Embed Size (px)
Citation preview
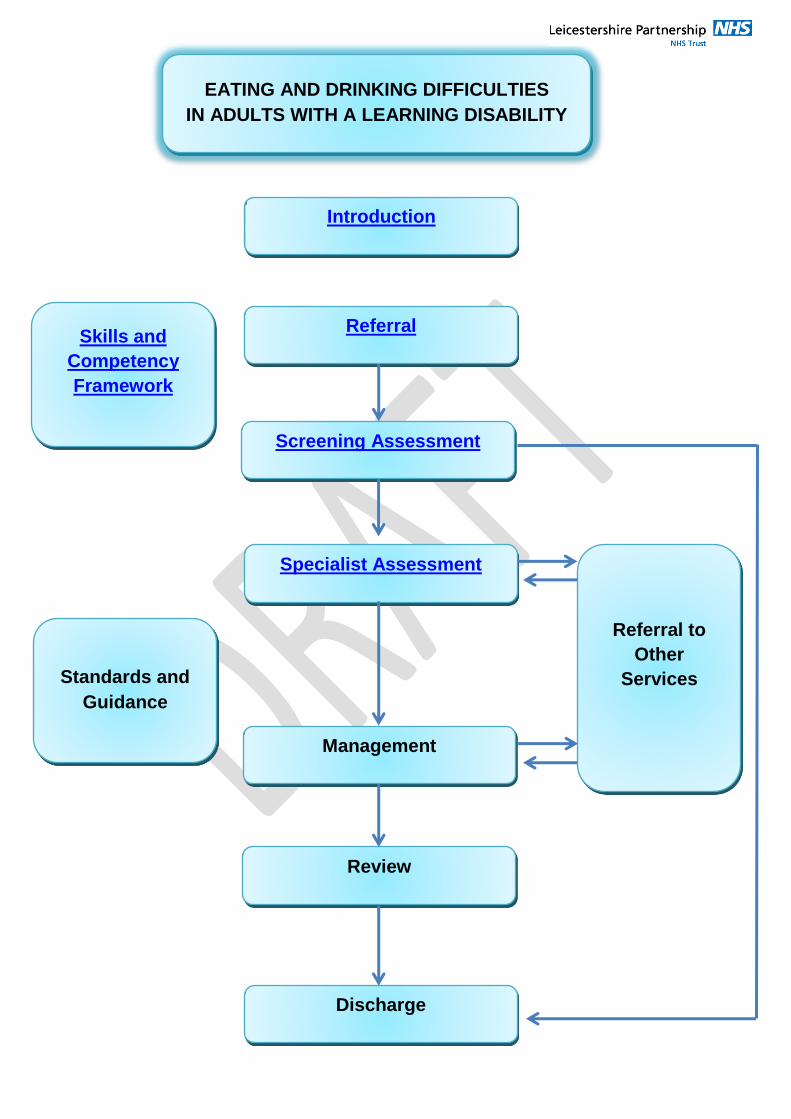
EATING AND DRINKING DIFFICULTIES
IN ADULTS WITH A LEARNING DISABILITY
Introduction
Referral
Specialist Assessment
Review
Management
Screening Assessment
Discharge
Referral to
Other
Services
Skills and
Competency
Framework
Standards and
Guidance
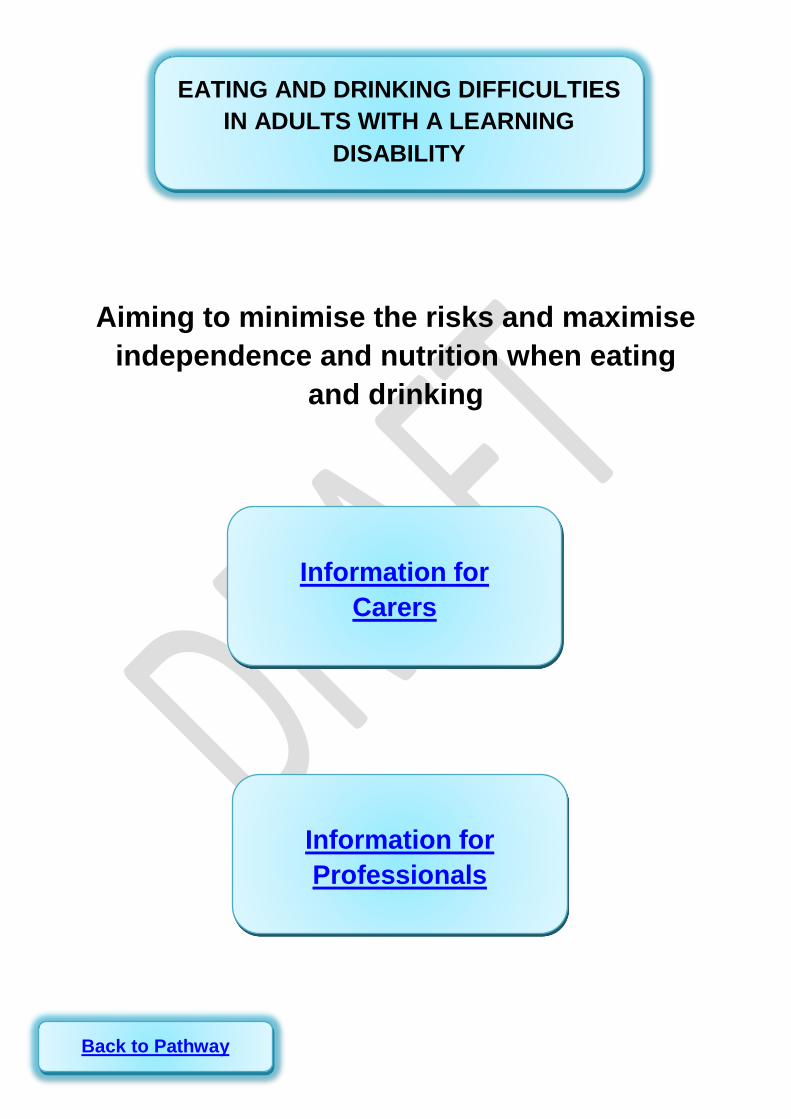
Aiming to minimise the risks and maximise
independence and nutrition when eating
and drinking
EATING AND DRINKING DIFFICULTIES
IN ADULTS WITH A LEARNING
DISABILITY
Information for
Professionals
Information for
Carers
Back to Pathway

