Embed Size (px)
Citation preview

Error! No text of specified style in document. | Error! Use the Home tab to apply Section title to the text that you want to appear
here.
[Type here]
East London Health and Care Partnerships
Population Health Analytics Assessment – Final Report February 2018
This report and the work connected therewith are subject to the Terms and Conditions of the G-Cloud Order Form dated 19 September 2017 between East London Health and Care Partnership (ELHCP) and Deloitte. The report is
produced solely for the use of ELHCP for the purpose of assisting management with their assessment of the Population Health Analytics. Its contents should not be quoted or referred to in whole or in part without our prior written consent except as required by law. Deloitte LLP will accept no responsibility to any third party, as the report has not been prepared, and is not intended for any other purpose.
Deloitte Confidential: Public Sector – For Approved External Use

2 Deloitte Confidential: Public Sector – For Approved External Use
Contents
1 Executive Summary 3
2 Introduction 6
3 Summary & Recommendations 12
4 Key Observations 29
Appendix A – Scope and Approach 36
Appendix B – Population Health Analytics Maturity Matrix 38
Appendix C – Interviewees 39
Appendix D – Interim Operating Models 41
Appendix E – Glossary of Terms 43
Statement of Responsibility 45

3 Deloitte Confidential: Public Sector – For Approved External Use
1 Executive Summary
Based on the work undertaken, we conclude that the current population
health data platforms within the East London Health and Care Partnership
provide a maturing capability with the potential to enable advanced
population health analytics going forward. However, current analytics
capabilities are significantly less mature. Analytics capability will be
essential to releasing benefit for the Partnership through the identification
of population health insight to drive change in clinical care delivery. An
integrated approach should be taken to developing these capabilities,
based on population health need and efficacious use cases.
1.1 Overall conclusion
Population health analytics capabilities are recognised as being essential to enable the implementation of Accountable
Care Systems (ACSs). Significant progress has been made by ELHCP in establishing the east London Patient Record
(eLPR), providing a shared care record through the integration of Cerner and EMIS systems within the STP.
Additionally, the Discovery Programme has established a new data service for the local geography, collating data
from primary and secondary care to enable analysis for purposes of improving patient care and outcomes. Sharing
and aggregating data in this way is bringing to patients and clinicians.
Based on the work undertaken, the existing digital strategies, activities and platforms provide a good foundation for
the further development of population health analytics capabilities across the East London Health and Care
Partnership (ELHCP). These capabilities now need to be further developed and disbursed across the partnership.
The use of data within ACSs in the future will be fundamentally different to the way in which data is currently used
in the delivery of healthcare. Currently, data is primarily used as a tool to support the existing operating model
requirements of contract monitoring and performance management. The complexity of the clinical data sets, and the
sophistication of analyses required to determine population health needs, and to measure improvements in outcomes
for patients and service users, is a significant change, and greater than that which currently exists within health
systems across ELHCP.
In an ACS, data will be used to drive service delivery and support service improvement. As the commissioner and
provider separation is removed, both the local datasets and data models change to enable analysis, drive clinical
workflow and promote patient activation. The oversight and assurance role of bodies within a partnership responsible
for both providing and commissioning services changes from a process of contract management over healthcare
providers to an assessment of how to use available resource to enable the best outcomes. The maturing governance
structures, digital capabilities, leadership vision and clinical aspiration of the ELHCP health system provide a strong
foundation for delivering these future state requirements. However, significant change is required to align analytical,
operational, clinical and financial capabilities on a systematic basis to develop strong population health capabilities
to support frontline care delivery within ELHCP.
“Access to the system is the best thing since sliced bread! The dark shadow of what was
going on at the hospital has been lifted and there are many times when tests are not sent
down the link but are on the system which shows a huge amount of time in not having to
contact the hospital.” – Waltham Forest and East London EL GP

4 Deloitte Confidential: Public Sector – For Approved External Use
1.2 Key observations
Existing data platforms provide an effective foundation for population health analytics
In developing the eLPR and the Discovery platform, ELHCP have established an excellent foundation upon which
further population health analytics capabilities can be built. Additionally, other datasets have been developed within
the STP footprint (refer to section 3.1.3 below), including analytics within Tower Hamlets Vanguard on patient centric
data sets and a data cube within the ELHCP transformation programme, which provide further utility for population
health requirements.
However, inconsistent knowledge and understanding of the data platforms and their capability was identified, limiting
the extent to which data platforms are being effectively used across ELHCP at present. Clinical adoption of available
datasets is also currently limited, and there is a risk of duplicative activities where existing capabilities and data are
not aligned with the vision for the STP.
Efforts are being made to engage clinical, operational and financial leaders across the STP to support the development
of understanding and capability, however the penetration of engagement has been limited to date. There is a need
to broaden the discussion regarding both the data platforms, and population health analytics capabilities, in order to
ensure a consistent understanding of the utility of data platforms available.
The existing operating model, within which data is used primarily for contract monitoring and performance
management purposes, there is an understandable focus on ensuring existing requirements can be met. This has
limited the extent to which data is both available and shared on the existing data platforms. Additionally, we
identified cautious behaviours with regards to sharing data. While it is recognised that collaboration is essential, and
the necessary direction of travel, there remains a reluctance to share data across organisational boundaries,
particularly in community and mental health services, where service tendering and consequent competition is more
prevalent.
There is a need to enhance the use and adoption of data platforms, moving from transactions and collection of data,
to using data to inform the delivery of services for the improvement of outcomes and realisation of cost efficiency.
The ability to apply the principles of a Learning Health System (refer to section 2.1 below) will be essential to support
ELHCP in the development of delivery enhancements, and sharing identified improvements across the STP.
Analytics capabilities are under-developed
Capabilities demonstrated are mature within the current operating model (refer to section 3.1), however are not
focussed on population health requirements. Analytics teams across the STP are focussed on delivering against the
current operating constructs and requirements for analytics, resulting in limited capacity and capability to focus on
the analysis of population health datasets, and the rich clinical data contained therein.
A strategic approach to developing analytics capability, focussed on specific use cases and priority patient cohorts
should be adopted. Benefits of such an approach would be further enhanced in the use of principles from Learning
Health Systems, to identify and analyse data to test clinical interventions that would improve the health of specific
patient cohorts. Engaging analytics leaders across the STP in the developing this strategy should also address
duplication in datasets, evident between existing CCG, STP structures and CSU functions.
Local Digital Roadmaps within each geography of the STP outline the digital ambitions across ELHCP. These individual
health economy plans can now be developed as a single STP-wide plan. An essential part of this forward plan will
be to ensure a co-ordinated STP-wide plan is developed to enhance the maturity and adoption of clinical information
systems across health and social care organisations. This will be foundational to developing enhanced clinical
workflow and patient activations capabilities across ELHCP. Current contractual levers or mechanisms could be
developed further to encourage improved data coverage and data quality.
The understanding and measurement of resource utilisation at patient level is a necessary aspect of population health
analytics, particularly where the financial impact of new clinical models requires assessment. There is a requirement
to focus on developing the enabling capabilities, specifically patient level costing across patient pathways, to enable
the reform of financial flows as well as developing the incentive and payment mechanisms themselves.

5 Deloitte Confidential: Public Sector – For Approved External Use
1.3 Summary Recommendations
Complex data systems, such as the one that will be required to enable population health and place-based care across
ELHCP, require definition and design. Through the Digital Enablement Programme, ELHCP should take the lead in
establishing the analytics delivery approach and enabling mechanisms to ensure the development of enhanced
population health analytics capabilities across the STP, while also considering the opportunity to provide a broader
leadership role for population health analytics across London. We have described (at Section 3.2) a possible future-
state approach to the use of data that may assist in realising the benefits of data analysis to identify population
health priorities, measure the impact of new care models and contribute to sustainable patterns of resource
utilisation.
Detailed recommendations to support ELHCP in progressing towards the implementation of population health
analytics have been captured in Section 3.3 of this report. In the implementation of recommendations, further
enhancements to the current programmatic approach will be required.
The scope of our work was limited to the health technology and analytics functions of ELHCP, yet we recognise that
the ability to deliver population health analytics for ACSs will be dependent on the support and collaboration of
organisations outside of the direct influence of ELHCP, such as NEL CSU, and the London Digital Programme, all of
which have a role in supporting population health analytics capabilities going forward.
Phased approach to implement population health analytics capabilities
A phased approach and indicative timing to support in implementing the future-state approach is outlined at Figure 1. This approach would be based on Friedman’s Learning Health system, incorporating with regular review, feedback and amendment cycles. Change should be implemented through interim operating models (IOMs) as summarised
below.
Figure 1: IOM highlighting the phased approach to implementing changes

6 Deloitte Confidential: Public Sector – For Approved External Use
2 Introduction
2.1 Context
The East London Health and Care Partnership seeks to deliver on the
principles outlined in the ‘Five Year Forward View’ by improving patient
outcomes, through partnership working and collaboration across north east
London.
The ‘Five Year Forward View’ (FYFV) called for improved integration across health and care settings. New care models
seek to improve the sustainability of the NHS, making the best use of available funding at a population-level.
Sustainability and Transformation Plans (STPs) have been developed to outline the plans for the delivery of health
and social care services, focussed on a population within a defined geographical footprint.
Additionally, the ‘Next Steps on the Five Year Forward View’ outlines the desire to accelerate and support local NHS
commissioners and providers to build upon and strengthen STPs to support the establishment of Accountable Care
Systems (ACSs). ACSs bring together NHS organisations and local authorities to take collective responsibility for the
resources necessary to deliver population health and improve outcomes.
Originally established as the north east London STP, the East London Health and Social Care Partnership (ELHCP)
has the aim of measurably improving health and wellbeing outcomes for the people of North East London. In order
to achieve its aim, ELHCP recognises the requirement to develop new models of care focussed on prevention and
out-of-hospital care, working in partnership with organisations across the STP to commission, contract and deliver
safe and efficient services.
ELHCP brings together three distinct systems across north east London, to progress system reform. The systems
within ELHCP are City & Hackney (C&H), Waltham Forest and East London (WEL), and Barking Havering and
Redbridge (BHR). A programme has been established to progress the vision of the STP, and deliver the system
design components and workstreams outlined below:
Figure 2: ELHCP Programme workstream structure
7 Deloitte Confidential: Public Sector – For Approved External Use
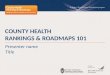
Digital leaders have commissioned a review of the population health analytics capabilities that are in place to support
the delivery of the STP’s transformation programme. Our assessment was undertaken during September and October
2017, and considered a current state assessment to enable the development of strategic and tactical
recommendations to further support the development of both digital and analytics capability within the Partnership.
Digital Enablement workstreams have been established for Shared Records, Patient Enablement, Advanced system-
wide analytics and digital infrastructure, with structures established across each geography within the STP, as
outlined below:
Figure 3: ELHCP Digital Enabler Governance structure
Significant progress has been made by ELHCP in establishing the eLPR, providing a shared care record through the
integration of Cerner and EMIS systems within the STP. Functionality enabled by the eLPR includes Acute hospital
access to GP records, secondary care appointments and results available to GPs, while also providing the mechanism
cross-organisation for approval and sign-up to data sharing. Work is continuing to expand the systems and
organisations from which data within the eLPR is collated, to further enhance data sharing and interoperability across
the STP.
Within the ELHCP geographic footprint, Newham CCG, City & Hackney CCG, Waltham Forest CCG and Tower Hamlets
CCG are working in collaboration with the Endeavour Healthcare Charity on the Discovery Programme. The Discovery
Programme has established a new data service for the local geography, collating data from primary and secondary
care to enable analysis for purposes of improving patient care and outcomes.
Data within the Discovery Programme includes EMIS extracts from in excess of 100 GP practices as at August 2017
(to be updated for October 2017 figures). Additionally, admissions, discharges, and transfers (ADT) data is being
received by Discovery from both Homerton Hospital and Barts Hospital. It is the intention of the programme to
broaden the scope of the data sets collected by Discovery (including mental health data and local authority data),
while also broadening the footprint beyond the current CCGs, to cover the whole of the STP providing the basis for
an effective population health data platform.
The ability to share data and learn from good practise across the three geographies within ELHCP will be critical, and
is a key requirement for the delivery of effective population health analytics capability. Population health analytics
plays a crucial role in identifying, enabling and measuring the changes in care models necessary within effective

