-
7/31/2019 Ecb Ch04 Pancreas
1/22
Ultrasound of the pancreas 28.07.2010 18:06 1
EFSUMB European Course Book
Editor: Christoph F. Dietrich
PancreasDOnofrio Mirko1, Vullierme Marie-Pierre2, Vlek
Vlastimil3, Principe Francesco1,
Canestrini Stefano1, Gallotti Anna
1, Pozzi Mucelli Roberto
1
1Department of Radiology, GB Rossi University Hospital, Verona,
Italy;
2Department of
Radiology, Beaujon Hospital, Paris, France;3Department of
Radiology, Brno University
Hospital, Czech Republic.
-
7/31/2019 Ecb Ch04 Pancreas
2/22
Ultrasound of the pancreas 28.07.2010 18:06 2
Content
Content
.......................................................................................................................................
2
Topographic Remarks
................................................................................................................2
Pancreas
anatomy.......................................................................................................................
2
Pancreatic and peripancreatic veins
.......................................................................................3Pancreatic
and peripancreatic arteries
....................................................................................3
Pancreatic ductal system
........................................................................................................
3
Pancreas
development............................................................................................................4
US study of the pancreas and anatomy
......................................................................................4
Doppler study of the pancreas and vascular
anatomy................................................................6
Pancreatic diffuse inflammatory
disease....................................................................................
8
Acute
pancreatitis...................................................................................................................
8
Chronic
pancreatitis................................................................................................................
9
Autoimmune pancreatitis
.....................................................................................................
10
Pancreatic focal inflammatory disease
.....................................................................................12
Mass-forming
pancreatitis....................................................................................................
12Pseudocyst............................................................................................................................
12
Pancreatic solid neoplasm
........................................................................................................
13
Ductal adenocarcinoma
........................................................................................................
13
Endocrine tumors
.................................................................................................................
14
Lymphoma
...........................................................................................................................
16
Metastases
............................................................................................................................
16
Pancreatic cystic
neoplasm.......................................................................................................
16
Serous
cystadenoma.............................................................................................................16
Mucin producing neoplasms
................................................................................................
17
Mucinous
cystoadenoma..................................................................................................
17Mucinous cystoadenocarcinoma
......................................................................................18
IPMN....................................................................................................................................19
References
................................................................................................................................
19
Topographic Remarks
The pancreas is a medium retroperitoneal organ, slightly
flattened and tapered, located
transversally in front of the main vessels, at the level of the
first or second lumbar vertebra. It
has to be considered a quite fixed posterior organ.
It presents a sligthly oblique shape extending left-upward, with
the cephalic portion generallyin a lower position compared to the
body and the tail. It lies against the vertebral column,
which determines a slight curvature of the organ, and is
surrounded by soft retroperitoneal and
peritoneal tissue.
Pancreas anatomy
The pancreas is a compound racemose gland, which exocrine
excretion of is represented by
the pancreatic juice, an important digestive fluid, while the
endocrine secretion consists of
enzymes involved in sugar metabolism.
The pancreas is usually divided in four parts: head, with the
uncinate process, neck, body andtail.
-
7/31/2019 Ecb Ch04 Pancreas
3/22
Ultrasound of the pancreas 28.07.2010 18:06 3
The head lies within the curve of the duodenum and appears
completely leaned against the
posterior abdominal wall in contact with the inferior vena cava
behind and the portal vein at
the top.
The uncinate process originates from the lower left portion of
the head and lies posteriorly to
the superior mesenteric vessels.
The neck or isthmus generally appears as a slight constriction
connecting the head to thebody. It is located in front of the
superior mesenteric vein and completely overlaid on its
anterior surface by the posterior parietal peritoneum; its
postero-inferior surface is related to
the origin of the portal vein, formed by the junction of the
superior mesenteric and splenic
veins.
The body appears leaned against the posterior abdominal wall by
the white line of Toldt. Here
the posterior parietal peritoneum, which overlays the front face
of the pancreatic body, limits
the posterior face of the epiploon retrocavity. The pancreatic
body is frontally covered by the
gastric cavity while posteriorly is in contact with the splenic
vein; moreover it is related with
the superior mesenteric artery and the left renal vein, which
courses between the superior
mesenteric artery and the aorta to merge into the inferior vena
cava. The superior margin is
slightly anteriorly crossed by the splenic artery, which arises
from the celiac artery, whereasthe inferior margin lies upon the
duodenojejunal flexure.
The tail is quite posteriorly orientated, left-upward, getting
in touch with the splenic hilum as
well as the left adrenal gland and upper kidney. It represents
the mobile part of the gland and,
similarly to the body, is separated from the stomach by the
epiploon retrocavity.
The anteroposterior dimension of the pancreas varies greatly
among individuals and tends to
decrease with the age. The indicative measurements are: head 2
cm; neck 1 cm; body and
tail 1-2 cm, whereas the mean length is 13-15 cm [(1)].
Pancreatic and peripancreatic veins
The veins of the pancreas open into the splenic and superior
mesenteric veins, from whichjunction the portal vein
originates.
The superior mesenteric vein runs over the uncinate process,
whereas the splenic vein, rising
from the splenic hilum, courses along the supero-posterior
surface of the pancreas.
Pancreatic and peripancreatic arteries
The arteries of the pancreas derive from the splenic and the
pancreaticoduodenal branches of
the hepatic and superior mesenteric arteries.
The splenic artery, arising from the celiac artery, runs along
the superior margin of the gland.
From it, some arteries perpendicular to the splenic artery,
enter the bodys and tails
parenchyma. In 92% of cases also the common hepatic artery,
which courses along thesuperior margin of first portion of the
duodenum and continues into the proper hepatic and
gastroduodenal arteries, arises from the celiac artery [(2)].
The gastroduodenal artery courses
along its ventral surface.
The superior mesenteric artery, arising from the aorta behind
the lower portion of the
pancreatic body, courses anteriorly to the uncinate process and
the third portion of the
duodenum.
Pancreatic ductal system
The pancreatic ductal system is represented by the main
pancreatic duct (Wirsungs duct) and
the accessory, functional or not, pancreatic duct (Santorinis
duct).
