or recurrent tumor is
important for planning new interventions. (14).
There is suggestive evidence that MRI is more
accurate than other radiological modalities in the
detection of residual or recurrent tumors. (15)
Preliminary studies are being conducted to assess
the role of diffusion-weighted MRI and MR
spectroscopy in addition to conventional MRI in
evaluating tumor response after loco-regional
therapies. (16). The aim of this study was to study
the serum level of Alpha feto protein iso form L3
in patients with HCC before and after
management (Radiofrequency Ablation, TACE)
combined with contrast enhanced MRI, to
diagnose early recurrence.
Patients and Methods
Patients and diagnosis: Serum level of Alpha Feto
Protein L3 was measured using an ELISA kit in
50 subjects divided into three groups; group I
consisted of twenty patients with HCC before
and after radiofrequency ablation (RF), group II
Twenty patients with HCC before and after
TACE, group III Ten patients with cirrhosis
without HCC. Response to treatment was
determined using contrast enhanced MRI.
Methods: In our study, HCC was diagnosed by
Triphasic CT abdomen and serum Alpha feto
protein (L1). The following Patients were
excluded from interventional therapy: - Stage (C)
HCC with portal invasion. -Stage (D) HCC with
distant metastasis. - Child C patients.
Measurement of Alpha Feto protein L3: - Serum
Alpha Feto Protein L 3. (AFP-L3 ELISA Kit
(Catalog No: E1117h): AFP.L3 ELISA kit applies
the quantitative sandwich enzyme immunoassay
technique. 11. Response to therapy was determined
using Contrast enhanced MRI.
Statistical Analysis
All analyses were performed using ANOVA test.
All values are expressed as the mean ±standard
deviation. Variables significantly deviating from
normal distribution were logarithmically
transformed. (F = ANOVA test, P = probability).
Results
In our study, there was a significant difference
regarding BUN and serum creatinine before and
after RF and between controls and the studied
groups after intervention. There was also a
significant difference in radiofrequency ablation
group before and after intervention with fasting
blood sugar level. Regarding liver enzymes there
was a significant difference before and after
TACE and between controls and the studied
groups after intervention in the present study.
Regarding direct serum bilirubin, there was a
significant difference before and after RF, and
between controls and the studied groups after
intervention. Regarding prothrombin activity, a
significant difference was found in group I. Also a
significant difference between the studied groups
after intervention and controls as regards the
prothrombin activity. Also a significant difference
was found in TACE patients before and after
intervention regarding serum GGT and Alkaline
phosphatase. There was also a significant
difference between the studied groups before

intervention and controls as well as groups after
intervention and control. In the present study,
Regarding Serum alpha feto protein l1, a
significant difference (reduction) was found in RF
patients before and after intervention as regard the
level of apha feto protein l1, also a significant
difference (reduction) was found in TACE
patients before and after intervention. Also a
significant difference was found in RF patients
before and after intervention as regard the level of
apha feto protein l3, also a significant difference
was found in TACE patients before and after
intervention. There was a significant difference
between the studied groups before intervention
and controls but no significant difference between
groups after intervention and controls. (Table1;
Figure 1) There was no significant correlation
between alpha feto protein L1 and response to
intervention, on the other hand a significant
positive correlation was found between the
studied groups after intervention regarding Alpha
feto protein L3 and response to intervention. In
the present study, a cutoff value of AFP-L3 was
26.0 IU was obtained to determine the respose to
therapy. Values less than or equal to 26.0 IU was
associated with a complete response (assessed by
Contrast enhanced MRI) with a sensitivity of 87%
and a specificity of 50%. (Figure 2) (Figure 3)
(Figure 4). In our study a significant difference
was found in RF patients before and after
intervention as regard the level of C reactive
protein (CRP), also a significant difference was
found in TACE patients before and after
intervention. Regarding serum D dimer, a
significant difference was found in RF patients
before and after intervention as regard the level of
D dimer, also a significant difference was found
in TACE patients before and after intervention.
There was a significant difference between the
studied groups before intervention and controls.
Table (1): Comparison between the different studied groups regarding alpha-feto protein l3, alpha-feto protein l1
Group
P1 P2 Pts subjected to RF Pts subjected toTACE Controls
Before After Before After
Alpha feto protein l3
0.001* 0.089
Minimum 1.0 1.0 1.5 1.0 1.2
Maximum 50.0 21.0 24.0 12.0 13.0
Mean 23.7 6.2 12.5 3.2 5.2
SD 16.4 5.8 6.6 3.5 4.9
Median 17.0 3.3 12.0 1.6 1.8
P+ 0.000* 0.000*
Alpha.feto protein L1
0.209 0.115
Minimum 5.1 5.1 2.5 10.0 120.0
Maximum 829.0 111.0 720.0 210.0 120.0
Mean 161.6 32.4 170.8 62.4 120.0
SD 236.3 33.9 179.1 64.5 0.0
Median 55.0 22.0 111.5 21.5 120.0
P+ 0.004* 0.000*
Z: Wilcoxon test
* P < 0.05 (significant

