Embed Size (px)
Citation preview

03/29/2017
1
ECG Recognition of STEMI Imposters
Kul Aggarwal, MD, MRCP, FACCProfessor of Clinical Medicine, Division of Cardiology
University of Missouri‐Columbia &
Chief, Cardiology Section, Harry S Truman VA Hospital
Normal ECG
Real STEMI characteristics
How to spot Imposters
Overview
US hospital discharges: Unstable angina/NSTEMI and STEMI
AHA. Heart Disease and Stroke Statistics–2005 Update.
STEMI = ST-elevation myocardial infarction (MI), or Q-wave MINSTEMI = non–ST-elevation MI, or non–Q-wave MI
1.67 million hospital discharges
STEMI
1.17 million discharges per year
500,000 discharges per year
Acute coronary syndromes
UA/NSTEMI

03/29/2017
2
ECG is a cornerstone in the diagnosis of STEMI• Chest pain
• ECG
• Cardiac Enzymes (biomarkers)
Confounding factors• It may be “normal”• It may show subtle abnormalities
• It may show a change from previous
• It may show pre‐existing abnormalities
• It may be “false positive”
Overview
Identification of ACS Patients in the EDPatients with the following symptoms and signs require immediate
assessment by the triage nurse for the initiation of the ACS
protocol:
Chest pain or severe epigastric pain, nontraumatic in origin, with components typical of myocardial ischemia or MI:• Central/substernal compression or crushing chest pain• Pressure, tightness, heaviness, cramping, burning, aching sensation• Unexplained indigestion, belching, epigastric pain• Radiating pain in neck, jaw, shoulders, back, or 1 or both arms
Associated dyspnea
Associated nausea/vomiting
Associated diaphoresis
If these symptoms are present, obtain stat ECG
5Adapted from the National Heart Attack Alert Program. Emergency Department: rapid identification and treatment of patients with acute myocardial infarction. US Department of Health and Human Services. US Public Health Service. National Institutes of Health. National Heart, Lung and Blood Institute; September 1993; NIH Publication No. 93-3278. Also see Table 2 of Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157.

03/29/2017
3
Normal ECG
ECG in AMI
Reciprocal ST depression powerful markerChange from previous ECGWidespread ST depressionIf no apparent ST depression/elevation, look for “silent” areas • Examine T waves in I, aVL• Posterior• high lateralEnsure that the date, time and demographics match!
Labs should not delay implementation of reperfusion therapy
Initial Recognition and Management
Do NOT wait for labs!!!

03/29/2017
4
Clinical context
Regionality
Clues
Reciprocal changes
Comparison
Some Key Considerations
• Could be LCx or RCA
• Could be associated with:• Posterior infarct• RV infarct
• Consider doing extra leads such as:• V4R, V5R, V6R• V7, V8, V9
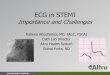
Inferior STEMI
03/29/2017
5
Inferior STEMI
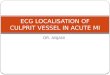
Anterior STEMI
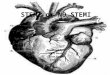
Inferior STEMI

03/29/2017
6
Anterolateral STEMI
Anterior MI, recent
Inferior infarct, old

03/29/2017
7
Inf + RV MI
Acute Posterolateral STEMI
True Posterior STEMI

03/29/2017
8
Reperfusion Arrhythmia: Accelerated Idioventricular Rhythm
Early Repolarization

03/29/2017
9
Pericarditis
Patient with normal coronaries at cath; subsequent diagnosis was myocarditis
Woman with stress CM

03/29/2017
10
Tako‐Tsubo (Stress) Cardiomyopathy:Broken Heart Syndrome
Elderly gentleman with stress CM, postop radical cystectomy, blood loss
Woman with idiopathic CM (EF 20%)

03/29/2017
11
Woman with normal coronary arteries;diagnosis in this patient was HOCM
Hyperkalemia
Hyperkalemia, Severe
03/29/2017
12
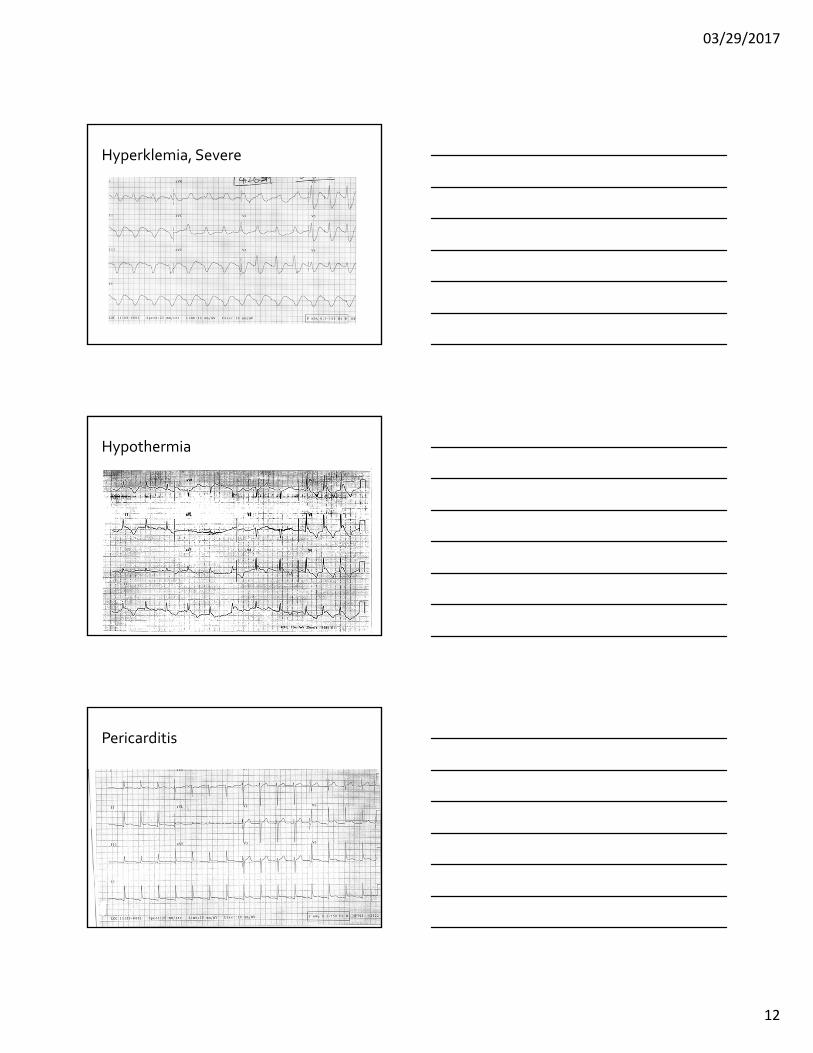
Hyperklemia, Severe
Hypothermia
Pericarditis

