Embed Size (px)
Citation preview

TpisJrtp
M
ACJo4mwdlb
UA
0d
Echocardiographic and Clinical Risk Factors for Atrial Fibrillationin Hypertensive Patients With Ischemic Stroke
Jacob I. Haft, MD*, and Louis E. Teichholz, MD
Atrial fibrillation (AF) is a common cause of ischemic stroke. Because anticoagulation canprevent many of these strokes, identifying patients with occult intermittent AF is impor-tant. Hypertension is a common precursor of stroke and AF. Prolonged nonselectiveelectrocardiographic monitoring of patients after ischemic stroke has yielded only a smallnumber of patients with occult intermittent AF. To determine the importance of AF innonhemorrhagic stroke, we retrospectively studied 799 patients admitted with ischemicstroke over 31 months. AF was present on the admitting electrocardiogram in 154 patients(19.3%), diagnosed later during the stroke admission in 58 (7.3%), and found only duringanother admission before/after the stroke admission in 46 (5.8%). AF was intermittent in123 patients, 47.7% (95% CI 41.6 to 53.8) of patients with AF, and not present on initialelectrocardiogram in 40.3% of patients with AF. In 633 patients with hypertension, AFoccurred in 34.9% versus 22.2% without hypertension (p <0.01). Echocardiogram revealeda left atrium >4.0 cm in 81.3% of patients with AF versus 42.4% of those without AF (oddsratio [OR] 5.85, 95% confidence interval [CI] 3.87 to 8.96, p <0.001); ejection fraction was<50% in 27.7% of patients with AF versus 12.6% of those without AF (OR 2.63, 95% CI1.65 to 4.22, p <0.001); and the left ventricle was >5.6 cm in 13.8% in patients with AFversus 6.7% in those without AF (OR 2.21, 95% CI 1.61 to 3.04, p <0.01). Clinically,congestive heart failure (31% vs 10.4%, OR 3.89, 95% CI 2.76 to 5.73) and coronary disease(31% vs 21.4%, OR 1.65, 95% CI 1.15 to 2.37) were present more often in patients with AF(p <0.001). Left ventricular hypertrophy, diastolic dysfunction, and diabetes were commonin all hypertensive patients with stroke. In conclusion, hypertensive patients with these riskfactors should undergo prolonged electrocardiographic event monitoring to identify occultintermittent AF so measures can be taken to prevent a second stroke and possibly a first
stroke. © 2008 Elsevier Inc. All rights reserved. (Am J Cardiol 2008;102:1348–1351)(sopetveadmgsga
sAavpwdEm(
o determine the importance of atrial fibrillation (AF) inatients with hypertension who have had strokes, we stud-ed 799 patients with ischemic stroke admitted to Hacken-ack University Medical Center from January 1, 2005 touly 31, 2007. We defined clinical and echocardiographicisk factors that might identify those patients with hyper-ension at risk for AF who would most likely benefit fromrolonged electrocardiographic event monitoring.
ethods
ll patients admitted to Hackensack University Medicalenter with a diagnosis of stroke from January 1, 2005 to
uly 31, 2007 were reviewed and those with a diagnosis ofcclusion of a cerebral artery (codes 434.00, 434.01,34.11, 434.91) were selected for study. Patients with aitral prosthesis or a discharge diagnosis of mitral stenosisere excluded (50 patients, 23 with AF, 27 without AFiagnosed). Demographic and diagnostic data were tabu-ated, including hypertension, congestive heart failure, dia-etes mellitus, and the presence of coronary artery disease
Division of Cardiology, Department of Internal Medicine, Hackensackniversity Medical Center, Hackensack, New Jersey. Manuscript receivedpril 13, 2008; revised manuscript received and accepted July 13, 2008.
*Corresponding author: Tel: 201-343-8505; fax: 201-569-4342.
