Embed Size (px)
Citation preview

Hindawi Publishing CorporationBioMed Research InternationalVolume 2013 Article ID 310483 11 pageshttpdxdoiorg1011552013310483
Review ArticleEchocardiography in the Era of MultimodalityCardiovascular Imaging
Benoy Nalin Shah12
1 Cardiovascular Biomedical Research Unit Royal Brompton Hospital Sydney Street London SW3 6NP UK2National Heart amp Lung Institute Imperial College London SW7 2AZ UK
Correspondence should be addressed to Benoy Nalin Shah benoydoctorsorguk
Received 11 April 2013 Accepted 11 June 2013
Academic Editor Dirk Bandorski
Copyright copy 2013 Benoy Nalin Shah This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Echocardiography remains the most frequently performed cardiac imaging investigation and is an invaluable tool for detailed andaccurate evaluation of cardiac structure and function Echocardiography nuclear cardiology cardiac magnetic resonance imagingand cardiovascular-computed tomography comprise the subspeciality of cardiovascular imaging and these techniques are oftenused together for a multimodality comprehensive assessment of a number of cardiac diseases This paper provides the generalcardiologist and physician with an overview of state-of-the-art modern echocardiography summarising established indications aswell as highlighting advances in stress echocardiography three-dimensional echocardiography deformation imaging and contrastechocardiography Strengths and limitations of echocardiography are discussed as well as the growing role of real-time three-dimensional echocardiography in the guidance of structural heart interventions in the cardiac catheter laboratory
1 Introduction
The beginning of the twenty-first century in cardiovascularimaging has been dominated by one theme ldquomultimodalityrdquoIt is currently the buzz word of imaging as the ldquotraditionalrdquotechniques of echocardiography and nuclear cardiology havebeen complimented by the more ldquomodernrdquo techniques ofcardiovascular magnetic resonance (CMR) and cardiac-computed tomography (CCT) Cardiovascular imaging hasseen an unprecedented growth in demand fuelled by tech-nological advances and wider availability of these modalities[1] Each of these techniques has strengths and weaknesses(Table 1) and in combination they are used widely in themanagement of patients with coronary heart disease valvularheart diseases heart failure congenital heart disease andarrhythmias The aim of this review is to provide a compre-hensive overview of contemporary echocardiography for thegeneral cardiologist and physician summarising establishedindications with the supporting evidence and also highlight-ing recent technological advances within the subspecialityparticularly in stress three-dimensional echocardiographydeformation imaging and contrast echocardiography and
the emerging role of real-time echocardiography for guidanceof interventional procedures
2 The Evolution of Cardiac Ultrasound
Echocardiography has witnessed dramatic improvements intechnology over the past 25 years Aside from the plain chestX-ray it remains the primarymdashand thus most frequentlyperformedmdashcardiac imaging investigationAwealth of struc-tural (anatomical) and haemodynamic (physiological) infor-mation can be ascertained from one examination Fromthe one-dimensional M-mode echocardiogram to real-timethree-dimensional imaging an echocardiographic study in2013 can reveal physiology and pathology in detail previouslyunimaginable
The numerous modalities within echocardiography fur-nish the scanning sonographer or physician with a wide arrayof technologies for complete assessment of cardiac morphol-ogy and function The high temporal resolution of M-modeechocardiography permits accurate depiction of rapidlymov-ing structures and retains relevance in todayrsquos practice
2 BioMed Research International
Table 1 A summary table comparing the four main modalities in cardiac imaging
Echocardiography Nuclear cardiology CMR CCTAvailability +++ ++ ++ ++Cost + ++ ++ ++Ionising radiation minus ++ minus ++Extracardiac information + + +++ +++Coronary artery assessment + minus ++ +++Assessment of systolic function +++ ++ +++ ++Assessment of diastolic function +++ + + +Assessment of valvular function +++ minus ++ +Physiological stress testing + + minus minus
Pharmacological stress testing + + + minus
Contraindication minus minus Most implanted devices minus
Limited by renal failure minus minus + +Risk of claustrophobia minus + ++ +
2D transthoracic echocardiography (TTE) forms the basisof visual assessment of cardiac chambers and valves andpermits identification of structural abnormalities Dopplerechocardiography comprising spectral Doppler (pulsedwaveand continuous wave) and colour Doppler imaging identi-fies the direction velocity amplitude and timing of bloodflow through the heart This information has an enormousnumber of usesmdashDoppler echocardiography remains the cor-nerstone of evaluating the severity of stenotic and regurgitantvalve diseases estimating LV filling pressures (and thus con-firming the diagnosis of diastolic dysfunction and in symp-tomatic patients heart failure with preserved ejection frac-tion) detection of intracavity and subvalvular obstructionin hypertrophic cardiomyopathy and for identification ofintracardiac shunts (eg septal defects)
Transoesophageal echocardiography (TOE) permits de-tailed views of most cardiac structures and has a very widenumber of indications from exclusion of atrial appendagethrombus prior to cardioversion through to investigation ofsuspected cardioembolic stroke [2] In most centres TOEremains the imaging technique of choice for precise assess-ment of mechanisms and severity of valvular heart diseaseand their associated complications (Figure 1) Although semi-invasive in nature TOE is generally well tolerated and has anexcellent safety profile [3 4]
3 Specific Advances
31 Stress Echocardiography Stress echocardiography (SE)has progressed significantly over the past three decadesto become one of the most widely utilised imaging tech-niques for evaluation of patients with known or suspectedcoronary artery disease (CAD) Once heavily criticised forbeing too ldquooperator dependentrdquo several technical advanceshave dramatically improved the accuracymdashand reducedvariabilitymdashof SE These include firstly the advent of tissueharmonic imaging which was shown to improve diagnosticaccuracy for detection of CAD over fundamental frequencyimaging in exercise [5] and dobutamine [6] SE secondly theintroduction of digital cine loop acquisition with side-by-side display of rest and stress images for ease of comparison
and thirdly and possibly most importantly the availabilityof ultrasound contrast agents for improved visualisation ofthe endocardial border and LV cavity during rest and stressimaging [7]
SE has numerous advantages as a stress technique but alsosome disadvantages Its advantages include the ubiquitousavailability of echocardiography machines and thus the lowinfrastructure cost lack of exposure to ionising radiationsafety multiple stressor options (physiological (treadmillor bicycle) or pharmacological (inotropes or vasodilators))portability and the substantial supporting evidence baseaccrued over the past 20 years The option of performingphysiological stress is important as this should always be thepreferred stress technique in an attempt to reproduce patientrsquossymptoms and also determine their functional aerobic capac-ity Disadvantages include a lower sensitivity than perfusiontechniques and suboptimal image quality in some patientsdespite use of ultrasound contrast
In the United Kingdom SE is nowmdashalong with myocar-dial perfusion scintigraphy and CMRmdashrecommended overexercise electrocardiography (ex-ECG) for the investigationof patients with chest pain suspected to be angina pectoris [8]A randomised controlled trial showed that SE is more cost-effective than ex-ECG for establishing the diagnosis of CADin patients hospitalised with chest pain [9] and a recent largereal-world study of the incorporation of SE into a chest painunit has confirmed the feasibility and prognostic value of thisapproach in routine practice [10]
There is also now growing appreciation of the potentialclinical value of SE for ldquononcoronaryrdquo applications (seeTable 2) in particular the dynamic assessment of valvularheart diseases These patients have traditionally been evalu-ated by resting echocardiography only although their symp-toms are typically induced by exertion Exercise echocardio-graphy can be used to risk stratify asymptomatic patientswith severe aortic stenosis (AS) Stress-induced increases inmean transaortic gradient [11 12] and pulmonary pressures[13] are associated with worse outcome Furthermore low-dose dobutamine stress echocardiography is frequently usedto differentiate true severe AS from ldquopseudosevererdquo AS inpatients with low-flow low-gradient aortic stenosis [14]
BioMed Research International 3
LV
RALA
(a)
Ao
LA
LV
(b)
AoV
(c) (d)
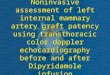
Figure 1 A patient with previousmitral valve repair attendedwith increasing breathlessness 2D-TTE revealed two jets ofmitral regurgitation(panel (a)) 2D-TOE suggested the presence of a paravalvular leak (panel (b) see arrows) Three-dimensional TOE revealed dehiscence ofthe posterior aspect of the mitral annuloplasty ring (panel (c) see arrow) and real-time 3D colour during TOE confirmed the presence ofa reguritant jet (arrow) through this defect (panel (d)) The patient subsequently underwent redo mitral valve surgery (LA left atrium RAright atrium LV left ventricle Ao aorta AoV aortic valve)
Table 2 Contemporary indications for stress echocardiography
Indication Parameter(s) measuredCoronary applications
Myocardial ischaemia Wall thickening at rest versus stressMyocardial viability Wall thickening at rest low-dose and peak stress
Noncoronary applications(A) Valve disease
Asymptomatic severe AS Exercise-induced change in mean transaortic gradientExercise-induced change in peak transtricuspid gradient
Low-flow low-gradient AS LVOT and AoV VTI at rest and low-dose dobutamine stressSymptomatic mildmoderate MS Exercise-induced change in mean transmitral and transtricuspid gradientsSymptomatic moderate MR Exercise-induced changes in EROA and pulmonary pressures
(B) CardiomyopathyHCM Exercise-induced dynamic LVOT obstructionDCM Contractile reserve in response to low-dose dobutamine
ICMAssessment of global LV contractile reserveAssessment of viability in posterolateral walls (for guiding LV lead placement)Assess exercise capacity objectivelyAssess inducibility of tachyarrhythmias
(AS aortic stenosis MS mitral stenosis MR mitral regurgitation LVOT left ventricular outflow tract AoV aortic valve EROA effective regurgitant orificearea VTI velocity time integral HCM hypertrophic cardiomyopathy DCM dilated cardiomyopathy ICM ischaemic cardiomyopathy)
4 BioMed Research International
Rest
(a)
Rest
(b)
Stress
(c)
Stress
(d)
Figure 2 A patient with moderate mitral stenosis but worsening exertional dyspnoea underwent exercise SE At rest mean transmitralgradient was 5mmHg (a) and transtricuspid pressure gradient was 24mmHg (b) After 7-minute BRUCE protocol treadmill exercise meantransmitral gradient significantly increased to 27mmHg (c) and transtricuspid pressure gradient had more than doubled to 51mmHg (d)The patient subsequently underwent balloon mitral valvuloplasty with excellent symptomatic relief
Exercise SE is also helpful in certain patients with mitralvalve disease Patients with mitral stenosis (MS) who havesymptoms disproportionate to the degree of MS at rest (egmarked exertional dyspnoea but only moderate MS at rest)should undergo exercise SEmdashan increase inmean transmitralgradient to gt15mmHg or pulmonary artery pressure togt60mmHg is an indication for valve intervention (Figure 2)The dynamic nature of ischaemic mitral regurgitation (MR)was previously shown in a quantitative Doppler echocardio-graphy study using exercise stress in patients with ischaemiccardiomyopathy (ICM) recently admitted with pulmonaryoedema and comparing with ICM patients without pul-monary oedema [15] Patientswith recent pulmonary oedemahad significantly greater increases in MR and pulmonarypressures during exercise than those without pulmonaryoedema The same group has also demonstrated the clinicalvalue of exercise SE in patients with degenerative MR [16] Arecent analysis clearly indicated the value of SE in valve dis-ease in daily clinical practice and also suggested expansion ofSE in valve disease beyond that indicated by current guide-lines [17]
Aside from valvular heart disease exercise SE can also beused in patients with hypertrophic cardiomyopathy to revealdynamic left ventricular outflow tract obstruction (Figure 3)[18] Finally myocardial contractile reserve determined bySE can identify those patients that will experience LV reverse
remodelling following cardiac resynchronisation therapy[19]
32 Three-Dimensional Echocardiography Three-dimen-sional (3D) echocardiography is widely perceived as a noveltechnique but the initial work on 3D echocardiography datesback three decades [20 21] However significant technicaladvances have reduced the size of the transducer improvedspeed of image processing and importantly allowed real-time 3D imaging This has been made possible with theadvent of fully sampled matrix array transducer technology[22]
3D-TTE has numerous proven uses in clinical practice Ithas been shown to be superior to 2D-TTE and equal to CMRfor assessment of ventricular volumes [23] cardiacmass [24]and calculation of ejection fraction [25] The latter is espe-cially useful clinically in patients that require serial EFassessment (eg cancer patients receiving chemotherapeuticagents with potential cardiotoxicity) as 2D-TTE can sufferfrom underestimation of true volumes due to chamber fore-shortening 3D-TTE has also been used to assess ventricularmechanical dyssynchrony [26] and of clinical relevancedyssynchronydemonstrated by real-time 3D-TTE canpredictlong-term response to cardiac resynchronization therapy[27] 3D-TTE has also been proved to be valuable in assess-ment of valvular heart diseasemdashit can provide information
BioMed Research International 5
(a) (b)
(c)
Figure 3 A 47-year-old man with hypertrophic cardiomyopathy underwent exercise SE At rest peak gradient across the aortic valve was12mmHg (panel (a)) Repeat assessment during a held Valsalva manoeuvre revealed that the peak gradient was now 63mmHg (panel (b))which indicates that exercise-induced LVOTobstruction is highly likelyThis was indeed confirmed that at peak stress themaximumgradienthad increased to 135mmHg (panel (c)) Note the late systolic peaking of the Doppler profile in panels (b) and (c) indicative of dynamic ratherthan fixed outflow tract obstruction The patient was commenced on beta-blocker therapy following the test results
previously only easily determined by TOE (eg mitral valvescallop assessment in mitral regurgitation) The accuracy ofcalculation of aortic valve area in aortic stenosis has also beenshown to be improved by using 3D-TTE due to more preciseassessment of outflow tract dimensions [28]
The most significant advance however has been in3D-TOE [29] Real-time 3D zoom and live 3D imaging pro-vide unique views of the heart and allow superior detection ofpathology especially valvular diseases 3D echocardiographyis most valuable in cases of complex pathology A simple P2prolapse of the mitral valve is usually evident from 2D imag-ing but a combination of flail scallop(s) and prolapse +minuschordal rupture may be more challenging on 2D and anyconfusion is usually dispelled with 3D imaging As discussedin the following the feasibility of real-time 3D-TOEhasmadeit an essential adjunct in guiding invasive procedures in thecatheter laboratory also
33 Deformation Imaging ldquoMyocardial Mechanicsrdquo Thecomplex orientation of myocardial fibresmdashradial circumfer-ential and longitudinalmdashhas been recognised for a long timeThe theory that tissue motion as opposed to endocardial
excursion is important in assessment ventricular function isalso not newmdashM-mode echocardiography was used to relatemyocardial velocity to ventricular function in the 1970s [30]
Tissue Doppler imaging (TDI) and speckle trackingechocardiography (STE) are techniques that permit detailedanalysis of regional as well as global cardiac function throughunique temporal and spatial data processing TDI deliberatelyfilters out the low amplitude high frequency signals from theblood-pool in order to allow analysis of the high amplitudeand low frequency signals frommyocardium itself [31] TDI ismost frequently used to assist in determining diastolic func-tion and LV filling pressures by means of the 1198641198641015840 ratio [32](where 1198641015840 is the early motion of the mitral annulus backtowards the cardiac base from the apex) The longitudinalfunction of both ventricles is also assessed with TDI where 1198781015840represents the peak systolic velocity of the left or right ventri-cle These parameters have become routine measurements inclinical practice due to a combination of their reproducibilityand diagnostic and prognostic importance
STE is based on the principle of following (or tracking)the unique ldquospeckle patternrdquo of amyocardial segment throughthe cardiac cycle (see Figure 4) One advantage of STE is that
6 BioMed Research International
(a) (b)
(c) (d)
Figure 4 Examples of strain imaging using speckle tracking echocardiography On the top row are images from a normal healthy volunteer(apical 4-chamber view on the left and summary strain scores with bulls-eye plot on the right) and on the bottom row are correspondingimages from a patient with severe ischaemic cardiomyopathy Note that the healthy volunteer has normal longitudinal strain in all segmentswith a global strain score of minus189 whereas the cardiomyopathy patient has highly abnormal strains with a significantly depressed globalstrain score of just minus50
it removes the possibility of falsely designating myocardiumas having normal function when ldquovelocityrdquo is in fact due totethering (eg adjacent scar) or translational motion due tomovement of the whole heart (both potential limitations ofTDI [33]) BothTDI and STE can be used tomeasuremyocar-dial strain a dimensionless quantity defined as the unitchange in length of an object relative to its original lengthStrain rate is its derivative with respect to time (ie rate ofchange of strain and usually expressed as 1sec (or secminus1)) Innormal myocardial segments there is shortening in systole(negative strain and strain rates) and lengthening in diastole(positive strain and strain rates) as cardiomyocytes return totheir resting state [33]
A wealth of data has been accumulated on the potentialclinical value of strain and strain rate assessment in a numberof cardiac diseases [34] Normal ranges have also beendefined [35] STE-derived strain imaging has been shownto have additive benefit for detection of CAD in patientsundergoing dobutamine SE [36] and the superior ability ofstrain imaging to predict outcome in patients undergoingdobutamine SE has also been shown [37] Strain imaging is anaccurate technique for detecting viablemyocardium particu-larly when strain parameters are assessed at rest and followinglow-dose dobutamine SE [38 39] Strain imaging has alsobeen studied extensively for detecting dyssynchrony and thuspredicting response to cardiac resynchronisation therapy[40] Recently it was shown that targeted placement of the LVpacing lead to the site of latest mechanical activationmdashaselucidated by STEmdashwas associated with favourable reverseremodelling fewer repeat hospitalizations and improvedfunctional capacity compared to patients with standard
placement of LV leads [41] TDI can also be used to assesscardiac dyssynchrony This has become a controversial topichowever as the PROSPECT trial [42] suggested no echocar-diographic parameter(s) could accurately predict favourableresponse to biventricular pacing though numerous author-ities worldwide were quick to highlight surprisingly funda-mental flaws in the trialrsquos methodology [43]
Potentially of great clinical relevance is the fact that STEcan reveal subclinical LV dysfunction in hearts with appar-ently normal systolic function as measured by EF and thuscould have a role in detecting cardiac involvement in systemicdiseases [44] unusual or rare conditions [45] and also fordetecting early evidence of cardiotoxicity in cancer patientsreceiving chemotherapy [46] At present strain and strainrate imaging remains predominantly research tools but showsconsiderable promise for translation into clinical practiceThe limitations of STE include the requirement of goodimage quality and variability between different software andhardware manufacturers
34 Contrast Echocardiography Ultrasound contrast agents(UCAs) consist of gas-filled microspheres which displayunique acoustic properties when exposed to ultrasoundwaves Contrast bubbles resonate when exposed to an ultra-sound wave This is predominantly a nonlinear oscillation(ie expansion and contraction of the bubble are not equal)at the ultrasound frequencies used in diagnostic imagingMicrobubbles are several million times more effective atscattering sound than red blood cells resulting in a greatlyenhanced ldquoblood poolrdquo signal [47] The blood pool agents
BioMed Research International 7
(a) (b)
(c) (d)Figure 5 Apical 4-chamber images taken before ((a) and (b)) and after ((c) and (d)) ultrasound contrast injection in a patient attending forroutine transthoracic echocardiography At rest endocardial definition at end diastole (a) and end systole (b) was poor and did not permitquantitation of ejection fraction or assessment of regional (segmental) function Following a single bolus injection of contrast endocardialborder visualisation was significantly improved at end diastole (c) and end systole (d) allowing regional and global systolic assessments
developed consist of a gaseous material encapsulated withina stabilizing outer shell These microbubbles are typicallyslightly smaller than erythrocytes allowing free passagewithin the circulation and effectively acting as red cell tracers[48]
The first generation UCAs consisted of air surrounded byan albumin shell [49] Unfortunately these agents had a veryshort lifespan in vivo and thus had limited utility in diagnostictests The second generation of UCAs addressed this issueby changing both components of microbubblesmdashthe air wasreplaced by inert gases with high molecular weight highdensity and low solubility such as sulphur hexafluoride(SonoVue) or perfluorocarbons (eg Optison or Definity)The outer shell is now made using phospholipids which also
confer greater stability They are used to produce a strongerultrasonic signal than that generated by tissues and thus aremost commonly used to improve image quality (Figure 5)
There is ample evidence demonstrating that UCAsimprove estimation of global [50] and regional [51] LV sys-tolic functions UCAs improve the accuracy of measurementof LV volumes and ejection fraction also [52 53] As UCAsimprove overall image quality they also help detect structuralabnormalities such as noncompaction cardiomyopathy [54]apical hypertrophic cardiomyopathy [55] and left ventric-ular thrombus [56] Their biggest use however is in stressechocardiography The use of contrast significantly reducesthe number of ldquouninterpretablerdquo studies [7] and thus is cost-effective as it reduces additional testing [57] This has helped
8 BioMed Research International
establish stress echocardiography as a front-line investigationin assessment of patients with known or suspected coronaryartery disease
The majority (90) of the blood within the myocardialwalls reside within capillaries [58] Thus the intensity of thecontrast signal when the myocardium is fully saturated withcontrast reflects the concentration of microbubbles withinmyocardial capillaries [59] and consequently capillary ormyocardial blood volume Appreciation of this fact led to therecognition that echocardiography could be used to assessmyocardial perfusion a technique now known as myocardialcontrast echocardiography (MCE) A high intensity (highmechanical index) ldquoflashrdquo or impulse is used to destroy themicrobubbles in the myocardial capillaries and their rate ofreplenishment is observed Delayed replenishment manifestsas a perfusion defect and is the hallmark of ischaemia duringMCE The first papers on MCE dates back to three decades[60 61] and since then it has accumulated a large evidencebase to support its use in the detection of CAD [62] Finallyas presence of contrast denotes vascularity UCAs can also beused in patients with intracardiac masses in order to distin-guish between avascularmasses (eg thrombus) and vascularmasses such as tumours [63]
4 lsquolsquoInterventional Echocardiologyrsquorsquo Dawn ofa New Super-Specialty
The advances in 3D echocardiographymdashin particular theadvent of a fully sampled matrix array transducer allowingreal-time 3D-TOEmdashhas brought the echocardiologist to theforefront of catheter-lab-based procedures in structural heartdisease Real-time 3D-TOE is now considered bymany a pre-requisite for guidance of percutaneous treatment of aorticstenosis (transcatheter aortic valve implantation (TAVI))mitral regurgitation (eg MitraClip devices) closure of theleft atrial appendage and of atrial septal defects (ASDs andPFOs) The incremental value of 3D-TOE over 2D-TOEduring TAVI procedures was recently demonstrated in alarge single-centre study [64] Indeed real-time 3D-TOE isexpanding its use further and for example has been usedto guide electrophysiological procedures such as ablation ofatrial flutter and fibrillation (helping reduce significantly theuse of fluoroscopy) [65]
Intracardiac echocardiography (ICE) performed in thecatheter laboratory using single-use percutaneous 2D probesintroduced transvenously (eg via the femoral vein) is alsowidely used to guide interventions [66] Its biggest advantageover TOE is the ability to obtain similar echo views withoutthe need for general anaesthesia with its attendant costs andpotential risks Therefore ICE has been used in preference toTOE for a number of procedures including atrial fibrillation[67] and ventricular tachycardia [68] ablation proceduresclosure of septal defects [69] TAVI procedures [70] and toguide CRT procedures [71] However the significant limita-tion of ICE is expensive given that the probes must be dis-posed of after a single use
The echocardiologist performing such studies needs tohave a sound grasp of normal cardiac and valvular anatomy
and combine quick thinking with speedy manual dexterityThis skill set is not necessarily acquired during conventionaltraining Heshe may be called upon to provide urgent infor-mation in case of sudden unexplained patient deterioration(eg sudden hypotension during TAVI due to entanglementof the delivery system in the mitral subvalvular apparatuscausing acute severe mitral regurgitation) The need for suchindividuals is likely to be restricted to tertiary units butin large centres one can imagine such a person spendinga significant amount of time in the cardiac catheter lab-oratories Appropriate training will be required to ensurethat we produce cardiologists capable of performing suchstudiesmdashhence one can envisage the birth of a super-special-ity of ldquointerventional echocardiologyrdquo
5 Limitations
Echocardiography does have certain limitations which meritdiscussionThe greatest advantage of cross-sectional imaging(ie CMR and CCT) over echocardiography is the informa-tion available on extracardiac structures The aorta aorticarch pulmonary artery and pulmonary veins are far moreclearly seen by these modalities and are often poorly seen ornot seen at all by echocardiography Thus assessment of pul-monary veins in patients awaiting an atrial fibrillation abla-tion procedure assessment of the aortic arch and descendingthoracic aorta in patients with chronic aortic dissection orcoarctation and serial assessment of patients with previouscoarctation repair for example will generally be performedby CMR or CCT
Echocardiography can also suffer from poor image qual-ity despite the use of ultrasound contrast agentsThis is mostoften seen in patientswho are extremely underweight or over-weight but also in patients with chronic airways disease orchest wall deformities (eg pectus excavatum) Patients onintensive care units who are frequently supine and may bemechanically ventilated also often have challenging TTEimages although TOE can resolve such difficulties
6 Conclusion
Echocardiography permits accurate assessment of myocar-dial structure function and perfusion Echocardiography isthus in itself a multimodality imaging technique The fieldof echocardiography is diverse and encompasses numerousindividual techniquesmdashsome with established clinical valuewhilst others showmuch promise in researchThe expandingrole of echocardiography within current clinical practice isunderpinned by continual technological advances and justi-fied by the accumulating evidence of clinical value of thesetechniques when utilised in daily practice
References
[1] L J Shaw T HMarwickW A Zoghbi et al ldquoWhy all the focuson cardiac imagingrdquo JACC Cardiovascular Imaging vol 3 no7 pp 789ndash794 2010
[2] F A Flachskampf L Badano W G Daniel et al ldquoRecommen-dations for transoesophageal echocardiography update 2010rdquo
BioMed Research International 9
European Journal of Echocardiography vol 11 no 7 pp 557ndash5762010
[3] W G Daniel R ErbelW Kasper et al ldquoSafety of transesophag-eal echocardiography A multicenter survey of 10419 examina-tionsrdquo Circulation vol 83 no 3 pp 817ndash821 1991
[4] J N Hilberath D A Oakes S K Shernan B E Bulwer M NDrsquoAmbra and H K Eltzschig ldquoSafety of transesophageal echo-cardiographyrdquo Journal of the American Society of Echocardiog-raphy vol 23 no 11 pp 1115ndash1127 2010
[5] D G Skolnick S G Sawada H Feigenbaum and D S SegarldquoEnhanced endocardial visualization with noncontrast har-monic imaging during stress echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 12 no 7 pp 559ndash5631999
[6] F B Sozzi D Poldermans J J Bax et al ldquoSecond harmonicimaging improves sensitivity of dobutamine stress echocar-diography for the diagnosis of coronary artery diseaserdquo TheAmerican Heart Journal vol 142 no 1 pp 153ndash159 2001
[7] J C Plana I A Mikati H Dokainish et al ldquoA randomizedcross-over study for evaluation of the effect of image optimiza-tion with contrast on the diagnostic accuracy of dobutamineechocardiography in coronary artery disease The OPTIMIZEtrialrdquo JACC Cardiovascular Imaging vol 1 no 2 pp 145ndash1522008
[8] J S Skinner L Smeeth J M Kendall P C Adams and ATimmis ldquoNICE guidance Chest pain of recent onset assess-ment and diagnosis of recent onset chest pain or discomfort ofsuspected cardiac originrdquo Heart vol 96 no 12 pp 974ndash9782010
[9] P Jeetley L Burden B Stoykova and R Senior ldquoClinical andeconomic impact of stress echocardiography compared withexercise electrocardiography in patients with suspected acutecoronary syndrome but negative troponin a prospective ran-domized controlled studyrdquo European Heart Journal vol 28 no2 pp 204ndash211 2007
[10] BN ShahG Balaji A Alhajiri I S Ramzy S Ahmadvazir andR Senior ldquoThe incremental diagnostic and prognostic valueof contemporary stress echocardiography in a chest pain unitmortality and morbidity outcomes from a real-world settingrdquoCirculation Cardiovascular Imaging vol 6 no 2 pp 202ndash2092013
[11] P Lancellotti F LeboisM Simon C Tombeux C Chauvel andL A Pierard ldquoPrognostic importance of quantitative exerciseDoppler echocardiography in asymptomatic valvular aorticstenosisrdquo Circulation vol 112 no 9 supplement pp I377ndashI3822005
[12] S Marechaux Z Hachicha A Bellouin et al ldquoUsefulness ofexercise-stress echocardiography for risk stratification of trueasymptomatic patients with aortic valve stenosisrdquo EuropeanHeart Journal vol 31 no 11 pp 1390ndash1397 2010
[13] P Lancellotti J Magne E Donal et al ldquoDeterminants andprognostic significance of exercise pulmonary hypertension inasymptomatic severe aortic stenosisrdquoCirculation vol 126 no 7pp 851ndash859 2012
[14] JMonin JQuereMMonchi et al ldquoLow-gradient aortic steno-sis Operative risk stratification and predictors for long-termoutcome a multicenter study using dobutamine stress hemo-dynamicsrdquo Circulation vol 108 no 3 pp 319ndash324 2003
[15] L A Pierard and P Lancellotti ldquoThe role of ischemic mitralregurgitation in the pathogenesis of acute pulmonary edemardquoThe New England Journal of Medicine vol 351 no 16 pp 1627ndash1634 2004
[16] J Magne P Lancellotti and L A Pierard ldquoExercise-inducedchanges in degenerative mitral regurgitationrdquo Journal of theAmericanCollege of Cardiology vol 56 no 4 pp 300ndash309 2010
[17] S Bhattacharyya V Kamperidis B N Shah et al ldquo152 Clinicalutility and prognostic value of appropriateness criteria in stressechocardiography for evaluation of valvular heart diseaserdquoHeart vol 99 pp A89ndashA90 2013
[18] B J Gersh B J Maron R O Bonow et al ldquo2011 ACCFAHAguideline for the diagnosis and treatment of hypertrophic cardi-omyopathyrdquo Journal of the American College of Cardiology vol58 no 25 pp e212ndashe260 2011
[19] P Lancellotti M Senechal M Moonen et al ldquoMyocardial con-tractile reserve during exercise predicts left ventricular reverseremodelling after cardiac resynchronization therapyrdquo Euro-pean Journal of Echocardiography vol 10 no 5 pp 663ndash6682009
[20] M Matsumoto M Inoue S Tamura K Tanaka and H AbeldquoThree-dimensional echocardiography for spatial visualizationand volume calculation of cardiac structuresrdquo Journal of ClinicalUltrasound vol 9 no 4 pp 157ndash165 1981
[21] K H Sheikh S W Smith O von Ramm and J Kisslo ldquoReal-time three-dimensional echocardiography feasibility and ini-tial userdquo Echocardiography vol 8 no 1 pp 119ndash125 1991
[22] L Sugeng L Weinert K Thiele and R M Lang ldquoReal-timethree-dimensional echocardiography using a novelmatrix arraytransducerrdquo Echocardiography vol 20 no 7 pp 623ndash635 2003
[23] N P Nikitin C Constantin P H Loh et al ldquoNew generation3-dimensional echocardiography for left ventricular volumetricand functional measurements comparison with cardiac mag-netic resonancerdquo European Journal of Echocardiography vol 7no 5 pp 365ndash372 2006
[24] V Mor-Avi L Sugeng L Weinert et al ldquoFast measurement ofleft ventricular mass with real-time three-dimensional echocar-diography comparison withmagnetic resonance imagingrdquoCir-culation vol 110 no 13 pp 1814ndash1818 2004
[25] L Sugeng V Mor-Avi L Weinert et al ldquoQuantitative assess-ment of left ventricular size and function side-by-side compari-son of real-time three-dimensional echocardiography and com-puted tomography with magnetic resonance referencerdquo Cir-culation vol 114 no 7 pp 654ndash661 2006
[26] S Kapetanakis M T Kearney A Siva N Gall M Cooklinand M J Monaghan ldquoReal-time three-dimensional echocar-diography a novel technique to quantify global left ventricularmechanical dyssynchronyrdquo Circulation vol 112 no 7 pp 992ndash1000 2005
[27] O I I Soliman M L Geleijnse D A M J Theuns et alldquoUsefulness of left ventricular systolic dyssynchrony by real-time three-dimensional echocardiography to predict long-termresponse to cardiac resynchronization therapyrdquo The AmericanJournal of Cardiology vol 103 no 11 pp 1586ndash1591 2009
[28] A V Khaw R S von Bardeleben C Strasser et al ldquoDirect mea-surement of left ventricular outflow tract by transthoracic real-time 3D-echocardiography increases accuracy in assessment ofaortic valve stenosisrdquo International Journal of Cardiology vol136 no 1 pp 64ndash71 2009
[29] L Sugeng S K Shernan I S Salgo et al ldquoLive 3-dimensionaltransesophageal echocardiography Initial experience using thefully-sampled matrix array proberdquo Journal of the American Col-lege of Cardiology vol 52 no 6 pp 446ndash449 2008
[30] D G Gibson T A Prewitt and D J Brown ldquoAnalysis of leftventricular wall movement during isovolumic relaxation and its
10 BioMed Research International
relation to coronary artery diseaserdquo The British Heart Journalvol 38 no 10 pp 1010ndash1019 1976
[31] P Palka A Lange A D Fleming G R Sutherland L N FeenandW NMcDicken ldquoDoppler tissue imaging myocardial wallmotion velocities in normal subjectsrdquo Journal of the AmericanSociety of Echocardiography vol 8 no 5 pp 659ndash668 1995
[32] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressures acomparative simultaneous Doppler-catheterization studyrdquo Cir-culation vol 102 no 15 pp 1788ndash1794 2000
[33] H Blessberger and T Binder ldquoTwo dimensional speckle track-ing echocardiography basic principlesrdquoHeart vol 96 no 9 pp716ndash722 2010
[34] J Gorcsan III and H Tanaka ldquoEchocardiographic assessmentof myocardial strainrdquo Journal of the American College of Cardi-ology vol 58 no 14 pp 1401ndash1413 2011
[35] T H Marwick R L Leano J Brown et al ldquoMyocardial strainmeasurement with 2-dimensional speckle-tracking echocardi-ography Definition of normal rangerdquo JACC CardiovascularImaging vol 2 no 1 pp 80ndash84 2009
[36] A C T Ng M Sitges P N Pham et al ldquoIncrementalvalue of 2-dimensional speckle tracking strain imaging to wallmotion analysis for detection of coronary artery disease inpatients undergoing dobutamine stress echocardiographyrdquoTheAmerican Heart Journal vol 158 no 5 pp 836ndash844 2009