-
7/31/2019 Ecb Ch04 Pancreas
4/22
Ultrasound of the pancreas 28.07.2010 18:06 4
The main pancreatic duct takes origin from the junction of the
small ducts of the tail lobules.
It ranges transversely from the left to the right through the
substance of the pancreatic body to
flow into the major duodenal papilla (of Vater) jointly with the
common bile duct. It appears
as a thin hypoechoic line bordered by two echogenic margins and
its diameter varies from a
maximum of 3 mm in young adults to 5 mm in the erderly. The
common bile duct, crossing
the anterior surface of the portal vein to the right of the
proper hepatic artery, runs behind thefirst portion of the duodenum
to arrive into the parenchyma of the pancreatic head, close to
the second portion of the duodenum.
The accessory pancreatic duct (Santorinis duct) originates from
the duct of Wirsung and
crosses just the head of the pancreas, more superficially than
to the main duct, to flow into the
minor duodenal papilla, 2 cm higher than the major one.
Pancreas development
The pancreas developes in two parts, the dorsal and the ventral.
The dorsal part arises as a
diverticulum from the dorsal side of the duodenum, just above
the hepatic digression and,
growing upward and backward into the dorsal mesogastrium, forms
a part of the head and theuncinate process as well as body and tail
as a whole.
The ventral portion appears as a diverticulum from the primitive
bile-duct, forming the
remaining part of the head and the uncinate process. As a
consequence the duct of the dorsal
part (accessory pancreatic duct) opens independently into the
duodenum, while the duct of the
ventral part (main pancreatic duct) opens together with the
common bile-duct. Around the
sixth week of gestation the two parts of the pancreas meet and
fuse, establishing a
communication between their ducts. After that, the terminal part
of the accessory duct
undergoes just a little enlargement and its opening into the
duodenum is sometimes
obliterated, whereas the pancreatic duct increases in size and
forms the main duct of the
gland.
At first the pancreas is directed upward and backward between
the two layers of the dorsalmesogastrium, which give it a complete
peritoneal sheath, its surfaces facing the right and the
left side. With the change in the position of the stomach, the
dorsal mesogastrium is drawn
downward and to the left, so that the right side of the pancreas
is directed backward and the
left forward. The right surface ends connected to the posterior
abdominal wall and the
peritoneum covering it undergoes absorption; thus, in the adult,
the gland appears to lie
behind the peritoneal cavity.
US study of the pancreas and anatomy
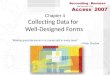
The study of the pancreas includes transverse, longitudinal and
angled oblique scan planes[Figure 1].
-
7/31/2019 Ecb Ch04 Pancreas
5/22
Ultrasound of the pancreas 28.07.2010 18:06 5
Figure 1 Pancreas. Ultrasound oblique scan of the pancreatic
gland with visualization of thepancreatic tail, the body, the
isthmus and the upper part of the head of the pancreas.
The plane passing through the emergency of the celiac trunk
should identify the body-tail, in
relation with the presence of gastric gas; the left portions of
the gland result partially covered
by bowel gas.
The plane passing through the splenic vein demonstrates the
typical comma morphology,
and by this scan is easily possible to evidence the body with
the Wirsungs duct [Figure 2]
and the isthmus of the pancreas on the vein confluence of the
splenic with the superior
mesenteric.
At the level of the lateral border of the head are often seen
ventrally the gastroduodenal artery,represented by anechoic image,
and dorsally the common bile duct.
Figure 2 Wirsungs duct. Ultrasound oblique scan of the
pancreatic body with visualizationof the main pancreatic duct
(arrow).
-
7/31/2019 Ecb Ch04 Pancreas
6/22
Ultrasound of the pancreas 28.07.2010 18:06 6
The scan passing through the mesenteric vessels visualizes the
lower portion of the pancreatic
head and the uncinate process, anatomically located between the
superior mesenteric vein and
the inferior vena cava. Moreover the superior mesenteric artery
appears in front of the aorta,
to the left of the superior mesenteric vein.
The longitudinal scans are executed on the four anatomic parts
of the pancreas. The head is
visualized in all its extension, as well as its relationship
with the inferior vena cava. Itscephalic portion is cranially
delimited by the portal vein and the first duodenal part; more
caudally it relates with the third duodenal portion.
By a longitudinal and slightly oblique scan is usually possible
to visualize the intra-pancreatic
common bile duct [Figure 3].
Figure 3 Intrapancreatic common bile duct. Ultrasound
longitudinal and slightly obliquescan of the pancreatic head with
visualization of the Wirsungs duct and theintrapancreatic tract of
the common bile duct (arrow).
The scans at the neck level need the superior mesenteric vein as
reference point; it is
visualizable up to the junction with the splenic vein. Just more
dorsally is possible to
recognize the uncinate process.
The Wirsungs duct can be visualized at the level of the
pancreatic body [Figure 2].
The reference point on the body is represented by the splenic
vessels, transversally orientated,
which course on the superior border.
The tail can be visualized by a longitudinal anterior scan, even
if the demonstration of thisanatomic structure is often difficult,
owing to the gastric gas covering.
The left intercostal scans are generally used to localize the
caudal portion by using the splenic
acustic window.
Doppler study of the pancreas and vascular anatomy
Doppler studies are an integral part of ultrasound examination
of the pancreas [(3)].
The peripancreatic vascular structures evaluated and well
recognized are the portal vein, the
tripod trunk, the splenic artery and vein, the gastrodudenal
artery, the superior mesenteric
artery and vein, the aorta and the inferior vena cava; whereas
just a few parenchymal vessels
are usually appreciable in normal conditions. However the
visualization of smaller
-
7/31/2019 Ecb Ch04 Pancreas
7/22
Ultrasound of the pancreas 28.07.2010 18:06 7
peripancreatic [Figure 4] and intrapancreatic [Figure 5] vessels
is possible thanks to the
increased Doppler sensitivity.
Figure 4 Gastroduodenal artery. Color-Doppler ultrasound
longitudinal scan of the
pancreatic head with the visualization of the gastroduodenal
artery.
Figure 5 Pancreatic arterial arcades. Power-Doppler ultrasound
transversal scan of thepancreatic head with the visualization of
the pancreatic arterial arcades.
