Embed Size (px)
Citation preview

A good understandingof the electrical activityof the heart is key to theaccurate interpretationof ECGs
ECG interpretation in sm~all anim~als1. Understanding the electricityof the heart MIKE MARTIN
Mike Martingraduated fromDublin in 1986. In1997, he founded hisown cardiorespiratoryreferral practice,the VeterinaryCardiorespiratoryCentre, in Kenilworth,Warwickshire. Heholds the certificateand diploma inveterinary cardiologyand is an RCVSSpecialist inCardiology. He is thecurrent chairmanof the VeterinaryCardiorespiratorySociety and is a pastrecipient of theBSAVA's Dunkin andMelton Awards.
THIS article, the first of three aimed at assisting those in practice in interpreting electrocardiograms(ECGs), discusses the electrical activity of the heart and how this relates to the complexes seen on an ECG.It also describes the clinical findings on auscultation and palpation of the pulse. It must be rememberedthat an ECG trace should always be interpreted in the light of a thorough clinical examination of thecardiovascular system, with particular attention being paid to heart rate and rhythm, pulse rate, andidentification of pulse deficits, if present. The second article in the series, to be published in the nextissue, will discuss the abnormalities associated with the conduction system of the heart. The final article,to be published in the May issue, will outline a practical approach to interpreting ECGs.
THE ELECTRICITY OF THE HEART
The heart must contract in a coordinated atrioventricularsequence to act efficiently as a 'circulatory pump'. To dothis, the cardiac muscle cells must receive an electricalstimulus. It is this electrical activity that is detected byan electrocardiograph (see box below).
The electrical stimulus must first depolarise the twoatria and then, with an appropriate time interval, stimu-late the two ventricles. The heart must then repolarise(while 'refilling') in time for the next electrical stimulusand contraction and must do so repeatedly, increasing inrate with a rise in demand and, conversely, slowing atrest.
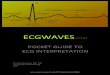
Atrioventricular /Sinoatrial node Atrioventricularnode \ring|
\ Right atrium | Left atrium J
\| / ~~~~~Left\\ {_ _ ~~~bundle
Bundle bacof His
Rightbundle -
branch
Anteriorfascicle
Posterior- fascicle
Purkinje- fibres
anI
Simply put, an electrocardiograph (ECG machine)is a voltmeter (or galvanometer) that records thechanging electrical activity of the heart between a
positive and negative electrode. Electrocardiogra-phy is the process of recording these electricalchanges.
Although a positive and negative electrode can
be placed almost anywe on, or 1n, the body torecord electrical changes, the most common andsimplest method is to place these electrodes on thelegs of an animal. This is referred to as body surfacelimb ECG recording.
The heart's electrical circuit. Reproducedwith permission from Blackwell Science
FORMATION OF THE NORMALP-QRS-T COMPLEXMost of the cells within the heart have the ability to
generate their own electrical activity, but the sinoatrialnode is the fastest to do so and is, therefore, the 'ratecontroller' or pacemaker of the heart. The rate of thesinoatrial node is influenced by the balance in autonomictone, involving the sympathetic (which increases the rate)and parasympathetic (which decreases the rate) systems.
The sinoatrial node normally initiates the electricaldischarge for each cardiac cycle. Depolarisation spreads
In Practice * MARCH 200214
Sinoatrial_nodeI
Right
..
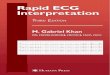
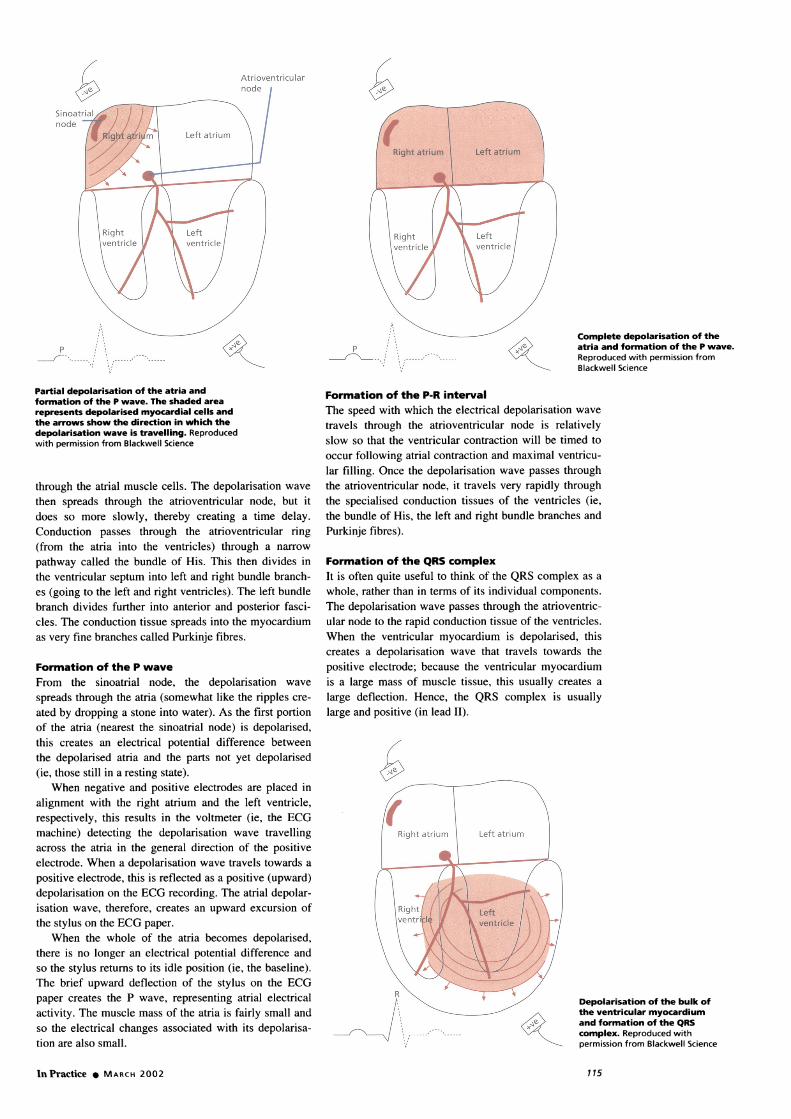
Complete depolarisation of theatria and formation of the P wave.Reproduced with permission fromBlackwell Science
Partial depolarisation of the atria andformation of the P wave. The shaded area
represents depolarised myocardial cells andthe arrows show the direction in which thedepolarisation wave is travelling. Reproducedwith permission from Blackwell Science