[37] C B Ingul E Rozis S A Slordahl and T H Marwick ldquoIncre-mental value of strain rate imaging to wall motion analysisfor prediction of outcome in patients undergoing dobutaminestress echocardiographyrdquo Circulation vol 115 no 10 pp 1252ndash1259 2007
[38] R Hoffmann E Altiok B Nowak et al ldquoStrain rate measure-ment by Doppler echocardiography allows improved assess-ment of myocardial viability in patients with depressed left ven-tricular functionrdquo Journal of the American College of Cardiologyvol 39 no 3 pp 443ndash449 2002
[39] L Hanekom C Jenkins L Jeffries et al ldquoIncremental valueof strain rate analysis as an adjunct to wall-motion scoring forassessment of myocardial viability by dobutamine echocardio-graphy a follow-up study after revascularizationrdquo Circulationvol 112 no 25 pp 3892ndash3900 2005
[40] H Tanaka H Nesser T Buck et al ldquoDyssynchrony by speckle-tracking echocardiography and response to cardiac resynchro-nization therapy results of the speckle tracking and resynchro-nization (STAR) studyrdquo European Heart Journal vol 31 no 14pp 1690ndash1700 2010
[41] F Z Khan M S Virdee C R Palmer et al ldquoTargeted leftventricular lead placement to guide cardiac resynchronizationtherapy the TARGET study a randomized controlled trialrdquoJournal of the American College of Cardiology vol 59 no 17 pp1509ndash1518 2012
[42] E S Chung A R Leon L Tavazzi et al ldquoResults of the predic-tors of response to CRT (PROSPECT) trialrdquoCirculation vol 117no 20 pp 2608ndash2616 2008
[43] J J Bax and J Gorcsan III ldquoEchocardiography and noninvasiveimaging in cardiac resynchronization therapy Results of thePROSPECT (predictors of response to cardiac resynchroniza-tion therapy) study in perspectiverdquo Journal of the American Col-lege of Cardiology vol 53 no 21 pp 1933ndash1943 2009
[44] B N Shah M de Villa R S Khattar and R Senior ldquoImagingcardiac sarcoidosis the incremental benefit of speckle trackingechocardiographyrdquo Echocardiography 2013
[45] J KramerM Niemann D Liu et al ldquoTwo-dimensional speckletracking as a non-invasive tool for identification of myocardialfibrosis in Fabry diseaserdquoEuropeanHeart Journal vol 34 no 21pp 1587ndash1596 2013
[46] J L Hare J K Brown R Leano C Jenkins N Woodwardand T H Marwick ldquoUse of myocardial deformation imaging todetect preclinical myocardial dysfunction before conventionalmeasures in patients undergoing breast cancer treatment withtrastuzumabrdquo The American Heart Journal vol 158 no 2 pp294ndash301 2009
[47] M J Stewart ldquoContrast echocardiographyrdquoHeart vol 89 no 3pp 342ndash348 2003
[48] R Janardhanan G Dwivedi S Hayat and R Senior ldquoMyocar-dial contrast echocardiography a new tool for assessment ofmyocardial perfusionrdquo Indian Heart Journal vol 57 no 3 pp210ndash216 2005
[49] S B Feinstein F J T Cate W Zwehl et al ldquoTwo-dimensionalcontrast echocardiography I In vitro development and quanti-tative analysis of echo contrast agentsrdquo Journal of the AmericanCollege of Cardiology vol 3 no 1 pp 14ndash20 1984
[50] R Hoffmann S von Bardeleben F T Cate et al ldquoAssessmentof systolic left ventricular function a multi-centre comparisonof cineventriculography cardiac magnetic resonance imagingunenhanced and contrast-enhanced echocardiographyrdquo Euro-pean Heart Journal vol 26 no 6 pp 607ndash616 2005
[51] R Hoffmann S von Bardeleben J D Kasprzak et al ldquoAnalysisof regional left ventricular function by cineventriculographycardiac magnetic resonance imaging and unenhanced andcontrast-enhanced echocardiography a multicenter compari-son of methodsrdquo Journal of the American College of Cardiologyvol 47 no 1 pp 121ndash128 2006
[52] W G Hundley A M Kizilbash I Afridi F Franco R MPeshock and P A Grayburn ldquoAdministration of an intravenousperfluorocarbon contrast agent improves echocardiographicdetermination of left ventricular volumes and ejection fractioncomparison with cine magnetic resonance imagingrdquo Journal ofthe American College of Cardiology vol 32 no 5 pp 1426ndash14321998
[53] S Malm S Frigstad E Sagberg H Larsson and T SkjaerpeldquoAccurate and reproducible measurement of left ventricularvolume and ejection fraction by contrast echocardiography acomparison with magnetic resonance imagingrdquo Journal of theAmerican College of Cardiology vol 44 no 5 pp 1030ndash10352004
[54] B K Koo D Choi J W Ha S M Kang N Chung and S YCho ldquoIsolated noncompaction of the ventricular myocardiumcontrast echocardiographic findings and review of the litera-turerdquo Echocardiography vol 19 no 2 pp 153ndash156 2002
[55] P Soman J Swinburn M Callister N G Stephens and RSenior ldquoApical hypertrophic cardiomyopathy bedside diagno-sis by intravenous contrast echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 14 no 4 pp 311ndash3132001
[56] S Thanigaraj K B Schechtman and J E Perez ldquoImprovedechocardiographic delineation of left ventricular thrombuswith the use of intravenous second-generation contrast imageenhancementrdquo Journal of the American Society of Echocardiog-raphy vol 12 no 12 pp 1022ndash1026 1999
[57] S Thanigaraj R F Nease Jr K B Schechtman R L Wade SLoslo and J E Perez ldquoUse of contrast for image enhancementduring stress echocardiography is cost-effective and reduces
BioMed Research International 11
additional diagnostic testingrdquo The American Journal of Cardi-ology vol 87 no 12 pp 1430ndash1432 2001
[58] S Kaul and A R Jayaweera ldquoCoronary and myocardial bloodvolumes noninvasive tools to assess the coronary microcircu-lationrdquo Circulation vol 96 no 3 pp 719ndash724 1997
[59] K Wei A R Jayaweera S Firoozan A Linka D M Skybaand S Kaul ldquoBasis for detection of stenosis using venousadministration of microbubbles during myocardial contrastechocardiography bolus or continuous infusionrdquo Journal of theAmeri-canCollege of Cardiology vol 32 no 1 pp 252ndash260 1998
[60] W F Armstrong T M Mueller E L Kinney E G Tickner JC Dillon and H Feigenbaum ldquoAssessment of myocardial per-fusion abnormalities with contrast-enhanced two-dimensionalechocardiographyrdquo Circulation vol 66 no 1 pp 166ndash173 1982
[61] C Tei T Sakamaki PM Shah et al ldquoMyocardial contrast echo-cardiography a reproducible technique of myocardial opacifi-cation for identifying regional perfusion deficitsrdquo Circulationvol 67 no 3 pp 585ndash593 1983
[62] R Senior H BecherMMonaghan et al ldquoContrast echocardio-graphy evidence-based recommendations by european associ-ation of echocardiographyrdquo European Journal of Echocardiogra-phy vol 10 no 2 pp 194ndash212 2009
[63] S Bhattacharyya R Khattar andR Senior ldquoCharacterisation ofintra-cardiacmasses bymyocardial contrast echocardiographyrdquoInternational Journal of Cardiology vol 163 no 1 pp e11ndashe132013
[64] L A Smith R Dworakowski A Bhan et al ldquoReal-time three-dimensional transesophageal echocardiography adds value totranscatheter aortic valve implantationrdquo Journal of theAmericanSociety of Echocardiography vol 26 no 4 pp 359ndash369 2013
[65] F Regoli F F Faletra G Nucifora et al ldquoFeasibility and acuteefficacy of radiofrequency ablation of cavotricuspid isthmus-dependent atrial flutter guided by real-time 3D TEErdquo JACCCardiovascular Imaging vol 4 no 7 pp 716ndash726 2011
[66] S S Kim ZM Hijazi R M Lang and B P Knight ldquoThe use ofintracardiac echocardiography and other intracardiac imagingtools to guide noncoronary cardiac interventionsrdquo Journal of theAmerican College of Cardiology vol 53 no 23 pp 2117ndash21282009
[67] JMMangrum J PMounsey L C Kok J P DiMarco andD EHaines ldquoIntracardiac echocardiography-guided anatomicallybased radiofrequency ablation of focal atrial fibrillation origi-nating from pulmonary veinsrdquo Journal of the American Collegeof Cardiology vol 39 no 12 pp 1964ndash1972 2002
[68] R Bala J F Ren M D Hutchinson et al ldquoAssessing epicardialsubstrate using intracardiac echocardiography during VT abla-tionrdquo Circulation Arrhythmia and Electrophysiology vol 4 no5 pp 667ndash673 2011
[69] C Vigna N Marchese M Zanchetta et al ldquoEchocardio-graphic guidance of percutaneous patent foramen ovale closurehead-to-head comparison of transesophageal versus rotationalintracardiac echocardiographyrdquo Echocardiography vol 29 no9 pp 1103ndash1110 2012
[70] T Bartel N Bonaros L Muller et al ldquoIntracardiac echocar-diography a new guiding tool for transcatheter aortic valvereplacementrdquo Journal of the American Society of Echocardiog-raphy vol 24 no 9 pp 966ndash975 2011
[71] R Bai L Di Biase P Mohanty et al ldquoPositioning of left ventric-ular pacing lead guided by intracardiac echocardiography withvector velocity imaging during cardiac resynchronization ther-apy procedurerdquo Journal of Cardiovascular Electrophysiology vol22 no 9 pp 1034ndash1041 2011

2 BioMed Research International
Table 1 A summary table comparing the four main modalities in cardiac imaging
Echocardiography Nuclear cardiology CMR CCTAvailability +++ ++ ++ ++Cost + ++ ++ ++Ionising radiation minus ++ minus ++Extracardiac information + + +++ +++Coronary artery assessment + minus ++ +++Assessment of systolic function +++ ++ +++ ++Assessment of diastolic function +++ + + +Assessment of valvular function +++ minus ++ +Physiological stress testing + + minus minus
Pharmacological stress testing + + + minus
Contraindication minus minus Most implanted devices minus
Limited by renal failure minus minus + +Risk of claustrophobia minus + ++ +
2D transthoracic echocardiography (TTE) forms the basisof visual assessment of cardiac chambers and valves andpermits identification of structural abnormalities Dopplerechocardiography comprising spectral Doppler (pulsedwaveand continuous wave) and colour Doppler imaging identi-fies the direction velocity amplitude and timing of bloodflow through the heart This information has an enormousnumber of usesmdashDoppler echocardiography remains the cor-nerstone of evaluating the severity of stenotic and regurgitantvalve diseases estimating LV filling pressures (and thus con-firming the diagnosis of diastolic dysfunction and in symp-tomatic patients heart failure with preserved ejection frac-tion) detection of intracavity and subvalvular obstructionin hypertrophic cardiomyopathy and for identification ofintracardiac shunts (eg septal defects)
Transoesophageal echocardiography (TOE) permits de-tailed views of most cardiac structures and has a very widenumber of indications from exclusion of atrial appendagethrombus prior to cardioversion through to investigation ofsuspected cardioembolic stroke [2] In most centres TOEremains the imaging technique of choice for precise assess-ment of mechanisms and severity of valvular heart diseaseand their associated complications (Figure 1) Although semi-invasive in nature TOE is generally well tolerated and has anexcellent safety profile [3 4]
3 Specific Advances
31 Stress Echocardiography Stress echocardiography (SE)has progressed significantly over the past three decadesto become one of the most widely utilised imaging tech-niques for evaluation of patients with known or suspectedcoronary artery disease (CAD) Once heavily criticised forbeing too ldquooperator dependentrdquo several technical advanceshave dramatically improved the accuracymdashand reducedvariabilitymdashof SE These include firstly the advent of tissueharmonic imaging which was shown to improve diagnosticaccuracy for detection of CAD over fundamental frequencyimaging in exercise [5] and dobutamine [6] SE secondly theintroduction of digital cine loop acquisition with side-by-side display of rest and stress images for ease of comparison
and thirdly and possibly most importantly the availabilityof ultrasound contrast agents for improved visualisation ofthe endocardial border and LV cavity during rest and stressimaging [7]
SE has numerous advantages as a stress technique but alsosome disadvantages Its advantages include the ubiquitousavailability of echocardiography machines and thus the lowinfrastructure cost lack of exposure to ionising radiationsafety multiple stressor options (physiological (treadmillor bicycle) or pharmacological (inotropes or vasodilators))portability and the substantial supporting evidence baseaccrued over the past 20 years The option of performingphysiological stress is important as this should always be thepreferred stress technique in an attempt to reproduce patientrsquossymptoms and also determine their functional aerobic capac-ity Disadvantages include a lower sensitivity than perfusiontechniques and suboptimal image quality in some patientsdespite use of ultrasound contrast
In the United Kingdom SE is nowmdashalong with myocar-dial perfusion scintigraphy and CMRmdashrecommended overexercise electrocardiography (ex-ECG) for the investigationof patients with chest pain suspected to be angina pectoris [8]A randomised controlled trial showed that SE is more cost-effective than ex-ECG for establishing the diagnosis of CADin patients hospitalised with chest pain [9] and a recent largereal-world study of the incorporation of SE into a chest painunit has confirmed the feasibility and prognostic value of thisapproach in routine practice [10]
There is also now growing appreciation of the potentialclinical value of SE for ldquononcoronaryrdquo applications (seeTable 2) in particular the dynamic assessment of valvularheart diseases These patients have traditionally been evalu-ated by resting echocardiography only although their symp-toms are typically induced by exertion Exercise echocardio-graphy can be used to risk stratify asymptomatic patientswith severe aortic stenosis (AS) Stress-induced increases inmean transaortic gradient [11 12] and pulmonary pressures[13] are associated with worse outcome Furthermore low-dose dobutamine stress echocardiography is frequently usedto differentiate true severe AS from ldquopseudosevererdquo AS inpatients with low-flow low-gradient aortic stenosis [14]
BioMed Research International 3
LV
RALA
(a)
Ao
LA
LV
(b)
AoV
(c) (d)
Figure 1 A patient with previousmitral valve repair attendedwith increasing breathlessness 2D-TTE revealed two jets ofmitral regurgitation(panel (a)) 2D-TOE suggested the presence of a paravalvular leak (panel (b) see arrows) Three-dimensional TOE revealed dehiscence ofthe posterior aspect of the mitral annuloplasty ring (panel (c) see arrow) and real-time 3D colour during TOE confirmed the presence ofa reguritant jet (arrow) through this defect (panel (d)) The patient subsequently underwent redo mitral valve surgery (LA left atrium RAright atrium LV left ventricle Ao aorta AoV aortic valve)
Table 2 Contemporary indications for stress echocardiography
Indication Parameter(s) measuredCoronary applications
Myocardial ischaemia Wall thickening at rest versus stressMyocardial viability Wall thickening at rest low-dose and peak stress
Noncoronary applications(A) Valve disease
Asymptomatic severe AS Exercise-induced change in mean transaortic gradientExercise-induced change in peak transtricuspid gradient
Low-flow low-gradient AS LVOT and AoV VTI at rest and low-dose dobutamine stressSymptomatic mildmoderate MS Exercise-induced change in mean transmitral and transtricuspid gradientsSymptomatic moderate MR Exercise-induced changes in EROA and pulmonary pressures
(B) CardiomyopathyHCM Exercise-induced dynamic LVOT obstructionDCM Contractile reserve in response to low-dose dobutamine
ICMAssessment of global LV contractile reserveAssessment of viability in posterolateral walls (for guiding LV lead placement)Assess exercise capacity objectivelyAssess inducibility of tachyarrhythmias
(AS aortic stenosis MS mitral stenosis MR mitral regurgitation LVOT left ventricular outflow tract AoV aortic valve EROA effective regurgitant orificearea VTI velocity time integral HCM hypertrophic cardiomyopathy DCM dilated cardiomyopathy ICM ischaemic cardiomyopathy)
4 BioMed Research International
Rest
(a)
Rest
(b)
Stress
(c)
Stress
(d)
Figure 2 A patient with moderate mitral stenosis but worsening exertional dyspnoea underwent exercise SE At rest mean transmitralgradient was 5mmHg (a) and transtricuspid pressure gradient was 24mmHg (b) After 7-minute BRUCE protocol treadmill exercise meantransmitral gradient significantly increased to 27mmHg (c) and transtricuspid pressure gradient had more than doubled to 51mmHg (d)The patient subsequently underwent balloon mitral valvuloplasty with excellent symptomatic relief
Exercise SE is also helpful in certain patients with mitralvalve disease Patients with mitral stenosis (MS) who havesymptoms disproportionate to the degree of MS at rest (egmarked exertional dyspnoea but only moderate MS at rest)should undergo exercise SEmdashan increase inmean transmitralgradient to gt15mmHg or pulmonary artery pressure togt60mmHg is an indication for valve intervention (Figure 2)The dynamic nature of ischaemic mitral regurgitation (MR)was previously shown in a quantitative Doppler echocardio-graphy study using exercise stress in patients with ischaemiccardiomyopathy (ICM) recently admitted with pulmonaryoedema and comparing with ICM patients without pul-monary oedema [15] Patientswith recent pulmonary oedemahad significantly greater increases in MR and pulmonarypressures during exercise than those without pulmonaryoedema The same group has also demonstrated the clinicalvalue of exercise SE in patients with degenerative MR [16] Arecent analysis clearly indicated the value of SE in valve dis-ease in daily clinical practice and also suggested expansion ofSE in valve disease beyond that indicated by current guide-lines [17]
Aside from valvular heart disease exercise SE can also beused in patients with hypertrophic cardiomyopathy to revealdynamic left ventricular outflow tract obstruction (Figure 3)[18] Finally myocardial contractile reserve determined bySE can identify those patients that will experience LV reverse
remodelling following cardiac resynchronisation therapy[19]
32 Three-Dimensional Echocardiography Three-dimen-sional (3D) echocardiography is widely perceived as a noveltechnique but the initial work on 3D echocardiography datesback three decades [20 21] However significant technicaladvances have reduced the size of the transducer improvedspeed of image processing and importantly allowed real-time 3D imaging This has been made possible with theadvent of fully sampled matrix array transducer technology[22]
3D-TTE has numerous proven uses in clinical practice Ithas been shown to be superior to 2D-TTE and equal to CMRfor assessment of ventricular volumes [23] cardiacmass [24]and calculation of ejection fraction [25] The latter is espe-cially useful clinically in patients that require serial EFassessment (eg cancer patients receiving chemotherapeuticagents with potential cardiotoxicity) as 2D-TTE can sufferfrom underestimation of true volumes due to chamber fore-shortening 3D-TTE has also been used to assess ventricularmechanical dyssynchrony [26] and of clinical relevancedyssynchronydemonstrated by real-time 3D-TTE canpredictlong-term response to cardiac resynchronization therapy[27] 3D-TTE has also been proved to be valuable in assess-ment of valvular heart diseasemdashit can provide information
BioMed Research International 5
(a) (b)
(c)
Figure 3 A 47-year-old man with hypertrophic cardiomyopathy underwent exercise SE At rest peak gradient across the aortic valve was12mmHg (panel (a)) Repeat assessment during a held Valsalva manoeuvre revealed that the peak gradient was now 63mmHg (panel (b))which indicates that exercise-induced LVOTobstruction is highly likelyThis was indeed confirmed that at peak stress themaximumgradienthad increased to 135mmHg (panel (c)) Note the late systolic peaking of the Doppler profile in panels (b) and (c) indicative of dynamic ratherthan fixed outflow tract obstruction The patient was commenced on beta-blocker therapy following the test results
previously only easily determined by TOE (eg mitral valvescallop assessment in mitral regurgitation) The accuracy ofcalculation of aortic valve area in aortic stenosis has also beenshown to be improved by using 3D-TTE due to more preciseassessment of outflow tract dimensions [28]
The most significant advance however has been in3D-TOE [29] Real-time 3D zoom and live 3D imaging pro-vide unique views of the heart and allow superior detection ofpathology especially valvular diseases 3D echocardiographyis most valuable in cases of complex pathology A simple P2prolapse of the mitral valve is usually evident from 2D imag-ing but a combination of flail scallop(s) and prolapse +minuschordal rupture may be more challenging on 2D and anyconfusion is usually dispelled with 3D imaging As discussedin the following the feasibility of real-time 3D-TOEhasmadeit an essential adjunct in guiding invasive procedures in thecatheter laboratory also
33 Deformation Imaging ldquoMyocardial Mechanicsrdquo Thecomplex orientation of myocardial fibresmdashradial circumfer-ential and longitudinalmdashhas been recognised for a long timeThe theory that tissue motion as opposed to endocardial
excursion is important in assessment ventricular function isalso not newmdashM-mode echocardiography was used to relatemyocardial velocity to ventricular function in the 1970s [30]
Tissue Doppler imaging (TDI) and speckle trackingechocardiography (STE) are techniques that permit detailedanalysis of regional as well as global cardiac function throughunique temporal and spatial data processing TDI deliberatelyfilters out the low amplitude high frequency signals from theblood-pool in order to allow analysis of the high amplitudeand low frequency signals frommyocardium itself [31] TDI ismost frequently used to assist in determining diastolic func-tion and LV filling pressures by means of the 1198641198641015840 ratio [32](where 1198641015840 is the early motion of the mitral annulus backtowards the cardiac base from the apex) The longitudinalfunction of both ventricles is also assessed with TDI where 1198781015840represents the peak systolic velocity of the left or right ventri-cle These parameters have become routine measurements inclinical practice due to a combination of their reproducibilityand diagnostic and prognostic importance
STE is based on the principle of following (or tracking)the unique ldquospeckle patternrdquo of amyocardial segment throughthe cardiac cycle (see Figure 4) One advantage of STE is that
6 BioMed Research International
(a) (b)
(c) (d)
Figure 4 Examples of strain imaging using speckle tracking echocardiography On the top row are images from a normal healthy volunteer(apical 4-chamber view on the left and summary strain scores with bulls-eye plot on the right) and on the bottom row are correspondingimages from a patient with severe ischaemic cardiomyopathy Note that the healthy volunteer has normal longitudinal strain in all segmentswith a global strain score of minus189 whereas the cardiomyopathy patient has highly abnormal strains with a significantly depressed globalstrain score of just minus50
it removes the possibility of falsely designating myocardiumas having normal function when ldquovelocityrdquo is in fact due totethering (eg adjacent scar) or translational motion due tomovement of the whole heart (both potential limitations ofTDI [33]) BothTDI and STE can be used tomeasuremyocar-dial strain a dimensionless quantity defined as the unitchange in length of an object relative to its original lengthStrain rate is its derivative with respect to time (ie rate ofchange of strain and usually expressed as 1sec (or secminus1)) Innormal myocardial segments there is shortening in systole(negative strain and strain rates) and lengthening in diastole(positive strain and strain rates) as cardiomyocytes return totheir resting state [33]
A wealth of data has been accumulated on the potentialclinical value of strain and strain rate assessment in a numberof cardiac diseases [34] Normal ranges have also beendefined [35] STE-derived strain imaging has been shownto have additive benefit for detection of CAD in patientsundergoing dobutamine SE [36] and the superior ability ofstrain imaging to predict outcome in patients undergoingdobutamine SE has also been shown [37] Strain imaging is anaccurate technique for detecting viablemyocardium particu-larly when strain parameters are assessed at rest and followinglow-dose dobutamine SE [38 39] Strain imaging has alsobeen studied extensively for detecting dyssynchrony and thuspredicting response to cardiac resynchronisation therapy[40] Recently it was shown that targeted placement of the LVpacing lead to the site of latest mechanical activationmdashaselucidated by STEmdashwas associated with favourable reverseremodelling fewer repeat hospitalizations and improvedfunctional capacity compared to patients with standard
placement of LV leads [41] TDI can also be used to assesscardiac dyssynchrony This has become a controversial topichowever as the PROSPECT trial [42] suggested no echocar-diographic parameter(s) could accurately predict favourableresponse to biventricular pacing though numerous author-ities worldwide were quick to highlight surprisingly funda-mental flaws in the trialrsquos methodology [43]
Potentially of great clinical relevance is the fact that STEcan reveal subclinical LV dysfunction in hearts with appar-ently normal systolic function as measured by EF and thuscould have a role in detecting cardiac involvement in systemicdiseases [44] unusual or rare conditions [45] and also fordetecting early evidence of cardiotoxicity in cancer patientsreceiving chemotherapy [46] At present strain and strainrate imaging remains predominantly research tools but showsconsiderable promise for translation into clinical practiceThe limitations of STE include the requirement of goodimage quality and variability between different software andhardware manufacturers
34 Contrast Echocardiography Ultrasound contrast agents(UCAs) consist of gas-filled microspheres which displayunique acoustic properties when exposed to ultrasoundwaves Contrast bubbles resonate when exposed to an ultra-sound wave This is predominantly a nonlinear oscillation(ie expansion and contraction of the bubble are not equal)at the ultrasound frequencies used in diagnostic imagingMicrobubbles are several million times more effective atscattering sound than red blood cells resulting in a greatlyenhanced ldquoblood poolrdquo signal [47] The blood pool agents
BioMed Research International 7
(a) (b)
(c) (d)Figure 5 Apical 4-chamber images taken before ((a) and (b)) and after ((c) and (d)) ultrasound contrast injection in a patient attending forroutine transthoracic echocardiography At rest endocardial definition at end diastole (a) and end systole (b) was poor and did not permitquantitation of ejection fraction or assessment of regional (segmental) function Following a single bolus injection of contrast endocardialborder visualisation was significantly improved at end diastole (c) and end systole (d) allowing regional and global systolic assessments
developed consist of a gaseous material encapsulated withina stabilizing outer shell These microbubbles are typicallyslightly smaller than erythrocytes allowing free passagewithin the circulation and effectively acting as red cell tracers[48]
The first generation UCAs consisted of air surrounded byan albumin shell [49] Unfortunately these agents had a veryshort lifespan in vivo and thus had limited utility in diagnostictests The second generation of UCAs addressed this issueby changing both components of microbubblesmdashthe air wasreplaced by inert gases with high molecular weight highdensity and low solubility such as sulphur hexafluoride(SonoVue) or perfluorocarbons (eg Optison or Definity)The outer shell is now made using phospholipids which also
confer greater stability They are used to produce a strongerultrasonic signal than that generated by tissues and thus aremost commonly used to improve image quality (Figure 5)
There is ample evidence demonstrating that UCAsimprove estimation of global [50] and regional [51] LV sys-tolic functions UCAs improve the accuracy of measurementof LV volumes and ejection fraction also [52 53] As UCAsimprove overall image quality they also help detect structuralabnormalities such as noncompaction cardiomyopathy [54]apical hypertrophic cardiomyopathy [55] and left ventric-ular thrombus [56] Their biggest use however is in stressechocardiography The use of contrast significantly reducesthe number of ldquouninterpretablerdquo studies [7] and thus is cost-effective as it reduces additional testing [57] This has helped
8 BioMed Research International
establish stress echocardiography as a front-line investigationin assessment of patients with known or suspected coronaryartery disease
The majority (90) of the blood within the myocardialwalls reside within capillaries [58] Thus the intensity of thecontrast signal when the myocardium is fully saturated withcontrast reflects the concentration of microbubbles withinmyocardial capillaries [59] and consequently capillary ormyocardial blood volume Appreciation of this fact led to therecognition that echocardiography could be used to assessmyocardial perfusion a technique now known as myocardialcontrast echocardiography (MCE) A high intensity (highmechanical index) ldquoflashrdquo or impulse is used to destroy themicrobubbles in the myocardial capillaries and their rate ofreplenishment is observed Delayed replenishment manifestsas a perfusion defect and is the hallmark of ischaemia duringMCE The first papers on MCE dates back to three decades[60 61] and since then it has accumulated a large evidencebase to support its use in the detection of CAD [62] Finallyas presence of contrast denotes vascularity UCAs can also beused in patients with intracardiac masses in order to distin-guish between avascularmasses (eg thrombus) and vascularmasses such as tumours [63]
4 lsquolsquoInterventional Echocardiologyrsquorsquo Dawn ofa New Super-Specialty
The advances in 3D echocardiographymdashin particular theadvent of a fully sampled matrix array transducer allowingreal-time 3D-TOEmdashhas brought the echocardiologist to theforefront of catheter-lab-based procedures in structural heartdisease Real-time 3D-TOE is now considered bymany a pre-requisite for guidance of percutaneous treatment of aorticstenosis (transcatheter aortic valve implantation (TAVI))mitral regurgitation (eg MitraClip devices) closure of theleft atrial appendage and of atrial septal defects (ASDs andPFOs) The incremental value of 3D-TOE over 2D-TOEduring TAVI procedures was recently demonstrated in alarge single-centre study [64] Indeed real-time 3D-TOE isexpanding its use further and for example has been usedto guide electrophysiological procedures such as ablation ofatrial flutter and fibrillation (helping reduce significantly theuse of fluoroscopy) [65]
Intracardiac echocardiography (ICE) performed in thecatheter laboratory using single-use percutaneous 2D probesintroduced transvenously (eg via the femoral vein) is alsowidely used to guide interventions [66] Its biggest advantageover TOE is the ability to obtain similar echo views withoutthe need for general anaesthesia with its attendant costs andpotential risks Therefore ICE has been used in preference toTOE for a number of procedures including atrial fibrillation[67] and ventricular tachycardia [68] ablation proceduresclosure of septal defects [69] TAVI procedures [70] and toguide CRT procedures [71] However the significant limita-tion of ICE is expensive given that the probes must be dis-posed of after a single use
The echocardiologist performing such studies needs tohave a sound grasp of normal cardiac and valvular anatomy
and combine quick thinking with speedy manual dexterityThis skill set is not necessarily acquired during conventionaltraining Heshe may be called upon to provide urgent infor-mation in case of sudden unexplained patient deterioration(eg sudden hypotension during TAVI due to entanglementof the delivery system in the mitral subvalvular apparatuscausing acute severe mitral regurgitation) The need for suchindividuals is likely to be restricted to tertiary units butin large centres one can imagine such a person spendinga significant amount of time in the cardiac catheter lab-oratories Appropriate training will be required to ensurethat we produce cardiologists capable of performing suchstudiesmdashhence one can envisage the birth of a super-special-ity of ldquointerventional echocardiologyrdquo
5 Limitations
Echocardiography does have certain limitations which meritdiscussionThe greatest advantage of cross-sectional imaging(ie CMR and CCT) over echocardiography is the informa-tion available on extracardiac structures The aorta aorticarch pulmonary artery and pulmonary veins are far moreclearly seen by these modalities and are often poorly seen ornot seen at all by echocardiography Thus assessment of pul-monary veins in patients awaiting an atrial fibrillation abla-tion procedure assessment of the aortic arch and descendingthoracic aorta in patients with chronic aortic dissection orcoarctation and serial assessment of patients with previouscoarctation repair for example will generally be performedby CMR or CCT
Echocardiography can also suffer from poor image qual-ity despite the use of ultrasound contrast agentsThis is mostoften seen in patientswho are extremely underweight or over-weight but also in patients with chronic airways disease orchest wall deformities (eg pectus excavatum) Patients onintensive care units who are frequently supine and may bemechanically ventilated also often have challenging TTEimages although TOE can resolve such difficulties
6 Conclusion
Echocardiography permits accurate assessment of myocar-dial structure function and perfusion Echocardiography isthus in itself a multimodality imaging technique The fieldof echocardiography is diverse and encompasses numerousindividual techniquesmdashsome with established clinical valuewhilst others showmuch promise in researchThe expandingrole of echocardiography within current clinical practice isunderpinned by continual technological advances and justi-fied by the accumulating evidence of clinical value of thesetechniques when utilised in daily practice
References
[1] L J Shaw T HMarwickW A Zoghbi et al ldquoWhy all the focuson cardiac imagingrdquo JACC Cardiovascular Imaging vol 3 no7 pp 789ndash794 2010
[2] F A Flachskampf L Badano W G Daniel et al ldquoRecommen-dations for transoesophageal echocardiography update 2010rdquo
BioMed Research International 9
European Journal of Echocardiography vol 11 no 7 pp 557ndash5762010
[3] W G Daniel R ErbelW Kasper et al ldquoSafety of transesophag-eal echocardiography A multicenter survey of 10419 examina-tionsrdquo Circulation vol 83 no 3 pp 817ndash821 1991
[4] J N Hilberath D A Oakes S K Shernan B E Bulwer M NDrsquoAmbra and H K Eltzschig ldquoSafety of transesophageal echo-cardiographyrdquo Journal of the American Society of Echocardiog-raphy vol 23 no 11 pp 1115ndash1127 2010
[5] D G Skolnick S G Sawada H Feigenbaum and D S SegarldquoEnhanced endocardial visualization with noncontrast har-monic imaging during stress echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 12 no 7 pp 559ndash5631999
[6] F B Sozzi D Poldermans J J Bax et al ldquoSecond harmonicimaging improves sensitivity of dobutamine stress echocar-diography for the diagnosis of coronary artery diseaserdquo TheAmerican Heart Journal vol 142 no 1 pp 153ndash159 2001
[7] J C Plana I A Mikati H Dokainish et al ldquoA randomizedcross-over study for evaluation of the effect of image optimiza-tion with contrast on the diagnostic accuracy of dobutamineechocardiography in coronary artery disease The OPTIMIZEtrialrdquo JACC Cardiovascular Imaging vol 1 no 2 pp 145ndash1522008
[8] J S Skinner L Smeeth J M Kendall P C Adams and ATimmis ldquoNICE guidance Chest pain of recent onset assess-ment and diagnosis of recent onset chest pain or discomfort ofsuspected cardiac originrdquo Heart vol 96 no 12 pp 974ndash9782010
[9] P Jeetley L Burden B Stoykova and R Senior ldquoClinical andeconomic impact of stress echocardiography compared withexercise electrocardiography in patients with suspected acutecoronary syndrome but negative troponin a prospective ran-domized controlled studyrdquo European Heart Journal vol 28 no2 pp 204ndash211 2007
[10] BN ShahG Balaji A Alhajiri I S Ramzy S Ahmadvazir andR Senior ldquoThe incremental diagnostic and prognostic valueof contemporary stress echocardiography in a chest pain unitmortality and morbidity outcomes from a real-world settingrdquoCirculation Cardiovascular Imaging vol 6 no 2 pp 202ndash2092013
[11] P Lancellotti F LeboisM Simon C Tombeux C Chauvel andL A Pierard ldquoPrognostic importance of quantitative exerciseDoppler echocardiography in asymptomatic valvular aorticstenosisrdquo Circulation vol 112 no 9 supplement pp I377ndashI3822005
[12] S Marechaux Z Hachicha A Bellouin et al ldquoUsefulness ofexercise-stress echocardiography for risk stratification of trueasymptomatic patients with aortic valve stenosisrdquo EuropeanHeart Journal vol 31 no 11 pp 1390ndash1397 2010
[13] P Lancellotti J Magne E Donal et al ldquoDeterminants andprognostic significance of exercise pulmonary hypertension inasymptomatic severe aortic stenosisrdquoCirculation vol 126 no 7pp 851ndash859 2012
[14] JMonin JQuereMMonchi et al ldquoLow-gradient aortic steno-sis Operative risk stratification and predictors for long-termoutcome a multicenter study using dobutamine stress hemo-dynamicsrdquo Circulation vol 108 no 3 pp 319ndash324 2003
[15] L A Pierard and P Lancellotti ldquoThe role of ischemic mitralregurgitation in the pathogenesis of acute pulmonary edemardquoThe New England Journal of Medicine vol 351 no 16 pp 1627ndash1634 2004