These leaflets may help you to decide whether to refer:
Eating and Drinking information leaflet Information for Carers (From NPSA 2007) If you decide you need further help, use the appropriate referral form for where you live. You can fill it in and send it to the address given or ask your GP to make the referral. If the person to be referred is coughing when eating or drinking, it would be helpful to have a record of coughing incidents to bring with you to the appointment. If the person has choked, check with this alert document what to do. You could complete a choking incident form to bring with you to the appointment. If the person is losing weight or refusing food, you could complete a Food diary chart to bring with you to the appointment. The Food First leaflet will give you some tips to keep a person’s weight healthy until your appointment. Further information for carers link A10
You may find the following websites helpful
NPSA npsa.nhs.uk
MENCAP www.mencap.org.uk
Alzheimers society www.alzheimers.org.uk
Caroline Walker trust www.cwt.org.uk
BILD www.bild.org.uk
Rett UK www.rettuk
Information for Carers
Back to Pathway
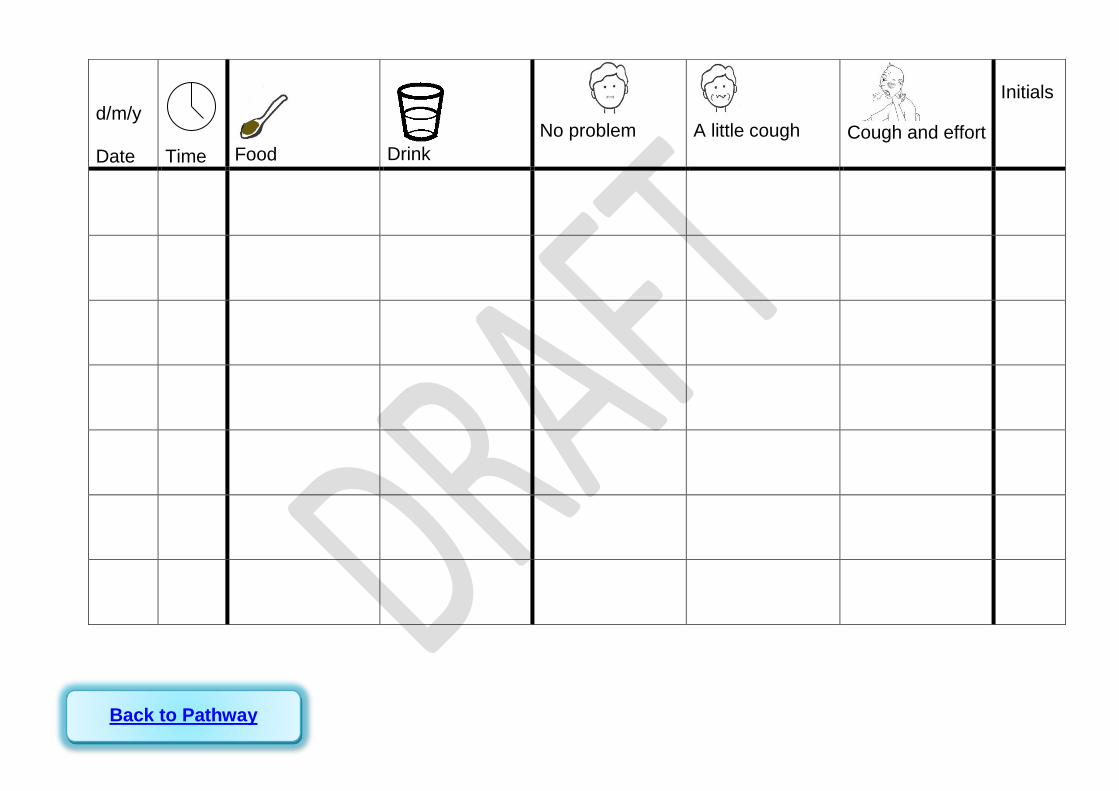
d/m/y Date
Time
Food
Drink
No problem
A little cough
Cough and effort
Initials
Back to Pathway
Problems with swallowing food and drink
(dysphagia) can be life threatening.
If you are concerned that someone is having difficulty when
eating or drinking, first decide –
Is it an emergency?
ALERT
Yes This is life
threatening e.g.
difficulty breathing,
turning blue, choking,
severe distress
whilst eating or
drinking.
What should you
do? Use your first aid
procedures.
Call for an
ambulance.
Later make a full
report of the
incident and tell your
GP about the
incident.
No - any of these signs whilst eating
may suggest problems with swallowing:
coughing, choking, some distress, face
reddening, eyes watering, nose running,
or breathlessness. In this case refer to
Speech and language therapy (SALT)
(See below).
Swallowing difficulties are often
associated with other health problems.
If you are concerned about the person’s
general health, contact the GP as soon
as possible.
Make a referral to Speech and
language therapy through the Learning
Disability Team for an assessment.
(SALT does not respond to emergency
referrals and you may have to wait for
up to a month to see someone)
If the person has an eating and
drinking plan and you are not sure of the
recommendations or think the plan
needs updating contact the Learning
disability team.
Back to Pathway
Continued overleaf………
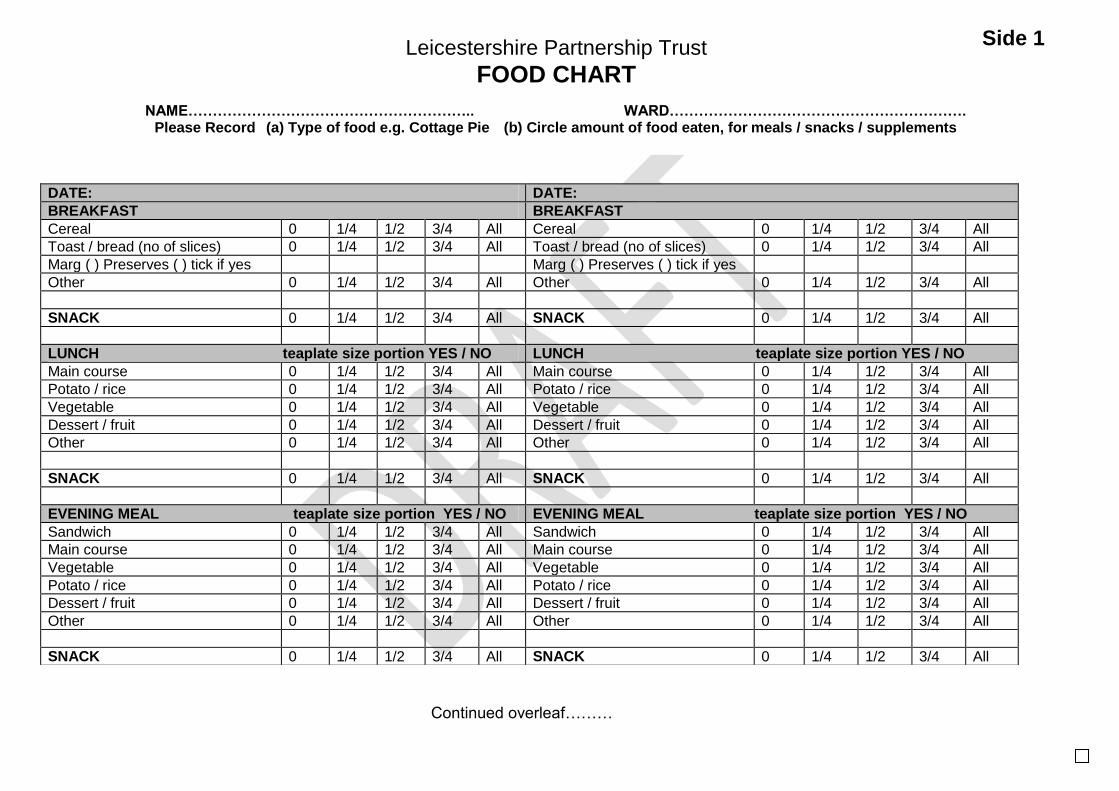
DATE: DATE:
BREAKFAST BREAKFAST
Cereal 0 1/4 1/2 3/4 All Cereal 0 1/4 1/2 3/4 All
Toast / bread (no of slices) 0 1/4 1/2 3/4 All Toast / bread (no of slices) 0 1/4 1/2 3/4 All
Marg ( ) Preserves ( ) tick if yes Marg ( ) Preserves ( ) tick if yes
Other 0 1/4 1/2 3/4 All Other 0 1/4 1/2 3/4 All
SNACK 0 1/4 1/2 3/4 All SNACK 0 1/4 1/2 3/4 All
LUNCH teaplate size portion YES / NO LUNCH teaplate size portion YES / NO
Main course 0 1/4 1/2 3/4 All Main course 0 1/4 1/2 3/4 All
Potato / rice 0 1/4 1/2 3/4 All Potato / rice 0 1/4 1/2 3/4 All
Vegetable 0 1/4 1/2 3/4 All Vegetable 0 1/4 1/2 3/4 All
Dessert / fruit 0 1/4 1/2 3/4 All Dessert / fruit 0 1/4 1/2 3/4 All
Other 0 1/4 1/2 3/4 All Other 0 1/4 1/2 3/4 All
SNACK 0 1/4 1/2 3/4 All SNACK 0 1/4 1/2 3/4 All
EVENING MEAL teaplate size portion YES / NO EVENING MEAL teaplate size portion YES / NO
Sandwich 0 1/4 1/2 3/4 All Sandwich 0 1/4 1/2 3/4 All
Main course 0 1/4 1/2 3/4 All Main course 0 1/4 1/2 3/4 All
Vegetable 0 1/4 1/2 3/4 All Vegetable 0 1/4 1/2 3/4 All
Potato / rice 0 1/4 1/2 3/4 All Potato / rice 0 1/4 1/2 3/4 All
Dessert / fruit 0 1/4 1/2 3/4 All Dessert / fruit 0 1/4 1/2 3/4 All
Other 0 1/4 1/2 3/4 All Other 0 1/4 1/2 3/4 All
SNACK 0 1/4 1/2 3/4 All SNACK 0 1/4 1/2 3/4 All
Leicestershire Partnership Trust
FOOD CHART
NAME………………………………………………….. WARD……………………………………………………. Please Record (a) Type of food e.g. Cottage Pie (b) Circle amount of food eaten, for meals / snacks / supplements
Side 1
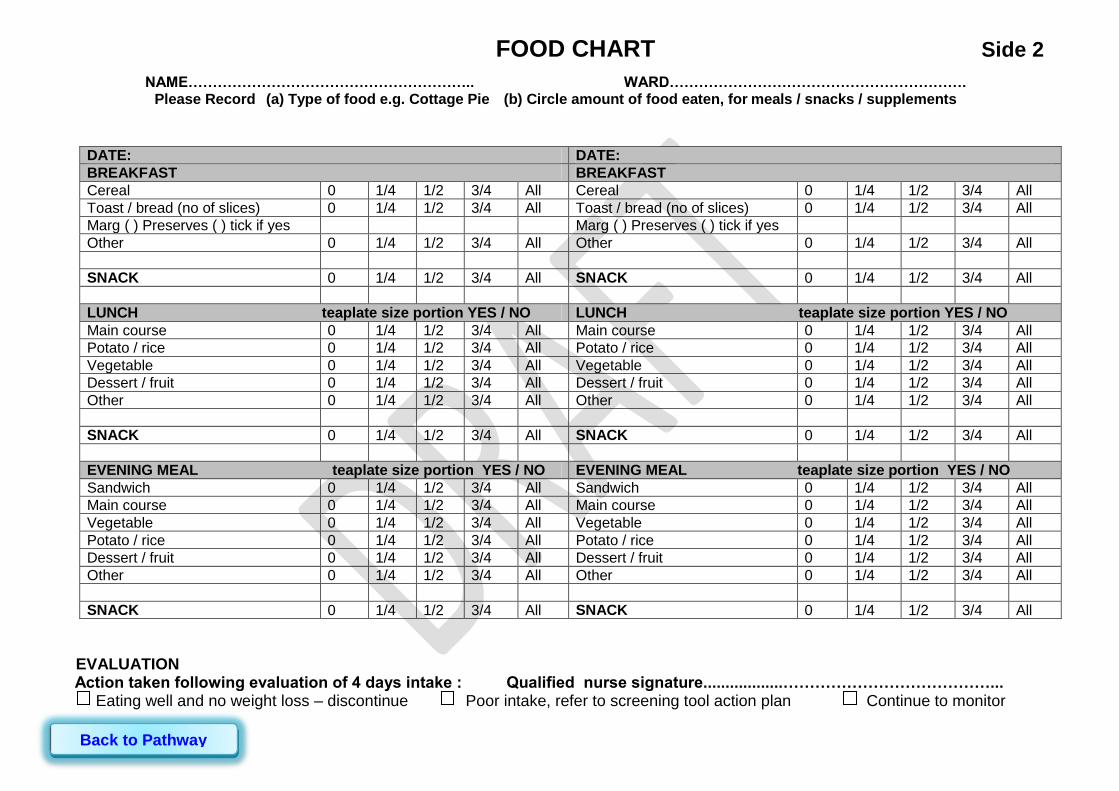
EVALUATION Action taken following evaluation of 4 days intake : Qualified nurse signature..................…………………………………... Eating well and no weight loss – discontinue Poor intake, refer to screening tool action plan Continue to monitor
DATE: DATE:
BREAKFAST BREAKFAST
Cereal 0 1/4 1/2 3/4 All Cereal 0 1/4 1/2 3/4 All
Toast / bread (no of slices) 0 1/4 1/2 3/4 All Toast / bread (no of slices) 0 1/4 1/2 3/4 All
Marg ( ) Preserves ( ) tick if yes Marg ( ) Preserves ( ) tick if yes
Other 0 1/4 1/2 3/4 All Other 0 1/4 1/2 3/4 All
SNACK 0 1/4 1/2 3/4 All SNACK 0 1/4 1/2 3/4 All
LUNCH teaplate size portion YES / NO LUNCH teaplate size portion YES / NO
Main course 0 1/4 1/2 3/4 All Main course 0 1/4 1/2 3/4 All
Potato / rice 0 1/4 1/2 3/4 All Potato / rice 0 1/4 1/2 3/4 All
Vegetable 0 1/4 1/2 3/4 All Vegetable 0 1/4 1/2 3/4 All
Dessert / fruit 0 1/4 1/2 3/4 All Dessert / fruit 0 1/4 1/2 3/4 All
Other 0 1/4 1/2 3/4 All Other 0 1/4 1/2 3/4 All
SNACK 0 1/4 1/2 3/4 All SNACK 0 1/4 1/2 3/4 All
EVENING MEAL teaplate size portion YES / NO EVENING MEAL teaplate size portion YES / NO
Sandwich 0 1/4 1/2 3/4 All Sandwich 0 1/4 1/2 3/4 All
Main course 0 1/4 1/2 3/4 All Main course 0 1/4 1/2 3/4 All
Vegetable 0 1/4 1/2 3/4 All Vegetable 0 1/4 1/2 3/4 All
Potato / rice 0 1/4 1/2 3/4 All Potato / rice 0 1/4 1/2 3/4 All
Dessert / fruit 0 1/4 1/2 3/4 All Dessert / fruit 0 1/4 1/2 3/4 All
Other 0 1/4 1/2 3/4 All Other 0 1/4 1/2 3/4 All
SNACK 0 1/4 1/2 3/4 All SNACK 0 1/4 1/2 3/4 All
FOOD CHART Side 2
NAME………………………………………………….. WARD……………………………………………………. Please Record (a) Type of food e.g. Cottage Pie (b) Circle amount of food eaten, for meals / snacks / supplements
Back to Pathway
Introduction / Overview
Referral Forms
Eating and Drinking Leaflet
Triaging Referrals
List of Foundation Workers
ICD10 Codes
List of medications that may affect swallowing
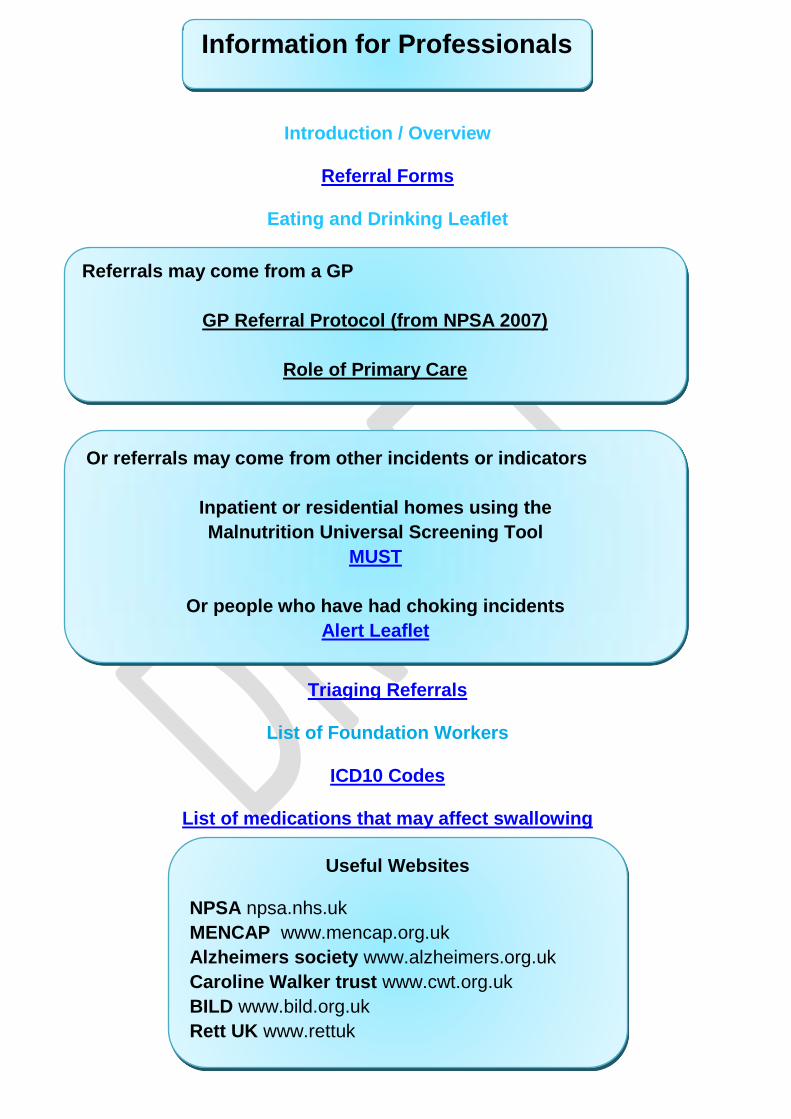
Information for Professionals
Referrals may come from a GP
GP Referral Protocol (from NPSA 2007)
Role of Primary Care
Or referrals may come from other incidents or indicators
Inpatient or residential homes using the
Malnutrition Universal Screening Tool
MUST
Or people who have had choking incidents
Alert Leaflet
Useful Websites
NPSA npsa.nhs.uk
MENCAP www.mencap.org.uk
Alzheimers society www.alzheimers.org.uk
Caroline Walker trust www.cwt.org.uk
BILD www.bild.org.uk
Rett UK www.rettuk

NUTRITIONAL SCREENING TOOL (MUST)
COMPLETE ON FIRST SCREEN - DATE :
Current Weight
_______ kg
Measured / Recall PLEASE CIRCLE
Height
______ m
Measured / Recall PLEASE CIRCLE
Body Mass Index (BMI)
______
USE CHART TO
CALCULATE FROM CURRENT WEIGHT
AND HEIGHT
Weight 3-6 months ago
_______ kg
Measured / Recall
/ Don’t Know PLEASE CIRCLE
% Weight Loss Change in weight
YES / NO / Don’t know
IF YES USE CHART TO CALCULATE % USING CURRENT AND PREVIOUS
WEIGHT
MUST SCORE
DATE
A BMI Less than 18.5 = 2 Between 18.5 and 20 = 1 More than 20 = 0
Please circle score
2 1 0
2 1 0
2 1 0
2 1 0
B % Weight loss NB Oedema may mask loss of muscle weight
More than 10% = 2 Between 5 and 10% or visual loss of weight if not known = 1 Less than 5 = 0
2
1 0
2
1 0
2
1 0
2
1 0
C Starvation score
NO or likely to be NO Intake for > 5days: YES = 2
NO = 0
2 0
2 0
2 0
2 0
TOTAL RISK LOW = 0 MEDIUM = 1 HIGH = 2
Add scores to give RISK If score 1 or more start Nutrition Treatment plan overleaf. If no improvement or score > 4 refer to Dietitian
Write in
total score
NUTRITIONAL TREATMENT PLAN STARTED? YES NO NOT NEEDED
Please circle
SIGN
WEIGH PATIENT WEEKLY AND DOCUMENT ON WEIGHT CHART
Back to Pathway
Please place client / service user label
here.

