Embed Size (px)
DESCRIPTION
ECG 2 Kids
Citation preview

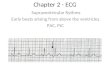
ECG #2[Cardiac Dysrhythmias]

SA NODE
AV NODE
RIGHT BUNDLE BRANCH
LEFT BUNDLE BRANCH
PURKINJEE FIBERS
ELECTRICAL CONDUCTION OF THE HEART

Common Pediatric ArrhythmiasMost common dysrhythmias in children are: • Supraventricular tachycardia• Bradycardia• Sinus arrhythmia
• Atrial fibrillation• Atrial flutter• Ventricular tachycardia and fibrillation• Rarely found in children.
• However! Children with congenital heart disease may present with any arrhythmia!
• Abnormal rhythms specifically related to their heart disease or damage caused by surgical repair are the arrhythmias most usually seen. [Blocks!]

A Quick Note About Dominance and T Waves
• Right ventricular dominance determined by analyzing a 12-lead ECG
• Larger portion of the QRS waveform in V1.• With right ventricular dominance, the R
wave is larger than the S wave in V1.
• Also T Wave inversion in V1-V3 Normal

Before we start looking at the rhythms
• Why do people have arrhythmias?
• What is the difference between a bad arrhythmia and a not-so-bad arrhythmia?

What do we look at when reading rhythms
• Assess the rate
• Assess rhythm/regularity
• Identify and examine P waves
• Assess intervals (evaluate conduction)
– PR interval, QRS duration, QT interval
• Evaluate overall appearance of the rhythm
– ST segment elevation/depression
– T wave inversion
• Interpret rhythm and evaluate clinical significance

Rhythm/Regularity
• When analyzing a rhythm strip, determine:– Atrial (P-P intervals) rhythm
– Ventricular (R-R intervals) rhythm
• If rhythm is regular, R-R intervals (or P-P intervals if assessing atrial rhythm) are same
– Plus or minus 10% acceptable

Sinus Dysrhythmias

Sinus RhythmRate 60-100 beats/min
Rhythm Regular
P waves Uniform in appearance, positive (upright) in lead II, one precedes each QRS complex
PR interval
0.12-0.20 second and constant from beat to beat
QRS 0.10 second or less

Sinus Rhythm

Sinus BradycardiaRate Less than 60 beats/min
Rhythm Regular
P waves Uniform in appearance, positive (upright) in lead II, one precedes each QRS complex
PR interval 0.12-0.20 second and constant from beat to beat
QRS 0.10 second or less

• In adults a rate less than 60• But variability in heart rates in pediatric
patients For example, heart rate of 80 in a newborn infant would be considered sinus bradycardia.
• Sinus bradycardia is a common rhythm of children in severe distress.
• Cardiovascular system response to hypoxia and certain drugs.


Sinus Tachycardia
Rate 101 - 180 beats/min
Rhythm Regular
P waves Uniform in appearance, positive (upright) in lead II, one precedes each QRS complex; at very fast rates it may be difficult to distinguish a P wave from a T wave
PR interval 0.12-0.20 second and constant from beat to beat
QRS 0.10 second or less


Sinus Arrhythmia
Rate 60 - 100 beats/min
Rhythm Irregular
P waves Uniform in appearance, positive (upright) in lead II, one precedes each QRS complex; at very fast rates it may be difficult to distinguish a P wave from a T wave
PR interval 0.12-0.20 second and constant from beat to beat
QRS 0.10 second or less


Atrial Dysrhythmias

Premature Atrial Complexes
Rate Usually within normal range, but depends on underlying rhythm
Rhythm Regular with premature beats
P waves Premature (occurring earlier than the next expected sinus P wave), positive (upright) in lead II, one precedes each QRS complex, often differ in shape from sinus P waves – may be flattened, notched, pointed, biphasic, or lost in the preceding T wave
PR interval May be normal or prolonged depending on the prematurity of the beat
QRS Usually less than 0.10 second but may be wide (aberrant) or absent, depending on the prematurity of the beat. The QRS of the PAC is similar in shape to those of the underlying rhythm unless the PAC is abnormally conducted.

Premature Atrial Complexes (PACs)

Wandering Atrial Pacemaker
Rate 60-100 bpm
Rhythm Irregula
P waves P waves vary in shape depending on site of impulse origin. May be upright, inverted, or biphasic. Must see three (3) different P wave shapes to diagnose WAP.
PR interval 0.12-0.20 seconds (variable)
QRS Usually less than 0.10 second.