8 Deloitte Confidential: Public Sector – For Approved External Use
accountable care systems. This assessment has therefore consider the potential of the data platforms and digital
strategy available within ELHCP to deliver this capability effectively.
To ensure effective engagement in and use of the existing data platforms, the Digital workstream within ELHCP aims
to establish and benefit from the principles of a Learning Health System1. Learning health systems adopt cyclical
improvement approaches, through the use of technical and social approaches to learn and improve with every patient
who is treated across the partnership. This approach therefore informs the implementation process to test and
develop the population health platforms within the Partnership. The principles of a health learning health system,
as outlined by Professor Charles P. Friedman, are reflected below:
Figure 4: Friedman’s Learning Health System Cycle
According to Professor Friedman, any Learning Healthcare System has the following three components (Friedman 2015):
1. Afferent (Blue) side: Assemble the data from various sources Analyse the data by various means Interpret the findings
2. Efferent (Red) side:
Feeding findings back into the system in various formats Changing practice
3. Scale: Can be institutional, national, international
In order to align with this approach we have considered our findings in the context of this learning cycle and
recommendations identified make reference to this improvement method.
2.2 Methodology and approach
The maturity of population health analytics capability can be considered against the six core capabilities, highlighted
below. Deloitte have used this taxonomy, developed through extensive use in US health systems, to inform our
assessment of health analytics capabilities across ELHCP.
Interoperability,
Integration, HIE
Connects healthcare information and data via Application Programming Interfaces (APIs), Health Information Exchange (HIE) or messaging protocols across the ACSs for clinicians and patients to access.
Data Aggregation and Management
Aggregates data from disparate sources to improve transparency across the ACS
1 Charles P. Friedman, 2014 - http://www.learninghealthcareproject.org/section/background/learning-healthcare-system

9 Deloitte Confidential: Public Sector – For Approved External Use
Analytics (including Risk
Stratification) Enables insight-driven analysis that is both descriptive and prescriptive
Reporting Delivers a self-serve solution for performance management across the ACS
Clinical Workflow Orchestrates the execution of activities from disparate systems constituting the care continuum and ACS
Patient Activation Enables the patient to manage their own care needs and drives
required clinical workflow.
Component activities that enable increased population health analytics maturity within each of the six capabilities
are outlined in Figure 5 below.
Figure 5: Population Health Analytics capability maturity
To further support in the definition of maturity for population health analytics capabilities, the delivery outcomes of
the capabilities outline in Figure 5 are described in their mature state below:
Clinical Operational Financial Technology and Data
People
Real-time visualisation of patient interactions with services across the care system, and
personal patient
technology
Near real-time visualisation of
resource use to enable demand profiling and system-wide variation
identification
Near real-time cost allocation and visualisation of
consistent metrics across the care system
Consistent, high quality data collection, data architecture and security across the
care system
People and teams understand the
operational and clinical requirements of data collections and can
enact the analytics requirements, to
generate meaningful
insights

10 Deloitte Confidential: Public Sector – For Approved External Use
Drawing upon our population health analytics maturity framework, we considered population health analytics
capabilities across four key lines of enquiry enabling the practical linkage of the concepts outlined in Figure 5 with
service delivery within ELHCP:
i. Operational: capability to operationalise place-based health analytics to embed data analytics into
day-to-day working, enable the delivery of new clinical workflows and support patient self-help and
direct engagement in their care;
ii. Clinical: capability to harness health analytics to enable governance and delivery of clinical care and
associated research requirements through technology-enabled place-based care models;
iii. Financial: capability to use health analytics to understand and create mechanisms to manage
financial flows and payment mechanisms to support the achievement of place-based care outcomes;
iv. Technical: capability of technology, analytics and associated governance frameworks to deliver and
scale to provide the technology infrastructure required to support place-based care.
In completing our assessment of population health analytics capabilities, we met with 58 Operational, Clinical,
Financial, and Technical stakeholders from across ELHCP, through both interviews and workshops. Three workshops
were held with Operational, Financial and Technical leads to enable consideration of leading practise, barriers, and
future ambitions for population health analytics within ELHCP. A list of all stakeholders we met with in performing
our assessment has been captured in Appendix C below.
An outcome-based population health analytics maturity matrix which outlines the mature state capabilities against
each of these lenses can be found at Appendix B.

11 Deloitte Confidential: Public Sector – For Approved External Use
2.3 How to use this report
To aid the reader, we have outlined below how the report has been developed, and how it should be read in figure 6
below.
Figure 6: How to read this report
2.4 Acknowledgement
We would like to thank all staff from across ELHCP for their co-operation during this assessment. A list of the staff
involved during the assessment is included at Appendix C.

12 Deloitte Confidential: Public Sector – For Approved External Use
3 Summary & Recommendations
3.1 Current state assessment
The functions and structures associated with health analytics across ELHCP are complex. Analytics functions and
capabilities are dispersed across multiple organisations, within primary, community, mental health and secondary
care, commissioning support unit and local authority organisations. They are represented diagrammatically in Figure
7 below.
Figure 7: ELHCP Organisations
Analytics functions and capabilities in each organisation within ELHCP are aligned with current organisational
requirements and reporting priorities focusing on the financial, statutory and performance reporting requirements.
Additionally, North East London Commissioning Support Unit (NEL CSU) provide analytics support to organisations
across the ELHCP, but are not a formal member. Based on their understanding of the analytics capabilities across
the Partnership, it is recognised by ELHCP Digital Leadership that current operating model will not support the delivery
of effective population health analytics and that enhanced analytical capability is required going forward.
3.1.1 Population Health analytics capability maturity
In performing our assessment, we sought stakeholder perspectives on the relative maturity of their analytics
capabilities within ELHCP constituent organisations. The population health analytics capability curve was used in
order to assess maturity in a consistent manner.
Organisational assessment
The current-state assessment presented in Figure 8 below, informed by discussions with stakeholders across
organisations within the STP, aggregates maturity by geographical region within the STP. In doing so, variances in
maturity across local geographies within the STP are highlighted.
The maturity presented within Figure 8 below has been determined on the following basis:
Self-assessment of maturity, informed by discussion with stakeholders;
Assessment of maturity considers the current operating model for analytics, and the extent to which current
maturity supports its delivery; and
Provides an organisational view of maturity, aggregated by STP geography.

13 Deloitte Confidential: Public Sector – For Approved External Use
Figure 8: Population Health Analytics capability maturity within current operating model, informed by stakeholder discussions
STP Leadership assessment
Digital enablement workstream leaders also considered maturity against the same assessment framework, and
determined an additional view of current state maturity across each geography in the STP, based on the ability to
aggregate and analyse data across patient pathways, in accordance with the desired future geographical constructs.
Maturity considered against a future operating model is presented in Figure 9 below:
Figure 9: Population Health Analytics capability maturity, considered against the target operating model, informed by Digital
Enablement workstream leadership (* BHR assessment to be completed by digital leadership)
14 Deloitte Confidential: Public Sector – For Approved External Use
The assessment (Figure 8) indicates participant’s views of the maturity of their analytics capabilities within the
current operating model. As such, capability maturity reflects the existing programmes of work within the local
geographies and organisations. The current maturity also reflects the beginning of the adoption of digital platforms
that enable population health activities across the all the geographies in the STP. Specifically the assessment
indicates:
1. Comparatively high levels of maturity for interoperability and integration capabilities as evidenced in the use
and adoption of the eLPR and Discovery platforms. Notably the core building blocks of patient master index
and data security architecture are present providing a firm foundation for other activities.
2. Developing capabilities in data aggregation and reporting capabilities reflecting the use of data to support
the commissioning and performance accountability frameworks. However it was noted by participants that
this maturity assessment reflects the ability to aggregate data according to the current organisational
constructs and does not indicate that data can be aggregated at a patient level across care pathways or for
a specific patient cohort within a geography.
3. The analytics maturity assessment aligns closely with the views expressed by interview and workshop
participants. It indicates that the ability to use and gain benefit from the existing datasets through analytical
techniques such as risk stratification, patient cohort identification and actuarial modelling, are developing.
Whilst maturity in reporting appears higher, it is important to note that the reporting and visualisation
capabilities need to display data analysed using these techniques is yet to be developed systematically.
4. In common with other health economies, where we have undertaken similar assessments, the clinical
workflow and patient activation capabilities are still maturing. Good practice examples exist and demonstrate
an emergent, higher level of maturity. For example, the algorithms for reduced use of NSAID in people with
CVD, the increased use of high intensity statins in people with CVD and increases in anticoagulation therapies
for AF (and reduction in aspirin monotherapy) in primary care are examples drawn from a number of analyses
using primary care data that are currently influencing clinical practice and benefitting patients. In secondary
care proactive identification of acute kidney injury and major limb trauma, provide use cases that have
succeeded in delivering actionable, near real-time insights to clinicians using the data currently collected
within the health system. These areas of good practice indicate the potential to further develop this capability
and, aligned with service improvement initiatives, to generate further use cases that can demonstrate direct
benefit for patients.
5. Through discussion with operational and financial leaders, the need to use data within existing data platforms
to inform service planning and commissioning decisions across the STP was highlighted. The potential for
clinical and care patient variation analysis is significant and could be realised at pace given the integrated
datasets in place. Plans in place to increase the volume and scope of these datasets by the end of the
calendar year 2017 will further enhance the potential.
6. Patient activation capabilities offer significant transformative value to the health system. Examples of good
practice, such as the development of the ‘My Mind’ application in North East London Foundation Trust
(NELFT), indicate that the technologies can be applied effectively within specific care models. Improving
availability of on-line scheduling and access to medical records in primary care is a clear example of the
benefit of digital patient engagement within their healthcare record. The challenge now is to consider the use
of these patient enabling technologies in service re-design and quality improvement initiatives, whilst
continuing to develop the underlying infrastructure and capabilities (for example a patient health record) to
deliver the value of this change for patients.
Interesting variation exists when the organisational focus to the maturity assessment is compared with the STP
perspective. Specifically:
Maturity in data aggregation capabilities is reduced, reflecting a further requirement to share and link data
between institutions, as opposed to collecting and holding data at an organisational level. This indicates that
the foundations for data sharing are in place, and that further opportunity to share and link data sets should
be explored.