Clinical applications of the Doppler studies of peripancreatic
vessels include the assessment
of patency and features of blood flow.
Doppler and pulsed-Doppler appearance of peripancreatic vessels
has been well documented
[(1;2)]. In normal conditions, the mean speed of blood in
peripancreatic arteries is about 103
18 cm/s in the celiac trunk, 78 16 cm/s in the hepatic artery,
85 18 cm/s in the splenic
artery and 100 22 cm/s in the superior mesenteric artery [(1)].
Mean portal flow velocity is
-
7/31/2019 Ecb Ch04 Pancreas
8/22
Ultrasound of the pancreas 28.07.2010 18:06 8
12-20 cm/s. The resistance index in the superior mesenteric
artery is in general higher than in
the other arterial vessels [(1)].
Abnormal signals and physiological variations in Doppler
waveform in peripancreatic vessels
are not quite understood, because of the influence of
physiologic, pharmacologic and
pathological conditions [(1)]. However, Doppler examination
allows recognizing the changes
produced by diseases in peripancreatic vessels.
Pancreatic diffuse inflammatory disease
Acute pancreatitis
Acute pancreatitis is an acute inflammatory process that may
include suppuration, necrosis
and hemorrhage of pancreatic tissue, with variable involvement
of other regional and remote
tissues. Diagnosis is usually based on the laboratory assay of
serum amylase and lipase levels
[(3)]. Acute pancreatitis is classified as mild (interstitial
edema) [Figure 6] or severe (necrosis,
fluid collections) [Figure 7]. Biliary stones can be detected at
the time of the diagnosis.Peripancreatic collections [Figure 7] and
then pseudocysts follow the different timing of the
disease.
Figure 6 Mild acute pancreatitis. Ultrasound oblique scan of the
pancreatic gland showsenlargement of the gland with the body
appearing slightly hypoechoic in respect tothe head.
-
7/31/2019 Ecb Ch04 Pancreas
9/22
Ultrasound of the pancreas 28.07.2010 18:06 9
Figure 7 Severe acute pancreatitis and pancreatic fluid
collection. Ultrasound oblique scan ofthe pancreatic glad with
visualization of huge inhomogeneous fluid collection at
thepancreatic body-tail.
Normal US findings can be seen in patients with mild acute
pancreatitis. Although the
pancreas can appear normal in acute pancreatitis, the most
frequent findings are focal or
diffuse enlargement of the gland with a decrease of normal
echogenicity [Figure 6].
The pancreas is seen as more hypoechoic than the liver and the
pancreatic texture may also
appear heterogeneous. Acute pancreatitis can be focal or
diffuse, depending on its distribution
[(4)].
At contrast-enhanced ultrasound (CEUS) the pancreatic segment
involved by mild acute
pancreatitis shows an increased contrast enhancement due to
hyperemia. Severe acute
pancreatitis is characterized by the presence of large confluent
necrotic areas and CEUS may
improve the identification and delimitation of the these
necrotic areas, which appear as
avascular at dynamic imaging [(5;6)].
Chronic pancreatitis
Chronic pancreatitis is an inflammatory disease characterized by
the replacement of the
pancreatic glandular elements by fibrous tissue. It is
clinically characterized by a progressive
pancreatic functional loss [(7)]. Although early morphologic
changes of chronic pancreatitis
are difficult to recognize at imaging, the findings of advanced
disease are readily detected.
Alterations in size of the pancreas may be seen in fewer than
half of patients affected by
chronic pancreatitis [(8-10)]. Atrophy and focal alterations in
pancreatic size are the mosteasily identified changes, expression
of advanced stages. The glandular contours appear
irregular, sharp and sometimes lumpy.
Echogenicity of the pancreas is usually increased in chronic
pancreatitis due to adipose
infiltration [(11)] and fibrosis [(12-14)]. However since the
presence in elderly and obese
subjects, it is not a specific parameter. Parenchymal echo
structure alteration, on the other
hand, is a more specific sign of chronic pancreatitis. The
pancreatic echotexture is
inhomogeneous and coarse due to the coexistence of hyperechoic
and hypoechoic foci,
fibrosis and inflammation signs respectively [(12;14)]. These
findings are described in 50%-
70% of cases [(9;10)]. In patients affected by severe exocrine
pancreatic insufficiency this
percentage increases to about 80% [(8)], therefore showing the
fairly good sensitivity of this
finding. Apparent normality of the glandular echotexture in
chronic pancreatitis is reported in
the literature in up to 40% of cases and expected especially in
the early stages of the disease
-
7/31/2019 Ecb Ch04 Pancreas
10/22
Ultrasound of the pancreas 28.07.2010 18:06 10
[(9; 1517)]. However, state-of-the-art US imaging has good
capabilities for identifying the
fine alterations of glandular texture present in the early
stages of the disease, making the
evaluation of pancreatic echostructural alterations an important
finding for diagnosis.
The most important diagnostic criterion for chronic pancreatitis
is the presence of pancreatic
calcifications [(18)], whose identification is
pathognomonic.
Caliber abnormalities in chronic pancreatitis are essentially
represented by main pancreaticduct dilation.
Wirsungs duct can be considered dilated when its caliber is
larger than 3 mm [(14)], with a
sensitivity of about 60%70% [(10;11)] and a specificity, of
about 80%90% [(10;19;20)].
The limits of the reported sensitivity reflect the minor
frequency of duct dilation in initial
and/or light cases of chronic pancreatitis. In the early phases
of chronic pancreatitis the
Wirsung duct may have a normal diameter [(12)]. Moreover,
compression of the main
pancreatic duct may lead to secondary obstructive chronic
pancreatitis upstream of the
obstacle, with the same pathogenetic mechanism. Solid and cystic
lesions may cause duct
compression (benign) or infiltration (malignant) if contiguous
to the main pancreatic duct,
with progressive development of obstructive chronic pancreatitis
upstream [(11)].
Therefore the most significant US findings in chronic
pancreatitis are pancreatic duct dilationand intraductal
calcifications [Figure 8].
Figure 8 Chronic pancreatitis. Ultrasound oblique scan of the
pancreatic glad shows mainpancreatic duct dilation and
calcifications.
