Embed Size (px)
DESCRIPTION
Ebola Virus Disease. Dr. Oluwafemi Akinyele Popoola Lecturer and Consultant Community Physician. Session Objectives. Describe the epidemiology of Ebola virus Highlight past outbreaks State main symptoms - PowerPoint PPT Presentation
Citation preview

Ebola Virus Disease
Dr. Oluwafemi Akinyele PopoolaLecturer and Consultant
Community Physician
Lecture delivered at Bodija-Ashi Baptist Church14thSeptember, 2014.

Session Objectives
• Describe the epidemiology of Ebola virus• Highlight past outbreaks• State main symptoms• Describe how knowledge of the epidemiology
and transmission dynamics of Ebola Virus informs its control strategies

What is Ebola Virus Disease
• Ebola Virus Disease: is one of the numerous viral Hemorrhagic Fevers. It is a severe, often fatal disease in humans and nonhuman primates – CDC
• Incubation period 2-21days (usual 8 – 10 days) • Causation: infection with a virus
– Family Filoviridae and genus Ebolavirus– Five subspecies of Ebolavirus
• Zaire ebolavirus; Sudan ebolavirus; Tai Forest ebolavirus; and Bundibugyo ebolavirus
• Reston ebolavirus (disease only in nonhuman primates)
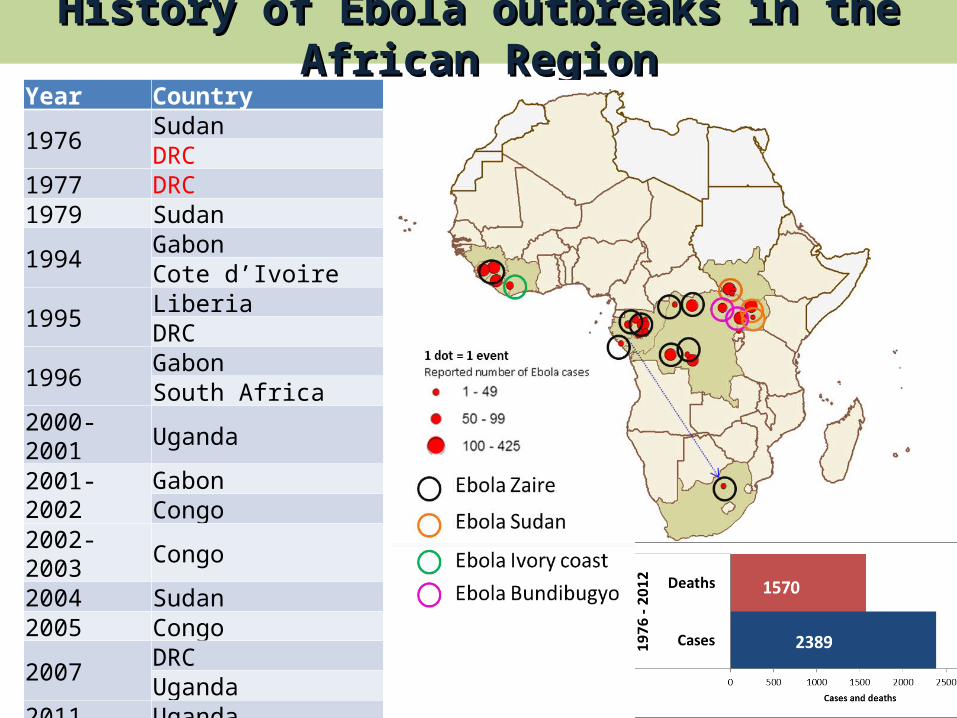
Year Country
1976SudanDRC
1977 DRC1979 Sudan
1994GabonCote d’Ivoire
1995LiberiaDRC
1996GabonSouth Africa
2000-2001 Uganda
2001-2002GabonCongo
2002-2003 Congo2004 Sudan2005 Congo
2007DRCUganda
2011 Uganda2012 Uganda
DRC
History of Ebola outbreaks in the African RegionHistory of Ebola outbreaks in the African Region