[16] J Magne P Lancellotti and L A Pierard ldquoExercise-inducedchanges in degenerative mitral regurgitationrdquo Journal of theAmericanCollege of Cardiology vol 56 no 4 pp 300ndash309 2010
[17] S Bhattacharyya V Kamperidis B N Shah et al ldquo152 Clinicalutility and prognostic value of appropriateness criteria in stressechocardiography for evaluation of valvular heart diseaserdquoHeart vol 99 pp A89ndashA90 2013
[18] B J Gersh B J Maron R O Bonow et al ldquo2011 ACCFAHAguideline for the diagnosis and treatment of hypertrophic cardi-omyopathyrdquo Journal of the American College of Cardiology vol58 no 25 pp e212ndashe260 2011
[19] P Lancellotti M Senechal M Moonen et al ldquoMyocardial con-tractile reserve during exercise predicts left ventricular reverseremodelling after cardiac resynchronization therapyrdquo Euro-pean Journal of Echocardiography vol 10 no 5 pp 663ndash6682009
[20] M Matsumoto M Inoue S Tamura K Tanaka and H AbeldquoThree-dimensional echocardiography for spatial visualizationand volume calculation of cardiac structuresrdquo Journal of ClinicalUltrasound vol 9 no 4 pp 157ndash165 1981
[21] K H Sheikh S W Smith O von Ramm and J Kisslo ldquoReal-time three-dimensional echocardiography feasibility and ini-tial userdquo Echocardiography vol 8 no 1 pp 119ndash125 1991
[22] L Sugeng L Weinert K Thiele and R M Lang ldquoReal-timethree-dimensional echocardiography using a novelmatrix arraytransducerrdquo Echocardiography vol 20 no 7 pp 623ndash635 2003
[23] N P Nikitin C Constantin P H Loh et al ldquoNew generation3-dimensional echocardiography for left ventricular volumetricand functional measurements comparison with cardiac mag-netic resonancerdquo European Journal of Echocardiography vol 7no 5 pp 365ndash372 2006
[24] V Mor-Avi L Sugeng L Weinert et al ldquoFast measurement ofleft ventricular mass with real-time three-dimensional echocar-diography comparison withmagnetic resonance imagingrdquoCir-culation vol 110 no 13 pp 1814ndash1818 2004
[25] L Sugeng V Mor-Avi L Weinert et al ldquoQuantitative assess-ment of left ventricular size and function side-by-side compari-son of real-time three-dimensional echocardiography and com-puted tomography with magnetic resonance referencerdquo Cir-culation vol 114 no 7 pp 654ndash661 2006
[26] S Kapetanakis M T Kearney A Siva N Gall M Cooklinand M J Monaghan ldquoReal-time three-dimensional echocar-diography a novel technique to quantify global left ventricularmechanical dyssynchronyrdquo Circulation vol 112 no 7 pp 992ndash1000 2005
[27] O I I Soliman M L Geleijnse D A M J Theuns et alldquoUsefulness of left ventricular systolic dyssynchrony by real-time three-dimensional echocardiography to predict long-termresponse to cardiac resynchronization therapyrdquo The AmericanJournal of Cardiology vol 103 no 11 pp 1586ndash1591 2009
[28] A V Khaw R S von Bardeleben C Strasser et al ldquoDirect mea-surement of left ventricular outflow tract by transthoracic real-time 3D-echocardiography increases accuracy in assessment ofaortic valve stenosisrdquo International Journal of Cardiology vol136 no 1 pp 64ndash71 2009
[29] L Sugeng S K Shernan I S Salgo et al ldquoLive 3-dimensionaltransesophageal echocardiography Initial experience using thefully-sampled matrix array proberdquo Journal of the American Col-lege of Cardiology vol 52 no 6 pp 446ndash449 2008
[30] D G Gibson T A Prewitt and D J Brown ldquoAnalysis of leftventricular wall movement during isovolumic relaxation and its
10 BioMed Research International
relation to coronary artery diseaserdquo The British Heart Journalvol 38 no 10 pp 1010ndash1019 1976
[31] P Palka A Lange A D Fleming G R Sutherland L N FeenandW NMcDicken ldquoDoppler tissue imaging myocardial wallmotion velocities in normal subjectsrdquo Journal of the AmericanSociety of Echocardiography vol 8 no 5 pp 659ndash668 1995
[32] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressures acomparative simultaneous Doppler-catheterization studyrdquo Cir-culation vol 102 no 15 pp 1788ndash1794 2000
[33] H Blessberger and T Binder ldquoTwo dimensional speckle track-ing echocardiography basic principlesrdquoHeart vol 96 no 9 pp716ndash722 2010
[34] J Gorcsan III and H Tanaka ldquoEchocardiographic assessmentof myocardial strainrdquo Journal of the American College of Cardi-ology vol 58 no 14 pp 1401ndash1413 2011
[35] T H Marwick R L Leano J Brown et al ldquoMyocardial strainmeasurement with 2-dimensional speckle-tracking echocardi-ography Definition of normal rangerdquo JACC CardiovascularImaging vol 2 no 1 pp 80ndash84 2009
[36] A C T Ng M Sitges P N Pham et al ldquoIncrementalvalue of 2-dimensional speckle tracking strain imaging to wallmotion analysis for detection of coronary artery disease inpatients undergoing dobutamine stress echocardiographyrdquoTheAmerican Heart Journal vol 158 no 5 pp 836ndash844 2009
[37] C B Ingul E Rozis S A Slordahl and T H Marwick ldquoIncre-mental value of strain rate imaging to wall motion analysisfor prediction of outcome in patients undergoing dobutaminestress echocardiographyrdquo Circulation vol 115 no 10 pp 1252ndash1259 2007
[38] R Hoffmann E Altiok B Nowak et al ldquoStrain rate measure-ment by Doppler echocardiography allows improved assess-ment of myocardial viability in patients with depressed left ven-tricular functionrdquo Journal of the American College of Cardiologyvol 39 no 3 pp 443ndash449 2002
[39] L Hanekom C Jenkins L Jeffries et al ldquoIncremental valueof strain rate analysis as an adjunct to wall-motion scoring forassessment of myocardial viability by dobutamine echocardio-graphy a follow-up study after revascularizationrdquo Circulationvol 112 no 25 pp 3892ndash3900 2005
[40] H Tanaka H Nesser T Buck et al ldquoDyssynchrony by speckle-tracking echocardiography and response to cardiac resynchro-nization therapy results of the speckle tracking and resynchro-nization (STAR) studyrdquo European Heart Journal vol 31 no 14pp 1690ndash1700 2010
[41] F Z Khan M S Virdee C R Palmer et al ldquoTargeted leftventricular lead placement to guide cardiac resynchronizationtherapy the TARGET study a randomized controlled trialrdquoJournal of the American College of Cardiology vol 59 no 17 pp1509ndash1518 2012
[42] E S Chung A R Leon L Tavazzi et al ldquoResults of the predic-tors of response to CRT (PROSPECT) trialrdquoCirculation vol 117no 20 pp 2608ndash2616 2008
[43] J J Bax and J Gorcsan III ldquoEchocardiography and noninvasiveimaging in cardiac resynchronization therapy Results of thePROSPECT (predictors of response to cardiac resynchroniza-tion therapy) study in perspectiverdquo Journal of the American Col-lege of Cardiology vol 53 no 21 pp 1933ndash1943 2009
[44] B N Shah M de Villa R S Khattar and R Senior ldquoImagingcardiac sarcoidosis the incremental benefit of speckle trackingechocardiographyrdquo Echocardiography 2013
[45] J KramerM Niemann D Liu et al ldquoTwo-dimensional speckletracking as a non-invasive tool for identification of myocardialfibrosis in Fabry diseaserdquoEuropeanHeart Journal vol 34 no 21pp 1587ndash1596 2013
[46] J L Hare J K Brown R Leano C Jenkins N Woodwardand T H Marwick ldquoUse of myocardial deformation imaging todetect preclinical myocardial dysfunction before conventionalmeasures in patients undergoing breast cancer treatment withtrastuzumabrdquo The American Heart Journal vol 158 no 2 pp294ndash301 2009
[47] M J Stewart ldquoContrast echocardiographyrdquoHeart vol 89 no 3pp 342ndash348 2003
[48] R Janardhanan G Dwivedi S Hayat and R Senior ldquoMyocar-dial contrast echocardiography a new tool for assessment ofmyocardial perfusionrdquo Indian Heart Journal vol 57 no 3 pp210ndash216 2005
[49] S B Feinstein F J T Cate W Zwehl et al ldquoTwo-dimensionalcontrast echocardiography I In vitro development and quanti-tative analysis of echo contrast agentsrdquo Journal of the AmericanCollege of Cardiology vol 3 no 1 pp 14ndash20 1984
[50] R Hoffmann S von Bardeleben F T Cate et al ldquoAssessmentof systolic left ventricular function a multi-centre comparisonof cineventriculography cardiac magnetic resonance imagingunenhanced and contrast-enhanced echocardiographyrdquo Euro-pean Heart Journal vol 26 no 6 pp 607ndash616 2005
[51] R Hoffmann S von Bardeleben J D Kasprzak et al ldquoAnalysisof regional left ventricular function by cineventriculographycardiac magnetic resonance imaging and unenhanced andcontrast-enhanced echocardiography a multicenter compari-son of methodsrdquo Journal of the American College of Cardiologyvol 47 no 1 pp 121ndash128 2006
[52] W G Hundley A M Kizilbash I Afridi F Franco R MPeshock and P A Grayburn ldquoAdministration of an intravenousperfluorocarbon contrast agent improves echocardiographicdetermination of left ventricular volumes and ejection fractioncomparison with cine magnetic resonance imagingrdquo Journal ofthe American College of Cardiology vol 32 no 5 pp 1426ndash14321998
[53] S Malm S Frigstad E Sagberg H Larsson and T SkjaerpeldquoAccurate and reproducible measurement of left ventricularvolume and ejection fraction by contrast echocardiography acomparison with magnetic resonance imagingrdquo Journal of theAmerican College of Cardiology vol 44 no 5 pp 1030ndash10352004
[54] B K Koo D Choi J W Ha S M Kang N Chung and S YCho ldquoIsolated noncompaction of the ventricular myocardiumcontrast echocardiographic findings and review of the litera-turerdquo Echocardiography vol 19 no 2 pp 153ndash156 2002
[55] P Soman J Swinburn M Callister N G Stephens and RSenior ldquoApical hypertrophic cardiomyopathy bedside diagno-sis by intravenous contrast echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 14 no 4 pp 311ndash3132001
[56] S Thanigaraj K B Schechtman and J E Perez ldquoImprovedechocardiographic delineation of left ventricular thrombuswith the use of intravenous second-generation contrast imageenhancementrdquo Journal of the American Society of Echocardiog-raphy vol 12 no 12 pp 1022ndash1026 1999
[57] S Thanigaraj R F Nease Jr K B Schechtman R L Wade SLoslo and J E Perez ldquoUse of contrast for image enhancementduring stress echocardiography is cost-effective and reduces
BioMed Research International 11
additional diagnostic testingrdquo The American Journal of Cardi-ology vol 87 no 12 pp 1430ndash1432 2001
[58] S Kaul and A R Jayaweera ldquoCoronary and myocardial bloodvolumes noninvasive tools to assess the coronary microcircu-lationrdquo Circulation vol 96 no 3 pp 719ndash724 1997
[59] K Wei A R Jayaweera S Firoozan A Linka D M Skybaand S Kaul ldquoBasis for detection of stenosis using venousadministration of microbubbles during myocardial contrastechocardiography bolus or continuous infusionrdquo Journal of theAmeri-canCollege of Cardiology vol 32 no 1 pp 252ndash260 1998
[60] W F Armstrong T M Mueller E L Kinney E G Tickner JC Dillon and H Feigenbaum ldquoAssessment of myocardial per-fusion abnormalities with contrast-enhanced two-dimensionalechocardiographyrdquo Circulation vol 66 no 1 pp 166ndash173 1982
[61] C Tei T Sakamaki PM Shah et al ldquoMyocardial contrast echo-cardiography a reproducible technique of myocardial opacifi-cation for identifying regional perfusion deficitsrdquo Circulationvol 67 no 3 pp 585ndash593 1983
[62] R Senior H BecherMMonaghan et al ldquoContrast echocardio-graphy evidence-based recommendations by european associ-ation of echocardiographyrdquo European Journal of Echocardiogra-phy vol 10 no 2 pp 194ndash212 2009
[63] S Bhattacharyya R Khattar andR Senior ldquoCharacterisation ofintra-cardiacmasses bymyocardial contrast echocardiographyrdquoInternational Journal of Cardiology vol 163 no 1 pp e11ndashe132013
[64] L A Smith R Dworakowski A Bhan et al ldquoReal-time three-dimensional transesophageal echocardiography adds value totranscatheter aortic valve implantationrdquo Journal of theAmericanSociety of Echocardiography vol 26 no 4 pp 359ndash369 2013
[65] F Regoli F F Faletra G Nucifora et al ldquoFeasibility and acuteefficacy of radiofrequency ablation of cavotricuspid isthmus-dependent atrial flutter guided by real-time 3D TEErdquo JACCCardiovascular Imaging vol 4 no 7 pp 716ndash726 2011
[66] S S Kim ZM Hijazi R M Lang and B P Knight ldquoThe use ofintracardiac echocardiography and other intracardiac imagingtools to guide noncoronary cardiac interventionsrdquo Journal of theAmerican College of Cardiology vol 53 no 23 pp 2117ndash21282009
[67] JMMangrum J PMounsey L C Kok J P DiMarco andD EHaines ldquoIntracardiac echocardiography-guided anatomicallybased radiofrequency ablation of focal atrial fibrillation origi-nating from pulmonary veinsrdquo Journal of the American Collegeof Cardiology vol 39 no 12 pp 1964ndash1972 2002
[68] R Bala J F Ren M D Hutchinson et al ldquoAssessing epicardialsubstrate using intracardiac echocardiography during VT abla-tionrdquo Circulation Arrhythmia and Electrophysiology vol 4 no5 pp 667ndash673 2011
[69] C Vigna N Marchese M Zanchetta et al ldquoEchocardio-graphic guidance of percutaneous patent foramen ovale closurehead-to-head comparison of transesophageal versus rotationalintracardiac echocardiographyrdquo Echocardiography vol 29 no9 pp 1103ndash1110 2012
[70] T Bartel N Bonaros L Muller et al ldquoIntracardiac echocar-diography a new guiding tool for transcatheter aortic valvereplacementrdquo Journal of the American Society of Echocardiog-raphy vol 24 no 9 pp 966ndash975 2011
[71] R Bai L Di Biase P Mohanty et al ldquoPositioning of left ventric-ular pacing lead guided by intracardiac echocardiography withvector velocity imaging during cardiac resynchronization ther-apy procedurerdquo Journal of Cardiovascular Electrophysiology vol22 no 9 pp 1034ndash1041 2011

BioMed Research International 3
LV
RALA
(a)
Ao
LA
LV
(b)
AoV
(c) (d)
Figure 1 A patient with previousmitral valve repair attendedwith increasing breathlessness 2D-TTE revealed two jets ofmitral regurgitation(panel (a)) 2D-TOE suggested the presence of a paravalvular leak (panel (b) see arrows) Three-dimensional TOE revealed dehiscence ofthe posterior aspect of the mitral annuloplasty ring (panel (c) see arrow) and real-time 3D colour during TOE confirmed the presence ofa reguritant jet (arrow) through this defect (panel (d)) The patient subsequently underwent redo mitral valve surgery (LA left atrium RAright atrium LV left ventricle Ao aorta AoV aortic valve)
Table 2 Contemporary indications for stress echocardiography
Indication Parameter(s) measuredCoronary applications
Myocardial ischaemia Wall thickening at rest versus stressMyocardial viability Wall thickening at rest low-dose and peak stress
Noncoronary applications(A) Valve disease
Asymptomatic severe AS Exercise-induced change in mean transaortic gradientExercise-induced change in peak transtricuspid gradient
Low-flow low-gradient AS LVOT and AoV VTI at rest and low-dose dobutamine stressSymptomatic mildmoderate MS Exercise-induced change in mean transmitral and transtricuspid gradientsSymptomatic moderate MR Exercise-induced changes in EROA and pulmonary pressures
(B) CardiomyopathyHCM Exercise-induced dynamic LVOT obstructionDCM Contractile reserve in response to low-dose dobutamine
ICMAssessment of global LV contractile reserveAssessment of viability in posterolateral walls (for guiding LV lead placement)Assess exercise capacity objectivelyAssess inducibility of tachyarrhythmias
(AS aortic stenosis MS mitral stenosis MR mitral regurgitation LVOT left ventricular outflow tract AoV aortic valve EROA effective regurgitant orificearea VTI velocity time integral HCM hypertrophic cardiomyopathy DCM dilated cardiomyopathy ICM ischaemic cardiomyopathy)
4 BioMed Research International
Rest
(a)
Rest
(b)
Stress
(c)
Stress
(d)
Figure 2 A patient with moderate mitral stenosis but worsening exertional dyspnoea underwent exercise SE At rest mean transmitralgradient was 5mmHg (a) and transtricuspid pressure gradient was 24mmHg (b) After 7-minute BRUCE protocol treadmill exercise meantransmitral gradient significantly increased to 27mmHg (c) and transtricuspid pressure gradient had more than doubled to 51mmHg (d)The patient subsequently underwent balloon mitral valvuloplasty with excellent symptomatic relief
Exercise SE is also helpful in certain patients with mitralvalve disease Patients with mitral stenosis (MS) who havesymptoms disproportionate to the degree of MS at rest (egmarked exertional dyspnoea but only moderate MS at rest)should undergo exercise SEmdashan increase inmean transmitralgradient to gt15mmHg or pulmonary artery pressure togt60mmHg is an indication for valve intervention (Figure 2)The dynamic nature of ischaemic mitral regurgitation (MR)was previously shown in a quantitative Doppler echocardio-graphy study using exercise stress in patients with ischaemiccardiomyopathy (ICM) recently admitted with pulmonaryoedema and comparing with ICM patients without pul-monary oedema [15] Patientswith recent pulmonary oedemahad significantly greater increases in MR and pulmonarypressures during exercise than those without pulmonaryoedema The same group has also demonstrated the clinicalvalue of exercise SE in patients with degenerative MR [16] Arecent analysis clearly indicated the value of SE in valve dis-ease in daily clinical practice and also suggested expansion ofSE in valve disease beyond that indicated by current guide-lines [17]
Aside from valvular heart disease exercise SE can also beused in patients with hypertrophic cardiomyopathy to revealdynamic left ventricular outflow tract obstruction (Figure 3)[18] Finally myocardial contractile reserve determined bySE can identify those patients that will experience LV reverse
remodelling following cardiac resynchronisation therapy[19]
32 Three-Dimensional Echocardiography Three-dimen-sional (3D) echocardiography is widely perceived as a noveltechnique but the initial work on 3D echocardiography datesback three decades [20 21] However significant technicaladvances have reduced the size of the transducer improvedspeed of image processing and importantly allowed real-time 3D imaging This has been made possible with theadvent of fully sampled matrix array transducer technology[22]
3D-TTE has numerous proven uses in clinical practice Ithas been shown to be superior to 2D-TTE and equal to CMRfor assessment of ventricular volumes [23] cardiacmass [24]and calculation of ejection fraction [25] The latter is espe-cially useful clinically in patients that require serial EFassessment (eg cancer patients receiving chemotherapeuticagents with potential cardiotoxicity) as 2D-TTE can sufferfrom underestimation of true volumes due to chamber fore-shortening 3D-TTE has also been used to assess ventricularmechanical dyssynchrony [26] and of clinical relevancedyssynchronydemonstrated by real-time 3D-TTE canpredictlong-term response to cardiac resynchronization therapy[27] 3D-TTE has also been proved to be valuable in assess-ment of valvular heart diseasemdashit can provide information
BioMed Research International 5
(a) (b)
(c)
Figure 3 A 47-year-old man with hypertrophic cardiomyopathy underwent exercise SE At rest peak gradient across the aortic valve was12mmHg (panel (a)) Repeat assessment during a held Valsalva manoeuvre revealed that the peak gradient was now 63mmHg (panel (b))which indicates that exercise-induced LVOTobstruction is highly likelyThis was indeed confirmed that at peak stress themaximumgradienthad increased to 135mmHg (panel (c)) Note the late systolic peaking of the Doppler profile in panels (b) and (c) indicative of dynamic ratherthan fixed outflow tract obstruction The patient was commenced on beta-blocker therapy following the test results
previously only easily determined by TOE (eg mitral valvescallop assessment in mitral regurgitation) The accuracy ofcalculation of aortic valve area in aortic stenosis has also beenshown to be improved by using 3D-TTE due to more preciseassessment of outflow tract dimensions [28]
The most significant advance however has been in3D-TOE [29] Real-time 3D zoom and live 3D imaging pro-vide unique views of the heart and allow superior detection ofpathology especially valvular diseases 3D echocardiographyis most valuable in cases of complex pathology A simple P2prolapse of the mitral valve is usually evident from 2D imag-ing but a combination of flail scallop(s) and prolapse +minuschordal rupture may be more challenging on 2D and anyconfusion is usually dispelled with 3D imaging As discussedin the following the feasibility of real-time 3D-TOEhasmadeit an essential adjunct in guiding invasive procedures in thecatheter laboratory also
33 Deformation Imaging ldquoMyocardial Mechanicsrdquo Thecomplex orientation of myocardial fibresmdashradial circumfer-ential and longitudinalmdashhas been recognised for a long timeThe theory that tissue motion as opposed to endocardial
excursion is important in assessment ventricular function isalso not newmdashM-mode echocardiography was used to relatemyocardial velocity to ventricular function in the 1970s [30]
Tissue Doppler imaging (TDI) and speckle trackingechocardiography (STE) are techniques that permit detailedanalysis of regional as well as global cardiac function throughunique temporal and spatial data processing TDI deliberatelyfilters out the low amplitude high frequency signals from theblood-pool in order to allow analysis of the high amplitudeand low frequency signals frommyocardium itself [31] TDI ismost frequently used to assist in determining diastolic func-tion and LV filling pressures by means of the 1198641198641015840 ratio [32](where 1198641015840 is the early motion of the mitral annulus backtowards the cardiac base from the apex) The longitudinalfunction of both ventricles is also assessed with TDI where 1198781015840represents the peak systolic velocity of the left or right ventri-cle These parameters have become routine measurements inclinical practice due to a combination of their reproducibilityand diagnostic and prognostic importance
STE is based on the principle of following (or tracking)the unique ldquospeckle patternrdquo of amyocardial segment throughthe cardiac cycle (see Figure 4) One advantage of STE is that
6 BioMed Research International
(a) (b)
(c) (d)
Figure 4 Examples of strain imaging using speckle tracking echocardiography On the top row are images from a normal healthy volunteer(apical 4-chamber view on the left and summary strain scores with bulls-eye plot on the right) and on the bottom row are correspondingimages from a patient with severe ischaemic cardiomyopathy Note that the healthy volunteer has normal longitudinal strain in all segmentswith a global strain score of minus189 whereas the cardiomyopathy patient has highly abnormal strains with a significantly depressed globalstrain score of just minus50
it removes the possibility of falsely designating myocardiumas having normal function when ldquovelocityrdquo is in fact due totethering (eg adjacent scar) or translational motion due tomovement of the whole heart (both potential limitations ofTDI [33]) BothTDI and STE can be used tomeasuremyocar-dial strain a dimensionless quantity defined as the unitchange in length of an object relative to its original lengthStrain rate is its derivative with respect to time (ie rate ofchange of strain and usually expressed as 1sec (or secminus1)) Innormal myocardial segments there is shortening in systole(negative strain and strain rates) and lengthening in diastole(positive strain and strain rates) as cardiomyocytes return totheir resting state [33]
A wealth of data has been accumulated on the potentialclinical value of strain and strain rate assessment in a numberof cardiac diseases [34] Normal ranges have also beendefined [35] STE-derived strain imaging has been shownto have additive benefit for detection of CAD in patientsundergoing dobutamine SE [36] and the superior ability ofstrain imaging to predict outcome in patients undergoingdobutamine SE has also been shown [37] Strain imaging is anaccurate technique for detecting viablemyocardium particu-larly when strain parameters are assessed at rest and followinglow-dose dobutamine SE [38 39] Strain imaging has alsobeen studied extensively for detecting dyssynchrony and thuspredicting response to cardiac resynchronisation therapy[40] Recently it was shown that targeted placement of the LVpacing lead to the site of latest mechanical activationmdashaselucidated by STEmdashwas associated with favourable reverseremodelling fewer repeat hospitalizations and improvedfunctional capacity compared to patients with standard
placement of LV leads [41] TDI can also be used to assesscardiac dyssynchrony This has become a controversial topichowever as the PROSPECT trial [42] suggested no echocar-diographic parameter(s) could accurately predict favourableresponse to biventricular pacing though numerous author-ities worldwide were quick to highlight surprisingly funda-mental flaws in the trialrsquos methodology [43]
Potentially of great clinical relevance is the fact that STEcan reveal subclinical LV dysfunction in hearts with appar-ently normal systolic function as measured by EF and thuscould have a role in detecting cardiac involvement in systemicdiseases [44] unusual or rare conditions [45] and also fordetecting early evidence of cardiotoxicity in cancer patientsreceiving chemotherapy [46] At present strain and strainrate imaging remains predominantly research tools but showsconsiderable promise for translation into clinical practiceThe limitations of STE include the requirement of goodimage quality and variability between different software andhardware manufacturers
34 Contrast Echocardiography Ultrasound contrast agents(UCAs) consist of gas-filled microspheres which displayunique acoustic properties when exposed to ultrasoundwaves Contrast bubbles resonate when exposed to an ultra-sound wave This is predominantly a nonlinear oscillation(ie expansion and contraction of the bubble are not equal)at the ultrasound frequencies used in diagnostic imagingMicrobubbles are several million times more effective atscattering sound than red blood cells resulting in a greatlyenhanced ldquoblood poolrdquo signal [47] The blood pool agents
BioMed Research International 7
(a) (b)
(c) (d)Figure 5 Apical 4-chamber images taken before ((a) and (b)) and after ((c) and (d)) ultrasound contrast injection in a patient attending forroutine transthoracic echocardiography At rest endocardial definition at end diastole (a) and end systole (b) was poor and did not permitquantitation of ejection fraction or assessment of regional (segmental) function Following a single bolus injection of contrast endocardialborder visualisation was significantly improved at end diastole (c) and end systole (d) allowing regional and global systolic assessments
developed consist of a gaseous material encapsulated withina stabilizing outer shell These microbubbles are typicallyslightly smaller than erythrocytes allowing free passagewithin the circulation and effectively acting as red cell tracers[48]
The first generation UCAs consisted of air surrounded byan albumin shell [49] Unfortunately these agents had a veryshort lifespan in vivo and thus had limited utility in diagnostictests The second generation of UCAs addressed this issueby changing both components of microbubblesmdashthe air wasreplaced by inert gases with high molecular weight highdensity and low solubility such as sulphur hexafluoride(SonoVue) or perfluorocarbons (eg Optison or Definity)The outer shell is now made using phospholipids which also
confer greater stability They are used to produce a strongerultrasonic signal than that generated by tissues and thus aremost commonly used to improve image quality (Figure 5)
There is ample evidence demonstrating that UCAsimprove estimation of global [50] and regional [51] LV sys-tolic functions UCAs improve the accuracy of measurementof LV volumes and ejection fraction also [52 53] As UCAsimprove overall image quality they also help detect structuralabnormalities such as noncompaction cardiomyopathy [54]apical hypertrophic cardiomyopathy [55] and left ventric-ular thrombus [56] Their biggest use however is in stressechocardiography The use of contrast significantly reducesthe number of ldquouninterpretablerdquo studies [7] and thus is cost-effective as it reduces additional testing [57] This has helped
8 BioMed Research International
establish stress echocardiography as a front-line investigationin assessment of patients with known or suspected coronaryartery disease
The majority (90) of the blood within the myocardialwalls reside within capillaries [58] Thus the intensity of thecontrast signal when the myocardium is fully saturated withcontrast reflects the concentration of microbubbles withinmyocardial capillaries [59] and consequently capillary ormyocardial blood volume Appreciation of this fact led to therecognition that echocardiography could be used to assessmyocardial perfusion a technique now known as myocardialcontrast echocardiography (MCE) A high intensity (highmechanical index) ldquoflashrdquo or impulse is used to destroy themicrobubbles in the myocardial capillaries and their rate ofreplenishment is observed Delayed replenishment manifestsas a perfusion defect and is the hallmark of ischaemia duringMCE The first papers on MCE dates back to three decades[60 61] and since then it has accumulated a large evidencebase to support its use in the detection of CAD [62] Finallyas presence of contrast denotes vascularity UCAs can also beused in patients with intracardiac masses in order to distin-guish between avascularmasses (eg thrombus) and vascularmasses such as tumours [63]
4 lsquolsquoInterventional Echocardiologyrsquorsquo Dawn ofa New Super-Specialty
The advances in 3D echocardiographymdashin particular theadvent of a fully sampled matrix array transducer allowingreal-time 3D-TOEmdashhas brought the echocardiologist to theforefront of catheter-lab-based procedures in structural heartdisease Real-time 3D-TOE is now considered bymany a pre-requisite for guidance of percutaneous treatment of aorticstenosis (transcatheter aortic valve implantation (TAVI))mitral regurgitation (eg MitraClip devices) closure of theleft atrial appendage and of atrial septal defects (ASDs andPFOs) The incremental value of 3D-TOE over 2D-TOEduring TAVI procedures was recently demonstrated in alarge single-centre study [64] Indeed real-time 3D-TOE isexpanding its use further and for example has been usedto guide electrophysiological procedures such as ablation ofatrial flutter and fibrillation (helping reduce significantly theuse of fluoroscopy) [65]
Intracardiac echocardiography (ICE) performed in thecatheter laboratory using single-use percutaneous 2D probesintroduced transvenously (eg via the femoral vein) is alsowidely used to guide interventions [66] Its biggest advantageover TOE is the ability to obtain similar echo views withoutthe need for general anaesthesia with its attendant costs andpotential risks Therefore ICE has been used in preference toTOE for a number of procedures including atrial fibrillation[67] and ventricular tachycardia [68] ablation proceduresclosure of septal defects [69] TAVI procedures [70] and toguide CRT procedures [71] However the significant limita-tion of ICE is expensive given that the probes must be dis-posed of after a single use
The echocardiologist performing such studies needs tohave a sound grasp of normal cardiac and valvular anatomy
and combine quick thinking with speedy manual dexterityThis skill set is not necessarily acquired during conventionaltraining Heshe may be called upon to provide urgent infor-mation in case of sudden unexplained patient deterioration(eg sudden hypotension during TAVI due to entanglementof the delivery system in the mitral subvalvular apparatuscausing acute severe mitral regurgitation) The need for suchindividuals is likely to be restricted to tertiary units butin large centres one can imagine such a person spendinga significant amount of time in the cardiac catheter lab-oratories Appropriate training will be required to ensurethat we produce cardiologists capable of performing suchstudiesmdashhence one can envisage the birth of a super-special-ity of ldquointerventional echocardiologyrdquo
5 Limitations
Echocardiography does have certain limitations which meritdiscussionThe greatest advantage of cross-sectional imaging(ie CMR and CCT) over echocardiography is the informa-tion available on extracardiac structures The aorta aorticarch pulmonary artery and pulmonary veins are far moreclearly seen by these modalities and are often poorly seen ornot seen at all by echocardiography Thus assessment of pul-monary veins in patients awaiting an atrial fibrillation abla-tion procedure assessment of the aortic arch and descendingthoracic aorta in patients with chronic aortic dissection orcoarctation and serial assessment of patients with previouscoarctation repair for example will generally be performedby CMR or CCT
Echocardiography can also suffer from poor image qual-ity despite the use of ultrasound contrast agentsThis is mostoften seen in patientswho are extremely underweight or over-weight but also in patients with chronic airways disease orchest wall deformities (eg pectus excavatum) Patients onintensive care units who are frequently supine and may bemechanically ventilated also often have challenging TTEimages although TOE can resolve such difficulties
6 Conclusion
Echocardiography permits accurate assessment of myocar-dial structure function and perfusion Echocardiography isthus in itself a multimodality imaging technique The fieldof echocardiography is diverse and encompasses numerousindividual techniquesmdashsome with established clinical valuewhilst others showmuch promise in researchThe expandingrole of echocardiography within current clinical practice isunderpinned by continual technological advances and justi-fied by the accumulating evidence of clinical value of thesetechniques when utilised in daily practice
References
[1] L J Shaw T HMarwickW A Zoghbi et al ldquoWhy all the focuson cardiac imagingrdquo JACC Cardiovascular Imaging vol 3 no7 pp 789ndash794 2010
[2] F A Flachskampf L Badano W G Daniel et al ldquoRecommen-dations for transoesophageal echocardiography update 2010rdquo
BioMed Research International 9
European Journal of Echocardiography vol 11 no 7 pp 557ndash5762010
[3] W G Daniel R ErbelW Kasper et al ldquoSafety of transesophag-eal echocardiography A multicenter survey of 10419 examina-tionsrdquo Circulation vol 83 no 3 pp 817ndash821 1991
[4] J N Hilberath D A Oakes S K Shernan B E Bulwer M NDrsquoAmbra and H K Eltzschig ldquoSafety of transesophageal echo-cardiographyrdquo Journal of the American Society of Echocardiog-raphy vol 23 no 11 pp 1115ndash1127 2010
[5] D G Skolnick S G Sawada H Feigenbaum and D S SegarldquoEnhanced endocardial visualization with noncontrast har-monic imaging during stress echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 12 no 7 pp 559ndash5631999
[6] F B Sozzi D Poldermans J J Bax et al ldquoSecond harmonicimaging improves sensitivity of dobutamine stress echocar-diography for the diagnosis of coronary artery diseaserdquo TheAmerican Heart Journal vol 142 no 1 pp 153ndash159 2001
[7] J C Plana I A Mikati H Dokainish et al ldquoA randomizedcross-over study for evaluation of the effect of image optimiza-tion with contrast on the diagnostic accuracy of dobutamineechocardiography in coronary artery disease The OPTIMIZEtrialrdquo JACC Cardiovascular Imaging vol 1 no 2 pp 145ndash1522008
[8] J S Skinner L Smeeth J M Kendall P C Adams and ATimmis ldquoNICE guidance Chest pain of recent onset assess-ment and diagnosis of recent onset chest pain or discomfort ofsuspected cardiac originrdquo Heart vol 96 no 12 pp 974ndash9782010
[9] P Jeetley L Burden B Stoykova and R Senior ldquoClinical andeconomic impact of stress echocardiography compared withexercise electrocardiography in patients with suspected acutecoronary syndrome but negative troponin a prospective ran-domized controlled studyrdquo European Heart Journal vol 28 no2 pp 204ndash211 2007
[10] BN ShahG Balaji A Alhajiri I S Ramzy S Ahmadvazir andR Senior ldquoThe incremental diagnostic and prognostic valueof contemporary stress echocardiography in a chest pain unitmortality and morbidity outcomes from a real-world settingrdquoCirculation Cardiovascular Imaging vol 6 no 2 pp 202ndash2092013
[11] P Lancellotti F LeboisM Simon C Tombeux C Chauvel andL A Pierard ldquoPrognostic importance of quantitative exerciseDoppler echocardiography in asymptomatic valvular aorticstenosisrdquo Circulation vol 112 no 9 supplement pp I377ndashI3822005
[12] S Marechaux Z Hachicha A Bellouin et al ldquoUsefulness ofexercise-stress echocardiography for risk stratification of trueasymptomatic patients with aortic valve stenosisrdquo EuropeanHeart Journal vol 31 no 11 pp 1390ndash1397 2010
[13] P Lancellotti J Magne E Donal et al ldquoDeterminants andprognostic significance of exercise pulmonary hypertension inasymptomatic severe aortic stenosisrdquoCirculation vol 126 no 7pp 851ndash859 2012
[14] JMonin JQuereMMonchi et al ldquoLow-gradient aortic steno-sis Operative risk stratification and predictors for long-termoutcome a multicenter study using dobutamine stress hemo-dynamicsrdquo Circulation vol 108 no 3 pp 319ndash324 2003
[15] L A Pierard and P Lancellotti ldquoThe role of ischemic mitralregurgitation in the pathogenesis of acute pulmonary edemardquoThe New England Journal of Medicine vol 351 no 16 pp 1627ndash1634 2004
[16] J Magne P Lancellotti and L A Pierard ldquoExercise-inducedchanges in degenerative mitral regurgitationrdquo Journal of theAmericanCollege of Cardiology vol 56 no 4 pp 300ndash309 2010
