Embed Size (px)
DESCRIPTION
Economic Benefits of Health Research in Saskatchewan (2008)
Citation preview
The Economic Benefits of Health Research in Saskatchewan
Prepared for: Saskatchewan Health Research Foundation
By:
Ian Peach, Director,
Saskatchewan Institute of Public Policy
Jim Marshall Chief Economist
Saskatchewan Institute of Public Policy
April 28, 2008

Disclaimer: This paper was prepared under contract from the Saskatchewan Health Research Foundation by the Saskatchewan Institute of Public Policy. All analysis, discussion and conclusions of the paper are the responsibility of the authors and do not represent the position of the Saskatchewan Health Research Foundation or of the Saskatchewan Institute of Public Policy.

Table Of Contents Executive Summary Page 1 I. Introduction Page 5 II. Direct and Indirect Economic Impact of Health Research Page 7
III. Productivity Benefits of Health Research Page 15 IV. Commercial Benefits of Health Research Page 19 V. Other External Benefits of Health Research Page 25 VI. Potential Savings to the Health Care System Page 29 VII. Conclusions Page 31


1
Executive Summary
Health research is primarily conducted to discover and develop better methods for maintaining, restoring or achieving a greater quality of life in the population through improved health. As such, all health research must first be aimed at improving health care or the prevention of health problems among the general population and must be judged primarily against that objective. There is an increasing interest, however, in a secondary impact of health research -- its economic and social effects within society. This study focuses on four main mechanisms by which socio-economic impacts are generated:
• the direct and indirect economic effects of health research activity itself; • the effect of health research on productivity within the economy; • the impact of the commercialization of health research; and • the influence of health research on reducing health care costs or increasing health
care effectiveness.
In looking at these mechanisms, the study attempts to identify the extent to which Saskatchewan has been affected by health research activity.
Research uses resources, in the form of labour and materials and capital equipment to produce a product, largely, knowledge, which may be further converted, in the case of medical sciences research, into treatments, prevention strategies, diagnostic technologies and other methods to improve health within the population. The employment of these resources in the research activity is itself an economic activity. Based on the data available, it is estimated that, in 2003, the total value of health research conducted in Saskatchewan was $79.7 million. By applying established input/output multipliers to this figure, one can estimate both the gross and net economic impact on the province of health research activity conducted within the province. The estimate of gross economic impact is:
• A direct contribution of $50.2M in Gross Domestic Product and a total (direct and indirect) contribution of $61.4M.
• A direct contribution of $79.7M to provincial output and a total contribution of $99.6M.
• A direct contribution of 1,238 jobs and a total contribution of 1,445 jobs. The estimated net impact (essentially the impact of funds coming into the province from outside sources, estimated to be $32M in 2003) is:
• A direct contribution of $20.2M in Gross Domestic Product and a total (direct and indirect) contribution of $24.6M.

2
• A direct contribution of $32.0M to provincial output and a total contribution of $40.0M.
• A direct contribution of 497 jobs and a total contribution of 580 jobs.
The value of the productivity gains in Saskatchewan of health research conducted in the province, on the other hand, is much more difficult to estimate, because of the way in which the productivity gains arising from research are dispersed. Productivity and longevity gains within Saskatchewan are minutely likely to have been derived from Saskatchewan research (as opposed to research elsewhere) and that Saskatchewan research is only minutely likely to improve productivity and/or longevity in Saskatchewan (even though it may have a large impact world-wide). While it may be possible to suggest that health science research in Saskatchewan has an expected social rate of return of 67 per cent, the social rate of return to Saskatchewan from Saskatchewan-based research is likely to be a very tiny fraction of that rate, since most benefits are likely to be derived by populations outside the province. Available information would suggest that there is also limited commercialization of health research occurring in Saskatchewan. The available lists of business enterprises in Saskatchewan engaged in pharmaceutical and medicine manufacturing and medical equipment and supplies manufacturing suggest that such businesses in the province are only rarely engaged in the conversion of health research into commercial products. There are, however, input/output multipliers available for these two industries in Saskatchewan and these estimate that an investment of $1M in pharmaceutical manufacturing in Saskatchewan would add a total of $90,000 to the province’s Gross Domestic Product, $1.3M to total output, and 13.96 jobs (considering both the direct and indirect impact). Similarly, an investment of $1M in the manufacture of medical equipment and supplies would add a total of $650,000 to the province’s Gross Domestic Product, $1.21M to total output, and 12.29 jobs (considering both the direct and indirect impact). This data can also be used on for evaluation of specific research projects, by applying them to the product of the potential total value of commercialization to follow a research project times the probability that commercialization will be achieved and will be located in Saskatchewan. It may also be possible that the process of conducting health research attracts other people to work in Saskatchewan in health and health sciences who would not otherwise choose to come here. In addition to the attraction of health and science workers, it may also be possible that health research attracts and retains a student population in the province which would otherwise choose to study elsewhere. These two pools of resources, people who work in health and related science occupations and those who study in related areas, provide the basis for continuing health care advancements in the province, including potential further research into health and health care. From 1996 to 2006, there has been an overall increase in employment of 7,300 (27.9 per cent) in “Health Occupations” in Saskatchewan and an increase of 6,900 (or 46.0 per cent) in employment in “Natural and Applied Sciences and Related Occupations”.

3
Overall, the two occupations have increased by 14,200 employees (or 34.5 per cent) in the ten year period between 1996 and 2006. It appears that employment in the two occupations most likely to be affected by health research has increased fairly steadily since 1996 and, more to the point, more rapidly than the overall growth in employment in the province. While these two occupations comprised 9.0 per cent of the overall employment in the province in 1996, by 2006, they made up 11.3 per cent of the provincial total employment, even though overall employment in the province had risen by almost 35,000 (or 7.6 per cent) over that period. It is not possible to estimate how important the role of health research is in individuals’ choices of employment, especially in light of other dominant determinants such as availability of employment and relative wage rates. Nevertheless, the important and growing proportion of employment in the province may be encouraged somewhat by the fact that health-related research is funded within Saskatchewan. Another potential indirect impact of funded health research may appear in terms of the effect on choices of programs of study by students in Saskatchewan. As with the employment choices discussed above, it is not clear the extent to which students will be affected in their choices by the extent of research funding but it is probable that the level of research activity is at least one of the factors students consider when they choose which institution to attend and which programs of study to follow within those institutions. While there has been some fluctuation in enrolment numbers over the period, it appears that in 2004-05, there were 6,117 students in the province enrolled in a program related to health research or in which their choice of study may have been influenced by the level of health research in the province. This was an overall increase in the number of such students of 1,221 (or 24.9 per cent) from ten years earlier. It appears that the number of students in Saskatchewan university programs whose choice of enrolments may have been influenced by the level of funding for health-related research may have increased in the past ten years, as the enrolments in relevant course programs have increased both in absolute terms and as a percentage of the total university enrolments within the province. Since these students form the basis for further research efforts, as well as the provision of health care services within the province, the growth in their numbers and relative importance is an important indicator of future capacity in the field. While it may be difficult to identify the extent to which health research funding contributes to the attraction and maintenance of either a health sciences workforce or a student population in health and natural sciences, it is clear from the increases in both of these areas that the potential impact of research funding beyond those who are directly involved in the research has been increasing dramatically within the province. The final source of economic benefit from health sciences research is in savings in health care costs resulting directly from the research results. This may take the form of more effective treatments, shorter periods of recovery from illness, more effective and/or cheaper means of illness prevention and/or reduced health resources in patient care. There has been some limited research done on this question in the past and this is examined for implications for potential savings in health care in Saskatchewan.

4
5
I. Introduction
Health research is primarily conducted to discover and develop better methods for maintaining, restoring or achieving a greater quality of life in the population through improved health. Within this field is research in biomedical science, clinical investigation, health services and systems, and determinants of population health. Biomedical science is designed to develop new treatment technologies, such as pharmaceuticals or medical equipment, to improve the treatment of illness. Clinical investigation and health services and systems research are designed to improve the efficiency and/or effectiveness of treatment. Lastly, determinants of population health research are designed to avoid the need for the treatment of illness. There is an increasing interest in a secondary impact of health research -- its economic and social effects within society. While this is not generally an objective of health research, there has been some suggestion within the literature that research activity within the health field has several direct and indirect effects on the economy and on broad social conditions. It is this secondary effect of health research which is the focus of this study. Building on the literature and data available, the study will focus on four main mechanisms by which socio-economic impacts are generated and attempt to identify the extent to which Saskatchewan has been affected by health research activity1. The first mechanism is the direct and indirect economic effects of health research activity itself. In conducting their research, health researchers employ themselves, research assistants, laboratory technicians, support staff and others. In addition, these activities require the purchase and use of materials and equipment, creating activity in firms that supply such needs. All this amounts to economic activity, jobs, income and business activity within the province. This report will use accepted methodology, employing economic multipliers identified by Statistics Canada, to estimate the level of health research activity within the province and to identify the direct and indirect economic impact of health sciences research conducted within the province. The final report will also provide results from a survey of health science researchers to determine the number of persons directly involved in health science research projects within Saskatchewan. Health research has another indirect effect on the province’s economic and social conditions, through the application of the results of health services and policy research in the prevention of ill health and the better delivery of health care to the sick. This, in turn, has an effect on productivity within the economy. Healthy people live longer, more productive lives and experience reduced rates of absenteeism from work, in addition to the improved quality of life noted above. Again, using accepted methods, this report will identify and estimate the value of improved productivity within the population resulting from health sciences improvements that have stemmed from research activity. 1 The mechanisms described below are discussed in Martin Buxton, Steve Hanney and Teri Jones, “Estimating the Economic Value to Societies of the Impact of Medical Research: a Critical Review”, Bulletin of the World Health Organization, Vol. 82 (10), pp. 733-739.