15 Deloitte Confidential: Public Sector – For Approved External Use
Analytics and reporting capabilities are assessed as developing, but no capabilities are assessed as being in
a mature state across the STP as a whole, reflecting the need to develop and use analytical techniques
beyond the specific existing clinical use cases identified in Section 3.1.1.
Clinical workflow and activation capabilities are identified as more mature that the perspective of participant
organisations, reflecting the leadership’s knowledge of capabilities displayed through advanced use cases. It
is acknowledged that whilst these capabilities exist in defined clinical areas, there are developing mechanisms
to scale this good practice to reach a mature state, such as Primary Care improvement supported by CEG.
It is very encouraging to see clinical teams engaged in data analysis in these specific areas and using the
insight gained from analysis to impact and improve care delivery.
We compared to the view of digital leadership, as evidenced in this maturity assessment, operational leaders
considered maturity in the analytics capabilities to be lower, citing the need to improve the quality of analysis
to inform resource utilisation decisions and the need to triangulate data sets, particularly public health data
sets with available clinical data to achieve a fuller picture of opportunities to improve care or reduce costs.
This difference of opinion is explored further in Section 3.3 Recommendations.
The maturity assessments and associated interviews have led to the development of the following key observation
regarding health analytics capability across ELHCP.
3.1.2 Discovery and eLPR platforms and capability
The Discovery and eLPR demonstrate mature capability to interoperate and aggregate data across the health
and social care geographies. There are clear plans in place to extend their data coverage and capabilities
going forward. Furthermore, increasing clinical use of the eLPR is being evidenced month on month (increase
in views of eLPR in September from approximately 60,000 to 70,000).
Clinicians interviewed were able to articulate the benefits of the eLPR in their everyday practice, specifically
valuing the tool as a mechanism of communication between healthcare organisations. It also allows clinicians
to make decisions with a wider breadth of knowledge and clinical history, thereby reducing the need for
additional telephone conversations, repeat patient visits and diagnostics. As further data sources from mental
health and community providers are added the transformational capability of the aggregated data set was
recognised and welcomed.
There is a recognised need to spread the adoption and use of the eLPR across the partnership. Some clinicians
expressed the need to have a summary of patient activities as the information available on patients at first
use was reported to be difficult to navigate, effecting the inclination to adopt the system within clinical
practice.
The Discovery platform is recognised within the partnership, and across London, as offering the capability to
undertake advanced population health analytics. Discovery also has the capability to support the further
development of specific clinical use cases through the identification of priority patient cohorts. In doing so,
additional or changed clinical interventions could positively impact the aetiology of disease or reduce the
requirement for resource usage in care delivery.
Knowledge of the Discovery platform and how to navigate the processes to access the data held within the
system were well understood within the research and secondary care clinical community. There was
significant support for use of the data to inform specific clinical use cases and improve care delivered to
related patient cohorts. However the process to access and design use cases and specific question sets to
enable access to the Discovery platform was not well understood across the ELHCP transformation
workstreams, with participants unclear as how to access or analyse the data source available to them.
In discussion with teams outside the immediate digital enablement workstream and practicing clinicians,
there is an inconsistent knowledge of the data platforms and their capability, and value to developing care
and payment models. Specifically the analytics role within the ELHCP digital workstream was not well
understood by interviewees.

16 Deloitte Confidential: Public Sector – For Approved External Use
Communications are perceived as well-led but there is concern that key messages are not consistently
understood within constituent organisations. Interviewees also observed that communication about the
progression of the digital plan could be improved, particularly within social care, to allow for alignment of
activities between the sectors.
3.1.3 Analytics capacity and capability
The digital and analytical capabilities within the transformation workstream are often elided. Enacting these
capabilities requires different skills and tools, particularly for population health analysis. However, these
capabilities are under-developed when compare with the digital capability in evidence.
Aggregated data sets in place form a good basis for undertaking analytics that can inform clinical care
delivery. However there is the danger of duplication with the development of a number of data sources that
could be used as the basis for this analysis. Data management systems were identified as in development
or use include:
The Discovery Platform;
A data cube within ELHCP transformation programme;
NELIE within NEL CSU;
Analytics work within Tower Hamlets Vanguard on patient centric data sets; and
‘Health Analytics’ platform within the BHR health system.
There was concern that scarce resources were duplicating work in establishing and running different data
management services and there was opportunity to identify a single dataset and realign analytics resources
to progress the use of the single dataset at a faster pace.
Capability is limited by the current constructs and requirements for analytics, with focus being applied to
contractual reporting, finance and performance within healthcare and statutory requirements within social
care. Clinicians expressed concern that limited analytics capability is therefore available to analyse the rich
clinical datasets that are available, hampering the ability to gain insight and triangulate data sources to
predict or measure the impact of clinical intervention. Analytical capability also exists within NEL CSU. These
capabilities were not being actively engaged in the development of system analytics capabilities and there
was a perception that the resource and capability was not well aligned to the requirements of the system to
develop population health analytics.
There is a recognised need for additional skills to progress predictive and actuarial modelling skills. Currently
this is being sourced as needed by organisations across the STP, with methods and tools chosen for specific
requirements.
There is a lack of alignment between identified population health needs, the aims and intentions of
transformation programmes and the data sources, data items and data coverage required to measure
progress effectively.
3.1.4 Application mapping, data governance and coverage
The applications in use across ELHCP provide a high-level of commonality, as highlighted in Figure 9 below.
We were informed of quality improvement activities undertaken to enable consistent data capture within
EMIS through the use of standardised templates and data fields linked to codified data structures that enable
the use of datasets comparatively across populations. This provides a strong platform for further use of data
from native systems through aggregation in population health platforms.
However during interviews with both CIOs and transformation practitioners, issues were identified with the
multiple instances and software versions, limiting the value of aggregated data. This was further
compounded by the differing levels of adoption and methods of use of the systems. For example the same
field in the same version of the software may be used to enter different data in hospitals treating the same
patient cohort, thereby making basic activity comparisons between providers challenging.

17 Deloitte Confidential: Public Sector – For Approved External Use
Figure 10: Core clinical applications across primary and secondary health care in ELHCP, including eLPR integration
There was recognition of the need to progress work relating to data lineage, governance, coverage and
assurance as part of the work to progress digital and analytical maturity across ELHCP. Participants identified
that there was opportunity to do this in support of specific clinical initiatives, thereby increasing clinical
engagement in the definition, collection and use of the data recorded as part of the patient pathway. The
aspiration for this alignment of purpose and process was clearly in evidence, although practitioners were
struggling to enact their aim, referencing lack of governance forums and processes on data quality and data
recording as a concern.
The Barking, Havering and Redbridge system demonstrated increased multiplicity of primary care systems,
with the majority systems indicated in Figure 10 above representing only 50% coverage, with the use of
Vision in 40% of practices. This variation in core systems could lead to the generation of datasets that are
not comparable and require additional data manipulation to create useable datasets. The Medway patient
administration system (PAS) is in use at Barking, Havering and Redbridge University Hospitals NHS Trust
(BHRUT). Designed as an administration system, it may not have the breadth and depth of functionality
required when compared to an integrated EPR. This indicates that in the long term further investment in
clinical systems may be required to collect the rich clinical data sets through the process of delivering care
that will enable mature population focused analytics across this health system.
3.1.5 Alignment of digital, analytics, transformation and commissioning capability to achieve benefit
for patients
The history of innovation and partnership working in geographies across the Partnership, particularly in the
work of Tower Hamlets Together vanguard initiative, has generated an enthusiasm for and commitment to
improvement and change. Specific examples of improvement that have the potential to utilise the benefits
of the existing digital platforms include the social prescribing initiatives in place across Tower Hamlets CCG
and the quality improvement programmes within primary care that are being rolled out across all Partnership
CCGs.
Evidence of quality improvement teams accessing the rich datasets held with the existing data platforms was
not identified. Such data could be used to assess the impact of changes implemented and provide useful
data to inform service evaluation. Opportunity exists to increase the access to the existing data platforms

18 Deloitte Confidential: Public Sector – For Approved External Use
and undertake fast-paced analyses, or ‘sprints’, to identified patient cohorts where changes in clinical practise
could improve care and reduce cost. There was an appetite to undertake these activities, recognising that it
would be possible to identify further use cases quickly and consider how best to implement them using
existing improvement initiatives. Even if implementation was not possible for some use cases, testing data
quality through analysis will further highlight opportunities to improve quality and generate further
opportunities to improve patient care.
3.1.6 Digital maturity and adoption
Digital maturity and adoption vary significantly across providers, particularly secondary and community
providers. As such the rich clinical data needed to progress population health analytics and link findings to
clinical outcomes will be missing from the data sets held within both the eLPR and the Discovery platform.
Each constituent organisation has plans to improve maturity in their digital capability, with progress achieved
at the Homerton Hospital NHS Foundation Trust and Barts Health. However, workshop participants articulated
that resource constraints will delay digital maturity and consequently the ability of clinical teams to collect
clinical data in structured formats to enable sharing of consistent data sets to realise the benefits of population
health analytics in its fullest extent.
Community and mental health providers were also demonstrating increased use of technology in the
recording of clinical care. However they also cited the relative immaturity of national datasets, definitions
and contractual mechanisms as a reason why the data captured focused primarily on the recording of clinical
care activities, rather than the collection of diagnostic, care planning or procedural data.
Variation in digital maturity and adoption will impact the ability of the Partnership to leverage the value of
the population health platforms they have developed. However there is the clear will and aspiration to make
incremental improvements of digital capability within provider organisations which will create a good
foundation for the progression of population health analytics around specific patient cohorts and in
partnership within relevant clinical teams.
3.1.7 Financial flows development
ELHCP are taking active steps to consider the future of financial flows in their partnership and determine how
resource allocation could be undertaken differently within an ACS. A consultation securing the views of
participant organisations has recently closed, and information is being collated to form the basis of forward
plans
In support of this initiative a workshop and interviews where held with senior finance leaders across the
partnership. The workshop focussed on understanding the maturity of the datasets underpinning existing
financial mechanisms and the plans to progress the maturity of these datasets to support the development
of population-based resource allocation. Informed by the workshop and interviews, a maturity assessment
of financial data sets is shown below:

19 Deloitte Confidential: Public Sector – For Approved External Use
Figure 11: Population health financial flows maturity assessment
In completing this assessment financial leaders were of the opinion that increasing maturity of clinical
datasets was the priority for the Partnership and that associated financial data sets could be built upon good
quality clinical data. However in assessing their current maturity, participants considered that:
1. Existing financial flow mechanisms and supporting datasets were mature in their use within the
current operating model across provider settings;
2. A number of provider organisations identified progress in the development of service line reporting
and patient level costing. Maturity was therefore differential across providers, with underlying data
capture, consistency of costing methodologies and capacity of finance and analytics teams to
support the development of capability, particularly PLICS, identified as rate limiting factors; and
3. Whilst the concept of resource profiles at patient level was well understood and agreed, capacity
and capability within costing functions was not sufficient to progress this requirement or to consider
linking datasets between organisations to progress pathway costing. Care pattern variation or
assessment was recognised as providing an excellent basis for such work and the need for a
consistent costing methodology and approach at pathway level was seen as an important
requirement to progress this requirement.
The maturity assessment outlined the following key observations regarding relationship between financial
flows requirements and health analytics capability across ELHCP:
1. Clear commitment to leveraging data to modernise approaches to commissioning. The current
consultation process was seen as a good basis upon which to build a future consensus of opinion
and develop an agreed strategy. However, concern was expressed about the financial impact of
any changes and the potential to shift demand pressures and create financial instability if moves to
capped or capitated models were undertaken too swiftly.
2. There are currently no contractual or performance mechanisms that encourage resource utilisation
at a patient level. A consistent view was expressed that effort should be focused on developing a
common approach to the use of existing capabilities such as SLR and PLICS in developing the

20 Deloitte Confidential: Public Sector – For Approved External Use
underlying data sets to inform the development of new payment models. Designing and agreeing
a consistent costing method was seen as important by provider organisations of all types to enable
the development of patient pathway costing over time. Without a common agreed method, data
sets and resource allocations would be inconsistent between organisations and therefore not
comparable when linked across pathways.
3. Participants observed that the existing accountability mechanisms within the contract for services
that focus on data quality where not employed. This is resulting in a lost opportunity to focus
services on the collection of data that would inform both clinical care and the development of
financial flows mechanisms into the future.
4. Opportunity exists to develop a progressive approach to financial flows that focus on engaging
clinicians and organisations in improving data collection and data quality. Current CQUINS
mechanisms were identified as an opportunity to incentivise the collection of clinical data and
associated activity data items within and between organisations across an identified patient
pathway. Applied effectively this mechanism could help to address issues of data coverage and
data quality, encouraging organisations to agree data items across patient pathways and focus on
continually improving the accuracy of data collection.

21 Deloitte Confidential: Public Sector – For Approved External Use
3.2 Future state
It is important to consider the desired future state for ELHCP and the delivery of population health analytics in order
to progress the recommendations and next steps identified in the assessment. Informed by discussions with ELHCP
management, and the Transformation Programme, we have identified the following key characteristics of the future
state for population health analytics across ELHCP:
Single integrated clinical data view, populated from all organisations within the STP, and available to view,
update and analyse in near real-time by clinical and non-clinical staff;
Active approach to population health analytics to drive improvements in patient care and health and wellbeing
outcomes, using a common, accessible visualisation platform;
Progress and activities aligned with the needs of patients and service users, based on an informed
understanding of population need;
Support the enactment of an effective learning health system, in which data are used to inform the
development of best practise which can be tested and shared across constituent organisations to improve
outcomes for patients.
ELHCP digital leadership have identified through the workshops with colleagues their aspirations for their future
analytics capabilities using the maturity model. The aspirations for capability by 2021 across the STP are highlighted
below:
Figure 12: Future state aspiration for STP aggregate maturity
Presented in the table below, Digital leadership identified the outputs of the enabling digital and analytical capabilities
both now (highlighted as orange below) and in the future (highlighted as green below), describing the forward
aspiration of the partnership.

22 Deloitte Confidential: Public Sector – For Approved External Use
In considering the current state assessment, future-state capability aspirations and the defining characteristics of
digitally-enabled care, we have developed a future-state approach to the use of data that may assist in realising the
benefits of data analysis to identify population health priorities, measure the impact of new care models and
contribute to sustainable patterns of resource utilisation.
Figure 13: Illustrative future state structure
The maturing governance structures, digital capabilities, leadership vision and clinical aspiration of the health system
provide a strong foundation for delivering this future state. Specifically future state system characteristics would
include:
1. Further development of the integrated data view, with the additional navigational and visualisation tools at
patient and population level to allow clinicians and service planners to access the use the data more readily.
Over time, consideration should be given to merging the eLPR, Discovery, and other data platforms as richer
clinical datasets are available in near-real time and the appropriate analytics techniques develop to allow
interrogation of the data.
2. Aligning the service improvement activities that are the focus of the transformation workstreams with the
local population health need identified in the localities. This will enable the creation of priority patient

23 Deloitte Confidential: Public Sector – For Approved External Use
populations or clinical use cases, where the combined capability of clinical expertise, analytics and quality
improvement can be combined to improve patient care.
3. Ensuring that the governance model in place to lead ELHCP adopts, promotes and resources the priorities
and builds multi-disciplinary teams around the specific clinical use cases. Analytical capability across the STP
should be co-ordinated to design, test and measure the impact of new care models on an iterative basis in
line with the principles of Friedman’s Learning Health System.
4. Aligning incentives to encourage the collection of data, improvement in the quality of care and the use of
data in clinical care will be an important mechanism to enable the measurement of the impact of new care
models. There is an opportunity to reward improving data coverage and data quality and thereby incentivise
organisations and clinical teams to collect data as part of the process of care. Particular benefit could be
achieved by aligning these incentives across a patient pathway.
5. Consider the development of specific clinical and business processes that are aligned with delivery support
functions and oversight and assurance functions. Clarity in the use of identified and de-identified data and
the purposes for which these data will be used will be critical to building and maintaining public confidence
in the way patient level data is used to deliver and plan healthcare. As confidence in the use of data builds
it will be important to consider carefully how those data are used for oversight and assurance purposes. Data
must continue to be seen as a tool to improve patient care and not an instrument that is used punitively to
compare performance of organisations. The focus on improvement, reducing variation and meeting
population health needs will lead to improved performance if service models are effectively enacted.
6. Enabling capabilities are required and should be systematically developed to allow the process of using the
available data to be transacted effectively. Examples include codifying and reusing information governance
policies and procedures, applied consistently across the health economy, developing consistent data
definitions and standards and creating (or using) effective verification services for patients and staff are all
critical to continuing to mature the population health analytics capabilities within the Partnership.
7. A formalised quality improvement method based on Friedman’s Learning Health System, which builds on the
existing afferent capabilities, creating additional analytical capability to identify patient cohorts and interpret
the findings of analysis. Efferent processes to design, test and evaluate care models that provide an
efficacious method of changing clinical practice, possibly as part of existing quality improvement
methodologies, could then be deployed to embed change and provide the basis for scaling benefit across the
partnership. Developing a capability; people, skills, tools, methods and processes, that can define, refine and
repeat this method and train others to use it, will be an important vehicle for using the insights from
population health data and achieving tangible resulting change.

24 Deloitte Confidential: Public Sector – For Approved External Use
3.3 Recommendations
In performing our assessment, and in analysis performed by ELHCP2, practical benefits for patients and staff have
been acknowledged by clinicians as a result of work undertaken to date with the adoption of eLPR have been
highlighted:
Further work is necessary to continue to support the vision for ELHCP and deliver further benefits for clinicians and
patients in improving outcomes. The following recommendations have been identified, structured according to the
current state assessment in section 3 above. Collectively they represent the key areas required to progress towards
the future state approach identified in Section 3.2:
# Recommendations
Discovery and eLPR platforms capability
1
Raise awareness of digital platform functionality and capabilities
A clear articulation of the ELHCP digital infrastructures and platforms that hold data should be developed to raise the awareness of the platforms more broadly across the STP. Functionality across digital platforms should be differentiated from the analytics capabilities required to use the available data in order to gain insight into the healthcare needs and resource usage across the economy.
To further support in raising awareness, digital infrastructure and platform capabilities should be articulated alongside implemented use cases across operational, financial and quality improvement teams within the Partnership.
2 Analysis undertaken by ELHCP, captured within “Benefits study - evaluation of the East London Patient Record, version 1.1”

25 Deloitte Confidential: Public Sector – For Approved External Use
# Recommendations
2
Define the ELHCP analytics delivery approach
The forward analytics delivery approach should be defined and documented, outlining aspiration for the
use of a single data platform and visualisation capability across ELHCP. This approach will avoid
duplication of data platforms and maximise the available investment in existing platforms.
Consideration should be given to drawing together analytics capabilities across constituent organisations
including NEL CSU, to focus specifically on enabling clinical practice change through data-generated
insight. Embedding this capability within a multi-disciplinary team of clinicians and research could lead
to significant progress in developing use cases and impacting clinical pathways at pace.
3
Establish an enabling mechanism for access to and assessment of the data in the Discovery
Programme
Define and implement a mechanism, supported by ELHCP, to enable multi-disciplinary and services teams
to access the data held within the Discovery Platform to support the completion of population needs
analysis. Specific focus should be given to understanding patient cohort service usage to enable the
development of appropriate hypotheses and question sets that can be used to design data queries.
4
Support a broader London role in population health analytics
Build upon the capabilities developed within East London, and position the STP to work in partnership
with the London Digital Programme. Consider the ability of the Discovery Platform, eLPR and in the
future, the East London Data Repository, to exemplify the use of a longitudinal patient record to support
enhancements in care delivery, outcomes and research and consequently be the basis for further
development of the concept within East London and across a broader geographical footprint.
Analytics capacity and capability
5
Establish governance mechanisms to develop and agree the analytics strategy
Governance structures and processes should be established to enable the analytics strategy for ELHCP
to be developed. The structure should ensure cross-organisation analytics community engagement and
input in order to consider and agree the following:
Consistent data platforms, data management services, structures, data sets, analysis,
application sets and reporting, including where and how existing digital platforms should be
linked, or developed separately, to draw on benefits of each and avoid undue duplication in the
system;
Data quality improvement requirements and standards;
Opportunities for sharing expertise, resource and reporting approaches across clinical pathways
and organisations (see Recommendation 2);
Development of a skills framework, outlining the required analytical capabilities required and an
associated implementation and training plan; and
Identification of population health use cases to ensure data collected are complete and
comparable.
Developing frameworks based on holding health systems to account collectively for health
outcomes, will be required in the future and the effective implementation of the analytics
strategy will be essential to enact this accountability
The STP can support this aspiration by defining the wider governance systems and processes
through which revised accountability frameworks would be enacted.