[17] S Bhattacharyya V Kamperidis B N Shah et al ldquo152 Clinicalutility and prognostic value of appropriateness criteria in stressechocardiography for evaluation of valvular heart diseaserdquoHeart vol 99 pp A89ndashA90 2013
[18] B J Gersh B J Maron R O Bonow et al ldquo2011 ACCFAHAguideline for the diagnosis and treatment of hypertrophic cardi-omyopathyrdquo Journal of the American College of Cardiology vol58 no 25 pp e212ndashe260 2011
[19] P Lancellotti M Senechal M Moonen et al ldquoMyocardial con-tractile reserve during exercise predicts left ventricular reverseremodelling after cardiac resynchronization therapyrdquo Euro-pean Journal of Echocardiography vol 10 no 5 pp 663ndash6682009
[20] M Matsumoto M Inoue S Tamura K Tanaka and H AbeldquoThree-dimensional echocardiography for spatial visualizationand volume calculation of cardiac structuresrdquo Journal of ClinicalUltrasound vol 9 no 4 pp 157ndash165 1981
[21] K H Sheikh S W Smith O von Ramm and J Kisslo ldquoReal-time three-dimensional echocardiography feasibility and ini-tial userdquo Echocardiography vol 8 no 1 pp 119ndash125 1991
[22] L Sugeng L Weinert K Thiele and R M Lang ldquoReal-timethree-dimensional echocardiography using a novelmatrix arraytransducerrdquo Echocardiography vol 20 no 7 pp 623ndash635 2003
[23] N P Nikitin C Constantin P H Loh et al ldquoNew generation3-dimensional echocardiography for left ventricular volumetricand functional measurements comparison with cardiac mag-netic resonancerdquo European Journal of Echocardiography vol 7no 5 pp 365ndash372 2006
[24] V Mor-Avi L Sugeng L Weinert et al ldquoFast measurement ofleft ventricular mass with real-time three-dimensional echocar-diography comparison withmagnetic resonance imagingrdquoCir-culation vol 110 no 13 pp 1814ndash1818 2004
[25] L Sugeng V Mor-Avi L Weinert et al ldquoQuantitative assess-ment of left ventricular size and function side-by-side compari-son of real-time three-dimensional echocardiography and com-puted tomography with magnetic resonance referencerdquo Cir-culation vol 114 no 7 pp 654ndash661 2006
[26] S Kapetanakis M T Kearney A Siva N Gall M Cooklinand M J Monaghan ldquoReal-time three-dimensional echocar-diography a novel technique to quantify global left ventricularmechanical dyssynchronyrdquo Circulation vol 112 no 7 pp 992ndash1000 2005
[27] O I I Soliman M L Geleijnse D A M J Theuns et alldquoUsefulness of left ventricular systolic dyssynchrony by real-time three-dimensional echocardiography to predict long-termresponse to cardiac resynchronization therapyrdquo The AmericanJournal of Cardiology vol 103 no 11 pp 1586ndash1591 2009
[28] A V Khaw R S von Bardeleben C Strasser et al ldquoDirect mea-surement of left ventricular outflow tract by transthoracic real-time 3D-echocardiography increases accuracy in assessment ofaortic valve stenosisrdquo International Journal of Cardiology vol136 no 1 pp 64ndash71 2009
[29] L Sugeng S K Shernan I S Salgo et al ldquoLive 3-dimensionaltransesophageal echocardiography Initial experience using thefully-sampled matrix array proberdquo Journal of the American Col-lege of Cardiology vol 52 no 6 pp 446ndash449 2008
[30] D G Gibson T A Prewitt and D J Brown ldquoAnalysis of leftventricular wall movement during isovolumic relaxation and its
10 BioMed Research International
relation to coronary artery diseaserdquo The British Heart Journalvol 38 no 10 pp 1010ndash1019 1976
[31] P Palka A Lange A D Fleming G R Sutherland L N FeenandW NMcDicken ldquoDoppler tissue imaging myocardial wallmotion velocities in normal subjectsrdquo Journal of the AmericanSociety of Echocardiography vol 8 no 5 pp 659ndash668 1995
[32] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressures acomparative simultaneous Doppler-catheterization studyrdquo Cir-culation vol 102 no 15 pp 1788ndash1794 2000
[33] H Blessberger and T Binder ldquoTwo dimensional speckle track-ing echocardiography basic principlesrdquoHeart vol 96 no 9 pp716ndash722 2010
[34] J Gorcsan III and H Tanaka ldquoEchocardiographic assessmentof myocardial strainrdquo Journal of the American College of Cardi-ology vol 58 no 14 pp 1401ndash1413 2011
[35] T H Marwick R L Leano J Brown et al ldquoMyocardial strainmeasurement with 2-dimensional speckle-tracking echocardi-ography Definition of normal rangerdquo JACC CardiovascularImaging vol 2 no 1 pp 80ndash84 2009
[36] A C T Ng M Sitges P N Pham et al ldquoIncrementalvalue of 2-dimensional speckle tracking strain imaging to wallmotion analysis for detection of coronary artery disease inpatients undergoing dobutamine stress echocardiographyrdquoTheAmerican Heart Journal vol 158 no 5 pp 836ndash844 2009
[37] C B Ingul E Rozis S A Slordahl and T H Marwick ldquoIncre-mental value of strain rate imaging to wall motion analysisfor prediction of outcome in patients undergoing dobutaminestress echocardiographyrdquo Circulation vol 115 no 10 pp 1252ndash1259 2007
[38] R Hoffmann E Altiok B Nowak et al ldquoStrain rate measure-ment by Doppler echocardiography allows improved assess-ment of myocardial viability in patients with depressed left ven-tricular functionrdquo Journal of the American College of Cardiologyvol 39 no 3 pp 443ndash449 2002
[39] L Hanekom C Jenkins L Jeffries et al ldquoIncremental valueof strain rate analysis as an adjunct to wall-motion scoring forassessment of myocardial viability by dobutamine echocardio-graphy a follow-up study after revascularizationrdquo Circulationvol 112 no 25 pp 3892ndash3900 2005
[40] H Tanaka H Nesser T Buck et al ldquoDyssynchrony by speckle-tracking echocardiography and response to cardiac resynchro-nization therapy results of the speckle tracking and resynchro-nization (STAR) studyrdquo European Heart Journal vol 31 no 14pp 1690ndash1700 2010
[41] F Z Khan M S Virdee C R Palmer et al ldquoTargeted leftventricular lead placement to guide cardiac resynchronizationtherapy the TARGET study a randomized controlled trialrdquoJournal of the American College of Cardiology vol 59 no 17 pp1509ndash1518 2012
[42] E S Chung A R Leon L Tavazzi et al ldquoResults of the predic-tors of response to CRT (PROSPECT) trialrdquoCirculation vol 117no 20 pp 2608ndash2616 2008
[43] J J Bax and J Gorcsan III ldquoEchocardiography and noninvasiveimaging in cardiac resynchronization therapy Results of thePROSPECT (predictors of response to cardiac resynchroniza-tion therapy) study in perspectiverdquo Journal of the American Col-lege of Cardiology vol 53 no 21 pp 1933ndash1943 2009
[44] B N Shah M de Villa R S Khattar and R Senior ldquoImagingcardiac sarcoidosis the incremental benefit of speckle trackingechocardiographyrdquo Echocardiography 2013
[45] J KramerM Niemann D Liu et al ldquoTwo-dimensional speckletracking as a non-invasive tool for identification of myocardialfibrosis in Fabry diseaserdquoEuropeanHeart Journal vol 34 no 21pp 1587ndash1596 2013
[46] J L Hare J K Brown R Leano C Jenkins N Woodwardand T H Marwick ldquoUse of myocardial deformation imaging todetect preclinical myocardial dysfunction before conventionalmeasures in patients undergoing breast cancer treatment withtrastuzumabrdquo The American Heart Journal vol 158 no 2 pp294ndash301 2009
[47] M J Stewart ldquoContrast echocardiographyrdquoHeart vol 89 no 3pp 342ndash348 2003
[48] R Janardhanan G Dwivedi S Hayat and R Senior ldquoMyocar-dial contrast echocardiography a new tool for assessment ofmyocardial perfusionrdquo Indian Heart Journal vol 57 no 3 pp210ndash216 2005
[49] S B Feinstein F J T Cate W Zwehl et al ldquoTwo-dimensionalcontrast echocardiography I In vitro development and quanti-tative analysis of echo contrast agentsrdquo Journal of the AmericanCollege of Cardiology vol 3 no 1 pp 14ndash20 1984
[50] R Hoffmann S von Bardeleben F T Cate et al ldquoAssessmentof systolic left ventricular function a multi-centre comparisonof cineventriculography cardiac magnetic resonance imagingunenhanced and contrast-enhanced echocardiographyrdquo Euro-pean Heart Journal vol 26 no 6 pp 607ndash616 2005
[51] R Hoffmann S von Bardeleben J D Kasprzak et al ldquoAnalysisof regional left ventricular function by cineventriculographycardiac magnetic resonance imaging and unenhanced andcontrast-enhanced echocardiography a multicenter compari-son of methodsrdquo Journal of the American College of Cardiologyvol 47 no 1 pp 121ndash128 2006
[52] W G Hundley A M Kizilbash I Afridi F Franco R MPeshock and P A Grayburn ldquoAdministration of an intravenousperfluorocarbon contrast agent improves echocardiographicdetermination of left ventricular volumes and ejection fractioncomparison with cine magnetic resonance imagingrdquo Journal ofthe American College of Cardiology vol 32 no 5 pp 1426ndash14321998
[53] S Malm S Frigstad E Sagberg H Larsson and T SkjaerpeldquoAccurate and reproducible measurement of left ventricularvolume and ejection fraction by contrast echocardiography acomparison with magnetic resonance imagingrdquo Journal of theAmerican College of Cardiology vol 44 no 5 pp 1030ndash10352004
[54] B K Koo D Choi J W Ha S M Kang N Chung and S YCho ldquoIsolated noncompaction of the ventricular myocardiumcontrast echocardiographic findings and review of the litera-turerdquo Echocardiography vol 19 no 2 pp 153ndash156 2002
[55] P Soman J Swinburn M Callister N G Stephens and RSenior ldquoApical hypertrophic cardiomyopathy bedside diagno-sis by intravenous contrast echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 14 no 4 pp 311ndash3132001
[56] S Thanigaraj K B Schechtman and J E Perez ldquoImprovedechocardiographic delineation of left ventricular thrombuswith the use of intravenous second-generation contrast imageenhancementrdquo Journal of the American Society of Echocardiog-raphy vol 12 no 12 pp 1022ndash1026 1999
[57] S Thanigaraj R F Nease Jr K B Schechtman R L Wade SLoslo and J E Perez ldquoUse of contrast for image enhancementduring stress echocardiography is cost-effective and reduces
BioMed Research International 11
additional diagnostic testingrdquo The American Journal of Cardi-ology vol 87 no 12 pp 1430ndash1432 2001
[58] S Kaul and A R Jayaweera ldquoCoronary and myocardial bloodvolumes noninvasive tools to assess the coronary microcircu-lationrdquo Circulation vol 96 no 3 pp 719ndash724 1997
[59] K Wei A R Jayaweera S Firoozan A Linka D M Skybaand S Kaul ldquoBasis for detection of stenosis using venousadministration of microbubbles during myocardial contrastechocardiography bolus or continuous infusionrdquo Journal of theAmeri-canCollege of Cardiology vol 32 no 1 pp 252ndash260 1998
[60] W F Armstrong T M Mueller E L Kinney E G Tickner JC Dillon and H Feigenbaum ldquoAssessment of myocardial per-fusion abnormalities with contrast-enhanced two-dimensionalechocardiographyrdquo Circulation vol 66 no 1 pp 166ndash173 1982
[61] C Tei T Sakamaki PM Shah et al ldquoMyocardial contrast echo-cardiography a reproducible technique of myocardial opacifi-cation for identifying regional perfusion deficitsrdquo Circulationvol 67 no 3 pp 585ndash593 1983
[62] R Senior H BecherMMonaghan et al ldquoContrast echocardio-graphy evidence-based recommendations by european associ-ation of echocardiographyrdquo European Journal of Echocardiogra-phy vol 10 no 2 pp 194ndash212 2009
[63] S Bhattacharyya R Khattar andR Senior ldquoCharacterisation ofintra-cardiacmasses bymyocardial contrast echocardiographyrdquoInternational Journal of Cardiology vol 163 no 1 pp e11ndashe132013
[64] L A Smith R Dworakowski A Bhan et al ldquoReal-time three-dimensional transesophageal echocardiography adds value totranscatheter aortic valve implantationrdquo Journal of theAmericanSociety of Echocardiography vol 26 no 4 pp 359ndash369 2013
[65] F Regoli F F Faletra G Nucifora et al ldquoFeasibility and acuteefficacy of radiofrequency ablation of cavotricuspid isthmus-dependent atrial flutter guided by real-time 3D TEErdquo JACCCardiovascular Imaging vol 4 no 7 pp 716ndash726 2011
[66] S S Kim ZM Hijazi R M Lang and B P Knight ldquoThe use ofintracardiac echocardiography and other intracardiac imagingtools to guide noncoronary cardiac interventionsrdquo Journal of theAmerican College of Cardiology vol 53 no 23 pp 2117ndash21282009
[67] JMMangrum J PMounsey L C Kok J P DiMarco andD EHaines ldquoIntracardiac echocardiography-guided anatomicallybased radiofrequency ablation of focal atrial fibrillation origi-nating from pulmonary veinsrdquo Journal of the American Collegeof Cardiology vol 39 no 12 pp 1964ndash1972 2002
[68] R Bala J F Ren M D Hutchinson et al ldquoAssessing epicardialsubstrate using intracardiac echocardiography during VT abla-tionrdquo Circulation Arrhythmia and Electrophysiology vol 4 no5 pp 667ndash673 2011
[69] C Vigna N Marchese M Zanchetta et al ldquoEchocardio-graphic guidance of percutaneous patent foramen ovale closurehead-to-head comparison of transesophageal versus rotationalintracardiac echocardiographyrdquo Echocardiography vol 29 no9 pp 1103ndash1110 2012
[70] T Bartel N Bonaros L Muller et al ldquoIntracardiac echocar-diography a new guiding tool for transcatheter aortic valvereplacementrdquo Journal of the American Society of Echocardiog-raphy vol 24 no 9 pp 966ndash975 2011
[71] R Bai L Di Biase P Mohanty et al ldquoPositioning of left ventric-ular pacing lead guided by intracardiac echocardiography withvector velocity imaging during cardiac resynchronization ther-apy procedurerdquo Journal of Cardiovascular Electrophysiology vol22 no 9 pp 1034ndash1041 2011

4 BioMed Research International
Rest
(a)
Rest
(b)
Stress
(c)
Stress
(d)
Figure 2 A patient with moderate mitral stenosis but worsening exertional dyspnoea underwent exercise SE At rest mean transmitralgradient was 5mmHg (a) and transtricuspid pressure gradient was 24mmHg (b) After 7-minute BRUCE protocol treadmill exercise meantransmitral gradient significantly increased to 27mmHg (c) and transtricuspid pressure gradient had more than doubled to 51mmHg (d)The patient subsequently underwent balloon mitral valvuloplasty with excellent symptomatic relief
Exercise SE is also helpful in certain patients with mitralvalve disease Patients with mitral stenosis (MS) who havesymptoms disproportionate to the degree of MS at rest (egmarked exertional dyspnoea but only moderate MS at rest)should undergo exercise SEmdashan increase inmean transmitralgradient to gt15mmHg or pulmonary artery pressure togt60mmHg is an indication for valve intervention (Figure 2)The dynamic nature of ischaemic mitral regurgitation (MR)was previously shown in a quantitative Doppler echocardio-graphy study using exercise stress in patients with ischaemiccardiomyopathy (ICM) recently admitted with pulmonaryoedema and comparing with ICM patients without pul-monary oedema [15] Patientswith recent pulmonary oedemahad significantly greater increases in MR and pulmonarypressures during exercise than those without pulmonaryoedema The same group has also demonstrated the clinicalvalue of exercise SE in patients with degenerative MR [16] Arecent analysis clearly indicated the value of SE in valve dis-ease in daily clinical practice and also suggested expansion ofSE in valve disease beyond that indicated by current guide-lines [17]
Aside from valvular heart disease exercise SE can also beused in patients with hypertrophic cardiomyopathy to revealdynamic left ventricular outflow tract obstruction (Figure 3)[18] Finally myocardial contractile reserve determined bySE can identify those patients that will experience LV reverse
remodelling following cardiac resynchronisation therapy[19]
32 Three-Dimensional Echocardiography Three-dimen-sional (3D) echocardiography is widely perceived as a noveltechnique but the initial work on 3D echocardiography datesback three decades [20 21] However significant technicaladvances have reduced the size of the transducer improvedspeed of image processing and importantly allowed real-time 3D imaging This has been made possible with theadvent of fully sampled matrix array transducer technology[22]
3D-TTE has numerous proven uses in clinical practice Ithas been shown to be superior to 2D-TTE and equal to CMRfor assessment of ventricular volumes [23] cardiacmass [24]and calculation of ejection fraction [25] The latter is espe-cially useful clinically in patients that require serial EFassessment (eg cancer patients receiving chemotherapeuticagents with potential cardiotoxicity) as 2D-TTE can sufferfrom underestimation of true volumes due to chamber fore-shortening 3D-TTE has also been used to assess ventricularmechanical dyssynchrony [26] and of clinical relevancedyssynchronydemonstrated by real-time 3D-TTE canpredictlong-term response to cardiac resynchronization therapy[27] 3D-TTE has also been proved to be valuable in assess-ment of valvular heart diseasemdashit can provide information
BioMed Research International 5
(a) (b)
(c)
Figure 3 A 47-year-old man with hypertrophic cardiomyopathy underwent exercise SE At rest peak gradient across the aortic valve was12mmHg (panel (a)) Repeat assessment during a held Valsalva manoeuvre revealed that the peak gradient was now 63mmHg (panel (b))which indicates that exercise-induced LVOTobstruction is highly likelyThis was indeed confirmed that at peak stress themaximumgradienthad increased to 135mmHg (panel (c)) Note the late systolic peaking of the Doppler profile in panels (b) and (c) indicative of dynamic ratherthan fixed outflow tract obstruction The patient was commenced on beta-blocker therapy following the test results
previously only easily determined by TOE (eg mitral valvescallop assessment in mitral regurgitation) The accuracy ofcalculation of aortic valve area in aortic stenosis has also beenshown to be improved by using 3D-TTE due to more preciseassessment of outflow tract dimensions [28]
The most significant advance however has been in3D-TOE [29] Real-time 3D zoom and live 3D imaging pro-vide unique views of the heart and allow superior detection ofpathology especially valvular diseases 3D echocardiographyis most valuable in cases of complex pathology A simple P2prolapse of the mitral valve is usually evident from 2D imag-ing but a combination of flail scallop(s) and prolapse +minuschordal rupture may be more challenging on 2D and anyconfusion is usually dispelled with 3D imaging As discussedin the following the feasibility of real-time 3D-TOEhasmadeit an essential adjunct in guiding invasive procedures in thecatheter laboratory also
33 Deformation Imaging ldquoMyocardial Mechanicsrdquo Thecomplex orientation of myocardial fibresmdashradial circumfer-ential and longitudinalmdashhas been recognised for a long timeThe theory that tissue motion as opposed to endocardial
excursion is important in assessment ventricular function isalso not newmdashM-mode echocardiography was used to relatemyocardial velocity to ventricular function in the 1970s [30]
Tissue Doppler imaging (TDI) and speckle trackingechocardiography (STE) are techniques that permit detailedanalysis of regional as well as global cardiac function throughunique temporal and spatial data processing TDI deliberatelyfilters out the low amplitude high frequency signals from theblood-pool in order to allow analysis of the high amplitudeand low frequency signals frommyocardium itself [31] TDI ismost frequently used to assist in determining diastolic func-tion and LV filling pressures by means of the 1198641198641015840 ratio [32](where 1198641015840 is the early motion of the mitral annulus backtowards the cardiac base from the apex) The longitudinalfunction of both ventricles is also assessed with TDI where 1198781015840represents the peak systolic velocity of the left or right ventri-cle These parameters have become routine measurements inclinical practice due to a combination of their reproducibilityand diagnostic and prognostic importance
STE is based on the principle of following (or tracking)the unique ldquospeckle patternrdquo of amyocardial segment throughthe cardiac cycle (see Figure 4) One advantage of STE is that
6 BioMed Research International
(a) (b)
(c) (d)
Figure 4 Examples of strain imaging using speckle tracking echocardiography On the top row are images from a normal healthy volunteer(apical 4-chamber view on the left and summary strain scores with bulls-eye plot on the right) and on the bottom row are correspondingimages from a patient with severe ischaemic cardiomyopathy Note that the healthy volunteer has normal longitudinal strain in all segmentswith a global strain score of minus189 whereas the cardiomyopathy patient has highly abnormal strains with a significantly depressed globalstrain score of just minus50
it removes the possibility of falsely designating myocardiumas having normal function when ldquovelocityrdquo is in fact due totethering (eg adjacent scar) or translational motion due tomovement of the whole heart (both potential limitations ofTDI [33]) BothTDI and STE can be used tomeasuremyocar-dial strain a dimensionless quantity defined as the unitchange in length of an object relative to its original lengthStrain rate is its derivative with respect to time (ie rate ofchange of strain and usually expressed as 1sec (or secminus1)) Innormal myocardial segments there is shortening in systole(negative strain and strain rates) and lengthening in diastole(positive strain and strain rates) as cardiomyocytes return totheir resting state [33]
A wealth of data has been accumulated on the potentialclinical value of strain and strain rate assessment in a numberof cardiac diseases [34] Normal ranges have also beendefined [35] STE-derived strain imaging has been shownto have additive benefit for detection of CAD in patientsundergoing dobutamine SE [36] and the superior ability ofstrain imaging to predict outcome in patients undergoingdobutamine SE has also been shown [37] Strain imaging is anaccurate technique for detecting viablemyocardium particu-larly when strain parameters are assessed at rest and followinglow-dose dobutamine SE [38 39] Strain imaging has alsobeen studied extensively for detecting dyssynchrony and thuspredicting response to cardiac resynchronisation therapy[40] Recently it was shown that targeted placement of the LVpacing lead to the site of latest mechanical activationmdashaselucidated by STEmdashwas associated with favourable reverseremodelling fewer repeat hospitalizations and improvedfunctional capacity compared to patients with standard
placement of LV leads [41] TDI can also be used to assesscardiac dyssynchrony This has become a controversial topichowever as the PROSPECT trial [42] suggested no echocar-diographic parameter(s) could accurately predict favourableresponse to biventricular pacing though numerous author-ities worldwide were quick to highlight surprisingly funda-mental flaws in the trialrsquos methodology [43]
Potentially of great clinical relevance is the fact that STEcan reveal subclinical LV dysfunction in hearts with appar-ently normal systolic function as measured by EF and thuscould have a role in detecting cardiac involvement in systemicdiseases [44] unusual or rare conditions [45] and also fordetecting early evidence of cardiotoxicity in cancer patientsreceiving chemotherapy [46] At present strain and strainrate imaging remains predominantly research tools but showsconsiderable promise for translation into clinical practiceThe limitations of STE include the requirement of goodimage quality and variability between different software andhardware manufacturers
34 Contrast Echocardiography Ultrasound contrast agents(UCAs) consist of gas-filled microspheres which displayunique acoustic properties when exposed to ultrasoundwaves Contrast bubbles resonate when exposed to an ultra-sound wave This is predominantly a nonlinear oscillation(ie expansion and contraction of the bubble are not equal)at the ultrasound frequencies used in diagnostic imagingMicrobubbles are several million times more effective atscattering sound than red blood cells resulting in a greatlyenhanced ldquoblood poolrdquo signal [47] The blood pool agents
BioMed Research International 7
(a) (b)
(c) (d)Figure 5 Apical 4-chamber images taken before ((a) and (b)) and after ((c) and (d)) ultrasound contrast injection in a patient attending forroutine transthoracic echocardiography At rest endocardial definition at end diastole (a) and end systole (b) was poor and did not permitquantitation of ejection fraction or assessment of regional (segmental) function Following a single bolus injection of contrast endocardialborder visualisation was significantly improved at end diastole (c) and end systole (d) allowing regional and global systolic assessments
developed consist of a gaseous material encapsulated withina stabilizing outer shell These microbubbles are typicallyslightly smaller than erythrocytes allowing free passagewithin the circulation and effectively acting as red cell tracers[48]
The first generation UCAs consisted of air surrounded byan albumin shell [49] Unfortunately these agents had a veryshort lifespan in vivo and thus had limited utility in diagnostictests The second generation of UCAs addressed this issueby changing both components of microbubblesmdashthe air wasreplaced by inert gases with high molecular weight highdensity and low solubility such as sulphur hexafluoride(SonoVue) or perfluorocarbons (eg Optison or Definity)The outer shell is now made using phospholipids which also
confer greater stability They are used to produce a strongerultrasonic signal than that generated by tissues and thus aremost commonly used to improve image quality (Figure 5)
There is ample evidence demonstrating that UCAsimprove estimation of global [50] and regional [51] LV sys-tolic functions UCAs improve the accuracy of measurementof LV volumes and ejection fraction also [52 53] As UCAsimprove overall image quality they also help detect structuralabnormalities such as noncompaction cardiomyopathy [54]apical hypertrophic cardiomyopathy [55] and left ventric-ular thrombus [56] Their biggest use however is in stressechocardiography The use of contrast significantly reducesthe number of ldquouninterpretablerdquo studies [7] and thus is cost-effective as it reduces additional testing [57] This has helped
8 BioMed Research International
establish stress echocardiography as a front-line investigationin assessment of patients with known or suspected coronaryartery disease
The majority (90) of the blood within the myocardialwalls reside within capillaries [58] Thus the intensity of thecontrast signal when the myocardium is fully saturated withcontrast reflects the concentration of microbubbles withinmyocardial capillaries [59] and consequently capillary ormyocardial blood volume Appreciation of this fact led to therecognition that echocardiography could be used to assessmyocardial perfusion a technique now known as myocardialcontrast echocardiography (MCE) A high intensity (highmechanical index) ldquoflashrdquo or impulse is used to destroy themicrobubbles in the myocardial capillaries and their rate ofreplenishment is observed Delayed replenishment manifestsas a perfusion defect and is the hallmark of ischaemia duringMCE The first papers on MCE dates back to three decades[60 61] and since then it has accumulated a large evidencebase to support its use in the detection of CAD [62] Finallyas presence of contrast denotes vascularity UCAs can also beused in patients with intracardiac masses in order to distin-guish between avascularmasses (eg thrombus) and vascularmasses such as tumours [63]
4 lsquolsquoInterventional Echocardiologyrsquorsquo Dawn ofa New Super-Specialty
The advances in 3D echocardiographymdashin particular theadvent of a fully sampled matrix array transducer allowingreal-time 3D-TOEmdashhas brought the echocardiologist to theforefront of catheter-lab-based procedures in structural heartdisease Real-time 3D-TOE is now considered bymany a pre-requisite for guidance of percutaneous treatment of aorticstenosis (transcatheter aortic valve implantation (TAVI))mitral regurgitation (eg MitraClip devices) closure of theleft atrial appendage and of atrial septal defects (ASDs andPFOs) The incremental value of 3D-TOE over 2D-TOEduring TAVI procedures was recently demonstrated in alarge single-centre study [64] Indeed real-time 3D-TOE isexpanding its use further and for example has been usedto guide electrophysiological procedures such as ablation ofatrial flutter and fibrillation (helping reduce significantly theuse of fluoroscopy) [65]
Intracardiac echocardiography (ICE) performed in thecatheter laboratory using single-use percutaneous 2D probesintroduced transvenously (eg via the femoral vein) is alsowidely used to guide interventions [66] Its biggest advantageover TOE is the ability to obtain similar echo views withoutthe need for general anaesthesia with its attendant costs andpotential risks Therefore ICE has been used in preference toTOE for a number of procedures including atrial fibrillation[67] and ventricular tachycardia [68] ablation proceduresclosure of septal defects [69] TAVI procedures [70] and toguide CRT procedures [71] However the significant limita-tion of ICE is expensive given that the probes must be dis-posed of after a single use
The echocardiologist performing such studies needs tohave a sound grasp of normal cardiac and valvular anatomy
and combine quick thinking with speedy manual dexterityThis skill set is not necessarily acquired during conventionaltraining Heshe may be called upon to provide urgent infor-mation in case of sudden unexplained patient deterioration(eg sudden hypotension during TAVI due to entanglementof the delivery system in the mitral subvalvular apparatuscausing acute severe mitral regurgitation) The need for suchindividuals is likely to be restricted to tertiary units butin large centres one can imagine such a person spendinga significant amount of time in the cardiac catheter lab-oratories Appropriate training will be required to ensurethat we produce cardiologists capable of performing suchstudiesmdashhence one can envisage the birth of a super-special-ity of ldquointerventional echocardiologyrdquo
5 Limitations
Echocardiography does have certain limitations which meritdiscussionThe greatest advantage of cross-sectional imaging(ie CMR and CCT) over echocardiography is the informa-tion available on extracardiac structures The aorta aorticarch pulmonary artery and pulmonary veins are far moreclearly seen by these modalities and are often poorly seen ornot seen at all by echocardiography Thus assessment of pul-monary veins in patients awaiting an atrial fibrillation abla-tion procedure assessment of the aortic arch and descendingthoracic aorta in patients with chronic aortic dissection orcoarctation and serial assessment of patients with previouscoarctation repair for example will generally be performedby CMR or CCT
Echocardiography can also suffer from poor image qual-ity despite the use of ultrasound contrast agentsThis is mostoften seen in patientswho are extremely underweight or over-weight but also in patients with chronic airways disease orchest wall deformities (eg pectus excavatum) Patients onintensive care units who are frequently supine and may bemechanically ventilated also often have challenging TTEimages although TOE can resolve such difficulties
6 Conclusion
Echocardiography permits accurate assessment of myocar-dial structure function and perfusion Echocardiography isthus in itself a multimodality imaging technique The fieldof echocardiography is diverse and encompasses numerousindividual techniquesmdashsome with established clinical valuewhilst others showmuch promise in researchThe expandingrole of echocardiography within current clinical practice isunderpinned by continual technological advances and justi-fied by the accumulating evidence of clinical value of thesetechniques when utilised in daily practice
References
[1] L J Shaw T HMarwickW A Zoghbi et al ldquoWhy all the focuson cardiac imagingrdquo JACC Cardiovascular Imaging vol 3 no7 pp 789ndash794 2010
[2] F A Flachskampf L Badano W G Daniel et al ldquoRecommen-dations for transoesophageal echocardiography update 2010rdquo
BioMed Research International 9
European Journal of Echocardiography vol 11 no 7 pp 557ndash5762010
[3] W G Daniel R ErbelW Kasper et al ldquoSafety of transesophag-eal echocardiography A multicenter survey of 10419 examina-tionsrdquo Circulation vol 83 no 3 pp 817ndash821 1991
[4] J N Hilberath D A Oakes S K Shernan B E Bulwer M NDrsquoAmbra and H K Eltzschig ldquoSafety of transesophageal echo-cardiographyrdquo Journal of the American Society of Echocardiog-raphy vol 23 no 11 pp 1115ndash1127 2010
[5] D G Skolnick S G Sawada H Feigenbaum and D S SegarldquoEnhanced endocardial visualization with noncontrast har-monic imaging during stress echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 12 no 7 pp 559ndash5631999
[6] F B Sozzi D Poldermans J J Bax et al ldquoSecond harmonicimaging improves sensitivity of dobutamine stress echocar-diography for the diagnosis of coronary artery diseaserdquo TheAmerican Heart Journal vol 142 no 1 pp 153ndash159 2001
[7] J C Plana I A Mikati H Dokainish et al ldquoA randomizedcross-over study for evaluation of the effect of image optimiza-tion with contrast on the diagnostic accuracy of dobutamineechocardiography in coronary artery disease The OPTIMIZEtrialrdquo JACC Cardiovascular Imaging vol 1 no 2 pp 145ndash1522008
[8] J S Skinner L Smeeth J M Kendall P C Adams and ATimmis ldquoNICE guidance Chest pain of recent onset assess-ment and diagnosis of recent onset chest pain or discomfort ofsuspected cardiac originrdquo Heart vol 96 no 12 pp 974ndash9782010
[9] P Jeetley L Burden B Stoykova and R Senior ldquoClinical andeconomic impact of stress echocardiography compared withexercise electrocardiography in patients with suspected acutecoronary syndrome but negative troponin a prospective ran-domized controlled studyrdquo European Heart Journal vol 28 no2 pp 204ndash211 2007
[10] BN ShahG Balaji A Alhajiri I S Ramzy S Ahmadvazir andR Senior ldquoThe incremental diagnostic and prognostic valueof contemporary stress echocardiography in a chest pain unitmortality and morbidity outcomes from a real-world settingrdquoCirculation Cardiovascular Imaging vol 6 no 2 pp 202ndash2092013
[11] P Lancellotti F LeboisM Simon C Tombeux C Chauvel andL A Pierard ldquoPrognostic importance of quantitative exerciseDoppler echocardiography in asymptomatic valvular aorticstenosisrdquo Circulation vol 112 no 9 supplement pp I377ndashI3822005
[12] S Marechaux Z Hachicha A Bellouin et al ldquoUsefulness ofexercise-stress echocardiography for risk stratification of trueasymptomatic patients with aortic valve stenosisrdquo EuropeanHeart Journal vol 31 no 11 pp 1390ndash1397 2010
[13] P Lancellotti J Magne E Donal et al ldquoDeterminants andprognostic significance of exercise pulmonary hypertension inasymptomatic severe aortic stenosisrdquoCirculation vol 126 no 7pp 851ndash859 2012
[14] JMonin JQuereMMonchi et al ldquoLow-gradient aortic steno-sis Operative risk stratification and predictors for long-termoutcome a multicenter study using dobutamine stress hemo-dynamicsrdquo Circulation vol 108 no 3 pp 319ndash324 2003
[15] L A Pierard and P Lancellotti ldquoThe role of ischemic mitralregurgitation in the pathogenesis of acute pulmonary edemardquoThe New England Journal of Medicine vol 351 no 16 pp 1627ndash1634 2004
[16] J Magne P Lancellotti and L A Pierard ldquoExercise-inducedchanges in degenerative mitral regurgitationrdquo Journal of theAmericanCollege of Cardiology vol 56 no 4 pp 300ndash309 2010
[17] S Bhattacharyya V Kamperidis B N Shah et al ldquo152 Clinicalutility and prognostic value of appropriateness criteria in stressechocardiography for evaluation of valvular heart diseaserdquoHeart vol 99 pp A89ndashA90 2013
[18] B J Gersh B J Maron R O Bonow et al ldquo2011 ACCFAHAguideline for the diagnosis and treatment of hypertrophic cardi-omyopathyrdquo Journal of the American College of Cardiology vol58 no 25 pp e212ndashe260 2011
[19] P Lancellotti M Senechal M Moonen et al ldquoMyocardial con-tractile reserve during exercise predicts left ventricular reverseremodelling after cardiac resynchronization therapyrdquo Euro-pean Journal of Echocardiography vol 10 no 5 pp 663ndash6682009
[20] M Matsumoto M Inoue S Tamura K Tanaka and H AbeldquoThree-dimensional echocardiography for spatial visualizationand volume calculation of cardiac structuresrdquo Journal of ClinicalUltrasound vol 9 no 4 pp 157ndash165 1981
[21] K H Sheikh S W Smith O von Ramm and J Kisslo ldquoReal-time three-dimensional echocardiography feasibility and ini-tial userdquo Echocardiography vol 8 no 1 pp 119ndash125 1991
[22] L Sugeng L Weinert K Thiele and R M Lang ldquoReal-timethree-dimensional echocardiography using a novelmatrix arraytransducerrdquo Echocardiography vol 20 no 7 pp 623ndash635 2003
[23] N P Nikitin C Constantin P H Loh et al ldquoNew generation3-dimensional echocardiography for left ventricular volumetricand functional measurements comparison with cardiac mag-netic resonancerdquo European Journal of Echocardiography vol 7no 5 pp 365ndash372 2006
[24] V Mor-Avi L Sugeng L Weinert et al ldquoFast measurement ofleft ventricular mass with real-time three-dimensional echocar-diography comparison withmagnetic resonance imagingrdquoCir-culation vol 110 no 13 pp 1814ndash1818 2004
[25] L Sugeng V Mor-Avi L Weinert et al ldquoQuantitative assess-ment of left ventricular size and function side-by-side compari-son of real-time three-dimensional echocardiography and com-puted tomography with magnetic resonance referencerdquo Cir-culation vol 114 no 7 pp 654ndash661 2006
[26] S Kapetanakis M T Kearney A Siva N Gall M Cooklinand M J Monaghan ldquoReal-time three-dimensional echocar-diography a novel technique to quantify global left ventricularmechanical dyssynchronyrdquo Circulation vol 112 no 7 pp 992ndash1000 2005