6
A third benefit of health research comes in the form of economic activity involved in producing products and services previously developed through research. This activity has been referred to as the “commercialization” of research. It results when the outcomes of research are converted into the production of goods and services. This production of health products and services creates jobs and incomes within the economy, either within the production process itself or within the supply chain supporting the production process, again improving the standard of living within the province. Finally, a socio-economic benefit is derived from the application of health care technologies and health improvement and maintenance methods in the health care system, thereby reducing health care costs and/or increasing health care effectiveness. In this case, technology and information identified through research is applied to make health care and overall population wellness more readily or more effectively achieved, reducing the resource requirements of health care and prevention and releasing resources to be applied to improved standards of living.

7
II. Direct and Indirect Economic Impact of Health Research
Introduction As noted above, research uses resources, in the form of labour and materials and capital equipment to produce a product, largely knowledge, which may be further converted into a number of activities. The employment of resources in the research activity is itself an economic activity. In the process of conducting research, researchers, assistants, technicians and support staff earn a living, support their families and maintain themselves as members of the community. Research activity also requires supplies and other inputs, providing support for local businesses that earn their living through the provision of those supplies. This economic impact is separate and distinct from the health value of the results of research and the economic and social value of the products of research, which will be discussed later. The economic impact can be estimated using common techniques if the level of activity can be reasonably estimated and if the interaction between the activity and the rest of the economy can be estimated. The Level of Health Research in Saskatchewan It is difficult to find data on the amount of health research conducted within the province. This is understandable since basic research, by its very nature, is often conducted without advance knowledge of its ultimate applications. It is not clear which research activities may have “health” applications in the final analysis and, therefore, it is not clear of what “health research” is constituted. Further uncertainty may arise in the definition of “research”. Sometimes it is not clear what constitutes a “research activity”. Time spent in a laboratory might be a clear research activity while time spent in a classroom or seminar might be considered something other than research activity, despite the fact it may, through knowledge transfer or sheer inspiration, lead directly to advances in research or research methodology. Similarly, the activities of research scientists might well be considered “research activity”, while the efforts of administrators and support staff, perhaps not directly involved in the research process but without which the research could not proceed, is less clear. Additional uncertainty arises because research is often conducted independently and sometimes under rules of confidentiality, depending on the nature of the research and the source of funding for the research. In this case, there is no centralized registry of research activity to allow for an accounting of the extent that research is conducted within the province in any field, much less to the level of specificity required to identify “health research”. Fortunately, there are estimates of the level of activity within the province, especially from Statistics Canada. In a special study released in May of 2006, Statistics Canada estimated total spending on research and development in the health field in Canada2 The study defined research and development as “creative work undertaken on a systematic 2 Statistics Canada, “Estimates of total spending on research and development in the health field in Canada, 1988 to 2005”, Science Statistics Service Bulletin, vol.30, no.3, Science, Innovation and Electronic Information Division, Statistics Canada, May 2006, pp.1-10 (Catalogue 88-001-XIE).

8
basis in order to increase the stock of scientific and technical knowledge and the use of this knowledge to devise new applications.”3 The definition of health research used in the study is based on various surveys of institutions, with the surveys for the most part having asked for an identification of research and development expenditures on “health” as a socio-economic objective, research and development expenditures in the “health field,” or those which are “health-related,” and include estimates of activity levels by conducting agency and by funding agency. 4 While there is, of necessity, some uncertainty about whether all survey respondents used a broad definition of “health” that would include all four forms of health research identified above, the definitions of health supplied are broad enough that all forms could have been included in the responses. Thus, the data from this study provides the best estimate of total research activity in Saskatchewan in the health field that is available. The national estimates of activity in 2003 are included in Table 1, below. Table 1: Gross Domestic Expenditure on Research and Development in the Health Field by Performing Sector and Funding Sector, Canada, 2003 ($ million) Performing
SectorFunding
SectorFederal Government $ 196 $ 1,029
Provincial Governments $ 44 $ 364
Business Enterprise $ 1,856 $ 1,466
Higher Education $ 3,086 $ 1,300
Private Non-Profit Agency $ 52 $ 391
Foreign $ 0 $ 684
Total $ 5,234 $ 5,234
Source: Statistics Canada, Catalogue No. 88-001-XIE, p. 4. From this table, it can be seen that, in 2003, there was $5.2 billion spent on research and development in the health field across Canada. Most of this research was performed in either the higher education sector or the business enterprise sector, which together accounted for 94.4 per cent of the total research and development performed in the health field. Funding for this research came from all 6 sources listed in the study but was dominated by business enterprise (at 28.0 per cent), higher education (at 24.8 per cent) and the federal government (at 19.7 per cent). These three top funding agencies provided the funding for 72.5 per cent of all the health research conducted in Canada in 2003.
3 Ibid., p. 2. 4 Ibid., p. 2. It should be noted that research and development expenditures by business enterprises were based on survey results in various business enterprise sectors in the North American Industry Classification System. While primarily business enterprises in “scientific” or “technological” sectors, research in the sector “health care and social assistance” sector was also included.

9
Unfortunately, a complete set of parallel data is not available by province within Canada. Some data is available in the study by province, however, and a breakdown of the research and development activity conducted by the Higher Education sector is provided for Saskatchewan in Table 2, below. Table 2: Saskatchewan Higher Education Gross Domestic Expenditure on Research and Development in the Health Field by Sector and Funding Sector, 2003 ($ million) Funding Sector Saskatchewan Canada
Federal Government $ 15.8 $ 813.7
Provincial Governments $ 8.9 $ 305.4
Business Enterprise $ 0.0 $ 267.3
Higher Education $ 33.3 $ 1,299.8Private Non-Profit Agency $ 7.0 $ 369.1
Foreign $ 0.3 $ 30.3
Total $ 65.3 $ 3,085.6
Source: Statistics Canada, Catalogue No. 88-001-XIE, p. 6. In this case, it can be seen that Saskatchewan’s higher education sector spent $65.3 million on research and development in the health field in 2003, or 2.1 per cent of the total research performed by higher education in Canada in that year. The most notable difference in funding arrangements between Saskatchewan and the rest of Canada is that, while private enterprise funded 8.7 per cent of the health research conducted in higher education across Canada, the Saskatchewan higher education sector received no research funding from business enterprise in 2003. This difference was mainly compensated for by the fact that higher education provided 51.0 per cent of the funding for such research in Saskatchewan as compared to only 42.1 per cent of the funding nationally. Similar data on the research effort is not available for the other performing sectors on a province by province basis. In a separate exercise, however, Statistics Canada identified the research and development spending on health research performed by the business enterprise sector in Saskatchewan at $9 million in 2003.5 When combined with the research activity conducted by the higher education sector in Saskatchewan as outlined in Table 2 above, this would bring the total spending on health research performed by higher education and business enterprise in Saskatchewan to $74.3 million in 2003. This amount represents 1.5 per cent of the value of health research performed by these two key sectors in Canada as identified in Table 1, above.
5 E-mail correspondence from Louise Earl, Chief, Science and Technology, Science, Innovation and Electronic Information Division, Statistics Canada, August 23, 2006.