26 Deloitte Confidential: Public Sector – For Approved External Use
# Recommendations
Alignment of digital, analytics, transformation and commissioning capability to achieve benefit for
patients 6
Assess, design, implement and measure outcome improvement initiatives
Priority patient cohorts in each of the three geographies of the STP should be determined. Specific
analytical resource should be identified to undertake a needs and care pattern assessment, in order to
design an improvement intervention.
Based on Friedman’s Learning Cycle, specifically focusing on developing efferent processes, activities
should include the following:
Population needs assessment completed by the three geographies across the STP;
Each geography within the STP should propose priority patient cohorts aligned with the services
offered, population health need and future demography;
Design outcome measures, metrics and data sets that can form the basis of a process to measure
outcomes;
Measure the impact of interventions, including both (proxy) outcomes and resources utilisation.
Consideration could be given to aligning areas of intervention with existing clinical transformation
programmes, such as primary care quality improvement or the Transforming Services Together
programme; and
Trial advance analytical techniques of actuarial modelling and predictive analysis in these areas
and consider aligning this work with a new mechanism for financial remuneration that rewards
the delivery of reduced care costs across a pathway.
This approach will enable the limited resource available to be focused on clinical areas of high priority
which are aligned with the clinical and service improvement capability required to design and deliver
change and secure an impact in each geography. Iterating this process, based on clinical use case, will
enact the principles within Friedman’s Learning Cycle, build change capability and importantly impact
patient experience and outcomes over time.
The implementation of recommendations should be phased and iterative, supported by regular review,
feedback and amendment to enable responsiveness to patient and staff needs. To assist the Partnership
in progressing to the future state approach, we have developed a series of interim operating models
(IOMS) identifying required activities over time. This approach associated tasks is outlined in detail at
Appendix D
Application mapping, data governance and convergence
7
Work with providers to further enhance common application landscape
In order to support integration and interoperability, common applications should continue to be used
where possible, across the STP. ELHCP should work with provider organisations within the STP to agree
an approach to migrating to a common version of applications in use. Specifically within the BHR system,
consideration should be given to developing a migration path to increase the commonality and
interoperability of system usage, and the functionality of systems in use to focus on the capture of clinical
data sets.
27 Deloitte Confidential: Public Sector – For Approved External Use
# Recommendations
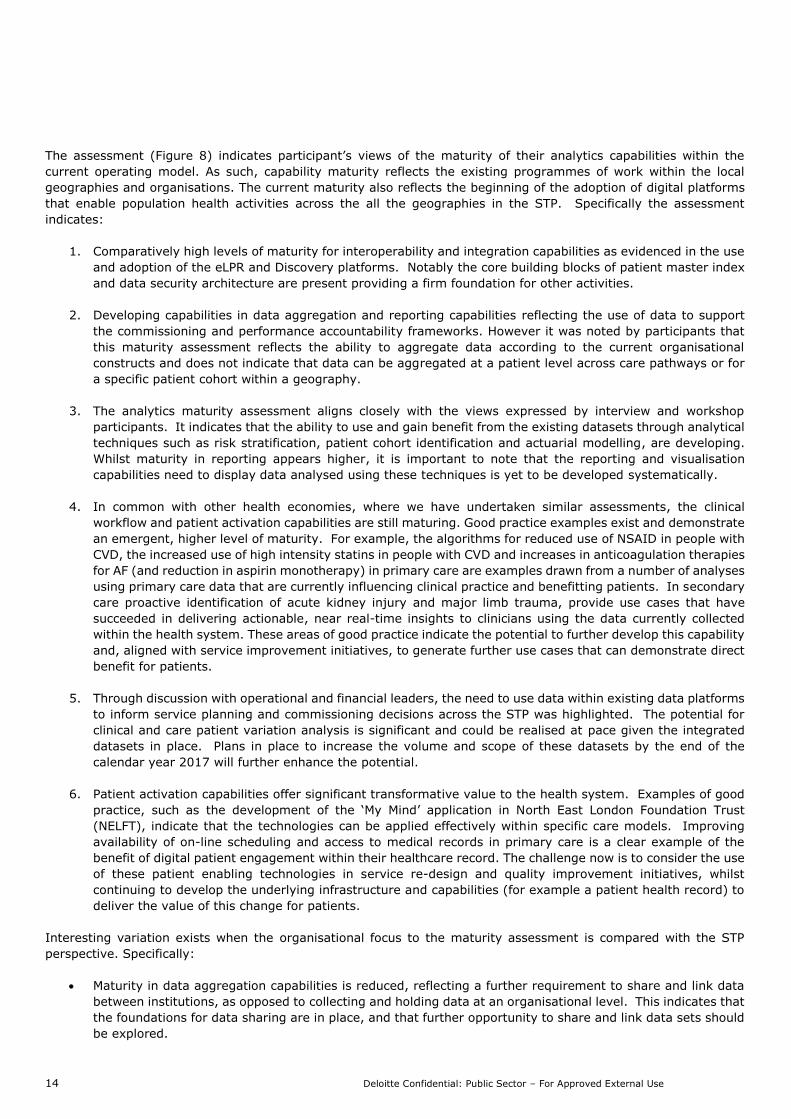
8
Definition of agreed data sets and data definitions, aligned with patient cohorts
A minimum dataset and common data definitions should be agreed for specific patient cohorts. ELHCP
should establish cross-provider groups, based around identified patient cohorts, in order to agree
minimum data sets and data definitions to enable specific service improvement interventions across the
STP.
Additionally, to develop data sharing for the East London Data Repository, commissioners should work
with GPs and Local Authorities to enable sharing of patient-level data on activity, spend/cost and
outcomes (where data is available).
These groups should work under the strategic guidance of an analytics leadership group that defines the
parameters of their work in terms of the analytical tool sets and visualisation applications in use to enable
the display and interpretation of data.
Digital maturity and adoption
9
Incentivise the adoption of improved data collection and quality
In order to support the quality of data at source, existing contractual mechanisms should be used to
focus healthcare provider organisations on data quality. Specific outcome measures, metrics and data
items should be aligned to the use of contractual mechanisms such as CQUINS. By improving data
collection processes at source, data quality and data convergence across providers and patient pathways
will be improved.
Additionally, consideration should be given to aligning increased digital maturity and adoption of
electronic care records with STP accountability and reward mechanisms. This could be agreed in a
progressive manner over time, beginning with incentives to collect data, progressing to reward for
improved data quality, consistency of data item definition and then the analysis and use of data to
provide insight.
10
Develop a plan and pathway to increased digital maturity
An STP-wide plan should be developed to understand the path to increased digital maturity for existing
providers to assess the pace at which full clinical, financial and outcomes data sets will be available to
enable mature population health analytics.
Financial Flow Mechanisms
11
Develop a consistent method and approach to patient level costing across constituent
organisations within the Partnership.
Consistency in patient-level costing should be established. ELHCP should develop a strategy and
approach to the development of patient level costing capability across the partnership. Focus should
shift from setting prices and remunerating care on a fee for services basis. Instead an assessment of
costs in different care settings, and ideally across care pathways, should inform the remuneration of
care.

28 Deloitte Confidential: Public Sector – For Approved External Use
# Recommendations
12
Datasets should align resource to activities at patient level
The development of patient pathway clinical data sets to improve patient care should be prioritised. This
should consider how to align these data sets with the allocation of resource to activities at a patient level.
Such an approach will have the following benefits:
Create a data set of manageable size and complexity to allow for resource identification at patient
level;
Encourage organisations to collaborate on the definition of cost allocation methodologies and use
them consistently across a patient pathway; and
Create the ability to model the financial impact of new models of care through the application of
predictive techniques based on clinically endorsed models of care.
In the absence of open book accounting, system partners may use commissioning spend as a proxy for
cost. Systems should work jointly develop apportionment methodologies at patient level where possible,
and use these to enable initial cohort and pathway analysis.

29 Deloitte Confidential: Public Sector – For Approved External Use
4 Key Observations
We have identified the following observations in performing our assessment, and presented these on a thematic
basis. Associated recommendations, as captured in the Executive Summary and Section 3.4, have been aligned with
each observation. Recommendations have been developed to address multiple observations in some cases.
# Observation
4.1 Inconsistency in understanding and capabilities in respect of population health analytics
4.2 Maturing workstream and STP governance
4.3 Existing datasets may not be complete
4.4 Existing capability is aligned with, and limited by current analytics constructs
4.5 Limited incentives to capture and share data
4.6 Variation in the adoption and use of clinical data platforms
4.7 Challenge identified in the adoption of changes
4.8 Understanding and engagement within the STP on the nature and content of digital platforms remains limited
4.9 Information Governance
4.1 Inconsistency in understanding and capabilities in respect of population health analytics
Observation
The current understanding of population health analytics within stakeholder groups across ELHCP is varied. This
includes variances in both the understanding of the capability requirements for population health analytics, and of
the data platforms and functionality available to ELHCP.
Current understanding of population health analytics is also represented by the difference in the use of analytics
across organisations within the STP. Varying degrees of maturity with respect to population health analytics were
articulated by stakeholders. When considered against the population health analytics maturity framework (section
3.1.1 above, and Appendix B), we have identified variation across geographies in the STP, both in terms of maturity
and understanding of population health analytics capabilities within stakeholder discussions.
Inconsistent knowledge of the available data platforms and their capability was articulated by participants, including
the value to developing care and payment models. Specifically the analytics role within the ELHCP digital workstream
was not well understood by interviewees.
Further impacting the current-state understanding and capabilities is existing operating model for analytics. Current
constructs focus analytics capabilities on transacting commissioning activities and monitoring constitutional and
regulatory performance requirements (as outlined in observation 4.4 below).
Implication
The clarity and depth of understanding of population health analytics requirements, and of the data available, will
inform the approach taken towards the development of population health analytics within constituent organisations
or geographies across ELHCP. The pace of change, and the extent to which efforts are focussed on activities that
will have the greatest impact, may therefore be limited.
# Recommendation
1 Raise awareness of digital platform functionality and capabilities
3 Establish and enabling mechanism for Discovery access and assessment
5 Establish governance mechanisms to develop and agree the analytics strategy