Repeat MUST weekly or if condition changes – Using new weight Nursing Nutrition Care Plan For Patients At ‘Medium or High Risk’ Of
Malnutrition.
Complete detailed Nutrition Checklist Tool
Order a special diet if appropriate e.g. Gluten free, diabetic.
Refer onto Eating and Drinking pathway (LD clients) or write appropriate treatment plan
Assist with ordering suitable meal choices (Suggest High Energy ( ) main courses and puddings and ‘Chefs Specials’ - see ward menus for details). Or fortify foods prepared according to instructions provided (see home hand book).
Offer the patient additional items for snacks between meals.
Encourage milk and milky drinks.
Offer 1 Build up drink per day (savoury or sweet) Unless contraindicated e.g. renal disease, lactose intolerant, milk allergy or patients following low residue diets. Contact ward Dietitian for advice.
Offer assistance with eating and drinking, when required or follow eating and drinking plan or treatment plan
Treat underlying conditions such as nausea, vomiting, diarrhoea, constipation.
Commence food and drink record charts for all meals and snacks. REVIEW INTAKE AFTER FOUR DAYS, if intake remains minimal, and a referral has not already been made, refer to your ward or community dietitian.
Refer to your ward Dietitian if: o MUST score is greater than 4 o Tube feeding needs considering o Nil By Mouth > 5 days o MUST score increases or there is no improvement on medium/high risk nutrition
care plan o Specialist advice is required following diagnosis, or a full nutritional assessment is
required in response to clinical judgment.
Repeat weight and MUST weekly – if weight drops >1kg/week refer to your ward Dietitian
Ensure that prior to discharge the patient is reviewed by the ward Dietitian. This will ensure the
patient receives appropriate advice for home, and the need for any supplements can be
assessed.
MEDIUM/HIGH RISK
If Dietetic referral is required please document
DATE made and SIGN here.
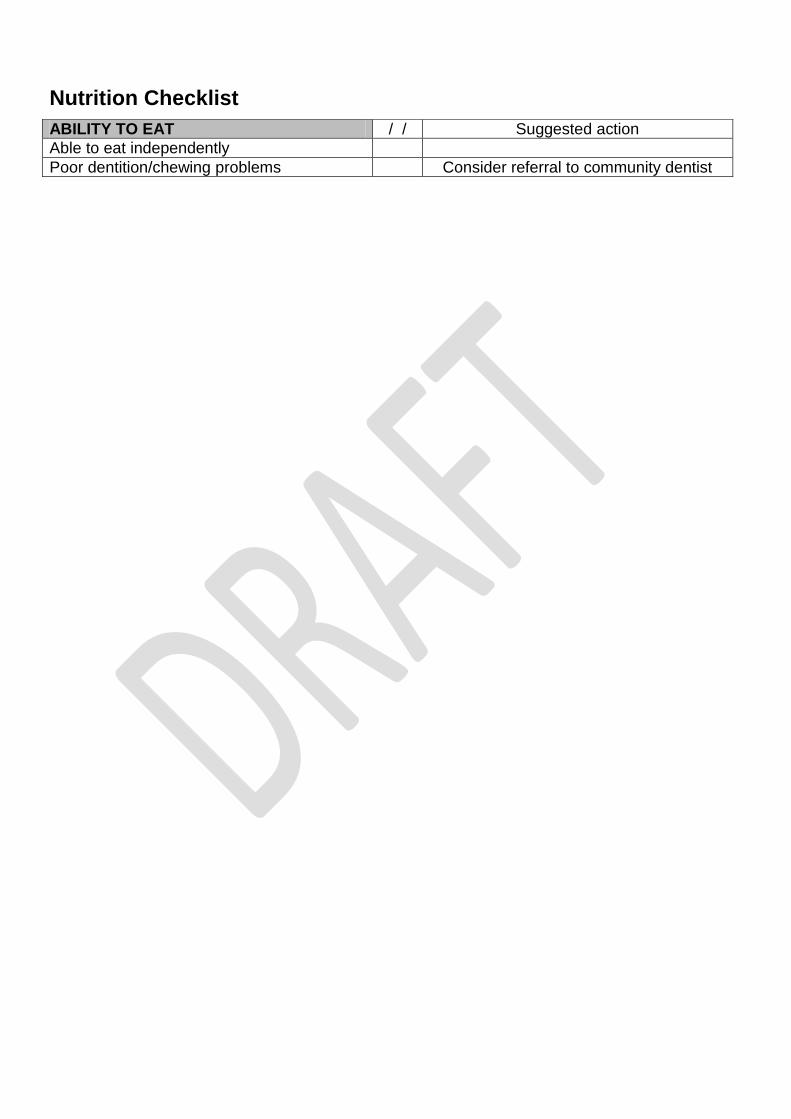
Nutrition Checklist
ABILITY TO EAT / / Suggested action
Able to eat independently
Poor dentition/chewing problems Consider referral to community dentist
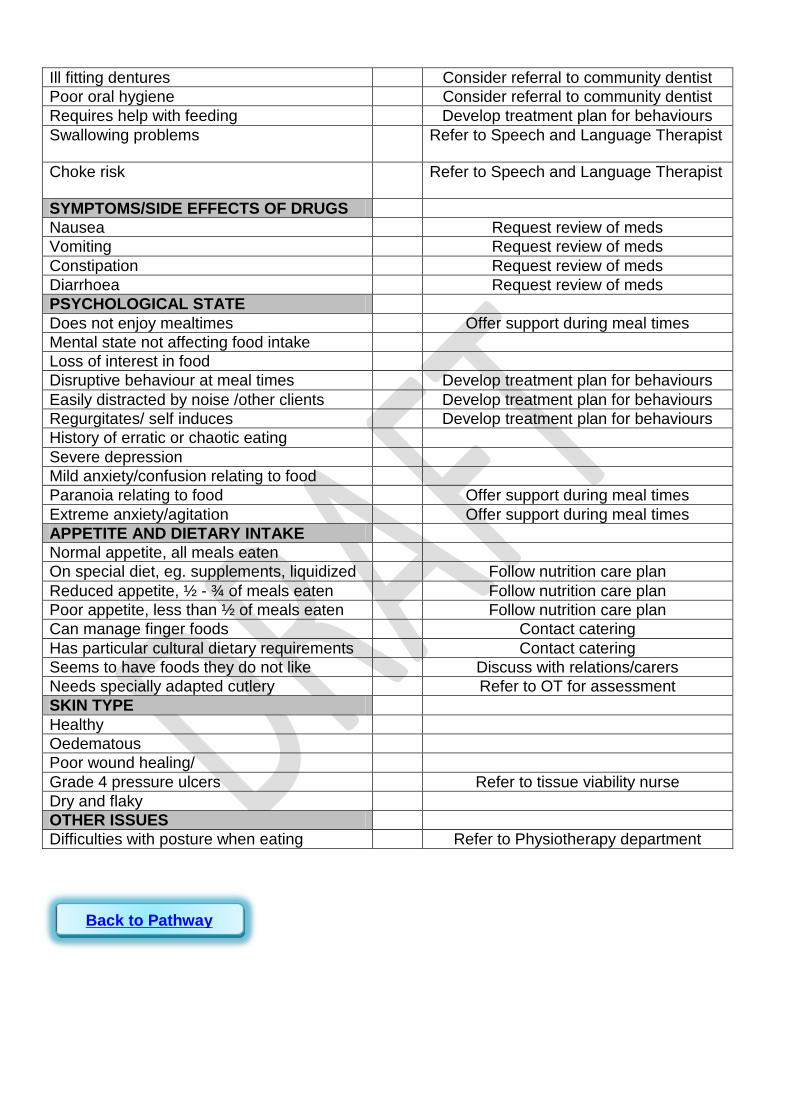
Ill fitting dentures Consider referral to community dentist
Poor oral hygiene Consider referral to community dentist
Requires help with feeding Develop treatment plan for behaviours
Swallowing problems Refer to Speech and Language Therapist
Choke risk Refer to Speech and Language Therapist
SYMPTOMS/SIDE EFFECTS OF DRUGS
Nausea Request review of meds
Vomiting Request review of meds
Constipation Request review of meds
Diarrhoea Request review of meds
PSYCHOLOGICAL STATE
Does not enjoy mealtimes Offer support during meal times
Mental state not affecting food intake
Loss of interest in food
Disruptive behaviour at meal times Develop treatment plan for behaviours
Easily distracted by noise /other clients Develop treatment plan for behaviours
Regurgitates/ self induces Develop treatment plan for behaviours
History of erratic or chaotic eating
Severe depression
Mild anxiety/confusion relating to food
Paranoia relating to food Offer support during meal times
Extreme anxiety/agitation Offer support during meal times
APPETITE AND DIETARY INTAKE
Normal appetite, all meals eaten
On special diet, eg. supplements, liquidized Follow nutrition care plan
Reduced appetite, ½ - ¾ of meals eaten Follow nutrition care plan
Poor appetite, less than ½ of meals eaten Follow nutrition care plan
Can manage finger foods Contact catering
Has particular cultural dietary requirements Contact catering
Seems to have foods they do not like Discuss with relations/carers
Needs specially adapted cutlery Refer to OT for assessment
SKIN TYPE
Healthy
Oedematous
Poor wound healing/
Grade 4 pressure ulcers Refer to tissue viability nurse
Dry and flaky
OTHER ISSUES
Difficulties with posture when eating Refer to Physiotherapy department
Back to Pathway
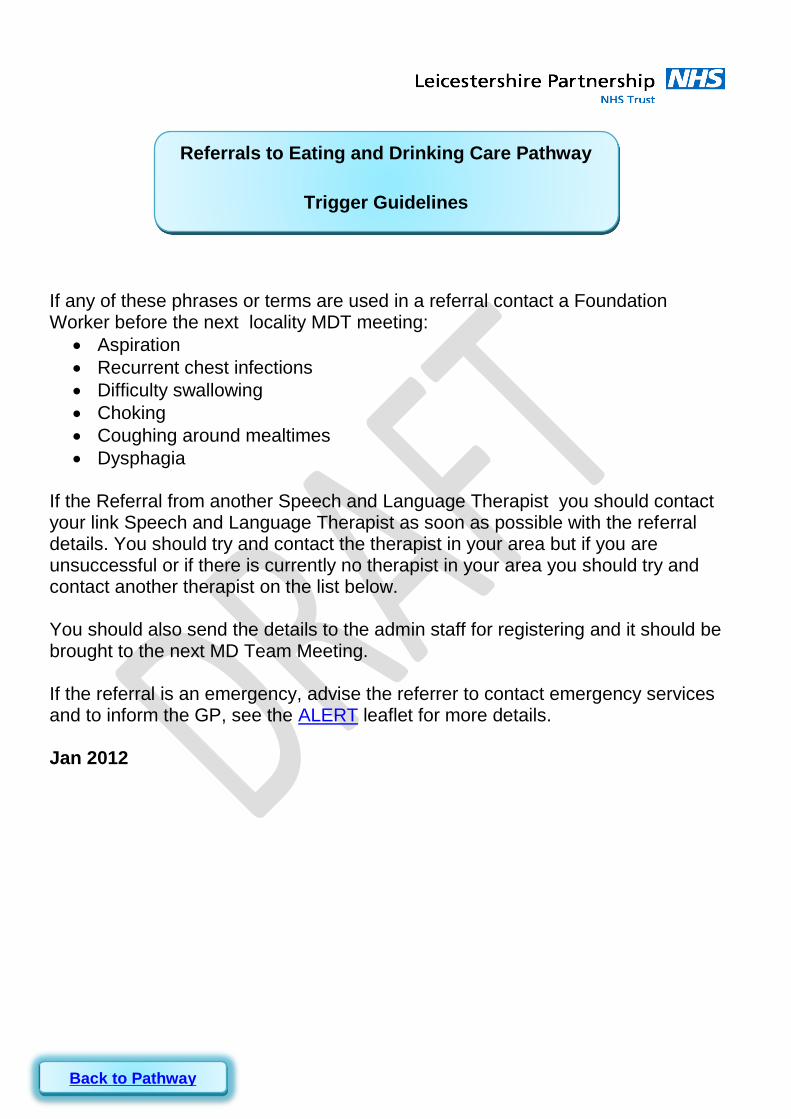
If any of these phrases or terms are used in a referral contact a Foundation Worker before the next locality MDT meeting:
Aspiration
Recurrent chest infections
Difficulty swallowing
Choking
Coughing around mealtimes
Dysphagia If the Referral from another Speech and Language Therapist you should contact your link Speech and Language Therapist as soon as possible with the referral details. You should try and contact the therapist in your area but if you are unsuccessful or if there is currently no therapist in your area you should try and contact another therapist on the list below. You should also send the details to the admin staff for registering and it should be brought to the next MD Team Meeting. If the referral is an emergency, advise the referrer to contact emergency services and to inform the GP, see the ALERT leaflet for more details. Jan 2012
Referrals to Eating and Drinking Care Pathway
Trigger Guidelines
Back to Pathway
There may be many contributory diagnoses for a person with
learning disability.
The most frequently used ICD10 codes are:
R13
Dysphagia
ICD10 Codes
Back to Pathway
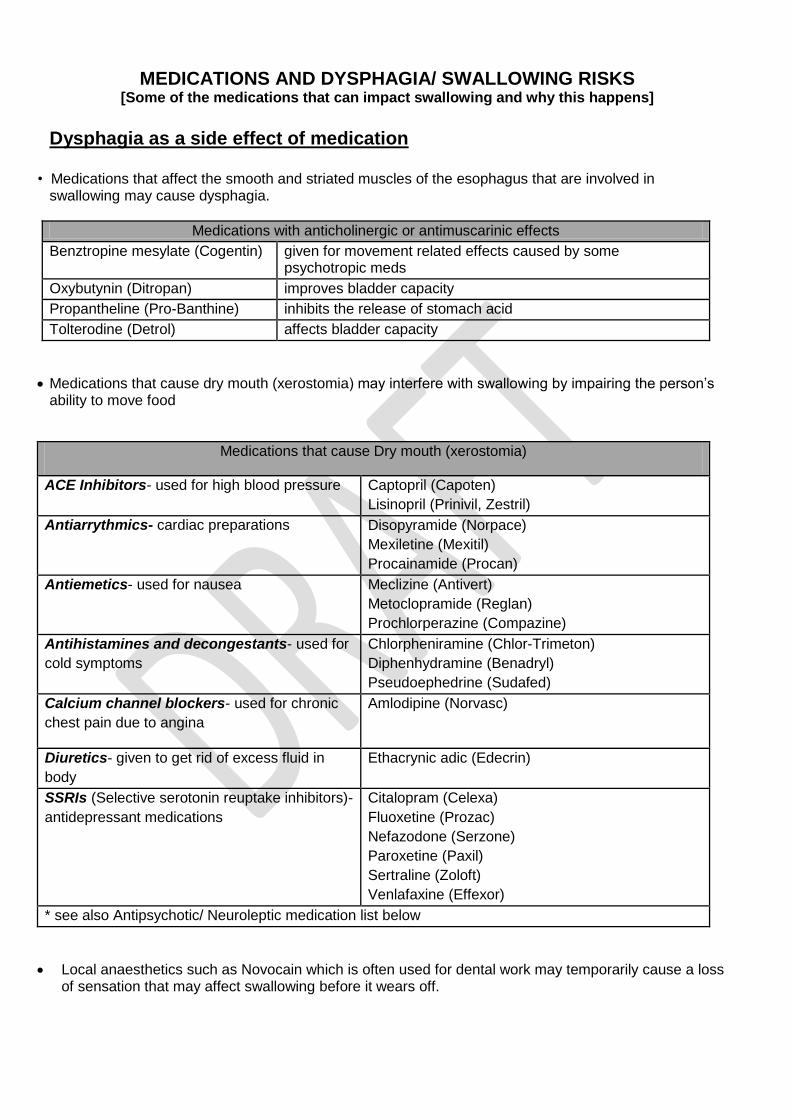
MEDICATIONS AND DYSPHAGIA/ SWALLOWING RISKS [Some of the medications that can impact swallowing and why this happens]
Dysphagia as a side effect of medication
• Medications that affect the smooth and striated muscles of the esophagus that are involved in swallowing may cause dysphagia.
Medications with anticholinergic or antimuscarinic effects
Benztropine mesylate (Cogentin) given for movement related effects caused by some psychotropic meds
Oxybutynin (Ditropan) improves bladder capacity
Propantheline (Pro-Banthine) inhibits the release of stomach acid
Tolterodine (Detrol) affects bladder capacity
Medications that cause dry mouth (xerostomia) may interfere with swallowing by impairing the person’s ability to move food
Medications that cause Dry mouth (xerostomia)
ACE Inhibitors- used for high blood pressure Captopril (Capoten)
Lisinopril (Prinivil, Zestril)
Antiarrythmics- cardiac preparations Disopyramide (Norpace)
Mexiletine (Mexitil)
Procainamide (Procan)
Antiemetics- used for nausea Meclizine (Antivert)
Metoclopramide (Reglan)
Prochlorperazine (Compazine)
Antihistamines and decongestants- used for
cold symptoms
Chlorpheniramine (Chlor-Trimeton)
Diphenhydramine (Benadryl)
Pseudoephedrine (Sudafed)
Calcium channel blockers- used for chronic
chest pain due to angina
Amlodipine (Norvasc)
Diuretics- given to get rid of excess fluid in
body
Ethacrynic adic (Edecrin)
SSRIs (Selective serotonin reuptake inhibitors)-
antidepressant medications
Citalopram (Celexa)
Fluoxetine (Prozac)
Nefazodone (Serzone)
Paroxetine (Paxil)
Sertraline (Zoloft)
Venlafaxine (Effexor)
* see also Antipsychotic/ Neuroleptic medication list below
Local anaesthetics such as Novocain which is often used for dental work may temporarily cause a loss of sensation that may affect swallowing before it wears off.
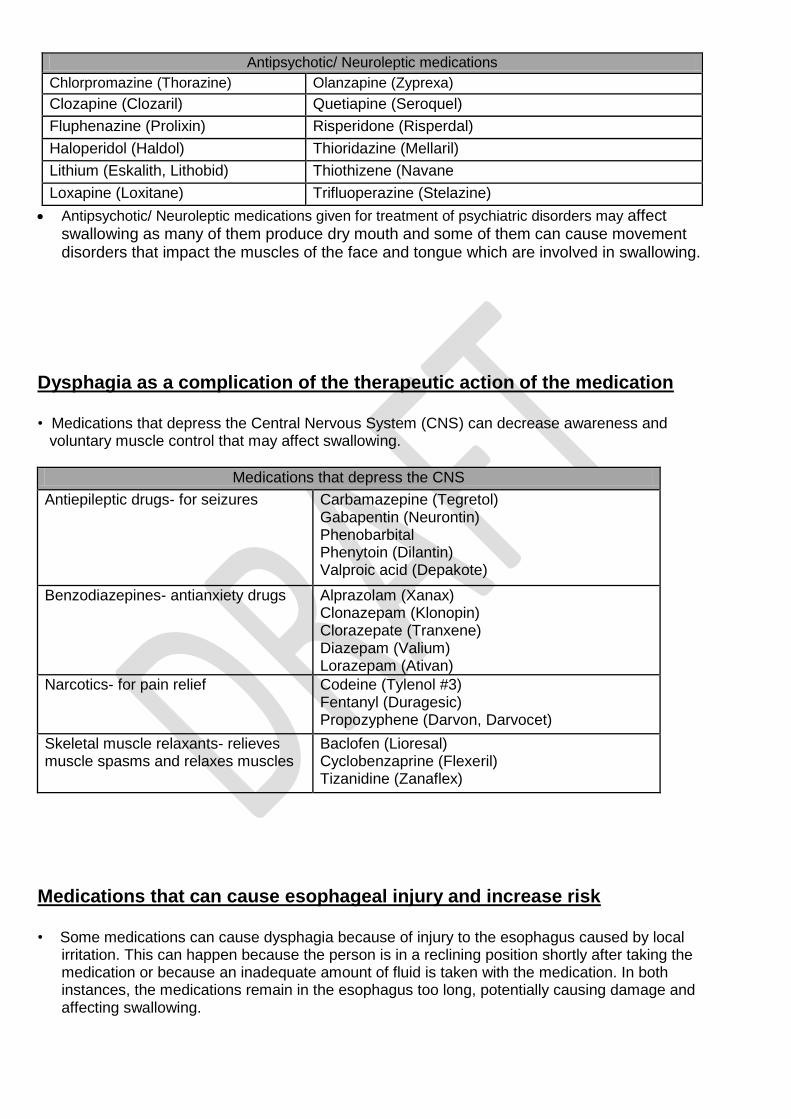
Antipsychotic/ Neuroleptic medications given for treatment of psychiatric disorders may affect swallowing as many of them produce dry mouth and some of them can cause movement disorders that impact the muscles of the face and tongue which are involved in swallowing.
Dysphagia as a complication of the therapeutic action of the medication
• Medications that depress the Central Nervous System (CNS) can decrease awareness and voluntary muscle control that may affect swallowing.
Medications that depress the CNS
Antiepileptic drugs- for seizures Carbamazepine (Tegretol) Gabapentin (Neurontin) Phenobarbital Phenytoin (Dilantin) Valproic acid (Depakote)
Benzodiazepines- antianxiety drugs Alprazolam (Xanax) Clonazepam (Klonopin) Clorazepate (Tranxene) Diazepam (Valium) Lorazepam (Ativan)
Narcotics- for pain relief Codeine (Tylenol #3) Fentanyl (Duragesic) Propozyphene (Darvon, Darvocet)
Skeletal muscle relaxants- relieves muscle spasms and relaxes muscles
Baclofen (Lioresal) Cyclobenzaprine (Flexeril) Tizanidine (Zanaflex)
Medications that can cause esophageal injury and increase risk
• Some medications can cause dysphagia because of injury to the esophagus caused by local irritation. This can happen because the person is in a reclining position shortly after taking the medication or because an inadequate amount of fluid is taken with the medication. In both instances, the medications remain in the esophagus too long, potentially causing damage and affecting swallowing.
Antipsychotic/ Neuroleptic medications
Chlorpromazine (Thorazine) Olanzapine (Zyprexa)
Clozapine (Clozaril) Quetiapine (Seroquel)
Fluphenazine (Prolixin) Risperidone (Risperdal)
Haloperidol (Haldol) Thioridazine (Mellaril)
Lithium (Eskalith, Lithobid) Thiothizene (Navane
Loxapine (Loxitane) Trifluoperazine (Stelazine)
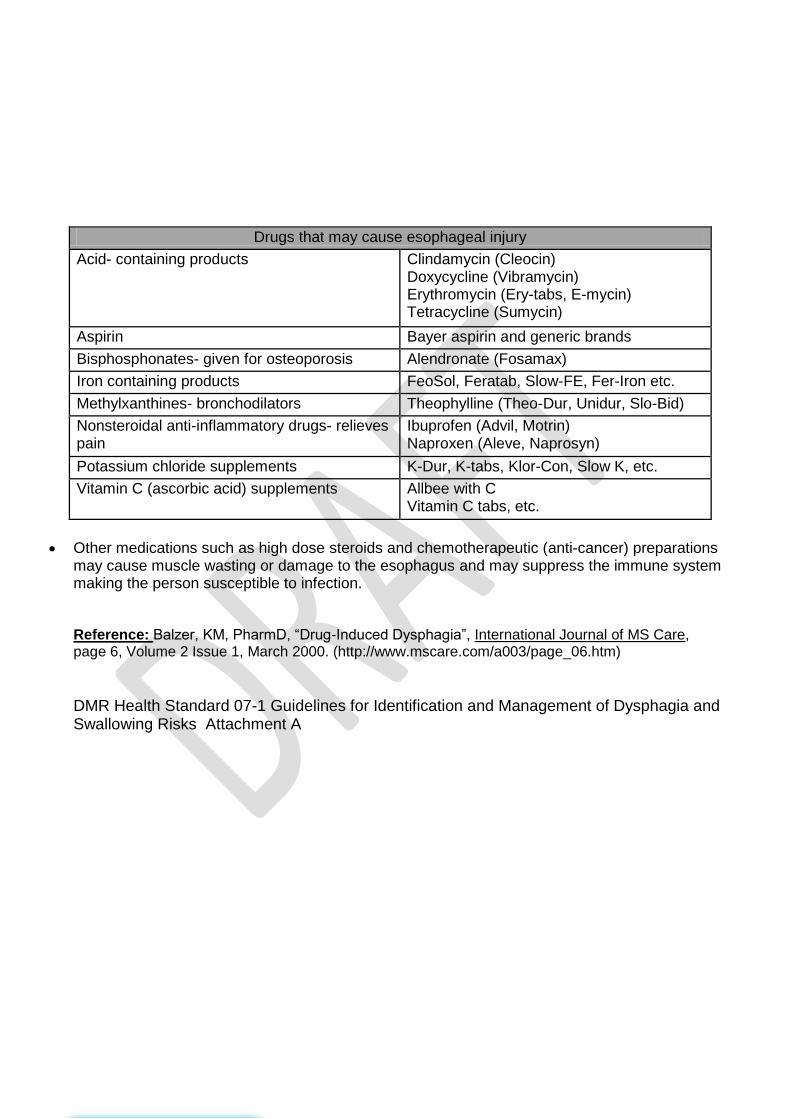
Other medications such as high dose steroids and chemotherapeutic (anti-cancer) preparations
may cause muscle wasting or damage to the esophagus and may suppress the immune system making the person susceptible to infection. Reference: Balzer, KM, PharmD, “Drug-Induced Dysphagia”, International Journal of MS Care, page 6, Volume 2 Issue 1, March 2000. (http://www.mscare.com/a003/page_06.htm) DMR Health Standard 07-1 Guidelines for Identification and Management of Dysphagia and Swallowing Risks Attachment A
Drugs that may cause esophageal injury
Acid- containing products Clindamycin (Cleocin) Doxycycline (Vibramycin) Erythromycin (Ery-tabs, E-mycin) Tetracycline (Sumycin)
Aspirin Bayer aspirin and generic brands
Bisphosphonates- given for osteoporosis Alendronate (Fosamax)
Iron containing products FeoSol, Feratab, Slow-FE, Fer-Iron etc.
Methylxanthines- bronchodilators Theophylline (Theo-Dur, Unidur, Slo-Bid)
Nonsteroidal anti-inflammatory drugs- relieves pain
Ibuprofen (Advil, Motrin) Naproxen (Aleve, Naprosyn)
Potassium chloride supplements K-Dur, K-tabs, Klor-Con, Slow K, etc.
Vitamin C (ascorbic acid) supplements Allbee with C Vitamin C tabs, etc.