Autoimmune pancreatitis
Autoimmune pancreatitis is a particular type of chronic
pancreatitis, with a very recent
pathological definition. It is characterized by periductal
inflammation, mainly substained by
lymphocytic infiltration, with evolution to fibrosis. As opposed
to the other forms of chronic
pancreatitis, the pancreas is increased in volume, usually in a
diffused way with the typical
sausage aspect and the Wirsung duct is compressed or string-like
[(21)]. US features
include reduced echogenicity of the gland, diffuse or focal
pancreatic enlargement, absence of
any fluid collection or calcification. US findings are typical
in the diffuse form when the
entire gland is involved [Figure 9a]. The Wirsungs duct is
compressed by glandular inflamed
parenchyma. The overall sensitivity of US in the diagnosis of
chronic pancreatitis is variable,with an average range in most
series of 60%70% [(7;8)].
-
7/31/2019 Ecb Ch04 Pancreas
11/22
Ultrasound of the pancreas 28.07.2010 18:06 11
Figure 9 Autoimmune pancreatitis. a) Ultrasound oblique scan of
the pancreatic glad showsdiffuse enlargement of the gland with the
typical sausage aspect in absence of anyfluid collection or
calcification. b) at CEUS diffuse moderate enhancement is
visible.
a
b
CEUS of autoimmune pancreatitis shows moderate diffuse
enhancement in the early contrast-enhanced phase, though
inhomogeneous [Figure 9b].
Contrast medium washout is usually slow but progressive. CEUS
findings may be especially
useful in the study of focal forms of autoimmune chronic
pancreatitis, in which differential
diagnosis with ductal adenocarcinoma is a priority [(22)].
Autoimmune chronic pancreatitis
shows a remarkable response to steroid therapy because of its
autoimmune pathogenesis
[(23;24)].
-
7/31/2019 Ecb Ch04 Pancreas
12/22
Ultrasound of the pancreas 28.07.2010 18:06 12
Pancreatic focal inflammatory disease
Mass-forming pancreatitis
Mass-forming chronic pancreatitis usually occurs in patients
with a history of chronic
pancreatitis [(25)] and must be differentiated from pancreatic
ductal adenocarcinoma. AtCEUS, a mass-forming chronic pancreatitis
shows a parenchymographic enhancement,
characterized by an enhancement pattern always comparable to
that of the surrounding
pancreatic parenchyma. However, in long-standing chronic
inflammatory processes,
inhomogeneous hypovascularization of the lesion may be observed,
probably owing to the
presence of a large amount of fibrosis and the differential
diagnosis becomes more difficult
[(5;26;27)].
Pseudocyst
Pseudocysts can be a complication of severe acute pancreatitis
[Figure 10] or can occur in
chronic pancreatitis [(22)]. Characterized by a fibrous wall
without an epithelial lining [(28)],pseudocysts must be
differentiated from pancreatic cystic tumors, especially
mucinous
cystadenomas (MCAs), as they require completely different
therapeutic approaches [(28)].
CEUS has a crucial role in differential diagnosis of pseudocysts
and pancreatic cystic tumors,
better evaluating the micro-vascularization of the intralesional
inclusions.
Figure 10 Pseudocyst. Ultrasound oblique scan of the pancreatic
body shows huge roundedcystic lesion after severe acute
pancreatitis.
Even if characterized by an inhomogeneous content at
conventional US, all the inclusions in
pseudocysts are always completely avascular, becoming
homogeneously anechoic during
CEUS examination [(26)].
-
7/31/2019 Ecb Ch04 Pancreas
13/22
Ultrasound of the pancreas 28.07.2010 18:06 13
Pancreatic solid neoplasm
Ductal adenocarcinoma
About 90% of pancreatic tumors are ductal adenocarcinomas.
Theyre composed of
infiltrating epithelium resuming ductal structures. In almost
two thirds of patients withpancreatic adenocarcinoma, the tumor is
located in the head of the pancreas; while involves
the body and/or the tail, or diffusely infiltrates the entire
gland in the rest of them.
Macroscopically, ductal adenocarcinoma appears as schirrous
infiltrating mass [(29-32)].
Masses in the head of the pancreas cause a ductal obstruction
with secondary dilation of both
the common bile duct and the pancreatic duct, resulting in the
so-called double-duct sign.
However this presentation can also be present in the case of
chronic pancreatitis. In
particularly aggressive forms of adenocarcinoma the development
of necrosis or colliquation
is common, resulting from the difference between the growth rate
and the formation of
microvessels by angiogenesis. The necrotic/fluid part of the
tumor is mainly located centrally.
A ductal adenocarcinoma is characterized by infiltrative margins
with diffusion to the tumor
to the adjacent parenchyma and structures. This feature could
explain the common lack of
clear-cut margins during examinations. More frequently, at US,
the adenocarcinoma appears
hypoechoic to the adjacent pancreatic parenchyma [Figure
11].
Figure 11 Ductal adenocarcinoma. Ultrasound oblique scan of the
pancreatic body showshypoechoic mass with ill-defined infiltrative
margins and upstream main pancreaticduct dilation.
The main pancreatic duct is usually infiltrated and upstream
dilated. Doppler studies show
poor or no vascularity inside the lesion. The vascular invasion
is defined by a focal absence of
the echogenic interface of the vessel wall, or by a narrow
lumen, with changes in blood flow
velocity [(33-35)]. Principal criteria of unresectable
pancreatic cancer are liver or peritoneal
metastases and invasion of major peripancreatic vessels
[(36)].
At CEUS, ductal adenocarcinoma enhancement is poor in all
contrast-enhanced phases
[Figure 12].
-
7/31/2019 Ecb Ch04 Pancreas
14/22
Ultrasound of the pancreas 28.07.2010 18:06 14
Figure 12 Ductal adenocarcinoma. Contrast-enhanced ultrasound
transversal scan of thepancreatic head showing a markedly
hypovascularized mass with upstream mainpancreatic duct
dilation.
The margins and size of the lesion are more clearly visible. The
depiction of tumoral margins
at CEUS is more accurate at a low enhancement of pancreatic
adenocarcinoma [(37)], because
in cases of well-differentiated lesions the mass tends to be
isovascular compared to the
remaining parenchyma and the margins of the tumor are no longer
visualized. Relationship
with peripancreatic arterial and venous vessels can also be
evaluated for local staging
[(26;27;37:38)].