�E-mail address: [email protected] (J.I. Haft).002-9149/08/$ – see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2008.07.009
myocardial infarction, coronary angioplasty, coronarytent, or coronary bypass surgery). All electrocardiogramsf each patients with stroke in the hospital database wererinted out and reviewed (approximately 5,000, 1 to 56lectrocardiograms per patient) including all available elec-rocardiograms from the stroke admission and from all pre-ious or subsequent admissions. Persistent AF was consid-red present if all electrocardiograms on the strokedmission and thereafter showed AF. Intermittent AF wasiagnosed if, in patients with AF on the initial stroke ad-ission electrocardiogram, any subsequent electrocardio-
ram showed normal sinus rhythm, or, in those patients withinus rhythm on their initial stroke admission electrocardio-ram, any electrocardiogram before or after the initial strokedmission electrocardiogram showed AF.
Available echocardiographic findings in all patients withtroke and hypertension who had persistent or intermittentF and in a random selection of 290 patients with stroke
nd hypertension without the diagnosis of AF were re-iewed. Left atrial (LA) enlargement was consideredresent if the dimension was �4.0 cm. Systolic dysfunctionas present if the ejection fraction was �50%; diastolicysfunction was present if the A wave was greater than thewave on tissue Doppler and/or on Doppler flow across theitral valve during diastole. We diagnosed left ventricular
LV) enlargement if the end-diastolic LV dimension was
5.6 cm. LV hypertrophy was diagnosed if the septal andwww.AJConline.org
pt
Dwmcdpe2Kewt1PaR
R
CAisAhawhsip(C
d(AC
wTr
i
pdu2ognp21wd
htLAtpLwd2wp1idtiiAdwo
D
Aawsmhswoanttinhdd
hh
TD
V
A
IP
1349Arrhythmias and Conduction Disturbances/Atrial Fibrillation in Ischemic Stroke
osterior wall dimensions were �1.2 cm or �1.1 cm andhe reader diagnosed LV hypertrophy.
Continuous data were tested for fit to normality by the’Agostino-Pearson omnibus normality test. Data, whichere normally distributed, were compared by a parametricethod (unpaired t test); non-normally distributed data were
ompared by Mann-Whitney test. For normally distributedata, mean � 1 SD and 95% confidence interval (CI) arerovided. All categorical data were analyzed by Fisher’sxact test (for 2 � 2 cross tabulation) or chi-square test (for� n cross tabulation). One-way analysis of variance andruskal-Wallis test were done to compare LA size and
jection fraction among the 3 groups (hypertensive patientsith intermittent AF, persistent AF, and no AF). After