Figure (1): Comparison between the different studied groups regarding Serum alpha feto protein L3 (IU /L)
Area Under the Curve
Test Result Variable(s): alfa.l3
Area Std. Error Asymptotic Sig. Asymptotic 95% Confidence Interval
Lower Bound Upper Bound
.653 .110 .186 .438 .868
Fig (2): The receiver operating characteristic (ROC) curve for AFP-L3 in the total number of study patients. (IU /L)

Figure (3): male patient 62 years with HCC on cirrhotic liver managed by TACE and follow up MRI showing heterogeneous
signal intensity in T2 (a) with no definite activity in triphasic study ( b-d)

Figure 4: (a) De novo HCC at segment IV, (b,c) showing T2 hyperintense signal, (d) washin washout enhancement dynamics
with delayed capsular enhancement in triphasic study (e,f)
Discussion
In the present study, Regarding Serum alpha feto
protein l1, a significant difference (reduction) was
found in RF patients before and after intervention
as regard the level of apha feto protein l1, also a
significant difference (reduction) was found in
TACE patients before and after intervention. Also
a significant difference was found in RF patients
before and after intervention as regard the level of
apha feto protein l3 (P = 0.000*), also a

significant difference was found in TACE patients
before and after intervention (P = 0.000*). There
was a significant difference between the studied
groups before intervention and controls but no
significant difference between groups after
intervention and controls (P1 = 0.001*, P2 =
0.089*) respectively. There was no significant
correlation between alpha feto protein L1 and
response of intervention (Z = 0.54, 1.6
respectively) (p = 0.589, 0.117) respectively, in
the other hand a significant positive correlation
was found between the studied groups after
intervention regarding Alpha feto protein L3 and
response to intervention (Z = 4.3, p = 0.000*)
Karger AG et al, (17) found that when serum
Alpha feto protein L 3 levels before and at six
months after treatment were compared, 599 cases
remained negative, 113 remained positive, 83
underwent conversion from positive to negative
(negative conversion), and 46 underwent
conversion from negative to positive (positive
conversion). When survival rates were
investigated, the constantly negative and negative
conversion groups had more favorable survival
rates than the constantly positive and positive
conversion group. Beppu et al, (18) found that
regarding the cumulative recurrence-free survival
rates by elevation of pretreatment fetoprotein
(AFP) in patients who underwent the combination
of chemoembolization and RFA, There was no
significant difference between patients with or
without elevated pretreatment AFP levels
(P=0.7045). Regarding the cumulative recurrence-
free survival rates by elevation of pretreatment
Lens culinaris agglutinin A-reactive fraction of
AFP (AFP-L3) in patients who underwent the
combination of chemoembolization and RFA.
Beppu et al, (18) found also that the recurrence-
free survival rate was significantly lower in
patients with than without elevated pretreatment
AFP-L3 levels (P=0.0231). In the present study, a
cutoff value of AFP-L3 was 26.0 IU was obtained
to determine the respose to therapy. Values less
than or equal to 26.0 IU was associated with a
complete response with a sensitivity of 87% and a
specificity of 50%. Cheng H et al, (19) in the total
number of his study patients; both sensitivity and
specificity of AFP-L3 used for prediction of HCC
in the following 2 years were 71% if the cutoff
value was 15%. The sensitivity decreased to
66.5% while the specificity increased to 82% if
the cutoff ratio was 17.5%. In our study a
significant difference was found in RF patients
before and after intervention as regard the level of
C reactive protein (CRP), also a significant
difference was found in TACE patients before and
after intervention. While no significant difference
was found between the studied groups before
intervention and controls, a significant difference
was found for groups after intervention and
controls. Zhiyun Z et al, (20) pooled results showed
that high expression level of serum CRP (≥10
mg/L) was associated with poor overall survival
and recurrence free survival in HCC. Serum CRP
overexpression (≥10 mg/L) was also significantly
associated with the presence of tumor vascular
invasion, multiple tumors, larger tumor size, and
advanced TNM stage. He also found that serum
CRP overexpression (≥10 mg/L) tended to be
correlated with poor differentiation. Regarding
serum D dimer, a significant difference was found
in RF patients before and after intervention as
regard the level of D dimer, also a significant
difference was found in TACE patients before and
after intervention. There was a significant
difference between the studied groups before
intervention and controls. Chien-Sen T et al, (41)
found an elevation of plasma D-dimer levels
which indicates the activation of coagulation and
fibrinolysis. He also found plasma D-dimer levels
to be correlated with the presence of central
necrosis, higher Child's grade, advanced TNM
stage, and the presence of portal vein thrombosis
when plasma D-dimer levels were compared
between different clinic-pathologic groups. In the
present study, a significant positive correlation
was found in groups before intervention regarding
serum levels of alpha feto protein L1 and L3 , on
the other hand a negative correlation was found
between groups after intervention regarding serum
levels of alpha feto protein L1 and L3. AFP L1
has been proposed as a predictor of patient