The degree of tumoral differentiation of the adenocarcinoma
influences the microvascular
density [(26;27;37:38)]. Moreover, the pattern of enhancement of
pancreatic adenocarcinoma
influences the depiction of tumoral margins at CEUS [(37)].
After studying a pancreatic lesion during the arterial,
pancreatic and venous phases, the
presence of liver metastases have to be excluded during the late
phase [(26)].
Since US often represents the first technique performed, the use
of CEUS will improve the
diagnostic accuracy when a focal hypoechoic solid lesion has
been detected.
Endocrine tumors
Pancreatic endocrine tumors or islet cell tumors arise from the
neuroendocrine cells of the
pancreas. These tumors are classified as functioning or
nonfunctioning, based on the presence
or not of symptoms related to hormone production. Insulinomas
and gastrinomas are the most
common functioning islet cell tumors and they are usually small
at the time of diagnosis. The
other functioning neuroendocrine tumors (vipoma, glucagonoma and
somatostatinoma) are
rare, account for about 20% of functioning neuroendocrine tumors
of the pancreas [(39;40)].
Nonfunctioning tumors are frequently large at diagnosis [Figure
13a] and often malignant
[(41)].
Figure 13 Endocrine tumor (nonfunctioning). a) Ultrasound
transversal scan of the pancreatichead shows large hypoechoic mass
with well-defined margins and upstream mainpancreatic duct
dilation. b) the lesion is hypervascular at
contrast-enhancedultrasound.
a
-
7/31/2019 Ecb Ch04 Pancreas
15/22
Ultrasound of the pancreas 28.07.2010 18:06 15
b
Insulinomas are usually benign and solitary pancreatic lesions,
while gastrinomas tend to be
malignant and multiple.
Insulinomas represent the most frequently found functioning
neuroendocrine tumors of the
pancreas (about 60% of all neuroendocrine tumors), benign
(85%99%) and single (93%
98%) [(42;43)] in the majority of cases. Insulinoma appears as
hypoechoic pancreatic
nodules, usually capsulated.
At the time of clinical presentation 50% of the tumors are
smaller than 1.5 cm [(40)]. When
malignant their diameter is generally >3 cm and about a third
of these have metastases at the
time of diagnosis [(42;43)]. The mean diameter of insulinomas
is
-
7/31/2019 Ecb Ch04 Pancreas
16/22
Ultrasound of the pancreas 28.07.2010 18:06 16
which only the pancreatic side is correctly explorable by US
[(39;40)]. Identification of
pancreatic gastrinomas can be easy considering their moderate
size [(40;45)]. Liver metastatic
lesions are present in 60% of cases at the time of diagnosis
[(40;46)].
Nonfunctioning islet cell tumors represent up to 33% of
neuroendocrine tumors of the
pancreas [(47)], ranging from 1 to 20 cm in diameter and showing
a high malignancy rate, up
to 90% [(47;48)]. However they are less aggressive than
adenocarcinomas. These tumors,characterized by predominantly
expansive growth, are not clinically apparent until adjacent
viscera and structures have become involved. At US they appear
well marginated and usually
easy to detect, thanks to their size. Due to their dimensions,
necrosis and hemorrhage can be
present, developing a typical inhomogeneous appearance,
sometimes accompanied by very
small intralesional calcifications. Larger nonfunctioning islet
cell tumors show cystic
degeneration or cystic changes [(39)]. The finding of numerous
intratumoral vascular spots is
typical of neuroendocrine pancreatic tumors at color-Doppler. In
particular, a spot pattern
can be demonstrated in both large and small endocrine tumors
[(39)]. However, while positive
Doppler results predict hypervascularization of the lesion, a
Doppler silence can also be
present in hypervascular endocrine tumors because of the small
size of the tumoral vascular
network.At CEUS, different enhancement patterns can be observed
in relation to the size of tumors
and tumoral vessels. Voluminous endocrine tumors show a rapid
and intense enhancement in
the early contrast-enhanced phase [Figure 13b], with the
exception of necrotic intralesional
areas [(39;49;50]. In moderate-sized neuroendocrine pancreatic
tumors, a capillary blush
enhancement can be present in the early contrast-enhanced phase,
then becoming hypoechoic
in the late contrast-enhanced phase [(39;49;50].
Nonfunctioning neuroendocrine tumors can also be
hypovascularized, depending on the
amount of stroma inside the lesion which is dense and hyalinized
[(22)].
LymphomaPancreatic lymphoma is represented by the non-Hodgkin
B-cell histotype and usually
associated with lymph nodes or lesions in other organs. US shows
focal or diffuse pancreatic
enlargement, hypoechoic relative to the normal pancreatic
parenchyma. [(36)]
Metastases
Pancreatic metastases are rare. Primary tumors that most
frequently metastasize to the
pancreas are from lung, breast, kidney and the melanoma [(51)].
Pancreatic metastases can
appear as focal or multifocal, often as well demarcated lesions
in patients with a known
primary neoplasm. [(36)].
CEUS may well demonstrate the enhancement of pancreatic
metastases from renal cellcarcinoma, as they are clearly
hypervascular, allowing differential diagnosis against ductal
adenocarcinoma. However, their features cannot be differentiated
from that of endocrine
tumors and the differential diagnosis is therefore based on the
clinical history and symptoms
and finally on cytology [(52;53)].
Pancreatic cystic neoplasm
Serous cystadenoma
Serous cystadenoma (SCA) is a benign lesion. It is usually
located in the head of the pancreas
and generally characterized by tiny cysts of
-
7/31/2019 Ecb Ch04 Pancreas
17/22
Ultrasound of the pancreas 28.07.2010 18:06 17
glycogen-rich serous, transonic at US. If extremely microcystic
SCA can have a solid
appearance at US and CT.
