Embed Size (px)
Citation preview

PSYCHIATRIC DISORDERS
Eating disorders acrossculturesMervat Nasser
AbstractThe cultivation of the body ideal and promotion of thinness values in
fashion, media and the diet industry have been repeatedly shown to
account for the increased prevalence of eating disorders. It is evident in
women in certain sub-cultures where the demand for thinness for career
advancement is endemic. There is also a correlation between eating disor-
ders and the level of modernization and urbanization characteristic of
western industrialized societies, linking it to increased social mobility,
dietary changes as well as changes within family structures. Eating disor-
ders were, therefore, thought to be unique to the ‘western culture’, an
impression that was initially substantiated by the apparent absence of
these disorders in non-western societies. However, the notion of the
culture specificity of eating disorders began to be challenged following
reports from different parts of the world when eating disorders emerged
in non-western societies. This was believed at first to be a product of
a simple identification with western cultural norms in this respect.
However, ‘westernization’ was too simplistic and needed to be broken
down to see the forces that may lie behind it. These included increased
consumerism, shift from collectivist to individualist patterns, changing
gender roles and increased alienation of the individual. Subsequently,
the individual was forced to resort to the ‘body’ as a new medium for
expressing this cultural confusion and distress. Eating disorders are an
example of such socio-pathology and needs to be seen now as a marker
of ‘transition’ and symptomatic of cultures caught in a process of change.
Keywords body language; body medium; changing gender roles;
consumerism; cultural distress; culture transition; dietary changes; diet
industry; eating disorders; endemic thinness; individual alienation;
media; social mobility; urbanization
Eating disorders: the evolution of the socio-cultural model
Starvation, vomiting and purging following binging, are all self-
inflicted body regulatory mechanisms that collectively came to
be known as eating disorders. This term encompasses its two
extremes anorexia and bulimia and all that lie between, a spec-
trum of weight/shape-focused behaviours of varying degrees of
morbidity.
Eating disorders are considered unique among psychiatric
disorders in the degree to which social and cultural factors
influence their epidemiology and development. The nature of the
eating-disorder syndrome and the fact that it clearly merges with
the prevalent and the culturally acceptable behaviour of dieting
called for an interpretation that that is grounded in the culture we
Mervat Nasser MD MPhil FRCPsych is a Consultant Psychiatrist and visiting
Senior Research Fellow at the Institute of Psychiatry (KCL), London, UK.
Conflicts of interest: none declared.
PSYCHIATRY 8:9 34
live in. The phenomenon was therefore (understandably) linked
to the cultivation of a certain type of body ideal and the
promotion of thinness values through media, fashion and the diet
industry. Subclinical cases or partial syndrome that merge with
normal dieting behaviour were generally estimated to be five
times more common than the full-blown syndromes, a finding
that was consistent with the ‘spectrum hypothesis’ of eating
disorders and ran parallel to reported steady increase in the rate
of their occurrence in the latter half of the twentieth century.
The socio-cultural model of eating disorders was further
supported by the susceptibility of certain sub-cultural groups to
develop these disorders, such as dancers, models and athletes
where the demand for thinness is endemic. This epidemiological
research has also shown a clear and consistent ‘gender bias’
where women were found to be ten times more at risk for such
disorders than men. This skewed distribution, made feminist
theorists see these disorders as metaphorical of the ‘modern
woman’s dilemma’ being torn between a desire to conform to old
traditional stereotypes of womanhood and new values related to
what the modern woman’s ought to be. This sense of ‘gender
ambivalence’ was noted to be felt by women, particularly at
times of historical and cultural change. Even among the small
proportion of men who develop such disorders, a dispropor-
tionate number of them also have doubts or uncertainties about
their gender identity.
Another finding that emerged in the 1990s was the apparent
increase in the prevalence of eating disorders in proportion to the
level of ‘urbanization’ in any given society. This was explained
on the basis of social mobility and changes within family struc-
ture with a tendency towards nuclearization. Also, as cities
urbanize, eating patterns, food preferences and meal times seem
to change, with the inevitable rise in the rates of obesity and
a subsequent increase in weight consciousness and disordered
patterns of eating.