10
It should be noted that, from Table 1, above, these two sectors accounted for 94.4 per cent of the health research performed in Canada in 2003. If they account for a similar preponderance of the research conducted within Saskatchewan, it is reasonable to estimate the total research effort within the province in 2003 to be ($74.3 million/ 94.4 per cent =) $79.7 million. This provides a reasonable estimate of the level of research activity in the health field within Saskatchewan, at least in terms of the total cost of research conducted. This is an important first step in assessing the economic impact of the research activity on the Saskatchewan economy. Assessing the Gross Economic Impact All economic activity has been categorized through a system of definitions known as the “North American Industry Classification System” (NAICS). This allows a consistent set of definitions to be applied for analytical purposes, especially in undertaking input/output analysis, as will be seen below. The system divides the economy into industries or sectors using a three-digit code for a sector, a four-digit code for a sub-sector and up to six digits to codify a specific activity. For example, Code 541 is “Professional, Scientific and Technical Services.” Included in this is Code 5417 – “Scientific Research and Development Services,” which includes research and development in the “physical, engineering and life sciences” (Code 54171) and research and development in the “social sciences and humanities” (Code 54172.6 This classification would seem to be the most appropriate one within the NAICS system for health research. Statistics Canada also publishes economic multipliers based on input/output data for the provincial economies. For Saskatchewan, the latest available is for the 2002 calendar year. These identify, among other things, the extent to which activity in any particular sector translates into gross output, Gross Domestic Product and employment, through a series of multipliers that can be applied to activity levels. These multipliers are also provided on the basis of NAICS codes, with breakdowns provided to as fine a level as can be allowed, subject to confidentiality requirements of the Statistics Act. In the case of Saskatchewan and the research and development activity discussed above, the finest published NAICS code is Code 541: “Professional, Scientific and Technical Services” which includes the health research activity discussed above along with a wide variety of other services7. Nevertheless, this classification is the closest to the pure research function described above for purposes of assessing economic impact. The multipliers for this industry are shown in Table 3 below.
6 Statistics Canada, North American Industry Classification System, Ottawa, 2003, catalogue No. 12-501-XPE, pp. 443-4. 7 Statistics Canada, 2002 Provincial Input/Output Multipliers, Saskatchewan, Medium Industry Aggregation, December 21, 2005, Catalogue No.: 15F0046XDB.
11
Table 3: Input/Output Multipliers for Professional, Scientific and Technical Services for Saskatchewan, 2002
Direct ImpactDirect and
Indirect ImpactGross Domestic Product (Intensity Ratio) 0.63 0.77
Output (intensity ratio) 1.00 1.25
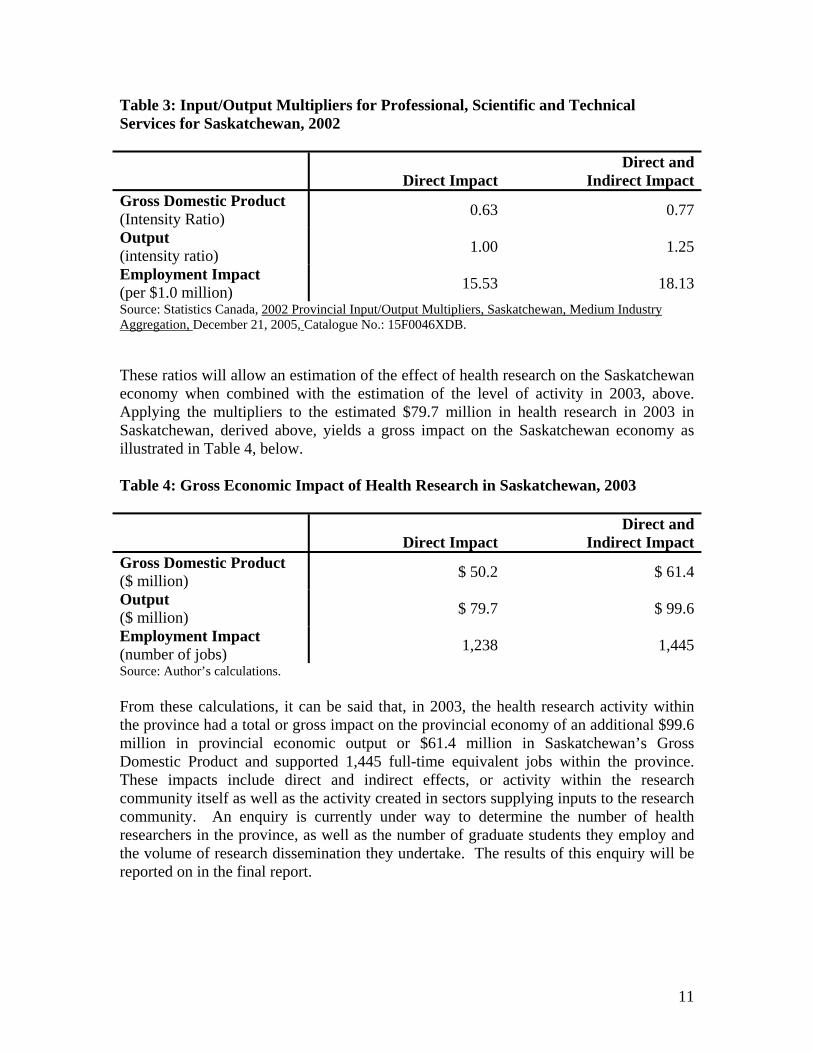
Employment Impact (per $1.0 million) 15.53 18.13Source: Statistics Canada, 2002 Provincial Input/Output Multipliers, Saskatchewan, Medium Industry Aggregation, December 21, 2005, Catalogue No.: 15F0046XDB. These ratios will allow an estimation of the effect of health research on the Saskatchewan economy when combined with the estimation of the level of activity in 2003, above. Applying the multipliers to the estimated $79.7 million in health research in 2003 in Saskatchewan, derived above, yields a gross impact on the Saskatchewan economy as illustrated in Table 4, below. Table 4: Gross Economic Impact of Health Research in Saskatchewan, 2003
Direct ImpactDirect and
Indirect ImpactGross Domestic Product ($ million) $ 50.2 $ 61.4
Output ($ million) $ 79.7 $ 99.6
Employment Impact (number of jobs) 1,238 1,445Source: Author’s calculations. From these calculations, it can be said that, in 2003, the health research activity within the province had a total or gross impact on the provincial economy of an additional $99.6 million in provincial economic output or $61.4 million in Saskatchewan’s Gross Domestic Product and supported 1,445 full-time equivalent jobs within the province. These impacts include direct and indirect effects, or activity within the research community itself as well as the activity created in sectors supplying inputs to the research community. An enquiry is currently under way to determine the number of health researchers in the province, as well as the number of graduate students they employ and the volume of research dissemination they undertake. The results of this enquiry will be reported on in the final report.

12
Assessing the Net Economic Impact It should be noted, however, that the research activity discussed above includes a substantial amount of activity funded internally within the Saskatchewan economy, either by the provincial government or the educational institutions within the province. It would be appropriate, therefore, to recognize that this funding for research does not represent “new” injections to the economy since they are funded within the province and, presumably, would be used for some other purpose were they not directed towards health research. To calculate the level of impact of “net injections” to the provincial economy, one could adjust by either deducting from the calculations above the expected economic impacts of an alternate use of the research funding or by deducting from the total funding inputs those that are generated within the province itself and could be otherwise employed within the economy. The first approach would require an assumption about alternate uses for internally generated funds. One reasonable assumption would be to assume that, if they were not used for health research, they would be directed towards an alternate research objective. Since the multipliers identified in Table 3 (above) would also apply to that calculation, the result of this approach would be mathematically equivalent to the second approach. As such, a reasonable approach to determining the net economic benefit of the research activity would be to deduct from the calculations an amount representing the funding generated internally to the province’s economy, leaving a funding base of “new injections to the economy” or funds entering the province from outside for research purposes. From Table 2, above, it can be seen that, of the $65.3 million in health research estimated by Statistics Canada to have been conducted by “Higher Education” in Saskatchewan in 2003, $42.2 million (or 64.6 per cent) was funded either by the higher education sector itself or by the provincial government. Deducting this “internal funding” would leave 35.4 per cent or $23.1 million of the research funding as “external injections”. This approach ignores the fact that some of the health research in Saskatchewan is conducted by and funded by private enterprise, non-profit organizations and the federal government. The calculations above indicated these additional research efforts would add to the $65.3 million to an estimated total activity level of $79.7 million within the province. There are no estimates of the sources of funding for research conducted outside of the higher education sector in Saskatchewan, but Table 1 provides a national breakdown of funding sources for all health research in Canada in 2003. From Table 1, it can be seen that 40.2 per cent of health research in Canada in 2003 was funded by the federal government, private enterprise, non-profit organizations or foreign sources. This could provide a proxy for “external funding” of health research in Saskatchewan and yield an estimated value of externally funded health research of (40.2% X $79.7 million =) $32.0 million in 2003 in Saskatchewan. Employing the multipliers in Table 3 above to these values provides an estimated net economic impact as illustrated in Table 5, below.
13
Table 5: Net Economic Impact of Health Research in Saskatchewan, 2003
Direct ImpactDirect and
Indirect ImpactGross Domestic Product ($ million) $ 20.2 $ 24.6
Output ($ million) $ 32.0 $ 40.0
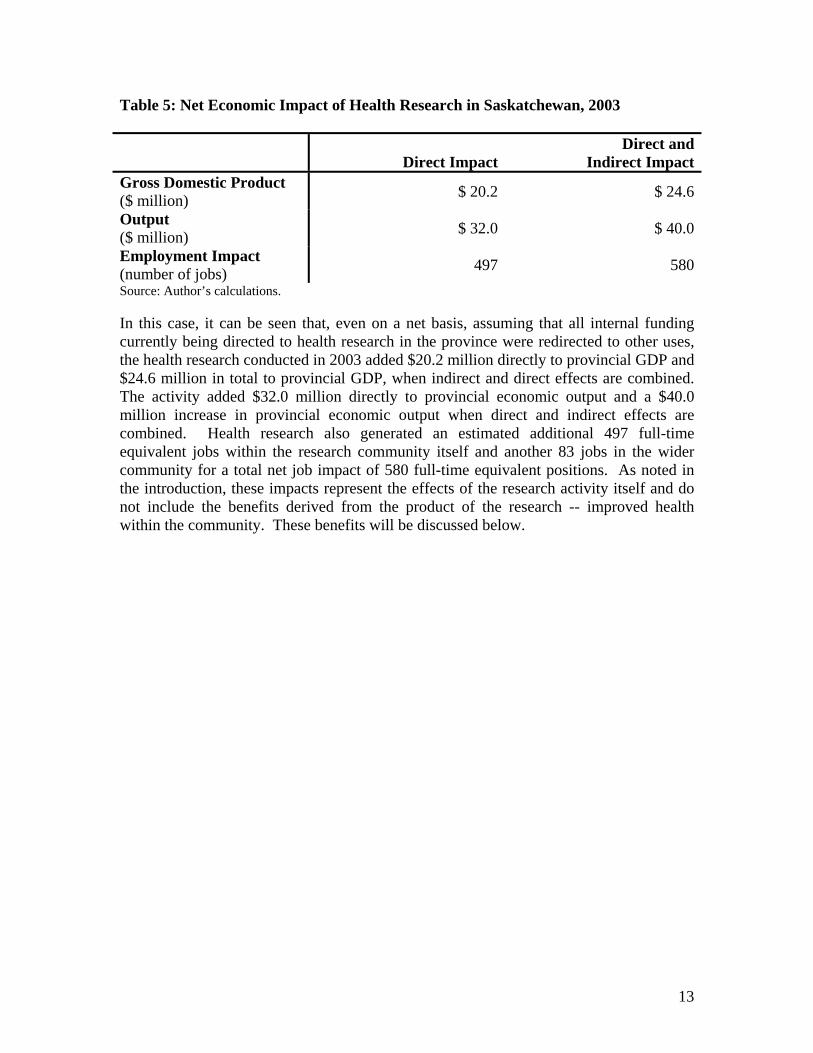
Employment Impact (number of jobs) 497 580Source: Author’s calculations. In this case, it can be seen that, even on a net basis, assuming that all internal funding currently being directed to health research in the province were redirected to other uses, the health research conducted in 2003 added $20.2 million directly to provincial GDP and $24.6 million in total to provincial GDP, when indirect and direct effects are combined. The activity added $32.0 million directly to provincial economic output and a $40.0 million increase in provincial economic output when direct and indirect effects are combined. Health research also generated an estimated additional 497 full-time equivalent jobs within the research community itself and another 83 jobs in the wider community for a total net job impact of 580 full-time equivalent positions. As noted in the introduction, these impacts represent the effects of the research activity itself and do not include the benefits derived from the product of the research -- improved health within the community. These benefits will be discussed below.