survival and tumor recurrence after surgery, loco-
regional therapies, and systemic chemotherapy.
This new role derives from the strong correlation
detected between AFP values, tumor dimensions,
and microvascular invasion, all well-known
predictors of HCC recurrence. AFP-L3, is also
extremely useful as an index of prognostication
and for the degree of biological malignancy of
hepatocellular carcinoma. (22) . Tateishi R et al, (23)
an analysis performed on 416 patients showed that
AFP >100 ng/mL and AFP-L3 >15% before
radiofrequency ablation were significant
predictors for the risk of HCC recurrence and
were significantly correlated with each other.
AFP-L3 was related to progression from
moderately differentiated to poorly differentiated
HCC.
Conclusions
Combination of AFP-L3 and Contrast enhanced
MRI could improve the diagnostic value for HCC
detection in patients with or without increased
AFP levels. AFP-L3 study provides a clue in HCC
detection in patients with persistent elevation of
AFP. The sensitivities of AFP-L3 from our study
were generally around 87%, while the specificity
was around 50 %.AFP-L3, is extremely useful as
an index of prognostication and for the degree of
biological malignancy of hepatocellular
carcinoma. AFP-L3 levels should be followed
closely to predict and detect HCC recurrence
following RFA and TACE
Recommendations
Tumor markers have almost the same utility for
the detection of recurrent HCCs after therapy as
for detection of initial HCCs, therefore it is
strongly recommended the combined
measurement of Alpha feto protein L1 and L3 to
predict and detect HCC recurrence following RFA
or TACE. Further studies are needed to clarify the
relationship between the size of the tumor and
Alpha feto protein L3 level.We recommend post
treatment quantitative measurement of CRP to
determine response to treatment.We recommend
the alternate use of triphasic computerized
tomography and contrast enhanced MRI for
follow up after intervention in HCC.
References
1. Cha C, DeMatteo RP, Blumgart LH. Surgery and
ablative therapy for hepatocellular carcinoma. J Clin
Gastroenterol 2002; 35: S130–S7.
2. Baig JA, Alam JM, Mahmood SR, Baig M, Shaheen R,
Sultana I,et al: Hepatocellular carcinoma (HCC) and
diagnostic significance of Afetoprotein (AFP). J Ayub
Med Coll Abbottabad 2009, 21:725.
3. Tong MJ, Hsien C, Song JJ, Kao JH, Sun HE, Hsu L, et
al: Factors associated with progression to
hepatocellular carcinoma and to death from liver
complications in patients with HBsAg-positive
cirrhosis. Dig Dis Sci 2009; 54:1337–46.
4. Chan SL, Mo FK, Johnson PJ, Hui EP, Ma BB, Ho
WM, et al: New utility of an old marker: serial alpha-
fetoprotein measurement in predicting radiologic
response and survival of patients with hepatocellular
carcinoma undergoing systemic chemotherapy. J Clin
Oncol 2009, 27:446–52.
5. Braga L, Guller U, Semelka RC. Pre-, peri-, and post-
treatment imaging of liver lesions. Radiol Clin North
Am 2005; 43:915–27.
6. Befeler AS, Di Bisceglie AM. Hepatocellular
carcinoma: diagnosis and treatment. Gastroenterology
2002; 122:1609–19.
7. Goldberg SN, Gazelle GS, Mueller PR. Thermal ablation
therapy for focal malignancy: a unified approach to
underlying principles, techniques, and diagnostic
imaging guidance. AJR Am J Roentgenol 2000;
174:323–31.
8. Liaw YF, Tai DI, Chu CM, Lin DY, Sheen IS, Chen TJ,
et al. Early detection of hepatocellular carcinoma in
patients with chronic type B hepatitis: a prospective
study. Gastroenterology 1986;90:263–7.
9. Fujiyama S, Tanaka M, Maeda S, Ashihara H, Hirata R,
Tomita K.. Tumor markers in early diagnosis, follow-
up and management of patients with hepatocellular
carcinoma. Oncology2002;62: 57–63.
10 . Liaw YF, Tai DI, Chu CM, Chen TJ. The development
of cirrhosis in patients with chronic type B hepatitis: a
prospective study. Hepatology 1988;8:493–6.
11. Oka H, Tamori A, Kuroki T, Kobayashi K, Yamamoto
S. Prospective study of alpha-fetoprotein in cirrhotic
patients monitored for development of hepatocellular
carcinoma. Hepatology 1994;19:61–6.
12. Tamura Y, Igarashi M, Suda T, Wakai T, Shirai Y,
Umemura T, et al: Fucosylated fraction of alpha-
fetoprotein as a predictor of prognosis in patients with
hepatocellular carcinoma after curative treatment. Dig
Dis Sci 2010;55:2095–101.
13. Tada T, Kumada T, Toyoda H, Kiriyama S, Sone Y,
Tanikawa M, et al: Relationship between Lens culinaris