30 Deloitte Confidential: Public Sector – For Approved External Use
4.2 Maturing workstream and STP governance
Observation
Tiered governance mechanisms and structures have been defined for the ELHCP Transformation Programme,
including those of the Digital workstream. Structures are defined for digital enablement groups in each of the
geographies, reporting into the STP-wide Digital Strategy Group. Additionally, requirements for considering and
approving initiatives have been defined, which outline that consideration should be given to the alignment of proposed
initiatives against the strategy, priorities and principles of ELHCP.
However, systematic use of the multiple datasets available to the STP to determine population health need was not
evident. The ability to identify the needs of the population within each geography, or the needs of patients and
service users within constituent organisations, will be essential when determining the priority areas of focus for
population health analytics activities and initiatives.
As identified in 4.1 above, the knowledge and understanding of population health analytics varies across stakeholder
groups and geographies. The governance for the programme continues to mature, and further development is
required to enhance the knowledge and understanding of population health analytics across ELHCP, to effectively
enable population needs assessments.
It was identified that organisational governance supporting the development and direction of analytics is not currently
aligned across the STP. For example, supporting organisational governance structures are aligned with the financial
constructs for existing analytics capabilities (observation 4.4 below), as opposed to the broader application of
population health analytics being developed by ELHCP.
Additionally, we were informed that consistent standards for structured data are not yet defined for use by clinical
services and constituent organisations across ELCHP, leading to the inconsistent the collection and collation of data
items. This effects the ability of ELHCP programme teams to compare data items and data sets across institutions
and has consequent impact on the validity of any comparative analysis or care pattern assessment using these data.
Pockets of good practise and innovative activities were highlighted within workshops and discussions with ELHCP
stakeholders. However, the governance currently in operation does not enable a structured approach to sharing
experiences, mature practise and learnings across constituent organisations for the benefit of the STP and population
health and social care outcomes.
Implication
The implementation of a coherent vision for population health analytics within the STP will require effective
governance, to enable stakeholder engagement and buy-in across organisational boundaries, and support in
establishing common standards within the STP. Additionally, where experiences, learning and good practise is not
effectively shared, there is a risk that improvements and benefits are not made available in a timely and structured
manner to organisations and the population across all geographies.
Furthermore, where population needs are not assessed on a consistent basis, supported by a complete and consistent
dataset, there is a risk that the priority areas for focus cannot be identified. Valuable resources may not be used in
areas that would support the greatest benefit within each organisation geography within the STP.
# Recommendation
2 Define the ELHCP analytics delivery approach
5 Establish governance mechanisms to develop and agree the analytics strategy
10 Develop a plan and pathway to increased digital maturity
4.3 Existing datasets may not be complete
Observation
There is an alignment of clinical applications across ELHCP, including those in use within both the primary and
secondary care settings. A summary of core clinical applications, and integration with the eLPR is outlined in Figure
10 above. This provides a strong basis for further use of data from native systems through aggregation in population
health platforms.

31 Deloitte Confidential: Public Sector – For Approved External Use
While there is a degree of commonality of systems across the STP, a number of challenges were identified which
impact the effectiveness of the datasets available, including:
Availability and completeness of data within datasets: Data is not collected from all organisations within the
STP, whether in the East London Shared Care Record, or in the Discovery platform. Specifically, access to
local authority data remains limited, and in the early stages of aggregation. There is a recognition that the
ability to access local authority data would enable improvements in the delivery of services
Comparability of data: CIOs and transformation practitioners identified challenges as a result of multiple
instances and software versions across the common applications, limiting the value of aggregated data. This
was further compounded by the differing levels of adoption and methods of use of the systems. For example
the same field in the same version of the software may be used to entre different data in hospitals treating
the same patient cohort, thereby making basic activity comparisons between providers challenging.
Linkage of data sets to identify population health need: In addition to availability, the ability to link local
authority data with health care data is challenging, where a common identifier is not available.
Implication
The ability to perform effective population needs assessments, and inform the priority areas of focus for
population health analytics will be limited where the data available to support such assessments is not complete.
There is a risk that areas of focus are not the most appropriate for the population of East London, reducing the
potential impact and improvements in care delivery and outcomes. Additionally, the benefits that may be realised
through collective datasets and analysis will be limited across the STP as a whole, where data from all
organisations is not included.
# Recommendation
7 Work with providers to further enhance common application landscape
8 Definition of agreed data sets and data definitions, aligned with patient cohorts
10 Develop a plan and pathway to increased digital maturity
12 Datasets should align resource to activities at patient level
4.4 Existing capability is aligned with, and limited by, current analytics constructs
Observation
The structure of current analytics functions, associated capability, and supporting data is typically aligned with current
contractual reporting requirements. This includes both statutory reporting for Public Health and social care, and
finance and performance reporting requirements for provider Trusts.
Mature capability was articulated by stakeholders with respect to interoperability and data leakage, and data
management and aggregation, as outlined in figure 8 above, aligned with the current operating model. However,
the development of more advanced population health capability has been limited by the constraints of the current
operating model. We were informed by both operational and clinical stakeholders that limited analytics capacity and
capability is available to support the analysis of the available datasets, including supporting capability provided by
NEL CSU. We were informed that CSU capability was also aligned with the current operating model, and were not
sufficient for future requirements of the STP.
The capacity of the ELHCP programme to deliver population health requirements is limited, placing reliance on
organisations to support in the development of priorities and population health capabilities. However, our assessment
also identified that the capability of both resources and technology across organisations within the STP varies. This
has impacted bot the consistency with which data is collected and available and the extent to which integration and
interoperability is currently possible (as identified in observation 4.3 above).
Organisational capability has impacted the extent to which population health analytics, and the use of data for
purposes outside of the current operating model has progressed within organisations. For example, priority within
Barts Health is given to ensuring the technology infrastructure is maintained, with the adoption of digital working

32 Deloitte Confidential: Public Sector – For Approved External Use
often varying by clinician or service, due to the limitations of available resource and professional capacity to increase
digital maturity.
Implication
The development of capability and availability of rich clinical data is limited by the focus of analytics on financial and
statutory reporting requirements. Consequently, the ability to gain insight and triangulate data sources to predict
or measure the impact of clinical intervention may be further limited. There is a risk that the current capacity is
disproportionately focussed on delivering existing operating model requirements, and that capability is not sufficient
to support the development of population health analytics across all organisations within the STP.
# Recommendation
5 Establish governance mechanisms to develop and agree the analytics strategy
6 Assess, design, implement and measure outcome improvement initiatives
9 Incentivise the adoption of improved data collection and quality
11 Develop a consistent method and approach to patient level costing across constituent organisations within
the Partnership
12 Datasets should align resource to activities at patient level
4.5 Limited incentives to capture and share data
Observation
Capability and capacity for analytics is focussed primarily on ensuring contractual and performance requirements for
reporting can be achieved, and to ensure payments for services being delivered are received (as identified in 4.4).
Stakeholders across health and social care recognised the possible benefits of capturing broader data, there are
currently limited incentives for organisations to capture and report outside of the current analytics constructs and
financial incentives.
Concern was expressed in how broader data, outside of current contractual and reporting requirements, may be used
punitively against provider organisations, resulting in a reluctance to capture and share richer data more broadly. It
is recognised by organisations that there is a need to work collaboratively to enable effective population health, and
support the improvement of outcomes across the STP.
However, current incentives focus on the performance of individual organisations against defined contractual
requirements. Coupled with the fact that organisations are also competing to win and provide services often within
the same geographic footprint, further impacts ability to effectively adapt to a mind-set of collaboration and
openness. This is particularly applicable within the community and mental health settings, where service contracts
are typically competed for on a more frequent basis, both with NHS and private health providers.
Consequently, data, associated analysis and outcomes can have a commercial and competitive ‘value’ which may
impact on the willingness to share data across the STP. Organisations who commented on this situation, recognised
the need to share data to inform population health needs assessment and were keen to do so, but were cognisant of
the possible impact on their ability to compete for service contracts in the future.
Implication
Where incentives are not aligned with embedding data quality improvement and availability of data, the willingness
of health and social care organisations to share information, and to dedicate the necessary capacity and capability
to doing so is likely to be limited.
# Recommendation
5 Develop a data quality improvement strategy
9 Incentivise the adoption of improved data collection and quality
4.6 Variation in the adoption and use of clinical data platforms
Observation
The Discovery platform and eLPR demonstrate mature capability to interoperate and aggregate data across the health

33 Deloitte Confidential: Public Sector – For Approved External Use
and social care geographies within the STP. Furthermore, there are clear plans in place to expand the data coverage
and capabilities going forward, including across mental health and local authority data. Work is ongoing to support
the further development of Discovery, including the implementation of Artificial Intelligence (AI) tools to be provided
by the University of Pennsylvania.
The STP has seen significant adoption and use of the eLPR, with approximately 75,000 views of patient data in
September 2017. The majority of views are recorded across GPs, with Acute, Mental Health and Community Trusts
also accessing the record. GPs stakeholders interviewed as part of the assessment have commented that access to
a broader patient history has enhanced their ability to inform and engage with patients, both in the planning and
delivery of their care. Existing platform provide a good basis for both analysis and reporting and clinical workflow
and patient activation.
However, the eLPR and the Discovery data platforms are not used universally across the STP, including both in the
collection and provision of data, and in accessing the platforms to inform clinical care decisions. While it is understood
that access to the Discovery Data platform has been limited to date, with further work necessary before the platform
and data is made available broadly, the eLPR is available to organisations across the STP. As identified in observation
4.4 above, it is recognised that adoption and use of clinical data platform to inform care decisions is impacted by the
current operating model and reporting requirements.
Implication
Variation in the adoption of the available clinical applications across the STP will contribute to the risk of an incomplete
dataset. While the ability to interpret and act upon data and information will rely on the maturity of clinical capability
within organisations, where datasets are not adopted and used, the ability of the Partnership to leverage the value
of the population health platforms will be limited.
# Recommendation
1 Raise awareness of digital platform functionality and capabilities
3 Establish and enabling mechanism for Discovery access and assessment
4 Support a broader London role in population health analytics
7 Work with providers to further enhance common application landscape
9 Incentivise the adoption of improved data collection and quality
10 Develop a plan and pathway to increased digital maturity
4.7 Challenge identified in the adoption of changes
Observation
It is recognised that East London is innovative, and demonstrating progress in the use of data as an enabler for
delivering population health and improved outcomes for patients and service users. However, the willingness and
ability to adopt changes was identified by participants as a significant barrier to enhancing the consistency with which
data, analytics and technology are currently used to support care delivery within the STP.
Challenges contributing the varied adoption of change have been identified in a number of areas, including:
Patient access to data and information is varied within the STP, with City & Hackney identified as the 3rd
worst region in London for accessing GP online.
There is a perception amongst stakeholder groups that those patients and service users in greatest need are
the least likely to be able to access their data and consequently least willing to engage with health services
digitally.
Varied clinical adoption of technology within Trusts (as identified in 4.4 above). Additionally, some clinicians
expressed the requirement for summary information, as the current information available was, at first use,
difficult to navigate. As such, the inclination to adopt the system was impacted;
Concern over duplication of activities with the STP has limited progress and adoption at local level (for
example, rolling out a patient portal at NELFT, and broader engagement in local authority data sharing –
both of which are perceived as an ELHCP responsibility).