14

15
III. Productivity Benefits of Health Research
Introduction A healthy population results in individuals that live longer and suffer from illness less often or less severely during their lifetime. This means individuals are more able to engage in productive activity at any point in their life and that their longer lifespan will allow for more opportunities for productive activity over a longer period. Rate of Return Approach Some early work by S. Mushkin8 focussed on identifying the value of increased productivity within society that could be attributed to health research and its application to improved health within the population. This approach estimated the reduction in morbidity and premature mortality that had occurred in the United States of America between 1930 and 1975 and estimated the share of that improvement that could be attributed to bio-medical research. By determining the total productivity gained through reduced absenteeism and longer life spans, Mushkin deducted the cost of that bio-medical research and calculated a rate of return on medical research of 47 per cent. In other words, according to Mushkin, every dollar of medical research resulted in productivity increases in society which returned the value of the research and an additional return of 47 per cent per year. For example, if a medical research project has a total cost of $10 million and yields an improvement in health which takes 20 years to become obsolete, the $10 million expense would result in society-wide average annual productivity gains to recover the $10 million over 20 years ($10million/20 years) plus an additional productivity gain of 4.7 million per year ($10 million X 47%) or a total productivity gain of:
($10 million/20) + ($10 million X .47) = $5.2 million per year. Assuming an equivalent productivity gain for all health research, the Mushkin analysis would suggest the $79.7 million in health research in Saskatchewan in 2003 would have an ultimate impact on annual productivity between $41 million and $44 million, depending on the expected time to obsolescence of the results of the research. One limitation to this approach, sometimes called the human capital approach, is in the fact that it assumes that additional resources in the form of greater available work time would be employed in productive effort within the economy. In other words, this approach assumes that there is not a problem of unemployment within the economy. There are, however, other, more severe limitations to the extent to which this approach 8 S. Mushkin, Biomedical Research: Costs and Benefits, Cambridge (MA); Ballinger Publishing Company: 1979 as reported in Martin Buxton, Steve Hanney and Teri Jones, op.cit., p.736.

16
can be practically employed to evaluate health research in Saskatchewan. These limitations will be discussed below after examining some other approaches that have been employed elsewhere. Valuation of Life Approach Another approach that has been employed involves attempts to estimate the intrinsic value of a human life based on individuals’ efforts to preserve their own lives. In this case, the self-evaluation of a human life is used as the basis for establishing the worth of health research. By estimating the degree to which health research has contributed to extended lives and multiplying that time extension by the value that individuals place on their own lives, the social value of health research can be estimated. For example, David M. Cutler and Grant Miller estimated the value of one additional year of a human life at between $37,000 and $100,000 in the United States in 20039. Using this as the basis for their calculation, they were able to determine that the rate of return on clean water technology in United States cities was a ratio of 23 to 1, implying that every dollar spent on water quality returned $23 to the population in increased life expectancy. While the focus of their work was on water quality infrastructure, as opposed to health research, the identification of a valuation to human life extension is a step forward in determining the benefits of health research. W. Nordhaus estimated the self-evaluation of human life by using the value of efforts undertaken by individuals to avoid death by common causes and the probability of death from those causes to establish an estimated value of a “prevention of fatality” at around $3.0 million in the United States.10 A similar approach by Kip Viscusi suggested that, based on their spending on brake systems and air bags in automobiles, an average adult in the United States would pay between $300 and $700 to reduce their likelihood of dying in a car crash by 1 in 1,000, leading to an estimate of the self-valuation of an entire life at $3 million to $7 million and a valuation of one additional year of healthy life of $100,00011. This same approach of estimating individual’s willingness to pay to avoid fatality was also employed by Murphy and Topel to go one step further in estimating the value of health research to society through the value of increased health and longevity caused by research12. In this research, Murphy and Topel estimate the total value of longevity gains from 1970 to 2000 to be worth $3.2 trillion per year to the entire United States of
9 David Cutler and Grant Miller, “The Role of Public Health Improvements in Health Advances: The 20th Century united States”, National Bureau of Economic Research, Working Paper number 10511, May, 2004, p. 22. 10 W. Nordhaus, “The Health of Nations: The Contribution of Improved Health to Living Standards” in K. Murphy and R. Topel (eds.), Measuring the Gains from Medical Research: an Economic Approach, Chicago: the University of Chicago Press, 2003, pp. 9-40. 11 W.K. Visccsi, Fatal Tradeoffs, Oxford University Press, 1992 as cited in Samuel Silverstein, “What does economic research tell us about the benefits of investments in medical health research and training?”, p.13. 12 Kevin M. Murphy and Robert H. Topel, “The Value of Health and Longevity”, National Bureau of Economic Research, Working Paper number 11405, June 2005.

17
America and the longevity gains over the entire 20th century to be worth a cumulative value of $1.3 million per person in the United States. Their estimates are that a one per cent reduction in mortality rates from disease would be worth an estimated $500 billion to the current and future population of the United States. An equivalent value to the Saskatchewan economy would be approximately $1.3 billion. Lichtenberg13 used the same approach to the self-evaluation of human life and then, by estimating the success of pharmaceutical research in developing successful treatment options and their average impact on longevity, was able to ascribe to the total of pharmaceutical research in the United States an average rate of return of around 67 per cent. In other words, a dollar spent on pharmaceutical research returned the cost of the research over its obsolescence period plus an additional $0.67 per year in social benefits throughout the period to obsolescence. Limitations to the Approach Whether the human capital approach of Mushkin or the self-evaluating, “willingness-to-pay” approach of others is employed, these studies suffer a major limitation in their application to Saskatchewan policy evaluation. The limitation stems mainly from the fact that they were conducted using United States data to evaluate research within the Untied States. The U.S. economy is, by far, the largest in the world in both absolute and relative terms. It is more likely than any other economy in the world to benefit from increased longevity, and increased productivity, by virtue of having the highest production to begin with. It is also more likely to derive greater benefits from any given increase in longevity, by virtue of the fact that the average value of life is higher to begin with. One study in the United States determined that the elasticity of the value of human life with respect to GDP per capita was between 1.5 and 1.714, implying that, as GDP increases by one percentage point, the value of human life within that economy increases at a faster rate of 1.5 percentage points to 1.7 percentage points. A large economy with a very high level of GNP per capita is more likely to derive absolute benefit and proportionately more benefits from productivity increases stemming from health research. The United States also has a very large health research community, increasing the likelihood that health research undertaken will be of greater benefit to the United States population, partly because research will focus on issues of greatest interest to the United States population and partly because their results are most likely to affect health in the United States first. Most of these studies draw a direct link between the whole of health research in the U.S. and the whole of productivity or longevity gains in the U.S. Since the United States dominates in both the share of health research and the share of
13 F. Lichtenberg, “Pharmaceutical Innovation, Mortality Reduction and Economic Growth”, in K. Murphy and R. Topel (eds.), Measuring the Gains from Medical Research: an Economic Approach, Chicago, University of Chicago Press, 2003, pp. 74–109. 14 Dora L. Costa and Matthew E. Kahn, “Changes in the Value of Life: 1940-1980”, National Bureau of Economic Research, Working Papers, Number 9396, 2002.