esting was done with the Dunn multiple comparison test in-way analysis of variance. All calculations were made inrism software (GraphPad Corp., San Diego, California) oncomputer platform using Windows XP (Microsoft, Inc.,edmond, Washington).
esults
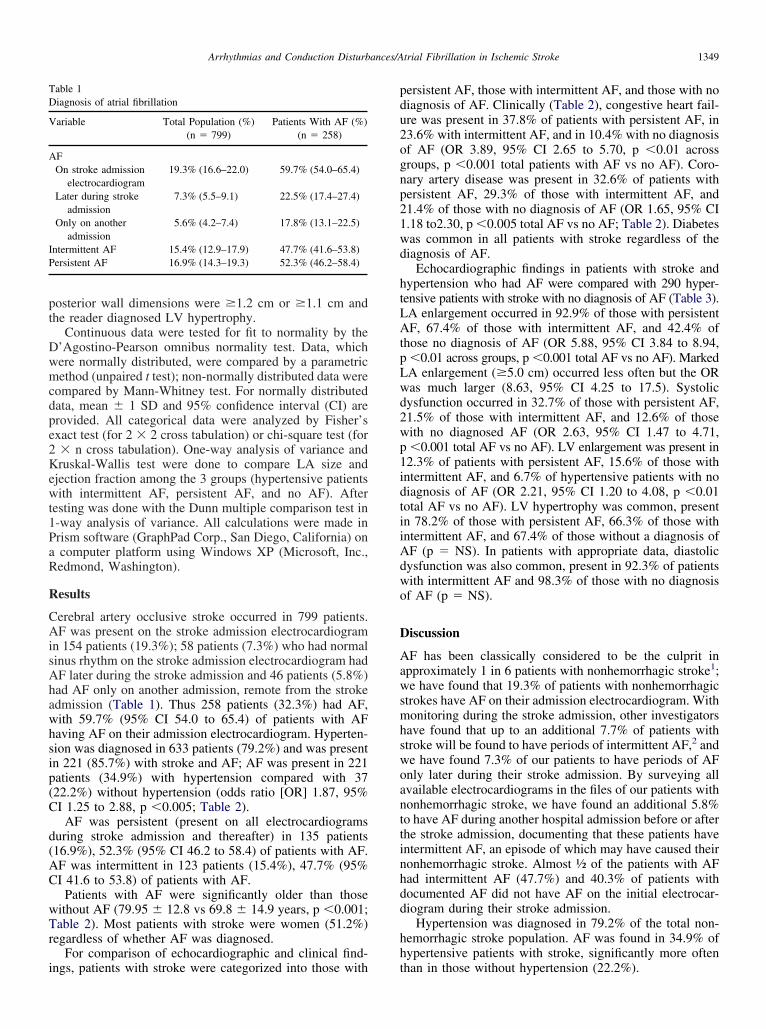
erebral artery occlusive stroke occurred in 799 patients.F was present on the stroke admission electrocardiogram
n 154 patients (19.3%); 58 patients (7.3%) who had normalinus rhythm on the stroke admission electrocardiogram hadF later during the stroke admission and 46 patients (5.8%)ad AF only on another admission, remote from the strokedmission (Table 1). Thus 258 patients (32.3%) had AF,ith 59.7% (95% CI 54.0 to 65.4) of patients with AFaving AF on their admission electrocardiogram. Hyperten-ion was diagnosed in 633 patients (79.2%) and was presentn 221 (85.7%) with stroke and AF; AF was present in 221atients (34.9%) with hypertension compared with 3722.2%) without hypertension (odds ratio [OR] 1.87, 95%I 1.25 to 2.88, p �0.005; Table 2).
AF was persistent (present on all electrocardiogramsuring stroke admission and thereafter) in 135 patients16.9%), 52.3% (95% CI 46.2 to 58.4) of patients with AF.F was intermittent in 123 patients (15.4%), 47.7% (95%I 41.6 to 53.8) of patients with AF.
Patients with AF were significantly older than thoseithout AF (79.95 � 12.8 vs 69.8 � 14.9 years, p �0.001;able 2). Most patients with stroke were women (51.2%)
egardless of whether AF was diagnosed.For comparison of echocardiographic and clinical find-
able 1iagnosis of atrial fibrillation
ariable Total Population (%) Patients With AF (%)(n � 799) (n � 258)
FOn stroke admission
electrocardiogram19.3% (16.6–22.0) 59.7% (54.0–65.4)
Later during strokeadmission
7.3% (5.5–9.1) 22.5% (17.4–27.4)
Only on anotheradmission
5.6% (4.2–7.4) 17.8% (13.1–22.5)
ntermittent AF 15.4% (12.9–17.9) 47.7% (41.6–53.8)ersistent AF 16.9% (14.3–19.3) 52.3% (46.2–58.4)
ngs, patients with stroke were categorized into those with t
ersistent AF, those with intermittent AF, and those with noiagnosis of AF. Clinically (Table 2), congestive heart fail-re was present in 37.8% of patients with persistent AF, in3.6% with intermittent AF, and in 10.4% with no diagnosisf AF (OR 3.89, 95% CI 2.65 to 5.70, p �0.01 acrossroups, p �0.001 total patients with AF vs no AF). Coro-ary artery disease was present in 32.6% of patients withersistent AF, 29.3% of those with intermittent AF, and1.4% of those with no diagnosis of AF (OR 1.65, 95% CI.18 to2.30, p �0.005 total AF vs no AF; Table 2). Diabetesas common in all patients with stroke regardless of theiagnosis of AF.