When an individual is referred to the Eating and Drinking Care
Pathway, a trained Foundation Worker will contact the person
or carers to arrange to carry out a Screening Assessment.
The Foundation Worker will leave Initial Assessment
recommendations at the first visit and then report back findings
from the assessment to the Locality LD team for further in depth
discussion
Screening Assessment Outcomes
Screening Assessment
If there are no further actions
needed after the screening
assessment, a discharge letter
is sent from the Locality LD
team
Further action needed after
screening will result in referral
on to the appropriate
professional member of the
Locality LD team for specialist
assessment
Back to Pathway
Skills and Competency
Framework
Interdisciplinary Dysphagia Competence Framework
(2009) Embed J2 here prob as externl link
Training for competencies
Awareness (Under development)
Carers
Foundation Worker
Specialist
Consultant
The consultant is required to carry out complex case work and
advanced assessments. If FEES and Videofluoroscopy are available
the consultant should be able to implement an assessment if
appropriate ( see competences from RCSLT).
The consultant also progresses work at a strategic level and work with
other services.
Currently there are no clear courses, although Manchester Metropolitan
University does offer an Advanced Dypshagia practitioner level course.
Back to Pathway
Foundation Workers are trained according to the Interdisciplinary
Dysphagia Competencies
Foundation Worker Training
Foundation workers receive an initial days training
This training takes one day. In the morning, presentations
are received from each of the different members of the
ALD team on their role in the E&D care pathway
FW’s receive annual updates which focus upon
Refreshing of process and theory
Updating on new process and new theory
Peer support and feeding back into the pathway
New issue information
2011 Focus on supplements in diets
2012 Focus on role of FW and choke reporting

Each professional is specialist in their own field
This is the point where each professional is specialist in their own field. For instance the OT would not be expected to do a specialist dysphagia (swallowing) assessment but would be the appropriate specialist professional for recommending the independence support for safe eating and drinking. Only the SLT would have specialist swallowing assessment skills. Each other professional has their specialist skill (see ‘Roles’ in the SEAD Pathway) Specialist swallowing skills are acquired locally by a qualified speech and language therapist who has attended and passed a Post graduate training course, having had some years experience. DMU provide a week-long course which includes a six-month period of mentoring and is fully assessed by the university through assignments.
Back to Pathway
Specialist Dysphagia Workers
Back to Pathway
Screening Assessment Tools may
Include
Case History Mealtime Observation
Protocol Guidelines MUST Screening Tool
Food Diary Cough Recording Chart
Choke Recording Forms List of medications that
may affect swallowing
DIS DAT Other Useful Leaflets
Capacity Assessment Consent form (from NPSA 2007)
Best Interest Documents Morgan Risk Assessment
Back to Pathway
Community Team for People with Learning Disabilities Mansion House, Leicester Frith Hospital, Groby Road, Leicester, LE3 9QF Tel: 0116 225 5200 Fax: 0116 225 5202
Eating and Drinking Case History Name: Preferred Name:
D.O.B. NHS Number:
Refer to core information: Health and social needs section and the HONOS section. Clients concerns about their eating and drinking
Carers main concerns around eating and drinking Name of carer:
Consent: Consent gained: Yes No (how was consent gained? If not, why?)
Refer to Core Information: Social Circumstances section for Weekly schedule and names of specific support workers ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………………
Please place client / service user label
here
Client Name: DOB: NHS Number:

Weight and appetite
1 Current weight without shoes:
2 BMI if known (Body Mass Index):
3 Has the MUST screening tool been completed with the client?
Yes/No/Don’t Know.
4 Has there been any unplanned weight loss in the last 6 months? If yes, how much?
Yes/No/Don’t Know.
Action: Refer to Dietician if unplanned weight loss of more than 5%
5 Has the person gained weight? If yes…
Yes/No/Don’t know.
Is the person’s weight gain affecting physical or mental health? Yes/No/Don’t Know.
Please give details: - Are there any known causes for weight gain?
Yes/No/Don’t know.
Please give details:-
Action: Refer to Community Nurse/ and/or Dietician if there are concerns
6. Have there been any changes to the person’s appetite, level of alertness or stamina during eating/drinking?
Yes/No/Don’t Know.
Please give details: -
Action: If yes, go to GP for blood tests and/or ask for a medication review
Client Name: DOB: NHS Number:
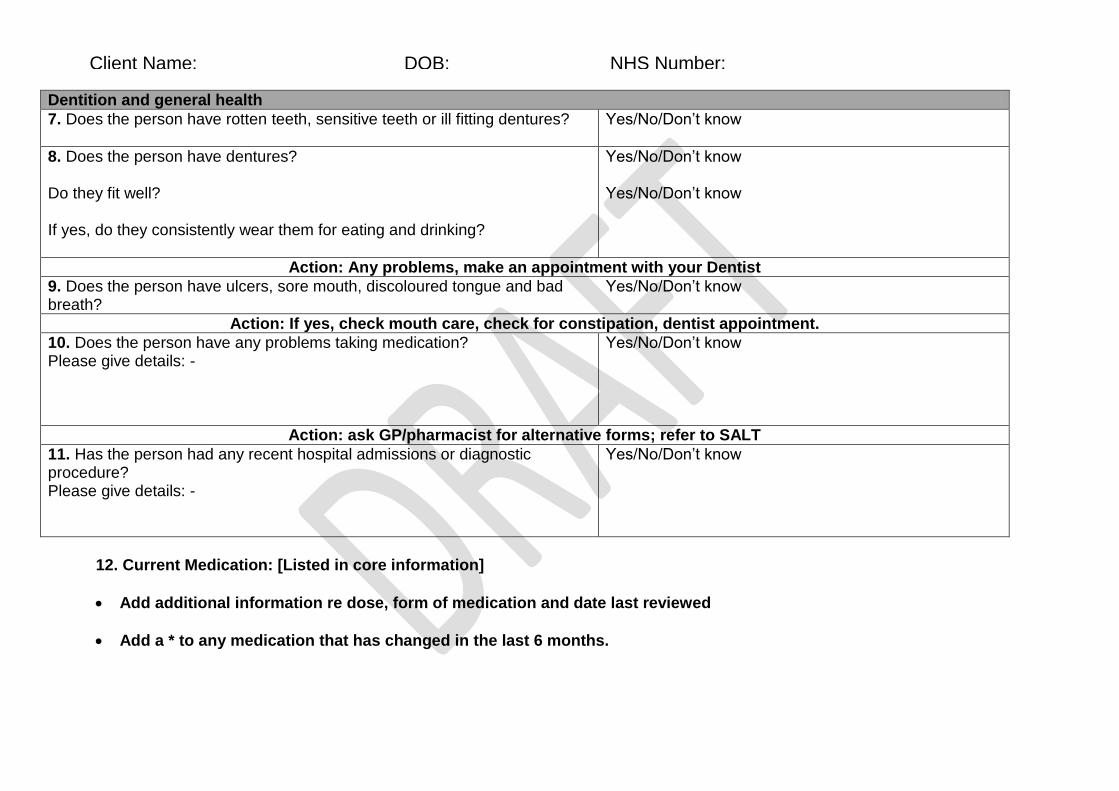
Dentition and general health
7. Does the person have rotten teeth, sensitive teeth or ill fitting dentures?
Yes/No/Don’t know
8. Does the person have dentures? Do they fit well? If yes, do they consistently wear them for eating and drinking?
Yes/No/Don’t know Yes/No/Don’t know
Action: Any problems, make an appointment with your Dentist
9. Does the person have ulcers, sore mouth, discoloured tongue and bad breath?
Yes/No/Don’t know
Action: If yes, check mouth care, check for constipation, dentist appointment.
10. Does the person have any problems taking medication? Please give details: -
Yes/No/Don’t know
Action: ask GP/pharmacist for alternative forms; refer to SALT
11. Has the person had any recent hospital admissions or diagnostic procedure? Please give details: -
Yes/No/Don’t know
12. Current Medication: [Listed in core information]
Add additional information re dose, form of medication and date last reviewed
Add a * to any medication that has changed in the last 6 months.
Client Name: DOB: NHS Number:
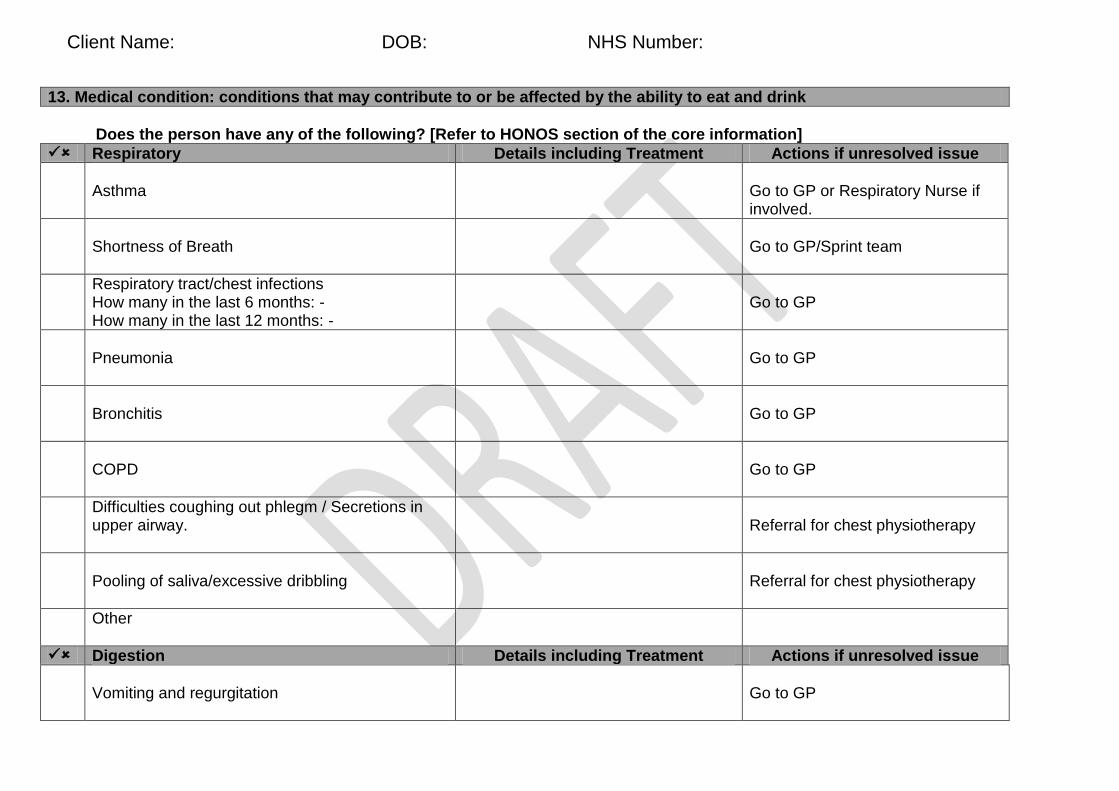
13. Medical condition: conditions that may contribute to or be affected by the ability to eat and drink
Does the person have any of the following? [Refer to HONOS section of the core information]
Respiratory Details including Treatment Actions if unresolved issue
Asthma
Go to GP or Respiratory Nurse if involved.
Shortness of Breath
Go to GP/Sprint team
Respiratory tract/chest infections How many in the last 6 months: - How many in the last 12 months: -
Go to GP
Pneumonia
Go to GP
Bronchitis
Go to GP
COPD
Go to GP
Difficulties coughing out phlegm / Secretions in upper airway.
Referral for chest physiotherapy
Pooling of saliva/excessive dribbling
Referral for chest physiotherapy
Other
Digestion Details including Treatment Actions if unresolved issue
Vomiting and regurgitation
Go to GP
Client Name: DOB: NHS Number:
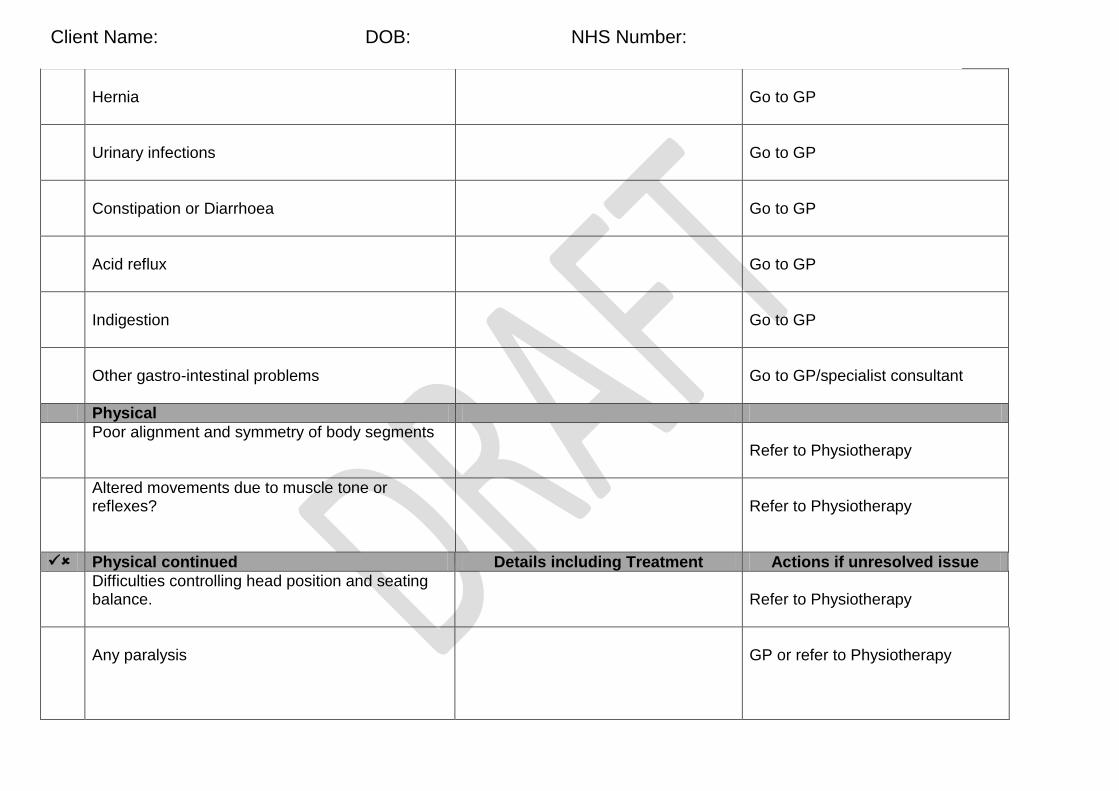
Hernia
Go to GP
Urinary infections
Go to GP
Constipation or Diarrhoea
Go to GP
Acid reflux
Go to GP
Indigestion
Go to GP
Other gastro-intestinal problems
Go to GP/specialist consultant
Physical
Poor alignment and symmetry of body segments
Refer to Physiotherapy
Altered movements due to muscle tone or reflexes?
Refer to Physiotherapy
Physical continued Details including Treatment Actions if unresolved issue
Difficulties controlling head position and seating balance.
Refer to Physiotherapy
Any paralysis
GP or refer to Physiotherapy
Client Name: DOB: NHS Number:
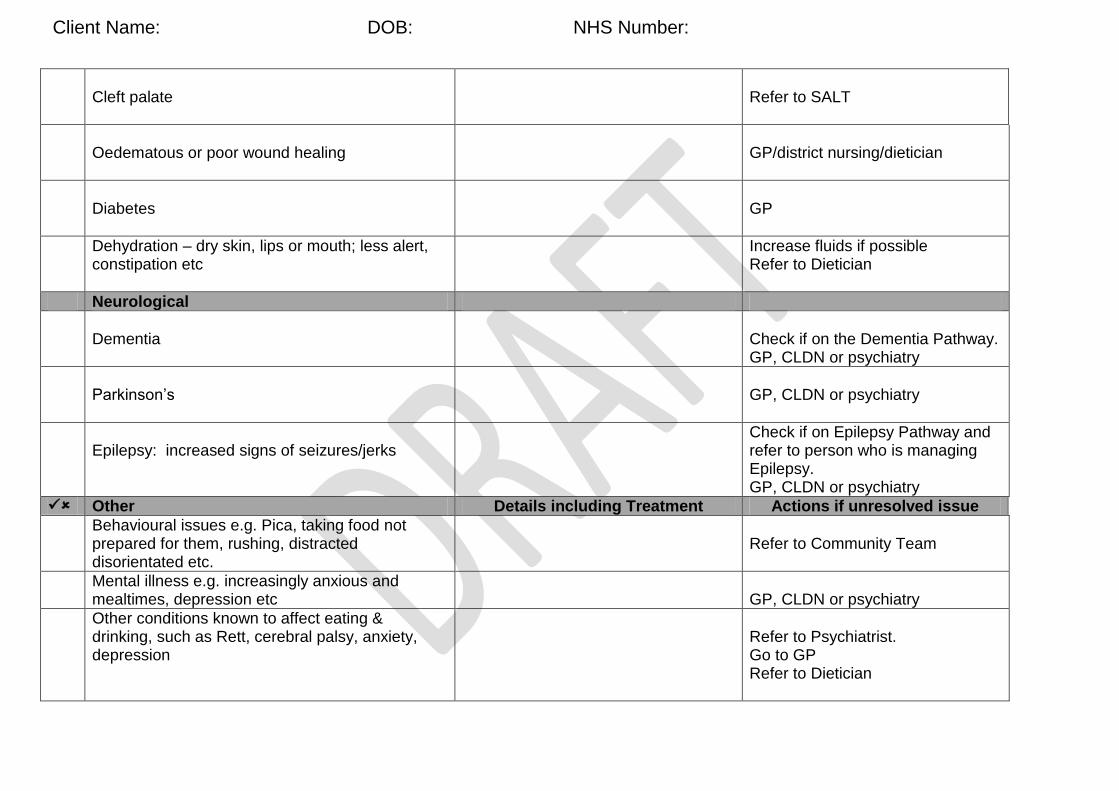
Cleft palate
Refer to SALT
Oedematous or poor wound healing
GP/district nursing/dietician
Diabetes
GP
Dehydration – dry skin, lips or mouth; less alert, constipation etc
Increase fluids if possible Refer to Dietician
Neurological
Dementia
Check if on the Dementia Pathway. GP, CLDN or psychiatry
Parkinson’s
GP, CLDN or psychiatry
Epilepsy: increased signs of seizures/jerks
Check if on Epilepsy Pathway and refer to person who is managing Epilepsy. GP, CLDN or psychiatry
Other Details including Treatment Actions if unresolved issue
Behavioural issues e.g. Pica, taking food not prepared for them, rushing, distracted disorientated etc.
Refer to Community Team
Mental illness e.g. increasingly anxious and mealtimes, depression etc
GP, CLDN or psychiatry
Other conditions known to affect eating & drinking, such as Rett, cerebral palsy, anxiety, depression
Refer to Psychiatrist. Go to GP Refer to Dietician
Client Name: DOB: NHS Number:
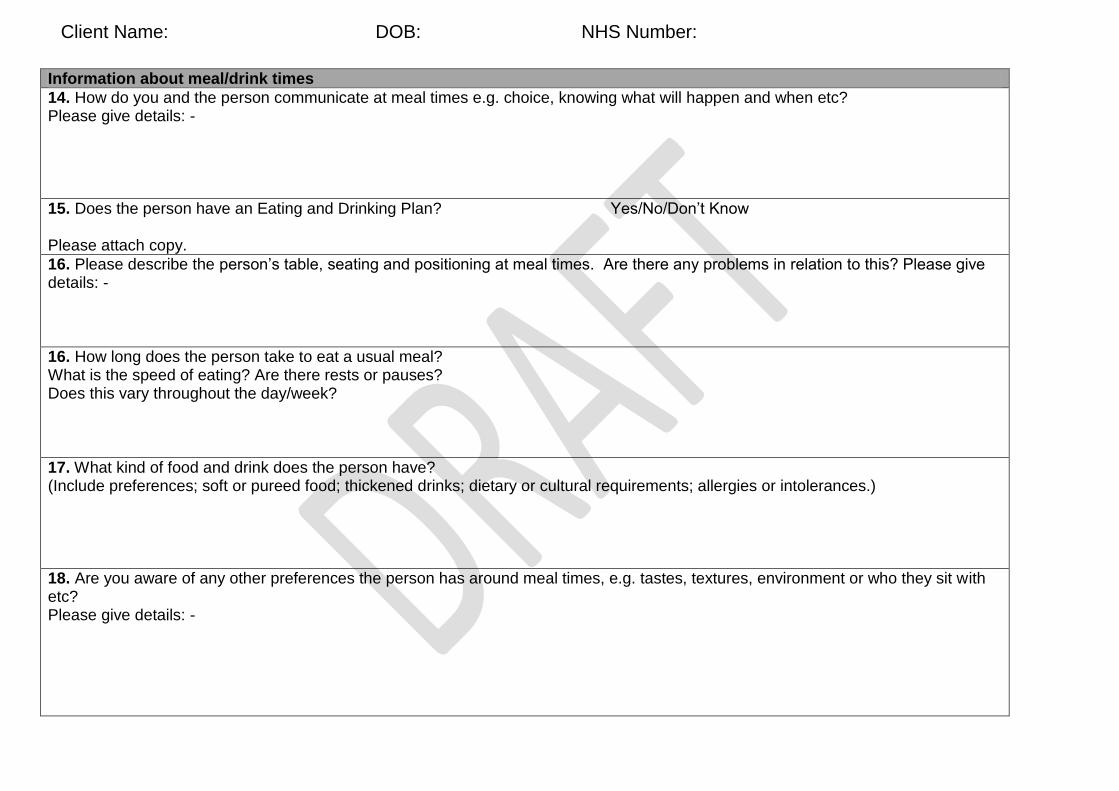
Information about meal/drink times
14. How do you and the person communicate at meal times e.g. choice, knowing what will happen and when etc? Please give details: -
15. Does the person have an Eating and Drinking Plan?
Please attach copy.
Yes/No/Don’t Know
16. Please describe the person’s table, seating and positioning at meal times. Are there any problems in relation to this? Please give details: -
16. How long does the person take to eat a usual meal? What is the speed of eating? Are there rests or pauses? Does this vary throughout the day/week?
17. What kind of food and drink does the person have? (Include preferences; soft or pureed food; thickened drinks; dietary or cultural requirements; allergies or intolerances.)
18. Are you aware of any other preferences the person has around meal times, e.g. tastes, textures, environment or who they sit with etc? Please give details: -
Client Name: DOB: NHS Number:

19. Is the person able to get their food to their mouth? What equipment is your client currently using? (e.g. plates, cutlery, cups, mats, individualised furniture etc) Do they overfill their mouth? Have there been any changes in skill level in relation to this?
22. Who regularly supports the person and manager details, if relevant? What is the usual staff:client ratio at a meal and time allowed for meal?
23. Where does the person currently go to have their meals? – note on timetable in core information if relevant.
24. Do you regularly see any of the following … food or drink comes out of his/her nose or mouth during eating and drinking food or tablets become stuck on the roof of their mouth, teeth or gums after or during eating? If so,
please describe where the food sticks and how you and/or the person frees up the food the person has difficulty chewing? the person has tears, effort to swallow, reddening face, wheezy/gurgling sound or coughing shortly after eating food or
drinking?
25. Has the person choked recently (e.g. within the last month). If yes please give details. (Has a choking incident form been completed? Do you need to complete an e-irf?)
Client Name: DOB: NHS Number:
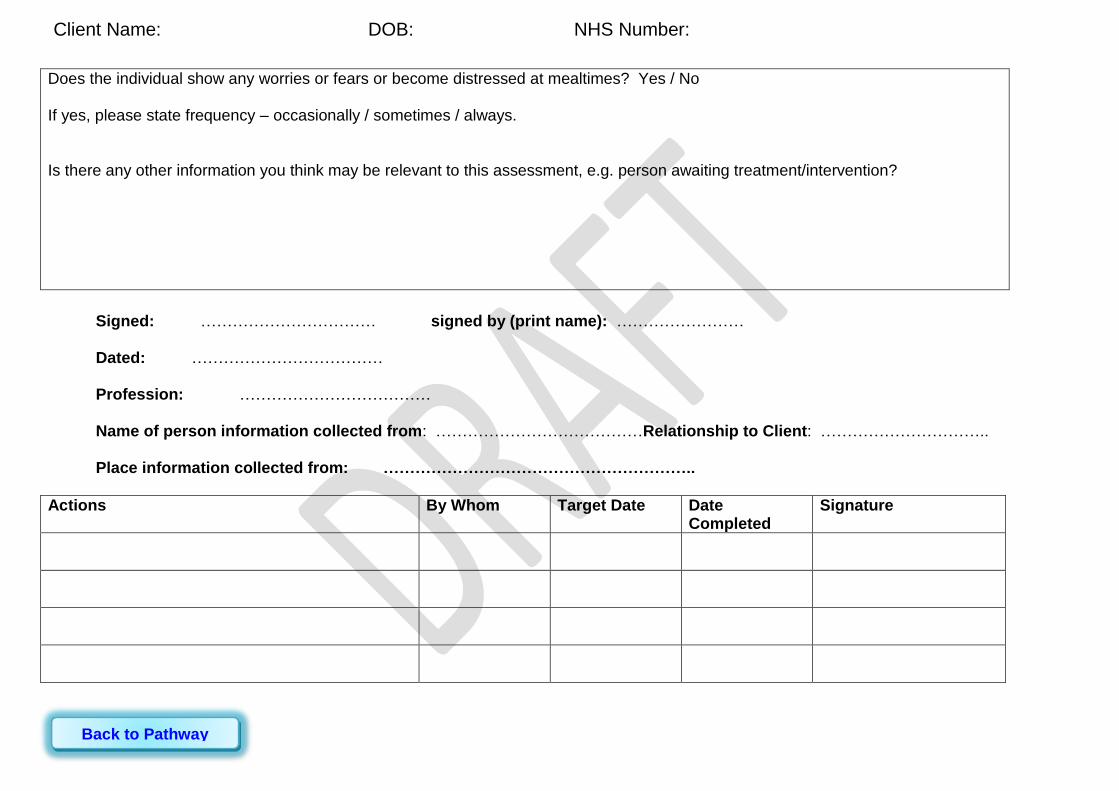
Does the individual show any worries or fears or become distressed at mealtimes? Yes / No If yes, please state frequency – occasionally / sometimes / always. Is there any other information you think may be relevant to this assessment, e.g. person awaiting treatment/intervention?
Signed: …………………………… signed by (print name): …………………… Dated: ……………………………… Profession: ……………………………… Name of person information collected from: …………………………………Relationship to Client: ………………………….. Place information collected from: …………………………………………………..
Actions By Whom Target Date Date Completed
Signature
Client Name: DOB: NHS Number:
Back to Pathway

Eating and Drinking
Initial Observation
Name: D.O.B.:
NHS Number: Date:
Place of Observation:
Consent: Consent gained: Yes No (if not, why, how was consent gained)
Activity Comments
Type of Food/Meal
Type of Drink
Amount of food/drink eaten:
Environment
Equipment used
Mobility/Seating and Positioning
Ability/Skill level to feed self, including speed
of eating
Please place client / service user label
here
Name: DOB: NHS Number:
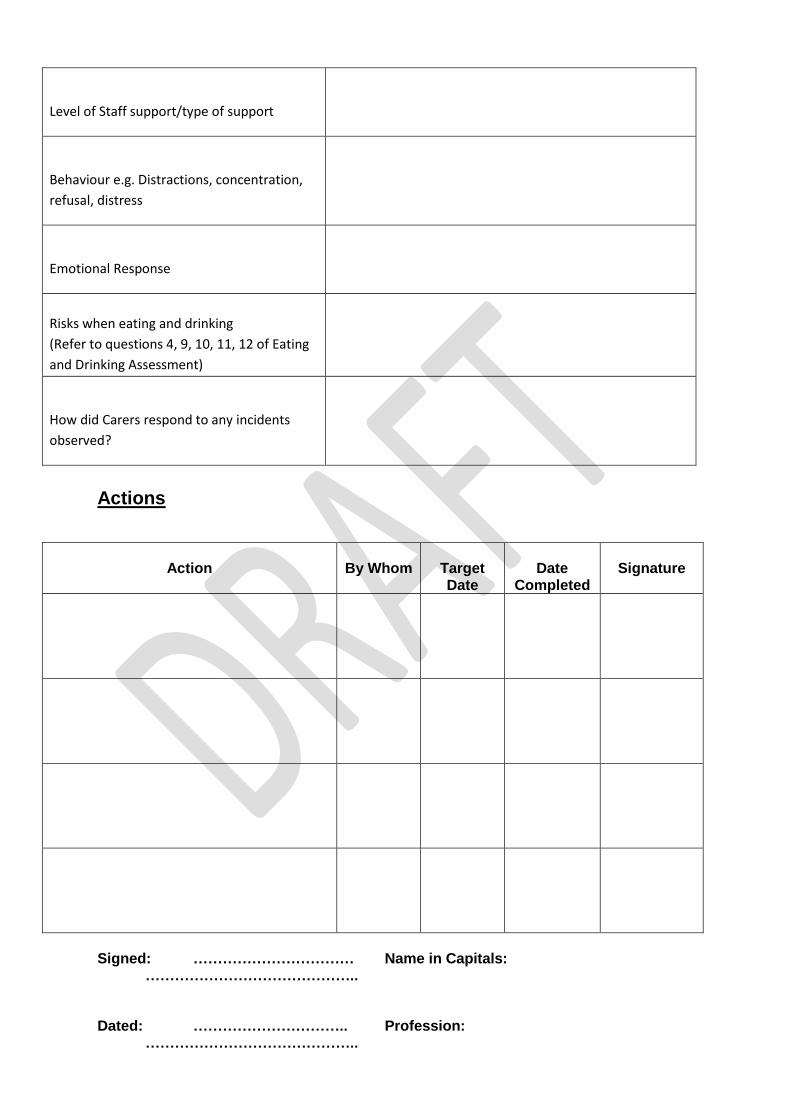
Level of Staff support/type of support
Behaviour e.g. Distractions, concentration,
refusal, distress
Emotional Response
Risks when eating and drinking
(Refer to questions 4, 9, 10, 11, 12 of Eating
and Drinking Assessment)
How did Carers respond to any incidents
observed?
Actions
Action
By Whom
Target Date
Date
Completed
Signature
Signed: …………………………… Name in Capitals: …………………………………….. Dated: ………………………….. Profession: ……………………………………..
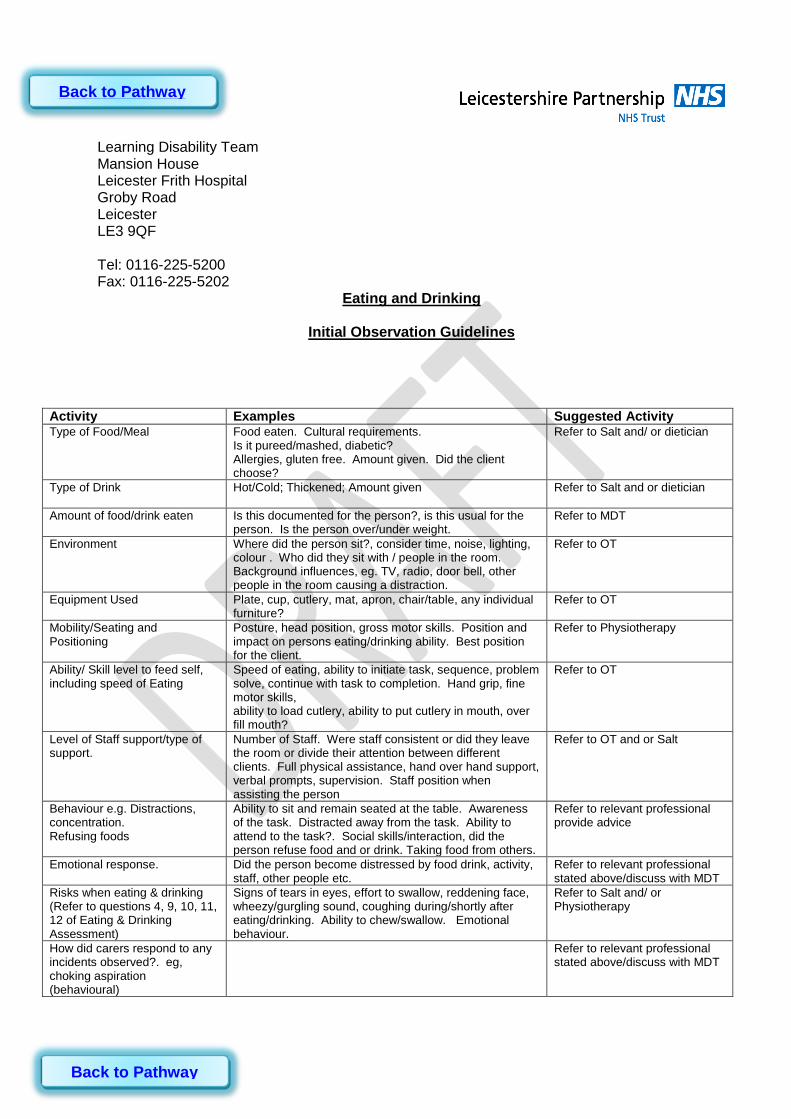
Learning Disability Team Mansion House Leicester Frith Hospital Groby Road Leicester LE3 9QF Tel: 0116-225-5200 Fax: 0116-225-5202
Eating and Drinking
Initial Observation Guidelines
Activity Examples Suggested Activity Type of Food/Meal Food eaten. Cultural requirements.
Is it pureed/mashed, diabetic? Allergies, gluten free. Amount given. Did the client choose?
Refer to Salt and/ or dietician
Type of Drink Hot/Cold; Thickened; Amount given
Refer to Salt and or dietician
Amount of food/drink eaten Is this documented for the person?, is this usual for the person. Is the person over/under weight.
Refer to MDT
Environment Where did the person sit?, consider time, noise, lighting, colour . Who did they sit with / people in the room. Background influences, eg. TV, radio, door bell, other people in the room causing a distraction.
Refer to OT
Equipment Used Plate, cup, cutlery, mat, apron, chair/table, any individual furniture?
Refer to OT
Mobility/Seating and Positioning
Posture, head position, gross motor skills. Position and impact on persons eating/drinking ability. Best position for the client.
Refer to Physiotherapy
Ability/ Skill level to feed self, including speed of Eating
Speed of eating, ability to initiate task, sequence, problem solve, continue with task to completion. Hand grip, fine motor skills, ability to load cutlery, ability to put cutlery in mouth, over fill mouth?
Refer to OT
Level of Staff support/type of support.
Number of Staff. Were staff consistent or did they leave the room or divide their attention between different clients. Full physical assistance, hand over hand support, verbal prompts, supervision. Staff position when assisting the person
Refer to OT and or Salt
Behaviour e.g. Distractions, concentration. Refusing foods
Ability to sit and remain seated at the table. Awareness of the task. Distracted away from the task. Ability to attend to the task?. Social skills/interaction, did the person refuse food and or drink. Taking food from others.
Refer to relevant professional provide advice
Emotional response.
Did the person become distressed by food drink, activity, staff, other people etc.
Refer to relevant professional stated above/discuss with MDT
Risks when eating & drinking (Refer to questions 4, 9, 10, 11, 12 of Eating & Drinking Assessment)
Signs of tears in eyes, effort to swallow, reddening face, wheezy/gurgling sound, coughing during/shortly after eating/drinking. Ability to chew/swallow. Emotional behaviour.
Refer to Salt and/ or Physiotherapy
How did carers respond to any incidents observed?. eg, choking aspiration (behavioural)
Refer to relevant professional stated above/discuss with MDT
Back to Pathway
Back to Pathway
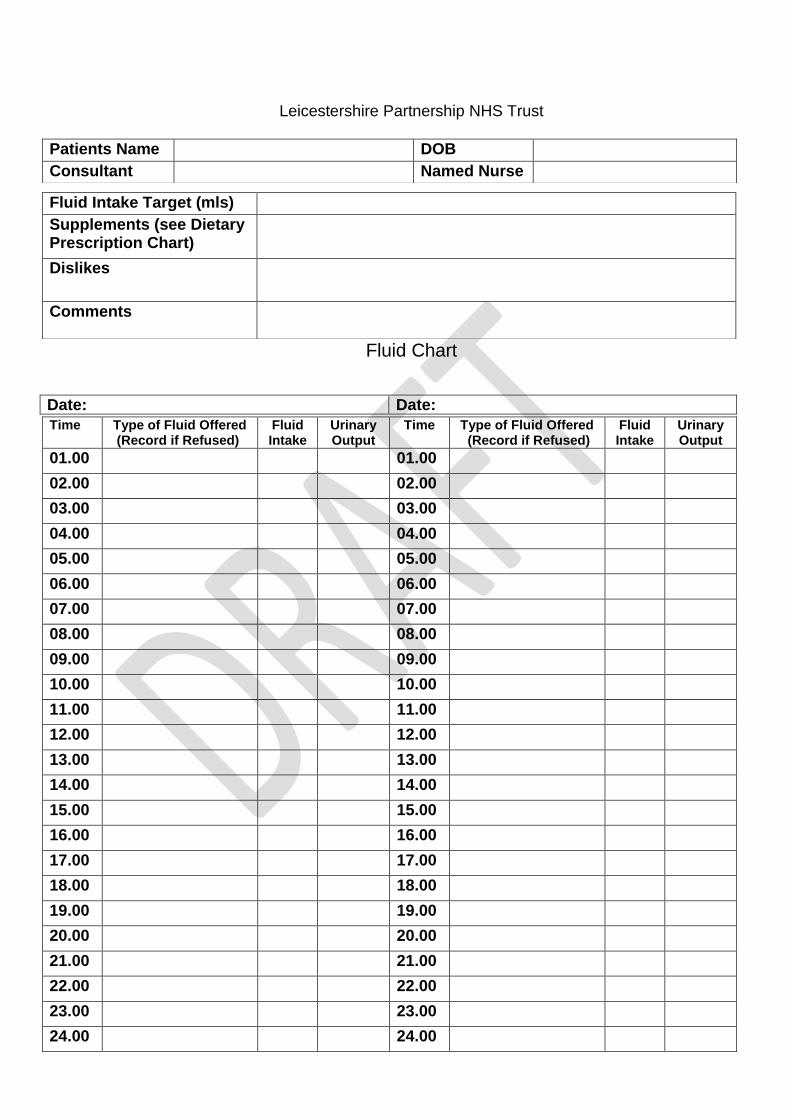
Leicestershire Partnership NHS Trust
Fluid Chart
Date: Date:
Patients Name DOB Consultant Named Nurse
Fluid Intake Target (mls) Supplements (see Dietary Prescription Chart)
Dislikes
Comments
Time Type of Fluid Offered (Record if Refused)
Fluid Intake
Urinary Output
Time Type of Fluid Offered (Record if Refused)
Fluid Intake
Urinary Output
01.00 01.00 02.00 02.00 03.00 03.00 04.00 04.00 05.00 05.00 06.00 06.00 07.00 07.00 08.00 08.00 09.00 09.00 10.00 10.00 11.00 11.00 12.00 12.00 13.00 13.00 14.00 14.00 15.00 15.00 16.00 16.00 17.00 17.00 18.00 18.00 19.00 19.00 20.00 20.00 21.00 21.00 22.00 22.00 23.00 23.00 24.00 24.00
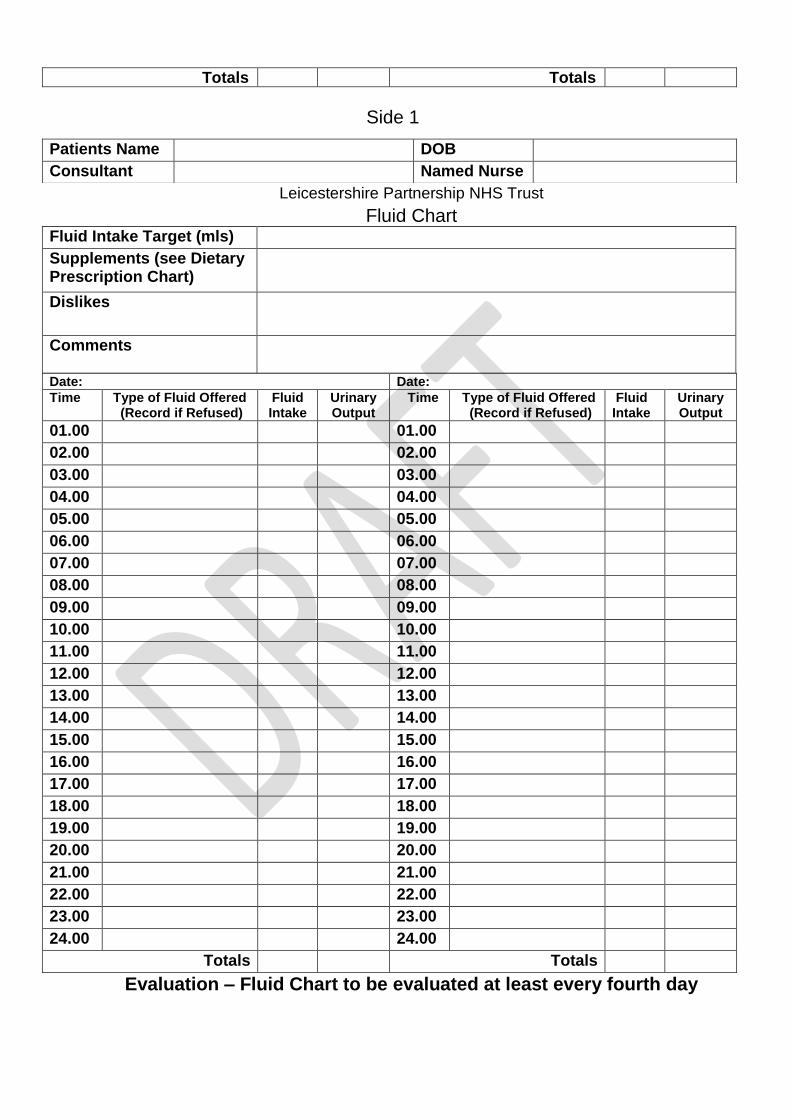
Totals Totals
Leicestershire Partnership NHS Trust
Fluid Chart
Evaluation – Fluid Chart to be evaluated at least every fourth day
Patients Name DOB Consultant Named Nurse
Fluid Intake Target (mls) Supplements (see Dietary Prescription Chart)
Dislikes
Comments
Date: Date:
Time Type of Fluid Offered (Record if Refused)
Fluid Intake
Urinary Output
Time Type of Fluid Offered (Record if Refused)
Fluid Intake
Urinary Output
01.00 01.00 02.00 02.00 03.00 03.00 04.00 04.00 05.00 05.00 06.00 06.00 07.00 07.00 08.00 08.00 09.00 09.00 10.00 10.00 11.00 11.00 12.00 12.00 13.00 13.00 14.00 14.00 15.00 15.00 16.00 16.00 17.00 17.00 18.00 18.00 19.00 19.00 20.00 20.00 21.00 21.00 22.00 22.00 23.00 23.00 24.00 24.00
Totals Totals
Side 1
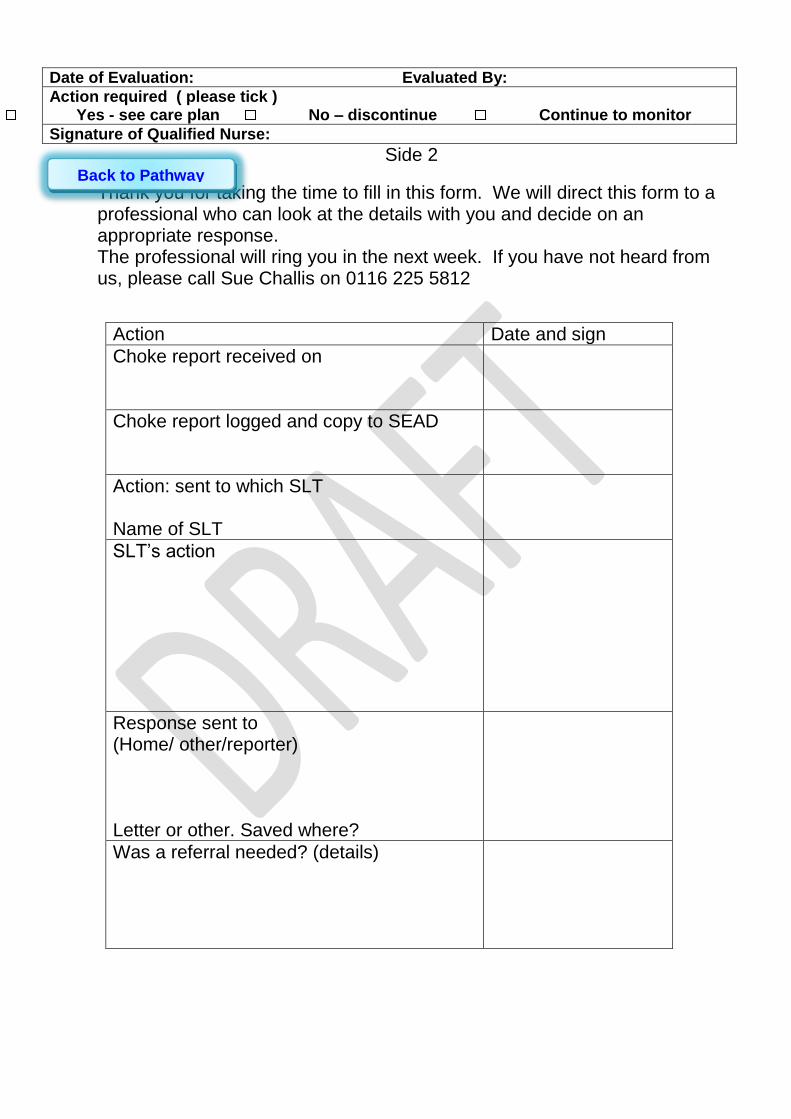
Date of Evaluation: Evaluated By:
Action required ( please tick ) Yes - see care plan No – discontinue Continue to monitor
Signature of Qualified Nurse:
Side 2
Thank you for taking the time to fill in this form. We will direct this form to a professional who can look at the details with you and decide on an appropriate response. The professional will ring you in the next week. If you have not heard from us, please call Sue Challis on 0116 225 5812
Action Date and sign
Choke report received on
Choke report logged and copy to SEAD
Action: sent to which SLT Name of SLT
SLT’s action
Response sent to (Home/ other/reporter) Letter or other. Saved where?
Was a referral needed? (details)
Back to Pathway
Back to Pathway
Other Useful Leaflets
Alert
Foods which give a high risk of choking
Supporting people who eat and drink too
fast
What is Dysphagia?
Supporting people with Dementia to eat
and drink
Back to Pathway