Ebola outbreak in Guinea, Liberia and Sierra Leone, Epicurve by week of onset, December 2013 to 19 July 2014 (n=1002)
Alert from Méliandou26 January
5 death w diarrhoea
Alert 13 March 15 cases inc. 9 deaths
21 MarchLabortory
Confirmation
Out
brea
k re
spon
se o
pera
tions
st
arte
d
26 May Sierra Leone
declared outbreak
31 March Liberia declared
outbreak
23 March WHO deployed multi-
diciplinary international experts
23 March Mobile laboratory deployed through
EDPLN
Case Definitions
Suspected (clinical) case: Any person ill or deceased with fever and hemorrhage. Documented prior contact with an EVD case is not required
•Confirmed CaseA case with laboratory confirmed diagnostic evidence of ebola virus infection.
Any person (living or dead) with contact with a clinical case of EVD and a history of acute fever. OR Any person (living or dead) with a history of acute fever and three or more of the following - headache/ vomiting/nausea/ loss of appetite/ diarrhea/ intense fatigue/ abdominal pain/ general muscular or articular pain/ difficulty in swallowing/ difficulty in breathing/ hiccoughs
OR Any unexplained death. Distinction between a suspected case and a probable case in practice relatively unimportant as far as outbreak control is concerned.
Probable case (with or without bleeding):
Definition of contactDefinition of contact
• A person without any symptoms has had physical contact with a case or the body fluids of a case within the last three weeks. The notion of physical contact may be proven or highly suspected such as having shared the same room/bed, cared for a patient, touched body fluids, or closely participated in a burial ceremony (physical contact with the corpse).
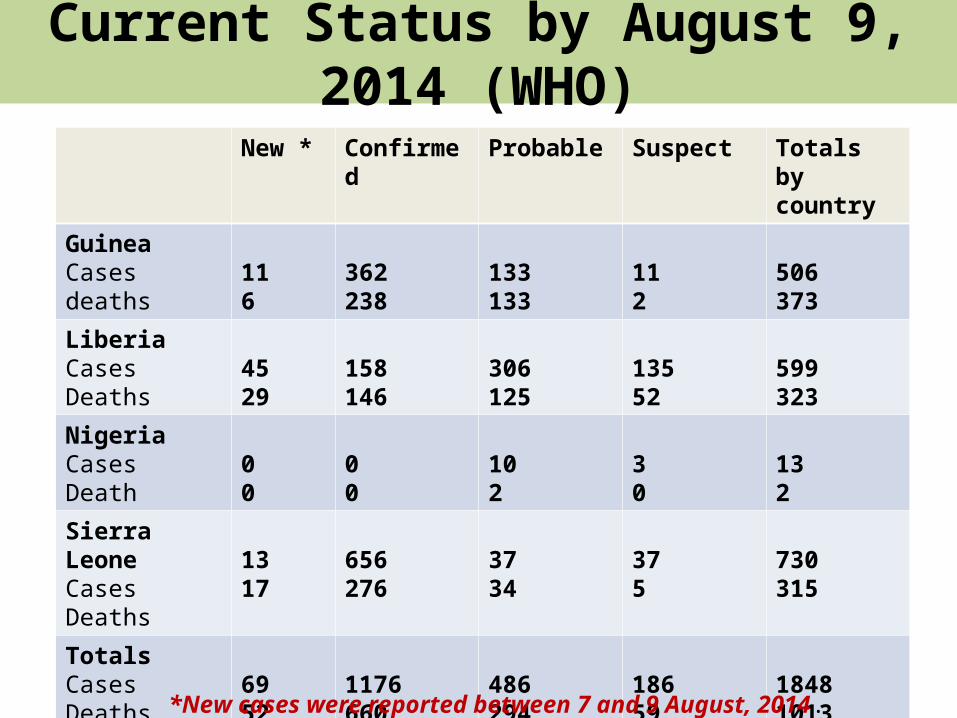
Current Status by August 9, 2014 (WHO)
New * Confirmed Probable Suspect Totals by country
GuineaCasesdeaths
116
362238
133133
112
506373
LiberiaCasesDeaths
4529
158146
306125
13552
599323
NigeriaCasesDeath
00
00
102
30
132
Sierra LeoneCasesDeaths
1317
656276
3734
375
730315
TotalsCasesDeaths
6952
1176660
486294
18659
18481013
*New cases were reported between 7 and 9 August, 2014.