Echocardiographic findings in patients with stroke andypertension who had AF were compared with 290 hyper-ensive patients with stroke with no diagnosis of AF (Table 3).A enlargement occurred in 92.9% of those with persistentF, 67.4% of those with intermittent AF, and 42.4% of
hose no diagnosis of AF (OR 5.88, 95% CI 3.84 to 8.94,�0.01 across groups, p �0.001 total AF vs no AF). MarkedA enlargement (�5.0 cm) occurred less often but the ORas much larger (8.63, 95% CI 4.25 to 17.5). Systolicysfunction occurred in 32.7% of those with persistent AF,1.5% of those with intermittent AF, and 12.6% of thoseith no diagnosed AF (OR 2.63, 95% CI 1.47 to 4.71,�0.001 total AF vs no AF). LV enlargement was present in
2.3% of patients with persistent AF, 15.6% of those withntermittent AF, and 6.7% of hypertensive patients with noiagnosis of AF (OR 2.21, 95% CI 1.20 to 4.08, p �0.01otal AF vs no AF). LV hypertrophy was common, presentn 78.2% of those with persistent AF, 66.3% of those withntermittent AF, and 67.4% of those without a diagnosis ofF (p � NS). In patients with appropriate data, diastolicysfunction was also common, present in 92.3% of patientsith intermittent AF and 98.3% of those with no diagnosisf AF (p � NS).
iscussion
F has been classically considered to be the culprit inpproximately 1 in 6 patients with nonhemorrhagic stroke1;e have found that 19.3% of patients with nonhemorrhagic
trokes have AF on their admission electrocardiogram. Withonitoring during the stroke admission, other investigators
ave found that up to an additional 7.7% of patients withtroke will be found to have periods of intermittent AF,2 ande have found 7.3% of our patients to have periods of AFnly later during their stroke admission. By surveying allvailable electrocardiograms in the files of our patients withonhemorrhagic stroke, we have found an additional 5.8%o have AF during another hospital admission before or afterhe stroke admission, documenting that these patients haventermittent AF, an episode of which may have caused theironhemorrhagic stroke. Almost ½ of the patients with AFad intermittent AF (47.7%) and 40.3% of patients withocumented AF did not have AF on the initial electrocar-iogram during their stroke admission.
Hypertension was diagnosed in 79.2% of the total non-emorrhagic stroke population. AF was found in 34.9% ofypertensive patients with stroke, significantly more often
han in those without hypertension (22.2%).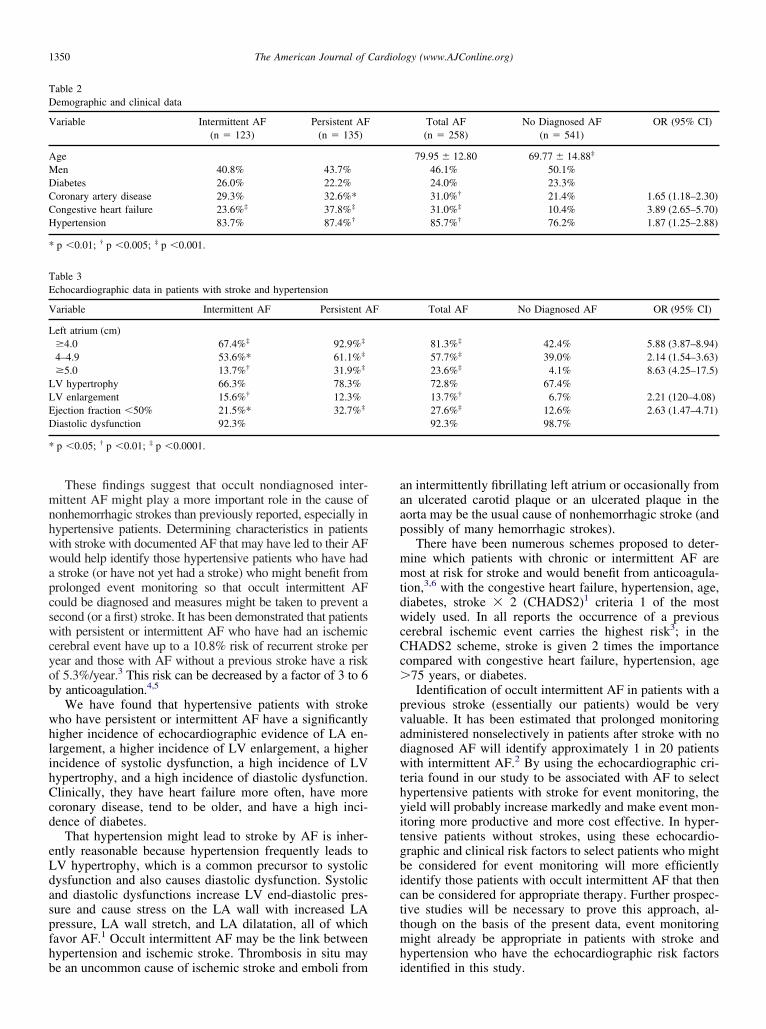
mnhwwapcswcyob
whlihCcd
eLdaspfhb
aaap
mmtdwcCc�
pvadwthyitgbicttmh
TD
V
AMDCCH
*
TE
V
L
LLED
*
1350 The American Journal of Cardiology (www.AJConline.org)