was visited today by to assess their eating and drinking. The following recommendations have been made. A full report and eating and drinking care plan will be produced shortly/This will be the final version
Initial Assessment recommendations for:
_____________________________________
NHS Number _________________ DOB __________
Current:
Actions / recommendations:
Drinks
Current:
Actions / recommendations:
Current:
Actions / recommendations:
Equipment
Current:
Actions / recommendations:
Assistance required
Current:
Actions / recommendations:
Position Things to look out for
Current:
Actions / recommendations:
Any problems please contact:
………………………………………………...
Telephone number:………………………….
Back to Pathway
Discharge is considered when
The individual is stable
Carers are confident and competent to carry out the Eating and Drinking Plan
Carers know how to review the Eating and Drinking Plan and know how and when to re-refer
When all these criteria are met, the individual is discharged and the information is relayed back to the GP and the Locality LD team
Discharge
Back to Pathway
Specialist Assessment
Who may be involved in Specialist
Assessment?
What may be included in Specialist
Assessment?
Back to Pathway

Individual
Knowledge of own likes, dislikes,
preferences, aspirations
(Person Centred Plan and
Health Action Plan)
Who may be involved in assessment?
Back to Pathway
Speech and Language Therapist
Assesses communication and
swallowing
Occupational Therapist
Assess functional skill level and
functional positioning in order to
maximise independence and
enable the individual’s skill level
within eating and drinking
Dietician
Assesses nutritional needs
Outreach Team
Assess significant behaviour
issues
Community LD Nurse
WAITING FOR INFO
Carer
Knowledge of the person and their likes
and dislikes, trialling treatment providing
direct support
Psychologist
LEADS TO BLANK
Health Facilitator
D19
Psychiatrist
Mental Health assessment if there are valid
concerns about conditions such as depression,
mania, psychosis, or and eating disorder that may
be impacting nutritional intake
Acute Liaison Nurse
Physiotherapist
Assesses positioning, posture and
management of secretions
The assessment will be person-centred
and tailored to individual needs and may include:
What may be included in
Specialist Assessment?
Direct Observation
Capacity
Sensory
Mental Health
Cognitive
Nutritional
Communication
Risk
Environmental
Case History
Psychological
Positioning
Physiological
Back to Pathway

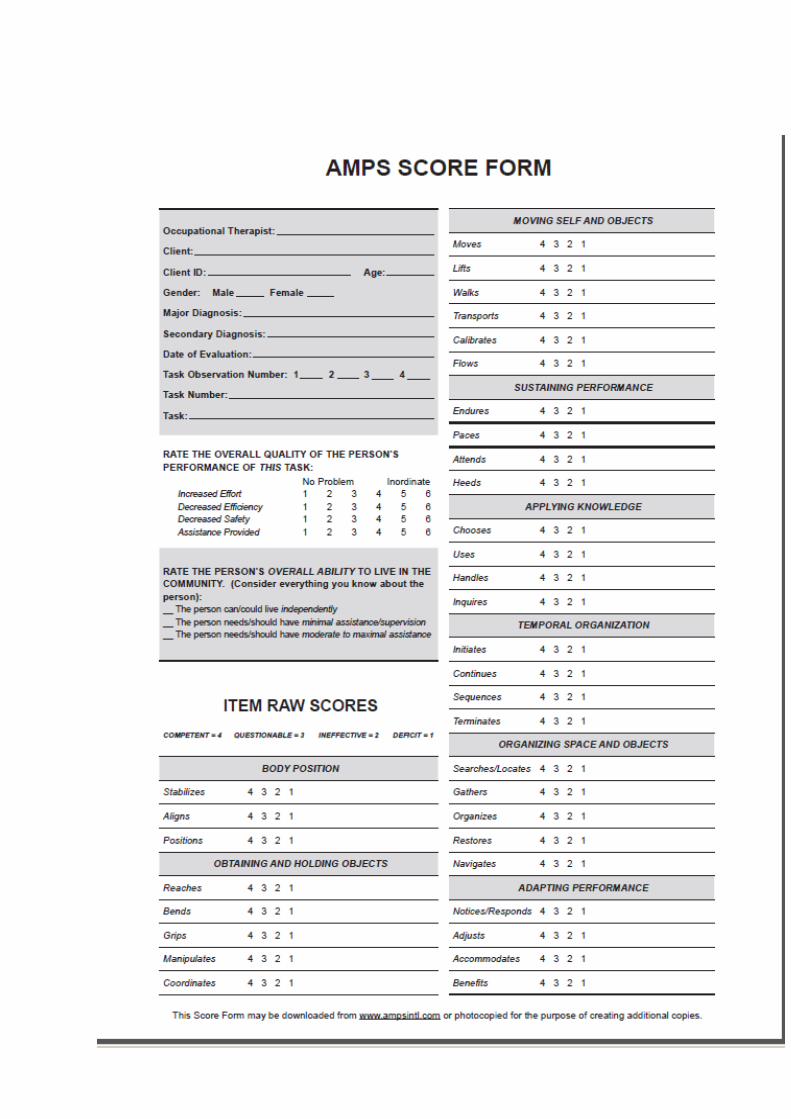
The Occupational Therapist considers the impact of physical, cognitive, perceptual, sensory and behavioural factors in the assessment and management of individuals with eating and drinking difficulties. This also reflects the environmental and social factors which affect the individual’s skills. This may involve:
Liaison with other professionals in the assessment of an individual’s positioning needs. This includes the use of appropriate seating and other physical supports to facilitate safe and effective eating and drinking.
Facilitation of independence through the use of adaptive equipment and education of individuals and their carer’s in appropriate feeding techniques, and the method and level of support required.
Assessment of individual’s cognitive and perceptual skills in relation to the task, such as understanding of sequence, orientation, problem solving and spatial awareness.
Assessing the impact of the individual’s behaviour, psychological and other social factors in order to promote safe and effective eating and drinking.
Assessment of individual’s sensory skills and needs.
The above are considered within the context of an individual’s environment with regards to the influences this has upon their skills and ability to function as independently as possible. Occupational Therapists will monitor and review recommendations made in line with the MDT Care Pathway. Some OTs are trained to have the required competency level for a Foundation Dysphagia Practitioner as part of the eating and drinking care pathway.
Eating and drinking OT assessment Eating and drinking OT assessment Sensory OT assessment 5c
Occupational Therapists Role in
Eating and Drinking
Back to Pathway