In up to 15% of cases, the tumor contains a central scar, which
may calcify. US imaging can
show the microcystic appearance of this lesion related to the
sponge macroscopic aspect. The
central scar, if present, is often visible as a central solid
echogenic portion of the tumor,
sometimes containing calcifications. The contours of the SCA are
always quite sinuous andthe wall is thin. The internal septa
normally are well orientated and centrally directed,
reaching the central scar with a definitive typical aspect of
the skeleton of this cystic lesion.
Numerous thin septa with a radial arrangement give to the lesion
its typical microcystic
aspect.
SCAs do not communicate with the main pancreatic duct. The
demonstration of that is
fundamental, especially when the lesion is large, because it
might compress the main
pancreatic duct, so upstream dilated [36].
At CEUS, intralesional septa enhancement improves the
identification of the microcystic
features of the lesion. The less common oligocystic or
macrocystic types of serous
cystadenoma present features indistinguishable from those of the
other macrocystic tumors of
the pancreas [(55;56)].
Mucin producing neoplasms
Mucin producing neoplasms of the pancreas may originate either
from the peripheral ducts
(mucinous cystic tumors) or from the main pancreatic duct and
its collateral branches
(intraductal papillary mucinous neoplasms; IPMNs) [(57)].
Mucinous cystoadenoma
Mucinous cystic neoplasm is a potentially malignant lesion. It
is most often located in the
body or tail of the pancreas in middle-aged women. The content
of the cyst is mucin. At US,
it appears as round or ovoid, usually unilocular lesionwith
thick wall and septa andoccasionally peripheral calcifications. The
mucinous content is viscous and may generate fine
echoes in the internal part of the lesion that covers the
internal wall of the cystic tumor and
may hale the inclusion such as internal septa and/or solid
papillary projections. The number
and the thickness of intralesional septa and nodules are not
always related to the grade of
malignancy. Mucinous tumors may spread, involve lymph nodes and
produce liver metastases
[(58;59].
CEUS may significantly improve the ultrasonographic detection of
parietal nodules. The
vascularization of septa and nodules can be demonstrated beaming
hyperechoic [Figure 14],
standing out against the lesional background, anechoic during
the dynamic imaging.
Therefore CEUS examination improves ultrasonographic
differential diagnosis between MCA
and pseudocyst, thanks to the identification and study of
inclusions vascularization in cystic
masses of the pancreas [(60)].
-
7/31/2019 Ecb Ch04 Pancreas
18/22
Ultrasound of the pancreas 28.07.2010 18:06 18
Figure 14 Mucinous cystadenoma. Ultrasound oblique scan of the
pancreatic body showsrounded cystic mass with small enhancing
septa.
Mucinous cystoadenocarcinoma
Mucinous cystoadenocarcinoma represents the malignant neoplastic
transformation of
mucinous cystoadenoma. Compared to the latter it is
characterized by thicker wall and septa,
disomogeneous content and a greater number of nodules [Figure
15], whose significant cell
proliferation is responsible for wall and then peripheral
structures invasion, leading to lymph
nodes involvement and liver metastases development
[(58;59)].
Figure 15 Mucinous cystadenocarcinoma. Ultrasound oblique scan
of the pancreatic bodyshows huge rounded cystic mass with thick
wall and several enhancing septa andnodules.
-
7/31/2019 Ecb Ch04 Pancreas
19/22
Ultrasound of the pancreas 28.07.2010 18:06 19
IPMN
Intraductal papillary mucinous neoplasm (IPMN) is recognized as
a dilation of the main
pancreatic duct and/or its branches or cyst formation with
proliferation of pancreatic ductal
epithelium and excessive production of mucin. IPMNs are
classified into the main duct type,
branch duct type, or a combination of the two [(61)]. The main
duct type can be localized or
diffuse. The localized main duct type of IPMN is characterized
by highly inhomogeneous
masses, related to neoplastic intraductal proliferation, with
upstream dilation of the main
pancreatic duct. The diffuse main type may be difficult to
distinguish from chronic
pancreatitis.
The branch duct mucinous tumor is characterized by cystic
ectasia of one or more branches,
forming masses. At US examination the mucin of IPMN, especially
the ductectatic mucin-
hypersecreting variant of the branch ducts, may not be easily
differentiated from the solid
portions of the tumor, which can therefore be mistakenly
reported as solid. Harmonic
imaging, with its better contrast resolution [(62;63)], may lead
to better identify the non solid
part of the leison, thanks to the demonstration of more or less
sharp intralesional interfaces.
However, at US, final diagnosis of IPMN by demonstrating the
communication with thepancreatic duct is difficult [(64)].
CEUS examination of the IPMNs may allow identification of
intraductal papillary tumoral
vegetations, especially in the papillary-villous variant,
demonstrating its vascularization.
CEUS can be a safe method to follow-up the border-line lesions
evaluating changes in
dimensions and vascularization of the inclusion. Considering
that, in this setting, CEUS has
the great advantage of being a noninvasive and low-cost
technique [(55)].
References
1.
Rumack C, Wilson SR, Charboneau JW. Diagnostic ultrasound. New
York: Mosby YearBook 1991; 145177.
2. Mittelstaedt CA. Abdominal ultrasound. New York: Mosby 1987;
163176.3. Weissleder R, Rieumont MJ, Wittenberg J Primer of
diagnostic imaging. 2nd ed. New
York: Mosby Year Book 1997; 220228.
4. Lorn I, Lasson A, Fork T, et al. New sonographic imaging
observations in focalpancreatitis. Eur Radiol 1999; 9:862867.
5. DOnofrio M, Zamboni G, Tognolini A, Malag R, Faccioli N,
Frulloni L, Pozzi MucelliR. Mass-forming pancreatitis: value of
CEUS. World J Gastroenterol 2006; 12:4181
4184.
6. Numata K, Ozawa Y, Kobayashi N, Kubota T, Akinori N, Nakatani
Y, Sugimori K,Imada T, Tanaka K. Contrast-enhanced sonography of
autoimmune pancreatitis:comparison with pathologic findings. J
Ultrasound Med 2004; 23:199206.
7. Freeny P, Lawson T. Radiology of the pancreas. New York:
Springer-Verlag 1982, 449.8. Bolondi L. Sonography of chronic
pancreatitis. Radiol Clin North Am 1989; 27:815833.9. Alpern MB,
Sandler MA, Kellman GM, Madrazo BL. Chronic pancreatitis:
ultrasonic
features. Radiology 1985; 155:215219.