SVT
Usually less than 0.10 secondQRS
Not measurablePR interval
No identifiable P wavesP Waves
Ventricular regular or irregular depending on AV conduction/blockade Rhythm
Atrial rate is unknown. Ventricular rate is 150-180 beats/min — determined by AV blockade.
Rate


• Most common arrhythmia seen in children. • It includes a variety of rhythms that emanate from the
sinus, atrial, or junctional areas of the heart. • By definition, all but ventricular rhythms are considered
supraventricular. • Supraventricular tachycardia is differentiated from sinus
tachycardia by the unusually fast rate and the patient's presentation.
• It can occur in normal healthy infants, children, and adolescents with an accessory pathway such as Wolf-Parkinson-White syndrome (WPW). [L to R in atria]

Px• Effect on the child must be assessed. • Can be asymptomatic or in extreme distress.• Child- asymptomatic should be continually monitored
and treated by a pediatric cardiologist.• Rapid rate decreases diastolic filling time, the child
also can have evidence of low cardiac output and poor systemic perfusion.
• If the child is showing signs of poor perfusion, the rhythm should be treated promptly with IV adenosine.
• If the child has inadequate blood pressure, then he or she should undergo synchronized cardioversion

Atrial Tachycardia
Usually less than 0.10 secondQRS
0.12-0.20 secondsPR interval
Abnormal morphology, often “perky”P Waves
Ventricular regular or irregular depending on AV conduction/blockade Rhythm
Atrial rate is unknown. Ventricular rate is 150-180 beats/min — determined by AV blockade.
Rate


Atrial Fibrillation
Usually less than 0.10 second but may be widened if an intraventricular conduction delay exists
QRS Duration
Not measurablePRI
No identifiable P waves; fibrillatory waves present. Erratic, wavy baseline. P Waves
Ventricular rhythm usually irregularly irregular Rhythm
Atrial rate usually greater than 400-600 beats/min; ventricular rate variable Rate

Atrial Fibrillation
• Atria are depolarized at a rate of 400 to 600 beats/min– the muscles of the atria to quiver (fibrillate)
• Results in:– Ineffectual atrial contraction
– Subsequent decrease in cardiac output
– Loss of atrial kick

Atrial Fibrillation

Atrial Flutter
Usually less than 0.10 second but may be widened if flutter waves are buried in QRS complex or an intraventricular conduction delay exists.
QRS
Not measurablePRI
No identifiable P waves; saw-toothed “flutter” waves are present P Waves
Atrial regular, ventricular regular or irregular depending on AV conduction/blockade
Rhythm
Atrial rate 250-350 beats/min, typically 300 beats/min; ventricular rate variable — determined by AV blockade. The ventricular rate will usually not exceed 180 beats per minute due to the intrinsic conduction rate of the AV junction.
Rate

Atrial Flutter

Premature Junctional Contractions [PJC’s]
Usually less than 0.10 second but may be wide (aberrant) or absent, depending on the prematurity of the beat. The QRS of the PJC is similar in shape to those of the underlying rhythm unless the PJC is abnormally conducted.
QRS
Absent or less than 0.12 secondsPR interval
Absent or invertedP Waves
IrregularRhythm
Atrial rate 250-350 beats/min, typically 300 beats/min; ventricular rate variable — determined by AV blockade. The ventricular rate will usually not exceed 180 beats per minute due to the intrinsic conduction rate of the AV junction. 60-100 bpm
Rate


Junctional Rhythm
Usually less than 0.10 secondsQRS
Absent or less than 0.12 secondsPR interval
Absent or invertedP Waves
RegularRhythm
40-60 bpmRate


Accelerated Junctional Rhythm
Usually less than 0.10 secondsQRS
Absent or less than 0.12 secondsPR interval
Absent or invertedP Waves
RegularRhythm
60-100 bpmRate


Junctional Tachycardia
Usually less than 0.10 secondsQRS
Absent or less than 0.12 secondsPR interval
Absent or invertedP Waves
RegularRhythm
Greater than 100 bpmRate


Blocks

First-Degree AV BlockRate Usually within normal range, but depends on underlying rhythm
Rhythm Regular
P waves Normal in size and shape, one positive (upright) P wave before each QRS in leads II, III, and aVF
PR interval Prolonged (greater than 0.20 second) but constant
QRS duration Usually 0.10 sec or less unless an intraventricular conduction delay exists

First-Degree AV Block

Second-Degree AV Block, Type I - Wenkebach
Rate Atrial rate is greater than the ventricular rate
Rhythm Atrial regular (P’s plot through); ventricular irregular
P waves Normal in size and shape. Some P waves are not followed by a QRS complex (more P’s than QRS’s).
PR interval Lengthens with each cycle (although lengthening may be very slight), until a P wave appears without a QRS complex. The PRI after the nonconducted beat is shorter than the interval preceding the nonconducted beat.
QRS Usually 0.10 second or less but is periodically dropped

Second-Degree AV Block, Type I

Second-Degree AV Block, Type II
Rate Atrial rate is greater than the ventricular rate. Ventricular rate is often slow.
Rhythm Atrial regular (P’s plot through). Ventricular irregular.
P waves Normal in size and shape. Some P waves are not followed by a QRS complex (more P’s than QRS’s).
PRI Within normal limits or slightly prolonged but constant for the conducted beats. There may be some shortening of the PR interval that follows a nonconducted P wave.
QRS Usually 0.10 second or greater, periodically absent after P waves

Second Degree AV Block (Mobitz
type II)

Complete AV BlockRate Atrial rate is greater than the ventricular rate. The ventricular rate is
determined by the origin of the escape rhythm.
Rhythm Atrial regular (P’s plot through). Ventricular regular. There is no relationship between the atrial and ventricular rhythms.
P waves Normal in size and shape.
PR interval None — the atria and ventricles beat independently of each other, thus there is no true PR interval.
QRS Narrow or wide depending on the location of the escape pacemaker and the condition of the intraventricular conduction system. Narrow = junctional pacemaker, wide = ventricular pacemaker.