So, within this framework, cultural, subcultural and inter-
cultural risks in the pathogenesis of eating disorders are easily
discernable. However, one of the most important aspects of the
socio-cultural argument has always been the apparent trans-
cultural variation whereby these disorders have been considered
rare or, indeed absent, in non-western societies (Box 1). This
made some regard eating disorders as a phenomenon unique to
western culture.
Eating disorders: from ‘western’ disorder to global phenomenon
The culture specificity of eating psychopathology to western
culture was initially based on an ‘epidemiologic evidence’, i.e. the
absence of sufficient published data to confirm their occurrence
in non-western cultures and societies. This was assumed to
reflect perceived differences in aesthetic standards and gender
role definitions between western and non-western societies. This
perception was, to large extent, rooted in a general tendency to
see non-western cultures as being static, isolated and remote
from forces of change that affected western societies. This was
particularly evident in the case of other women, whose roles
continued to be seen within a restricted framework of the
stereotyped and the traditional.
Notwithstanding the debate about culture and its definitions,
there is now increasing evidence that challenges the notion of the
7 � 2009 Elsevier Ltd. All rights reserved.

PSYCHIATRIC DISORDERS
western boundedness and shows these disorders to be no longer
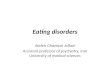
confined to one particular culture. Recent research from the
Middle East, the Far East, South America and Africa, all indicate
that eating disorders are now emerging in these societies with
similar or even higher rates to those reported in the West
(Figure 1, Box 2). The majority of this research was modelled on
community surveys carried out in the West where the Eating
Attitude Test Questionnaire (EAT) was the main instrument. The
EAT, is a self-report questionnaire that was originally devised to
elicit abnormalities in eating attitudes and measure a broad range
of symptoms characteristic of anorexia nervosa. Doubts were
understandably raised about the validity of the EAT in different
cultural settings and its susceptibility to cultural misinterpreta-
tion, and yet the EAT proved helpful at least in allowing
preliminary comparisons across cultures.
Percentage of dieting/abnormal eating attitudesworldwide
Countries
)%(
evi+t
aE
35
30
25
20
15
10
airtsuA
ynamreG
yragnuH
anihC
dnaloP
ylatIKU
tpygE
)A( learsI
acirfA .S
)K( learsI
anitnegrA
aidnInapaJ
5
0
Figure 1
Eating disorders e the socio-cultural model
C Culture specificity: assumed to be bound to ‘western’ culture
C Nature of psychopathology: symbolic of notions of thinness
cherished and promoted by the western culture
C Continuum of morbidity: merges with culturally acceptable
behaviours
C Reported increase over the past 50 years possibly in response
to increased emphasis on the ‘thinness ideal’
C Gender specific: women at risk by reason of gender
ambivalence
C Subcultural variations: more prevalent in dancers, models and
athletes where demand for thinness is endemic.
C Intra-cultural variations: possibly more prevalent in urban than
rural areas
Box 1
PSYCHIATRY 8:9 34
Identification with western norms in relation to body weight
and image was initially offered as an explanation for this
worldwide emergence of eating psychopathology, and in the
majority of these studies a correlation was found between eating
disorders in those societies and the level of their exposure to
western cultural norms in this respect.
The media was considered to play the main role in spreading
this ‘body ideal’ and in homogenizing perceptions worldwide in
this respect.
However, the effect of exposure to western culture combined
with the presence of strong religious values in some populations
and societies proved to be more significant particularly among
the Muslim Asian population in the UK as well as Muslim women
in the Gulf region and Iran. This showed that what is at stake
here is the issue of conflicted cultural values rather than the
simple exposure to different cultural norms.