through the atrial muscle cells. The depolarisation wave
then spreads through the atrioventricular node, but itdoes so more slowly, thereby creating a time delay.Conduction passes through the atrioventricular ring(from the atria into the ventricles) through a narrow
pathway called the bundle of His. This then divides inthe ventricular septum into left and right bundle branch-es (going to the left and right ventricles). The left bundlebranch divides further into anterior and posterior fasci-cles. The conduction tissue spreads into the myocardiumas very fine branches called Purkinje fibres.
Formation of the P waveFrom the sinoatrial node, the depolarisation wave
spreads through the atria (somewhat like the ripples cre-
ated by dropping a stone into water). As the first portionof the atria (nearest the sinoatrial node) is depolarised,this creates an electrical potential difference betweenthe depolarised atria and the parts not yet depolarised(ie, those still in a resting state).
When negative and positive electrodes are placed inalignment with the right atrium and the left ventricle,respectively, this results in the voltmeter (ie, the ECGmachine) detecting the depolarisation wave travellingacross the atria in the general direction of the positiveelectrode. When a depolarisation wave travels towards a
positive electrode, this is reflected as a positive (upward)depolarisation on the ECG recording. The atrial depolar-isation wave, therefore, creates an upward excursion ofthe stylus on the ECG paper.
When the whole of the atria becomes depolarised,there is no longer an electrical potential difference andso the stylus returns to its idle position (ie, the baseline).The brief upward deflection of the stylus on the ECGpaper creates the P wave, representing atrial electricalactivity. The muscle mass of the atria is fairly small andso the electrical changes associated with its depolarisa-tion are also small.
Formation of the P-R intervalThe speed with which the electrical depolarisation wave
travels through the atrioventricular node is relativelyslow so that the ventricular contraction will be timed to
occur following atrial contraction and maximal ventricu-lar filling. Once the depolarisation wave passes throughthe atrioventricular node, it travels very rapidly throughthe specialised conduction tissues of the ventricles (ie,the bundle of His, the left and right bundle branches andPurkinje fibres).
Formation of the QRS complexIt is often quite useful to think of the QRS complex as a
whole, rather than in terms of its individual components.The depolarisation wave passes through the atrioventric-ular node to the rapid conduction tissue of the ventricles.When the ventricular myocardium is depolarised, thiscreates a depolarisation wave that travels towards thepositive electrode; because the ventricular myocardiumis a large mass of muscle tissue, this usually creates a
large deflection. Hence, the QRS complex is usuallylarge and positive (in lead II).
Depolarisation of the bulk of
the ventricular myocardium
and formation of the QRS
-------------------complex. Reproduced with
permission from Blackwell Science
InPractice * MARCH 2002
Atrioventricularnode I
::,.I.
: I.p :: I."
e-,\ --.: I.
1.
115

Complete depolarisation and repolarisation of the atriaand ventricles and completion of the P-QRS-T complex.Reproduced with permission from Blackwell Science
Formation of the T waveAfter complete depolarisation of the ventricles, they thenrepolarise in time for the next stimulus. This phase ofrepolarisation creates a potential difference across theventricular myocardium until it is completely repolar-ised. This results in a deflection from the baseline (inlead II) which is termed the T wave.
The T wave in dogs and cats is very variable and canbe negative, positive or even biphasic (ie, a bit of both).