Occupational Therapist Assessment


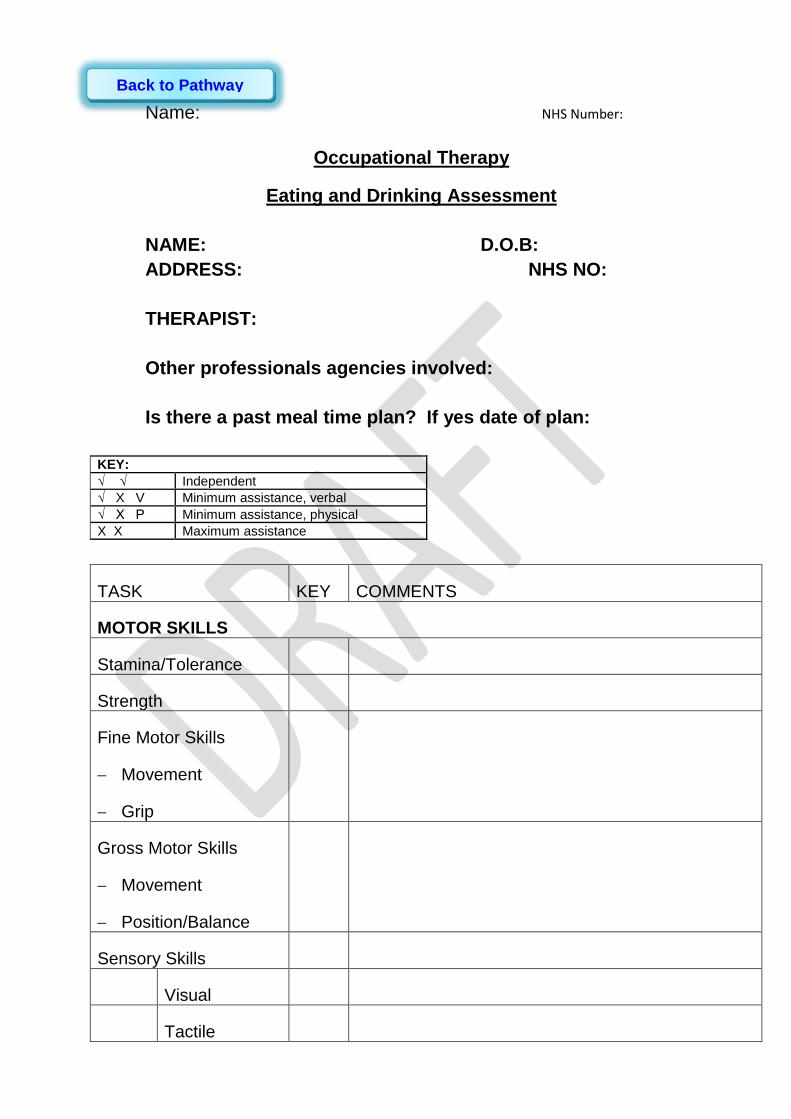
Name: NHS Number:
Occupational Therapy
Eating and Drinking Assessment
NAME: D.O.B:
ADDRESS: NHS NO:
THERAPIST:
Other professionals agencies involved:
Is there a past meal time plan? If yes date of plan:
KEY:
√ √ Independent
√ X V Minimum assistance, verbal
√ X P Minimum assistance, physical
X X Maximum assistance
TASK KEY COMMENTS
MOTOR SKILLS
Stamina/Tolerance
Strength
Fine Motor Skills
Movement
Grip
Gross Motor Skills
Movement
Position/Balance
Sensory Skills
Visual
Tactile
Back to Pathway
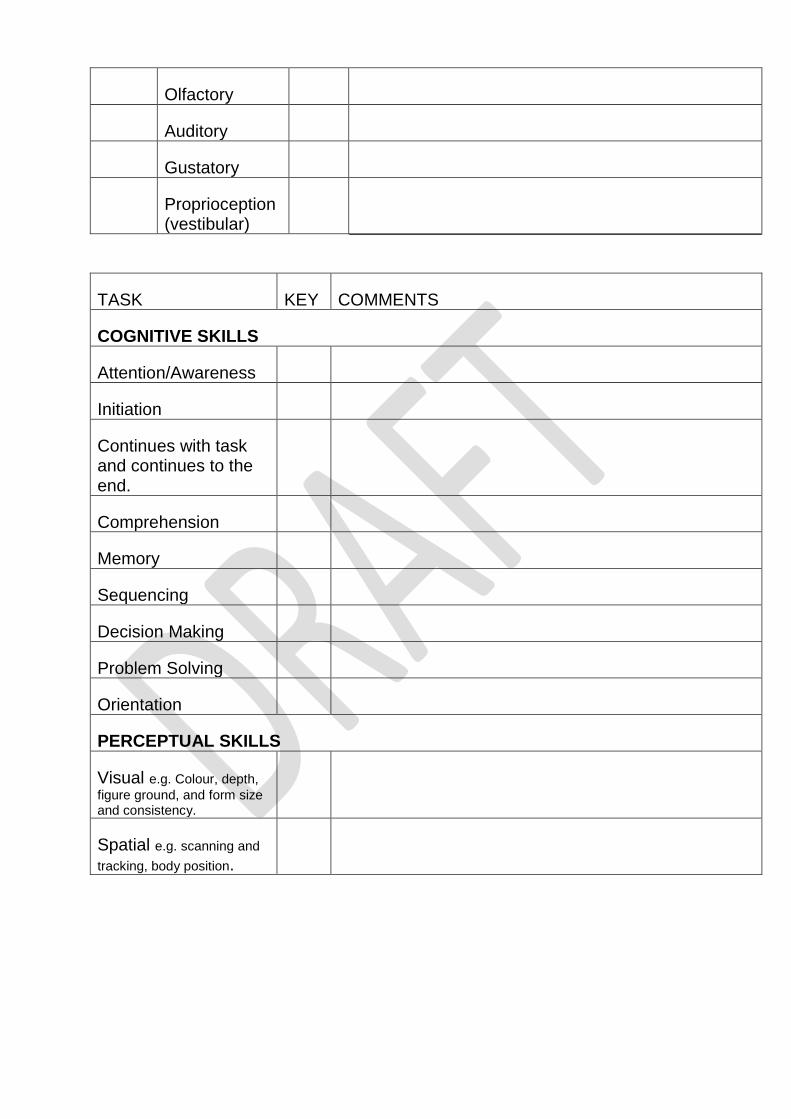
Olfactory
Auditory
Gustatory
Proprioception (vestibular)
TASK KEY COMMENTS
COGNITIVE SKILLS
Attention/Awareness
Initiation
Continues with task and continues to the end.
Comprehension
Memory
Sequencing
Decision Making
Problem Solving
Orientation
PERCEPTUAL SKILLS
Visual e.g. Colour, depth,
figure ground, and form size and consistency.
Spatial e.g. scanning and
tracking, body position.
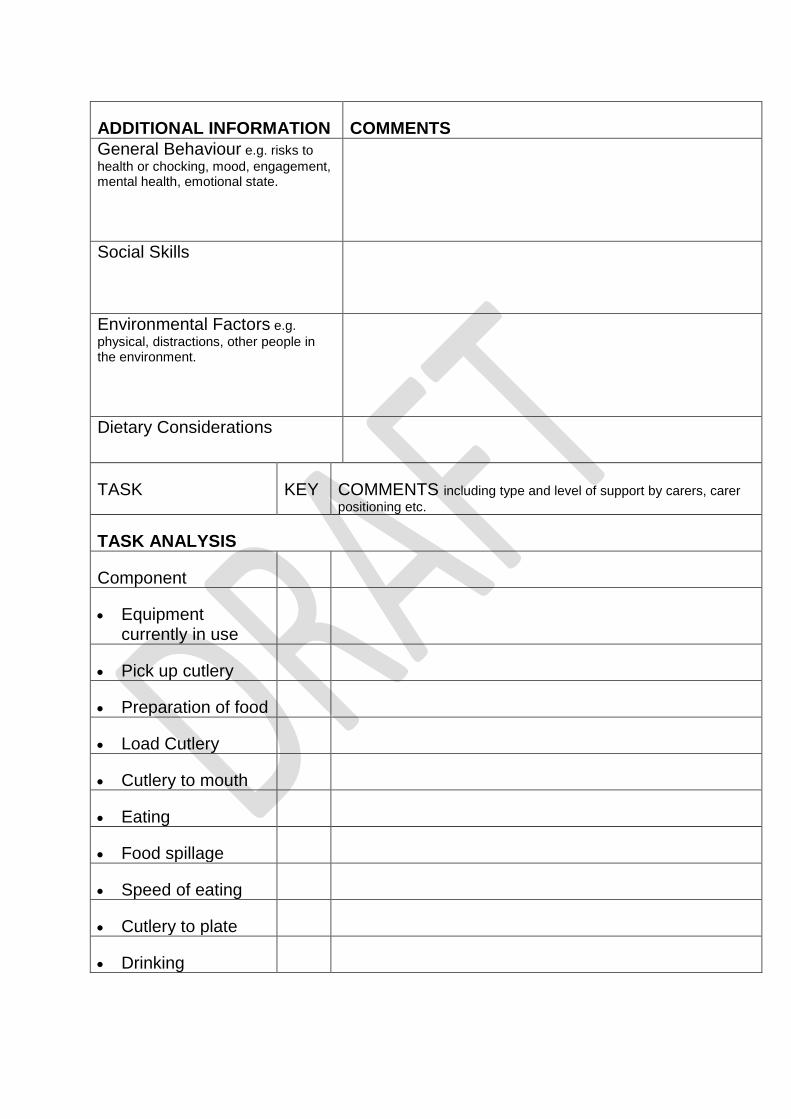
ADDITIONAL INFORMATION COMMENTS
General Behaviour e.g. risks to
health or chocking, mood, engagement, mental health, emotional state.
Social Skills
Environmental Factors e.g.
physical, distractions, other people in the environment.
Dietary Considerations
TASK KEY COMMENTS including type and level of support by carers, carer
positioning etc.
TASK ANALYSIS
Component
Equipment currently in use
Pick up cutlery
Preparation of food
Load Cutlery
Cutlery to mouth
Eating
Food spillage
Speed of eating
Cutlery to plate
Drinking
Considerations Equipment Considerations Materials:
Angles:
Size:
Shape:
Colour:
Weight:
Positioning Considerations
Environmental Considerations
Additional Considerations
E.g. task breakdown, intervention plan, staff training and support.
Therapist signature …………………………………………
Date …………………………………………
Back to Pathway
This is an in-house, non-standardised, assessment and observations sheet to inform
Occupational Therapists clinical reasoning for intervention and recommendations

The Role of the Dietitian
Role Definition
Assess individual to ensure that their diet is providing everything
that they need to remain healthy. They advise on ways to make
changes to improve the overall balance of the diet.
The Role of the Dietitian
Dietitians interpret the science of nutrition into practical
advice and guidance to enable people to make appropriate
lifestyle and food choices whilst taking into account the
individual’s circumstances and preferences.
This may involve:
Meeting with the individual to discuss diet and any alterations that may be required
Discussions with carers or other professionals to help facilitate changes
Advice around menu planning
Back to Pathway
The Speech and Language Therapist
Works with:
Communication Difficulties
Swallowing Difficulties
Back to Pathway
The pathway is person-centred, so this means that throughout the whole
pathway, the person should be included, informed and involved in decision
making at every level.
Communication is very important at mealtimes and when drinking.
It is important to gives choices about the meal, and help people to
know when the meal is anticipated.
It is important to know the person’s likes and dislikes- this should be
available in the person’s Person-Centred Plan
It is important to know when the person may be distressed- a DisDAt
tool may be useful here. (please embed link to DISDAT tool which
has been included elsewhere in pathway)
It is important to know when the person is trying to communicate such
as ‘stop’, ‘wait I am not ready’, ‘more please’, ‘I don’t want that!’ This
should be included in the person’s communication passport if they
have one. (please link to page for communication passport)
What Specialist assessment and intervention may the SLT do?
If the person’s communication requires specialist involvement, the Speech
Therapist may do a specialist communication assessment of understanding
and use of language.
The therapist may work with the support team to write a communication
passport for the individual and may also write a detailed report. ( link to
communication passport page)
The SLT will work with professionals and carers to help them understand
the best ways to involve you and communicate with you.
The SLT may recommend that a person needs supporting methods of
communication alongside speech such as using symbols, photos, pictures,
signing or other ways.
The SLT would support you and the carer to use these.
Communication Difficulties
Back to Pathway

How will the Speech therapist(SLT) assess swallowing?
Speech therapy assessment may include
Taking a detailed case history
Observing the person eating various textures and or drinking fluid
textures.
Observing the person eat a meal in their usual environments.
Detailed communication assessment of the carer and persons
interactions
Using Cervical Auscultation to listen to the sounds of breathing and
swallowing in the person’s throat. This means placing a stethoscope
on the person’s neck whilst swallowing whilst the therapist listens
carefully.
The speech therapist may also use a Pulse Oximeter to observe any
effect of eating and drinking on respiration and blood oxygen levels.
This entails clipping a monitor on to the person’s finger or ear or toe.
The speech therapist may suggest more detailed videofluoroscopic
assessment.
Cough and choke charts
Develop sensitive idea of food s managed or not
What will the Speech therapist do to help?
A Speech therapist assesses risks of swallowing: swallowing disability may
contribute to getting infections of the chest (chest infections) or lung
(pneumonia). Speech therapists work with the person, their carers and the
wider team to lessen risks of aspiration, choking or getting chest infections
and promote dignity, independence and enjoyment of the meal. The
speech therapist will try to accommodate the person’s wishes and cultural
needs.
Swallowing Difficulties

The SLT may suggest ways to make swallowing safer and better for you:
Modifying the texture of food or drink by using thickeners
Changing the speed of putting food/drink into the mouth
Changing the environment
Trying different ways to get food/fluid into the mouth
What if a person is at very high risk of aspiration and all other
adaptions have been tried and the difficulty persists? The speech
therapist may recommend that non-oral feeding is considered ( please put
link to Enteral feeding pathway /document here).
If enteral feeding goes ahead, the speech therapist could support the
person through this process, and would work out safe oral intake after the
PEG has been inserted.
The Speech therapist may also recommend referral on to other specialist
services or further tests from the GP. The Speech therapist would ask the
person’s permission and would liaise with the GP.
Back to Pathway

Accessible Information
Videfluoroscopy is radiographic imaging of the person’s swallow.
The person is required to attend an acute hospital in Leicester with a carer.
The person needs to give their consent to the procedure on the day.(unless it has been
decided the assessment is in the best interest of the person)
The staff team are fully trained: a combination of Speech therapist or Radiologist and
radiographer carry out the examination.
In advance, the SLT would work with carers to choose the best textures to trial and the
best ways in which to do this.
The person brings food and drink of a pre-arranged texture for the person to eat or drink.
The food or drink is mixed with a radiographic substance, depending on the risks
identified.
The person is seated between the camera and a monitor. As the person swallows, the
clinicians can observe and interpret the recording.
The SLT or Radiologist writes the report, sending a copy to the person and their GP.
Link to VF competences
Videofluroscopy
Back to Pathway
The Learning Disability Acute Liaison Nurse (ALN’S) Team
The team consists of three nurses with a learning disability background. The team members are: Katrina Dickens – Lead Nurse, Louise Hammond, and Lindsey Heald. The ALN’s are employed by the University Hospitals of Leicester Trust to help support patients with a learning disability who access the acute hospitals. This may be related to emergency admissions or via the planned care route. The role of the ALN’s means that they will need to interact with acute nursing staff, residential carers/supported living staff; families or carers; community learning disability teams and social workers. Once a patient has been identified to the ALN’s they will undertake a “meet and greet” visit. The ALN’s will follow the patients’ progress from admission to discharge. The ALN’s will also undertake the Learning disability Screening Tool if there are patients considered to have a learning disability but there may be some uncertainty. The work of the ALN’s focuses around the recommendations that were established under the Six Lives Report:
Accessible information within hospitals.
Complaints and experiences relating to people with learning disabilities and their carers.
Consent and capacity.
Reasonable adjustments.
the reasons for admission in relation to geographic areas on a yearly basis
To submit a yearly report to the Commissioners.
Learning Disability Awareness Training to the UHL staff.
The Learning Disability Acute Liaison Nurses can be contacted on: 0116 258 4382.
If they are not available, please leave a message on the answer machine
The things I do well
The things that are important to/for me
.
Back to Pathway
Health Action Plan Profile “ADD NAME”
“Add date plan started”
My health need:
Identified problem:
INSERT PICTURE
The things I want to try/ need to do
How best to support me
Who was involved in writing this plan:
Who can see this plan:.
Date What’s working
What’s Not working
Date Key Action’s from Health Appointment
Back to Pathway











![Eating and Drinking Habits of Americans 1 [1][1]](https://img.pdfslide.us/doc/110x75/55275ec349795994178b468b/eating-and-drinking-habits-of-americans-1-11.jpg)