Another major finding in this respect was the emergence of
eating psychopathology in Eastern Europe following the politico-
economic changes. Eating disorders were largely unreported in
Eastern Europe before the collapse of the communist regimes and
only began to appear in eastern European literature in the
nineties with reported high rates of abnormal eating attitudes in
Hungary, Poland and the Czech Republic. This was largely
attributed to the transition from state-controlled economy to
Countries reporting eating disorders
Argentina*
Australiaþ
Belgium
Brazil*
Canada
Chile
China*
Czech Republic
Denmarkþ
Egypt
France
Germany
Hong Kong*
Hungary
India*
Iranþ,*
Israelþ
Italy
Japan
Mexico*
the Netherlands
New Zealandþ
Nigeria
Norway
Poland
Portugal*
Singapore*
South Africa
(blacks)*
South Africa
(whites)þ
South Korea*
former Soviet
Union
Swedenþ
Switzerlandþ
Turkey*
United Arab
Emirates*
United Kingdomþ
United Statesþ
þ Formal epidemiological studies carried out.
* First reports since 1990.
Reproduced, with permission, from Gordon R. Eating disorders
East and West: a culture-bound syndrome unbound. In: Nasser
et al, eds. Eating disorders and cultures in transition. London:
Brunner-Routledge, 2001. p. 1e24.
Box 2
8 � 2009 Elsevier Ltd. All rights reserved.

PSYCHIATRIC DISORDERS
markets that undermined the collective social structure and
resulted in the disappearance of some of the social networks that
provided women with protection in their education, employment
and childcare rights. This resulted in greater ‘gender ambiva-
lence’ increasing the vulnerability of those women to eating
disorders (Box 2).
Eating disorders: the case of ethnic minority groups
The prevalence studies shown in Figure 1 went hand in hand with
studies of ethnic minorities in USA and UK. An increase in the
prevalence of eating disorders among black, Native Americans
and Hispanic communities in the USA was reported. Similar
results were also obtained among the Asian and the African-
Caribbean immigrant populations in the UK. The Asian pop-
ulation constitutes the largest immigrant population in the UK
and comprises Indians, Pakistanis and Bangladeshis. In the
majority of these studies, more cases of bulimic behaviour were
found among Asian schoolgirls than in their Caucasians
counterparts.
Cultural variations on how ‘Asian’ is defined between the US
and UK suggest that studies of Asian populations in these
countries actually differ in the types of samples they are exam-
ining. In the UK, these investigations typically involve individ-
uals who are ethnically south Asian (i.e. from India, Pakistan,
and Sri Lanka, etc.); in the US, the term ‘Asian American’ refers
to East Asian and South Asian countries. When Asian women
attending American schools in the US were compared with those
in Hong Kong, the former group showed evidence of increased
vulnerability to abnormal eating behaviours. It was argued,
however, that the over-reliance on the ‘fear of fatness’ as
a diagnostic criterion in eating psychopathology could have led
to a general underestimation of the magnitude of these problems
in societies like China, India and Japan.
The authors of these studies linked the susceptibility of the
immigrant population to eating disorders to their high aspirations
and achievement orientation, and more importantly to their
conflict over ‘racial identity’. It was noted that many of them felt
a strong need to correct a negative and traditionally stereotyped
racial image and had a powerful urge to fit into the host society
through conforming to the prevailing ideal of thinness/beauty.
A correlation was found between the level of acculturation
and morbid concern over weight. Dieting behaviour was found to
be equal among black and white females in the USA and
dysfunctional eating patterns were found to be more prevalent in
the African-Caribbean population in Britain than their white
counterparts. The issue of ‘racial identity’ and its relationship to
eating disorders was also studied among black South African
women after the fall of the apartheid regime, where the reported
increase of eating disorders following the political change was
linked to a sense of shifting identity and altered self-conception
among those South African females.
This shows that contrary to all initial assumptions immigrants
could be at a higher risk of developing eating psychopathology
than the native population (see Box 3).
