Embed Size (px)
Citation preview
EBM 2015
Infection and sepsisMasterclassIC Schiermonnikoog 2015
Contents• Critical care for Ebola infection
• Current problems with invasive aspergillosis
• Should patients with PJP be isolated?
• Polymixin B hemoperfusion for severe sepsis
• Early antibiotics but for whom?
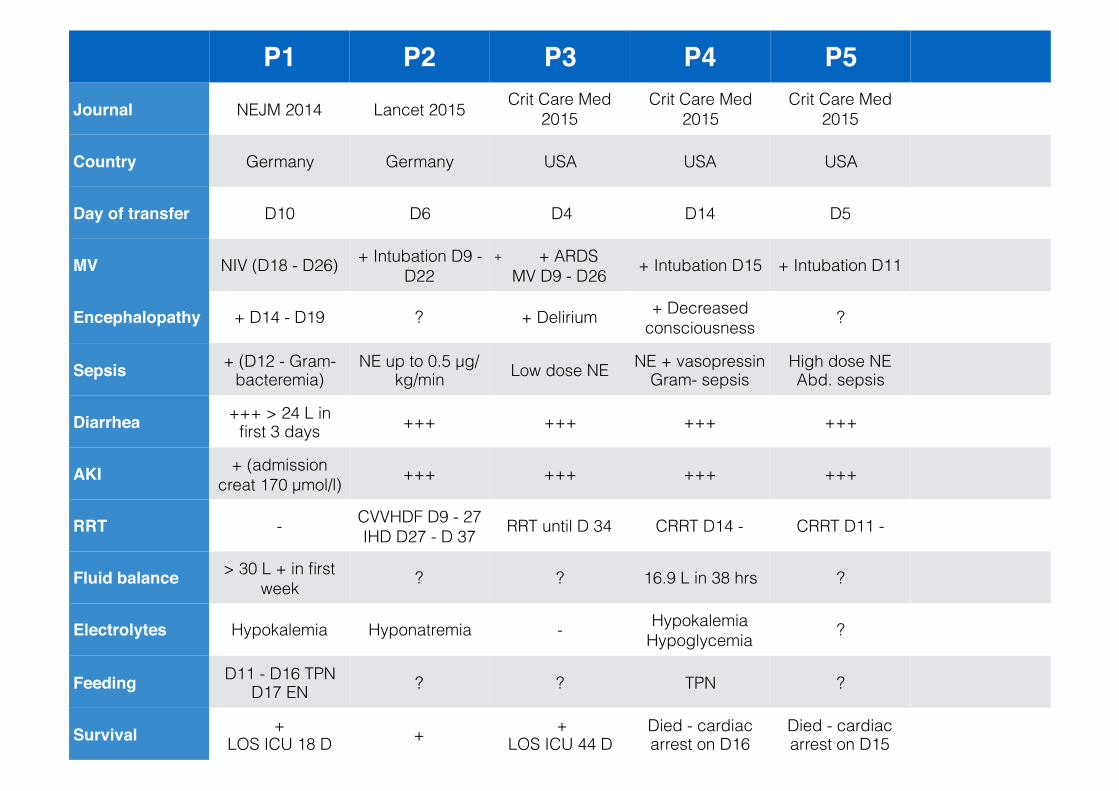
P1 P2 P3 P4 P5
Journal NEJM 2014 Lancet 2015 Crit Care Med 2015
Crit Care Med 2015
Crit Care Med 2015
Country Germany Germany USA USA USA
Day of transfer D10 D6 D4 D14 D5
MV NIV (D18 - D26) + Intubation D9 - D22
+ + ARDS MV D9 - D26 + Intubation D15 + Intubation D11
Encephalopathy + D14 - D19 ? + Delirium + Decreased consciousness ?
Sepsis + (D12 - Gram- bacteremia)
NE up to 0.5 μg/kg/min Low dose NE NE + vasopressin
Gram- sepsisHigh dose NE Abd. sepsis
Diarrhea +++ > 24 L in first 3 days +++ +++ +++ +++
AKI + (admission creat 170 μmol/l) +++ +++ +++ +++
RRT - CVVHDF D9 - 27 IHD D27 - D 37 RRT until D 34 CRRT D14 - CRRT D11 -
Fluid balance > 30 L + in first week ? ? 16.9 L in 38 hrs ?
Electrolytes Hypokalemia Hyponatremia - Hypokalemia Hypoglycemia ?
Feeding D11 - D16 TPN D17 EN ? ? TPN ?
Survival + LOS ICU 18 D + +
LOS ICU 44 DDied - cardiac arrest on D16
