Embed Size (px)
Citation preview

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 1/56
Lecture OutlineSee Syllabus for Detailed Objectives
1. Basis of the electrocardiogram
2. Review conductive athways
!. Standard limb leads". #$% waves& comle'es& intervals&
segments
(. )ector analysis of ventricular
deolari*ation
+. ,ugmented limb leads
-. $hest leads

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 2/56
he #lectrocardiogram
,s the cardiac mass deolari*es& time varying
differences in electrical otential e'ist on the bodysurface. he electrocardiogram is a recording of these
otential differences. he electrocardiogram is
roduced by a se/uence of cardiac action otentials0 it
is not a recording of an action otential.
#lectrohysiologists sea of the interior of the cell being
negative relative to the outside& whereas electrocardiograhers
sea of the cell being ositive on the outside relative to the
inside. hile this may seem confusing& the meaning is the same.
o roduce an electrocardiogram& cardiac cell membranes
deolari*e 3transition from ositive outside to negative outside4 in
se/uence& both in time and sace& as those membranes
e'erience action otentials.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 3/56
he entire surface of a stri of resting myocardium is ositively
charged 3relative to the interior of the cells of the fiber4 so that no
otential difference e'ists between electrodes , and B. , stri chart
recording of this #$% 3right 4 records *ero otential difference and so
remains at its baseline.
+-

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 4/56
he stri of myocardium deicted has been stimulated at its left side and
is now slightly more than half deolari*ed 3shaded area4. he surface of
the deolari*ed area is negatively charged 3relative to the interior of thecells of the fiber4 so that electrode B 3the ositive electrode4 is facing a
region of greater ositivity than is electrode ,. he stri chart recorder
at the right& which has been wired so that an uward deflection is written
when the ositive electrode B is more ositive than ,& thus inscribes an
ositive 3above baseline4 deflection. he deflection in this #$% reachesits ma'imum when e'actly half of the myocardial stri is deolari*ed.
- +

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 5/56
he stri of myocardium is now fully deolari*ed. hen the actionotentials of all cells are in hase 2& their e'ternal surfaces are negative
relative to their interiors. Because no otential differences e'ist along the
e'ternal 3or internal4 surfaces of the cells in the stri of myocardium&
electrodes , and B both face a similar degree of negativity. he
deflection in the #$% 3right 4 thus returns to the baseline and remainsthere until reolari*ation begins.
+-

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 6/56
Stri of myocardium in which reolari*ation has begun in the same
region that was first to be deolari*ed& i.e.& at the left. Because the cell
e'teriors in the reolari*ed region of the stri 3left4 have returned to
their normal& resting ositivity& ositive electrode B is facing a region of
greater negativity than is electrode ,. he #$% at the right thusinscribes a negative 3downward4 deflection.
+-
5f reolari*ation had
roceeded fromright to left& another&
identical uright
3ositive4 deflection
would have been
roduced.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 7/56
,fter the stri of myocardium has returned to its fully reolari*ed
state& the #$% 3right 4 returns to its baseline.
+-

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 8/56
• , wave of deolari*ation aroaching a
ositive electrode of an #$% lead systemcauses a ositive deflection. 3Some te'ts describe this
as 6current flow7 toward the ositive electrode.4
5t then follows that8
• , wave of deolari*ation moving away from a
ositive electrode of an #$% lead system causes a
negative deflection.
• , wave of reolari*ation aroaching a ositive
electrode of an #$% lead system causes a negative
deflection.
• , wave of reolari*ation moving away from a
ositive electrode of an #$% lead system causes aositive deflection.
REMEMBER THIS!!!!!

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 9/56
, ositive deflection means the tracing is above the
isoelectric 3*ero mv4 line. Such a deflection may be
ascending or descending. On the wave below& all
oints are 9OS55)#. On the descending limb& thedirection of deolari*ation is toward the ositive
electrode& just as it was on the ascending limb.
:;;;;;;;;;;;;;;;;;;;;;;;;;;;;;;;;;;- ;;;;;;;;;;;;;;;;;;;;;;

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 10/56

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 11/56
aves& $omle'es& Segments& and 5ntervals of the
#lectrocardiogram
ave8 Deflection that returns toward the 6baseline.7
$omle'es8 9ortion of the #$% that contains more than one wave.
Segment8 9ortion of the #$% that contains no wave.
5nterval8 9ortion of the #$% that contains at least one wave and one segment.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 12/56
aves& $omle'es& Segments& and 5ntervals of the #lectrocardiogram
<ote vertical and hori*ontal scales.
:.2 sec
:.:=
sec

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 13/56
Standard #$% limb
leads. hen the
electrical a'is 3netdirection of ventricular
deolari*ation4 is
directed downward and
to the left 3i.e.& toward
the ositive electrodeof lead 554& an uward
deflection of the #$%
occurs.
<ormally the net
direction of ventricular
deolari*ation is nearly
arallel to Lead 55.
.
L L
L ,R ,

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 14/56
Reflection of the vector of ventricular deolari*ation 3,4 on the
a'is of limb lead 5 3B4.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 15/56
>+: ?
9rojection of the vector of ventricular deolari*ation
3,4 on the a'es of the three limb leads
Learn to draw these a'es with correct angles and locations of theositive and negative electrodes.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 16/56

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 17/56
5f @RS is isoelectric in any lead& the direction of ventricular
deolari*ation will be erendicular to that a'is.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 18/56
Standard Limb Leads& ,ugmented Limb Leads& and Standard $hest Leads
Right
,rm
Right
,rm

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 19/56
,'es of the Standard and ,ugmented Limb LeadsLearn to draw these a'es with correct angles and locations of the
ositive and negative electrodes. <ote that the augmented limb leadsbisect the angles of the standard limb leads.
>!: ?
, f th St d d d , t d Li b L d

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 20/56
> 5
; a)R
> 55
> a)A> 555
;
a)L
; 5
>a)R
; 55;a)A
; 555
> a)L
,'es of the Standard and ,ugmented Limb Leads.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 21/56
9 di l $h t L d

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 22/56
9recordial or $hest Leads
6$urrent flow7 e/uals 6direction of deolari*ation.7

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 23/56
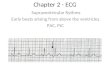
Standard $hest Leads
Why does the ECG change from V1 to V6?