Complete AV Block

Ventricular Dysrhythmias

Premature Ventricular Contractions (PVC’s)
Rate Depends on underlying rhythm
Rhythm Irregular
P waves Not present before most PVC’s
PR interval Generally not present
QRS duration Greater than 0.12 seconds


Idioventricular RhythmRate Less than 40 beats/minute
Rhythm Essentially regular
P waves May be present or absent. If present, they have no set relationship to the QRS complexes appearing between the QRS’s at a rate different from that of the IR.
PR interval Variable
QRS duration Greater than 0.12 second; often difficult to differentiate between the QRS and T wave


Accelerated Idioventricular RhythmRate Less than 40-100 beats/minute
Rhythm Essentially regular
P waves May be present or absent. If present, they have no set relationship to the QRS complexes appearing between the QRS’s at a rate different from that of the IR.
PR interval Variable
QRS duration Greater than 0.12 second; often difficult to differentiate between the QRS and T wave


Ventricular Tachycardia (VT)Rate 101-250 beats/minute
Rhythm Essentially regular
P waves May be present or absent. If present, they have no set relationship to the QRS complexes appearing between the QRS’s at a rate different from that of the VT.
PR interval None
QRS duration Greater than 0.12 second; often difficult to differentiate between the QRS and T wave

Ventricular Tachycardia

Torsades de Pointes (TdP)

Ventricular Fibrillation (VF)
Rate Cannot be determined because there are no discernible waves or complexes to measure
Rhythm Rapid and chaotic with no pattern or regularity
P waves Not discernible
PR Not discernible
QRS Not discernible

Ventricular Fibrillation (VF)

Ventricular Fibrillation• This dysrhythmia results in the absence of
cardiac output • The course of treatment for ventricular fibrillation
includes:– immediate defibrillation and ACLS protocols– Identification and treatment of the underlying cause is also needed

AsystoleRate Ventricular usually not discernible but atrial activity may be
observed (“P-wave” asystole)
Rhythm Ventricular not discernible, atrial may be discernible
P waves Usually not discernible
PRI Not measurable
QRS Absent

Asystole

Pulseless Electrical Activity

PEA – Causes• Hypovolemia
• Hydrogen Ions
• Hypoxia
• Hypothermia
• Hypo-/hyperkalemia
• Hypoglycemia
• Tension Pneumothorax
• Tamponade
• Thromboemboli (PE, MI)
• Toxins - Drug overdose / accidents (cyclic antidepressants, calcium channel blockers, beta-blockers, digoxin)
• Trauma

What do we look at when reading rhythms
• Assess the rate
• Assess rhythm/regularity
• Identify and examine P waves
• Assess intervals (evaluate conduction)
– PR interval, QRS duration,
• Evaluate overall appearance of the rhythm
– ST segment elevation/depression
– T wave inversion
• Interpret rhythm and evaluate clinical significance

What do we need to remember as Critical Care Nurses?
• Let’s start with what I don't need you to know– Ability to recognize funky weird rhythms– Ability to read all rhythms

OK now that we have establish what you don't have to know
what do I expect you to know?

• Every shift print off rhythm strip and place in chart
• Identify – Reg/irreg, PR interval, rate and rhythm– SR, SB, A. Fib, A. flutter, VT and VF – A
MUST– Something is wrong rhythms – the rest
• Know enough to get some help reading them

Remember
• Not always able to name an abnormal rhythm, but:
• Know normal rhythms
• Know fatal rhythms
• Report these rhythms

![Operating Manual Resting and Stress ECG · 2 [2] Resting and Stress ECG hardware, custo cardio 300 | page 6 Resting and Stress ECG Hardware, description of device for custo cardio](https://img.pdfslide.us/doc/110x75/6045c0eda729ce28bd5868a8/operating-manual-resting-and-stress-ecg-2-2-resting-and-stress-ecg-hardware-custo.jpg)
![Biometric Identification Using JPEG2000 Compressed ECG Signals · Fig.1 Block diagram of the 2-D ECG compression scheme[14]. Fig.2 Typical ECG waveform in time-domain. 2.1 Signal](https://img.pdfslide.us/doc/110x75/5f087eac7e708231d4224a9b/biometric-identiication-using-jpeg2000-compressed-ecg-signals-fig1-block-diagram.jpg)






![ECG Signal processing (2) ECE, UA. ECG signal processing - Case [1] Diagnosis of Cardiovascular Abnormalities From Compressed ECG: A Data Mining-Based](https://img.pdfslide.us/doc/110x75/56649dbf5503460f94ab3016/ecg-signal-processing-2-ece-ua-ecg-signal-processing-case-1-diagnosis.jpg)