QRS
This is because repolarisation of the myocardium insmall animals is a little random compared with humans,for example, in which repolarisation is very organisedand the T waves always share the same polarity as theQRS complexes (irrespective of the lead in which therecording is made). The diagnostic value of abnormali-ties in the T wave of small animals is therefore verylimited (whereas abnormal T waveforms in humans canbe very useful diagnostic features).
SINUS RHYTHMSA normally formed complex is termed a sinus complex;that is, there is a P wave for every QRS complex andT wave (or vice versa). A sequence of beats originatingfrom the sinoatrial node forms a rhythm, known as thesinus rhythm. There are four common sinus rhythms andthese are described below.
Normal sinus rhythmIn normnal sinus rhythm, the stimulus originates regularlyat a constant rate from the sinoatrial node (dominant pace-maker), depolarising the atria and ventricles normnally andproducing a coordinated atrioventricular contraction.
CLINICAL FINDINGS
Regular heart sounds are heard on auscultation (ie, lubbdupp) with a pulse for each heartbeat and at a rate whichis normal for age, breed and species.
ECG FEATURESThe ECG shows a normal P wave followed by normalQRS and T waves. The rhythm is regular (constant) andthe rate is normal for age, breed and species. The sizeof the ECG complexes are typically small in cats and,
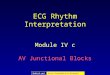
ECG from a dog showing P1normal sinus rhythm at a ~ ~ ~~~K.n ~ ~ \ srate of 140/minute. (Lead 11, ' V 'V "V "I 1 1I cm/mV, 25 mm/second)
ECG from a cat showing QRSnormal sinus rhythm at arate of 220/minute. Some AT .baseline drift associated fwith movement during theECG recording can also beseen. (Lead 11, I cm/mV,25 mm/second)
ORS
ECG from a dog showingrespiratory sinusarrhythmia at a rate ofapproximately 100/minute.Note also the slightvariation in P waveamplitude - this is termeda wandering pacemaker.(Lead 11, I cm/mV,25 mm/second)
116 ~~~~~~~~~~~~~~~~~~~InPractice * MARCH 2002116

therefore, obtaining an artefact-free tracing is importantin order to clearly identify the ECG complexes.
Sinus arrhythmiaIn the case of sinus arrhythmia, the stimulus originatesfrom the sinoatrial node, but the rate varies (increasesand decreases) regularly. This is usually associated withthe variation in autonomic tone which is often synchro-nous with respiration and is therefore sometimes calledrespiratory sinus arrhythmia.
CLINICAL FINDINGS
The heart rhythm varies with some regularity, increasingand decreasing in rate, and there is a pulse for everyheartbeat.
ECG FEATURES
The ECG shows a normal P wave followed by normalQRS and T waves. The rhythm varies in rate, often associ-ated with respiration. The rhythm is sometimes describedas being regularly irregular (ie, the variation in rate is fair-ly regular). The rate is normal for age, breed and species.
Sinus tachycardiaIn the case of sinus tachycardia, the sinoatrial node gen-erates an impulse and depolarisation which occurs fasterthan normal.
CLINICAL FINDINGS
The heart rate is faster than normal for age and breedwith a pulse for every heartbeat (although with a veryfast rate, the pulse may become weaker).
ECG FEATURESThe ECG shows a normal sinus rhythm but at a fasterrate than normal.
Sinus bradycardiaIn the case of sinus bradycardia, the sinoatrial node gen-erates an impulse and depolarisation which occurs moreslowly than normal. This can be a normal feature insome giant-breed dogs and in athletically fit animals.
CLINICAL FINDINGS
The heart rate is slower than normal for age and breed,with a pulse for every heartbeat.
ECG FEATURES
The ECG shows a normal sinus rhythm but at a slowerrate than normal.
ABNORMAL ELECTRICAL ACTIVITYOF THE HEART
Dysrhythmia literally means abnormal rhythm; arrhyth-mia is a synonymous term. Dysrhythmias include abnor-malities in rate, conduction or those associated withectopia (see box below). Dysrhythmias that are essential-ly slow are referred to as bradydysrhythmias, and thosethat are fast are termed tachydysrhythmias.
While there can be considerable variation in the'normal' morphology of a QRS complex for a particularanimal, it is nevertheless important to identify from theECG recording a normal sinus complex for the animalbeing examined. Once a normal complex has been iden-tified, the shape of the QRS complex and the T waveshould be noted. Depolarisation of the ventricles occursby conduction from (or through) the atrioventricularnode to produce this QRS complex and it is therefore ofparamount importance in any tracing to determine whichshape represents the conduction that has arisen via theatrioventricular node, especially if there are a variety ofshapes of QRS complexes.
Ectopia
Ectopia literally means 'in an abnormal place'. Inconnection with the heart, this refers to outside thesinoatrial node, the dominant pacemaker. Ectopicbeats arise as a result of various mechanisms due toa number of causes (eg, cardiac pathology, hypoxia,electrolyte imbalances).