[27] O I I Soliman M L Geleijnse D A M J Theuns et alldquoUsefulness of left ventricular systolic dyssynchrony by real-time three-dimensional echocardiography to predict long-termresponse to cardiac resynchronization therapyrdquo The AmericanJournal of Cardiology vol 103 no 11 pp 1586ndash1591 2009
[28] A V Khaw R S von Bardeleben C Strasser et al ldquoDirect mea-surement of left ventricular outflow tract by transthoracic real-time 3D-echocardiography increases accuracy in assessment ofaortic valve stenosisrdquo International Journal of Cardiology vol136 no 1 pp 64ndash71 2009
[29] L Sugeng S K Shernan I S Salgo et al ldquoLive 3-dimensionaltransesophageal echocardiography Initial experience using thefully-sampled matrix array proberdquo Journal of the American Col-lege of Cardiology vol 52 no 6 pp 446ndash449 2008
[30] D G Gibson T A Prewitt and D J Brown ldquoAnalysis of leftventricular wall movement during isovolumic relaxation and its
10 BioMed Research International
relation to coronary artery diseaserdquo The British Heart Journalvol 38 no 10 pp 1010ndash1019 1976
[31] P Palka A Lange A D Fleming G R Sutherland L N FeenandW NMcDicken ldquoDoppler tissue imaging myocardial wallmotion velocities in normal subjectsrdquo Journal of the AmericanSociety of Echocardiography vol 8 no 5 pp 659ndash668 1995
[32] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressures acomparative simultaneous Doppler-catheterization studyrdquo Cir-culation vol 102 no 15 pp 1788ndash1794 2000
[33] H Blessberger and T Binder ldquoTwo dimensional speckle track-ing echocardiography basic principlesrdquoHeart vol 96 no 9 pp716ndash722 2010
[34] J Gorcsan III and H Tanaka ldquoEchocardiographic assessmentof myocardial strainrdquo Journal of the American College of Cardi-ology vol 58 no 14 pp 1401ndash1413 2011
[35] T H Marwick R L Leano J Brown et al ldquoMyocardial strainmeasurement with 2-dimensional speckle-tracking echocardi-ography Definition of normal rangerdquo JACC CardiovascularImaging vol 2 no 1 pp 80ndash84 2009
[36] A C T Ng M Sitges P N Pham et al ldquoIncrementalvalue of 2-dimensional speckle tracking strain imaging to wallmotion analysis for detection of coronary artery disease inpatients undergoing dobutamine stress echocardiographyrdquoTheAmerican Heart Journal vol 158 no 5 pp 836ndash844 2009
[37] C B Ingul E Rozis S A Slordahl and T H Marwick ldquoIncre-mental value of strain rate imaging to wall motion analysisfor prediction of outcome in patients undergoing dobutaminestress echocardiographyrdquo Circulation vol 115 no 10 pp 1252ndash1259 2007
[38] R Hoffmann E Altiok B Nowak et al ldquoStrain rate measure-ment by Doppler echocardiography allows improved assess-ment of myocardial viability in patients with depressed left ven-tricular functionrdquo Journal of the American College of Cardiologyvol 39 no 3 pp 443ndash449 2002
[39] L Hanekom C Jenkins L Jeffries et al ldquoIncremental valueof strain rate analysis as an adjunct to wall-motion scoring forassessment of myocardial viability by dobutamine echocardio-graphy a follow-up study after revascularizationrdquo Circulationvol 112 no 25 pp 3892ndash3900 2005
[40] H Tanaka H Nesser T Buck et al ldquoDyssynchrony by speckle-tracking echocardiography and response to cardiac resynchro-nization therapy results of the speckle tracking and resynchro-nization (STAR) studyrdquo European Heart Journal vol 31 no 14pp 1690ndash1700 2010
[41] F Z Khan M S Virdee C R Palmer et al ldquoTargeted leftventricular lead placement to guide cardiac resynchronizationtherapy the TARGET study a randomized controlled trialrdquoJournal of the American College of Cardiology vol 59 no 17 pp1509ndash1518 2012
[42] E S Chung A R Leon L Tavazzi et al ldquoResults of the predic-tors of response to CRT (PROSPECT) trialrdquoCirculation vol 117no 20 pp 2608ndash2616 2008
[43] J J Bax and J Gorcsan III ldquoEchocardiography and noninvasiveimaging in cardiac resynchronization therapy Results of thePROSPECT (predictors of response to cardiac resynchroniza-tion therapy) study in perspectiverdquo Journal of the American Col-lege of Cardiology vol 53 no 21 pp 1933ndash1943 2009
[44] B N Shah M de Villa R S Khattar and R Senior ldquoImagingcardiac sarcoidosis the incremental benefit of speckle trackingechocardiographyrdquo Echocardiography 2013
[45] J KramerM Niemann D Liu et al ldquoTwo-dimensional speckletracking as a non-invasive tool for identification of myocardialfibrosis in Fabry diseaserdquoEuropeanHeart Journal vol 34 no 21pp 1587ndash1596 2013
[46] J L Hare J K Brown R Leano C Jenkins N Woodwardand T H Marwick ldquoUse of myocardial deformation imaging todetect preclinical myocardial dysfunction before conventionalmeasures in patients undergoing breast cancer treatment withtrastuzumabrdquo The American Heart Journal vol 158 no 2 pp294ndash301 2009
[47] M J Stewart ldquoContrast echocardiographyrdquoHeart vol 89 no 3pp 342ndash348 2003
[48] R Janardhanan G Dwivedi S Hayat and R Senior ldquoMyocar-dial contrast echocardiography a new tool for assessment ofmyocardial perfusionrdquo Indian Heart Journal vol 57 no 3 pp210ndash216 2005
[49] S B Feinstein F J T Cate W Zwehl et al ldquoTwo-dimensionalcontrast echocardiography I In vitro development and quanti-tative analysis of echo contrast agentsrdquo Journal of the AmericanCollege of Cardiology vol 3 no 1 pp 14ndash20 1984
[50] R Hoffmann S von Bardeleben F T Cate et al ldquoAssessmentof systolic left ventricular function a multi-centre comparisonof cineventriculography cardiac magnetic resonance imagingunenhanced and contrast-enhanced echocardiographyrdquo Euro-pean Heart Journal vol 26 no 6 pp 607ndash616 2005
[51] R Hoffmann S von Bardeleben J D Kasprzak et al ldquoAnalysisof regional left ventricular function by cineventriculographycardiac magnetic resonance imaging and unenhanced andcontrast-enhanced echocardiography a multicenter compari-son of methodsrdquo Journal of the American College of Cardiologyvol 47 no 1 pp 121ndash128 2006
[52] W G Hundley A M Kizilbash I Afridi F Franco R MPeshock and P A Grayburn ldquoAdministration of an intravenousperfluorocarbon contrast agent improves echocardiographicdetermination of left ventricular volumes and ejection fractioncomparison with cine magnetic resonance imagingrdquo Journal ofthe American College of Cardiology vol 32 no 5 pp 1426ndash14321998
[53] S Malm S Frigstad E Sagberg H Larsson and T SkjaerpeldquoAccurate and reproducible measurement of left ventricularvolume and ejection fraction by contrast echocardiography acomparison with magnetic resonance imagingrdquo Journal of theAmerican College of Cardiology vol 44 no 5 pp 1030ndash10352004
[54] B K Koo D Choi J W Ha S M Kang N Chung and S YCho ldquoIsolated noncompaction of the ventricular myocardiumcontrast echocardiographic findings and review of the litera-turerdquo Echocardiography vol 19 no 2 pp 153ndash156 2002
[55] P Soman J Swinburn M Callister N G Stephens and RSenior ldquoApical hypertrophic cardiomyopathy bedside diagno-sis by intravenous contrast echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 14 no 4 pp 311ndash3132001
[56] S Thanigaraj K B Schechtman and J E Perez ldquoImprovedechocardiographic delineation of left ventricular thrombuswith the use of intravenous second-generation contrast imageenhancementrdquo Journal of the American Society of Echocardiog-raphy vol 12 no 12 pp 1022ndash1026 1999
[57] S Thanigaraj R F Nease Jr K B Schechtman R L Wade SLoslo and J E Perez ldquoUse of contrast for image enhancementduring stress echocardiography is cost-effective and reduces
BioMed Research International 11
additional diagnostic testingrdquo The American Journal of Cardi-ology vol 87 no 12 pp 1430ndash1432 2001
[58] S Kaul and A R Jayaweera ldquoCoronary and myocardial bloodvolumes noninvasive tools to assess the coronary microcircu-lationrdquo Circulation vol 96 no 3 pp 719ndash724 1997
[59] K Wei A R Jayaweera S Firoozan A Linka D M Skybaand S Kaul ldquoBasis for detection of stenosis using venousadministration of microbubbles during myocardial contrastechocardiography bolus or continuous infusionrdquo Journal of theAmeri-canCollege of Cardiology vol 32 no 1 pp 252ndash260 1998
[60] W F Armstrong T M Mueller E L Kinney E G Tickner JC Dillon and H Feigenbaum ldquoAssessment of myocardial per-fusion abnormalities with contrast-enhanced two-dimensionalechocardiographyrdquo Circulation vol 66 no 1 pp 166ndash173 1982
[61] C Tei T Sakamaki PM Shah et al ldquoMyocardial contrast echo-cardiography a reproducible technique of myocardial opacifi-cation for identifying regional perfusion deficitsrdquo Circulationvol 67 no 3 pp 585ndash593 1983
[62] R Senior H BecherMMonaghan et al ldquoContrast echocardio-graphy evidence-based recommendations by european associ-ation of echocardiographyrdquo European Journal of Echocardiogra-phy vol 10 no 2 pp 194ndash212 2009
[63] S Bhattacharyya R Khattar andR Senior ldquoCharacterisation ofintra-cardiacmasses bymyocardial contrast echocardiographyrdquoInternational Journal of Cardiology vol 163 no 1 pp e11ndashe132013
[64] L A Smith R Dworakowski A Bhan et al ldquoReal-time three-dimensional transesophageal echocardiography adds value totranscatheter aortic valve implantationrdquo Journal of theAmericanSociety of Echocardiography vol 26 no 4 pp 359ndash369 2013
[65] F Regoli F F Faletra G Nucifora et al ldquoFeasibility and acuteefficacy of radiofrequency ablation of cavotricuspid isthmus-dependent atrial flutter guided by real-time 3D TEErdquo JACCCardiovascular Imaging vol 4 no 7 pp 716ndash726 2011
[66] S S Kim ZM Hijazi R M Lang and B P Knight ldquoThe use ofintracardiac echocardiography and other intracardiac imagingtools to guide noncoronary cardiac interventionsrdquo Journal of theAmerican College of Cardiology vol 53 no 23 pp 2117ndash21282009
[67] JMMangrum J PMounsey L C Kok J P DiMarco andD EHaines ldquoIntracardiac echocardiography-guided anatomicallybased radiofrequency ablation of focal atrial fibrillation origi-nating from pulmonary veinsrdquo Journal of the American Collegeof Cardiology vol 39 no 12 pp 1964ndash1972 2002
[68] R Bala J F Ren M D Hutchinson et al ldquoAssessing epicardialsubstrate using intracardiac echocardiography during VT abla-tionrdquo Circulation Arrhythmia and Electrophysiology vol 4 no5 pp 667ndash673 2011
[69] C Vigna N Marchese M Zanchetta et al ldquoEchocardio-graphic guidance of percutaneous patent foramen ovale closurehead-to-head comparison of transesophageal versus rotationalintracardiac echocardiographyrdquo Echocardiography vol 29 no9 pp 1103ndash1110 2012
[70] T Bartel N Bonaros L Muller et al ldquoIntracardiac echocar-diography a new guiding tool for transcatheter aortic valvereplacementrdquo Journal of the American Society of Echocardiog-raphy vol 24 no 9 pp 966ndash975 2011
[71] R Bai L Di Biase P Mohanty et al ldquoPositioning of left ventric-ular pacing lead guided by intracardiac echocardiography withvector velocity imaging during cardiac resynchronization ther-apy procedurerdquo Journal of Cardiovascular Electrophysiology vol22 no 9 pp 1034ndash1041 2011

BioMed Research International 5
(a) (b)
(c)
Figure 3 A 47-year-old man with hypertrophic cardiomyopathy underwent exercise SE At rest peak gradient across the aortic valve was12mmHg (panel (a)) Repeat assessment during a held Valsalva manoeuvre revealed that the peak gradient was now 63mmHg (panel (b))which indicates that exercise-induced LVOTobstruction is highly likelyThis was indeed confirmed that at peak stress themaximumgradienthad increased to 135mmHg (panel (c)) Note the late systolic peaking of the Doppler profile in panels (b) and (c) indicative of dynamic ratherthan fixed outflow tract obstruction The patient was commenced on beta-blocker therapy following the test results
previously only easily determined by TOE (eg mitral valvescallop assessment in mitral regurgitation) The accuracy ofcalculation of aortic valve area in aortic stenosis has also beenshown to be improved by using 3D-TTE due to more preciseassessment of outflow tract dimensions [28]
The most significant advance however has been in3D-TOE [29] Real-time 3D zoom and live 3D imaging pro-vide unique views of the heart and allow superior detection ofpathology especially valvular diseases 3D echocardiographyis most valuable in cases of complex pathology A simple P2prolapse of the mitral valve is usually evident from 2D imag-ing but a combination of flail scallop(s) and prolapse +minuschordal rupture may be more challenging on 2D and anyconfusion is usually dispelled with 3D imaging As discussedin the following the feasibility of real-time 3D-TOEhasmadeit an essential adjunct in guiding invasive procedures in thecatheter laboratory also
33 Deformation Imaging ldquoMyocardial Mechanicsrdquo Thecomplex orientation of myocardial fibresmdashradial circumfer-ential and longitudinalmdashhas been recognised for a long timeThe theory that tissue motion as opposed to endocardial
excursion is important in assessment ventricular function isalso not newmdashM-mode echocardiography was used to relatemyocardial velocity to ventricular function in the 1970s [30]
Tissue Doppler imaging (TDI) and speckle trackingechocardiography (STE) are techniques that permit detailedanalysis of regional as well as global cardiac function throughunique temporal and spatial data processing TDI deliberatelyfilters out the low amplitude high frequency signals from theblood-pool in order to allow analysis of the high amplitudeand low frequency signals frommyocardium itself [31] TDI ismost frequently used to assist in determining diastolic func-tion and LV filling pressures by means of the 1198641198641015840 ratio [32](where 1198641015840 is the early motion of the mitral annulus backtowards the cardiac base from the apex) The longitudinalfunction of both ventricles is also assessed with TDI where 1198781015840represents the peak systolic velocity of the left or right ventri-cle These parameters have become routine measurements inclinical practice due to a combination of their reproducibilityand diagnostic and prognostic importance
STE is based on the principle of following (or tracking)the unique ldquospeckle patternrdquo of amyocardial segment throughthe cardiac cycle (see Figure 4) One advantage of STE is that
6 BioMed Research International
(a) (b)
(c) (d)
Figure 4 Examples of strain imaging using speckle tracking echocardiography On the top row are images from a normal healthy volunteer(apical 4-chamber view on the left and summary strain scores with bulls-eye plot on the right) and on the bottom row are correspondingimages from a patient with severe ischaemic cardiomyopathy Note that the healthy volunteer has normal longitudinal strain in all segmentswith a global strain score of minus189 whereas the cardiomyopathy patient has highly abnormal strains with a significantly depressed globalstrain score of just minus50
it removes the possibility of falsely designating myocardiumas having normal function when ldquovelocityrdquo is in fact due totethering (eg adjacent scar) or translational motion due tomovement of the whole heart (both potential limitations ofTDI [33]) BothTDI and STE can be used tomeasuremyocar-dial strain a dimensionless quantity defined as the unitchange in length of an object relative to its original lengthStrain rate is its derivative with respect to time (ie rate ofchange of strain and usually expressed as 1sec (or secminus1)) Innormal myocardial segments there is shortening in systole(negative strain and strain rates) and lengthening in diastole(positive strain and strain rates) as cardiomyocytes return totheir resting state [33]
A wealth of data has been accumulated on the potentialclinical value of strain and strain rate assessment in a numberof cardiac diseases [34] Normal ranges have also beendefined [35] STE-derived strain imaging has been shownto have additive benefit for detection of CAD in patientsundergoing dobutamine SE [36] and the superior ability ofstrain imaging to predict outcome in patients undergoingdobutamine SE has also been shown [37] Strain imaging is anaccurate technique for detecting viablemyocardium particu-larly when strain parameters are assessed at rest and followinglow-dose dobutamine SE [38 39] Strain imaging has alsobeen studied extensively for detecting dyssynchrony and thuspredicting response to cardiac resynchronisation therapy[40] Recently it was shown that targeted placement of the LVpacing lead to the site of latest mechanical activationmdashaselucidated by STEmdashwas associated with favourable reverseremodelling fewer repeat hospitalizations and improvedfunctional capacity compared to patients with standard
placement of LV leads [41] TDI can also be used to assesscardiac dyssynchrony This has become a controversial topichowever as the PROSPECT trial [42] suggested no echocar-diographic parameter(s) could accurately predict favourableresponse to biventricular pacing though numerous author-ities worldwide were quick to highlight surprisingly funda-mental flaws in the trialrsquos methodology [43]
Potentially of great clinical relevance is the fact that STEcan reveal subclinical LV dysfunction in hearts with appar-ently normal systolic function as measured by EF and thuscould have a role in detecting cardiac involvement in systemicdiseases [44] unusual or rare conditions [45] and also fordetecting early evidence of cardiotoxicity in cancer patientsreceiving chemotherapy [46] At present strain and strainrate imaging remains predominantly research tools but showsconsiderable promise for translation into clinical practiceThe limitations of STE include the requirement of goodimage quality and variability between different software andhardware manufacturers
34 Contrast Echocardiography Ultrasound contrast agents(UCAs) consist of gas-filled microspheres which displayunique acoustic properties when exposed to ultrasoundwaves Contrast bubbles resonate when exposed to an ultra-sound wave This is predominantly a nonlinear oscillation(ie expansion and contraction of the bubble are not equal)at the ultrasound frequencies used in diagnostic imagingMicrobubbles are several million times more effective atscattering sound than red blood cells resulting in a greatlyenhanced ldquoblood poolrdquo signal [47] The blood pool agents
BioMed Research International 7
(a) (b)
(c) (d)Figure 5 Apical 4-chamber images taken before ((a) and (b)) and after ((c) and (d)) ultrasound contrast injection in a patient attending forroutine transthoracic echocardiography At rest endocardial definition at end diastole (a) and end systole (b) was poor and did not permitquantitation of ejection fraction or assessment of regional (segmental) function Following a single bolus injection of contrast endocardialborder visualisation was significantly improved at end diastole (c) and end systole (d) allowing regional and global systolic assessments
developed consist of a gaseous material encapsulated withina stabilizing outer shell These microbubbles are typicallyslightly smaller than erythrocytes allowing free passagewithin the circulation and effectively acting as red cell tracers[48]
The first generation UCAs consisted of air surrounded byan albumin shell [49] Unfortunately these agents had a veryshort lifespan in vivo and thus had limited utility in diagnostictests The second generation of UCAs addressed this issueby changing both components of microbubblesmdashthe air wasreplaced by inert gases with high molecular weight highdensity and low solubility such as sulphur hexafluoride(SonoVue) or perfluorocarbons (eg Optison or Definity)The outer shell is now made using phospholipids which also
confer greater stability They are used to produce a strongerultrasonic signal than that generated by tissues and thus aremost commonly used to improve image quality (Figure 5)
There is ample evidence demonstrating that UCAsimprove estimation of global [50] and regional [51] LV sys-tolic functions UCAs improve the accuracy of measurementof LV volumes and ejection fraction also [52 53] As UCAsimprove overall image quality they also help detect structuralabnormalities such as noncompaction cardiomyopathy [54]apical hypertrophic cardiomyopathy [55] and left ventric-ular thrombus [56] Their biggest use however is in stressechocardiography The use of contrast significantly reducesthe number of ldquouninterpretablerdquo studies [7] and thus is cost-effective as it reduces additional testing [57] This has helped
8 BioMed Research International
establish stress echocardiography as a front-line investigationin assessment of patients with known or suspected coronaryartery disease
The majority (90) of the blood within the myocardialwalls reside within capillaries [58] Thus the intensity of thecontrast signal when the myocardium is fully saturated withcontrast reflects the concentration of microbubbles withinmyocardial capillaries [59] and consequently capillary ormyocardial blood volume Appreciation of this fact led to therecognition that echocardiography could be used to assessmyocardial perfusion a technique now known as myocardialcontrast echocardiography (MCE) A high intensity (highmechanical index) ldquoflashrdquo or impulse is used to destroy themicrobubbles in the myocardial capillaries and their rate ofreplenishment is observed Delayed replenishment manifestsas a perfusion defect and is the hallmark of ischaemia duringMCE The first papers on MCE dates back to three decades[60 61] and since then it has accumulated a large evidencebase to support its use in the detection of CAD [62] Finallyas presence of contrast denotes vascularity UCAs can also beused in patients with intracardiac masses in order to distin-guish between avascularmasses (eg thrombus) and vascularmasses such as tumours [63]
4 lsquolsquoInterventional Echocardiologyrsquorsquo Dawn ofa New Super-Specialty
The advances in 3D echocardiographymdashin particular theadvent of a fully sampled matrix array transducer allowingreal-time 3D-TOEmdashhas brought the echocardiologist to theforefront of catheter-lab-based procedures in structural heartdisease Real-time 3D-TOE is now considered bymany a pre-requisite for guidance of percutaneous treatment of aorticstenosis (transcatheter aortic valve implantation (TAVI))mitral regurgitation (eg MitraClip devices) closure of theleft atrial appendage and of atrial septal defects (ASDs andPFOs) The incremental value of 3D-TOE over 2D-TOEduring TAVI procedures was recently demonstrated in alarge single-centre study [64] Indeed real-time 3D-TOE isexpanding its use further and for example has been usedto guide electrophysiological procedures such as ablation ofatrial flutter and fibrillation (helping reduce significantly theuse of fluoroscopy) [65]
Intracardiac echocardiography (ICE) performed in thecatheter laboratory using single-use percutaneous 2D probesintroduced transvenously (eg via the femoral vein) is alsowidely used to guide interventions [66] Its biggest advantageover TOE is the ability to obtain similar echo views withoutthe need for general anaesthesia with its attendant costs andpotential risks Therefore ICE has been used in preference toTOE for a number of procedures including atrial fibrillation[67] and ventricular tachycardia [68] ablation proceduresclosure of septal defects [69] TAVI procedures [70] and toguide CRT procedures [71] However the significant limita-tion of ICE is expensive given that the probes must be dis-posed of after a single use
The echocardiologist performing such studies needs tohave a sound grasp of normal cardiac and valvular anatomy
and combine quick thinking with speedy manual dexterityThis skill set is not necessarily acquired during conventionaltraining Heshe may be called upon to provide urgent infor-mation in case of sudden unexplained patient deterioration(eg sudden hypotension during TAVI due to entanglementof the delivery system in the mitral subvalvular apparatuscausing acute severe mitral regurgitation) The need for suchindividuals is likely to be restricted to tertiary units butin large centres one can imagine such a person spendinga significant amount of time in the cardiac catheter lab-oratories Appropriate training will be required to ensurethat we produce cardiologists capable of performing suchstudiesmdashhence one can envisage the birth of a super-special-ity of ldquointerventional echocardiologyrdquo
5 Limitations
Echocardiography does have certain limitations which meritdiscussionThe greatest advantage of cross-sectional imaging(ie CMR and CCT) over echocardiography is the informa-tion available on extracardiac structures The aorta aorticarch pulmonary artery and pulmonary veins are far moreclearly seen by these modalities and are often poorly seen ornot seen at all by echocardiography Thus assessment of pul-monary veins in patients awaiting an atrial fibrillation abla-tion procedure assessment of the aortic arch and descendingthoracic aorta in patients with chronic aortic dissection orcoarctation and serial assessment of patients with previouscoarctation repair for example will generally be performedby CMR or CCT
Echocardiography can also suffer from poor image qual-ity despite the use of ultrasound contrast agentsThis is mostoften seen in patientswho are extremely underweight or over-weight but also in patients with chronic airways disease orchest wall deformities (eg pectus excavatum) Patients onintensive care units who are frequently supine and may bemechanically ventilated also often have challenging TTEimages although TOE can resolve such difficulties
6 Conclusion
Echocardiography permits accurate assessment of myocar-dial structure function and perfusion Echocardiography isthus in itself a multimodality imaging technique The fieldof echocardiography is diverse and encompasses numerousindividual techniquesmdashsome with established clinical valuewhilst others showmuch promise in researchThe expandingrole of echocardiography within current clinical practice isunderpinned by continual technological advances and justi-fied by the accumulating evidence of clinical value of thesetechniques when utilised in daily practice
References
[1] L J Shaw T HMarwickW A Zoghbi et al ldquoWhy all the focuson cardiac imagingrdquo JACC Cardiovascular Imaging vol 3 no7 pp 789ndash794 2010
[2] F A Flachskampf L Badano W G Daniel et al ldquoRecommen-dations for transoesophageal echocardiography update 2010rdquo
BioMed Research International 9
European Journal of Echocardiography vol 11 no 7 pp 557ndash5762010
[3] W G Daniel R ErbelW Kasper et al ldquoSafety of transesophag-eal echocardiography A multicenter survey of 10419 examina-tionsrdquo Circulation vol 83 no 3 pp 817ndash821 1991
[4] J N Hilberath D A Oakes S K Shernan B E Bulwer M NDrsquoAmbra and H K Eltzschig ldquoSafety of transesophageal echo-cardiographyrdquo Journal of the American Society of Echocardiog-raphy vol 23 no 11 pp 1115ndash1127 2010
[5] D G Skolnick S G Sawada H Feigenbaum and D S SegarldquoEnhanced endocardial visualization with noncontrast har-monic imaging during stress echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 12 no 7 pp 559ndash5631999
[6] F B Sozzi D Poldermans J J Bax et al ldquoSecond harmonicimaging improves sensitivity of dobutamine stress echocar-diography for the diagnosis of coronary artery diseaserdquo TheAmerican Heart Journal vol 142 no 1 pp 153ndash159 2001
[7] J C Plana I A Mikati H Dokainish et al ldquoA randomizedcross-over study for evaluation of the effect of image optimiza-tion with contrast on the diagnostic accuracy of dobutamineechocardiography in coronary artery disease The OPTIMIZEtrialrdquo JACC Cardiovascular Imaging vol 1 no 2 pp 145ndash1522008
[8] J S Skinner L Smeeth J M Kendall P C Adams and ATimmis ldquoNICE guidance Chest pain of recent onset assess-ment and diagnosis of recent onset chest pain or discomfort ofsuspected cardiac originrdquo Heart vol 96 no 12 pp 974ndash9782010
[9] P Jeetley L Burden B Stoykova and R Senior ldquoClinical andeconomic impact of stress echocardiography compared withexercise electrocardiography in patients with suspected acutecoronary syndrome but negative troponin a prospective ran-domized controlled studyrdquo European Heart Journal vol 28 no2 pp 204ndash211 2007
[10] BN ShahG Balaji A Alhajiri I S Ramzy S Ahmadvazir andR Senior ldquoThe incremental diagnostic and prognostic valueof contemporary stress echocardiography in a chest pain unitmortality and morbidity outcomes from a real-world settingrdquoCirculation Cardiovascular Imaging vol 6 no 2 pp 202ndash2092013
[11] P Lancellotti F LeboisM Simon C Tombeux C Chauvel andL A Pierard ldquoPrognostic importance of quantitative exerciseDoppler echocardiography in asymptomatic valvular aorticstenosisrdquo Circulation vol 112 no 9 supplement pp I377ndashI3822005
[12] S Marechaux Z Hachicha A Bellouin et al ldquoUsefulness ofexercise-stress echocardiography for risk stratification of trueasymptomatic patients with aortic valve stenosisrdquo EuropeanHeart Journal vol 31 no 11 pp 1390ndash1397 2010
[13] P Lancellotti J Magne E Donal et al ldquoDeterminants andprognostic significance of exercise pulmonary hypertension inasymptomatic severe aortic stenosisrdquoCirculation vol 126 no 7pp 851ndash859 2012
[14] JMonin JQuereMMonchi et al ldquoLow-gradient aortic steno-sis Operative risk stratification and predictors for long-termoutcome a multicenter study using dobutamine stress hemo-dynamicsrdquo Circulation vol 108 no 3 pp 319ndash324 2003
[15] L A Pierard and P Lancellotti ldquoThe role of ischemic mitralregurgitation in the pathogenesis of acute pulmonary edemardquoThe New England Journal of Medicine vol 351 no 16 pp 1627ndash1634 2004
[16] J Magne P Lancellotti and L A Pierard ldquoExercise-inducedchanges in degenerative mitral regurgitationrdquo Journal of theAmericanCollege of Cardiology vol 56 no 4 pp 300ndash309 2010
[17] S Bhattacharyya V Kamperidis B N Shah et al ldquo152 Clinicalutility and prognostic value of appropriateness criteria in stressechocardiography for evaluation of valvular heart diseaserdquoHeart vol 99 pp A89ndashA90 2013
[18] B J Gersh B J Maron R O Bonow et al ldquo2011 ACCFAHAguideline for the diagnosis and treatment of hypertrophic cardi-omyopathyrdquo Journal of the American College of Cardiology vol58 no 25 pp e212ndashe260 2011
[19] P Lancellotti M Senechal M Moonen et al ldquoMyocardial con-tractile reserve during exercise predicts left ventricular reverseremodelling after cardiac resynchronization therapyrdquo Euro-pean Journal of Echocardiography vol 10 no 5 pp 663ndash6682009
[20] M Matsumoto M Inoue S Tamura K Tanaka and H AbeldquoThree-dimensional echocardiography for spatial visualizationand volume calculation of cardiac structuresrdquo Journal of ClinicalUltrasound vol 9 no 4 pp 157ndash165 1981
[21] K H Sheikh S W Smith O von Ramm and J Kisslo ldquoReal-time three-dimensional echocardiography feasibility and ini-tial userdquo Echocardiography vol 8 no 1 pp 119ndash125 1991
[22] L Sugeng L Weinert K Thiele and R M Lang ldquoReal-timethree-dimensional echocardiography using a novelmatrix arraytransducerrdquo Echocardiography vol 20 no 7 pp 623ndash635 2003
[23] N P Nikitin C Constantin P H Loh et al ldquoNew generation3-dimensional echocardiography for left ventricular volumetricand functional measurements comparison with cardiac mag-netic resonancerdquo European Journal of Echocardiography vol 7no 5 pp 365ndash372 2006
[24] V Mor-Avi L Sugeng L Weinert et al ldquoFast measurement ofleft ventricular mass with real-time three-dimensional echocar-diography comparison withmagnetic resonance imagingrdquoCir-culation vol 110 no 13 pp 1814ndash1818 2004
[25] L Sugeng V Mor-Avi L Weinert et al ldquoQuantitative assess-ment of left ventricular size and function side-by-side compari-son of real-time three-dimensional echocardiography and com-puted tomography with magnetic resonance referencerdquo Cir-culation vol 114 no 7 pp 654ndash661 2006
[26] S Kapetanakis M T Kearney A Siva N Gall M Cooklinand M J Monaghan ldquoReal-time three-dimensional echocar-diography a novel technique to quantify global left ventricularmechanical dyssynchronyrdquo Circulation vol 112 no 7 pp 992ndash1000 2005
[27] O I I Soliman M L Geleijnse D A M J Theuns et alldquoUsefulness of left ventricular systolic dyssynchrony by real-time three-dimensional echocardiography to predict long-termresponse to cardiac resynchronization therapyrdquo The AmericanJournal of Cardiology vol 103 no 11 pp 1586ndash1591 2009
[28] A V Khaw R S von Bardeleben C Strasser et al ldquoDirect mea-surement of left ventricular outflow tract by transthoracic real-time 3D-echocardiography increases accuracy in assessment ofaortic valve stenosisrdquo International Journal of Cardiology vol136 no 1 pp 64ndash71 2009
[29] L Sugeng S K Shernan I S Salgo et al ldquoLive 3-dimensionaltransesophageal echocardiography Initial experience using thefully-sampled matrix array proberdquo Journal of the American Col-lege of Cardiology vol 52 no 6 pp 446ndash449 2008
[30] D G Gibson T A Prewitt and D J Brown ldquoAnalysis of leftventricular wall movement during isovolumic relaxation and its
10 BioMed Research International
relation to coronary artery diseaserdquo The British Heart Journalvol 38 no 10 pp 1010ndash1019 1976
[31] P Palka A Lange A D Fleming G R Sutherland L N FeenandW NMcDicken ldquoDoppler tissue imaging myocardial wallmotion velocities in normal subjectsrdquo Journal of the AmericanSociety of Echocardiography vol 8 no 5 pp 659ndash668 1995
[32] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressures acomparative simultaneous Doppler-catheterization studyrdquo Cir-culation vol 102 no 15 pp 1788ndash1794 2000
[33] H Blessberger and T Binder ldquoTwo dimensional speckle track-ing echocardiography basic principlesrdquoHeart vol 96 no 9 pp716ndash722 2010
[34] J Gorcsan III and H Tanaka ldquoEchocardiographic assessmentof myocardial strainrdquo Journal of the American College of Cardi-ology vol 58 no 14 pp 1401ndash1413 2011
[35] T H Marwick R L Leano J Brown et al ldquoMyocardial strainmeasurement with 2-dimensional speckle-tracking echocardi-ography Definition of normal rangerdquo JACC CardiovascularImaging vol 2 no 1 pp 80ndash84 2009
[36] A C T Ng M Sitges P N Pham et al ldquoIncrementalvalue of 2-dimensional speckle tracking strain imaging to wallmotion analysis for detection of coronary artery disease inpatients undergoing dobutamine stress echocardiographyrdquoTheAmerican Heart Journal vol 158 no 5 pp 836ndash844 2009
[37] C B Ingul E Rozis S A Slordahl and T H Marwick ldquoIncre-mental value of strain rate imaging to wall motion analysisfor prediction of outcome in patients undergoing dobutaminestress echocardiographyrdquo Circulation vol 115 no 10 pp 1252ndash1259 2007
[38] R Hoffmann E Altiok B Nowak et al ldquoStrain rate measure-ment by Doppler echocardiography allows improved assess-ment of myocardial viability in patients with depressed left ven-tricular functionrdquo Journal of the American College of Cardiologyvol 39 no 3 pp 443ndash449 2002
[39] L Hanekom C Jenkins L Jeffries et al ldquoIncremental valueof strain rate analysis as an adjunct to wall-motion scoring forassessment of myocardial viability by dobutamine echocardio-graphy a follow-up study after revascularizationrdquo Circulationvol 112 no 25 pp 3892ndash3900 2005
[40] H Tanaka H Nesser T Buck et al ldquoDyssynchrony by speckle-tracking echocardiography and response to cardiac resynchro-nization therapy results of the speckle tracking and resynchro-nization (STAR) studyrdquo European Heart Journal vol 31 no 14pp 1690ndash1700 2010
[41] F Z Khan M S Virdee C R Palmer et al ldquoTargeted leftventricular lead placement to guide cardiac resynchronizationtherapy the TARGET study a randomized controlled trialrdquoJournal of the American College of Cardiology vol 59 no 17 pp1509ndash1518 2012
[42] E S Chung A R Leon L Tavazzi et al ldquoResults of the predic-tors of response to CRT (PROSPECT) trialrdquoCirculation vol 117no 20 pp 2608ndash2616 2008
[43] J J Bax and J Gorcsan III ldquoEchocardiography and noninvasiveimaging in cardiac resynchronization therapy Results of thePROSPECT (predictors of response to cardiac resynchroniza-tion therapy) study in perspectiverdquo Journal of the American Col-lege of Cardiology vol 53 no 21 pp 1933ndash1943 2009
[44] B N Shah M de Villa R S Khattar and R Senior ldquoImagingcardiac sarcoidosis the incremental benefit of speckle trackingechocardiographyrdquo Echocardiography 2013
[45] J KramerM Niemann D Liu et al ldquoTwo-dimensional speckletracking as a non-invasive tool for identification of myocardialfibrosis in Fabry diseaserdquoEuropeanHeart Journal vol 34 no 21pp 1587ndash1596 2013
[46] J L Hare J K Brown R Leano C Jenkins N Woodwardand T H Marwick ldquoUse of myocardial deformation imaging todetect preclinical myocardial dysfunction before conventionalmeasures in patients undergoing breast cancer treatment withtrastuzumabrdquo The American Heart Journal vol 158 no 2 pp294ndash301 2009
[47] M J Stewart ldquoContrast echocardiographyrdquoHeart vol 89 no 3pp 342ndash348 2003
[48] R Janardhanan G Dwivedi S Hayat and R Senior ldquoMyocar-dial contrast echocardiography a new tool for assessment ofmyocardial perfusionrdquo Indian Heart Journal vol 57 no 3 pp210ndash216 2005
[49] S B Feinstein F J T Cate W Zwehl et al ldquoTwo-dimensionalcontrast echocardiography I In vitro development and quanti-tative analysis of echo contrast agentsrdquo Journal of the AmericanCollege of Cardiology vol 3 no 1 pp 14ndash20 1984