03/29/2017
13
1st ECG in patient with hyperkalemia
Same patient as previous slide after resolution of hyperkalemia
1st ECG in patient with severe hyperkalemia
03/29/2017
14
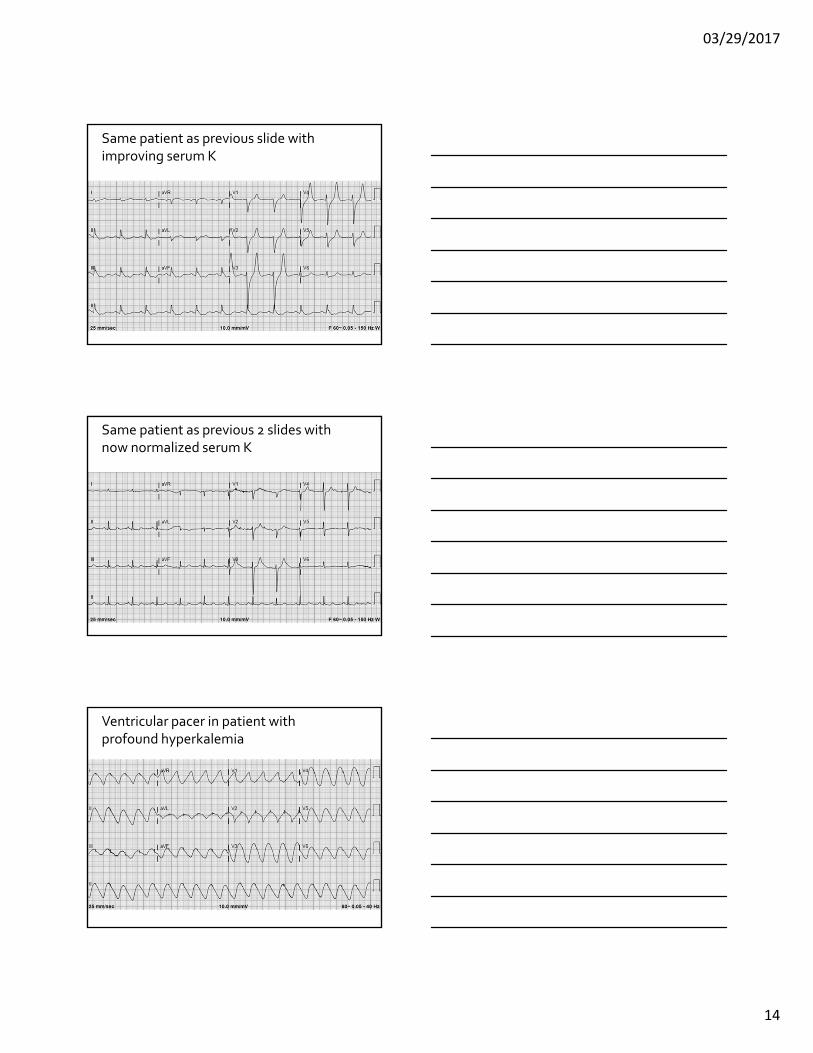
Same patient as previous slide with improving serum K
Same patient as previous 2 slides with now normalized serum K
Ventricular pacer in patient with profound hyperkalemia

03/29/2017
15
Same patient as previous slide after resolution of hyperkalemia
1st ECG after cardiac arrest; severe acidosis pH 6.8 (negative troponin and normal serum K)
Deep T wave Inversion:Neurologic Stroke

03/29/2017
16
• Left Bundle Branch Block• Clinical context• New VsOld
• Paced rhythm
• Posterior STEMI
Some Tough Situations
Bluetooth
Pre-Hospital ECG by EMS

03/29/2017
17
Iferior MI
Just for Fun!















![Cycle 8 report draft 3 - COnnecting REpositories(STEMI) [M] Patients with prehospital diagnosis of STEMI (confirmed on ECG) MC Care bundle for STEMI (M1 + M2 + M3 + M5) Exception to](https://img.pdfslide.us/doc/110x75/5e3775c3f813a914420739db/cycle-8-report-draft-3-connecting-repositories-stemi-m-patients-with-prehospital.jpg)