Embed Size (px)
Citation preview

J Clin Ultrasound 8213-215. June 1980
Echographic Characteristics of Malignant Lymph Nodes
Bruce J. Hillman, M.D., and Kai Haber, M.D.’
Abstract: We retrospectively reviewed the sonograms of 42 sequential patients for whom there was sonographic evidence of malignant lymphadenopathy. Twenty-three patients were known to have lymphoma, whereas 19 patients had lymph nodes involved with metastases. Each case was categorized according to the sonographic “texture” of the masses and the extent of sound transmission. Sonolucent masses were observed in 83% of the lymphoma cases and in 53% of patients with soft-tissue tumors. Nonetheless, a mixture of patterns was observed in nearly one-third of the cases. In 5 lymphoma patients there were enlarged lymph nodes that had all of the echographic qualities of simple cysts. Aside from this pattern, no correlation could be made between sonographic pattern and histologic diagnosis. Indexing Words: Lymphadenopathy . Malignancy . Tissue characterization
Recent studies have reported sonographic accu- racy comparable to that of lymphography for diagnosing malignant lymph node enlargement; this appears to be true for both lymphomatous nodes (1,2/ and metastasis-involved nodes I1,3). Furthermore, ultrasound has the added advan- tage of being able to image mesenteric, renal hilar, and other abdominal lymph nodes that do not commonly fill with contrast material during lymphography.
For these reasons, ultrasound is now fre- quently used in the diagnosis and staging of malignant lymph node disease, as well as for fol- lowing up the results of therapy. Despite this, the acoustic patterns representative of enlarged lymph nodes are diverse and may cause confusion in arriving at the correct sonographic diagnosis. The purpose of this report is to assess the var- iations in these patterns and to suggest possible relationships between the acoustic “texture” and histologic diagnosis of a malignant lymph node.
~~ ~~ ~ ~~~~~~ ~-
‘Picker Scholar, James Picker Foundation. From the Department of Radiology, University of Arizona Health Sciences Center, Tucson, AZ. Manuscript received Oc- tober 10, 1979; revised manuscript accepted November 20, 1979. For reprints contact Rrucc J . Hillman. M.U.. Depart- ment of Radiology, University of Arizona Health Sciences Center, Tucson AZ 85724.
0 1980 by John Wiley & Sons, Inc 0091-27511801030213-03 $01 .OO
METHODS
Over the past 3 yr, abdominal ultrasound scans were performed for 42 patients in whom there was echographic evidence of lymph node enlargement. Twenty-three of these patients were known to have lymphoma. In the other 19 patients, metas- tases from a variety of known primary malignan- cies were believed to be responsible for the lymph node enlargement. All sonograms were performed on either conventional gray-scale equipment (2.25- or 3.5-MHz transducers) or an Octoson water-bath-type scanner (2.5-MHz transducers). Although many of the patients were scanned on multiple occasions, only the initial examination for each patient (prior to therapeutic interven- tion) was reviewed as part of this study.
The authors, who were unaware of the clinical diagnoses, retrospectively reviewed the sono- grams. Each scan consisted of multiple transverse and longitudinal images. The authors confirmed the presence of enlarged lymph nodes in each case. Then, reading independently, each author evaluated the masses’ internal echo characteris- tics (echo-dense; complex; relatively echolucent with sparse internal echoes; echolucent) and, if lu- cent masses were present, judged the extent of distal sound transmission (fair; good; enhanced). Discrepancies in the evaluations were resolved by consultation between the reviewers. The patients’
213

214 B.J. HILLMAN AND K. HABER
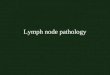
FIGURE 1. Transverse scan through the upper abdomen in a patient with lymphoma. The large arrow denotes a large echo-dense mass that is surrounded by smaller, predominantly lucent masses (small arrows) containing sparse echoes.
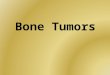
FIGURE 2. Longitudinal scan of a patient with lymphoma performed to the right of the midline that depicts multiple echolucent masses (arrows). These enlarged lymph nodes variously gave fair or good sound transmission.
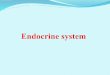
FIGURE 3 Longitudinal sonogram for a patient with lymphoma performed on the Octoson There was some electronic noise present, as evidenced by echoes within the superior mesenteric artery (small arrow) This same level of spurious noise was seen in the masses, which were echographically indistinguishable from cysts Note, in particular, the sharply defined margins and enhanced sound trans- mission manifested by three of the masses (white arrows)
clinical charts were then reviewed for their clini- cal diagnoses and evidence corroborating the presence of lymphadenopathy.
RESULTS
All of the patients used in this study had histolog- ically verified diagnoses. In addition, 9 of the 23 lymphoma patients had nonsonographic evidence of lymph node involvement (5 by biopsy, 2 by lymphography, and 1 each by CAT scan and intravenous urography). Of the 19 patients echographically positive for metastasis-involved lymph nodes, 6 were verified to have affected lymph nodes by other means (4 by tissue speci- men and 1 each by intravenous urography and angiography).
Table 1 correlates the sonographic findings with the patients’ known malignancies. A mix- ture of the internal echo patterns occurred in a number of cases (Fig. 11, accounting for the greater number of patterns tabulated than pa- tients scanned. Specifically, the multiple masses possessed two or more textures in 7 patients (30%) with lymphoma and in 5 patients (26%) with metastasis-affected nodes. Examples of relatively or absolutely echolucent masses (Fig. 2) were ob- served in 19 patients (83%) with lymphoma; this occurred in 10 patients (53%) with nodal metas- tases from primary soft-tissue tumors.
Table 2 demonstrates the relationships be- tween echolucent masses and the extent of sound transmission distal to the nodes these masses rep- resent. In 5 lymphoma patients, masses were ob- served that transmitted sound in an acoustically enhanced manner, indistinguishable from that usually attributed to cysts (Fig. 3). No case of nodal metastases showed this finding.
DISCUSSION
In our study there was considerable overlap in the internal echo patterns portraying lymphomatous and metastasis-affected lymph nodes. Whereas relatively or absolutely echolucent masses were observed in 83% of lymphoma patients, masses of similar appearance were frequently observed in patients with soft-tissue malignancies as well. Thus, internal echo characteristics alone seem in- sufficient to differentiate between the two condi- tions. This result is similar to results obtained in other attempts to sonographically characterize malignant tissues (4-6).
Of considerable interest, however, is the finding that some lymphomatous masses may SO
perfectly mimic cysts. The echographic qualities
JOURNAL OF CLINICAL ULTRASOUND