agglutinin-reactive alpha-fetoprotein and pathologic
features of hepatocellular carcinoma. Liver Int
2005;25:848–53.
14. Braga L, Guller U, Semelka RC. Pre-, peri-, and post-
treatment imaging of liver lesions. Radiol Clin North
Am 2005; 43:915–27.
15. Vossen JA, Buijs M, Kamel IR. Assessment of tumor
response on MR imaging after locoregional therapy.
Tech Vasc Interv Radiol 2006; 9:125–32.
16. Cho YK, Kim JK, Kim MY, Rhim H, Han JK.
Systematic review of randomized trials for
hepatocellular carcinoma treated with percutaneous
ablation therapies. Hepatology 2009; 49:453–9.
17. Karger AG and Kudo M. Alpha-fetoprotein-L3: Useful
or Useless for Hepatocellular Carcinoma. Liver Cancer
2013;2:151–2.
18. Beppu et al: Tumor markers in recurrent HCC.
International journal of molecular medicine;2010 ;26:
425-33.
19. Cheng H.T, Hau-Tsai C,Ya-Hui C, Yang-Yuan C,
Tzong-Hsien L, Dar-In T et al. AFP-L3 in liver
diseases with high AFP. J Chin Med Assoc
2007;70(8):310–7.
20. Zhiyun Z, Lin Z, Sheng G, Zhe Y, Jia y, Shusen Z.
Prognostic Role of C-Reactive Protein in
Hepatocellular Carcinoma: A Systematic Review and
Meta-Analysis. Int J Med Sci 2013; 10(6):653-64.
21. Chien-Sen T, Hoi-Wan L, Pao-Huei C, Wan-Long C,
Chung-Chou J, Chen-Guo K. Clinical significance of
plasma D-dimer levels and serum VEGF levels in
patients with hepatocellular carcinoma.Hepato-
gastroenterology 2004; 51(59):1454-8.
22. Lai Q, Merli M, Ginanni S et al., “Predictive factors of
recurrence of hepatocellular carcinoma after liver
transplantation: a multivariate analysis,”
Transplantation Proceedings 2009;41,(4), 1306–9.
23. Tateishi R. Percutaneous radiofrequency ablation for
HCC. An analysis of 1000 cases. Cancer 2006;
103:1201-9
.