Transmission Cycles• Animal to Man
• Initial source of outbreak in human populations• Often occurs in rural areas
• Man to Man• Source of epidemic propagation in human populations• All body fluids are infected• Infected humans only transmit the virus AFTER THEY
BECOME SICK!!!• Risk is increased during hospital care of infected
individuals • Improper disposal of dead bodies also transmits
disease

Routes of Transmission• Direct contact
• Blood or secretions of infected person• Infected needles and other equipments contaminated
with infected secretions• Others
• Through families and friends contact with infectious secretions of ill person
• Virus can still be present in semen 6 weeks after illness• Factors aiding transmission
• Hospital settings: inappropriate use of PPE; Lack of point of care risk assessment
• Community settings: burial rites; treatment seeking delays/denials

Transmission dynamics
• Natural reservoir not conclusive – However, WHO believes fruit bats may be the natural host
• First patient in outbreaks most likely infected by animal
• Health workers more susceptible to infection• Higher risk of transmission (high viral loads)
– Later stages : vomiting, diarrhoea, shock, haemorrhage

Hypothesis of Ebola Virus transmission at the human-animal interface

Symptoms of Ebola Virus Disease
MAIN
•Fever – at least 38C•Weakness•Diarrhoea•Vomiting•Headache•Joint and muscle aches•Stomach pain•Lack of appetite
ADDITIONAL•A Rash•Red Eyes•Hiccups•Cough •Sore throat•Chest pain•Difficulty breathing•Difficulty swallowing •Bleeding inside and outside of the body
Definitive Diagnosis• LABORATORY BASED
– Antibody-capture enzyme-linked immunosorbent assay (ELISA)
– Antigen detection tests – Serum neutralization test – Reverse transcriptase polymerase chain reaction
(RT-PCR) assay – Electron microscopy – Virus isolation by cell culture

HOW DO WE PREVENT EBOLA DISEASE INFECTIONS

Facts about the Virus?• Easily destroyed – soaps, detergent, chlorine,
heat.• Highly infectious• Highly pathogenic – causes a serious disease
with high risk of death• Humans only become infectious when sick• Virus shed in ALL body fluids• No evidence of air borne transmission• No licensed vaccine or specific treatment• Can only be diagnosed via specialised lab tests

Prevention Strategies
• Prevention of Community infections/HE–Prevention of new infections–Early recognition of infected individuals–Tracing and surveillance of contacts of
infected individuals• Prevention of hospital infections
–Isolation of infected individuals–Supportive treatment of infected
individuals
Community Prevention during Outbreaks
• Reducing the risk of wildlife-to-human transmission from contact with infected fruit bats or monkeys/apes/other bush meats and the consumption of their raw meat.
• Animals should be handled with gloves and other appropriate protective clothing.
• Animal products (blood and meat) should be thoroughly cooked before consumption.

Community Prevention during Outbreaks
• Close physical contact with Ebola patients should be avoided.
• Gloves and appropriate personal protective equipment should be worn when taking care of ill patients at home.
• Regular hand washing is required after visiting patients in hospital, as well as after taking care of patients at home
Community Prevention during Outbreaks
• Communities affected by Ebola should inform the population about the nature of the disease and about outbreak containment measures, including burial of the dead.
• People who have died from Ebola should be promptly and safely buried
• Manage rumours during outbreak• Do not hide cases or contacts

Control in Hospital Settings• Ebola is highly infectious and must be treated
in specialised isolation centres• Standard precautions for all patients• Infection based precautions for probable or
confirmed cases• Proper decontamination of all surfaces
Summary
• Ebola causes a serious disease with high risk of death
• Cases present with fever and other symptoms diagnosis requires specialised lab tests
• Prevention strategies– Practice good personal hygiene, frequent hand
washing with soap and water– Avoid close contact with possibly infected
individuals– Proper investigation and isolation of all cases– Tracing and surveillance of contacts of Ebola
patients

Thank you for your attention


















![Ebola virus disease [ bio project ]](https://img.pdfslide.us/doc/110x75/557d5e21d8b42ae1438b4dc3/ebola-virus-disease-bio-project-.jpg)