18
industrial production, it is much more likely that there would be a direct mathematical link between the world’s health research and increases in Unites States production. In much smaller economies, the link will be much more tenuous. If there are increases in longevity or productivity in Saskatchewan, for example, they are much more likely to have resulted from research outside the province than inside the province, simply because most health research happens outside Saskatchewan. There will be a mild relationship between Saskatchewan research and Saskatchewan productivity, even if there is a strong relationship between worldwide research and Saskatchewan productivity. Conversely, health research in Saskatchewan may lead to improvements in life expectancies and in reduced absenteeism of increased productivity, but such improvements are likely to be spread throughout the world, or at least throughout the industrialized world. Since Saskatchewan’s economy is only a very small part of the world-wide economic activity likely to be affected through any health advancement, only a very small proportion of the total benefits of Saskatchewan research would be derived within the province. Again, this suggests a weak mathematical relationship between Saskatchewan research and Saskatchewan productivity, even if there is a strong relationship between research in Saskatchewan and productivity worldwide. These two weak relationships between research in Saskatchewan and productivity in Saskatchewan would suggest very little likelihood of as strong a mathematical relationship between domestic research and domestic productivity in Saskatchewan as was found by researchers in the United States. Thus, productivity and longevity gains within Saskatchewan are minutely likely to have been derived from Saskatchewan research (as opposed to research elsewhere) and that Saskatchewan research is only minutely likely to improve productivity and/or longevity in Saskatchewan (even though it may have a large impact world-wide). While it may be possible to suggest that health research in Saskatchewan has an expected social rate of return of 67 per cent (using the Lichtenberg estimations, above), the social rate of return to Saskatchewan from Saskatchewan-based research is likely to be a very tiny fraction of that rate, since most benefits are likely to be derived by populations outside the province.

19
IV. Commercial Benefits of Health Research
Introduction As has been noted, the primary objective of health research is to discover and develop better methods for maintaining, restoring or achieving a greater quality of life in the population through improved health. In the biomedical science field, once these discoveries are made, they often require a production process to make their widespread application available. New drugs need pharmaceutical manufacturing facilities. Similarly, new medical diagnostic and treatment equipment needs manufacturing facilities to make them widely available throughout the world. The development of new production processes to produce goods and services resulting from biomedical research is often referred to as “commercialization”. Another benefit often ascribed to biomedical science research is the subsequent development of manufacturing and other facilities for the production of the new technologies resulting from research. This is distinct from the facilities required to produce the inputs to biomedical research which were included in the estimates of the indirect economic effects of health research in an earlier chapter. Estimates of the Impact of Commercialization L. Rosenberg examined the pharmaceutical industry in the United States and estimated that there were 500,000 jobs in the United States that existed within the biopharmaceutical industry that could attribute their existence directly to previous publicly-funded biomedical research15. Similar results have been reported by other publications, including a report on the United Kingdom which noted that “publicly funded research makes a health contribution to the maintenance of a healthy industrial sector”.16 In this particular report, several studies conducted in the United States were offered as support for the link between biomedical science research and subsequent commercial development. In another study in the United States, E. Mansfield surveyed large corporations in seven major industries to identify the proportion of their firms’ new products and processes that could not have been developed or would have been substantially delayed in the absence of academic research. Mansfield estimated that the worldwide social rate of return on such academic research, through commercialization impacts alone, was 28 per cent on research conducted between 1975 and 1978, with particular benefits accruing to the pharmaceutical industry.17
15 L. Rosenberg, “Exceptional economic returns on investments in medical research”, Medical Journal of Australia, vol. 177, 2002, pp. 368-71. 16 UK Evaluation Forum, Medical Research Council, Medical Research: Assessing the Benefits to Society, The Academy of Medical Sciences, Medical research Council and Wellcome Trust, May, 2006, p. 25. 17 E. Mansfield, “Academic Research and Industrial Innovation”, Research Policy, vol. 20, 1991, pp.1-12.
20
Commercialization in Saskatchewan As was the case with the evaluation of longevity improvements and increased productivity in the previous chapter, it is also difficult to draw direct linkages between Saskatchewan research and Saskatchewan commercial activities. With a very small commercial production sector at home, Saskatchewan research which does lead to commercial activity is very likely to do so somewhere outside of Saskatchewan. Conversely, it is very likely that any commercial activity developed within Saskatchewan and based on previous biomedical research will be based on research conducted elsewhere. There is very little public data available on commercial production of medical technology or medical treatments in Saskatchewan. There are NAICS Codes for Pharmaceutical and Medicine Manufacturing (Code: 3254) and for Medical Equipment and Supplies Manufacturing (Code: 3391)18 but any data on production from these sectors has been suppressed for confidentiality reasons. Such suppression occurs when sample sizes are so small as to be unreliable or when only a small number of producers are present, leading to the probability that confidential data could be released or derived if the data are published. The Saskatchewan Department of Industry and Resources maintains a database of Saskatchewan manufacturers that is accessible on-line and can be sorted according to the NAICS Codes (See Appendix A). A recent search of this database identified three firms categorized in NAICS Code: 3254, Pharmaceutical and Medicine Manufacturing, including a producer of “nutraceuticals”, a producer of nutraceuticals and bee pollen products and a producer of pharmaceutical products. The guide also lists 17 companies involved in NAICS Code 3391, Medical Equipment and Supplies Manufacturing, including 9 dental laboratories, two optical laboratories, three producers of therapeutic heating and cooling packs, a producer of massage tables, a producer of hospital garments and a producer of Hospital and restaurant equipment19. There is no clear link between any of these producers and biomedical research conducted in Saskatchewan in the past, although the one producer of pharmaceutical products is probably producing products that were once the subject of biomedical research. Another organization, AgWest Bio Inc., also maintains a directory of Saskatchewan companies and organizations involved or interested in “health and wellness” (See Appendix B). The directory identifies 53 such contacts in Saskatchewan, of which 10 are either government organizations or educational institutions. Another 7 represent industry organizations and another 6 represent research facilities within the province. The remaining 30 listings in the directory are predominately in the nutraceuticals and functional foods business and the agricultural service sector. The directory for groups interested in “medical and pharmaceutical” matters lists 23 entries, only three of which are in production of pharmaceutical products for human or animal use. The rest represent
18 Statistics Canada, North American Industry Classification System, op. cit., p.198-199 and pp. 273-274. 19 http://www.ir.gov.sk.ca/Default.aspx?DN=2968,2965,2936,Documents accessed on August 28, 2006.

21
government agencies, educational institutions or research institutions or facilities. 20 There are no data available on the output or sales activity of these companies or the pharmaceutical or nutraceutical and functional foods industries as a whole. Input/Output Multipliers While data are not available on the value of commercialized activity following biomedical sciences research, the provincial input/output tables developed by Statistics Canada do provide multipliers at the medium level for NAICS categories for pharmaceutical manufacturing and medical equipment manufacturing, the two industries most likely to spring from biomedical research. The multipliers for NAICS Code: 32541 (Pharmaceutical and Medicine Manufacturing21) are presented in Table 6, below. Table 6: Input/Output Multipliers for Pharmaceutical and Medicine Manufacturing for Saskatchewan, 2002
Direct ImpactDirect and
Indirect ImpactGross Domestic Product (Intensity Ratio) Na 0.09
Output (intensity ratio) Na 1.30
Employment Impact (per $1.0 million) Na 13.96Source: Statistics Canada, 2002 Provincial Input/Output Multipliers, Saskatchewan, Medium Industry Aggregation, December 21, 2005, Catalogue No.: 15F0046XDB. These data would suggest that any pharmaceutical manufacturing that does occur in Saskatchewan at, say, $1 million in total annual production, would add $1.3 million to total provincial output, $90,000 to Saskatchewan GDP and 13.96 jobs (full-time equivalent) in total, including all direct and indirect effects. It is important to note that this activity would have to be self-sustaining and free of any internal transfer (subsidy) support to have the calculated effects on the economy overall. The data isolating the direct effects are not available at this level of industry aggregation because, as noted above, the current industry in Saskatchewan is too small and/or concentrated to allow publication of data without jeopardizing confidentiality of reporting or the sample size in the survey is too small to ascertain statistically significant multipliers. The multipliers for NAICS Code: 3391 (Medical Equipment and Supplies Manufacturing22) are presented in Table 7, below.
20 http://www.agwest.sk.ca/directory/health.htm accessed on August 28, 2006. 21 Statistics Canada, 2002, op.cit., p. 199. 22 Statistics Canada, 2002, op.cit., pp. 273-274.