QRS
T
ECG from a dog showing sinus tachycardia at a rate of 200/minute. (Lead 11, 1 cm/mV, 25 mm/second)
11 QRS
: * * * f ~~~~~~~~~~~~~4
ECG from a dog showing sinus bradycardia at a rate of 30 to 40/minute. (Leads 11 and 111, cm/mV, 25 mm/second)
In Practice 0 MARCH 2002 117
Terminology
With an understanding of the terminology used, the interpretation of dysrhyth-mias due to ectopia becomes relatively easy. The term 'beat' implies that therehas been an actual contraction. In 'ECG speak', it is better to use the term
complex or depolarisation to describe waveforms on the ECG. Ectopic complexesmay be classified by the following:* SITE OF ORIGIN. Complexes may be either ventricular or supraventricular innature* TIMING. Ectopic complexes that occur before the next normal complex wouldhave been due are termed premature; those that occur following a pause, suchas a period of sinus arrest or in the case of complete heart block, are termedescape complexes* MORPHOLOGY. If all the ectopics in a tracing have a similar morphology to eachother, they are referred to as uniform; ectopics with different shapes are knownas multiform* NUMBER OF ECTOPICS. Premature ectopic complexes may occur singly, in pairs or
in runs of three or more; the last is referred to as tachycardia. Tachycardia may
be continuous, in which case it is known as persistent or sustained, or may beintermittent, which is termed paroxysmal* FREQUENCY. The number of premature ectopic complexes in a tracing may vary
from occasional to very frequent. When there is a set ratio, such as one sinuscomplex to one ectopic complex, this is known as bigeminy; when there is oneectopic to two sinus complexes, this is termed trigeminy
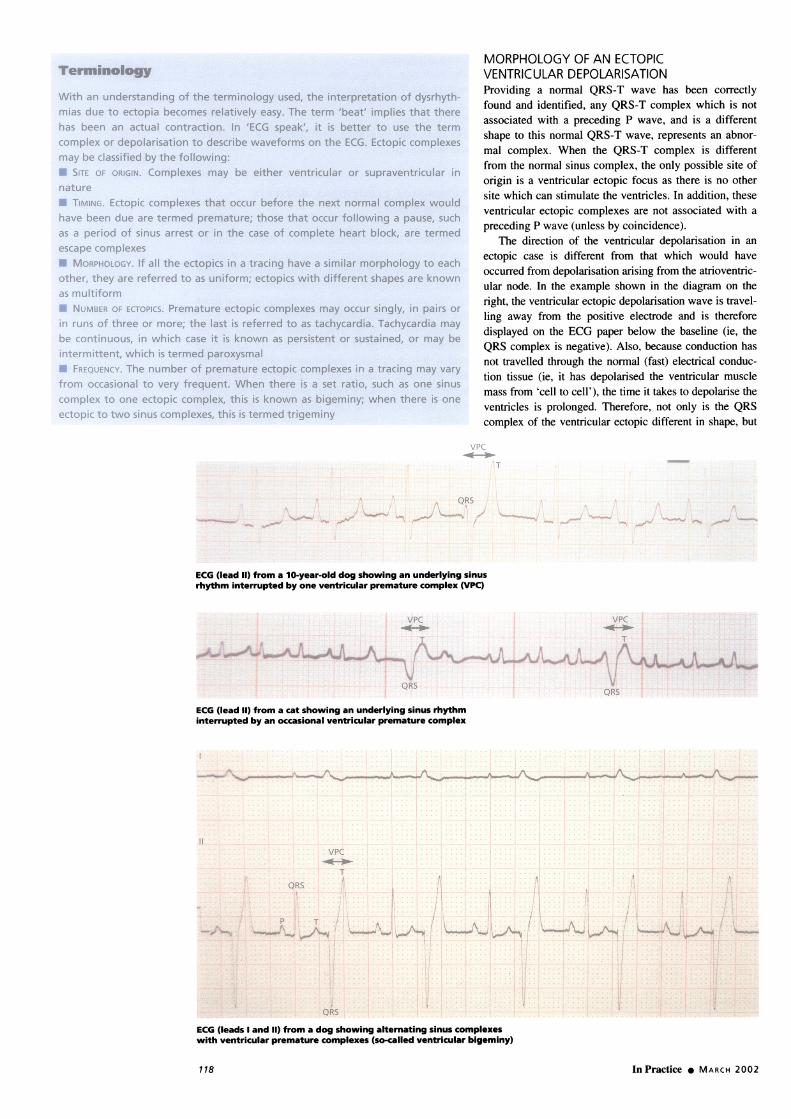
MORPHOLOGY OF AN ECTOPICVENTRICULAR DEPOLARISATIONProviding a normal QRS-T wave has been correctlytound and identified, any QRS-T complex which is notassociated with a preceding P wave, and is a differentshape to this normal QRS-T wave, represents an abnor-mal complex. When the QRS-T complex is differentfrom the normal sinus complex, the only possible site oforigin is a ventricular ectopic focus as there is no othersite which can stimulate the ventricles. In addition, theseventricular ectopic complexes are not associated with apreceding P wave (unless by coincidence).