These findings suggest that occult nondiagnosed inter-ittent AF might play a more important role in the cause of
onhemorrhagic strokes than previously reported, especially inypertensive patients. Determining characteristics in patientsith stroke with documented AF that may have led to their AFould help identify those hypertensive patients who have hadstroke (or have not yet had a stroke) who might benefit fromrolonged event monitoring so that occult intermittent AFould be diagnosed and measures might be taken to prevent aecond (or a first) stroke. It has been demonstrated that patientsith persistent or intermittent AF who have had an ischemic
erebral event have up to a 10.8% risk of recurrent stroke perear and those with AF without a previous stroke have a riskf 5.3%/year.3 This risk can be decreased by a factor of 3 to 6y anticoagulation.4,5
We have found that hypertensive patients with strokeho have persistent or intermittent AF have a significantlyigher incidence of echocardiographic evidence of LA en-argement, a higher incidence of LV enlargement, a higherncidence of systolic dysfunction, a high incidence of LVypertrophy, and a high incidence of diastolic dysfunction.linically, they have heart failure more often, have moreoronary disease, tend to be older, and have a high inci-ence of diabetes.
That hypertension might lead to stroke by AF is inher-ntly reasonable because hypertension frequently leads toV hypertrophy, which is a common precursor to systolicysfunction and also causes diastolic dysfunction. Systolicnd diastolic dysfunctions increase LV end-diastolic pres-ure and cause stress on the LA wall with increased LAressure, LA wall stretch, and LA dilatation, all of whichavor AF.1 Occult intermittent AF may be the link betweenypertension and ischemic stroke. Thrombosis in situ may
able 2emographic and clinical data
ariable Intermittent AF Persistent AF(n � 123) (n � 135)
geen 40.8% 43.7%iabetes 26.0% 22.2%oronary artery disease 29.3% 32.6%*ongestive heart failure 23.6%‡ 37.8%‡
ypertension 83.7% 87.4%†
p �0.01; † p �0.005; ‡ p �0.001.
able 3chocardiographic data in patients with stroke and hypertension
ariable Intermittent AF Persistent A
eft atrium (cm)�4.0 67.4%‡ 92.9%‡
4–4.9 53.6%* 61.1%‡
�5.0 13.7%† 31.9%‡
V hypertrophy 66.3% 78.3%V enlargement 15.6%† 12.3%jection fraction �50% 21.5%* 32.7%‡
iastolic dysfunction 92.3%
p �0.05; † p �0.01; ‡ p �0.0001.
e an uncommon cause of ischemic stroke and emboli from i
n intermittently fibrillating left atrium or occasionally fromn ulcerated carotid plaque or an ulcerated plaque in theorta may be the usual cause of nonhemorrhagic stroke (andossibly of many hemorrhagic strokes).
