-
8/14/2019 ECG Interpretation Theory
1/4
ECG Interpretation Theory
The Waveform
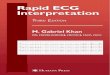
Figure 1: PQRST Complex
The electrocardiograph is a recording of the electrical activity
of the heart. The normal ECGis composed of:
P wave representing atrial depolarisation QRS complex which
represents ventricular depolarisation T wave, representing
ventricular repolarisation Occasionally a U wave can be seen If
present, it will be seen after the T wave.
The direction of flow of electrical conduction or impulse in the
heart is called a vector.Impulses travel from a negative pole to a
positive pole. Impulses traveling toward a positiveelectrode will
be seen as a positive impulse (above the isoelectric line).
Impulses travelingaway from a positive pole will be seen as a
negative impulse (below the isoelectric line).Impulses traveling at
right angles (90 degree angle) to the axis of the lead may be seen
asisoelectric or biphasic.
Areas within a 12 Lead reading:
-
8/14/2019 ECG Interpretation Theory
2/4
ECG Interpretation can be done in 8 steps:
1. Rate and Rhythm
BPM Described as Abbreviation forEscribe
60-100 Sinus Rhythm /sr100 Tachycardia /st
Regular or Irregular? Are the R waves the same distance
apart?
2. P waveRepresents the electrical activity associated with the
initiation of the impulse from the SAnode and the passage through
the atria (atrial depolarisation). If the p wave is present,
upright and of normal morphology (shape) and size, it can be
assumed that the impulseoriginated in the sinus node.
The p wave should be:
Rounded in shape 0.12 seconds 2.5 mV (2.5 mm) in height
Normally upright in left sided and inferior leads (II, III, aVF,
V4 to V6, I and aVL) and invertedin aVR. There should be one p wave
per QRS complex.
3. Check Intervals
PR interval: measured from the beginning of p wave to the
beginning of the QRS, it isisoelectric and represents the time the
impulse is held in the AV node (delay). It is designedto slow down
the impulse to allow for atrial kick (the last 30% of blood ejected
from the atria)and protects ventricles from very fast rates.
The PR interval should be:
0.12-0.20 seconds in duration If it is greater than 0.20
seconds, AV Block is noted
First Degree AV Block: Note prolonged PR interval over 0.2
seconds from prolongedtransmission of impulse through the AV
junction.
Second Degree AV Block Type 1 (Wenckebach): ECG has a
lengthening PR interval.
Second Degree AV Block 2:1 : Every second P wave results in a
dropped beat.
Second Degree AV Block Type II (Mobitz II): Fixed PR and one or
more QRS complexesis dropped.
Third Degree AV Block : Full AV block with no obvious
association or teamwork betweenthe p waves and QRS complex.
-
8/14/2019 ECG Interpretation Theory
3/4
QRS complex : represents ventricular depolarisation, that is,
the time it takes for the impulseto travel down the bundle of His,
bundle branches and Purkinje fibres.
If the QRS interval is
below 0.10 seconds, this is normal if it is between 0.10-0.12,
minor IVCD is noted If it is above 0.12 seconds, IVCD or it can
assume the morphology of Left or Right
Bundle Branch BlockTo differentiate between the two, William
Morrow is a helpful mnemonic.
V1 V6
WiLLiaM
MoRRoW
Within LBBB, a W can be seen in the QRS complex in V1 and an M
in V6.Within RBBB , a M can be seen in the QRS complex in V 1 and
an W in V6.
Determine the Axis
5. Q(q) wave
First downward (negative) deflection May be written as Q or q
depending on the size of the waveform: if it is greater than a
quarter of the R wave it is usually written as a Q Normal Q
waves in leads V5, V6, I and aVL
Abnormal Q waves if a quarter of the height of R wave and less
than 0.04 seconds induration
Septal Q wave (Seen in V1 or V2)
6. R wave Progression
-
8/14/2019 ECG Interpretation Theory
4/4
First upward deflection Can be a R or r wave depending on height
Should become taller (and appear biphasic) than the S wave in
either V3/V4, and R
wave height may decrease slightly in lateral leads.
Premature R wave progression is noted if the QRS is positive
before V3. A R wave isPoor if the QRS does not become positive
until after V5.
7. ST segmentST segment starts at the end of the QRS complex and
terminates at the beginning of the Twave. J point is the junction
where the S wave and ST segment meet and is the indicator
forischaemia. The J point and ST segment should be on the baseline
or isoelectric. Is normal ifit is within 1mm of the isoelectric
line, and abnormal if above 1mm of the isoelectric line,indicates
ischaemia or infarction. Note on interpretation if there is an
abnormality ordownwards deflection of the ST segment.
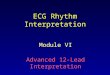
8. T Wave
T wave represents ventricular repolarisation and is normally
upright and rounded. It can beflattened, inverted, biphasic (above
and below the baseline or distorted by ST elevation
ordepression).
Peaked Inverted
Normal if T wave is in the same direction as the QRS complex,
and Normal T wave height is
usually less than two thirds of the R wave height. T wave
inversion in V5/V6 is alwaysabnormal. If present, it is noted as
Widespread/Insert area T wave abnormality.