Died - cardiac arrest on D15
Overall…..• 25 patients with EVD in resources-rich settings
• Mortality 20 - 26%

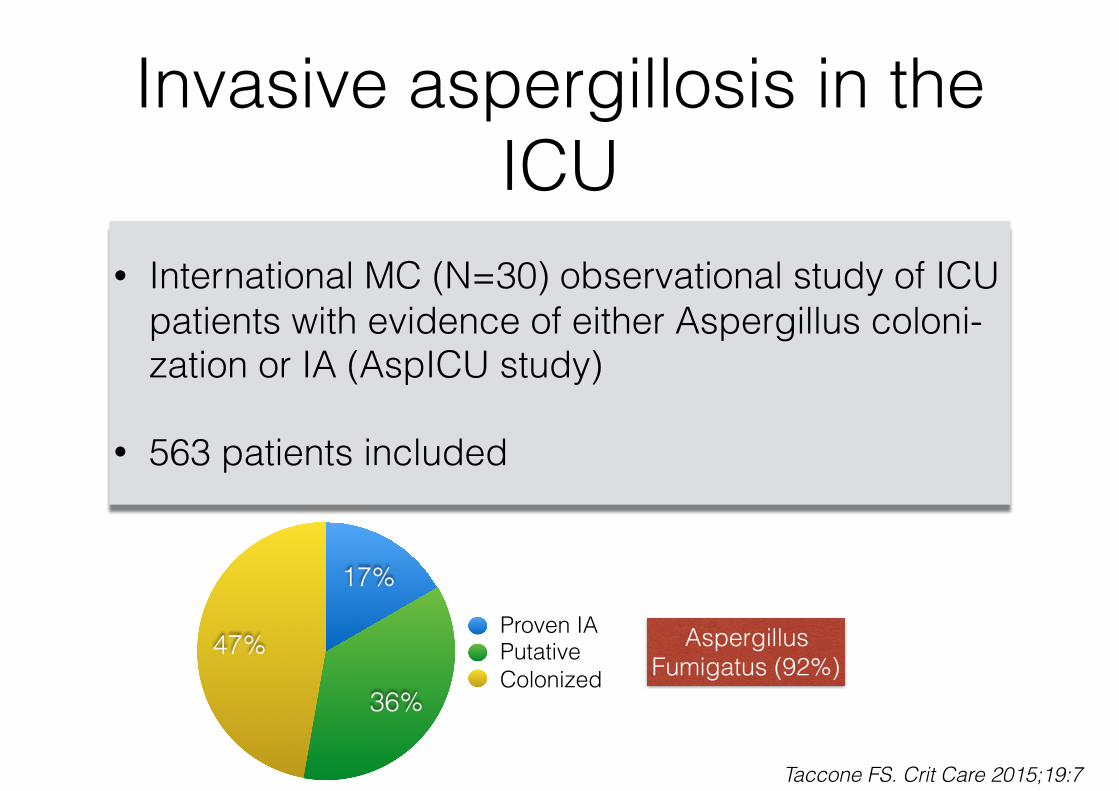
Invasive aspergillosis in the ICU
• International MC (N=30) observational study of ICU patients with evidence of either Aspergillus coloni- zation or IA (AspICU study)
• 563 patients included
47%
36%
17%Proven IAPutativeColonized
Aspergillus Fumigatus (92%)
Taccone FS. Crit Care 2015;19:7
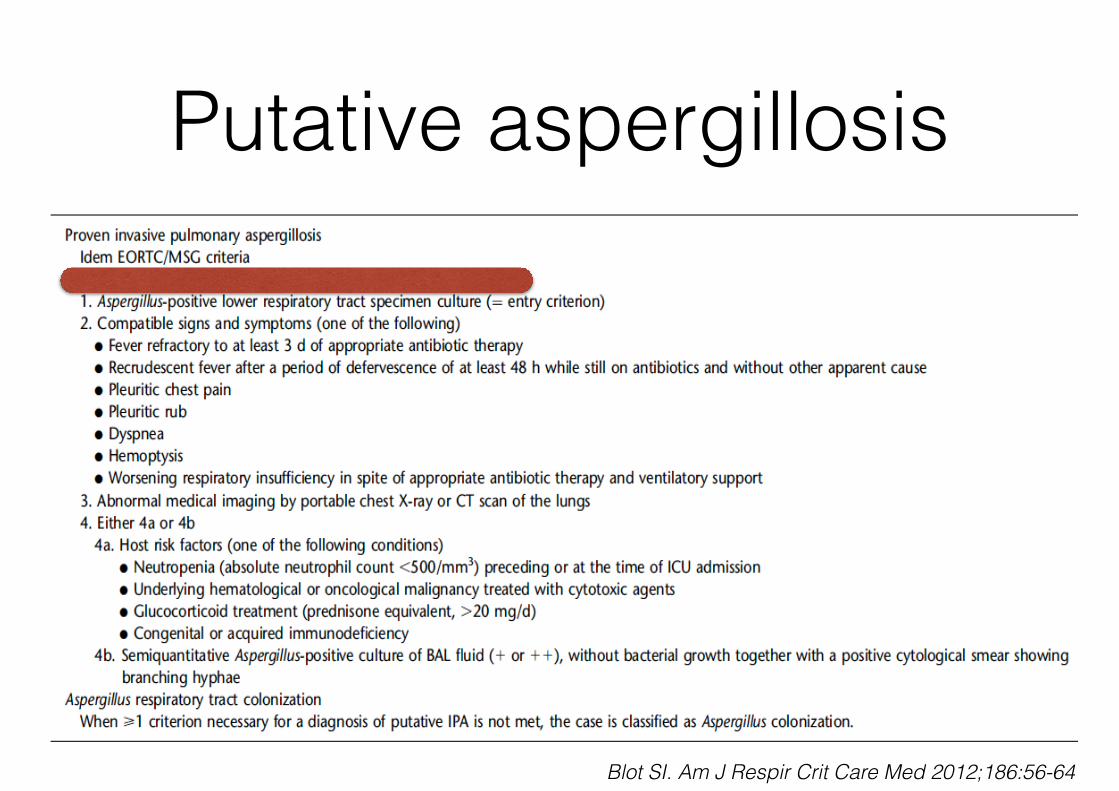
Putative aspergillosis
Blot SI. Am J Respir Crit Care Med 2012;186:56-64
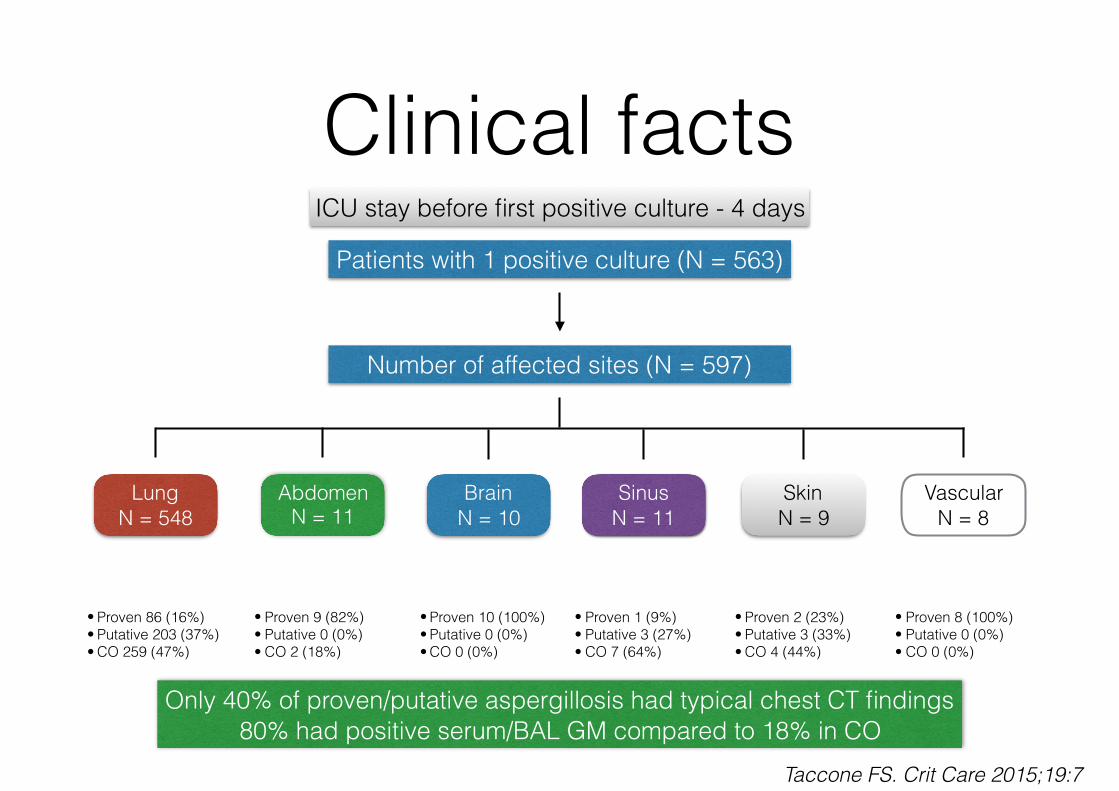
Clinical factsICU stay before first positive culture - 4 days
Patients with 1 positive culture (N = 563)
Number of affected sites (N = 597)
Lung N = 548
Abdomen N = 11
Brain N = 10
Sinus N = 11
Skin N = 9
Vascular N = 8
• Proven 86 (16%) • Putative 203 (37%) • CO 259 (47%)
• Proven 9 (82%) • Putative 0 (0%) • CO 2 (18%)
• Proven 10 (100%) • Putative 0 (0%) • CO 0 (0%)
• Proven 1 (9%) • Putative 3 (27%) • CO 7 (64%)
• Proven 2 (23%) • Putative 3 (33%) • CO 4 (44%)
• Proven 8 (100%) • Putative 0 (0%) • CO 0 (0%)
Taccone FS. Crit Care 2015;19:7