There have been numerous schemes proposed to deter-ine which patients with chronic or intermittent AF areost at risk for stroke and would benefit from anticoagula-
ion,3,6 with the congestive heart failure, hypertension, age,iabetes, stroke � 2 (CHADS2)1 criteria 1 of the mostidely used. In all reports the occurrence of a previous
erebral ischemic event carries the highest risk3; in theHADS2 scheme, stroke is given 2 times the importanceompared with congestive heart failure, hypertension, age75 years, or diabetes.Identification of occult intermittent AF in patients with a
revious stroke (essentially our patients) would be veryaluable. It has been estimated that prolonged monitoringdministered nonselectively in patients after stroke with noiagnosed AF will identify approximately 1 in 20 patientsith intermittent AF.2 By using the echocardiographic cri-
eria found in our study to be associated with AF to selectypertensive patients with stroke for event monitoring, theield will probably increase markedly and make event mon-toring more productive and more cost effective. In hyper-ensive patients without strokes, using these echocardio-raphic and clinical risk factors to select patients who mighte considered for event monitoring will more efficientlydentify those patients with occult intermittent AF that thenan be considered for appropriate therapy. Further prospec-ive studies will be necessary to prove this approach, al-hough on the basis of the present data, event monitoringight already be appropriate in patients with stroke and
ypertension who have the echocardiographic risk factors
Total AF No Diagnosed AF OR (95% CI)(n � 258) (n � 541)
79.95 � 12.80 69.77 � 14.88‡
46.1% 50.1%24.0% 23.3%31.0%† 21.4% 1.65 (1.18–2.30)31.0%‡ 10.4% 3.89 (2.65–5.70)85.7%† 76.2% 1.87 (1.25–2.88)
Total AF No Diagnosed AF OR (95% CI)
81.3%‡ 42.4% 5.88 (3.87–8.94)57.7%‡ 39.0% 2.14 (1.54–3.63)23.6%‡ 4.1% 8.63 (4.25–17.5)72.8% 67.4%13.7%† 6.7% 2.21 (120–4.08)27.6%‡ 12.6% 2.63 (1.47–4.71)92.3% 98.7%
F
dentified in this study.

AWdSUft
1
2
3
4
5
6
1351Arrhythmias and Conduction Disturbances/Atrial Fibrillation in Ischemic Stroke
cknowledgment: We thank Stephen Moran, director, andilliam Ahearn, analyst in the knowledge management
epartment, and Patricia Ernest, Arlene Fretz, and Deborahchoenborn in the cardiology department at Hackensackniversity Medical Center, and Rupen Parikh, MD, cardiac
ellow at the Seton Hall Postgraduate Medical Program, forheir invaluable help in the preparation of this report.
. Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA,Halperin JL, Leheuzey J-Y, Kay N, Lowe JE, et al. ACC/AHA/ESC 2006guidelines for the management of patients with atrial fibrillation: a report ofthe American College of Cardiology/American Heart Association taskforce on practice guidelines and European Society of Cardiology commit-tee for practice guidelines (writing committee to revise the 2001 guidelinesfor the management of patients with atrial fibrillation): developed in col-laboration with the European Heart Rhythm Association and the Heart
Rhythm Society. Circulation 2006;114(suppl):e257–e354.. Liao J, Zahira K, Scallan C, Morillo C, O’Donnell M. Noninvasivecardiac monitoring for detecting paroxysmal atrial fibrillation or flutterafter acute ischemic stroke. A systematic review. Stroke 2007;38:2935–2940.
. Gage BF, van Walraven C, Pearce L, Hart RG, Koudstaal PJ, BoodeBSP, Petersen P. Selecting patients with atrial fibrillation for anticoag-ulation: stroke risk stratification in patients taking aspirin. Circulation2004;110:2287–2292.
. Singer DE, Albers GW, Dalen JE, Go AS, Halperin JL, Manning WJ.Antithrombotic therapy in atrial fibrillation. The seventh ACCP confer-ence on antithrombotic and thrombolytic therapy. Chest 2004;126(suppl):429S–456S.
. Hart RG. Atrial fibrillation and stroke prevention. N Engl J Med 2003;349:1015–1016.
. Atrial Fibrillation Investigators. Risk factors for stroke and efficacy ofantithrombotic therapy in atrial fibrillation. Analysis of pooled datafrom five randomized controlled trials. Arch Intern Med 1994;154:
1449–1457.