[50] R Hoffmann S von Bardeleben F T Cate et al ldquoAssessmentof systolic left ventricular function a multi-centre comparisonof cineventriculography cardiac magnetic resonance imagingunenhanced and contrast-enhanced echocardiographyrdquo Euro-pean Heart Journal vol 26 no 6 pp 607ndash616 2005
[51] R Hoffmann S von Bardeleben J D Kasprzak et al ldquoAnalysisof regional left ventricular function by cineventriculographycardiac magnetic resonance imaging and unenhanced andcontrast-enhanced echocardiography a multicenter compari-son of methodsrdquo Journal of the American College of Cardiologyvol 47 no 1 pp 121ndash128 2006
[52] W G Hundley A M Kizilbash I Afridi F Franco R MPeshock and P A Grayburn ldquoAdministration of an intravenousperfluorocarbon contrast agent improves echocardiographicdetermination of left ventricular volumes and ejection fractioncomparison with cine magnetic resonance imagingrdquo Journal ofthe American College of Cardiology vol 32 no 5 pp 1426ndash14321998
[53] S Malm S Frigstad E Sagberg H Larsson and T SkjaerpeldquoAccurate and reproducible measurement of left ventricularvolume and ejection fraction by contrast echocardiography acomparison with magnetic resonance imagingrdquo Journal of theAmerican College of Cardiology vol 44 no 5 pp 1030ndash10352004
[54] B K Koo D Choi J W Ha S M Kang N Chung and S YCho ldquoIsolated noncompaction of the ventricular myocardiumcontrast echocardiographic findings and review of the litera-turerdquo Echocardiography vol 19 no 2 pp 153ndash156 2002
[55] P Soman J Swinburn M Callister N G Stephens and RSenior ldquoApical hypertrophic cardiomyopathy bedside diagno-sis by intravenous contrast echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 14 no 4 pp 311ndash3132001
[56] S Thanigaraj K B Schechtman and J E Perez ldquoImprovedechocardiographic delineation of left ventricular thrombuswith the use of intravenous second-generation contrast imageenhancementrdquo Journal of the American Society of Echocardiog-raphy vol 12 no 12 pp 1022ndash1026 1999
[57] S Thanigaraj R F Nease Jr K B Schechtman R L Wade SLoslo and J E Perez ldquoUse of contrast for image enhancementduring stress echocardiography is cost-effective and reduces
BioMed Research International 11
additional diagnostic testingrdquo The American Journal of Cardi-ology vol 87 no 12 pp 1430ndash1432 2001
[58] S Kaul and A R Jayaweera ldquoCoronary and myocardial bloodvolumes noninvasive tools to assess the coronary microcircu-lationrdquo Circulation vol 96 no 3 pp 719ndash724 1997
[59] K Wei A R Jayaweera S Firoozan A Linka D M Skybaand S Kaul ldquoBasis for detection of stenosis using venousadministration of microbubbles during myocardial contrastechocardiography bolus or continuous infusionrdquo Journal of theAmeri-canCollege of Cardiology vol 32 no 1 pp 252ndash260 1998
[60] W F Armstrong T M Mueller E L Kinney E G Tickner JC Dillon and H Feigenbaum ldquoAssessment of myocardial per-fusion abnormalities with contrast-enhanced two-dimensionalechocardiographyrdquo Circulation vol 66 no 1 pp 166ndash173 1982
[61] C Tei T Sakamaki PM Shah et al ldquoMyocardial contrast echo-cardiography a reproducible technique of myocardial opacifi-cation for identifying regional perfusion deficitsrdquo Circulationvol 67 no 3 pp 585ndash593 1983
[62] R Senior H BecherMMonaghan et al ldquoContrast echocardio-graphy evidence-based recommendations by european associ-ation of echocardiographyrdquo European Journal of Echocardiogra-phy vol 10 no 2 pp 194ndash212 2009
[63] S Bhattacharyya R Khattar andR Senior ldquoCharacterisation ofintra-cardiacmasses bymyocardial contrast echocardiographyrdquoInternational Journal of Cardiology vol 163 no 1 pp e11ndashe132013
[64] L A Smith R Dworakowski A Bhan et al ldquoReal-time three-dimensional transesophageal echocardiography adds value totranscatheter aortic valve implantationrdquo Journal of theAmericanSociety of Echocardiography vol 26 no 4 pp 359ndash369 2013
[65] F Regoli F F Faletra G Nucifora et al ldquoFeasibility and acuteefficacy of radiofrequency ablation of cavotricuspid isthmus-dependent atrial flutter guided by real-time 3D TEErdquo JACCCardiovascular Imaging vol 4 no 7 pp 716ndash726 2011
[66] S S Kim ZM Hijazi R M Lang and B P Knight ldquoThe use ofintracardiac echocardiography and other intracardiac imagingtools to guide noncoronary cardiac interventionsrdquo Journal of theAmerican College of Cardiology vol 53 no 23 pp 2117ndash21282009
[67] JMMangrum J PMounsey L C Kok J P DiMarco andD EHaines ldquoIntracardiac echocardiography-guided anatomicallybased radiofrequency ablation of focal atrial fibrillation origi-nating from pulmonary veinsrdquo Journal of the American Collegeof Cardiology vol 39 no 12 pp 1964ndash1972 2002
[68] R Bala J F Ren M D Hutchinson et al ldquoAssessing epicardialsubstrate using intracardiac echocardiography during VT abla-tionrdquo Circulation Arrhythmia and Electrophysiology vol 4 no5 pp 667ndash673 2011
[69] C Vigna N Marchese M Zanchetta et al ldquoEchocardio-graphic guidance of percutaneous patent foramen ovale closurehead-to-head comparison of transesophageal versus rotationalintracardiac echocardiographyrdquo Echocardiography vol 29 no9 pp 1103ndash1110 2012
[70] T Bartel N Bonaros L Muller et al ldquoIntracardiac echocar-diography a new guiding tool for transcatheter aortic valvereplacementrdquo Journal of the American Society of Echocardiog-raphy vol 24 no 9 pp 966ndash975 2011
[71] R Bai L Di Biase P Mohanty et al ldquoPositioning of left ventric-ular pacing lead guided by intracardiac echocardiography withvector velocity imaging during cardiac resynchronization ther-apy procedurerdquo Journal of Cardiovascular Electrophysiology vol22 no 9 pp 1034ndash1041 2011

6 BioMed Research International
(a) (b)
(c) (d)
Figure 4 Examples of strain imaging using speckle tracking echocardiography On the top row are images from a normal healthy volunteer(apical 4-chamber view on the left and summary strain scores with bulls-eye plot on the right) and on the bottom row are correspondingimages from a patient with severe ischaemic cardiomyopathy Note that the healthy volunteer has normal longitudinal strain in all segmentswith a global strain score of minus189 whereas the cardiomyopathy patient has highly abnormal strains with a significantly depressed globalstrain score of just minus50
it removes the possibility of falsely designating myocardiumas having normal function when ldquovelocityrdquo is in fact due totethering (eg adjacent scar) or translational motion due tomovement of the whole heart (both potential limitations ofTDI [33]) BothTDI and STE can be used tomeasuremyocar-dial strain a dimensionless quantity defined as the unitchange in length of an object relative to its original lengthStrain rate is its derivative with respect to time (ie rate ofchange of strain and usually expressed as 1sec (or secminus1)) Innormal myocardial segments there is shortening in systole(negative strain and strain rates) and lengthening in diastole(positive strain and strain rates) as cardiomyocytes return totheir resting state [33]
A wealth of data has been accumulated on the potentialclinical value of strain and strain rate assessment in a numberof cardiac diseases [34] Normal ranges have also beendefined [35] STE-derived strain imaging has been shownto have additive benefit for detection of CAD in patientsundergoing dobutamine SE [36] and the superior ability ofstrain imaging to predict outcome in patients undergoingdobutamine SE has also been shown [37] Strain imaging is anaccurate technique for detecting viablemyocardium particu-larly when strain parameters are assessed at rest and followinglow-dose dobutamine SE [38 39] Strain imaging has alsobeen studied extensively for detecting dyssynchrony and thuspredicting response to cardiac resynchronisation therapy[40] Recently it was shown that targeted placement of the LVpacing lead to the site of latest mechanical activationmdashaselucidated by STEmdashwas associated with favourable reverseremodelling fewer repeat hospitalizations and improvedfunctional capacity compared to patients with standard
placement of LV leads [41] TDI can also be used to assesscardiac dyssynchrony This has become a controversial topichowever as the PROSPECT trial [42] suggested no echocar-diographic parameter(s) could accurately predict favourableresponse to biventricular pacing though numerous author-ities worldwide were quick to highlight surprisingly funda-mental flaws in the trialrsquos methodology [43]
Potentially of great clinical relevance is the fact that STEcan reveal subclinical LV dysfunction in hearts with appar-ently normal systolic function as measured by EF and thuscould have a role in detecting cardiac involvement in systemicdiseases [44] unusual or rare conditions [45] and also fordetecting early evidence of cardiotoxicity in cancer patientsreceiving chemotherapy [46] At present strain and strainrate imaging remains predominantly research tools but showsconsiderable promise for translation into clinical practiceThe limitations of STE include the requirement of goodimage quality and variability between different software andhardware manufacturers
34 Contrast Echocardiography Ultrasound contrast agents(UCAs) consist of gas-filled microspheres which displayunique acoustic properties when exposed to ultrasoundwaves Contrast bubbles resonate when exposed to an ultra-sound wave This is predominantly a nonlinear oscillation(ie expansion and contraction of the bubble are not equal)at the ultrasound frequencies used in diagnostic imagingMicrobubbles are several million times more effective atscattering sound than red blood cells resulting in a greatlyenhanced ldquoblood poolrdquo signal [47] The blood pool agents
BioMed Research International 7
(a) (b)
(c) (d)Figure 5 Apical 4-chamber images taken before ((a) and (b)) and after ((c) and (d)) ultrasound contrast injection in a patient attending forroutine transthoracic echocardiography At rest endocardial definition at end diastole (a) and end systole (b) was poor and did not permitquantitation of ejection fraction or assessment of regional (segmental) function Following a single bolus injection of contrast endocardialborder visualisation was significantly improved at end diastole (c) and end systole (d) allowing regional and global systolic assessments
developed consist of a gaseous material encapsulated withina stabilizing outer shell These microbubbles are typicallyslightly smaller than erythrocytes allowing free passagewithin the circulation and effectively acting as red cell tracers[48]
The first generation UCAs consisted of air surrounded byan albumin shell [49] Unfortunately these agents had a veryshort lifespan in vivo and thus had limited utility in diagnostictests The second generation of UCAs addressed this issueby changing both components of microbubblesmdashthe air wasreplaced by inert gases with high molecular weight highdensity and low solubility such as sulphur hexafluoride(SonoVue) or perfluorocarbons (eg Optison or Definity)The outer shell is now made using phospholipids which also
confer greater stability They are used to produce a strongerultrasonic signal than that generated by tissues and thus aremost commonly used to improve image quality (Figure 5)
There is ample evidence demonstrating that UCAsimprove estimation of global [50] and regional [51] LV sys-tolic functions UCAs improve the accuracy of measurementof LV volumes and ejection fraction also [52 53] As UCAsimprove overall image quality they also help detect structuralabnormalities such as noncompaction cardiomyopathy [54]apical hypertrophic cardiomyopathy [55] and left ventric-ular thrombus [56] Their biggest use however is in stressechocardiography The use of contrast significantly reducesthe number of ldquouninterpretablerdquo studies [7] and thus is cost-effective as it reduces additional testing [57] This has helped
8 BioMed Research International
establish stress echocardiography as a front-line investigationin assessment of patients with known or suspected coronaryartery disease
The majority (90) of the blood within the myocardialwalls reside within capillaries [58] Thus the intensity of thecontrast signal when the myocardium is fully saturated withcontrast reflects the concentration of microbubbles withinmyocardial capillaries [59] and consequently capillary ormyocardial blood volume Appreciation of this fact led to therecognition that echocardiography could be used to assessmyocardial perfusion a technique now known as myocardialcontrast echocardiography (MCE) A high intensity (highmechanical index) ldquoflashrdquo or impulse is used to destroy themicrobubbles in the myocardial capillaries and their rate ofreplenishment is observed Delayed replenishment manifestsas a perfusion defect and is the hallmark of ischaemia duringMCE The first papers on MCE dates back to three decades[60 61] and since then it has accumulated a large evidencebase to support its use in the detection of CAD [62] Finallyas presence of contrast denotes vascularity UCAs can also beused in patients with intracardiac masses in order to distin-guish between avascularmasses (eg thrombus) and vascularmasses such as tumours [63]
4 lsquolsquoInterventional Echocardiologyrsquorsquo Dawn ofa New Super-Specialty
The advances in 3D echocardiographymdashin particular theadvent of a fully sampled matrix array transducer allowingreal-time 3D-TOEmdashhas brought the echocardiologist to theforefront of catheter-lab-based procedures in structural heartdisease Real-time 3D-TOE is now considered bymany a pre-requisite for guidance of percutaneous treatment of aorticstenosis (transcatheter aortic valve implantation (TAVI))mitral regurgitation (eg MitraClip devices) closure of theleft atrial appendage and of atrial septal defects (ASDs andPFOs) The incremental value of 3D-TOE over 2D-TOEduring TAVI procedures was recently demonstrated in alarge single-centre study [64] Indeed real-time 3D-TOE isexpanding its use further and for example has been usedto guide electrophysiological procedures such as ablation ofatrial flutter and fibrillation (helping reduce significantly theuse of fluoroscopy) [65]
Intracardiac echocardiography (ICE) performed in thecatheter laboratory using single-use percutaneous 2D probesintroduced transvenously (eg via the femoral vein) is alsowidely used to guide interventions [66] Its biggest advantageover TOE is the ability to obtain similar echo views withoutthe need for general anaesthesia with its attendant costs andpotential risks Therefore ICE has been used in preference toTOE for a number of procedures including atrial fibrillation[67] and ventricular tachycardia [68] ablation proceduresclosure of septal defects [69] TAVI procedures [70] and toguide CRT procedures [71] However the significant limita-tion of ICE is expensive given that the probes must be dis-posed of after a single use
The echocardiologist performing such studies needs tohave a sound grasp of normal cardiac and valvular anatomy
and combine quick thinking with speedy manual dexterityThis skill set is not necessarily acquired during conventionaltraining Heshe may be called upon to provide urgent infor-mation in case of sudden unexplained patient deterioration(eg sudden hypotension during TAVI due to entanglementof the delivery system in the mitral subvalvular apparatuscausing acute severe mitral regurgitation) The need for suchindividuals is likely to be restricted to tertiary units butin large centres one can imagine such a person spendinga significant amount of time in the cardiac catheter lab-oratories Appropriate training will be required to ensurethat we produce cardiologists capable of performing suchstudiesmdashhence one can envisage the birth of a super-special-ity of ldquointerventional echocardiologyrdquo
5 Limitations
Echocardiography does have certain limitations which meritdiscussionThe greatest advantage of cross-sectional imaging(ie CMR and CCT) over echocardiography is the informa-tion available on extracardiac structures The aorta aorticarch pulmonary artery and pulmonary veins are far moreclearly seen by these modalities and are often poorly seen ornot seen at all by echocardiography Thus assessment of pul-monary veins in patients awaiting an atrial fibrillation abla-tion procedure assessment of the aortic arch and descendingthoracic aorta in patients with chronic aortic dissection orcoarctation and serial assessment of patients with previouscoarctation repair for example will generally be performedby CMR or CCT
Echocardiography can also suffer from poor image qual-ity despite the use of ultrasound contrast agentsThis is mostoften seen in patientswho are extremely underweight or over-weight but also in patients with chronic airways disease orchest wall deformities (eg pectus excavatum) Patients onintensive care units who are frequently supine and may bemechanically ventilated also often have challenging TTEimages although TOE can resolve such difficulties
6 Conclusion
Echocardiography permits accurate assessment of myocar-dial structure function and perfusion Echocardiography isthus in itself a multimodality imaging technique The fieldof echocardiography is diverse and encompasses numerousindividual techniquesmdashsome with established clinical valuewhilst others showmuch promise in researchThe expandingrole of echocardiography within current clinical practice isunderpinned by continual technological advances and justi-fied by the accumulating evidence of clinical value of thesetechniques when utilised in daily practice
References
[1] L J Shaw T HMarwickW A Zoghbi et al ldquoWhy all the focuson cardiac imagingrdquo JACC Cardiovascular Imaging vol 3 no7 pp 789ndash794 2010
[2] F A Flachskampf L Badano W G Daniel et al ldquoRecommen-dations for transoesophageal echocardiography update 2010rdquo
BioMed Research International 9
European Journal of Echocardiography vol 11 no 7 pp 557ndash5762010
[3] W G Daniel R ErbelW Kasper et al ldquoSafety of transesophag-eal echocardiography A multicenter survey of 10419 examina-tionsrdquo Circulation vol 83 no 3 pp 817ndash821 1991
[4] J N Hilberath D A Oakes S K Shernan B E Bulwer M NDrsquoAmbra and H K Eltzschig ldquoSafety of transesophageal echo-cardiographyrdquo Journal of the American Society of Echocardiog-raphy vol 23 no 11 pp 1115ndash1127 2010
[5] D G Skolnick S G Sawada H Feigenbaum and D S SegarldquoEnhanced endocardial visualization with noncontrast har-monic imaging during stress echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 12 no 7 pp 559ndash5631999
[6] F B Sozzi D Poldermans J J Bax et al ldquoSecond harmonicimaging improves sensitivity of dobutamine stress echocar-diography for the diagnosis of coronary artery diseaserdquo TheAmerican Heart Journal vol 142 no 1 pp 153ndash159 2001
[7] J C Plana I A Mikati H Dokainish et al ldquoA randomizedcross-over study for evaluation of the effect of image optimiza-tion with contrast on the diagnostic accuracy of dobutamineechocardiography in coronary artery disease The OPTIMIZEtrialrdquo JACC Cardiovascular Imaging vol 1 no 2 pp 145ndash1522008
[8] J S Skinner L Smeeth J M Kendall P C Adams and ATimmis ldquoNICE guidance Chest pain of recent onset assess-ment and diagnosis of recent onset chest pain or discomfort ofsuspected cardiac originrdquo Heart vol 96 no 12 pp 974ndash9782010
[9] P Jeetley L Burden B Stoykova and R Senior ldquoClinical andeconomic impact of stress echocardiography compared withexercise electrocardiography in patients with suspected acutecoronary syndrome but negative troponin a prospective ran-domized controlled studyrdquo European Heart Journal vol 28 no2 pp 204ndash211 2007
[10] BN ShahG Balaji A Alhajiri I S Ramzy S Ahmadvazir andR Senior ldquoThe incremental diagnostic and prognostic valueof contemporary stress echocardiography in a chest pain unitmortality and morbidity outcomes from a real-world settingrdquoCirculation Cardiovascular Imaging vol 6 no 2 pp 202ndash2092013
[11] P Lancellotti F LeboisM Simon C Tombeux C Chauvel andL A Pierard ldquoPrognostic importance of quantitative exerciseDoppler echocardiography in asymptomatic valvular aorticstenosisrdquo Circulation vol 112 no 9 supplement pp I377ndashI3822005
[12] S Marechaux Z Hachicha A Bellouin et al ldquoUsefulness ofexercise-stress echocardiography for risk stratification of trueasymptomatic patients with aortic valve stenosisrdquo EuropeanHeart Journal vol 31 no 11 pp 1390ndash1397 2010
[13] P Lancellotti J Magne E Donal et al ldquoDeterminants andprognostic significance of exercise pulmonary hypertension inasymptomatic severe aortic stenosisrdquoCirculation vol 126 no 7pp 851ndash859 2012
[14] JMonin JQuereMMonchi et al ldquoLow-gradient aortic steno-sis Operative risk stratification and predictors for long-termoutcome a multicenter study using dobutamine stress hemo-dynamicsrdquo Circulation vol 108 no 3 pp 319ndash324 2003
[15] L A Pierard and P Lancellotti ldquoThe role of ischemic mitralregurgitation in the pathogenesis of acute pulmonary edemardquoThe New England Journal of Medicine vol 351 no 16 pp 1627ndash1634 2004
[16] J Magne P Lancellotti and L A Pierard ldquoExercise-inducedchanges in degenerative mitral regurgitationrdquo Journal of theAmericanCollege of Cardiology vol 56 no 4 pp 300ndash309 2010
[17] S Bhattacharyya V Kamperidis B N Shah et al ldquo152 Clinicalutility and prognostic value of appropriateness criteria in stressechocardiography for evaluation of valvular heart diseaserdquoHeart vol 99 pp A89ndashA90 2013
[18] B J Gersh B J Maron R O Bonow et al ldquo2011 ACCFAHAguideline for the diagnosis and treatment of hypertrophic cardi-omyopathyrdquo Journal of the American College of Cardiology vol58 no 25 pp e212ndashe260 2011
[19] P Lancellotti M Senechal M Moonen et al ldquoMyocardial con-tractile reserve during exercise predicts left ventricular reverseremodelling after cardiac resynchronization therapyrdquo Euro-pean Journal of Echocardiography vol 10 no 5 pp 663ndash6682009
[20] M Matsumoto M Inoue S Tamura K Tanaka and H AbeldquoThree-dimensional echocardiography for spatial visualizationand volume calculation of cardiac structuresrdquo Journal of ClinicalUltrasound vol 9 no 4 pp 157ndash165 1981
[21] K H Sheikh S W Smith O von Ramm and J Kisslo ldquoReal-time three-dimensional echocardiography feasibility and ini-tial userdquo Echocardiography vol 8 no 1 pp 119ndash125 1991
[22] L Sugeng L Weinert K Thiele and R M Lang ldquoReal-timethree-dimensional echocardiography using a novelmatrix arraytransducerrdquo Echocardiography vol 20 no 7 pp 623ndash635 2003
[23] N P Nikitin C Constantin P H Loh et al ldquoNew generation3-dimensional echocardiography for left ventricular volumetricand functional measurements comparison with cardiac mag-netic resonancerdquo European Journal of Echocardiography vol 7no 5 pp 365ndash372 2006
[24] V Mor-Avi L Sugeng L Weinert et al ldquoFast measurement ofleft ventricular mass with real-time three-dimensional echocar-diography comparison withmagnetic resonance imagingrdquoCir-culation vol 110 no 13 pp 1814ndash1818 2004
[25] L Sugeng V Mor-Avi L Weinert et al ldquoQuantitative assess-ment of left ventricular size and function side-by-side compari-son of real-time three-dimensional echocardiography and com-puted tomography with magnetic resonance referencerdquo Cir-culation vol 114 no 7 pp 654ndash661 2006
[26] S Kapetanakis M T Kearney A Siva N Gall M Cooklinand M J Monaghan ldquoReal-time three-dimensional echocar-diography a novel technique to quantify global left ventricularmechanical dyssynchronyrdquo Circulation vol 112 no 7 pp 992ndash1000 2005
[27] O I I Soliman M L Geleijnse D A M J Theuns et alldquoUsefulness of left ventricular systolic dyssynchrony by real-time three-dimensional echocardiography to predict long-termresponse to cardiac resynchronization therapyrdquo The AmericanJournal of Cardiology vol 103 no 11 pp 1586ndash1591 2009
[28] A V Khaw R S von Bardeleben C Strasser et al ldquoDirect mea-surement of left ventricular outflow tract by transthoracic real-time 3D-echocardiography increases accuracy in assessment ofaortic valve stenosisrdquo International Journal of Cardiology vol136 no 1 pp 64ndash71 2009
[29] L Sugeng S K Shernan I S Salgo et al ldquoLive 3-dimensionaltransesophageal echocardiography Initial experience using thefully-sampled matrix array proberdquo Journal of the American Col-lege of Cardiology vol 52 no 6 pp 446ndash449 2008
[30] D G Gibson T A Prewitt and D J Brown ldquoAnalysis of leftventricular wall movement during isovolumic relaxation and its
10 BioMed Research International
relation to coronary artery diseaserdquo The British Heart Journalvol 38 no 10 pp 1010ndash1019 1976
[31] P Palka A Lange A D Fleming G R Sutherland L N FeenandW NMcDicken ldquoDoppler tissue imaging myocardial wallmotion velocities in normal subjectsrdquo Journal of the AmericanSociety of Echocardiography vol 8 no 5 pp 659ndash668 1995
[32] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressures acomparative simultaneous Doppler-catheterization studyrdquo Cir-culation vol 102 no 15 pp 1788ndash1794 2000
[33] H Blessberger and T Binder ldquoTwo dimensional speckle track-ing echocardiography basic principlesrdquoHeart vol 96 no 9 pp716ndash722 2010
[34] J Gorcsan III and H Tanaka ldquoEchocardiographic assessmentof myocardial strainrdquo Journal of the American College of Cardi-ology vol 58 no 14 pp 1401ndash1413 2011
[35] T H Marwick R L Leano J Brown et al ldquoMyocardial strainmeasurement with 2-dimensional speckle-tracking echocardi-ography Definition of normal rangerdquo JACC CardiovascularImaging vol 2 no 1 pp 80ndash84 2009
[36] A C T Ng M Sitges P N Pham et al ldquoIncrementalvalue of 2-dimensional speckle tracking strain imaging to wallmotion analysis for detection of coronary artery disease inpatients undergoing dobutamine stress echocardiographyrdquoTheAmerican Heart Journal vol 158 no 5 pp 836ndash844 2009
[37] C B Ingul E Rozis S A Slordahl and T H Marwick ldquoIncre-mental value of strain rate imaging to wall motion analysisfor prediction of outcome in patients undergoing dobutaminestress echocardiographyrdquo Circulation vol 115 no 10 pp 1252ndash1259 2007
[38] R Hoffmann E Altiok B Nowak et al ldquoStrain rate measure-ment by Doppler echocardiography allows improved assess-ment of myocardial viability in patients with depressed left ven-tricular functionrdquo Journal of the American College of Cardiologyvol 39 no 3 pp 443ndash449 2002
[39] L Hanekom C Jenkins L Jeffries et al ldquoIncremental valueof strain rate analysis as an adjunct to wall-motion scoring forassessment of myocardial viability by dobutamine echocardio-graphy a follow-up study after revascularizationrdquo Circulationvol 112 no 25 pp 3892ndash3900 2005
[40] H Tanaka H Nesser T Buck et al ldquoDyssynchrony by speckle-tracking echocardiography and response to cardiac resynchro-nization therapy results of the speckle tracking and resynchro-nization (STAR) studyrdquo European Heart Journal vol 31 no 14pp 1690ndash1700 2010
[41] F Z Khan M S Virdee C R Palmer et al ldquoTargeted leftventricular lead placement to guide cardiac resynchronizationtherapy the TARGET study a randomized controlled trialrdquoJournal of the American College of Cardiology vol 59 no 17 pp1509ndash1518 2012
[42] E S Chung A R Leon L Tavazzi et al ldquoResults of the predic-tors of response to CRT (PROSPECT) trialrdquoCirculation vol 117no 20 pp 2608ndash2616 2008
[43] J J Bax and J Gorcsan III ldquoEchocardiography and noninvasiveimaging in cardiac resynchronization therapy Results of thePROSPECT (predictors of response to cardiac resynchroniza-tion therapy) study in perspectiverdquo Journal of the American Col-lege of Cardiology vol 53 no 21 pp 1933ndash1943 2009
[44] B N Shah M de Villa R S Khattar and R Senior ldquoImagingcardiac sarcoidosis the incremental benefit of speckle trackingechocardiographyrdquo Echocardiography 2013
[45] J KramerM Niemann D Liu et al ldquoTwo-dimensional speckletracking as a non-invasive tool for identification of myocardialfibrosis in Fabry diseaserdquoEuropeanHeart Journal vol 34 no 21pp 1587ndash1596 2013
[46] J L Hare J K Brown R Leano C Jenkins N Woodwardand T H Marwick ldquoUse of myocardial deformation imaging todetect preclinical myocardial dysfunction before conventionalmeasures in patients undergoing breast cancer treatment withtrastuzumabrdquo The American Heart Journal vol 158 no 2 pp294ndash301 2009
[47] M J Stewart ldquoContrast echocardiographyrdquoHeart vol 89 no 3pp 342ndash348 2003
[48] R Janardhanan G Dwivedi S Hayat and R Senior ldquoMyocar-dial contrast echocardiography a new tool for assessment ofmyocardial perfusionrdquo Indian Heart Journal vol 57 no 3 pp210ndash216 2005
[49] S B Feinstein F J T Cate W Zwehl et al ldquoTwo-dimensionalcontrast echocardiography I In vitro development and quanti-tative analysis of echo contrast agentsrdquo Journal of the AmericanCollege of Cardiology vol 3 no 1 pp 14ndash20 1984
[50] R Hoffmann S von Bardeleben F T Cate et al ldquoAssessmentof systolic left ventricular function a multi-centre comparisonof cineventriculography cardiac magnetic resonance imagingunenhanced and contrast-enhanced echocardiographyrdquo Euro-pean Heart Journal vol 26 no 6 pp 607ndash616 2005
[51] R Hoffmann S von Bardeleben J D Kasprzak et al ldquoAnalysisof regional left ventricular function by cineventriculographycardiac magnetic resonance imaging and unenhanced andcontrast-enhanced echocardiography a multicenter compari-son of methodsrdquo Journal of the American College of Cardiologyvol 47 no 1 pp 121ndash128 2006
[52] W G Hundley A M Kizilbash I Afridi F Franco R MPeshock and P A Grayburn ldquoAdministration of an intravenousperfluorocarbon contrast agent improves echocardiographicdetermination of left ventricular volumes and ejection fractioncomparison with cine magnetic resonance imagingrdquo Journal ofthe American College of Cardiology vol 32 no 5 pp 1426ndash14321998
[53] S Malm S Frigstad E Sagberg H Larsson and T SkjaerpeldquoAccurate and reproducible measurement of left ventricularvolume and ejection fraction by contrast echocardiography acomparison with magnetic resonance imagingrdquo Journal of theAmerican College of Cardiology vol 44 no 5 pp 1030ndash10352004
[54] B K Koo D Choi J W Ha S M Kang N Chung and S YCho ldquoIsolated noncompaction of the ventricular myocardiumcontrast echocardiographic findings and review of the litera-turerdquo Echocardiography vol 19 no 2 pp 153ndash156 2002
[55] P Soman J Swinburn M Callister N G Stephens and RSenior ldquoApical hypertrophic cardiomyopathy bedside diagno-sis by intravenous contrast echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 14 no 4 pp 311ndash3132001
[56] S Thanigaraj K B Schechtman and J E Perez ldquoImprovedechocardiographic delineation of left ventricular thrombuswith the use of intravenous second-generation contrast imageenhancementrdquo Journal of the American Society of Echocardiog-raphy vol 12 no 12 pp 1022ndash1026 1999
[57] S Thanigaraj R F Nease Jr K B Schechtman R L Wade SLoslo and J E Perez ldquoUse of contrast for image enhancementduring stress echocardiography is cost-effective and reduces
BioMed Research International 11
additional diagnostic testingrdquo The American Journal of Cardi-ology vol 87 no 12 pp 1430ndash1432 2001
[58] S Kaul and A R Jayaweera ldquoCoronary and myocardial bloodvolumes noninvasive tools to assess the coronary microcircu-lationrdquo Circulation vol 96 no 3 pp 719ndash724 1997
[59] K Wei A R Jayaweera S Firoozan A Linka D M Skybaand S Kaul ldquoBasis for detection of stenosis using venousadministration of microbubbles during myocardial contrastechocardiography bolus or continuous infusionrdquo Journal of theAmeri-canCollege of Cardiology vol 32 no 1 pp 252ndash260 1998
[60] W F Armstrong T M Mueller E L Kinney E G Tickner JC Dillon and H Feigenbaum ldquoAssessment of myocardial per-fusion abnormalities with contrast-enhanced two-dimensionalechocardiographyrdquo Circulation vol 66 no 1 pp 166ndash173 1982
[61] C Tei T Sakamaki PM Shah et al ldquoMyocardial contrast echo-cardiography a reproducible technique of myocardial opacifi-cation for identifying regional perfusion deficitsrdquo Circulationvol 67 no 3 pp 585ndash593 1983
[62] R Senior H BecherMMonaghan et al ldquoContrast echocardio-graphy evidence-based recommendations by european associ-ation of echocardiographyrdquo European Journal of Echocardiogra-phy vol 10 no 2 pp 194ndash212 2009
[63] S Bhattacharyya R Khattar andR Senior ldquoCharacterisation ofintra-cardiacmasses bymyocardial contrast echocardiographyrdquoInternational Journal of Cardiology vol 163 no 1 pp e11ndashe132013
[64] L A Smith R Dworakowski A Bhan et al ldquoReal-time three-dimensional transesophageal echocardiography adds value totranscatheter aortic valve implantationrdquo Journal of theAmericanSociety of Echocardiography vol 26 no 4 pp 359ndash369 2013
[65] F Regoli F F Faletra G Nucifora et al ldquoFeasibility and acuteefficacy of radiofrequency ablation of cavotricuspid isthmus-dependent atrial flutter guided by real-time 3D TEErdquo JACCCardiovascular Imaging vol 4 no 7 pp 716ndash726 2011
[66] S S Kim ZM Hijazi R M Lang and B P Knight ldquoThe use ofintracardiac echocardiography and other intracardiac imagingtools to guide noncoronary cardiac interventionsrdquo Journal of theAmerican College of Cardiology vol 53 no 23 pp 2117ndash21282009
[67] JMMangrum J PMounsey L C Kok J P DiMarco andD EHaines ldquoIntracardiac echocardiography-guided anatomicallybased radiofrequency ablation of focal atrial fibrillation origi-nating from pulmonary veinsrdquo Journal of the American Collegeof Cardiology vol 39 no 12 pp 1964ndash1972 2002
[68] R Bala J F Ren M D Hutchinson et al ldquoAssessing epicardialsubstrate using intracardiac echocardiography during VT abla-tionrdquo Circulation Arrhythmia and Electrophysiology vol 4 no5 pp 667ndash673 2011
[69] C Vigna N Marchese M Zanchetta et al ldquoEchocardio-graphic guidance of percutaneous patent foramen ovale closurehead-to-head comparison of transesophageal versus rotationalintracardiac echocardiographyrdquo Echocardiography vol 29 no9 pp 1103ndash1110 2012
[70] T Bartel N Bonaros L Muller et al ldquoIntracardiac echocar-diography a new guiding tool for transcatheter aortic valvereplacementrdquo Journal of the American Society of Echocardiog-raphy vol 24 no 9 pp 966ndash975 2011
[71] R Bai L Di Biase P Mohanty et al ldquoPositioning of left ventric-ular pacing lead guided by intracardiac echocardiography withvector velocity imaging during cardiac resynchronization ther-apy procedurerdquo Journal of Cardiovascular Electrophysiology vol22 no 9 pp 1034ndash1041 2011

BioMed Research International 7
(a) (b)
(c) (d)Figure 5 Apical 4-chamber images taken before ((a) and (b)) and after ((c) and (d)) ultrasound contrast injection in a patient attending forroutine transthoracic echocardiography At rest endocardial definition at end diastole (a) and end systole (b) was poor and did not permitquantitation of ejection fraction or assessment of regional (segmental) function Following a single bolus injection of contrast endocardialborder visualisation was significantly improved at end diastole (c) and end systole (d) allowing regional and global systolic assessments
developed consist of a gaseous material encapsulated withina stabilizing outer shell These microbubbles are typicallyslightly smaller than erythrocytes allowing free passagewithin the circulation and effectively acting as red cell tracers[48]
The first generation UCAs consisted of air surrounded byan albumin shell [49] Unfortunately these agents had a veryshort lifespan in vivo and thus had limited utility in diagnostictests The second generation of UCAs addressed this issueby changing both components of microbubblesmdashthe air wasreplaced by inert gases with high molecular weight highdensity and low solubility such as sulphur hexafluoride(SonoVue) or perfluorocarbons (eg Optison or Definity)The outer shell is now made using phospholipids which also
confer greater stability They are used to produce a strongerultrasonic signal than that generated by tissues and thus aremost commonly used to improve image quality (Figure 5)
There is ample evidence demonstrating that UCAsimprove estimation of global [50] and regional [51] LV sys-tolic functions UCAs improve the accuracy of measurementof LV volumes and ejection fraction also [52 53] As UCAsimprove overall image quality they also help detect structuralabnormalities such as noncompaction cardiomyopathy [54]apical hypertrophic cardiomyopathy [55] and left ventric-ular thrombus [56] Their biggest use however is in stressechocardiography The use of contrast significantly reducesthe number of ldquouninterpretablerdquo studies [7] and thus is cost-effective as it reduces additional testing [57] This has helped
8 BioMed Research International
establish stress echocardiography as a front-line investigationin assessment of patients with known or suspected coronaryartery disease
The majority (90) of the blood within the myocardialwalls reside within capillaries [58] Thus the intensity of thecontrast signal when the myocardium is fully saturated withcontrast reflects the concentration of microbubbles withinmyocardial capillaries [59] and consequently capillary ormyocardial blood volume Appreciation of this fact led to therecognition that echocardiography could be used to assessmyocardial perfusion a technique now known as myocardialcontrast echocardiography (MCE) A high intensity (highmechanical index) ldquoflashrdquo or impulse is used to destroy themicrobubbles in the myocardial capillaries and their rate ofreplenishment is observed Delayed replenishment manifestsas a perfusion defect and is the hallmark of ischaemia duringMCE The first papers on MCE dates back to three decades[60 61] and since then it has accumulated a large evidencebase to support its use in the detection of CAD [62] Finallyas presence of contrast denotes vascularity UCAs can also beused in patients with intracardiac masses in order to distin-guish between avascularmasses (eg thrombus) and vascularmasses such as tumours [63]