10.Bolondi L, Priori P, Gullo L, et al. Relationship between
morphological changes detectedby ultrasonography and pancreatic
esocrine function in chronic pancreatitis. Pancreas
1987; 2:222229.
11.Lankisch PG, Banks PA Chronic pancreatitis: etiology. In:
Lankisch PG, Banks PA (eds)Pancreatitis. New York: Springer Verlag
1998; 199208.
-
7/31/2019 Ecb Ch04 Pancreas
20/22
Ultrasound of the pancreas 28.07.2010 18:06 20
12.Lecesne R, Laurent F, Drouillard J, et al. Chronic
pancreatitis. In: Baert AL, Delorme G,Hoe LVan (eds) Radiology of
the pancreas. 2nd rev ed. New York: Springer Verlag 1999;
145180.
13.Husband JE, Meire HB, Kreel L. Comparison of ultrasound and
computer tomography inpancreatic diagnosis. Br J Radiol 1977;
50:855863.
14.Remer EM, Baker MB. Imaging of chronic pancreatitis. Radiol
Clin N Am 2002;40:12291242.15.Lees WR, Vallon AD, Denyer ME, et al.
Prospective study of ultrasonography in chronic
pancreatic disease. BMJ 1979; 1:162164.
16.Foley WD, Stewart ET, Lawson TL, et al. Computer tomography,
ultrasonography andechoscopic retrograde cholangiopancreatography
in the diagnosis of pancreatic disease: a
comparative study. Gastrointestinal Radiol 1980; 5:2935.
17.Grant TH, Efrusy ME. Ultrasound in the evaluation of chronic
pancreatitis. JAMA 1981;81:183188.
18.Homma T, Harada H, Koizumi M. Diagnostic criteria for chronic
pancreatitis by the JapanPancreas Society. Pancreas 1997;
15:1415.
19.Niederau C, Grendell JH. Diagnosis of chronic pancreatitis.
Gastroenterology 1985;88:19731995.
20.Hessel ST, Siegelman SS, McNeil BJ, et al. A prospective
evaluation of computertomography and ultrasound of the pancreas.
Radiology 1982; 143:129133.
21.Furukawa N, Muranaka T, Yasumori K, et al. Autoimmune
pancreatitis: radiologicfindings in three histologically proven
cases. J Comput Assist Tomogr 1998; 22:880883.
22.Faccioli N, Crippa S, Bassi C, D'Onofrio M. Contrast-enhanced
ultrasonography of thepancreas. Pancreatology. 2009;
9(5):560-6.
23.Okazaki K. Autoimmune-related pancreatitis. Curr Treat
Options Gastroenterol 2001;4:369375.
24.Kamisawa T, Yoshiike M, Egawa N, Nakajima H, Tsuruta K,
Okamoto A. Treatingpatients with autoimmune pancreatitis: results
from a long-term follow-up study.
Pancreatology 2005; 5:234240.
25.Kim T, Murakami T, Takamura M, Hori M, Takahashi S, Nakamori
S, Sakon M, Tanji Y,Wakasa K, Nakamura H. Pancreatic mass due to
chronic pancreatitis: correlation of CT
and MR imaging features with pathologic findings. AJR Am J
Roentgenol 2001; 177:367-
371.
26.D'Onofrio M, Zamboni G, Faccioli N, Capelli P, Pozzi Mucelli
R. Ultrasonography of thepancreas. 4. Contrastenhanced imaging.
Abdom Imaging 2007; 32:171-181.
27.Takeda K, Goto H, Hirooka Y, Itoh A, Hashimoto S, Niwa K,
Hayakawa T. Contrast-enhanced transabdominal ultrasonography in the
diagnosis of pancreatic mass lesions.Acta Radiol 2003;
44:103-106.
28.Procacci C, Biasiutti C, Carbognin G, Capelli P, El-Dalati G,
Falconi M, Misiani G,Ghirardi C, Zamboni G. Pancreatic neoplasms
and tumor-like conditions. Eur Radiol
2001; 11Suppl2:S167-S192
29.Cubilla Al, Fitzgerald PJ. Tumors of the esocrine pancreas.
2nd Series. Ed. Washington,DC: Armed Forces Institute of Pathology
1984.
30.O Connor TP, Wade TP, Sunwoo YC, et al. Small cell
undifferentiated carcinoma of thepancreas. Report of a patient with
tumor marker studies. Cancer 1992; 70:1514-1519
31.Tryka AF, Brooks JR. Histopathology in the evaluation of
total pancreatectomy for ductalcarcinoma. Ann Surg 1979;
190:373-381.
32.Yeo CJ, Cameron JL, Lillemoe KD, et al.
Pancreaticoduodenoctomy for cancer of thehead of the pancreas. 201
patients. Ann Surg 1995; 221:721-733.
http://www.ncbi.nlm.nih.gov/pubmed?term=%22Faccioli%20N%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Crippa%20S%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Bassi%20C%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22D%27Onofrio%20M%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22D%27Onofrio%20M%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Bassi%20C%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Crippa%20S%22%5BAuthor%5Dhttp://www.ncbi.nlm.nih.gov/pubmed?term=%22Faccioli%20N%22%5BAuthor%5D
-
7/31/2019 Ecb Ch04 Pancreas
21/22
Ultrasound of the pancreas 28.07.2010 18:06 21
33.Bertolotto M, D'Onofrio M, Martone E, Malag R, Pozzi Mucelli
R. Ultrasonography ofthe pancreas. 3. Doppler imaging. Abdom
Imaging 2007; 32:161-170.
34.Koito K, Namieno T, Nagakawa T, Hirokawa N, Ichimura T,
Syonai T, Yama N, SomeyaM, Nakata K, Sakata K, Hareyama M.
Pancreas: imaging diagnosis with color/power
Doppler ultrasonography, endoscopic ultrasonography, and
intraductal ultrasonography.
Eur J Radiol 2001; 38:94-104.35.Ueno N, Tomiyama T, Tano S, Wada
S, Miyata T. Color Doppler ultrasonography in the
diagnosis of portal vein invasion in patients with pancreatic
cancer. J Ultrasound Med
1997; 16:825-830
36.A. Martnez-Noguera, M. DOnofrio Ultrasonography of the
pancreas. 1. Conventionalimaging Abdom Imaging 2007;
32(2):136-149.