The direction of the ventricular depolarisation in anectopic case is different from that which would haveoccurred from depolarisation arising from the atrioventric-ular node. In the example shown in the diagram on theright, the ventricular ectopic depolarisation wave is travel-ling away from the positive electrode and is thereforedisplayed on the ECG paper below the baseline (ie, theQRS complex is negative). Also, because conduction hasnot travelled through the normal (fast) electrical conduc-tion tissue (ie, it has depolarised the ventricular musclemass from 'cell to cell'), the time it takes to depolarise theventricles is prolonged. Therefore, not only is the QRScomplex of the ventricular ectopic ditferent in shape, but
vPC
T
, ^ ~~~~~QRS1~~
*-ft -.W e 0% v1 / 'vA
ECG (lead 11) from a 10-year-old dog showing an underlying sinusrhythm interrupted by one ventricular premature complex (VPC)
VPC vPc
Ti
QRS QRS
ECG (lead 11) from a cat showing an underlying sinus rhythminterrupted by an occasional ventricular premature complex
I I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~I
I"'. _-s_,i1
il
A
.( .
it
Ij
ECG (leads I and 11) from a dog showing alternating sinus complexeswith ventricular premature complexes (so-called ventricular bigeminy)
In Practice MARCH 2002
11VPC
T
I'
QRS.,
~~~~~~~~~~~~~ I
.
I,
I
QRS
,'I
:,
1 18
T
A ventrearly), in v
complex. Iwith delaycomplex.
VentriculVentriculain dogs anwithin ththereforemyocardiucell (not w
CLINICAL F
Occasionalthe rhythnrthe 'extra'
tQRS
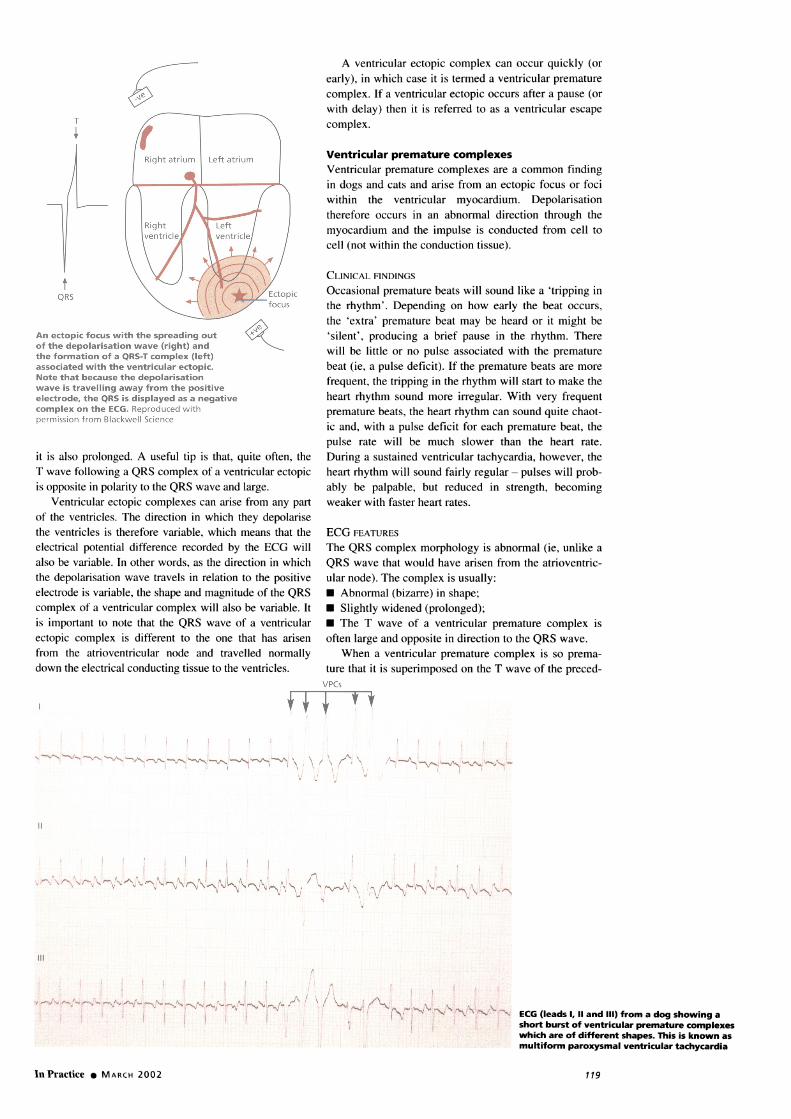
An ectopic focus with the spreading out I, 'silent', pof the depolarisation wave (right) and bthe formation of a QRS-T complex (left) will be litiassociated with the ventricular ectopic. beat (ie, aNote that because the depolarisation frequent, tlwave is travelling away from the positiveelectrode, the QRS is displayed as a negative heart rhytlcomplex on the ECG. Reproduced with prematurepermission from Blackwell Science ic and, wit
pulse rateit is also prolonged. A useful tip is that, quite often, the During a sT wave following a QRS complex of a ventricular ectopic heart rhythis opposite in polarity to the QRS wave and large. ably be p
Ventricular ectopic complexes can arise from any part weaker wilof the ventricles. The direction in which they depolarisethe ventricles is therefore variable, which means that the ECG FEATIelectrical potential difference recorded by the ECG will The QRS ealso be variable. In other words, as the direction in which QRS wavethe depolarisation wave travels in relation to the positive ular node).electrode is variable, the shape and magnitude of the QRS * Abnormcomplex of a ventricular complex will also be variable. It * Slightlyis important to note that the QRS wave of a ventricular * The Tectopic complex is different to the one that has arisen often largefrom the atrioventricular node and travelled normally When a
down the electrical conducting tissue to the ventricles. ture that itvPCs
II + t
ricular ectopic complex can occur quickly (orwhich case it is termed a ventricular prematureIf a ventricular ectopic occurs after a pause (or) then it is referred to as a ventricular escape
lar premature complexesr premature complexes are a common findingd cats and arise from an ectopic focus or focie ventricular myocardium. Depolarisationoccurs in an abnormal direction through theim and the impulse is conducted from cell toiithin the conduction tissue).