4 lsquolsquoInterventional Echocardiologyrsquorsquo Dawn ofa New Super-Specialty
The advances in 3D echocardiographymdashin particular theadvent of a fully sampled matrix array transducer allowingreal-time 3D-TOEmdashhas brought the echocardiologist to theforefront of catheter-lab-based procedures in structural heartdisease Real-time 3D-TOE is now considered bymany a pre-requisite for guidance of percutaneous treatment of aorticstenosis (transcatheter aortic valve implantation (TAVI))mitral regurgitation (eg MitraClip devices) closure of theleft atrial appendage and of atrial septal defects (ASDs andPFOs) The incremental value of 3D-TOE over 2D-TOEduring TAVI procedures was recently demonstrated in alarge single-centre study [64] Indeed real-time 3D-TOE isexpanding its use further and for example has been usedto guide electrophysiological procedures such as ablation ofatrial flutter and fibrillation (helping reduce significantly theuse of fluoroscopy) [65]
Intracardiac echocardiography (ICE) performed in thecatheter laboratory using single-use percutaneous 2D probesintroduced transvenously (eg via the femoral vein) is alsowidely used to guide interventions [66] Its biggest advantageover TOE is the ability to obtain similar echo views withoutthe need for general anaesthesia with its attendant costs andpotential risks Therefore ICE has been used in preference toTOE for a number of procedures including atrial fibrillation[67] and ventricular tachycardia [68] ablation proceduresclosure of septal defects [69] TAVI procedures [70] and toguide CRT procedures [71] However the significant limita-tion of ICE is expensive given that the probes must be dis-posed of after a single use
The echocardiologist performing such studies needs tohave a sound grasp of normal cardiac and valvular anatomy
and combine quick thinking with speedy manual dexterityThis skill set is not necessarily acquired during conventionaltraining Heshe may be called upon to provide urgent infor-mation in case of sudden unexplained patient deterioration(eg sudden hypotension during TAVI due to entanglementof the delivery system in the mitral subvalvular apparatuscausing acute severe mitral regurgitation) The need for suchindividuals is likely to be restricted to tertiary units butin large centres one can imagine such a person spendinga significant amount of time in the cardiac catheter lab-oratories Appropriate training will be required to ensurethat we produce cardiologists capable of performing suchstudiesmdashhence one can envisage the birth of a super-special-ity of ldquointerventional echocardiologyrdquo
5 Limitations
Echocardiography does have certain limitations which meritdiscussionThe greatest advantage of cross-sectional imaging(ie CMR and CCT) over echocardiography is the informa-tion available on extracardiac structures The aorta aorticarch pulmonary artery and pulmonary veins are far moreclearly seen by these modalities and are often poorly seen ornot seen at all by echocardiography Thus assessment of pul-monary veins in patients awaiting an atrial fibrillation abla-tion procedure assessment of the aortic arch and descendingthoracic aorta in patients with chronic aortic dissection orcoarctation and serial assessment of patients with previouscoarctation repair for example will generally be performedby CMR or CCT
Echocardiography can also suffer from poor image qual-ity despite the use of ultrasound contrast agentsThis is mostoften seen in patientswho are extremely underweight or over-weight but also in patients with chronic airways disease orchest wall deformities (eg pectus excavatum) Patients onintensive care units who are frequently supine and may bemechanically ventilated also often have challenging TTEimages although TOE can resolve such difficulties
6 Conclusion
Echocardiography permits accurate assessment of myocar-dial structure function and perfusion Echocardiography isthus in itself a multimodality imaging technique The fieldof echocardiography is diverse and encompasses numerousindividual techniquesmdashsome with established clinical valuewhilst others showmuch promise in researchThe expandingrole of echocardiography within current clinical practice isunderpinned by continual technological advances and justi-fied by the accumulating evidence of clinical value of thesetechniques when utilised in daily practice
References
[1] L J Shaw T HMarwickW A Zoghbi et al ldquoWhy all the focuson cardiac imagingrdquo JACC Cardiovascular Imaging vol 3 no7 pp 789ndash794 2010
[2] F A Flachskampf L Badano W G Daniel et al ldquoRecommen-dations for transoesophageal echocardiography update 2010rdquo
BioMed Research International 9
European Journal of Echocardiography vol 11 no 7 pp 557ndash5762010
[3] W G Daniel R ErbelW Kasper et al ldquoSafety of transesophag-eal echocardiography A multicenter survey of 10419 examina-tionsrdquo Circulation vol 83 no 3 pp 817ndash821 1991
[4] J N Hilberath D A Oakes S K Shernan B E Bulwer M NDrsquoAmbra and H K Eltzschig ldquoSafety of transesophageal echo-cardiographyrdquo Journal of the American Society of Echocardiog-raphy vol 23 no 11 pp 1115ndash1127 2010
[5] D G Skolnick S G Sawada H Feigenbaum and D S SegarldquoEnhanced endocardial visualization with noncontrast har-monic imaging during stress echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 12 no 7 pp 559ndash5631999
[6] F B Sozzi D Poldermans J J Bax et al ldquoSecond harmonicimaging improves sensitivity of dobutamine stress echocar-diography for the diagnosis of coronary artery diseaserdquo TheAmerican Heart Journal vol 142 no 1 pp 153ndash159 2001
[7] J C Plana I A Mikati H Dokainish et al ldquoA randomizedcross-over study for evaluation of the effect of image optimiza-tion with contrast on the diagnostic accuracy of dobutamineechocardiography in coronary artery disease The OPTIMIZEtrialrdquo JACC Cardiovascular Imaging vol 1 no 2 pp 145ndash1522008
[8] J S Skinner L Smeeth J M Kendall P C Adams and ATimmis ldquoNICE guidance Chest pain of recent onset assess-ment and diagnosis of recent onset chest pain or discomfort ofsuspected cardiac originrdquo Heart vol 96 no 12 pp 974ndash9782010
[9] P Jeetley L Burden B Stoykova and R Senior ldquoClinical andeconomic impact of stress echocardiography compared withexercise electrocardiography in patients with suspected acutecoronary syndrome but negative troponin a prospective ran-domized controlled studyrdquo European Heart Journal vol 28 no2 pp 204ndash211 2007
[10] BN ShahG Balaji A Alhajiri I S Ramzy S Ahmadvazir andR Senior ldquoThe incremental diagnostic and prognostic valueof contemporary stress echocardiography in a chest pain unitmortality and morbidity outcomes from a real-world settingrdquoCirculation Cardiovascular Imaging vol 6 no 2 pp 202ndash2092013
[11] P Lancellotti F LeboisM Simon C Tombeux C Chauvel andL A Pierard ldquoPrognostic importance of quantitative exerciseDoppler echocardiography in asymptomatic valvular aorticstenosisrdquo Circulation vol 112 no 9 supplement pp I377ndashI3822005
[12] S Marechaux Z Hachicha A Bellouin et al ldquoUsefulness ofexercise-stress echocardiography for risk stratification of trueasymptomatic patients with aortic valve stenosisrdquo EuropeanHeart Journal vol 31 no 11 pp 1390ndash1397 2010
[13] P Lancellotti J Magne E Donal et al ldquoDeterminants andprognostic significance of exercise pulmonary hypertension inasymptomatic severe aortic stenosisrdquoCirculation vol 126 no 7pp 851ndash859 2012
[14] JMonin JQuereMMonchi et al ldquoLow-gradient aortic steno-sis Operative risk stratification and predictors for long-termoutcome a multicenter study using dobutamine stress hemo-dynamicsrdquo Circulation vol 108 no 3 pp 319ndash324 2003
[15] L A Pierard and P Lancellotti ldquoThe role of ischemic mitralregurgitation in the pathogenesis of acute pulmonary edemardquoThe New England Journal of Medicine vol 351 no 16 pp 1627ndash1634 2004
[16] J Magne P Lancellotti and L A Pierard ldquoExercise-inducedchanges in degenerative mitral regurgitationrdquo Journal of theAmericanCollege of Cardiology vol 56 no 4 pp 300ndash309 2010
[17] S Bhattacharyya V Kamperidis B N Shah et al ldquo152 Clinicalutility and prognostic value of appropriateness criteria in stressechocardiography for evaluation of valvular heart diseaserdquoHeart vol 99 pp A89ndashA90 2013
[18] B J Gersh B J Maron R O Bonow et al ldquo2011 ACCFAHAguideline for the diagnosis and treatment of hypertrophic cardi-omyopathyrdquo Journal of the American College of Cardiology vol58 no 25 pp e212ndashe260 2011
[19] P Lancellotti M Senechal M Moonen et al ldquoMyocardial con-tractile reserve during exercise predicts left ventricular reverseremodelling after cardiac resynchronization therapyrdquo Euro-pean Journal of Echocardiography vol 10 no 5 pp 663ndash6682009
[20] M Matsumoto M Inoue S Tamura K Tanaka and H AbeldquoThree-dimensional echocardiography for spatial visualizationand volume calculation of cardiac structuresrdquo Journal of ClinicalUltrasound vol 9 no 4 pp 157ndash165 1981
[21] K H Sheikh S W Smith O von Ramm and J Kisslo ldquoReal-time three-dimensional echocardiography feasibility and ini-tial userdquo Echocardiography vol 8 no 1 pp 119ndash125 1991
[22] L Sugeng L Weinert K Thiele and R M Lang ldquoReal-timethree-dimensional echocardiography using a novelmatrix arraytransducerrdquo Echocardiography vol 20 no 7 pp 623ndash635 2003
[23] N P Nikitin C Constantin P H Loh et al ldquoNew generation3-dimensional echocardiography for left ventricular volumetricand functional measurements comparison with cardiac mag-netic resonancerdquo European Journal of Echocardiography vol 7no 5 pp 365ndash372 2006
[24] V Mor-Avi L Sugeng L Weinert et al ldquoFast measurement ofleft ventricular mass with real-time three-dimensional echocar-diography comparison withmagnetic resonance imagingrdquoCir-culation vol 110 no 13 pp 1814ndash1818 2004
[25] L Sugeng V Mor-Avi L Weinert et al ldquoQuantitative assess-ment of left ventricular size and function side-by-side compari-son of real-time three-dimensional echocardiography and com-puted tomography with magnetic resonance referencerdquo Cir-culation vol 114 no 7 pp 654ndash661 2006
[26] S Kapetanakis M T Kearney A Siva N Gall M Cooklinand M J Monaghan ldquoReal-time three-dimensional echocar-diography a novel technique to quantify global left ventricularmechanical dyssynchronyrdquo Circulation vol 112 no 7 pp 992ndash1000 2005
[27] O I I Soliman M L Geleijnse D A M J Theuns et alldquoUsefulness of left ventricular systolic dyssynchrony by real-time three-dimensional echocardiography to predict long-termresponse to cardiac resynchronization therapyrdquo The AmericanJournal of Cardiology vol 103 no 11 pp 1586ndash1591 2009
[28] A V Khaw R S von Bardeleben C Strasser et al ldquoDirect mea-surement of left ventricular outflow tract by transthoracic real-time 3D-echocardiography increases accuracy in assessment ofaortic valve stenosisrdquo International Journal of Cardiology vol136 no 1 pp 64ndash71 2009
[29] L Sugeng S K Shernan I S Salgo et al ldquoLive 3-dimensionaltransesophageal echocardiography Initial experience using thefully-sampled matrix array proberdquo Journal of the American Col-lege of Cardiology vol 52 no 6 pp 446ndash449 2008
[30] D G Gibson T A Prewitt and D J Brown ldquoAnalysis of leftventricular wall movement during isovolumic relaxation and its
10 BioMed Research International
relation to coronary artery diseaserdquo The British Heart Journalvol 38 no 10 pp 1010ndash1019 1976
[31] P Palka A Lange A D Fleming G R Sutherland L N FeenandW NMcDicken ldquoDoppler tissue imaging myocardial wallmotion velocities in normal subjectsrdquo Journal of the AmericanSociety of Echocardiography vol 8 no 5 pp 659ndash668 1995
[32] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressures acomparative simultaneous Doppler-catheterization studyrdquo Cir-culation vol 102 no 15 pp 1788ndash1794 2000
[33] H Blessberger and T Binder ldquoTwo dimensional speckle track-ing echocardiography basic principlesrdquoHeart vol 96 no 9 pp716ndash722 2010
[34] J Gorcsan III and H Tanaka ldquoEchocardiographic assessmentof myocardial strainrdquo Journal of the American College of Cardi-ology vol 58 no 14 pp 1401ndash1413 2011
[35] T H Marwick R L Leano J Brown et al ldquoMyocardial strainmeasurement with 2-dimensional speckle-tracking echocardi-ography Definition of normal rangerdquo JACC CardiovascularImaging vol 2 no 1 pp 80ndash84 2009
[36] A C T Ng M Sitges P N Pham et al ldquoIncrementalvalue of 2-dimensional speckle tracking strain imaging to wallmotion analysis for detection of coronary artery disease inpatients undergoing dobutamine stress echocardiographyrdquoTheAmerican Heart Journal vol 158 no 5 pp 836ndash844 2009
[37] C B Ingul E Rozis S A Slordahl and T H Marwick ldquoIncre-mental value of strain rate imaging to wall motion analysisfor prediction of outcome in patients undergoing dobutaminestress echocardiographyrdquo Circulation vol 115 no 10 pp 1252ndash1259 2007
[38] R Hoffmann E Altiok B Nowak et al ldquoStrain rate measure-ment by Doppler echocardiography allows improved assess-ment of myocardial viability in patients with depressed left ven-tricular functionrdquo Journal of the American College of Cardiologyvol 39 no 3 pp 443ndash449 2002
[39] L Hanekom C Jenkins L Jeffries et al ldquoIncremental valueof strain rate analysis as an adjunct to wall-motion scoring forassessment of myocardial viability by dobutamine echocardio-graphy a follow-up study after revascularizationrdquo Circulationvol 112 no 25 pp 3892ndash3900 2005
[40] H Tanaka H Nesser T Buck et al ldquoDyssynchrony by speckle-tracking echocardiography and response to cardiac resynchro-nization therapy results of the speckle tracking and resynchro-nization (STAR) studyrdquo European Heart Journal vol 31 no 14pp 1690ndash1700 2010
[41] F Z Khan M S Virdee C R Palmer et al ldquoTargeted leftventricular lead placement to guide cardiac resynchronizationtherapy the TARGET study a randomized controlled trialrdquoJournal of the American College of Cardiology vol 59 no 17 pp1509ndash1518 2012
[42] E S Chung A R Leon L Tavazzi et al ldquoResults of the predic-tors of response to CRT (PROSPECT) trialrdquoCirculation vol 117no 20 pp 2608ndash2616 2008
[43] J J Bax and J Gorcsan III ldquoEchocardiography and noninvasiveimaging in cardiac resynchronization therapy Results of thePROSPECT (predictors of response to cardiac resynchroniza-tion therapy) study in perspectiverdquo Journal of the American Col-lege of Cardiology vol 53 no 21 pp 1933ndash1943 2009
[44] B N Shah M de Villa R S Khattar and R Senior ldquoImagingcardiac sarcoidosis the incremental benefit of speckle trackingechocardiographyrdquo Echocardiography 2013
[45] J KramerM Niemann D Liu et al ldquoTwo-dimensional speckletracking as a non-invasive tool for identification of myocardialfibrosis in Fabry diseaserdquoEuropeanHeart Journal vol 34 no 21pp 1587ndash1596 2013
[46] J L Hare J K Brown R Leano C Jenkins N Woodwardand T H Marwick ldquoUse of myocardial deformation imaging todetect preclinical myocardial dysfunction before conventionalmeasures in patients undergoing breast cancer treatment withtrastuzumabrdquo The American Heart Journal vol 158 no 2 pp294ndash301 2009
[47] M J Stewart ldquoContrast echocardiographyrdquoHeart vol 89 no 3pp 342ndash348 2003
[48] R Janardhanan G Dwivedi S Hayat and R Senior ldquoMyocar-dial contrast echocardiography a new tool for assessment ofmyocardial perfusionrdquo Indian Heart Journal vol 57 no 3 pp210ndash216 2005
[49] S B Feinstein F J T Cate W Zwehl et al ldquoTwo-dimensionalcontrast echocardiography I In vitro development and quanti-tative analysis of echo contrast agentsrdquo Journal of the AmericanCollege of Cardiology vol 3 no 1 pp 14ndash20 1984
[50] R Hoffmann S von Bardeleben F T Cate et al ldquoAssessmentof systolic left ventricular function a multi-centre comparisonof cineventriculography cardiac magnetic resonance imagingunenhanced and contrast-enhanced echocardiographyrdquo Euro-pean Heart Journal vol 26 no 6 pp 607ndash616 2005
[51] R Hoffmann S von Bardeleben J D Kasprzak et al ldquoAnalysisof regional left ventricular function by cineventriculographycardiac magnetic resonance imaging and unenhanced andcontrast-enhanced echocardiography a multicenter compari-son of methodsrdquo Journal of the American College of Cardiologyvol 47 no 1 pp 121ndash128 2006
[52] W G Hundley A M Kizilbash I Afridi F Franco R MPeshock and P A Grayburn ldquoAdministration of an intravenousperfluorocarbon contrast agent improves echocardiographicdetermination of left ventricular volumes and ejection fractioncomparison with cine magnetic resonance imagingrdquo Journal ofthe American College of Cardiology vol 32 no 5 pp 1426ndash14321998
[53] S Malm S Frigstad E Sagberg H Larsson and T SkjaerpeldquoAccurate and reproducible measurement of left ventricularvolume and ejection fraction by contrast echocardiography acomparison with magnetic resonance imagingrdquo Journal of theAmerican College of Cardiology vol 44 no 5 pp 1030ndash10352004
[54] B K Koo D Choi J W Ha S M Kang N Chung and S YCho ldquoIsolated noncompaction of the ventricular myocardiumcontrast echocardiographic findings and review of the litera-turerdquo Echocardiography vol 19 no 2 pp 153ndash156 2002
[55] P Soman J Swinburn M Callister N G Stephens and RSenior ldquoApical hypertrophic cardiomyopathy bedside diagno-sis by intravenous contrast echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 14 no 4 pp 311ndash3132001
[56] S Thanigaraj K B Schechtman and J E Perez ldquoImprovedechocardiographic delineation of left ventricular thrombuswith the use of intravenous second-generation contrast imageenhancementrdquo Journal of the American Society of Echocardiog-raphy vol 12 no 12 pp 1022ndash1026 1999
[57] S Thanigaraj R F Nease Jr K B Schechtman R L Wade SLoslo and J E Perez ldquoUse of contrast for image enhancementduring stress echocardiography is cost-effective and reduces
BioMed Research International 11
additional diagnostic testingrdquo The American Journal of Cardi-ology vol 87 no 12 pp 1430ndash1432 2001
[58] S Kaul and A R Jayaweera ldquoCoronary and myocardial bloodvolumes noninvasive tools to assess the coronary microcircu-lationrdquo Circulation vol 96 no 3 pp 719ndash724 1997
[59] K Wei A R Jayaweera S Firoozan A Linka D M Skybaand S Kaul ldquoBasis for detection of stenosis using venousadministration of microbubbles during myocardial contrastechocardiography bolus or continuous infusionrdquo Journal of theAmeri-canCollege of Cardiology vol 32 no 1 pp 252ndash260 1998
[60] W F Armstrong T M Mueller E L Kinney E G Tickner JC Dillon and H Feigenbaum ldquoAssessment of myocardial per-fusion abnormalities with contrast-enhanced two-dimensionalechocardiographyrdquo Circulation vol 66 no 1 pp 166ndash173 1982
[61] C Tei T Sakamaki PM Shah et al ldquoMyocardial contrast echo-cardiography a reproducible technique of myocardial opacifi-cation for identifying regional perfusion deficitsrdquo Circulationvol 67 no 3 pp 585ndash593 1983
[62] R Senior H BecherMMonaghan et al ldquoContrast echocardio-graphy evidence-based recommendations by european associ-ation of echocardiographyrdquo European Journal of Echocardiogra-phy vol 10 no 2 pp 194ndash212 2009
[63] S Bhattacharyya R Khattar andR Senior ldquoCharacterisation ofintra-cardiacmasses bymyocardial contrast echocardiographyrdquoInternational Journal of Cardiology vol 163 no 1 pp e11ndashe132013
[64] L A Smith R Dworakowski A Bhan et al ldquoReal-time three-dimensional transesophageal echocardiography adds value totranscatheter aortic valve implantationrdquo Journal of theAmericanSociety of Echocardiography vol 26 no 4 pp 359ndash369 2013
[65] F Regoli F F Faletra G Nucifora et al ldquoFeasibility and acuteefficacy of radiofrequency ablation of cavotricuspid isthmus-dependent atrial flutter guided by real-time 3D TEErdquo JACCCardiovascular Imaging vol 4 no 7 pp 716ndash726 2011
[66] S S Kim ZM Hijazi R M Lang and B P Knight ldquoThe use ofintracardiac echocardiography and other intracardiac imagingtools to guide noncoronary cardiac interventionsrdquo Journal of theAmerican College of Cardiology vol 53 no 23 pp 2117ndash21282009
[67] JMMangrum J PMounsey L C Kok J P DiMarco andD EHaines ldquoIntracardiac echocardiography-guided anatomicallybased radiofrequency ablation of focal atrial fibrillation origi-nating from pulmonary veinsrdquo Journal of the American Collegeof Cardiology vol 39 no 12 pp 1964ndash1972 2002
[68] R Bala J F Ren M D Hutchinson et al ldquoAssessing epicardialsubstrate using intracardiac echocardiography during VT abla-tionrdquo Circulation Arrhythmia and Electrophysiology vol 4 no5 pp 667ndash673 2011
[69] C Vigna N Marchese M Zanchetta et al ldquoEchocardio-graphic guidance of percutaneous patent foramen ovale closurehead-to-head comparison of transesophageal versus rotationalintracardiac echocardiographyrdquo Echocardiography vol 29 no9 pp 1103ndash1110 2012
[70] T Bartel N Bonaros L Muller et al ldquoIntracardiac echocar-diography a new guiding tool for transcatheter aortic valvereplacementrdquo Journal of the American Society of Echocardiog-raphy vol 24 no 9 pp 966ndash975 2011
[71] R Bai L Di Biase P Mohanty et al ldquoPositioning of left ventric-ular pacing lead guided by intracardiac echocardiography withvector velocity imaging during cardiac resynchronization ther-apy procedurerdquo Journal of Cardiovascular Electrophysiology vol22 no 9 pp 1034ndash1041 2011

8 BioMed Research International
establish stress echocardiography as a front-line investigationin assessment of patients with known or suspected coronaryartery disease
The majority (90) of the blood within the myocardialwalls reside within capillaries [58] Thus the intensity of thecontrast signal when the myocardium is fully saturated withcontrast reflects the concentration of microbubbles withinmyocardial capillaries [59] and consequently capillary ormyocardial blood volume Appreciation of this fact led to therecognition that echocardiography could be used to assessmyocardial perfusion a technique now known as myocardialcontrast echocardiography (MCE) A high intensity (highmechanical index) ldquoflashrdquo or impulse is used to destroy themicrobubbles in the myocardial capillaries and their rate ofreplenishment is observed Delayed replenishment manifestsas a perfusion defect and is the hallmark of ischaemia duringMCE The first papers on MCE dates back to three decades[60 61] and since then it has accumulated a large evidencebase to support its use in the detection of CAD [62] Finallyas presence of contrast denotes vascularity UCAs can also beused in patients with intracardiac masses in order to distin-guish between avascularmasses (eg thrombus) and vascularmasses such as tumours [63]
4 lsquolsquoInterventional Echocardiologyrsquorsquo Dawn ofa New Super-Specialty
The advances in 3D echocardiographymdashin particular theadvent of a fully sampled matrix array transducer allowingreal-time 3D-TOEmdashhas brought the echocardiologist to theforefront of catheter-lab-based procedures in structural heartdisease Real-time 3D-TOE is now considered bymany a pre-requisite for guidance of percutaneous treatment of aorticstenosis (transcatheter aortic valve implantation (TAVI))mitral regurgitation (eg MitraClip devices) closure of theleft atrial appendage and of atrial septal defects (ASDs andPFOs) The incremental value of 3D-TOE over 2D-TOEduring TAVI procedures was recently demonstrated in alarge single-centre study [64] Indeed real-time 3D-TOE isexpanding its use further and for example has been usedto guide electrophysiological procedures such as ablation ofatrial flutter and fibrillation (helping reduce significantly theuse of fluoroscopy) [65]
Intracardiac echocardiography (ICE) performed in thecatheter laboratory using single-use percutaneous 2D probesintroduced transvenously (eg via the femoral vein) is alsowidely used to guide interventions [66] Its biggest advantageover TOE is the ability to obtain similar echo views withoutthe need for general anaesthesia with its attendant costs andpotential risks Therefore ICE has been used in preference toTOE for a number of procedures including atrial fibrillation[67] and ventricular tachycardia [68] ablation proceduresclosure of septal defects [69] TAVI procedures [70] and toguide CRT procedures [71] However the significant limita-tion of ICE is expensive given that the probes must be dis-posed of after a single use
The echocardiologist performing such studies needs tohave a sound grasp of normal cardiac and valvular anatomy
and combine quick thinking with speedy manual dexterityThis skill set is not necessarily acquired during conventionaltraining Heshe may be called upon to provide urgent infor-mation in case of sudden unexplained patient deterioration(eg sudden hypotension during TAVI due to entanglementof the delivery system in the mitral subvalvular apparatuscausing acute severe mitral regurgitation) The need for suchindividuals is likely to be restricted to tertiary units butin large centres one can imagine such a person spendinga significant amount of time in the cardiac catheter lab-oratories Appropriate training will be required to ensurethat we produce cardiologists capable of performing suchstudiesmdashhence one can envisage the birth of a super-special-ity of ldquointerventional echocardiologyrdquo
5 Limitations
Echocardiography does have certain limitations which meritdiscussionThe greatest advantage of cross-sectional imaging(ie CMR and CCT) over echocardiography is the informa-tion available on extracardiac structures The aorta aorticarch pulmonary artery and pulmonary veins are far moreclearly seen by these modalities and are often poorly seen ornot seen at all by echocardiography Thus assessment of pul-monary veins in patients awaiting an atrial fibrillation abla-tion procedure assessment of the aortic arch and descendingthoracic aorta in patients with chronic aortic dissection orcoarctation and serial assessment of patients with previouscoarctation repair for example will generally be performedby CMR or CCT
Echocardiography can also suffer from poor image qual-ity despite the use of ultrasound contrast agentsThis is mostoften seen in patientswho are extremely underweight or over-weight but also in patients with chronic airways disease orchest wall deformities (eg pectus excavatum) Patients onintensive care units who are frequently supine and may bemechanically ventilated also often have challenging TTEimages although TOE can resolve such difficulties
6 Conclusion
Echocardiography permits accurate assessment of myocar-dial structure function and perfusion Echocardiography isthus in itself a multimodality imaging technique The fieldof echocardiography is diverse and encompasses numerousindividual techniquesmdashsome with established clinical valuewhilst others showmuch promise in researchThe expandingrole of echocardiography within current clinical practice isunderpinned by continual technological advances and justi-fied by the accumulating evidence of clinical value of thesetechniques when utilised in daily practice
References
[1] L J Shaw T HMarwickW A Zoghbi et al ldquoWhy all the focuson cardiac imagingrdquo JACC Cardiovascular Imaging vol 3 no7 pp 789ndash794 2010
[2] F A Flachskampf L Badano W G Daniel et al ldquoRecommen-dations for transoesophageal echocardiography update 2010rdquo
BioMed Research International 9
European Journal of Echocardiography vol 11 no 7 pp 557ndash5762010
[3] W G Daniel R ErbelW Kasper et al ldquoSafety of transesophag-eal echocardiography A multicenter survey of 10419 examina-tionsrdquo Circulation vol 83 no 3 pp 817ndash821 1991
[4] J N Hilberath D A Oakes S K Shernan B E Bulwer M NDrsquoAmbra and H K Eltzschig ldquoSafety of transesophageal echo-cardiographyrdquo Journal of the American Society of Echocardiog-raphy vol 23 no 11 pp 1115ndash1127 2010
[5] D G Skolnick S G Sawada H Feigenbaum and D S SegarldquoEnhanced endocardial visualization with noncontrast har-monic imaging during stress echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 12 no 7 pp 559ndash5631999
[6] F B Sozzi D Poldermans J J Bax et al ldquoSecond harmonicimaging improves sensitivity of dobutamine stress echocar-diography for the diagnosis of coronary artery diseaserdquo TheAmerican Heart Journal vol 142 no 1 pp 153ndash159 2001
[7] J C Plana I A Mikati H Dokainish et al ldquoA randomizedcross-over study for evaluation of the effect of image optimiza-tion with contrast on the diagnostic accuracy of dobutamineechocardiography in coronary artery disease The OPTIMIZEtrialrdquo JACC Cardiovascular Imaging vol 1 no 2 pp 145ndash1522008
[8] J S Skinner L Smeeth J M Kendall P C Adams and ATimmis ldquoNICE guidance Chest pain of recent onset assess-ment and diagnosis of recent onset chest pain or discomfort ofsuspected cardiac originrdquo Heart vol 96 no 12 pp 974ndash9782010
[9] P Jeetley L Burden B Stoykova and R Senior ldquoClinical andeconomic impact of stress echocardiography compared withexercise electrocardiography in patients with suspected acutecoronary syndrome but negative troponin a prospective ran-domized controlled studyrdquo European Heart Journal vol 28 no2 pp 204ndash211 2007
[10] BN ShahG Balaji A Alhajiri I S Ramzy S Ahmadvazir andR Senior ldquoThe incremental diagnostic and prognostic valueof contemporary stress echocardiography in a chest pain unitmortality and morbidity outcomes from a real-world settingrdquoCirculation Cardiovascular Imaging vol 6 no 2 pp 202ndash2092013
[11] P Lancellotti F LeboisM Simon C Tombeux C Chauvel andL A Pierard ldquoPrognostic importance of quantitative exerciseDoppler echocardiography in asymptomatic valvular aorticstenosisrdquo Circulation vol 112 no 9 supplement pp I377ndashI3822005
[12] S Marechaux Z Hachicha A Bellouin et al ldquoUsefulness ofexercise-stress echocardiography for risk stratification of trueasymptomatic patients with aortic valve stenosisrdquo EuropeanHeart Journal vol 31 no 11 pp 1390ndash1397 2010
[13] P Lancellotti J Magne E Donal et al ldquoDeterminants andprognostic significance of exercise pulmonary hypertension inasymptomatic severe aortic stenosisrdquoCirculation vol 126 no 7pp 851ndash859 2012
[14] JMonin JQuereMMonchi et al ldquoLow-gradient aortic steno-sis Operative risk stratification and predictors for long-termoutcome a multicenter study using dobutamine stress hemo-dynamicsrdquo Circulation vol 108 no 3 pp 319ndash324 2003
[15] L A Pierard and P Lancellotti ldquoThe role of ischemic mitralregurgitation in the pathogenesis of acute pulmonary edemardquoThe New England Journal of Medicine vol 351 no 16 pp 1627ndash1634 2004
[16] J Magne P Lancellotti and L A Pierard ldquoExercise-inducedchanges in degenerative mitral regurgitationrdquo Journal of theAmericanCollege of Cardiology vol 56 no 4 pp 300ndash309 2010
[17] S Bhattacharyya V Kamperidis B N Shah et al ldquo152 Clinicalutility and prognostic value of appropriateness criteria in stressechocardiography for evaluation of valvular heart diseaserdquoHeart vol 99 pp A89ndashA90 2013
[18] B J Gersh B J Maron R O Bonow et al ldquo2011 ACCFAHAguideline for the diagnosis and treatment of hypertrophic cardi-omyopathyrdquo Journal of the American College of Cardiology vol58 no 25 pp e212ndashe260 2011
[19] P Lancellotti M Senechal M Moonen et al ldquoMyocardial con-tractile reserve during exercise predicts left ventricular reverseremodelling after cardiac resynchronization therapyrdquo Euro-pean Journal of Echocardiography vol 10 no 5 pp 663ndash6682009
[20] M Matsumoto M Inoue S Tamura K Tanaka and H AbeldquoThree-dimensional echocardiography for spatial visualizationand volume calculation of cardiac structuresrdquo Journal of ClinicalUltrasound vol 9 no 4 pp 157ndash165 1981
[21] K H Sheikh S W Smith O von Ramm and J Kisslo ldquoReal-time three-dimensional echocardiography feasibility and ini-tial userdquo Echocardiography vol 8 no 1 pp 119ndash125 1991
[22] L Sugeng L Weinert K Thiele and R M Lang ldquoReal-timethree-dimensional echocardiography using a novelmatrix arraytransducerrdquo Echocardiography vol 20 no 7 pp 623ndash635 2003
[23] N P Nikitin C Constantin P H Loh et al ldquoNew generation3-dimensional echocardiography for left ventricular volumetricand functional measurements comparison with cardiac mag-netic resonancerdquo European Journal of Echocardiography vol 7no 5 pp 365ndash372 2006
[24] V Mor-Avi L Sugeng L Weinert et al ldquoFast measurement ofleft ventricular mass with real-time three-dimensional echocar-diography comparison withmagnetic resonance imagingrdquoCir-culation vol 110 no 13 pp 1814ndash1818 2004
[25] L Sugeng V Mor-Avi L Weinert et al ldquoQuantitative assess-ment of left ventricular size and function side-by-side compari-son of real-time three-dimensional echocardiography and com-puted tomography with magnetic resonance referencerdquo Cir-culation vol 114 no 7 pp 654ndash661 2006
[26] S Kapetanakis M T Kearney A Siva N Gall M Cooklinand M J Monaghan ldquoReal-time three-dimensional echocar-diography a novel technique to quantify global left ventricularmechanical dyssynchronyrdquo Circulation vol 112 no 7 pp 992ndash1000 2005
[27] O I I Soliman M L Geleijnse D A M J Theuns et alldquoUsefulness of left ventricular systolic dyssynchrony by real-time three-dimensional echocardiography to predict long-termresponse to cardiac resynchronization therapyrdquo The AmericanJournal of Cardiology vol 103 no 11 pp 1586ndash1591 2009
[28] A V Khaw R S von Bardeleben C Strasser et al ldquoDirect mea-surement of left ventricular outflow tract by transthoracic real-time 3D-echocardiography increases accuracy in assessment ofaortic valve stenosisrdquo International Journal of Cardiology vol136 no 1 pp 64ndash71 2009
[29] L Sugeng S K Shernan I S Salgo et al ldquoLive 3-dimensionaltransesophageal echocardiography Initial experience using thefully-sampled matrix array proberdquo Journal of the American Col-lege of Cardiology vol 52 no 6 pp 446ndash449 2008
[30] D G Gibson T A Prewitt and D J Brown ldquoAnalysis of leftventricular wall movement during isovolumic relaxation and its
10 BioMed Research International
relation to coronary artery diseaserdquo The British Heart Journalvol 38 no 10 pp 1010ndash1019 1976
[31] P Palka A Lange A D Fleming G R Sutherland L N FeenandW NMcDicken ldquoDoppler tissue imaging myocardial wallmotion velocities in normal subjectsrdquo Journal of the AmericanSociety of Echocardiography vol 8 no 5 pp 659ndash668 1995
[32] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressures acomparative simultaneous Doppler-catheterization studyrdquo Cir-culation vol 102 no 15 pp 1788ndash1794 2000
[33] H Blessberger and T Binder ldquoTwo dimensional speckle track-ing echocardiography basic principlesrdquoHeart vol 96 no 9 pp716ndash722 2010
[34] J Gorcsan III and H Tanaka ldquoEchocardiographic assessmentof myocardial strainrdquo Journal of the American College of Cardi-ology vol 58 no 14 pp 1401ndash1413 2011
[35] T H Marwick R L Leano J Brown et al ldquoMyocardial strainmeasurement with 2-dimensional speckle-tracking echocardi-ography Definition of normal rangerdquo JACC CardiovascularImaging vol 2 no 1 pp 80ndash84 2009
[36] A C T Ng M Sitges P N Pham et al ldquoIncrementalvalue of 2-dimensional speckle tracking strain imaging to wallmotion analysis for detection of coronary artery disease inpatients undergoing dobutamine stress echocardiographyrdquoTheAmerican Heart Journal vol 158 no 5 pp 836ndash844 2009
[37] C B Ingul E Rozis S A Slordahl and T H Marwick ldquoIncre-mental value of strain rate imaging to wall motion analysisfor prediction of outcome in patients undergoing dobutaminestress echocardiographyrdquo Circulation vol 115 no 10 pp 1252ndash1259 2007
[38] R Hoffmann E Altiok B Nowak et al ldquoStrain rate measure-ment by Doppler echocardiography allows improved assess-ment of myocardial viability in patients with depressed left ven-tricular functionrdquo Journal of the American College of Cardiologyvol 39 no 3 pp 443ndash449 2002
[39] L Hanekom C Jenkins L Jeffries et al ldquoIncremental valueof strain rate analysis as an adjunct to wall-motion scoring forassessment of myocardial viability by dobutamine echocardio-graphy a follow-up study after revascularizationrdquo Circulationvol 112 no 25 pp 3892ndash3900 2005
[40] H Tanaka H Nesser T Buck et al ldquoDyssynchrony by speckle-tracking echocardiography and response to cardiac resynchro-nization therapy results of the speckle tracking and resynchro-nization (STAR) studyrdquo European Heart Journal vol 31 no 14pp 1690ndash1700 2010
[41] F Z Khan M S Virdee C R Palmer et al ldquoTargeted leftventricular lead placement to guide cardiac resynchronizationtherapy the TARGET study a randomized controlled trialrdquoJournal of the American College of Cardiology vol 59 no 17 pp1509ndash1518 2012
[42] E S Chung A R Leon L Tavazzi et al ldquoResults of the predic-tors of response to CRT (PROSPECT) trialrdquoCirculation vol 117no 20 pp 2608ndash2616 2008
[43] J J Bax and J Gorcsan III ldquoEchocardiography and noninvasiveimaging in cardiac resynchronization therapy Results of thePROSPECT (predictors of response to cardiac resynchroniza-tion therapy) study in perspectiverdquo Journal of the American Col-lege of Cardiology vol 53 no 21 pp 1933ndash1943 2009