Only 40% of proven/putative aspergillosis had typical chest CT findings 80% had positive serum/BAL GM compared to 18% in CO

Clinical facts70% of patients with proven / putative aspergillosis were in immunosuppressive
state (EORTC) Treatment no effect on survival
%
0
20
40
60
80
Mortality at 12 weeks
Proven Putative CO
38
67
79
%
0
20
40
60
80
Mortality for proven/putative IA
6673
Imuunosuppressed "Normal"NS
Taccone FS. Crit Care 2015;19:7

Azole resistanceSurveillance Collaboration on Aspergillus Resistance in Europe
Azole resistance 3.2%(0 - 26.1%)
Mainly TR34/L98H or TR46/Y121F/T289A resistancemechanism acquired from environment
Case fatality with azole resistance 70% van der Linden JWM. Emerg Infec Dis 2015;21:1041-1044
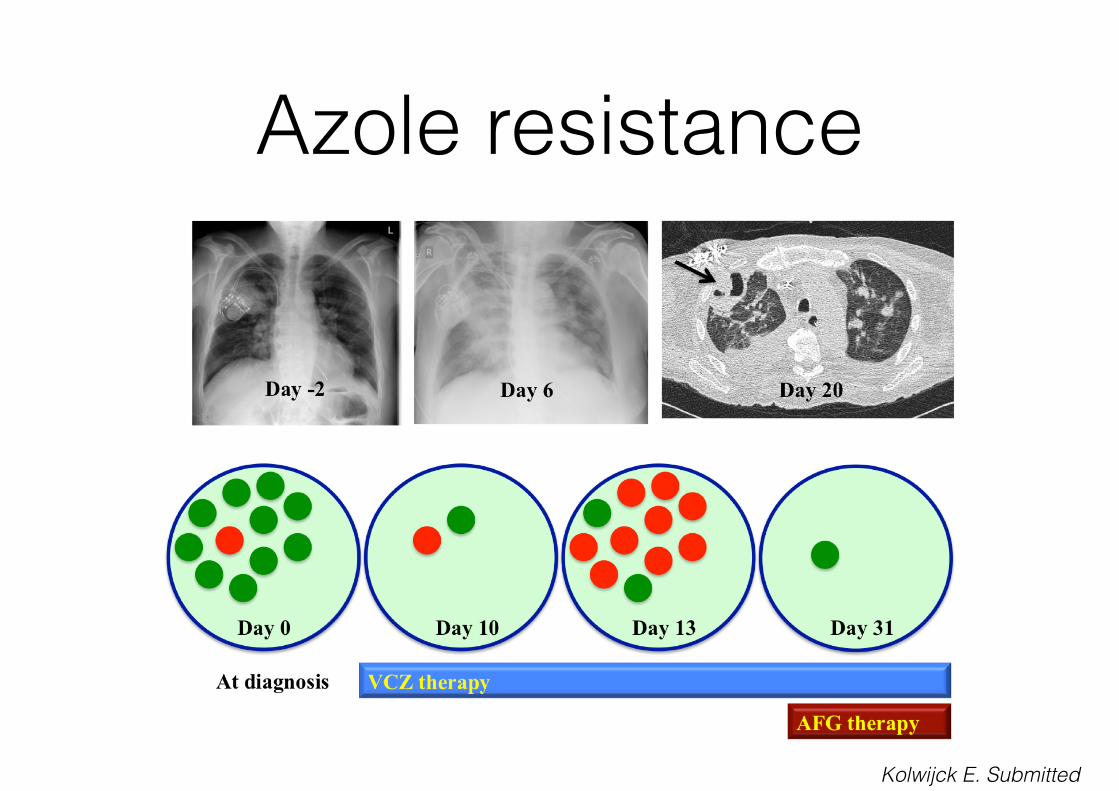
Azole resistance
Kolwijck E. Submitted

Voriconazol vs voriconazol + anidulafungin with HM or HCT
N = 454, suspected or documented IA
%
0
10
20
30
6 W mortality total group 12 W mortality total group 6 W mortality proven IA
15,7
29,3
19,3
27,339,4
27,5
P = 0.087 P = 0.037P = 0.077
Marr KA. Ann Intern Med 2015;162:81-89

Voriconazol dosing and hypoalbuminemia
• Intra- and interpatient concentration variation
• CYP450-mediated drug-drug interactions
• Genetic polymorphism CYP2C19 enzyme
• Age
