Embed Size (px)
Citation preview

Herniated Disc Management
Jason C. Eck, DO, MSOrthopedic Spine Surgeon
Southeastern Spine and NeurosurgeryChattanooga, TN

Disclosures
• No financial disclosures

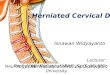
Herniated Disc
• Abnormal rupture of the soft central portion of the disc (nucleus pulposus) through the surrounding outer ring (annulus fibrosus). • About 95% of all disc herniation
cases, the L4-L5 or L5-S1 disc levels are involved

Herniated Disc
• Causes:• Trauma or injury to the disc• Disc degeneration• Congenital predisposition

Herniated Disc
• Classifications• Central
• Often associated with back pain only• May present with cauda equina syndrome
• Posterolateral• Most common (90-95%)• PLL is weakest here• Affects the traversing nerve root
• L4-L5 affects L5 nerve root• Foraminal
• Less common (5-10%)• Affects exiting nerve root
• L4/L5 affects L4 nerve root• Axillary
• Can affect both exiting and descending nerve roots

Herniated Disc
• Manifestations• Axial LBP
• May be discogenic or mechanical• Radicular pain
• Buttock and leg symptoms• Often worse with sitting• Worse with coughing, Valsalva,
sneezing• Cauda equina syndrome
• Bilateral leg pain• LE weakness• Saddle anesthesia• Bowel and bladder symptoms

Treatment
• Nonoperative• Rest• Medication
• NSAID’s• PO steroids• Steroid injections• Muscle relaxants• Nerve stabilizers
• PT• 90% improve without surgery

Treatment
• Surgical indications• Persistent pain lasting >6wks and
failing nonsurgical options• Progressive neurologic deficit• Intractable pain• Cauda equina symptoms

Treatment
• Surgery• Microdiscectomy
• Most common• MIS approach• Outpatient
• Fusion• Recurrent HNP• Instability• Calcified HNP
• Arthroplasty

Treatment
• Post op• Ambulating as tolerated• Minimize Bending/Lifting/Twisting
for ~6 weeks• Most gradually return to function• PT if needed

Treatment
• Risks of surgery• Infection• Recurrent HNP• Durotomy• Nerve injury• Vascular injury• Discitis• Medical complications

Questions??