34 Deloitte Confidential: Public Sector – For Approved External Use
While the adoption of change was identified by stakeholders as a barrier for both clinical and patient use of data,
there is currently no systematic and consistent approach to engaging with patients and service users across the STP.
Additionally, there is a need to develop a mechanism to consistently share and learn from good practise across the
STP, in order to support the case for change.
Implication
The ability to collect and use of data will be essential to identify opportunities to adapt the model of care delivery,
and improve outcomes for service users and patients. Where data, analytics and technology are not used in a
consistent manner, the ability to achieve benefits across the STP, focussed on the high priority services (identified
within each region) will be limited.
While there may be a reluctance from patients to use technology, benefits achievable will remain unknown, where
the use of data, analytics and technology is not made available to the population in a consistent manner.
# Recommendation
1 Raise awareness of digital platform functionality and capabilities
3 Establish and enabling mechanism for Discovery access and assessment
6 Assess, design, implement and measure outcome improvement initiatives
9 Incentivise the adoption of improved data collection and quality
4.8 Understanding and engagement within the STP on the nature and content of digital platforms
remains limited
Observation
Efforts have been made by the STP to engage with stakeholder groups across organisations, however the penetration
of engagement is more limited than expected. While communications are perceived to be well-led, Stakeholders
interviewed demonstrated a varied level of understanding and engagement with the Digital Enablement programme
on the nature and content of the digital platforms.
Variance has been apparent between stakeholder groups, and also across organisations as a result of inconsistent
understanding across organisations and stakeholder groups. In particular the level of understanding and engagement
with the programme from the Finance stakeholder group, was lower than amongst the CIO group. While this may
be expected given the technical nature of the changes being progressed, it is by no means a technical project, and
broad engagement across all stakeholder groups will be essential.
We were informed that communications and engagement at leadership level are strong, however there is limited
consistency in ensuring programme information is filtered effectively through organisations within the STP. Local
Authority engagement was also identified as a limitation currently.
Implication
While geographic and historic factors may impact the level of engagement across the STP, it is essential to ensure
the vision for the digital workstream within the ELHCP programme, and progress being made is communicated
effectively to those impacted by the change, and those who will be critical in adopting and driving forward associated
changes. Where this is not the case, there is a risk that benefits will not be realised to the extent expected, or in a
consistent manner. Additionally, valuable input into further development of priority initiatives may not be obtained
where engagement by the STP is not sufficient.
# Recommendation
1 Raise awareness of digital platform functionality and capabilities
5 Establish governance mechanisms to develop and agree the analytics strategy
4.9 Information Governance
Observation
Progress has been made to enable information sharing across the STP, as demonstrated by the eLPR and Discovery

35 Deloitte Confidential: Public Sector – For Approved External Use
platforms. Stakeholders recognised a clear focus on the requirements of Information Governance (IG), including
obtaining patient consent for their data to be used.
However, IG requirements were also identified as a challenge when seeking to share information across the STP. We
are informed that there remains a lack of clarity regarding the role of data controller, where data is shared across
organisational boundaries. In particular, the willingness of GPs to share patient data has been impacted, where there
is a perception that patients are not willing to share their data further.
There is an inconsistent understanding in the best approach to ensuring IG requirements can be met, while also
sharing identifiable patient data across organisational boundaries.
Implication
The ability for organisations within an STP to share and use data at a local level may be limited where IG requirements
are not fully understood and managed effectively to enable the necessary sharing of information. Consequently, the
pace at which data is shared and used to support population health analytics initiatives may be impacted.
# Recommendation
2 Define the ELHCP analytics delivery approach
5 Establish governance mechanisms to develop and agree the analytics strategy

36 Deloitte Confidential: Public Sector – For Approved External Use
Appendix A – Scope and Approach
Scope
B. Assess the maturity of the health analytics capability to support the outputs from four Digital Enablement
workstreams:
i. Shared care records;
ii. Patient enablement;
iii. Advanced system-wide analytics; and
iv. Digital infrastructure.
C. Assess the overall level of analytical maturity.
D. Provide commentary on the STP’s readiness to demonstrate population health capabilities with respect to data
analytics.
E. Provide commentary on the enabling capability of current and planned technology infrastructure.
Methodology and approach
Aligned to the scope of activities:
A. Assess the maturity of the health analytics capability to support the outputs from four Digital Enablement
workstreams:
i. Understand and comment on the objectives, progress and plans of the workstreams to support health
analytics capability, through the following lenses and key lines of enquiry:
i. Operational: capability to operationalise place-based health analytics to embed data
analytics into day-to-day working, enable the delivery of new clinical workflows and support
patient self-help and direct engagement in their care;
ii. Clinical: capability to harness health analytics to enable governance and delivery of clinical
care and associated research requirements through technology-enabled place-based care
models;
iii. Financial: capability to use health analytics to understand and create mechanisms to
manage financial flows and payment mechanisms to support the achievement of place-based
care outcomes;
iv. Technical: capability of technology, analytics and associated governance frameworks to
deliver and scale to provide the technology infrastructure required to support place-based
care.
ii. Assess through desktop review of Digital Enablement documentation and interviews with ELHCP
senior leadership.
B. Assess the overall level of analytical maturity.
i. Plot the Digital Enablement current position against Deloitte’s Health IT & Data Analytics Capabilities
and Maturity Framework, in order to assess maturity.
ii. Consider the current position against key enabling capabilities (interoperability, data aggregation and
management, risk stratification, reporting, clinical workflow and patient engagement).
iii. Conduct workshops to understand the perspectives of the following groups on: clinicians, patients,
informatics teams, ELHCP leadership.

37 Deloitte Confidential: Public Sector – For Approved External Use
C. Provide commentary on the ELHCP’s readiness to demonstrate population health capabilities with respect to
data analytics.
i. Define and agree expectations of the population health analytics criteria for STPs based on wider
NHS and global experience of place-based health system approaches.
ii. Compare findings on health analytics capabilities to the above criteria, taking into account enabling
processes such as workforce capability, information governance, identification of relevant clinical use
cases and clinical engagement, as factors to enhance maturity and readiness.
D. Provide commentary on the enabling capability of current and planned technology infrastructure:
i. Understand and comment on the nature of technology platforms used to deliver health analytics and
supporting technology infrastructure, including provider patient record applications, as a basis to
support the required activities of population health data analytics.
ii. Understand and comment on technology infrastructure enhancement plans as set out in the Local
Digital Roadmap.
iii. Compare findings to our wider knowledge of other population health initiatives.

38 Deloitte Confidential: Public Sector – For Approved External Use
Appendix B – Population Health Analytics
Maturity Matrix
In order to support the assessment, health analytics function capabilities were considered against a maturity matrix, as outlined below.
We are able to draw upon Deloitte’s international experience in the assessment and implementation of Accountable Care Organisation systems in the
US to establish a population health analytics maturity matrix against which existing capabilities can be assessed in a consistent manner. The maturity
matrix is outlined below, summarising mature-state practices in each area.
Figure 14: Maturity matrix highlighting innovative practices
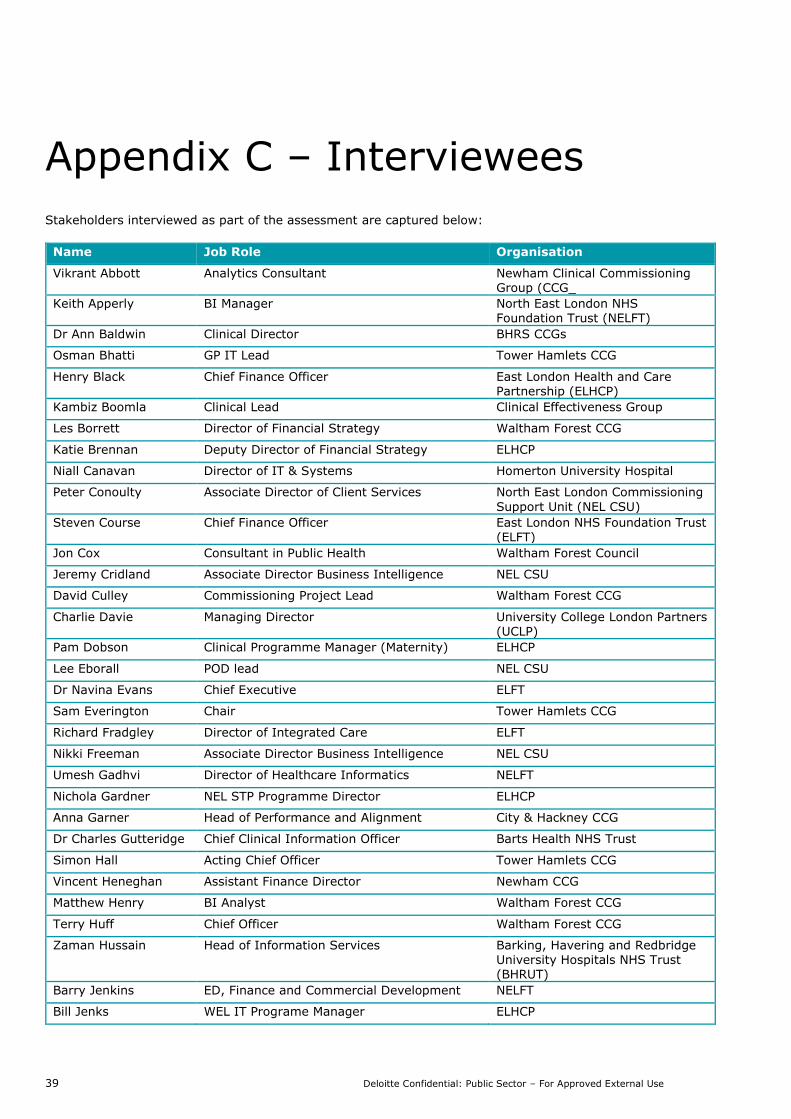
39 Deloitte Confidential: Public Sector – For Approved External Use
Appendix C – Interviewees
Stakeholders interviewed as part of the assessment are captured below:
Name Job Role Organisation
Vikrant Abbott Analytics Consultant Newham Clinical Commissioning Group (CCG_
Keith Apperly BI Manager North East London NHS Foundation Trust (NELFT)
Dr Ann Baldwin Clinical Director BHRS CCGs
Osman Bhatti GP IT Lead Tower Hamlets CCG
Henry Black Chief Finance Officer East London Health and Care Partnership (ELHCP)
Kambiz Boomla Clinical Lead Clinical Effectiveness Group
Les Borrett Director of Financial Strategy Waltham Forest CCG
Katie Brennan Deputy Director of Financial Strategy ELHCP
Niall Canavan Director of IT & Systems Homerton University Hospital
Peter Conoulty Associate Director of Client Services North East London Commissioning
Support Unit (NEL CSU)
Steven Course Chief Finance Officer East London NHS Foundation Trust (ELFT)
Jon Cox Consultant in Public Health Waltham Forest Council
Jeremy Cridland Associate Director Business Intelligence NEL CSU
David Culley Commissioning Project Lead Waltham Forest CCG
Charlie Davie Managing Director University College London Partners (UCLP)
Pam Dobson Clinical Programme Manager (Maternity) ELHCP
Lee Eborall POD lead NEL CSU
Dr Navina Evans Chief Executive ELFT
Sam Everington Chair Tower Hamlets CCG
Richard Fradgley Director of Integrated Care ELFT
Nikki Freeman Associate Director Business Intelligence NEL CSU
Umesh Gadhvi Director of Healthcare Informatics NELFT
Nichola Gardner NEL STP Programme Director ELHCP
Anna Garner Head of Performance and Alignment City & Hackney CCG
Dr Charles Gutteridge Chief Clinical Information Officer Barts Health NHS Trust
Simon Hall Acting Chief Officer Tower Hamlets CCG
Vincent Heneghan Assistant Finance Director Newham CCG
Matthew Henry BI Analyst Waltham Forest CCG
Terry Huff Chief Officer Waltham Forest CCG
Zaman Hussain Head of Information Services Barking, Havering and Redbridge University Hospitals NHS Trust
(BHRUT)
Barry Jenkins ED, Finance and Commercial Development NELFT
Bill Jenks WEL IT Programe Manager ELHCP
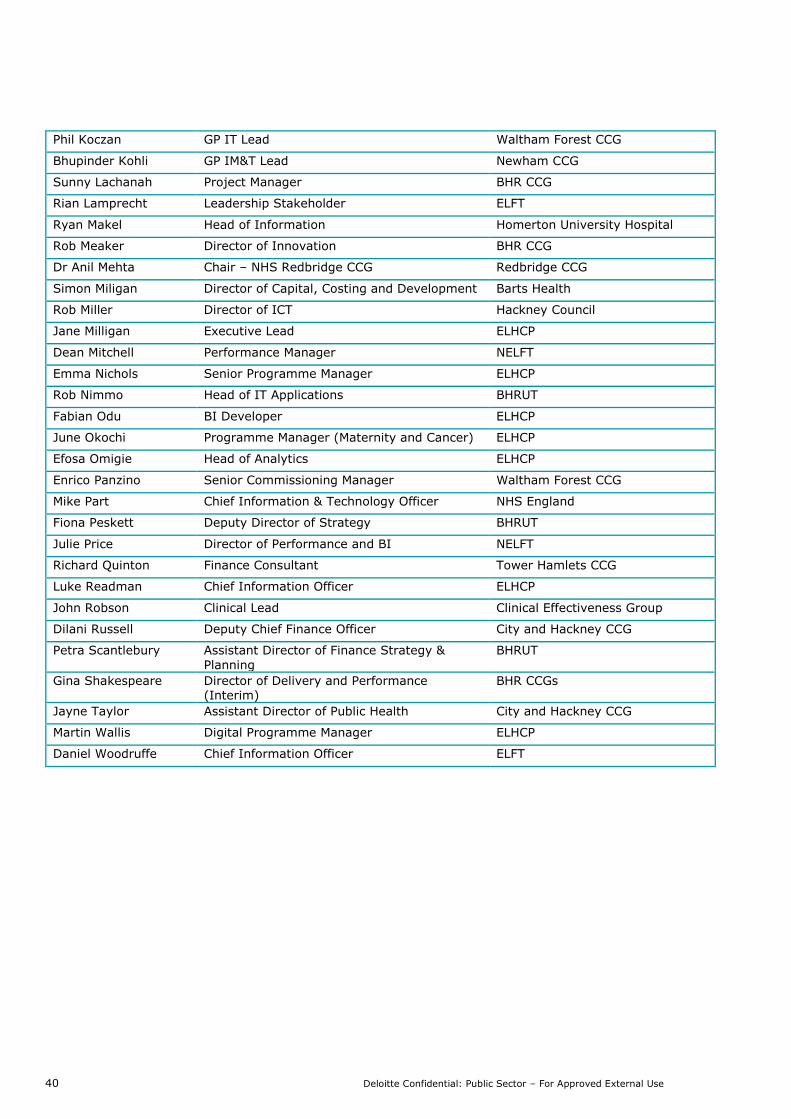
40 Deloitte Confidential: Public Sector – For Approved External Use
Phil Koczan GP IT Lead Waltham Forest CCG
Bhupinder Kohli GP IM&T Lead Newham CCG
Sunny Lachanah Project Manager BHR CCG
Rian Lamprecht Leadership Stakeholder ELFT
Ryan Makel Head of Information Homerton University Hospital
Rob Meaker Director of Innovation BHR CCG
Dr Anil Mehta Chair – NHS Redbridge CCG Redbridge CCG
Simon Miligan Director of Capital, Costing and Development Barts Health
Rob Miller Director of ICT Hackney Council
Jane Milligan Executive Lead ELHCP
Dean Mitchell Performance Manager NELFT
Emma Nichols Senior Programme Manager ELHCP
Rob Nimmo Head of IT Applications BHRUT
Fabian Odu BI Developer ELHCP
June Okochi Programme Manager (Maternity and Cancer) ELHCP
Efosa Omigie Head of Analytics ELHCP
Enrico Panzino Senior Commissioning Manager Waltham Forest CCG
Mike Part Chief Information & Technology Officer NHS England
Fiona Peskett Deputy Director of Strategy BHRUT
Julie Price Director of Performance and BI NELFT
Richard Quinton Finance Consultant Tower Hamlets CCG
Luke Readman Chief Information Officer ELHCP
John Robson Clinical Lead Clinical Effectiveness Group
Dilani Russell Deputy Chief Finance Officer City and Hackney CCG
Petra Scantlebury Assistant Director of Finance Strategy &
Planning
BHRUT
Gina Shakespeare Director of Delivery and Performance (Interim)
BHR CCGs
Jayne Taylor Assistant Director of Public Health City and Hackney CCG
Martin Wallis Digital Programme Manager ELHCP
Daniel Woodruffe Chief Information Officer ELFT

