-
8/13/2019 ECG basics and interpretations
1/12
-
8/13/2019 ECG basics and interpretations
2/12
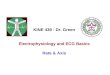
he electrical a)is is normally downward and to the left !ut we
can estimate it more accurately inindividual patients if we
understand from which direction* each recording lead measures the
ECG.
Figure 2. !rientation of the li"# leads sho$ing the direction
fro" $hich each lead%loo&s% at the heart
y convention, we record the standard surface ECG using /0
different recording lead directions,*though rather confusingly only
/1 recording electrodes on the skin are re2uired to achieve this.
'i)of these are recorded from the chest overlying the heart + the
chest or precordial leads . 3our arerecorded from the lim!s + the
limb leads . It is essential that each of the /1 recording
electrodes is
placed in its correct position, otherwise the appearance of the
ECG will !e changed significantly,preventing correct
interpretation.
he lim! leads record the ECG in the coronal plane, and so can !e
used to determine the electricala)is "which is usually measured
only in the coronal plane$. he lim! leads are called leads I, II,
III,A, A&L and A&3. 3igure 0 shows the relative directions
from which they look* at the heart. Ahori4ontal line through the
heart and directed to the left "e)actly in the direction of lead I$
isconventionally la!elled as the reference point of 1 degrees "1
o$. he directions from which otherleads look* at the heart are
descri!ed in terms of the angle in degrees from this !aseline.
he electrical a)is of depolarisation is also e)pressed in
degrees and is normally in the range from%51 1 to 6 71 1 . A
detailed e)planation of how to determine the a)is is !eyond the
scope of this
article !ut the principles mentioned here should help readers to
understand the concepts involved.
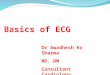
he chest leads record the ECG in the transverse or hori4ontal
plane, and are called &/, &0, &5, &8,&9 and
&: "see 3igure 5$.
Figure . 'ransverse section of the chest sho$ing the orientation
of the six chest leadsin relation to the heart
oltage and ti"ing intervals
It is conventional to record the ECG using standard measures for
amplitude of the electrical signaland for the speed at which the
paper moves during the recording. his allows;
Easy appreciation of heart rates and cardiac intervals and
-
8/13/2019 ECG basics and interpretations
3/12
wave inmost leads of an ECG, the > wave is in fact the sum of
the electrical signals from the two atria,which are usually
superimposed.
here is then a short, physiological delay as the
atrioventricular "A&$ node slows the electricaldepolarisation
!efore it proceeds to the ventricles. his delay is responsi!le for
the ># interval, ashort period where no electrical activity is
seen on the ECG, represented !y a straight hori4ontal or
isoelectric* line.
?epolarisation of the ventricles results in usually the largest
part of the ECG signal "!ecause of thegreater muscle mass in the
ventricles$ and this is known as the /* co"plex .
he @ wave is the first initial downward or negative* deflection
he # wave is then the ne)t upward deflection "provided it crosses
the isoelectric line and
!ecomes positive*$
he ' wave is then the ne)t deflection downwards, provided it
crosses the isoelectric line to!ecome !riefly negative !efore
returning to the isoelectric !aseline.
-
8/13/2019 ECG basics and interpretations
4/12
In the case of the ventricles, there is also an electrical
signal reflecting repolarisation of themyocardium. his is shown as
the *' seg"ent and the ' $ave . he ' segment is
normallyisoelectric, and the wave in most leads is an upright
deflection of varia!le amplitude and duration"see 3igures 9 and
:$.
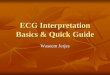
Figure 0. 'he "a or $aves of a single nor"a
l ECG pattern
Figure . Exa"ple of a nor"al 12 lead ECG3 notice the do$n$ard
deflection of all signalsrecorded fro" lead a /. 'his is nor"al+ as
the electrical axis is directly a$ay fro" thatlead
4or"al intervals
he recording of an ECG on standard paper allows the time taken
for the various phases ofelectrical depolarisation to !e measured,
usually in milliseconds. here is a recognised normalrange for such
intervals*;
-/ interval "measured from the !eginning of the > wave to the
first deflection of the @#'comple)$. ormal range /01 + 011 ms "5 +
9 small s2uares on ECG paper$.
/* duration "measured from first deflection of @#' comple) to
end of @#' comple) atisoelectric line$. ormal range up to /01 ms "5
small s2uares on ECG paper$.
' interval "measured from first deflection of @#' comple) to end
of wave at isoelectricline$. ormal range up to 881 ms "though
varies with heart rate and may !e slightly longer infemales$
Heart rate esti"ation fro" the ECG
'tandard ECG paper allows an appro)imate estimation of the heart
rate "(#$ from an ECGrecording. Each second of time is represented
!y 091 mm "9 large s2uares$ along the hori4ontala)is. 'o if the
num!er of large s2uares !etween each @#' comple) is;
9 % the (# is :1 !eats per minute. 5 % the (# is /11 per
minute.
0 % the (# is /91 per minute.
-
8/13/2019 ECG basics and interpretations
5/12
-
8/13/2019 ECG basics and interpretations
6/12
-
8/13/2019 ECG basics and interpretations
7/12
iagrams (elo7 indicate 7hich part the heart is (eing affected
and 7hat lead 7ouldsho7 the changes.