• Liver disease
• Coadministration drug with food
• Enteral feeding
• Switch from iv to oral medication

Protein binding
Hypoalbuminemia
More rapid elimination
(Only relevant for PPB > 70%)
Voriconazole PPB only 50% but saturated metabolism and only 2 % excreted unchanged in urine
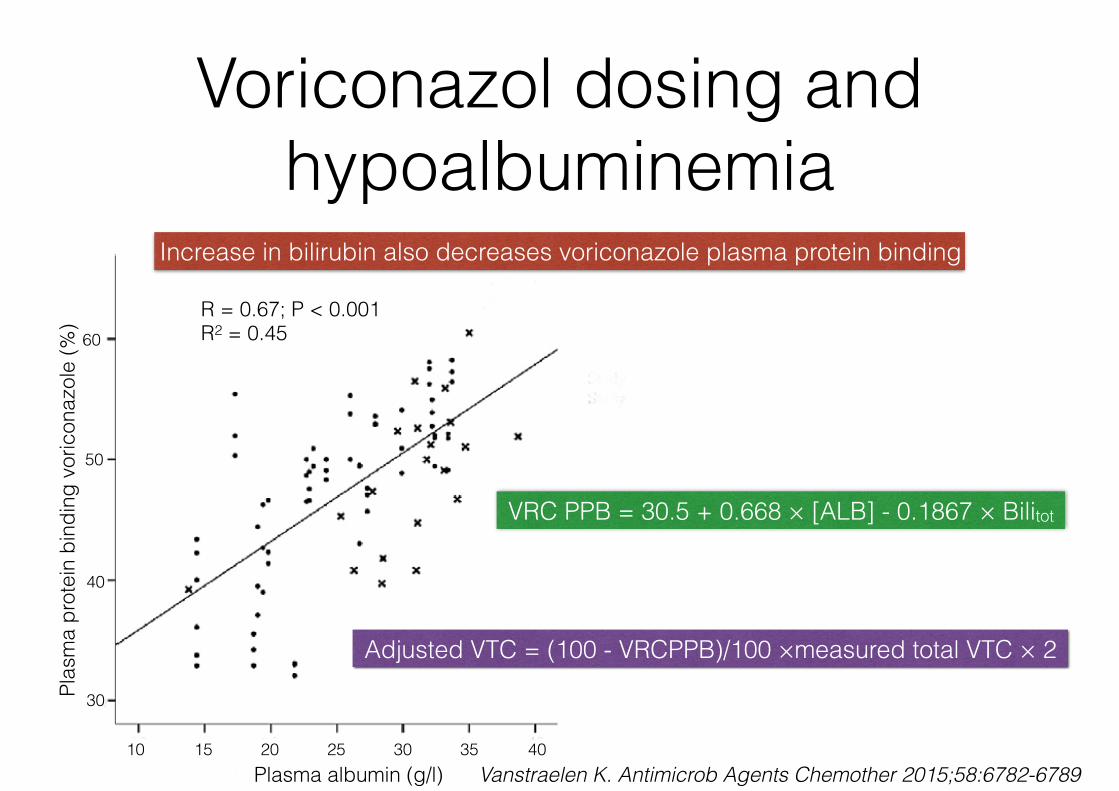
Voriconazol dosing and hypoalbuminemia
Plas
ma
prot
ein
bind
ing
voric
onaz
ole
(%)
Plasma albumin (g/l)10 15 20 25 30 35 40
30
40
50
60R = 0.67; P < 0.001 R2 = 0.45
Increase in bilirubin also decreases voriconazole plasma protein binding
VRC PPB = 30.5 + 0.668 × [ALB] - 0.1867 × Bilitot
Adjusted VTC = (100 - VRCPPB)/100 ×measured total VTC × 2
Vanstraelen K. Antimicrob Agents Chemother 2015;58:6782-6789

Vanstraelen K. Antimicrob Agents Chemother 2015;58:6782-6789
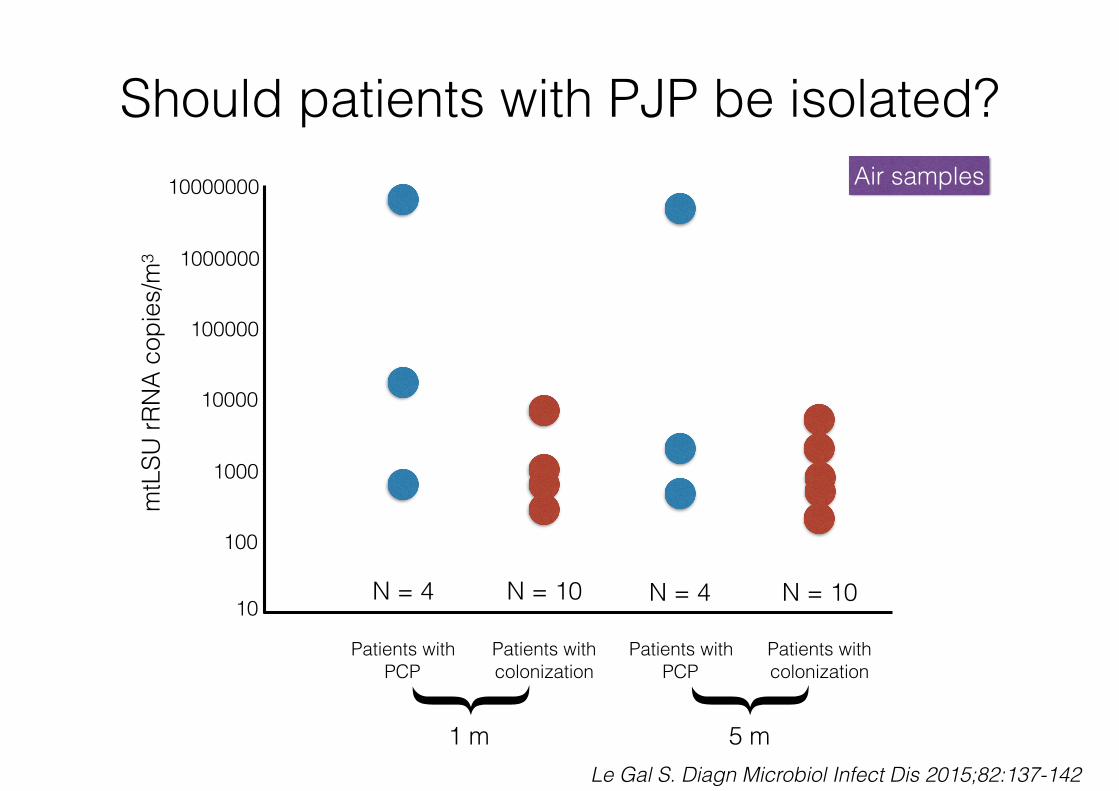
Should patients with PJP be isolated?
10
100
1000
10000
100000
1000000
10000000m
tLSU
rRN
A co
pies
/m3
Patients with PCP
Patients with colonization
Patients with PCP
Patients with colonization{ {
1 m 5 m
N = 4 N = 10 N = 4 N = 10
Air samples
Le Gal S. Diagn Microbiol Infect Dis 2015;82:137-142
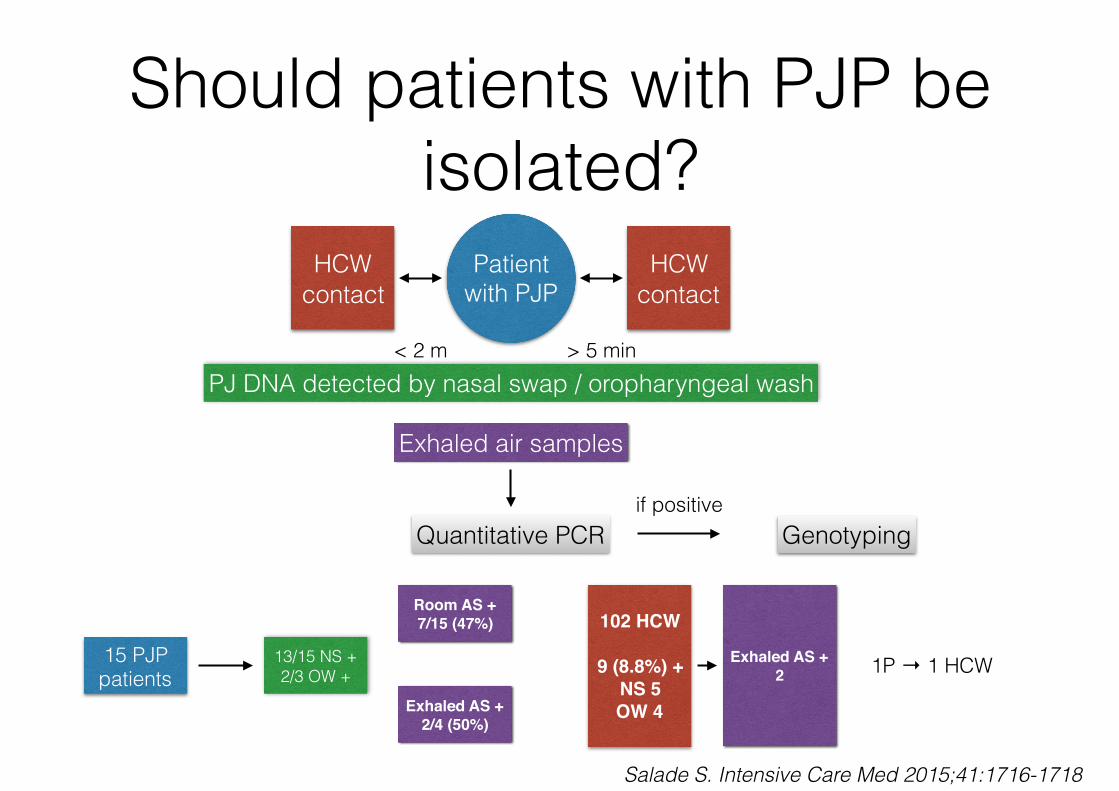
Should patients with PJP be isolated?