22
Table 7: Input/Output Multipliers for Medical Equipment and Supplies Manufacturing for Saskatchewan, 2002
Direct ImpactDirect and
Indirect ImpactGross Domestic Product (Intensity Ratio) Na 0.65
Output (intensity ratio) Na 1.21
Employment Impact (per $1.0 million) Na 12.29Source: Statistics Canada, 2002 Provincial Input/Output Multipliers, Saskatchewan, Medium Industry Aggregation, December 21, 2005, Catalogue No.: 15F0046XDB. These data would suggest that any self-sustaining medical equipment and supplies manufacturing that does occur in Saskatchewan at, say, $1 million in total annual production, would add $1,210,000 to total provincial output, $650,000 to Saskatchewan GDP and 12.29 jobs (full-time equivalent) in total, including all direct and indirect effects. As with the previous example, the data isolating the direct effects are not available at this level of industry aggregation because, as noted above, the current industry in Saskatchewan is too small and/or concentrated to allow publication of data without jeopardizing confidentiality of reporting or the sample size in the survey is too small to ascertain statistically significant multipliers. In both these cases, these data can also be used on for evaluation of specific research projects by applying them to the product of the potential total value of commercialization to follow a research project times the probability that commercialization will be achieved and will be located in Saskatchewan. Thus, for any given research project, one could determine the expected impact on the provincial economy through commercialization as: Ii = Pc x Ps x Mi x COe Where:
Ii is the expected impact on economic indicator i (GDP, Total Output or employment);
Pc is the probability that commercialization of a pharmaceutical or medical equipment product will result from the research activity being undertaken; Ps is the probability that commercialization will occur in Saskatchewan; Mi is the multiplier for the industry under consideration and the economic indicator i (GDP, Total Output, or employment) of interest; and, COe is the expected output from a self-sustaining commercial enterprise producing either pharmaceuticals or medical equipment.

23
If, for example, a research project has a 50 per cent probability of yielding commercial production of pharmaceuticals and a 20 per cent probability that commercialization would occur in Saskatchewan and an expected annual output of $10 million from production, the expected impact on Saskatchewan GDP would be: IGDP = .50 x .20 x $10 million x .09 = $90,000 per year. By calculating the expected value of economic impacts for all such research proposals, comparisons between proposals could be made on the basis of their expected commercial value to the economy, as well as their expected value to medical science and good health.