Reciprocal +hanges
Region of ! levation Region of ! epression Anterior leads V#4V%)
8nferior true posterior)
8nferior leads 88$ 888$ aVF) Anterior leads V#4V3 or lateral
lead#. aVL)Lateral leads 8$ aVF$ V&$
V') 8nferior leads 88$ 888$ aVF)
!rue Posterior Anterior leads V#4V3)#2 lead rapid assessment
erify a / is negative 8ssess rate and rhyth"
8xis deter"ination % Leads I and a&3
Conduction a#nor"alities9
L % seen in &/(ypertrophyAneurysm>ericarditis?rugs or
ElectrolytesEarly repolari4ation
6sche"ia+ 6n ury+ 6nfarct signs9
%wave inversions' segment elevation'ignificant @ waves
8cute =6 pattern9
8nterior9
' elevation in &/, &0, &5, &8' depression in II,
III, a&3
6nferior9 ' elevation in II, III, a&3
' depression in &/, &0, &5, or I, a&L
5ateral9 ' elevation in I, a&L, &9, &:
' depression in II, II, a&3
-
8/13/2019 ECG basics and interpretations
8/12
*eptal $all9 ' elevation in I, a&L, &/, &0-osterior9
tall and wide # waves and ' depression in &/, &0/ight
entricular9 ' elevations in &8#, &9#, &:#
"9 additional right chest wall electrodes placed on the chest in
the same positions as theprecordial leads$
Clinical pressentaion 'reat"ent plan
Electrical Current9
lectricity al7ays flo7s from positive to negative. !he
electrical current should flo7from negative to positive in the
normal healthy heart. o$ if this pattern is disrupted (ya 0detour0
or as in the heart$ 0an infarct0 or 0in"ury0 the +: recording 7ill
indicate thea(normal flo7 of current. =ith an infarcted heart$ the
electrical current flo7s opposite
of 7here it is e1pected to flo7. ence$ the elevated or depressed
! segment . Forinstance$ an inferior infaction 7ill sho7 an
elevation in lead 88$ 888 and aVF. !he normal
flo7 7ould (e 0isoelectrical0 and the ! segment 7ould (e
e>ualized or level. 6ut$ sincethe flo7 is going (ac*7ards around
the damaged heart muscle$ 7e see an elevation onthe record. 8t is
this precise measurement that can dictate e1actly 7here the infarct
islocated. 8f the ! segment is elevated in V2$ V3 and V%$ the
infarct is anterior. !hese
vie7s are loo*ing at the front or anterior area of the heart
muscle. !he current isflo7ing to7ard the positive electrode on the
patients chest. =hen the current is
disrupted$ it 7ill sho7 as an elevation in the ! segment versus
an isoelectric reading.
!hin* of it li*e this, An ?ray film is placed (ehind the heart
at the area (et7een theVentrical eptum. !he ?4Ray machine shoots
the picture from the anterior heart directly
a(ove the film. and the film catures the image. =e 7ould (e
loo*ing at the area of theheart at the eptal region 7hich 7ould (e
in +: terminology V3.
!he infract area 7ill have no electrical current. !he ! segment
7ill (e depressed !he in"ured area 7ill have ! elevations and 7ill
release +ardiac 9uscle enzimes.
!hese enzimes are +@$ 9yo:lo(in and !roponin 8
!he ishemic area may have ! elevations and +: cahnges to include
PV+ s$ PA+ sand PB+ s.
!he #2 Lead Photograph imulatneous a>uisition 2.& seconds
per vie7$ #/
seconds for a complete study
8 aVR V# V%
88 aVL V2 V&
888 aVF V3 V'#2 lead +:C a real time vedio recording of the
hearts electrical function.
!his record indicates a 0septal D anterior 8nfarct.0
-
8/13/2019 ECG basics and interpretations
9/12
8f you can comprehend 7hich 7ay the current is e1pected to flo7
in !he ?A?8AL V8 =and !he PR +-R 8AL V8 = of the heart$ then you
can diagnose 7hich area is effected ifit is an a(normal flo7...
ee the information (elo7.
#2 lead rapid interpretation +ommon +: Formation
6sceh"ia>6nverted ' $aves Inverted wave is symmetrical
waves are usually upright in leads I, II, and &0%&:6n
ury>Elevated *' seg"ent
'ignifies an acute process ' returns to !aseline with time If '
elevation is diffuse and unassociated with @ wavesor reciprocal
'
depression, consider pericarditis
Location of injury can !e determined in same manner as infarct
location
Fsually associated with reciprocal ' depression in other
leads6nfarction> $ave
'mall @s may !e normal in &9, &:, I and a&L A!normal
@ must !e one small s2uare "1.18 sec$ wide
Also a!normal if @%wave depth is greater than one%third of @#'
height inlead III
9a*ing the accurate Field iagnosis,
!here are elevations # mm )in t7o contegous connecting)
leads,Leads ad"acent to eachother...
!here is at least one lead 7ith reciprocal changes..
8f the E 7ave is more than #D3 the size of the R 7ave...
!a(le (elo7 sho7s 7hat the +: 7ould loo* li*e in the Vector
7here the heart is (eingaffescted. All other areas 7ould loo*
normal$ 7ithout elevation or depression. unless
there is an 0old 98.0 8n that case$ the prior damage 7ould sho7
up as a depressedsegment.
-
8/13/2019 ECG basics and interpretations
10/12
Anterior 8nfarction ' elevation without a!normal @ wave
Fsually associated with occlusion of the left anterior decending
!ranch ofthe left coronary artery "LCA$
Lateral 8nfarction ' elevation with without a!normal @ wave
-
8/13/2019 ECG basics and interpretations
11/12
-
8/13/2019 ECG basics and interpretations
12/12
important to paramnedic in the pre%hospital phase !ecause the
developement of the @%wave maytake hours and could easily !e missed
in the field.
Eventually, the ' segment will return to its !aseline and the
%wave resumes its normal position,leaving only the @%wave as
evidence that an infarction has occurred. #ecent research and
studieshave produced 79J accuracy in field diagnosis !y paramedics.
>erhaps some reasons wouldinclude other indications for '
changes. hey would include simple angina, drug effects,
andelectrolyte im!alance.