Patient with PJP
HCW contact
HCW contact
< 2 m > 5 minPJ DNA detected by nasal swap / oropharyngeal wash
Exhaled air samples
Quantitative PCRif positive
Genotyping
15 PJP patients
13/15 NS + 2/3 OW +
Room AS +7/15 (47%)
Exhaled AS +2/4 (50%)
102 HCW
9 (8.8%) +NS 5OW 4
Exhaled AS +2 1P → 1 HCW
Salade S. Intensive Care Med 2015;41:1716-1718

Polymyxin B hemoperfusion
EUPHRATES RCT septic shock + confirmed endotoxemia
90% reduction in LPS with 2 treatments (2hr)EUPHAS RCT trial 2009
EUPHAS -2 prospective web-based registry
015304560
Mortality
Control PMx

Polymyxin B Hemoperfusion• Prospective MC (18) RCT comparing conventional treatment with
conventional treatment + 2 sessions of polymyxin B hemoperfusion (ABDO-MIX trial)
• Septic shock after surgery for peritonitis
• Primary outcome: mortality at D 28
• Secondary outcomes: mortality at D 90, SOFA score variation within 3 days
Payen DM. Intensive Care Med 2015;41:975-984
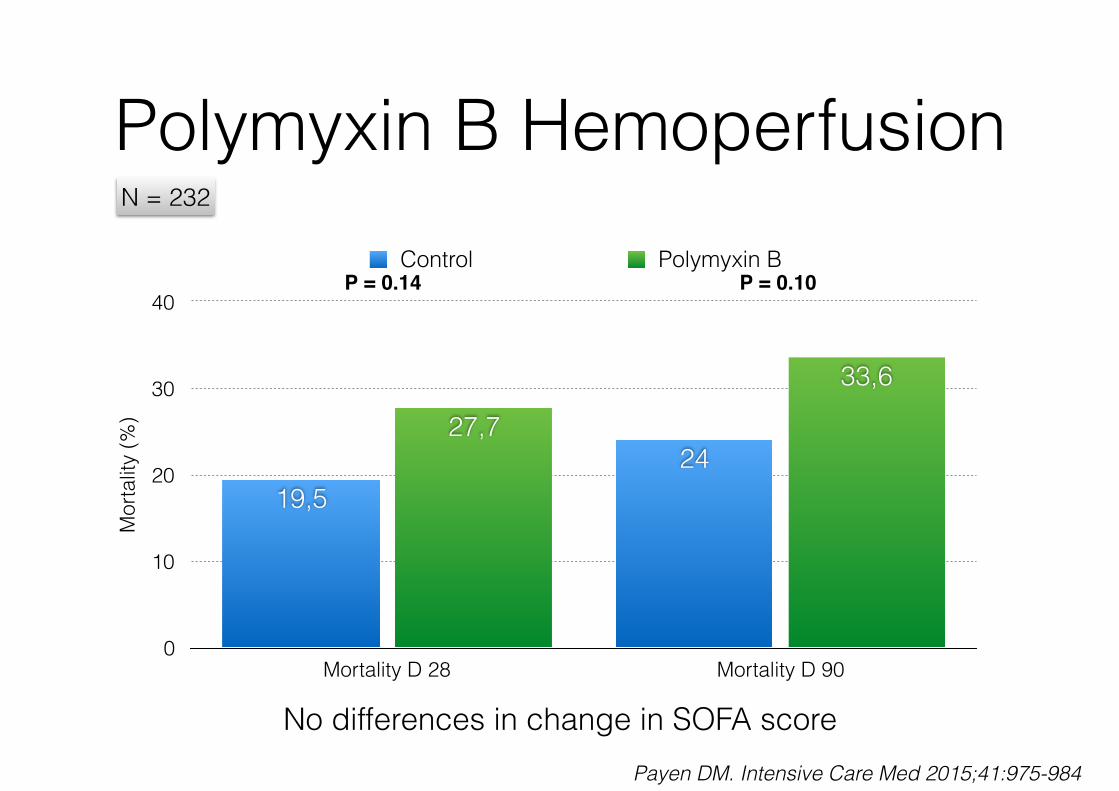
Polymyxin B HemoperfusionN = 232
Mor
talit
y (%
)
0
10
20
30
40
Mortality D 28 Mortality D 90
33,6
27,724
19,5
Control Polymyxin BP = 0.10P = 0.14
No differences in change in SOFA scorePayen DM. Intensive Care Med 2015;41:975-984
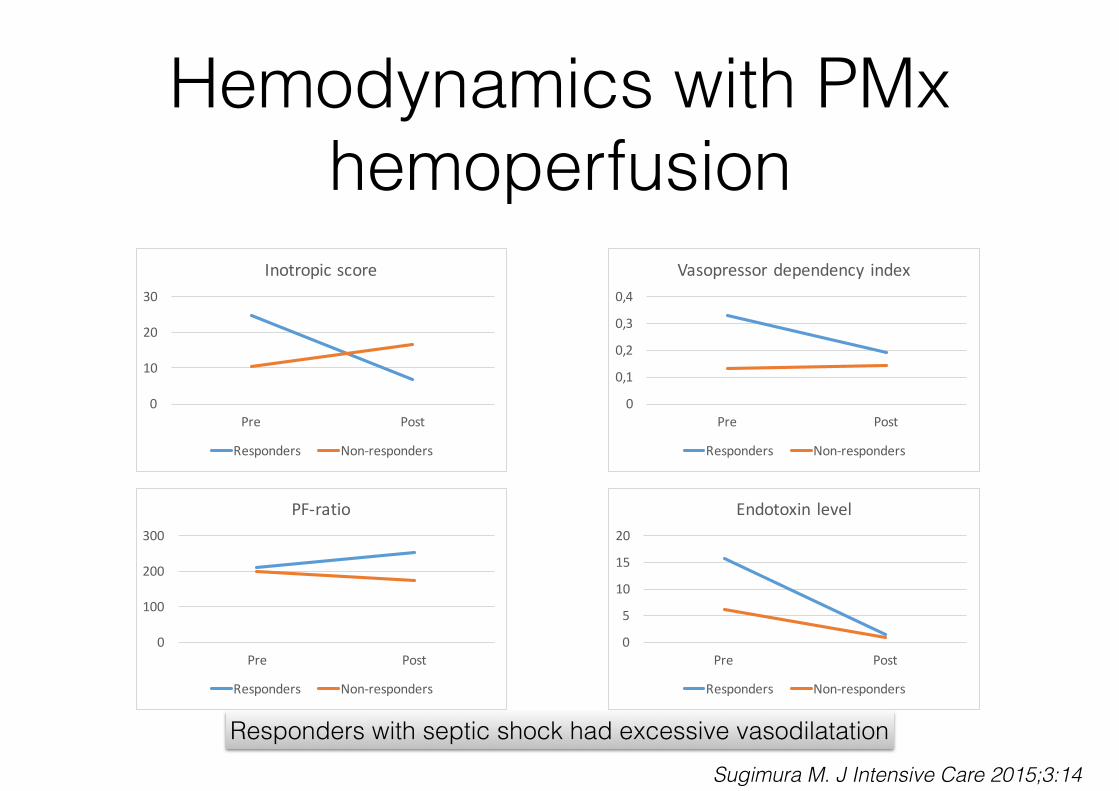
Hemodynamics with PMx hemoperfusion