ECHOGRAPHIC CHARACTERISTICS OF MALIGNANT LYMPH NODES
TABLE 1 Correlation of Masses‘ Internal Echo Characteristics and Cell Types*
215
Internal Echo Pattern
Histology and Number of Patients Echo-dense Complex
Relatively Echolucent Echolucent
Lymphoma (23) Sarcoma (03) Adenocarcinoma (07) Hypernephroma (03) Squamous (02) Anaplastic (01) Small cell (03)
*Multiple patterns were observed in some patients, accounting for the greater number of patterns tabulated than patients scanned
TABLE 2 Extent of Sound Transmission Through Echolucent Masses
Sound Through-transmission
Lucent Masses Fair Good Enhanced
Lymphoma (22) 6 11 5 Lymphatic metastases (1 1) 4 7 0
of cysts (anechoicity, smooth walls, and distal wall enhancement) have been frequently em- phasized. The last of these criteria has been cited as being particularly useful in differentiating be- tween cystic and solid masses in equivocal cases (7). Nonetheless, scattered reports citing in- stances in which solid masses have manifested acoustic enhancement have recently appeared (8,9). The common explanation for this phenome- non has been that particularly homogeneous masses (such as lymphoma) may have few inter- nal interfaces to reflect the sonic beam (10). In addition, increasing use of high-frequency high- energy transducers may be compounding the problem (9). What has not been evidenced in the literature but is suggested in this study is the fre- quency with which cyst-simulating solid masses may occur. Five of our 23 lymphoma patients had enlarged lymph nodes that were echographically indistinguishable from cysts. No such pattern was observed in metastasis-affected nodes.
Despite the difficulties cited, ultrasound re- mains a useful modality for the diagnosis of malignant lymph node enlargement f1-3). Ma- lignant lymphadenopathy may present with a diverse variety of sonographic appearances. Al- though a cystic appearance of nodal masses in neoplastic disease suggests the diagnosis of lym- phoma, reliable differentiation between lym-
phomatous and metastasis-involved lymph nodes is at present beyond the scope of ultrasound tissue characterization.
1
2.
3.
4.
5 .
6 .
7.
8.
9.
10.
REFERENCES
Vadrot D, Laval-Jeantet M, Vadrot M: Echog- raphy in the examination of abdominal lympha- denopathies. J Radio1 Electrol Med Nucl 59:399, 1978. Brascho DJ, Durant JR, Green LE: The accuracy of retroperitoneal ultrasonography in Hodgkin’s dis- ease and non-Hodgkin’s lymphoma. Radiology 125485, 1977. Burney BT, Klatte EC: Ultrasound and computed tomography of the abdomen in the staging and management of testicular carcinoma. Radiology 132:415, 1979. Hillman BJ, Smith EH, Gammelgaard J, et al: Ultrasonographic-pathologic correlation of malig- nant hepatic masses. Gastrointestinal Radiology 4:361, 1979. Maklad NF, Chuang VP, Doust BD, e t al: U1- trasonographic characterization of solid renal le- sions: Echographic, angiographic, and pathologic correlation. Radiology 123:733, 1977. Green B, Bree RL, Goldstein HM, et al: Grey scale ultrasound evaluation of hepatic neoplasms: Pat- terns and correlations. Radiology 124:203, 1977. Goldberg BB: Abdominal Grey Scale Ultrasonog- raphy. New York, John Wiley & Sons, 1977. Cunningham J J : Ultrasonic findings in isolated lymphoma of the spleen simulating splenic abscess. J Clin Ultrasound 6:412, 1978. Bree RL, Silver TM: Differential diagnosis of hypoechoic and anechoic masses with gray scale sonography: New observations. J Clin Ultrasound 7:249, 1979. Yeh HC, Wolf BS: Ultrasonography and computed tomography in the diagnosis of homogeneous masses. Radiology 123:425, 1977.
VOL. 8, NO. 3, JUNE 1980