Transitional cultural forces and the issue of acculturative stress
From what has been advanced so far, it is clear that disordered
forms of eating behaviour are grounded in the global culture of
PSYCHIATRY 8:9 34
modernity which characterizes many rapidly urbanizing parts of
the world today. These changes are bound to influence life and
dietary patterns, with a likely increase in the rates of obesity fol-
lowed by weight consciousness and disordered eating patterns.
These behaviours also reflect the tensions and conflicts of the
current cultural transition where a number of deregulatory forces
are in play, including markets and media with their power of
standardizing the aesthetic ideal and the marketing of this ideal
worldwide. Media and information technologies are also great
unifying powers that have the potential to dilute cultural speci-
ficity and undermine national boundaries, thus posing a threat to
cultural identity. Under these transitional circumstances, any
individual who has insufficient adaptive resources to support
adjustment to this new cultural environment is bound to suffer an
‘acculturative stress’, where the body becomes the platform of its
expression manifesting in eating disorders or any of its equivalents
or permeations. This clearly shows that eating disorders are far
from being just a simple compliance wild a Western cosmetic ideal
but a psychosocial pathology symptomatic of social transition,
where the body becomes a dominant means by which the tension
and crises of society are thematized (Box 4).
Transnational approaches to treatment and prevention
As one examines the movement of eating disorders from indi-
vidual neurosis to cultural marker of distress, caused by transi-
tional and conflicting cultural forces, it becomes increasingly
important to identify ways of operationalizing treatment and
prevention strategies.
Immigrants/ethnic minority groups: vulnerabilityfactors
C Confused and disturbed racial/cultural identity
C A strong need to correct a negative and traditionally stereo-
typed racial image
C Strong need to fit into the host society by conforming to the
prevailing aesthetic standard
C Desire for success, achievement and the fulfilment of higher
aspirations
Box 3
Transitional/de-regulatory ‘cultural’ forces
C The marketing of a standard aesthetic ideal through universal
media
C Life-style changes e change in work/dietary habits and
increased rates of obesity
C Increased levels of urbanization, migration and immigration
C Worldwide confusion over gender role definitions
C Revision of traditional national boundaries through universal
media and information networks
Box 4
9 � 2009 Elsevier Ltd. All rights reserved.

PSYCHIATRIC DISORDERS
The link between power and knowledge production has been
explored in a number of preventative strategies. For example, in
the participatory model empowering knowledge is constructed
through dialogue, self-inquiry and reflection based on life experi-
ences. Electronic connections may provide a new way of achieving
connectedness; linked by computer technology, individual
sufferers may be able to overcome their social and political isola-
tion and gain new insights into formulae for success and survival.
Other models of prevention can be employed, again through
producing computer programs or other types of mass media
geared towards the enhancement of self-esteem, teaching coping
skills and promoting positive cognitions related to negotiations of
power and control and to the significance of the individual in
relation to the environment.
Similar techniques are currently being used in the manage-
ment of eating disorders focusing on psycho-education and
self-help cognitive strategies as well as interactive web-based
multi-media therapeutic programmes that are likely to make
specialist therapies available to many more people who
PSYCHIATRY 8:9 350
traditionally would have been unable to access such help.
Recognition of these new mechanisms is likely to stimulate
research devoted to a transnational perspective for the preven-
tion and management of eating disorders. A
FURTHER READING
Nasser M. Culture and weight consciousness. London, New York:
Routledge, 1997.
Nasser M, Katzman M, Gordon R. Eating disorders and cultures in tran-
sition. London, New York: Brunner-Routledge, Taylor & Francis Group,
2001. p. 1e24.
Nasser M, Katzman M. Socio-cultural theories of eating disorders. In:
Treasure J, Schmidt U, van Furth E, eds. Handbook of eating disorders.
London: Wiley & Sons, 2003. p. 139e51.
Nasser M. Culture and eating disorders. In: Bhugra D, Bhui K, eds. Text-
book of cultural psychiatry. Cambridge, UK: Cambridge University
Press, 2007. p. 292e301.
� 2009 Elsevier Ltd. All rights reserved.