FINDINGSLI premature beats will sound like a 'tripping inn'. Depending on how early the beat occurs,'premature beat may be heard or it might beroducing a brief pause in the rhythm. Theretle or no pulse associated with the prematurepulse deficit). If the premature beats are more:he tripping in the rhythm will start to make thehm sound more irregular. With very frequentbeats, the heart rhythm can sound quite chaot-th a pulse deficit for each premature beat, thewill be much slower than the heart rate.
,ustained ventricular tachycardia, however, theim will sound fairly regular- pulses will prob-alpable, but reduced in strength, becomingLth faster heart rates.
URES
complex morphology is abnormal (ie, unlike athat would have arisen from the atrioventric-The complex is usually:
nal (bizarre) in shape;widened (prolonged);wave of a ventricular premature complex isand opposite in direction to the QRS wave.
a ventricular premature complex is so prema-is superimposed on the T wave of the preced-
Illl
! i#~~~I
XA.%1 K'rZ$'; v\ > '~"JlVP0'N ECG (leads 1, 11 and 111) from a dog showing ashort burst of ventricular premature complexeswhich are of different shapes. This is known asmultiform paroxysmal ventricular tachycardia
>
InPractice 0 MARCH 2002 119

ECG from a dog showing thephenomenon of R-on-T. This is wherea ventricular premature complex occursso early that it is superimposed on theT wave of the preceding ventricularpremature complex
inT comi1plex (sinus or ectopic), such that the ventricles
are depolairised before they haxve comipletely repolarisedfrom the preceding contraction, this is term-ied R-on-T.A runi of three or more ventriCular premlature complexesis knows as ventricular tachycar-dia.
MORPHOLOGY OF AN ECTOPICSUPRAVENTRICULAR DEPOLARISATIONAny ectopic stimulus arisinig above the ventricles is
reterred to as Supraventricular and can be divided into:
* Those which occur in the atrial muscle mass (atrialectopics); and* Those which arise firoIml within the atriovenitricularnode or bunldle ot His (junctional or nodal ectopics).
In-espective of where supraventricular ectopics arIise,
they musit traxvel down the bundle ot His and so depolarisethe ventricles as normal. Therefore, the morphology of theQRS complex associated with a supraventricular ectopic
The site of origin ofsupraventricular and ventricular \ectopic complexes. APC, atrialpremature complex;JPC, junctional prematurecomplex; VPC, ventricularpremature complex. Reproducedwith permission from Blackwell Science
is usually norm-i'al - thalt is, the samile as the QRS complexfor a siinus coImlplex (the exception being when there is
(aberrancy). This can make identificcation of a supraventric-
ulalr- ectopic difficLult. In the v ast majority of cases, how-ecer, it OCCurIs as a premature belt, which means that it is
primnartily recognised by its prematue timi-ng. The QRS of
a supraxventricular ectopic complex is the sarme shape as a
QRS of a normal sinus com1lplex and is recognised by its
premature timinlg and, usually, also by the absenice o' a
normal P \waxe.
While the timillg (in relation to its QRS complex) anldthe morphology of the P w axve (whichi iS usually differenitfrom a norm-lal P waxve) can aLid in identifying whether
the ectopic alrose from the atrial (atrial preImatule coIml-plex) or the atrioxentricular node (junctional or nodalpremlaL.ture complex). it is initially of little practicalimportcance in smlall anim-Ials. In addition, it does not
affect the managecrlemnt or treatmiienit in the vast major-ityof cases in smlall animials. Therefore, the distinctiolnbetween atriatl anid junctionial prematul-e coImIplexes
will not be discussed in this article aind both will bereferr-ed to by the broader term. supravxentricular premna-
tli-e comiiplexes.