24

25
V. Other External Benefits of Health Research
Introduction Aside from the benefits estimated so far, it is possible that research efforts in the health field generate additional external benefits in a number of forms. An earlier chapter provided an estimate of the direct and indirect employment impact of spending on health research, but it may also be possible that the process of conducting health research attracts other people to work in Saskatchewan in health and health sciences who would not otherwise choose to come here. In addition to the attraction of health and science workers, it may also be possible that health research attracts and retains a student population in the province which would otherwise choose to study elsewhere. These two pools of resources, people who work in health and related science occupations and those who study in related areas, provide the basis for continuing health care advancements in the province, including potential further research into health and health care. Related Employment Statistics Canada provides estimates of total employment by occupational category collected from the monthly Labour Force Survey. While the categories are very broad in nature, two which are of particular interest are “Health Occupations” and “Natural and Applied Sciences and Related Occupations”. Estimates of Employment Levels for these two occupations for Saskatchewan are provided in Table 8, below. Table 8: Saskatchewan Employment in Fields related to Health Research, 1996 to 2006
Calendar Year Health Occupations Natural and Applied Science Occupations
Combined Employment
(Employment in Thousands) 1996 26.2 15.0 41.2 1997 27.0 18.1 45.1 1998 26.2 17.3 43.5 1999 26.3 17.9 44.2 2000 27.7 16.9 44.6 2001 28.8 18.8 47.6 2002 29.6 17.7 47.3 2003 30.9 18.3 49.2 2004 31.8 19.3 51.1 2005 32.5 20.9 53.4 2006 33.5 21.9 55.4 Source: Statistics Canada, Labour Force Survey Estimates by National Occupational Classification for Statistics (CANSIM Table 282-0010) at http:/estat.statcan.ca/cgi-win/cnsmcgi.exe accessed on October 2, 2007.
26
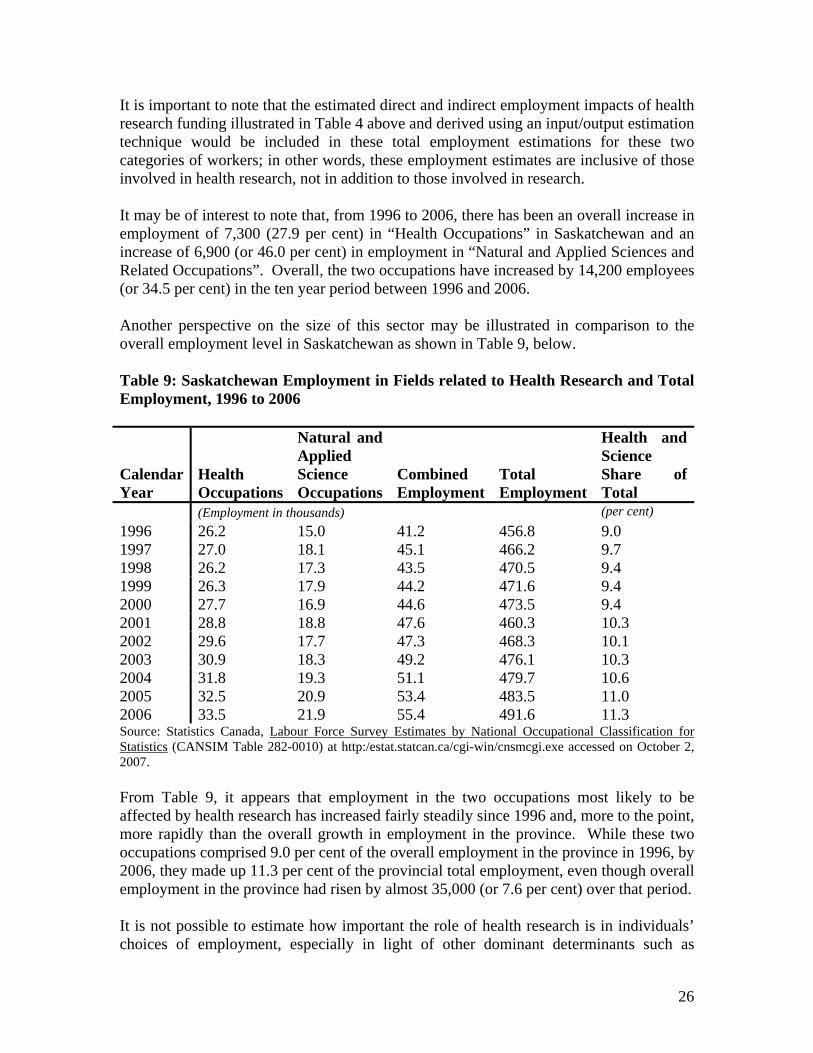
It is important to note that the estimated direct and indirect employment impacts of health research funding illustrated in Table 4 above and derived using an input/output estimation technique would be included in these total employment estimations for these two categories of workers; in other words, these employment estimates are inclusive of those involved in health research, not in addition to those involved in research. It may be of interest to note that, from 1996 to 2006, there has been an overall increase in employment of 7,300 (27.9 per cent) in “Health Occupations” in Saskatchewan and an increase of 6,900 (or 46.0 per cent) in employment in “Natural and Applied Sciences and Related Occupations”. Overall, the two occupations have increased by 14,200 employees (or 34.5 per cent) in the ten year period between 1996 and 2006. Another perspective on the size of this sector may be illustrated in comparison to the overall employment level in Saskatchewan as shown in Table 9, below. Table 9: Saskatchewan Employment in Fields related to Health Research and Total Employment, 1996 to 2006
Calendar Year
Health Occupations
Natural and Applied Science Occupations
Combined Employment
Total Employment
Health and Science Share of Total
(Employment in thousands) (per cent) 1996 26.2 15.0 41.2 456.8 9.0 1997 27.0 18.1 45.1 466.2 9.7 1998 26.2 17.3 43.5 470.5 9.4 1999 26.3 17.9 44.2 471.6 9.4 2000 27.7 16.9 44.6 473.5 9.4 2001 28.8 18.8 47.6 460.3 10.3 2002 29.6 17.7 47.3 468.3 10.1 2003 30.9 18.3 49.2 476.1 10.3 2004 31.8 19.3 51.1 479.7 10.6 2005 32.5 20.9 53.4 483.5 11.0 2006 33.5 21.9 55.4 491.6 11.3 Source: Statistics Canada, Labour Force Survey Estimates by National Occupational Classification for Statistics (CANSIM Table 282-0010) at http:/estat.statcan.ca/cgi-win/cnsmcgi.exe accessed on October 2, 2007. From Table 9, it appears that employment in the two occupations most likely to be affected by health research has increased fairly steadily since 1996 and, more to the point, more rapidly than the overall growth in employment in the province. While these two occupations comprised 9.0 per cent of the overall employment in the province in 1996, by 2006, they made up 11.3 per cent of the provincial total employment, even though overall employment in the province had risen by almost 35,000 (or 7.6 per cent) over that period. It is not possible to estimate how important the role of health research is in individuals’ choices of employment, especially in light of other dominant determinants such as
27
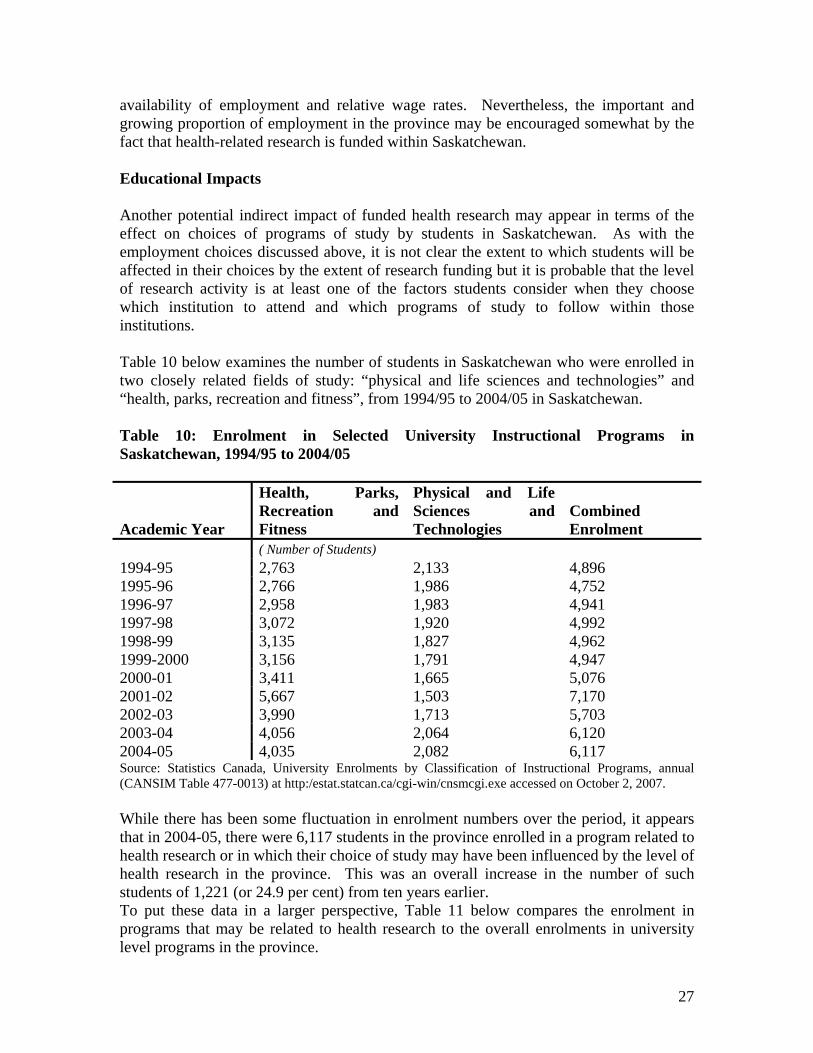
availability of employment and relative wage rates. Nevertheless, the important and growing proportion of employment in the province may be encouraged somewhat by the fact that health-related research is funded within Saskatchewan. Educational Impacts Another potential indirect impact of funded health research may appear in terms of the effect on choices of programs of study by students in Saskatchewan. As with the employment choices discussed above, it is not clear the extent to which students will be affected in their choices by the extent of research funding but it is probable that the level of research activity is at least one of the factors students consider when they choose which institution to attend and which programs of study to follow within those institutions. Table 10 below examines the number of students in Saskatchewan who were enrolled in two closely related fields of study: “physical and life sciences and technologies” and “health, parks, recreation and fitness”, from 1994/95 to 2004/05 in Saskatchewan. Table 10: Enrolment in Selected University Instructional Programs in Saskatchewan, 1994/95 to 2004/05
Academic Year
Health, Parks, Recreation and Fitness
Physical and Life Sciences and Technologies
Combined Enrolment
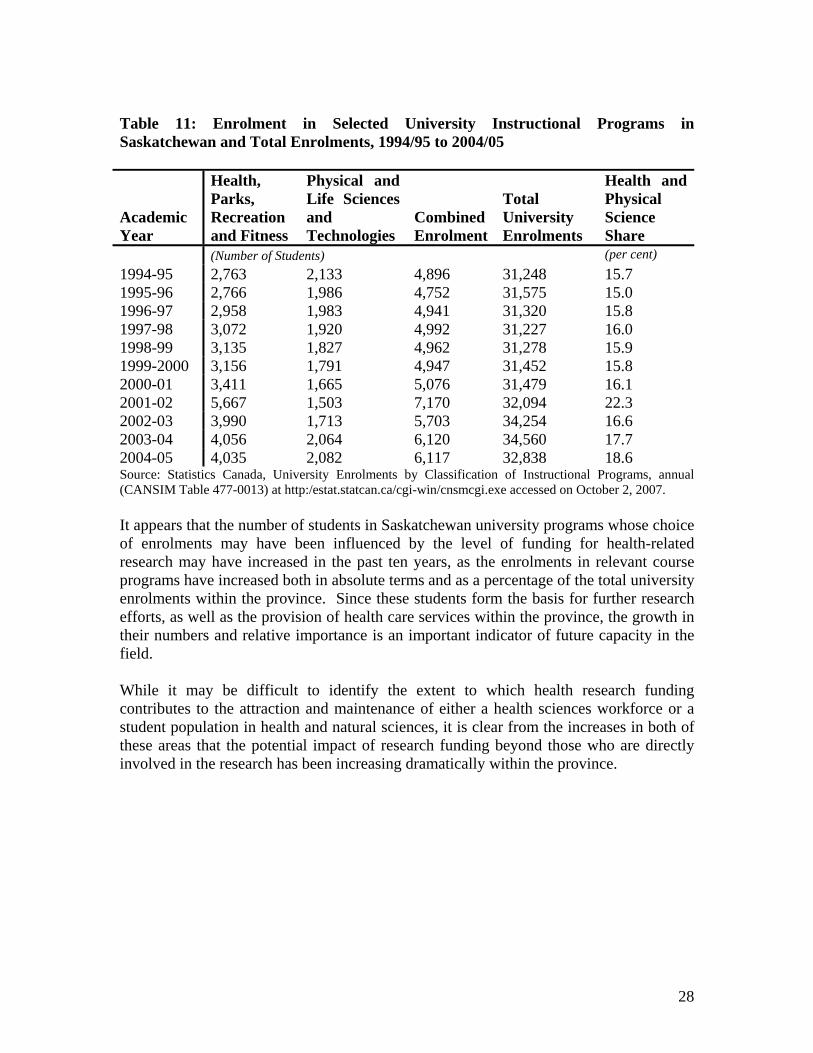
( Number of Students) 1994-95 2,763 2,133 4,896 1995-96 2,766 1,986 4,752 1996-97 2,958 1,983 4,941 1997-98 3,072 1,920 4,992 1998-99 3,135 1,827 4,962 1999-2000 3,156 1,791 4,947 2000-01 3,411 1,665 5,076 2001-02 5,667 1,503 7,170 2002-03 3,990 1,713 5,703 2003-04 4,056 2,064 6,120 2004-05 4,035 2,082 6,117 Source: Statistics Canada, University Enrolments by Classification of Instructional Programs, annual (CANSIM Table 477-0013) at http:/estat.statcan.ca/cgi-win/cnsmcgi.exe accessed on October 2, 2007. While there has been some fluctuation in enrolment numbers over the period, it appears that in 2004-05, there were 6,117 students in the province enrolled in a program related to health research or in which their choice of study may have been influenced by the level of health research in the province. This was an overall increase in the number of such students of 1,221 (or 24.9 per cent) from ten years earlier. To put these data in a larger perspective, Table 11 below compares the enrolment in programs that may be related to health research to the overall enrolments in university level programs in the province.
28
Table 11: Enrolment in Selected University Instructional Programs in Saskatchewan and Total Enrolments, 1994/95 to 2004/05
Academic Year
Health, Parks, Recreation and Fitness
Physical and Life Sciences and Technologies
Combined Enrolment
Total University Enrolments
Health and Physical Science Share
(Number of Students) (per cent) 1994-95 2,763 2,133 4,896 31,248 15.7 1995-96 2,766 1,986 4,752 31,575 15.0 1996-97 2,958 1,983 4,941 31,320 15.8 1997-98 3,072 1,920 4,992 31,227 16.0 1998-99 3,135 1,827 4,962 31,278 15.9 1999-2000 3,156 1,791 4,947 31,452 15.8 2000-01 3,411 1,665 5,076 31,479 16.1 2001-02 5,667 1,503 7,170 32,094 22.3 2002-03 3,990 1,713 5,703 34,254 16.6 2003-04 4,056 2,064 6,120 34,560 17.7 2004-05 4,035 2,082 6,117 32,838 18.6 Source: Statistics Canada, University Enrolments by Classification of Instructional Programs, annual (CANSIM Table 477-0013) at http:/estat.statcan.ca/cgi-win/cnsmcgi.exe accessed on October 2, 2007. It appears that the number of students in Saskatchewan university programs whose choice of enrolments may have been influenced by the level of funding for health-related research may have increased in the past ten years, as the enrolments in relevant course programs have increased both in absolute terms and as a percentage of the total university enrolments within the province. Since these students form the basis for further research efforts, as well as the provision of health care services within the province, the growth in their numbers and relative importance is an important indicator of future capacity in the field. While it may be difficult to identify the extent to which health research funding contributes to the attraction and maintenance of either a health sciences workforce or a student population in health and natural sciences, it is clear from the increases in both of these areas that the potential impact of research funding beyond those who are directly involved in the research has been increasing dramatically within the province.