37.Faccioli N, DOnofrio M, Malag R, Zamboni G, Falconi M,
Capelli P, Mucelli RP.Resectable pancreatic adenocarcinoma:
depiction of tumoral margins at CEUS. Pancreas
2008; 37:265268.
38.Oshikawa O, Tanaka S, Ioka T, Nakaizumi A, Hamada Y, Mitani
T. Dynamic sonographyof pancreatic tumors: comparison with dynamic
CT. AJR Am J Roentgenol 2002;
178:11331137.39.DOnofrio M, Mansueto GC, Falconi M, Procacci C.
Neuroendocrine pancreatic tumor:
value of contrast enhanced ultrasonography. Abdom Imaging 2004;
29:246258.
40.Ros PR, Mortele KJ. Imaging features of pancreatic neoplasms.
JBR-BTR 2001;84(6):239249.
41.Buetow PC, Miller DL, Parrino TV. Islet cell tumors of the
pancreas: clinical, radiologic,and pathologic correlation in
diagnosis and localization. Radiographics 1997; 17:453
472.
42.Liu TH, Tseng HC, Zhu Y. Insulinoma. An immunohistochemical
and morphologicanalysis of 95 cases. Cancer 1985; 56:14201429.
43.Stefanini P, Carbonni M, Patrassi N. Beta islet-cell tumors
of the pancreas: result of astudy on 1067 cases. Surgery 1974;
75:597.
44.Pereira PL, Wiskirchen J. Morphological and functional
investigations of neuroendocrinetumors of the pancreas. Eur Radiol
2003; 13(9):21332146.
45.Semelka RC, Cumming MJ, Shoenut JP, Magro, et al. Islet cell
tumors: comparison ofdynamic contrast-enhanced CT and MR imaging
with dynamic gadolinium enhancement
and fat suppression. Radiology 1993; 186(3):799802.
46.Mergo PJ, Helmberger TK, Buetow PC, et al. Pancreatic
neoplasm: MR imaging andpathologic correlation. Radiographics 1997;
17:281301.
47.Fugazzola C, Procacci C, Bergamo Andreis IA, Iacono C, et al.
The contribution ofultrasonography and computed tomography in the
diagnosis of nonfunctioning islet cell
tumors of the pancreas. Gastrointest Radiol 1990;
15(2):139144.48.Eckhauser FE, Cheung PS, Vinik AI, et al.
Nonfunctioning malignant neuroendocrinetumors of the pancreas.
Surgery 1986; 100:978988.
49.Malag R, DOnofrio M, Zamboni GA, Faccioli N, Falconi M,
Boninsegna L, MucelliRP. Contrast-enhanced sonography of
nonfunctioning pancreatic neuroendocrine tumors.
AJR Am J Roentgenol 2009; 192:424430.
50.DOnofrio M, Malag R, Zamboni G, Vasori S, Falconi M, Capelli
P, Mansueto G. CEUSbetter identifies pancreatic tumor
vascularization than helical CT. Pancreatology 2005;
5:398402.
51.Merkle EM, Braz T, Kolkythas O, et al. Metastases to the
pancreas. Br J Radiol 1998;71:12081214.
-
7/31/2019 Ecb Ch04 Pancreas
22/22
Ultrasound of the pancreas 28.07.2010 18:06 22
52.Flath B, Rickes S, Schweigert M, Lochs H, Possinger K, Wermke
W. Differentiation of apancreatic metastasis of a renal cell
carcinoma from a primary pancreatic carcinoma by
echo-enhanced power Doppler sonography. Pancreatology 2003;
3:349-351.
53.Megibow AJ. Secondary pancreatic tumors: imaging. In:Procacci
C, Megibow A, editors.Imaging of the pancreas: cystic and rare
tumors. Berlin: Springer-Verlag 2003; 277-288.
54.Procacci C. Pancreatic neoplasms and tumor-like conditions.
Eur Radiol 2001;11Suppl2:S167S192.55.DOnofrio M, Megibow AJ,
Faccioli N, Malag R, Capelli P, Falconi M, Mucelli
RP:.Comparison of contrast-enhanced sonography and MRI in
displaying anatomic
features of cystic pancreatic masses. AJR Am J Roentgenol 2007;
189:14351442.
56.DOnofrio M, Caffarri S, Zamboni G, Falconi M, Mansueto G.
CEUS in thecharacterization of pancreatic mucinous cystadenoma. J
Ultrasound Med 2004; 23: 1125
1129.
57.Procacci C, Graziani R, Bicego E, et al. Intraductal
mucinproducing tumors of thepancreas: imaging findings. Radiology
1996; 198:249257.
58.Tham RT, Heyerman HG, Falke TH, et al. Cystic fibrosis: MR
imaging of the pancreas.Radiology 1991; 179:183186.
59.Ros PR, Hamrick-Turner JE, Chiechi MV, et al. Cystic masses
of the pancreas.Radiographics 1992; 12:673686.
60.DOnofrio M, Zamboni G, Malago` R, Martone E, Falconi M,
Capelli P, Mansueto G.Pancreatic pathology. In: Quaia E (ed)
Contrast media in ultrasonography. Springer-
Verlag: Berlin 2005; 335347.
61.Procacci C, Megibow AJ, Carbognin G, et al. Intraductal
papillary mucinous tumor of thepancreas: a pictorial essay.
Radiographics 1999; 19:14471463.
62.Shapiro RS, Wagreich J, Parsons RB, et al. Tissue harmonic
imaging sonography:evaluation of image quality compared with
conventional sonography. AJR 1998;
171:1203-1206.
63. Bennett GL, Hann LE. Pancreatic ultrasonography. Surg Clin
North Am 2001; 81:259281.
64.Procacci C, Schenal G, Dalla Chiara E, et al. Intraductal
papillary mucinous tumors:imaging. In: Procacci C, Megibow AJ (eds)
Imaging of the pancreas cystic and rare
tumors. Berlin: Springer Verlag 2003; 97137.