0
10
20
30
Pre Post
Inotropicscore
Responders Non-responders
0
0,1
0,2
0,3
0,4
Pre Post
Vasopressordependency index
Responders Non-responders
0
100
200
300
Pre Post
PF-ratio
Responders Non-responders
0
5
10
15
20
Pre Post
Endotoxin level
Responders Non-responders
Responders with septic shock had excessive vasodilatationSugimura M. J Intensive Care 2015;3:14

Rapid adequate initiation of antibiotics essential
Septic shock (N = 2154)
Kumar A. Crit Care Med 2006;34:1589-1596
0.0
0.2
0.4
0.6
0.8
1.0
0-0.5 0.5-1 1-2 2-3 3-4 4-5 5-6 6-9 9-12 12-24 24-36 > 36
Time from onset hypotension (hrs)
Frac
tion
of to
tal p
atie
nts
Cumulative effective antimicrobial initiation
Survival fraction
BUT…..
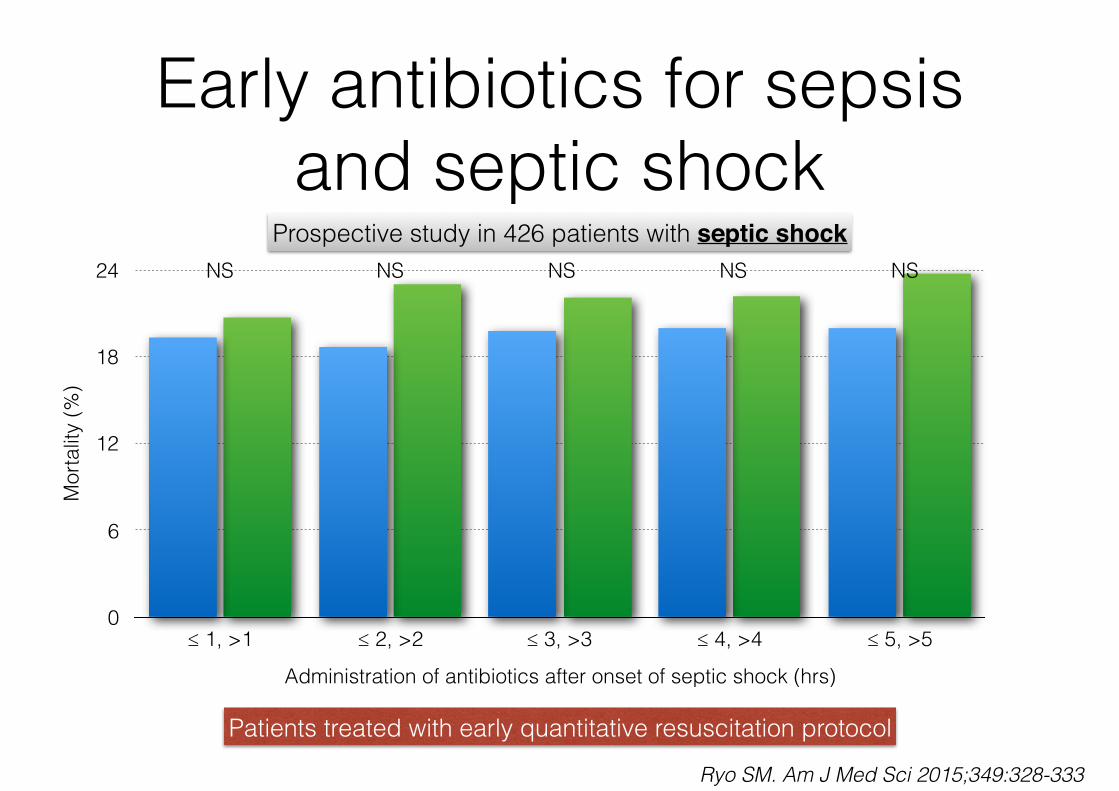
Early antibiotics for sepsis and septic shock
Prospective study in 426 patients with septic shock
Mor
talit
y (%
)
0
6
12
18
24
Administration of antibiotics after onset of septic shock (hrs)
≤ 1, >1 ≤ 2, >2 ≤ 3, >3 ≤ 4, >4 ≤ 5, >5
NS NS NS NS NS
Ryo SM. Am J Med Sci 2015;349:328-333
Patients treated with early quantitative resuscitation protocol
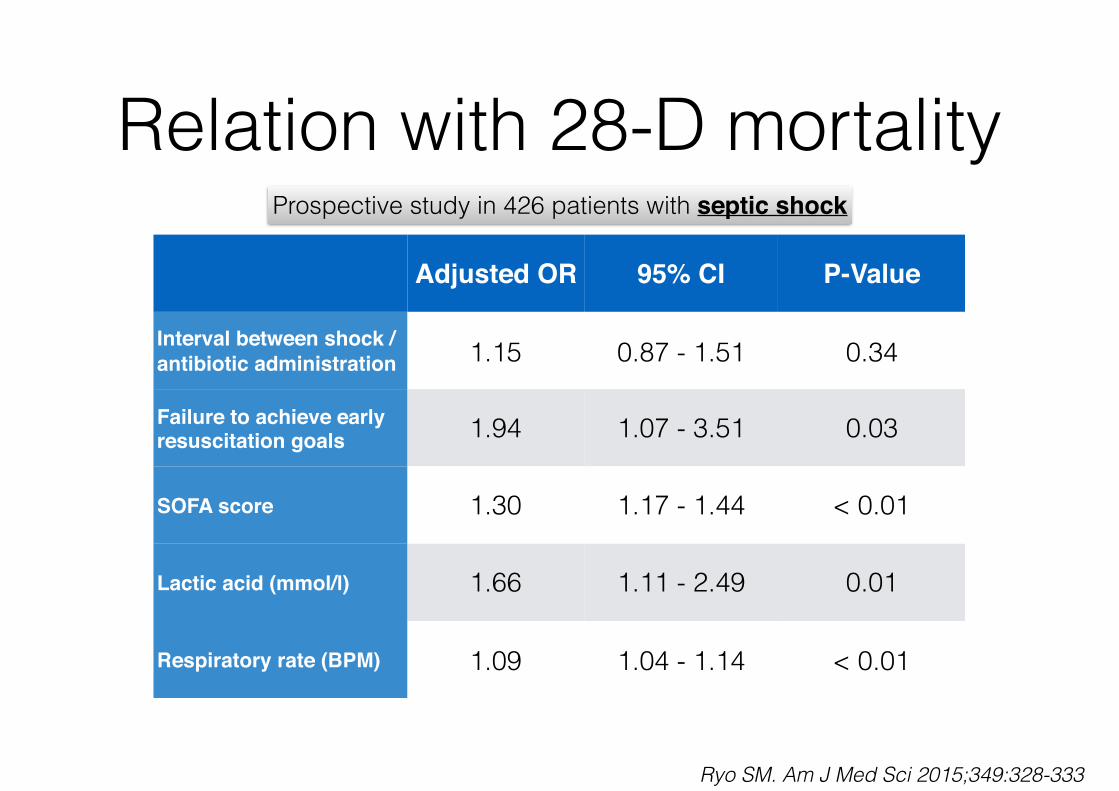
Relation with 28-D mortality
Adjusted OR 95% CI P-Value
Interval between shock / antibiotic administration 1.15 0.87 - 1.51 0.34