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 24/56
Lecture OutlineSee Syllabus for Detailed Objectives
1. ,bnormal waves and durations
2. ,ltered ventricular deolari*ation
!. Deolari*ation during diastole current of injury
". ,bnormal rates
(. $onduction blocs
+. #arly and abnormal e'citation ectoic beats and
reentry
-. Alutter and fibrillation
Many slides are from Textbook of Medical
Physiology by Guyton

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 25/56
,lterations in the @RS )oltage
• Cyertrohy increases voltage.
• Loss of myocardium decreases voltage.
• #'cessive fluid around the heart decreases voltage.
• #'cessive air in the lunges decreases voltage.
Guyton, Textbook of Medical Physiology, 7 ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 26/56
Duration of the @RS $omle'
<ormal8 :.:+: ; :.1:: sec
Duration increases with
• Cyertrohy
• Bundle Branch Bloc

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 27/56
,'es of the three biolar and three uniolar leads.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 28/56

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 29/56
Right ,'is DeviationR) Cyertrohy Due to 9ulmonary Stenosis
Guyton, Textbook of Medical Physiology, 7 ed
L ft , i D i ti D t S t i

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 30/56
Left ,'is Deviation Due to Systemic
Cyertension
%uyton& e'tboo of edical 9hysiology& - ed
L ft , i D i ti

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 31/56
Left ,'is DeviationLeft Bundle Branch Bloc
Guyton, Tetboo! of Medical "hysiology, # ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 32/56

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 33/56
Dislacement of the S Segment
$urrent of 5njury

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 34/56
$urrent of 5njury
he resence of deolari*ed myocardium during diastole shifts
the #$% away from the isoelectric line during diastole.
Cowever& by convention& we reference systolic ortions of the
#$% to the diastolic segment. hus& ischemic injury aears to
roduce S segment elevation or deression. $linically
seaing& S segment dislacement is an indication ofm ocardial ischemia.
During the S segment&
all of the ventricular
myocardium is
deolari*ed& so the
#$% is on the : m)&
isoelectric line. his is
true whether or notinjured tissue is
resent.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 35/56
Rhythms and ,rrhythmias
• Sinus 3S, nodal4 ; 5s the rate normalE
• #ctoic ; here is the abnormal acemaerE
• ,tria ; Suraventricular
• ,) <ode ; Suraventricular
• )entricle
• Reentry ; hereE
• $onduction Blocs ; hereE $onstant or
5ntermittentE
• 9ree'citation Syndromes ; #lectrical $onduction
Shortcut

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 36/56
Sinus achycardiaCeart Rate #'ceeding 1:: BeatsFinute
%uyton& e'tboo of edical 9hysiology& - ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 37/56

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 38/56
Sinus BradycardiaCeart Rate Less than +: BeatsFinute
%uyton& e'tboo of edical 9hysiology& - ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 39/56
Sinus ,rrhythmia
Ceart Rate 5ncreases During 5nsiration andDecreases During #'iration
%uyton& e'tboo of edical 9hysiology& - ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 40/56

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 41/56
S, <odal Bloc
%uyton& e'tboo of edical 9hysiology& - ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 42/56
Airst Degree ,) Bloc9rolonged 9R 5nterval
3greater than :.2: sec4
%uyton& e'tboo of edical 9hysiology& - ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 43/56
Second Degree ,) BlocOccasional Droed )entricular Beat
%uyton& e'tboo of edical 9hysiology& - ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 44/56
hird Degree ; $omlete ; ,) Bloc
%uyton& e'tboo of edical 9hysiology& - ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 45/56
9remature ,trial $ontraction39,$4
%uyton& e'tboo of edical 9hysiology& - ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 46/56
,) <odal 9remature $ontraction
%uyton& e'tboo of edical 9hysiology& - ed
<ote normal @RS comle'.
9remature )entricular $ontraction

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 47/56
9remature )entricular $ontraction
39)$4
<ote characteristics of a 9)$ that does not originate high in the
ventricular conduction system8
1. %reater duration& 24 Gnusual shae& !4 Aollowed by altered wave.
%uyton& e'tboo of edical 9hysiology& - ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 48/56
)entricular 9aro'ysmal achycardia
%uyton& e'tboo of edical 9hysiology& - ed

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 49/56
Reentry
Ree'citation of cardiac tissue through whiche'citation had reviously assed. here is no
new acemaer discharge.
, necessary condition for reentry is a region
with one;way conduction of e'citation& i.e.&
unidirectional bloc.
he refractory eriod of the reentered region
must be shorter than the roagation timearound the loo.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 50/56
Gnidirectional
Bloc

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 51/56
$onditions hat Aavor Reentry
• Slow conduction velocity
• Long athways
• Short Refractory eriods

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 52/56

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 53/56
,trial Alutter
%uyton& e'tboo of edical 9hysiology& - ed
<ote irregular ventricular rhythm.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 54/56
,trial Aibrillation
%uyton& e'tboo of edical 9hysiology& - ed
<ote irregular ventricular rhythm.

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 55/56

7/23/2019 ECG 1 and 2 2012
http://slidepdf.com/reader/full/ecg-1-and-2-2012 56/56
)entricular Aibrillation
%uyton& e'tboo of edical 9hysiology& - ed