Supraventricular premature complexesSuprax entricular premntature complexes arise romio 1an
ectopic tOCuS or foci aboxve the xventricles - that is. either
in the atria, the atrioxventriculaIr node or the bundle of'His. The xventricles are thein depolarised normally, hence
producing a normnal shaped QRS complcx with a normal
durationi.
CLINICAxI FINDINCiS
Clinically, it is not possible to distinguish supraventricular premiatLtre beats fromi xventricular premnatul-e beats.Occasional premn-ature beats will sounld like aI 'trippinl in
In Practice MARCH 2002
QRS
QRS
T
QRS
'lil f i;
T
I'
T
ECG from a dog showing only one
normal sinus complex; the rest are
all ventricular premature complexes(occurring at a rate of 200/minute).This is known as ventriculartachycardia
p
-I\r-* V* W i
T
Q~RS-
t
120

I ~~~~~~QRS QRSQR
- - N
77J
ECG from a dog showing a single supraventricular premature complex, recognised by its normal QRS morphology but
premature timing and no identifiable preceding P wave
I -I~I IQRS tQRS QRS
ECG from a dog showing a single supraventricular premature complex. On this occasion, there is a recognisable precedingP wave, which has an abnormal morphology compared to the other P waves - suggesting that this is an atrial prematurecomplex
QRS QRS54
T T~~~~R
T~~~~~ECG from a dog showing a short burst of supraventricular premature complexes this is termed paroxysmal
supraventricular tachycardia
QRS
ECG from a dog showing
a sustained run of
supraventricular premature\J\complexes (at a rate of
in te) this is te d
~~~~~~~~~~~~~~~~~~~~~~~~~Supraventricular tachycardia
the rhythm', with little or no pulse associated with the
premature beat. If the premature beats are more frequent,
the tripping in the rhythm will start to make the heart
rhythm sound more irregular. With very frequent pre-
mature beats, the heart rhythm can sound quite chaotic
and, with a pulse deficit for each premature beat, the
pulse rate will be much slower than the heart rate.
During a sustained supraventricular tachycardia, how-
ever, the heart rhythm will sound fairly regular- pulses
will probably be palpable, but reduced in strength,
becoming weaker with faster heart rates.
ECG FEATURES
QRS-T complexes, which have a normal morphology,
are seen to occur prematurely. The ECG features are:
Normal QRS morphology (except with bundle branch
block);
The QRS complex is seen to occur prematurely;
P waves may or may not be identified;
If P waves are seen, they are usually of an abnormal
morphology (ie, non-sinus) and the P-R interval may
differ from that seen in a normal sinus complex.
A run of three or more supraventricular premature
complexes is termed a supraventricular tachycardia,
which is usually at a rate in excess of 160/minute (but
can be as high as 400/minute) and regular. Supra-
ventricular tachycardias need to be distinguished from
sinus tachycardia.
Atrioventricular dissociation
The term atrioventricular dissociation describes the situ-
ation when the atria and ventricles are depolarised hy
separate, independent foci. This may occur due to an
accelerated junctional or ventricular rhythm, disturbed
atrioventricular conduction or depressed sinoatrial nodal
function.
InPractice MARCH 200212
QRS
121

ECG from a dog showingatrioventricular dissociation.Note how the P waves(arrowed) appear to drift inand out of the QRS complexes
CLINICAL FINDINGS
The heart rhythm will sound fairly normal and the pulseshould match the heart rate.
ECG FEATURES
The ECG shows a ventricular rate that is usually veryslightly faster than the atrial rate. The P waves mayoccur before, during or after the QRS complex. TheP waves and QRS complexes are independent of eachother, with the QRS complexes appearing to 'catch up'on the P waves. Atrioventricular dissociation should bedifferentiated from complete heart block. In the case ofheart block, the ventricular rate is slow and much lowerthan the atrial rate; in atrioventricular dissociation, theatrial and ventricular rates are not dissimilar (and usuallyat a normal or faster rate).
Atrial fibrillationFibrillation means rapid irregular small movements offibres. In atrial fibrillation, one of the most common
arrhythmias seen in small animals, depolarisation waves
occur randomly throughout the atria. As atrial fibrillation
originates above the ventricles, it can also be classifiedas a supraventricular arrhythmia.
CLINICAL FINDINGS
The heart rhythm sounds chaotic and the pulse rate isoften half the heart rate, especially with fast atrial fibril-lation. This is a very common arrhythmia in dogs andcan be strongly suspected on auscultation by its chaoticrhythm and 50 per cent pulse deficit. Very frequentpremature beats (ventricular or supraventricular) can
mimic it.