Failure to achieve early resuscitation goals 1.94 1.07 - 3.51 0.03
SOFA score 1.30 1.17 - 1.44 < 0.01
Lactic acid (mmol/l) 1.66 1.11 - 2.49 0.01
Respiratory rate (BPM) 1.09 1.04 - 1.14 < 0.01
Ryo SM. Am J Med Sci 2015;349:328-333
Prospective study in 426 patients with septic shock
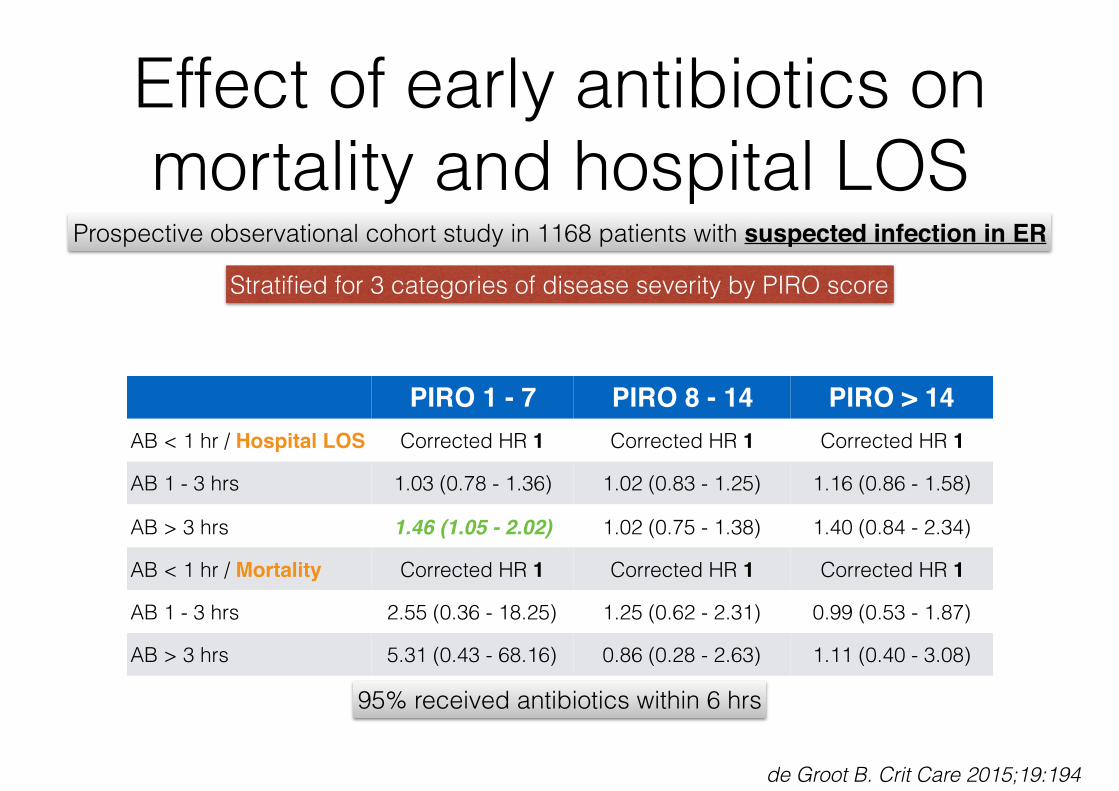
Effect of early antibiotics on mortality and hospital LOS
Prospective observational cohort study in 1168 patients with suspected infection in ER
Stratified for 3 categories of disease severity by PIRO score
PIRO 1 - 7 PIRO 8 - 14 PIRO > 14AB < 1 hr / Hospital LOS Corrected HR 1 Corrected HR 1 Corrected HR 1
AB 1 - 3 hrs 1.03 (0.78 - 1.36) 1.02 (0.83 - 1.25) 1.16 (0.86 - 1.58)
AB > 3 hrs 1.46 (1.05 - 2.02) 1.02 (0.75 - 1.38) 1.40 (0.84 - 2.34)
AB < 1 hr / Mortality Corrected HR 1 Corrected HR 1 Corrected HR 1
AB 1 - 3 hrs 2.55 (0.36 - 18.25) 1.25 (0.62 - 2.31) 0.99 (0.53 - 1.87)
AB > 3 hrs 5.31 (0.43 - 68.16) 0.86 (0.28 - 2.63) 1.11 (0.40 - 3.08)
95% received antibiotics within 6 hrs
de Groot B. Crit Care 2015;19:194
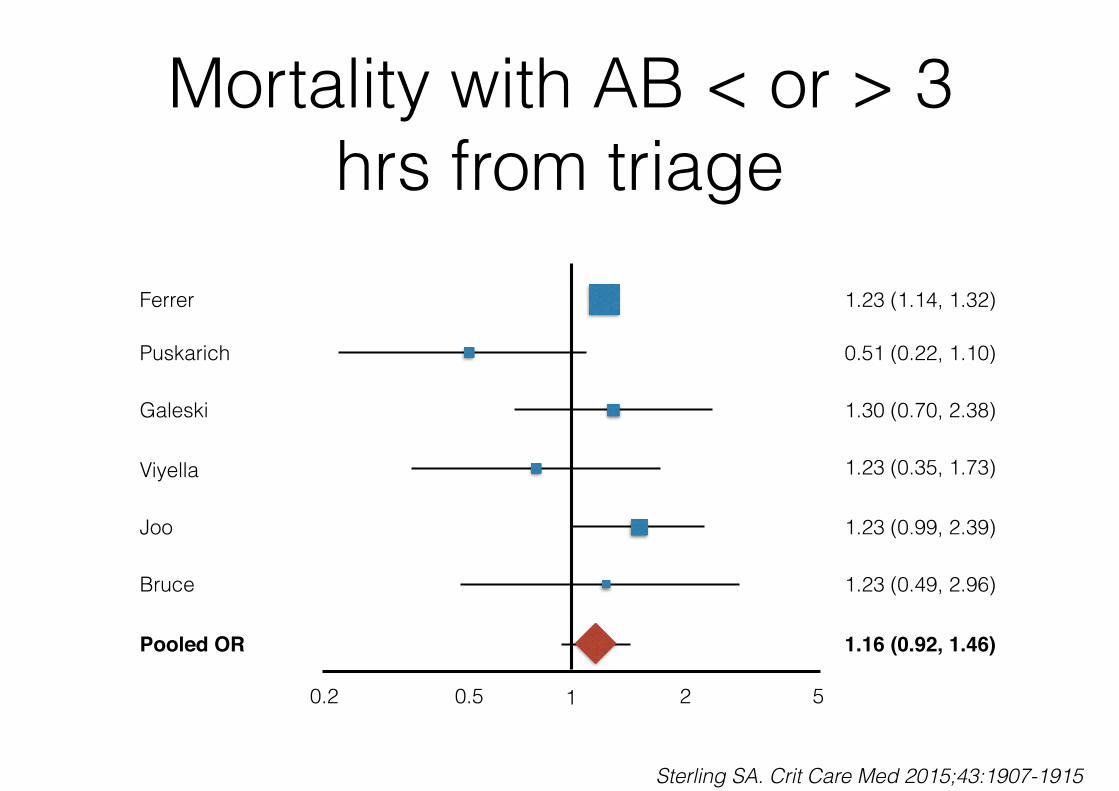
Mortality with AB < or > 3 hrs from triage
Ferrer
Puskarich
Galeski
Viyella
Joo
Bruce
Pooled OR
1 520.2 0.5
1.23 (1.14, 1.32)
0.51 (0.22, 1.10)
1.30 (0.70, 2.38)
1.23 (0.35, 1.73)
1.23 (0.99, 2.39)
