Embed Size (px)
Citation preview

EUROPEAN BOARD OF SURGERY EXAMINATION IN SURGICAL ONCOLOGY
2014
European Society of Surgical OncologyEducation and Training Committee – President: Dr. Lynda WyldReport presented by Ibrahim Edhemovic

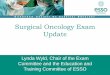
THE EBSQ SURGICAL ONCOLOGY EXAMINATION
0
5
10
15
20
25
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Applicant number

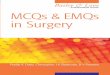
SURGICAL ONCOLOGY EXAM GEOGRAPHYCountry Spain Germany
Swiss UK
Hungary Czech Rep
Austria Cyprus
Belgium Greece
Arab Portugal
Turkey India
Ireland France
Croatia slovenia
italy

2014 CANDIDATE NUMBERS
• 23 applicants: all applicants eligible based on criteria
• 3 apologies: withdrawals for personal reasons
• 2 no shows
• 18 candidates examined

EXAM COMMITTEE: THE ETC OF ESSO
Name Gender Nationality Specialty
Lynda Wyld f UKBreast, sarcoma
Beate Rau f German HIPEC, pelvic, sarcoma and lung
Michel Rivoire m French Upper GI/HPB
Geerard Beets m NetherlandsColorectal
Marjut Leidenius f FinnishBreast
Odysseas Zoras m GreekMelanoma, sarcoma
Joost van der Vorst m DutchTrainee Representative
Ibrahim Edhemovic m SlovenianGI
Sergio Sandrucci m ItalianSarcoma, upper GI
Daniel Perez m Swiss Upper GI/HPB
Isabel Rubio f Spanish Breast
Dawid Murawa m PolishUpper GI and Breast
Plus additional examiners: Zen Rayter, Sebastian Aspinall and Marjolein Schmidt to cover breast and endocrine

2014 CANDIDATE SPECIALIST INTERESTS
Breast Endocrine Sarcoma Visceral (colorectal) Visceral (upper GI) Visceral (HPB) Melanoma
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X
X X X

MCQ 1: GENERAL SURGICAL ONCOLOGYCandidate Name %
1: Failed written 38
2 76
3 91
4 82
5 88
6: Borderline 58
7 82
8: Borderline 58
9: Borderline 52
10 64
11 61
12 64
13 70
14 82
15 88
16 73
17 73
18 70
Pass mark set using Anghoffreferencing. Borderline score +/-10% of pass mark.

EXCLUDED QUESTIONS
• 6 of the 40 MCQs were answered correctly by less than 20% (chance only)
• Review of questions: Poorly or confusingly phrased or overly specialist
• Excluded from analysis10
Which of the following statements regarding lung cancer is
incorrect
a Screening with computed tomography (CT) can reduce the
mortality in high risk patient populations
b Screening with CT produces an excessive number of false
positive findings
c Chest radiography is effective in screening for lung cancer
d Lung function tests are effective in the early detection of lung
cancer
e Serum antibody markers may be effective in screening for lung
cancer
Correct c
22 Which one of the following statements about types of medically utilised
radiation is incorrect
a Hypofractionation refers to the use of larger radiation doses per fraction
b Brachytherapy has a maximal radiation penetration depth of 2cm
c Accelerated fractionation is administration of normal fractions over a
shorter time span
d In most cases standard fractions are 1.8 to 2 Gy
e Protons deliver a minimal exit dose permitting normal tissue sparing
Correct b

MCQ 2: APPLIED CLINICALCandidate Number %
1 Failed 38
2: Borderline 56
3 88
4: Borderline 56
5 75
6 62
7 75
8 69
9 75
10 75
11: Borderline 50
12 69
13 94
14 56
15 81
16 68
17 63
18: Borderline 50
Pass mark set using Anghoff referencing. Borderline score +/- 10% of pass mark.

EXCLUDED QUESTIONS
• 4 questions had very poor scores of less than 20%
• Review indicated confusing, poorly written or overly specialist
• Excluded from analysis
3 Which one of the following statements about the use of acellular dermal
matrices (ADM) in breast reconstruction is incorrect?
a ADM are associated with a lower rate of capsule formation than fully
submuscular implant placement
b ADM reconstructions are associated with a higher short term failure rate
than non ADM procedures
c ADM reconstructions are associated with a higher rate of seroma
formation than non ADM reconstructions
d ADMs facilitate single stage or direct to implant reconstruction
e ADMs facilitate delayed reconstruction because of their high
elasticity
Correct e
20 A 64-year-old patient presents acutely with peritonitis. Past medical
history reveals type 2 diabetes, ischaemic heart disease, atherosclerosis,
weight loss of 8% within two months. Emergency abdominal CT shows air
under the diaphragm and cancer in the gastric body with infiltration
limited to the gastric wall and no dissemination. At laparotomy
perforation of the gastric tumour is confirmed. Which is the optimal
procedure?
a Two-stage surgery should be performed, dressing the
perforation/partial resection/gastrectomy during the emergency
laparotomy and completing the therapy, including total
gastrectomy and D2 lymphadenectomy, at a second stage
b If the patient’s general state is stable perform total gastrectomy
with D2 lymphadenectomy.
c Option a or b depending on clinical status
d Perform partial gastrectomy during the emergency laparotomy and
when the patient has recovered commence adjuvant ECF
chemotherapy in recognition of the fact that the disease was perforated
at presentation
e Dress the perforation during the emergency laparotomy. Instigate
palliative treatments as appropriate thereafter as perforation
means cure is not possible.
Correct c

ORAL EXAMINATION
• 2 viva examinations each of 30 minutes with 4 examiners
• 1 on academic papers and general theory
• 1 on specialist applied clinical cases

ACADEMIC VIVA
• Candidate have 1 hour to read 2 academic papers selected to reflect their nominated area of specialist interest
• 15 minutes examination on each with 2 examiners to discuss scientific critique and clinical relevance.
• Standard scoring criteria

CLINICAL VIVA
• 9 pre-submitted clinical cases with photos and radiology images
• Standard setting examiners meeting beforehand
• Standard numeric scores and subjective score (pass, fail, borderline)
• All borderline and fails discussed at examiners meeting to assess safety and competence to practice at consultant level in Europe.

ORAL EXAM RESULTName Academic Clinical
1: failed written. Did not sit oral exam NA NA
2 36 38
3 39 32
4 32 32
5 30 32
6 31 27
7 25 32
8: Failed oral exam, borderline on 1 written, fail
overall 12 24
9 22 28
10 36 33
11 27 28
12 28 22
13 40 32
14 36 34
15 39 36
16 34 30
17 34 30
18 32 24
Overall pass rate 16/18=89%

CESMA: EXTERNAL REVIEW
• Professor Zeev Goldik and Professor Daniel Mathysen from CESMA attended the exam as external observers
• Reviewed all documents and papers before the exam
• Reviewed protocols and quality assurance
• Observed examinations and interviewed candidates and examiners
• Attended examiners meeting and standard setting meeting

CESMA OUTCOME
• Anonymisation of candidates needed
• Independent scoring of vivas rather than by conferring between examiner pairs
• Generally to an acceptable standard
• Formal report awaited

PRIZE WINNERS
• Jean De Menezes (India): first prize
• 2 runners up:
• Hannes Neef and Andraz Perhavic




THANK YOU
• Special thanks to our external examiners: Professor Zeev Goldik and Professor Daniel Mathysen
• Special thanks to our administrative coordinators: Carine Lecoq and Ana Galan
• Thanks to the team of examiners!