[44] B N Shah M de Villa R S Khattar and R Senior ldquoImagingcardiac sarcoidosis the incremental benefit of speckle trackingechocardiographyrdquo Echocardiography 2013
[45] J KramerM Niemann D Liu et al ldquoTwo-dimensional speckletracking as a non-invasive tool for identification of myocardialfibrosis in Fabry diseaserdquoEuropeanHeart Journal vol 34 no 21pp 1587ndash1596 2013
[46] J L Hare J K Brown R Leano C Jenkins N Woodwardand T H Marwick ldquoUse of myocardial deformation imaging todetect preclinical myocardial dysfunction before conventionalmeasures in patients undergoing breast cancer treatment withtrastuzumabrdquo The American Heart Journal vol 158 no 2 pp294ndash301 2009
[47] M J Stewart ldquoContrast echocardiographyrdquoHeart vol 89 no 3pp 342ndash348 2003
[48] R Janardhanan G Dwivedi S Hayat and R Senior ldquoMyocar-dial contrast echocardiography a new tool for assessment ofmyocardial perfusionrdquo Indian Heart Journal vol 57 no 3 pp210ndash216 2005
[49] S B Feinstein F J T Cate W Zwehl et al ldquoTwo-dimensionalcontrast echocardiography I In vitro development and quanti-tative analysis of echo contrast agentsrdquo Journal of the AmericanCollege of Cardiology vol 3 no 1 pp 14ndash20 1984
[50] R Hoffmann S von Bardeleben F T Cate et al ldquoAssessmentof systolic left ventricular function a multi-centre comparisonof cineventriculography cardiac magnetic resonance imagingunenhanced and contrast-enhanced echocardiographyrdquo Euro-pean Heart Journal vol 26 no 6 pp 607ndash616 2005
[51] R Hoffmann S von Bardeleben J D Kasprzak et al ldquoAnalysisof regional left ventricular function by cineventriculographycardiac magnetic resonance imaging and unenhanced andcontrast-enhanced echocardiography a multicenter compari-son of methodsrdquo Journal of the American College of Cardiologyvol 47 no 1 pp 121ndash128 2006
[52] W G Hundley A M Kizilbash I Afridi F Franco R MPeshock and P A Grayburn ldquoAdministration of an intravenousperfluorocarbon contrast agent improves echocardiographicdetermination of left ventricular volumes and ejection fractioncomparison with cine magnetic resonance imagingrdquo Journal ofthe American College of Cardiology vol 32 no 5 pp 1426ndash14321998
[53] S Malm S Frigstad E Sagberg H Larsson and T SkjaerpeldquoAccurate and reproducible measurement of left ventricularvolume and ejection fraction by contrast echocardiography acomparison with magnetic resonance imagingrdquo Journal of theAmerican College of Cardiology vol 44 no 5 pp 1030ndash10352004
[54] B K Koo D Choi J W Ha S M Kang N Chung and S YCho ldquoIsolated noncompaction of the ventricular myocardiumcontrast echocardiographic findings and review of the litera-turerdquo Echocardiography vol 19 no 2 pp 153ndash156 2002
[55] P Soman J Swinburn M Callister N G Stephens and RSenior ldquoApical hypertrophic cardiomyopathy bedside diagno-sis by intravenous contrast echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 14 no 4 pp 311ndash3132001
[56] S Thanigaraj K B Schechtman and J E Perez ldquoImprovedechocardiographic delineation of left ventricular thrombuswith the use of intravenous second-generation contrast imageenhancementrdquo Journal of the American Society of Echocardiog-raphy vol 12 no 12 pp 1022ndash1026 1999
[57] S Thanigaraj R F Nease Jr K B Schechtman R L Wade SLoslo and J E Perez ldquoUse of contrast for image enhancementduring stress echocardiography is cost-effective and reduces
BioMed Research International 11
additional diagnostic testingrdquo The American Journal of Cardi-ology vol 87 no 12 pp 1430ndash1432 2001
[58] S Kaul and A R Jayaweera ldquoCoronary and myocardial bloodvolumes noninvasive tools to assess the coronary microcircu-lationrdquo Circulation vol 96 no 3 pp 719ndash724 1997
[59] K Wei A R Jayaweera S Firoozan A Linka D M Skybaand S Kaul ldquoBasis for detection of stenosis using venousadministration of microbubbles during myocardial contrastechocardiography bolus or continuous infusionrdquo Journal of theAmeri-canCollege of Cardiology vol 32 no 1 pp 252ndash260 1998
[60] W F Armstrong T M Mueller E L Kinney E G Tickner JC Dillon and H Feigenbaum ldquoAssessment of myocardial per-fusion abnormalities with contrast-enhanced two-dimensionalechocardiographyrdquo Circulation vol 66 no 1 pp 166ndash173 1982
[61] C Tei T Sakamaki PM Shah et al ldquoMyocardial contrast echo-cardiography a reproducible technique of myocardial opacifi-cation for identifying regional perfusion deficitsrdquo Circulationvol 67 no 3 pp 585ndash593 1983
[62] R Senior H BecherMMonaghan et al ldquoContrast echocardio-graphy evidence-based recommendations by european associ-ation of echocardiographyrdquo European Journal of Echocardiogra-phy vol 10 no 2 pp 194ndash212 2009
[63] S Bhattacharyya R Khattar andR Senior ldquoCharacterisation ofintra-cardiacmasses bymyocardial contrast echocardiographyrdquoInternational Journal of Cardiology vol 163 no 1 pp e11ndashe132013
[64] L A Smith R Dworakowski A Bhan et al ldquoReal-time three-dimensional transesophageal echocardiography adds value totranscatheter aortic valve implantationrdquo Journal of theAmericanSociety of Echocardiography vol 26 no 4 pp 359ndash369 2013
[65] F Regoli F F Faletra G Nucifora et al ldquoFeasibility and acuteefficacy of radiofrequency ablation of cavotricuspid isthmus-dependent atrial flutter guided by real-time 3D TEErdquo JACCCardiovascular Imaging vol 4 no 7 pp 716ndash726 2011
[66] S S Kim ZM Hijazi R M Lang and B P Knight ldquoThe use ofintracardiac echocardiography and other intracardiac imagingtools to guide noncoronary cardiac interventionsrdquo Journal of theAmerican College of Cardiology vol 53 no 23 pp 2117ndash21282009
[67] JMMangrum J PMounsey L C Kok J P DiMarco andD EHaines ldquoIntracardiac echocardiography-guided anatomicallybased radiofrequency ablation of focal atrial fibrillation origi-nating from pulmonary veinsrdquo Journal of the American Collegeof Cardiology vol 39 no 12 pp 1964ndash1972 2002
[68] R Bala J F Ren M D Hutchinson et al ldquoAssessing epicardialsubstrate using intracardiac echocardiography during VT abla-tionrdquo Circulation Arrhythmia and Electrophysiology vol 4 no5 pp 667ndash673 2011
[69] C Vigna N Marchese M Zanchetta et al ldquoEchocardio-graphic guidance of percutaneous patent foramen ovale closurehead-to-head comparison of transesophageal versus rotationalintracardiac echocardiographyrdquo Echocardiography vol 29 no9 pp 1103ndash1110 2012
[70] T Bartel N Bonaros L Muller et al ldquoIntracardiac echocar-diography a new guiding tool for transcatheter aortic valvereplacementrdquo Journal of the American Society of Echocardiog-raphy vol 24 no 9 pp 966ndash975 2011
[71] R Bai L Di Biase P Mohanty et al ldquoPositioning of left ventric-ular pacing lead guided by intracardiac echocardiography withvector velocity imaging during cardiac resynchronization ther-apy procedurerdquo Journal of Cardiovascular Electrophysiology vol22 no 9 pp 1034ndash1041 2011

BioMed Research International 9
European Journal of Echocardiography vol 11 no 7 pp 557ndash5762010
[3] W G Daniel R ErbelW Kasper et al ldquoSafety of transesophag-eal echocardiography A multicenter survey of 10419 examina-tionsrdquo Circulation vol 83 no 3 pp 817ndash821 1991
[4] J N Hilberath D A Oakes S K Shernan B E Bulwer M NDrsquoAmbra and H K Eltzschig ldquoSafety of transesophageal echo-cardiographyrdquo Journal of the American Society of Echocardiog-raphy vol 23 no 11 pp 1115ndash1127 2010
[5] D G Skolnick S G Sawada H Feigenbaum and D S SegarldquoEnhanced endocardial visualization with noncontrast har-monic imaging during stress echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 12 no 7 pp 559ndash5631999
[6] F B Sozzi D Poldermans J J Bax et al ldquoSecond harmonicimaging improves sensitivity of dobutamine stress echocar-diography for the diagnosis of coronary artery diseaserdquo TheAmerican Heart Journal vol 142 no 1 pp 153ndash159 2001
[7] J C Plana I A Mikati H Dokainish et al ldquoA randomizedcross-over study for evaluation of the effect of image optimiza-tion with contrast on the diagnostic accuracy of dobutamineechocardiography in coronary artery disease The OPTIMIZEtrialrdquo JACC Cardiovascular Imaging vol 1 no 2 pp 145ndash1522008
[8] J S Skinner L Smeeth J M Kendall P C Adams and ATimmis ldquoNICE guidance Chest pain of recent onset assess-ment and diagnosis of recent onset chest pain or discomfort ofsuspected cardiac originrdquo Heart vol 96 no 12 pp 974ndash9782010
[9] P Jeetley L Burden B Stoykova and R Senior ldquoClinical andeconomic impact of stress echocardiography compared withexercise electrocardiography in patients with suspected acutecoronary syndrome but negative troponin a prospective ran-domized controlled studyrdquo European Heart Journal vol 28 no2 pp 204ndash211 2007
[10] BN ShahG Balaji A Alhajiri I S Ramzy S Ahmadvazir andR Senior ldquoThe incremental diagnostic and prognostic valueof contemporary stress echocardiography in a chest pain unitmortality and morbidity outcomes from a real-world settingrdquoCirculation Cardiovascular Imaging vol 6 no 2 pp 202ndash2092013
[11] P Lancellotti F LeboisM Simon C Tombeux C Chauvel andL A Pierard ldquoPrognostic importance of quantitative exerciseDoppler echocardiography in asymptomatic valvular aorticstenosisrdquo Circulation vol 112 no 9 supplement pp I377ndashI3822005
[12] S Marechaux Z Hachicha A Bellouin et al ldquoUsefulness ofexercise-stress echocardiography for risk stratification of trueasymptomatic patients with aortic valve stenosisrdquo EuropeanHeart Journal vol 31 no 11 pp 1390ndash1397 2010
[13] P Lancellotti J Magne E Donal et al ldquoDeterminants andprognostic significance of exercise pulmonary hypertension inasymptomatic severe aortic stenosisrdquoCirculation vol 126 no 7pp 851ndash859 2012
[14] JMonin JQuereMMonchi et al ldquoLow-gradient aortic steno-sis Operative risk stratification and predictors for long-termoutcome a multicenter study using dobutamine stress hemo-dynamicsrdquo Circulation vol 108 no 3 pp 319ndash324 2003
[15] L A Pierard and P Lancellotti ldquoThe role of ischemic mitralregurgitation in the pathogenesis of acute pulmonary edemardquoThe New England Journal of Medicine vol 351 no 16 pp 1627ndash1634 2004
[16] J Magne P Lancellotti and L A Pierard ldquoExercise-inducedchanges in degenerative mitral regurgitationrdquo Journal of theAmericanCollege of Cardiology vol 56 no 4 pp 300ndash309 2010
[17] S Bhattacharyya V Kamperidis B N Shah et al ldquo152 Clinicalutility and prognostic value of appropriateness criteria in stressechocardiography for evaluation of valvular heart diseaserdquoHeart vol 99 pp A89ndashA90 2013
[18] B J Gersh B J Maron R O Bonow et al ldquo2011 ACCFAHAguideline for the diagnosis and treatment of hypertrophic cardi-omyopathyrdquo Journal of the American College of Cardiology vol58 no 25 pp e212ndashe260 2011
[19] P Lancellotti M Senechal M Moonen et al ldquoMyocardial con-tractile reserve during exercise predicts left ventricular reverseremodelling after cardiac resynchronization therapyrdquo Euro-pean Journal of Echocardiography vol 10 no 5 pp 663ndash6682009
[20] M Matsumoto M Inoue S Tamura K Tanaka and H AbeldquoThree-dimensional echocardiography for spatial visualizationand volume calculation of cardiac structuresrdquo Journal of ClinicalUltrasound vol 9 no 4 pp 157ndash165 1981
[21] K H Sheikh S W Smith O von Ramm and J Kisslo ldquoReal-time three-dimensional echocardiography feasibility and ini-tial userdquo Echocardiography vol 8 no 1 pp 119ndash125 1991
[22] L Sugeng L Weinert K Thiele and R M Lang ldquoReal-timethree-dimensional echocardiography using a novelmatrix arraytransducerrdquo Echocardiography vol 20 no 7 pp 623ndash635 2003
[23] N P Nikitin C Constantin P H Loh et al ldquoNew generation3-dimensional echocardiography for left ventricular volumetricand functional measurements comparison with cardiac mag-netic resonancerdquo European Journal of Echocardiography vol 7no 5 pp 365ndash372 2006
[24] V Mor-Avi L Sugeng L Weinert et al ldquoFast measurement ofleft ventricular mass with real-time three-dimensional echocar-diography comparison withmagnetic resonance imagingrdquoCir-culation vol 110 no 13 pp 1814ndash1818 2004
[25] L Sugeng V Mor-Avi L Weinert et al ldquoQuantitative assess-ment of left ventricular size and function side-by-side compari-son of real-time three-dimensional echocardiography and com-puted tomography with magnetic resonance referencerdquo Cir-culation vol 114 no 7 pp 654ndash661 2006
[26] S Kapetanakis M T Kearney A Siva N Gall M Cooklinand M J Monaghan ldquoReal-time three-dimensional echocar-diography a novel technique to quantify global left ventricularmechanical dyssynchronyrdquo Circulation vol 112 no 7 pp 992ndash1000 2005
[27] O I I Soliman M L Geleijnse D A M J Theuns et alldquoUsefulness of left ventricular systolic dyssynchrony by real-time three-dimensional echocardiography to predict long-termresponse to cardiac resynchronization therapyrdquo The AmericanJournal of Cardiology vol 103 no 11 pp 1586ndash1591 2009
[28] A V Khaw R S von Bardeleben C Strasser et al ldquoDirect mea-surement of left ventricular outflow tract by transthoracic real-time 3D-echocardiography increases accuracy in assessment ofaortic valve stenosisrdquo International Journal of Cardiology vol136 no 1 pp 64ndash71 2009
[29] L Sugeng S K Shernan I S Salgo et al ldquoLive 3-dimensionaltransesophageal echocardiography Initial experience using thefully-sampled matrix array proberdquo Journal of the American Col-lege of Cardiology vol 52 no 6 pp 446ndash449 2008
[30] D G Gibson T A Prewitt and D J Brown ldquoAnalysis of leftventricular wall movement during isovolumic relaxation and its
10 BioMed Research International
relation to coronary artery diseaserdquo The British Heart Journalvol 38 no 10 pp 1010ndash1019 1976
[31] P Palka A Lange A D Fleming G R Sutherland L N FeenandW NMcDicken ldquoDoppler tissue imaging myocardial wallmotion velocities in normal subjectsrdquo Journal of the AmericanSociety of Echocardiography vol 8 no 5 pp 659ndash668 1995
[32] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressures acomparative simultaneous Doppler-catheterization studyrdquo Cir-culation vol 102 no 15 pp 1788ndash1794 2000
[33] H Blessberger and T Binder ldquoTwo dimensional speckle track-ing echocardiography basic principlesrdquoHeart vol 96 no 9 pp716ndash722 2010
[34] J Gorcsan III and H Tanaka ldquoEchocardiographic assessmentof myocardial strainrdquo Journal of the American College of Cardi-ology vol 58 no 14 pp 1401ndash1413 2011
[35] T H Marwick R L Leano J Brown et al ldquoMyocardial strainmeasurement with 2-dimensional speckle-tracking echocardi-ography Definition of normal rangerdquo JACC CardiovascularImaging vol 2 no 1 pp 80ndash84 2009
[36] A C T Ng M Sitges P N Pham et al ldquoIncrementalvalue of 2-dimensional speckle tracking strain imaging to wallmotion analysis for detection of coronary artery disease inpatients undergoing dobutamine stress echocardiographyrdquoTheAmerican Heart Journal vol 158 no 5 pp 836ndash844 2009
[37] C B Ingul E Rozis S A Slordahl and T H Marwick ldquoIncre-mental value of strain rate imaging to wall motion analysisfor prediction of outcome in patients undergoing dobutaminestress echocardiographyrdquo Circulation vol 115 no 10 pp 1252ndash1259 2007
[38] R Hoffmann E Altiok B Nowak et al ldquoStrain rate measure-ment by Doppler echocardiography allows improved assess-ment of myocardial viability in patients with depressed left ven-tricular functionrdquo Journal of the American College of Cardiologyvol 39 no 3 pp 443ndash449 2002
[39] L Hanekom C Jenkins L Jeffries et al ldquoIncremental valueof strain rate analysis as an adjunct to wall-motion scoring forassessment of myocardial viability by dobutamine echocardio-graphy a follow-up study after revascularizationrdquo Circulationvol 112 no 25 pp 3892ndash3900 2005
[40] H Tanaka H Nesser T Buck et al ldquoDyssynchrony by speckle-tracking echocardiography and response to cardiac resynchro-nization therapy results of the speckle tracking and resynchro-nization (STAR) studyrdquo European Heart Journal vol 31 no 14pp 1690ndash1700 2010
[41] F Z Khan M S Virdee C R Palmer et al ldquoTargeted leftventricular lead placement to guide cardiac resynchronizationtherapy the TARGET study a randomized controlled trialrdquoJournal of the American College of Cardiology vol 59 no 17 pp1509ndash1518 2012
[42] E S Chung A R Leon L Tavazzi et al ldquoResults of the predic-tors of response to CRT (PROSPECT) trialrdquoCirculation vol 117no 20 pp 2608ndash2616 2008
[43] J J Bax and J Gorcsan III ldquoEchocardiography and noninvasiveimaging in cardiac resynchronization therapy Results of thePROSPECT (predictors of response to cardiac resynchroniza-tion therapy) study in perspectiverdquo Journal of the American Col-lege of Cardiology vol 53 no 21 pp 1933ndash1943 2009
[44] B N Shah M de Villa R S Khattar and R Senior ldquoImagingcardiac sarcoidosis the incremental benefit of speckle trackingechocardiographyrdquo Echocardiography 2013
[45] J KramerM Niemann D Liu et al ldquoTwo-dimensional speckletracking as a non-invasive tool for identification of myocardialfibrosis in Fabry diseaserdquoEuropeanHeart Journal vol 34 no 21pp 1587ndash1596 2013
[46] J L Hare J K Brown R Leano C Jenkins N Woodwardand T H Marwick ldquoUse of myocardial deformation imaging todetect preclinical myocardial dysfunction before conventionalmeasures in patients undergoing breast cancer treatment withtrastuzumabrdquo The American Heart Journal vol 158 no 2 pp294ndash301 2009
[47] M J Stewart ldquoContrast echocardiographyrdquoHeart vol 89 no 3pp 342ndash348 2003
[48] R Janardhanan G Dwivedi S Hayat and R Senior ldquoMyocar-dial contrast echocardiography a new tool for assessment ofmyocardial perfusionrdquo Indian Heart Journal vol 57 no 3 pp210ndash216 2005
[49] S B Feinstein F J T Cate W Zwehl et al ldquoTwo-dimensionalcontrast echocardiography I In vitro development and quanti-tative analysis of echo contrast agentsrdquo Journal of the AmericanCollege of Cardiology vol 3 no 1 pp 14ndash20 1984
[50] R Hoffmann S von Bardeleben F T Cate et al ldquoAssessmentof systolic left ventricular function a multi-centre comparisonof cineventriculography cardiac magnetic resonance imagingunenhanced and contrast-enhanced echocardiographyrdquo Euro-pean Heart Journal vol 26 no 6 pp 607ndash616 2005
[51] R Hoffmann S von Bardeleben J D Kasprzak et al ldquoAnalysisof regional left ventricular function by cineventriculographycardiac magnetic resonance imaging and unenhanced andcontrast-enhanced echocardiography a multicenter compari-son of methodsrdquo Journal of the American College of Cardiologyvol 47 no 1 pp 121ndash128 2006
[52] W G Hundley A M Kizilbash I Afridi F Franco R MPeshock and P A Grayburn ldquoAdministration of an intravenousperfluorocarbon contrast agent improves echocardiographicdetermination of left ventricular volumes and ejection fractioncomparison with cine magnetic resonance imagingrdquo Journal ofthe American College of Cardiology vol 32 no 5 pp 1426ndash14321998
[53] S Malm S Frigstad E Sagberg H Larsson and T SkjaerpeldquoAccurate and reproducible measurement of left ventricularvolume and ejection fraction by contrast echocardiography acomparison with magnetic resonance imagingrdquo Journal of theAmerican College of Cardiology vol 44 no 5 pp 1030ndash10352004
[54] B K Koo D Choi J W Ha S M Kang N Chung and S YCho ldquoIsolated noncompaction of the ventricular myocardiumcontrast echocardiographic findings and review of the litera-turerdquo Echocardiography vol 19 no 2 pp 153ndash156 2002
[55] P Soman J Swinburn M Callister N G Stephens and RSenior ldquoApical hypertrophic cardiomyopathy bedside diagno-sis by intravenous contrast echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 14 no 4 pp 311ndash3132001
[56] S Thanigaraj K B Schechtman and J E Perez ldquoImprovedechocardiographic delineation of left ventricular thrombuswith the use of intravenous second-generation contrast imageenhancementrdquo Journal of the American Society of Echocardiog-raphy vol 12 no 12 pp 1022ndash1026 1999
[57] S Thanigaraj R F Nease Jr K B Schechtman R L Wade SLoslo and J E Perez ldquoUse of contrast for image enhancementduring stress echocardiography is cost-effective and reduces
BioMed Research International 11
additional diagnostic testingrdquo The American Journal of Cardi-ology vol 87 no 12 pp 1430ndash1432 2001
[58] S Kaul and A R Jayaweera ldquoCoronary and myocardial bloodvolumes noninvasive tools to assess the coronary microcircu-lationrdquo Circulation vol 96 no 3 pp 719ndash724 1997
[59] K Wei A R Jayaweera S Firoozan A Linka D M Skybaand S Kaul ldquoBasis for detection of stenosis using venousadministration of microbubbles during myocardial contrastechocardiography bolus or continuous infusionrdquo Journal of theAmeri-canCollege of Cardiology vol 32 no 1 pp 252ndash260 1998
[60] W F Armstrong T M Mueller E L Kinney E G Tickner JC Dillon and H Feigenbaum ldquoAssessment of myocardial per-fusion abnormalities with contrast-enhanced two-dimensionalechocardiographyrdquo Circulation vol 66 no 1 pp 166ndash173 1982
[61] C Tei T Sakamaki PM Shah et al ldquoMyocardial contrast echo-cardiography a reproducible technique of myocardial opacifi-cation for identifying regional perfusion deficitsrdquo Circulationvol 67 no 3 pp 585ndash593 1983
[62] R Senior H BecherMMonaghan et al ldquoContrast echocardio-graphy evidence-based recommendations by european associ-ation of echocardiographyrdquo European Journal of Echocardiogra-phy vol 10 no 2 pp 194ndash212 2009
[63] S Bhattacharyya R Khattar andR Senior ldquoCharacterisation ofintra-cardiacmasses bymyocardial contrast echocardiographyrdquoInternational Journal of Cardiology vol 163 no 1 pp e11ndashe132013
[64] L A Smith R Dworakowski A Bhan et al ldquoReal-time three-dimensional transesophageal echocardiography adds value totranscatheter aortic valve implantationrdquo Journal of theAmericanSociety of Echocardiography vol 26 no 4 pp 359ndash369 2013
[65] F Regoli F F Faletra G Nucifora et al ldquoFeasibility and acuteefficacy of radiofrequency ablation of cavotricuspid isthmus-dependent atrial flutter guided by real-time 3D TEErdquo JACCCardiovascular Imaging vol 4 no 7 pp 716ndash726 2011
[66] S S Kim ZM Hijazi R M Lang and B P Knight ldquoThe use ofintracardiac echocardiography and other intracardiac imagingtools to guide noncoronary cardiac interventionsrdquo Journal of theAmerican College of Cardiology vol 53 no 23 pp 2117ndash21282009
[67] JMMangrum J PMounsey L C Kok J P DiMarco andD EHaines ldquoIntracardiac echocardiography-guided anatomicallybased radiofrequency ablation of focal atrial fibrillation origi-nating from pulmonary veinsrdquo Journal of the American Collegeof Cardiology vol 39 no 12 pp 1964ndash1972 2002
[68] R Bala J F Ren M D Hutchinson et al ldquoAssessing epicardialsubstrate using intracardiac echocardiography during VT abla-tionrdquo Circulation Arrhythmia and Electrophysiology vol 4 no5 pp 667ndash673 2011
[69] C Vigna N Marchese M Zanchetta et al ldquoEchocardio-graphic guidance of percutaneous patent foramen ovale closurehead-to-head comparison of transesophageal versus rotationalintracardiac echocardiographyrdquo Echocardiography vol 29 no9 pp 1103ndash1110 2012
[70] T Bartel N Bonaros L Muller et al ldquoIntracardiac echocar-diography a new guiding tool for transcatheter aortic valvereplacementrdquo Journal of the American Society of Echocardiog-raphy vol 24 no 9 pp 966ndash975 2011
[71] R Bai L Di Biase P Mohanty et al ldquoPositioning of left ventric-ular pacing lead guided by intracardiac echocardiography withvector velocity imaging during cardiac resynchronization ther-apy procedurerdquo Journal of Cardiovascular Electrophysiology vol22 no 9 pp 1034ndash1041 2011

10 BioMed Research International
relation to coronary artery diseaserdquo The British Heart Journalvol 38 no 10 pp 1010ndash1019 1976
[31] P Palka A Lange A D Fleming G R Sutherland L N FeenandW NMcDicken ldquoDoppler tissue imaging myocardial wallmotion velocities in normal subjectsrdquo Journal of the AmericanSociety of Echocardiography vol 8 no 5 pp 659ndash668 1995
[32] S R Ommen R A Nishimura C P Appleton et al ldquoClin-ical utility of Doppler echocardiography and tissue Dopplerimaging in the estimation of left ventricular filling pressures acomparative simultaneous Doppler-catheterization studyrdquo Cir-culation vol 102 no 15 pp 1788ndash1794 2000
[33] H Blessberger and T Binder ldquoTwo dimensional speckle track-ing echocardiography basic principlesrdquoHeart vol 96 no 9 pp716ndash722 2010
[34] J Gorcsan III and H Tanaka ldquoEchocardiographic assessmentof myocardial strainrdquo Journal of the American College of Cardi-ology vol 58 no 14 pp 1401ndash1413 2011
[35] T H Marwick R L Leano J Brown et al ldquoMyocardial strainmeasurement with 2-dimensional speckle-tracking echocardi-ography Definition of normal rangerdquo JACC CardiovascularImaging vol 2 no 1 pp 80ndash84 2009
[36] A C T Ng M Sitges P N Pham et al ldquoIncrementalvalue of 2-dimensional speckle tracking strain imaging to wallmotion analysis for detection of coronary artery disease inpatients undergoing dobutamine stress echocardiographyrdquoTheAmerican Heart Journal vol 158 no 5 pp 836ndash844 2009
[37] C B Ingul E Rozis S A Slordahl and T H Marwick ldquoIncre-mental value of strain rate imaging to wall motion analysisfor prediction of outcome in patients undergoing dobutaminestress echocardiographyrdquo Circulation vol 115 no 10 pp 1252ndash1259 2007
[38] R Hoffmann E Altiok B Nowak et al ldquoStrain rate measure-ment by Doppler echocardiography allows improved assess-ment of myocardial viability in patients with depressed left ven-tricular functionrdquo Journal of the American College of Cardiologyvol 39 no 3 pp 443ndash449 2002
[39] L Hanekom C Jenkins L Jeffries et al ldquoIncremental valueof strain rate analysis as an adjunct to wall-motion scoring forassessment of myocardial viability by dobutamine echocardio-graphy a follow-up study after revascularizationrdquo Circulationvol 112 no 25 pp 3892ndash3900 2005
[40] H Tanaka H Nesser T Buck et al ldquoDyssynchrony by speckle-tracking echocardiography and response to cardiac resynchro-nization therapy results of the speckle tracking and resynchro-nization (STAR) studyrdquo European Heart Journal vol 31 no 14pp 1690ndash1700 2010
[41] F Z Khan M S Virdee C R Palmer et al ldquoTargeted leftventricular lead placement to guide cardiac resynchronizationtherapy the TARGET study a randomized controlled trialrdquoJournal of the American College of Cardiology vol 59 no 17 pp1509ndash1518 2012
[42] E S Chung A R Leon L Tavazzi et al ldquoResults of the predic-tors of response to CRT (PROSPECT) trialrdquoCirculation vol 117no 20 pp 2608ndash2616 2008
[43] J J Bax and J Gorcsan III ldquoEchocardiography and noninvasiveimaging in cardiac resynchronization therapy Results of thePROSPECT (predictors of response to cardiac resynchroniza-tion therapy) study in perspectiverdquo Journal of the American Col-lege of Cardiology vol 53 no 21 pp 1933ndash1943 2009
[44] B N Shah M de Villa R S Khattar and R Senior ldquoImagingcardiac sarcoidosis the incremental benefit of speckle trackingechocardiographyrdquo Echocardiography 2013
[45] J KramerM Niemann D Liu et al ldquoTwo-dimensional speckletracking as a non-invasive tool for identification of myocardialfibrosis in Fabry diseaserdquoEuropeanHeart Journal vol 34 no 21pp 1587ndash1596 2013
[46] J L Hare J K Brown R Leano C Jenkins N Woodwardand T H Marwick ldquoUse of myocardial deformation imaging todetect preclinical myocardial dysfunction before conventionalmeasures in patients undergoing breast cancer treatment withtrastuzumabrdquo The American Heart Journal vol 158 no 2 pp294ndash301 2009
[47] M J Stewart ldquoContrast echocardiographyrdquoHeart vol 89 no 3pp 342ndash348 2003
[48] R Janardhanan G Dwivedi S Hayat and R Senior ldquoMyocar-dial contrast echocardiography a new tool for assessment ofmyocardial perfusionrdquo Indian Heart Journal vol 57 no 3 pp210ndash216 2005
[49] S B Feinstein F J T Cate W Zwehl et al ldquoTwo-dimensionalcontrast echocardiography I In vitro development and quanti-tative analysis of echo contrast agentsrdquo Journal of the AmericanCollege of Cardiology vol 3 no 1 pp 14ndash20 1984
[50] R Hoffmann S von Bardeleben F T Cate et al ldquoAssessmentof systolic left ventricular function a multi-centre comparisonof cineventriculography cardiac magnetic resonance imagingunenhanced and contrast-enhanced echocardiographyrdquo Euro-pean Heart Journal vol 26 no 6 pp 607ndash616 2005
[51] R Hoffmann S von Bardeleben J D Kasprzak et al ldquoAnalysisof regional left ventricular function by cineventriculographycardiac magnetic resonance imaging and unenhanced andcontrast-enhanced echocardiography a multicenter compari-son of methodsrdquo Journal of the American College of Cardiologyvol 47 no 1 pp 121ndash128 2006
[52] W G Hundley A M Kizilbash I Afridi F Franco R MPeshock and P A Grayburn ldquoAdministration of an intravenousperfluorocarbon contrast agent improves echocardiographicdetermination of left ventricular volumes and ejection fractioncomparison with cine magnetic resonance imagingrdquo Journal ofthe American College of Cardiology vol 32 no 5 pp 1426ndash14321998
[53] S Malm S Frigstad E Sagberg H Larsson and T SkjaerpeldquoAccurate and reproducible measurement of left ventricularvolume and ejection fraction by contrast echocardiography acomparison with magnetic resonance imagingrdquo Journal of theAmerican College of Cardiology vol 44 no 5 pp 1030ndash10352004
[54] B K Koo D Choi J W Ha S M Kang N Chung and S YCho ldquoIsolated noncompaction of the ventricular myocardiumcontrast echocardiographic findings and review of the litera-turerdquo Echocardiography vol 19 no 2 pp 153ndash156 2002
[55] P Soman J Swinburn M Callister N G Stephens and RSenior ldquoApical hypertrophic cardiomyopathy bedside diagno-sis by intravenous contrast echocardiographyrdquo Journal of theAmerican Society of Echocardiography vol 14 no 4 pp 311ndash3132001
[56] S Thanigaraj K B Schechtman and J E Perez ldquoImprovedechocardiographic delineation of left ventricular thrombuswith the use of intravenous second-generation contrast imageenhancementrdquo Journal of the American Society of Echocardiog-raphy vol 12 no 12 pp 1022ndash1026 1999
[57] S Thanigaraj R F Nease Jr K B Schechtman R L Wade SLoslo and J E Perez ldquoUse of contrast for image enhancementduring stress echocardiography is cost-effective and reduces
BioMed Research International 11
additional diagnostic testingrdquo The American Journal of Cardi-ology vol 87 no 12 pp 1430ndash1432 2001
[58] S Kaul and A R Jayaweera ldquoCoronary and myocardial bloodvolumes noninvasive tools to assess the coronary microcircu-lationrdquo Circulation vol 96 no 3 pp 719ndash724 1997
[59] K Wei A R Jayaweera S Firoozan A Linka D M Skybaand S Kaul ldquoBasis for detection of stenosis using venousadministration of microbubbles during myocardial contrastechocardiography bolus or continuous infusionrdquo Journal of theAmeri-canCollege of Cardiology vol 32 no 1 pp 252ndash260 1998
[60] W F Armstrong T M Mueller E L Kinney E G Tickner JC Dillon and H Feigenbaum ldquoAssessment of myocardial per-fusion abnormalities with contrast-enhanced two-dimensionalechocardiographyrdquo Circulation vol 66 no 1 pp 166ndash173 1982
[61] C Tei T Sakamaki PM Shah et al ldquoMyocardial contrast echo-cardiography a reproducible technique of myocardial opacifi-cation for identifying regional perfusion deficitsrdquo Circulationvol 67 no 3 pp 585ndash593 1983
[62] R Senior H BecherMMonaghan et al ldquoContrast echocardio-graphy evidence-based recommendations by european associ-ation of echocardiographyrdquo European Journal of Echocardiogra-phy vol 10 no 2 pp 194ndash212 2009
[63] S Bhattacharyya R Khattar andR Senior ldquoCharacterisation ofintra-cardiacmasses bymyocardial contrast echocardiographyrdquoInternational Journal of Cardiology vol 163 no 1 pp e11ndashe132013
[64] L A Smith R Dworakowski A Bhan et al ldquoReal-time three-dimensional transesophageal echocardiography adds value totranscatheter aortic valve implantationrdquo Journal of theAmericanSociety of Echocardiography vol 26 no 4 pp 359ndash369 2013
[65] F Regoli F F Faletra G Nucifora et al ldquoFeasibility and acuteefficacy of radiofrequency ablation of cavotricuspid isthmus-dependent atrial flutter guided by real-time 3D TEErdquo JACCCardiovascular Imaging vol 4 no 7 pp 716ndash726 2011
[66] S S Kim ZM Hijazi R M Lang and B P Knight ldquoThe use ofintracardiac echocardiography and other intracardiac imagingtools to guide noncoronary cardiac interventionsrdquo Journal of theAmerican College of Cardiology vol 53 no 23 pp 2117ndash21282009
[67] JMMangrum J PMounsey L C Kok J P DiMarco andD EHaines ldquoIntracardiac echocardiography-guided anatomicallybased radiofrequency ablation of focal atrial fibrillation origi-nating from pulmonary veinsrdquo Journal of the American Collegeof Cardiology vol 39 no 12 pp 1964ndash1972 2002
[68] R Bala J F Ren M D Hutchinson et al ldquoAssessing epicardialsubstrate using intracardiac echocardiography during VT abla-tionrdquo Circulation Arrhythmia and Electrophysiology vol 4 no5 pp 667ndash673 2011
[69] C Vigna N Marchese M Zanchetta et al ldquoEchocardio-graphic guidance of percutaneous patent foramen ovale closurehead-to-head comparison of transesophageal versus rotationalintracardiac echocardiographyrdquo Echocardiography vol 29 no9 pp 1103ndash1110 2012
[70] T Bartel N Bonaros L Muller et al ldquoIntracardiac echocar-diography a new guiding tool for transcatheter aortic valvereplacementrdquo Journal of the American Society of Echocardiog-raphy vol 24 no 9 pp 966ndash975 2011
[71] R Bai L Di Biase P Mohanty et al ldquoPositioning of left ventric-ular pacing lead guided by intracardiac echocardiography withvector velocity imaging during cardiac resynchronization ther-apy procedurerdquo Journal of Cardiovascular Electrophysiology vol22 no 9 pp 1034ndash1041 2011

BioMed Research International 11
additional diagnostic testingrdquo The American Journal of Cardi-ology vol 87 no 12 pp 1430ndash1432 2001
[58] S Kaul and A R Jayaweera ldquoCoronary and myocardial bloodvolumes noninvasive tools to assess the coronary microcircu-lationrdquo Circulation vol 96 no 3 pp 719ndash724 1997
[59] K Wei A R Jayaweera S Firoozan A Linka D M Skybaand S Kaul ldquoBasis for detection of stenosis using venousadministration of microbubbles during myocardial contrastechocardiography bolus or continuous infusionrdquo Journal of theAmeri-canCollege of Cardiology vol 32 no 1 pp 252ndash260 1998
[60] W F Armstrong T M Mueller E L Kinney E G Tickner JC Dillon and H Feigenbaum ldquoAssessment of myocardial per-fusion abnormalities with contrast-enhanced two-dimensionalechocardiographyrdquo Circulation vol 66 no 1 pp 166ndash173 1982
[61] C Tei T Sakamaki PM Shah et al ldquoMyocardial contrast echo-cardiography a reproducible technique of myocardial opacifi-cation for identifying regional perfusion deficitsrdquo Circulationvol 67 no 3 pp 585ndash593 1983
[62] R Senior H BecherMMonaghan et al ldquoContrast echocardio-graphy evidence-based recommendations by european associ-ation of echocardiographyrdquo European Journal of Echocardiogra-phy vol 10 no 2 pp 194ndash212 2009
[63] S Bhattacharyya R Khattar andR Senior ldquoCharacterisation ofintra-cardiacmasses bymyocardial contrast echocardiographyrdquoInternational Journal of Cardiology vol 163 no 1 pp e11ndashe132013
[64] L A Smith R Dworakowski A Bhan et al ldquoReal-time three-dimensional transesophageal echocardiography adds value totranscatheter aortic valve implantationrdquo Journal of theAmericanSociety of Echocardiography vol 26 no 4 pp 359ndash369 2013
[65] F Regoli F F Faletra G Nucifora et al ldquoFeasibility and acuteefficacy of radiofrequency ablation of cavotricuspid isthmus-dependent atrial flutter guided by real-time 3D TEErdquo JACCCardiovascular Imaging vol 4 no 7 pp 716ndash726 2011
[66] S S Kim ZM Hijazi R M Lang and B P Knight ldquoThe use ofintracardiac echocardiography and other intracardiac imagingtools to guide noncoronary cardiac interventionsrdquo Journal of theAmerican College of Cardiology vol 53 no 23 pp 2117ndash21282009
[67] JMMangrum J PMounsey L C Kok J P DiMarco andD EHaines ldquoIntracardiac echocardiography-guided anatomicallybased radiofrequency ablation of focal atrial fibrillation origi-nating from pulmonary veinsrdquo Journal of the American Collegeof Cardiology vol 39 no 12 pp 1964ndash1972 2002
[68] R Bala J F Ren M D Hutchinson et al ldquoAssessing epicardialsubstrate using intracardiac echocardiography during VT abla-tionrdquo Circulation Arrhythmia and Electrophysiology vol 4 no5 pp 667ndash673 2011
[69] C Vigna N Marchese M Zanchetta et al ldquoEchocardio-graphic guidance of percutaneous patent foramen ovale closurehead-to-head comparison of transesophageal versus rotationalintracardiac echocardiographyrdquo Echocardiography vol 29 no9 pp 1103ndash1110 2012
[70] T Bartel N Bonaros L Muller et al ldquoIntracardiac echocar-diography a new guiding tool for transcatheter aortic valvereplacementrdquo Journal of the American Society of Echocardiog-raphy vol 24 no 9 pp 966ndash975 2011
[71] R Bai L Di Biase P Mohanty et al ldquoPositioning of left ventric-ular pacing lead guided by intracardiac echocardiography withvector velocity imaging during cardiac resynchronization ther-apy procedurerdquo Journal of Cardiovascular Electrophysiology vol22 no 9 pp 1034ndash1041 2011