1.23 (0.49, 2.96)
1.16 (0.92, 1.46)
Sterling SA. Crit Care Med 2015;43:1907-1915
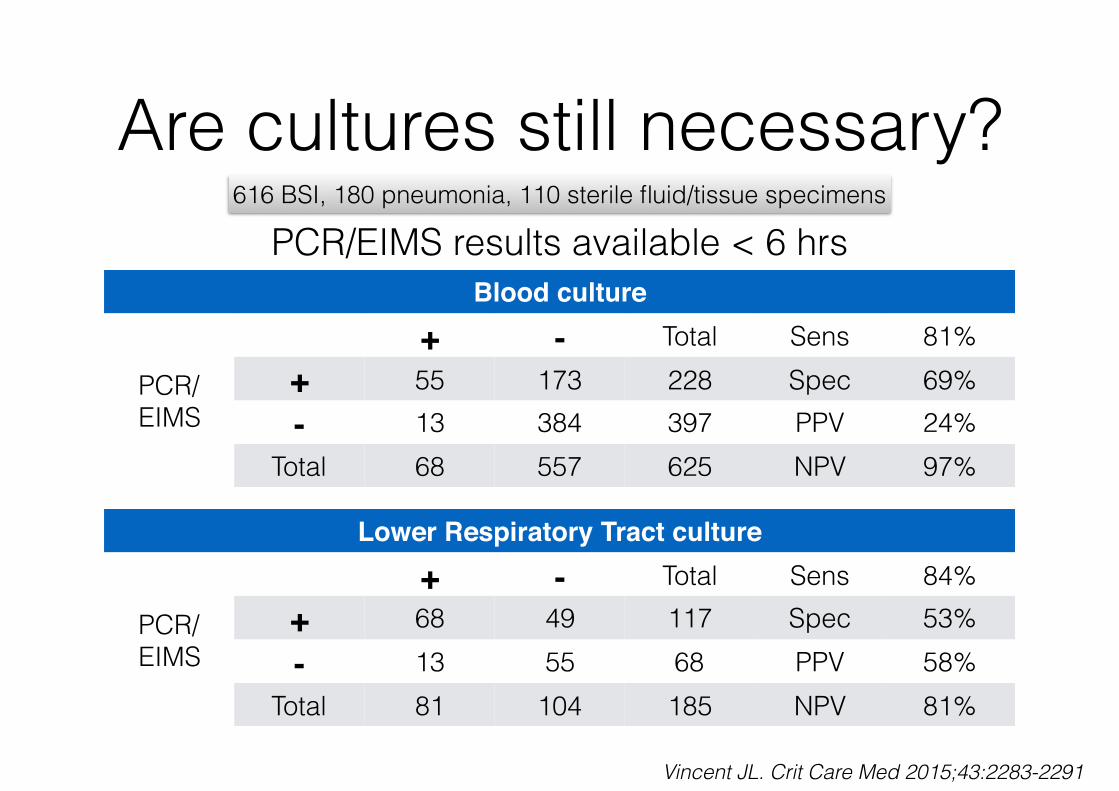
Are cultures still necessary?616 BSI, 180 pneumonia, 110 sterile fluid/tissue specimens
Blood culture
PCR/ EIMS
+ - Total Sens 81%+ 55 173 228 Spec 69%- 13 384 397 PPV 24%
Total 68 557 625 NPV 97%
PCR/EIMS results available < 6 hrs
Lower Respiratory Tract culture
PCR/ EIMS
+ - Total Sens 84%+ 68 49 117 Spec 53%- 13 55 68 PPV 58%
Total 81 104 185 NPV 81%
Vincent JL. Crit Care Med 2015;43:2283-2291

Conclusions• Mortality of severe Ebola cases with MODS is rather low
with modern ICU treatment - dehydration, diarrhea, AKI
• Antibiotics should be administered as soon as possible but only after adequate cultures have been taken
• Voriconazol resistance increases and double therapy may be indicated - be careful with hypoalbuminemia
• PJP could be an airborne transmissible disease
• Polymyxin-B hemoperfusion is not indicated (yet)





![Surviving Sepsis Campaign: International guidelines for ... · Sepsis is defined as infection plus systemic manifestations of infection (Table1) [12]. Severe sepsis is defined as](https://img.pdfslide.us/doc/110x75/5c92e4aa09d3f2195d8c1d10/surviving-sepsis-campaign-international-guidelines-for-sepsis-is-dened.jpg)