29
VI. Potential Savings to the Health Care System
Introduction The final source of economic benefit from health sciences research is in savings in health care costs resulting directly from the research results. This may take the form of more effective treatments, shorter periods of recovery from illness, more effective and/or cheaper means of illness prevention and/or reduced health resources in patient care. Previous Research A survey conducted for the World Health Organization in 200423 identified a number of studies that had been conducted in the United States, the United Kingdom and South America which had identified the benefits of improved or more effective treatments of specific illnesses (polio, tuberculosis, et cetera) to various economies. By and large, these earlier studies focussed on the benefits in terms of health care savings and were indifferent to the location of the research. As noted in the discussion above, research may yield benefits throughout the world and, conversely, benefits in health savings in any country may result from research anywhere in the world, depending on the rate of application in any given health care system and the prevalence of the health problem being studied. The Canadian Institute for Health Information has provided estimates of the total health care spending by province in Canada. Their estimates of spending for Saskatchewan are shown in Table 12, below. Table 12: Health Expenditures in Saskatchewan, 1996 to 2006 Calendar Year Private Sector Public Sector Combined Sectors (millions of current dollars) 1996 $ 625.0 $ 1,862.3 $ 2,487.3 1997 677.0 1,976.1 2,653.1 1998 669.8 2,103.5 2,773.3 1999 718.1 2,250.4 2,968.5 2000 766.5 2,381.2 3,147.7 2001 871.3 2,581.5 3,452.9 2002 901.3 2,725.4 3,626.7 2003 972.7 2,896.7 3,869.4 2004 1,012.7 3,108.6 4,121.2 2005 (forecast) 1,039.6 3,338.0 4,377.5 2006 (forecast) 1,078.4 3,615.0 4,693.4 Source: Canadian Institute for Health Information National Health Expenditure (NHEX) Database at http://qstat.cihi.ca/discoverer4i/viewer?eul accessed on October 2, 2007. 23 Martin Buxton, Steve Hanney and Teri Jones, op cit., pp.734.
30
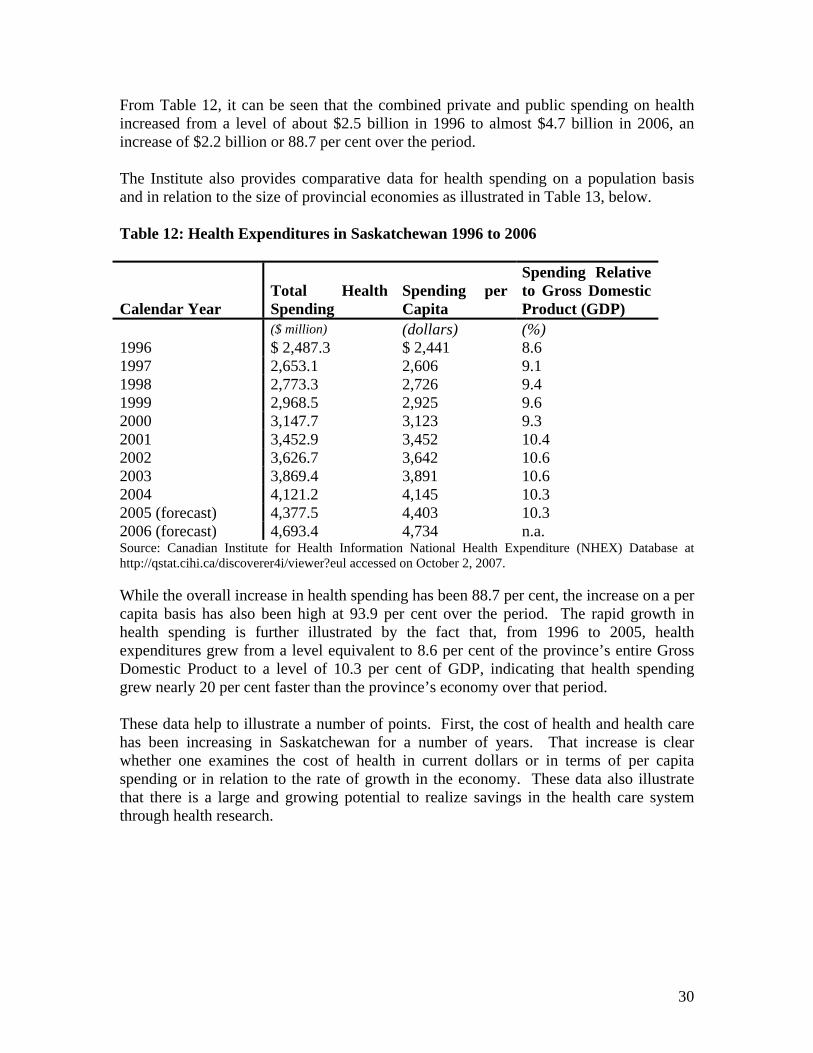
From Table 12, it can be seen that the combined private and public spending on health increased from a level of about $2.5 billion in 1996 to almost $4.7 billion in 2006, an increase of $2.2 billion or 88.7 per cent over the period. The Institute also provides comparative data for health spending on a population basis and in relation to the size of provincial economies as illustrated in Table 13, below. Table 12: Health Expenditures in Saskatchewan 1996 to 2006
Calendar Year Total Health Spending
Spending per Capita
Spending Relative to Gross Domestic Product (GDP)
($ million) (dollars) (%) 1996 $ 2,487.3 $ 2,441 8.6 1997 2,653.1 2,606 9.1 1998 2,773.3 2,726 9.4 1999 2,968.5 2,925 9.6 2000 3,147.7 3,123 9.3 2001 3,452.9 3,452 10.4 2002 3,626.7 3,642 10.6 2003 3,869.4 3,891 10.6 2004 4,121.2 4,145 10.3 2005 (forecast) 4,377.5 4,403 10.3 2006 (forecast) 4,693.4 4,734 n.a. Source: Canadian Institute for Health Information National Health Expenditure (NHEX) Database at http://qstat.cihi.ca/discoverer4i/viewer?eul accessed on October 2, 2007. While the overall increase in health spending has been 88.7 per cent, the increase on a per capita basis has also been high at 93.9 per cent over the period. The rapid growth in health spending is further illustrated by the fact that, from 1996 to 2005, health expenditures grew from a level equivalent to 8.6 per cent of the province’s entire Gross Domestic Product to a level of 10.3 per cent of GDP, indicating that health spending grew nearly 20 per cent faster than the province’s economy over that period. These data help to illustrate a number of points. First, the cost of health and health care has been increasing in Saskatchewan for a number of years. That increase is clear whether one examines the cost of health in current dollars or in terms of per capita spending or in relation to the rate of growth in the economy. These data also illustrate that there is a large and growing potential to realize savings in the health care system through health research.
31
VIII. Conclusions
This research suggests several conclusions important for assessing the value of research in Saskatchewan. First and foremost, one must always keep in mind that the primary purpose of health research is to discover and develop better methods for maintaining, restoring or achieving a greater quality of life for the population through improved health. The economic benefits of health research, to the extent they exist, should be understood to be merely a windfall benefit of good research that contributes to quality of life. With that said, it is clear from the calculations that health research does have a significant gross impact on Saskatchewan’s Gross Domestic Product and employment. The analysis of net impacts on GDP and employment also suggests that health research in Saskatchewan is a not insignificant contributor to the province’s economy. The extent of productivity and commercial benefits in Saskatchewan of health research in Saskatchewan, however, are difficult to estimate because of the way in which research is disseminated and utilized in the modern world. Available information would suggest that there is also limited commercialization of health research occurring in Saskatchewan. The available lists of business enterprises in Saskatchewan engaged in pharmaceutical and medicine manufacturing and medical equipment and supplies manufacturing suggest that such businesses in the province are only rarely engaged in the conversion of health research into commercial products. A similar problem arises with attributing the increases in employment and post-secondary enrollments in health-related fields to the existence of health research in Saskatchewan. Nonetheless, the statistics make it clear that both employment and post-secondary enrollment in health-related fields have been increasing over the last decade, and at a rate higher than that of the overall rate of growth in employment and post-secondary enrollments in the province. Clearly, health research is adding value both to the health system and to the province generally, though there is room for some further thinking about how to improve the utilization of health research.

32