ECG FEATURES
The QRS complexes have a normal morphology (simi-lar to that of supraventricular premature complexes,described above) and occur at a norm-al to fast rate. TheECG features are:* Normal QRS morphology (except when there isbundle branch block);* The R-R interval is irregular and chaotic (note this is
easier to hear on auscultation!);* The QRS complexes often vary in amplitude;
QRS QRS
T T~~~~~~~~~~~(
ECG from a dog showing atrial fibrillation with a ventricular response rate of 160/minute. Note the normal
(or supraventricular) morphology of the QRS complexes, the chaotic R-R intervals (this is actually easier to
hear on auscultation) and the absence of P waves
Q?RS
,~~~~
III
~~~~Vwv A\~~~~~~~~~~~ECG from a dog showingatrial fibrillation with aventricular response rateof nearly 300/minute
122 ~~~~~~~~~~~~~~~~~~~InPractice * MARCH 2002122

Escape rhythmsWhen the dominant pacemaker tissue (usually thesinoatrial node) fails to discharge for a long period,the pacemaker tissue with a slower intrinsic rate (junc-tional or ventricular) may then discharge and 'escape'control of the sinoatrial node. This is commonly seenin association with bradydysrhythmias (eg, sinusbradycardia, sinus arrest, atrioventricular block).
If escape rhythms did not develop, no electricalactivity of any kind would occur; this is termedasystole. It is a terminal event unless electrical activityreturns (hence, escape complexes are sometimesreferred to as rescue beats). Ventricular standstilloccurs if no escape rhythms develop during completeheart block (ie, there are P waves but no QRS com-
A /~~~~~~
* There are no recognisable P waves preceding theQRS complex;* Sometimes, fine irregular movements of the baseline- known as 'f waves' - are seen as a result of the atrialfibrillation waves. However, frequently these f waves areindistinguishable from baseline artefact (eg, muscletremor) in small animals.
Ventricular fibrillationVentricular fibrillation is nearly always a terminal eventassociated with cardiac arrest. The depolarisation wavesoccur randomly throughout the ventricles. There is there-fore no significant coordinated contraction to produceany cardiac output. If the heart is visualised or palpated,fine irregular movements of the ventricles are evidentand likened to a 'can of worms'. Ventricular fibrillationcan follow ventricular tachycardia.
CLINICAL FINDINGSNo heart sounds are heard. No pulse is palpable.
ECG FEATURESThe ECG shows coarse (larger) or fine (smaller) rapid,irregular and bizarre movement with no normal waves orcomplexes.
AcknowledgementThis article is based on material published in the author's bookentitled 'Small Animal ECGs: An Introductory Guide' (2000),Oxford, Blackwell Science, and is reproduced with permissionof the publisher.
Further readingDARKE, P., BONAGURA, J. D. & KELLY, D. F. (1996) Color Atlasof Veterinary Cardiology. London, Mosby-WolfeFOX, P. R., SISSON, D. & MOISE, N. S. (1999) Textbook of Canineand Feline Cardiology. Philadelphia, W. B. SaundersKITTLESON, M. D. & KIENLE, R. D. (1998) Small AnimalCardiovascular Medicine. St Louis, MosbyLUIS FUENTES, V. & SWIFT, S. (1998) Manual of Small AnimalCardiorespiratory Medicine and Surgery. Cheltenham, BSAVAMARTIN, M. (2000) Small Animal ECGs: An Introductory Guide.Oxford, Blackwell Science
plexes). Again, if ventricular electrical activity doesnot return, death is imminent.
Junctional escapes are fairly normal in shape(ie, junctional ectopic), whereas ventricular escapesare abnormal and bizarre (ie, ventricular ectopic).A continuous junctional escape rhythm occurs at arate of 60 to 70/minute and a continuous ventricularescape rhythm occurs at a rate of less than50/minute. Both types of escape rhythm may be seenin complete atrioventricular block.
As escape rhythms are rescue beats, they shouldnot be suppressed by any form of treatment.Treatment should be directed towards the under-lying bradydysrhythmia.
, ,
ECG showing ventricularfibrillation. Note the randomunorganised deflections
MARTIN, M. & CORCORAN, B. (1997) Cardiorespiratory Diseaseof the Dog and Cat. Oxford, Blackwell ScienceSMITH, F. W. R. & TILLEY, L. P. (1992) Rapid Interpretation of HeartSounds, Murmurs, and Arrhythmias. Philadelphia, Lea & FebigerTILLEY, L. P. (1992) Essentials of Canine and FelineElectrocardiography: Interpretation and Treatment, 3rd edn.Philadelphia, Lea & FebigerTILLEY, L. P. (1992) Self Assessment: Small Animal Arrhythmias.Philadelphia, Lea & Febiger
In Practice * MARCH 2002
InPracticeBinders
Binders for In Practice are available from:
McMillan-Scott Subscriber Services,6 Bourne Enterprise Centre, Wrotham Road,
Borough Green, Kent TN15 8DGTelephone 01732 884023, Fax 01732 884034
BVA members' price £7.50 (inc postage)
The red-coloured binders each hold a year'ssupply of issues
Payment with order please
123