41 Deloitte Confidential: Public Sector – For Approved External Use
Appendix D – Interim Operating Models
To assist the Partnership in progressing to the future state, we have developed the proposed interim operating models (IOMS), and supporting
activities over time, as outlined below.

42 Deloitte Confidential: Public Sector – For Approved External Use
ELHCP have complementary capabilities that, when aligned to improve, can support the health outcomes of the local
population. The interim operating models proposed outline activities over time that could assist in realising this
potential. Here we summarise the approach aligning these capabilities for maximum benefit:
1. Engage clinical and operational leaders in the scope and content of the information within the Discovery
Platform;
2. Develop a supported method to assist programme leaders to define key questions they would like to ask of
this data source;
3. Align this supported method to known population health needs assessments and identified priority activities;
4. Formulate questions to establish care pattern assessment and build patient profiles aligned to risk stratified
patient cohorts;
5. Align financial flows and patient-level costing approaches to establish the current resource profile of these
patient cohorts;
6. Working with clinical leaders define a proposed clinical model based on efficacious interventions, consider
adopted digital capability to deliver this service model, as appropriate to the patient cohort;
7. Invest in, and pilot, an alternative service model, leveraging existing good practice, such as social prescribing,
and existing quality improvement methods within primary, secondary and community care;
8. Define a commissioning model that incentivises the proposed care model and promotes high quality data
collection through reward for data accuracy, completeness and coverage;
9. Establish an agreed data set and monitoring method with service providers and clinical teams, use the eLPR
and other clinical data sets as appropriate to measure the care pattern of the target population, including
developing a visualisation of care interventions on as near real-time a basis as possible; and
10. Engage clinical teams in monitoring the impact of their intervention through a defined and regular cadence
of information to reflect patient system usage.
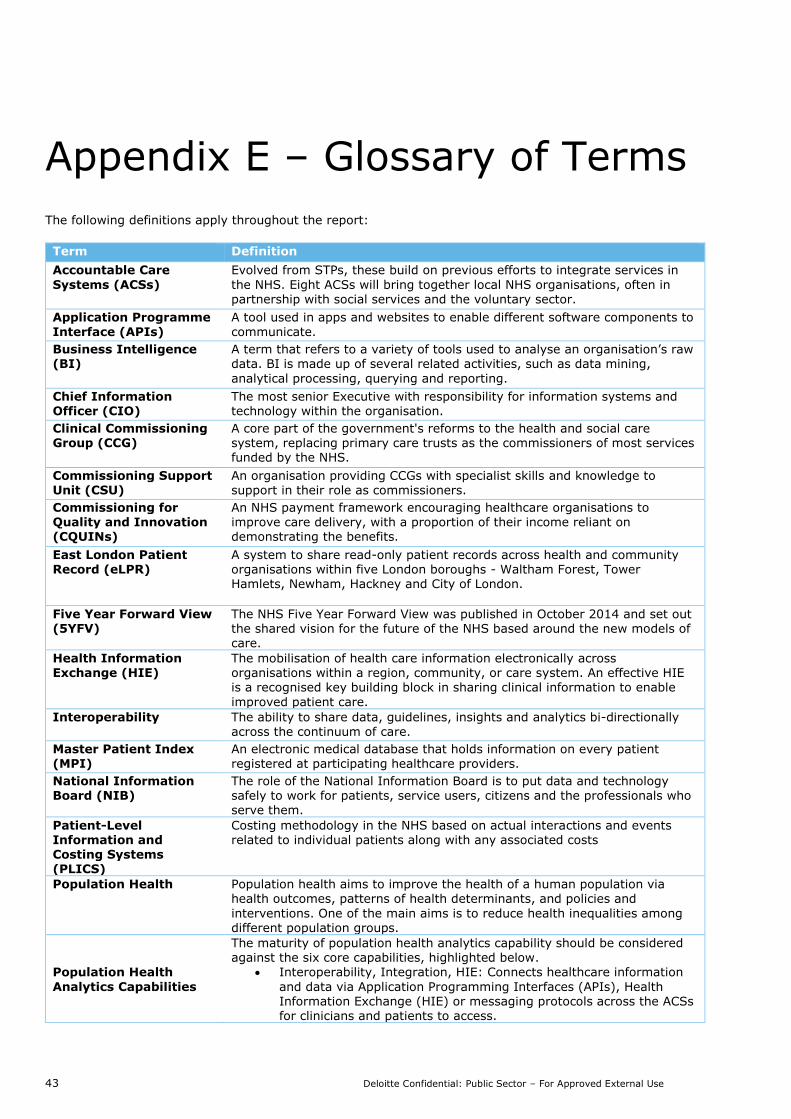
43 Deloitte Confidential: Public Sector – For Approved External Use
Appendix E – Glossary of Terms
The following definitions apply throughout the report:
Term Definition
Accountable Care
Systems (ACSs)
Evolved from STPs, these build on previous efforts to integrate services in
the NHS. Eight ACSs will bring together local NHS organisations, often in partnership with social services and the voluntary sector.
Application Programme
Interface (APIs)
A tool used in apps and websites to enable different software components to
communicate.
Business Intelligence (BI)
A term that refers to a variety of tools used to analyse an organisation’s raw data. BI is made up of several related activities, such as data mining,
analytical processing, querying and reporting.
Chief Information Officer (CIO)
The most senior Executive with responsibility for information systems and technology within the organisation.
Clinical Commissioning Group (CCG)
A core part of the government's reforms to the health and social care system, replacing primary care trusts as the commissioners of most services funded by the NHS.
Commissioning Support Unit (CSU)
An organisation providing CCGs with specialist skills and knowledge to support in their role as commissioners.
Commissioning for Quality and Innovation (CQUINs)
An NHS payment framework encouraging healthcare organisations to improve care delivery, with a proportion of their income reliant on demonstrating the benefits.
East London Patient Record (eLPR)
A system to share read-only patient records across health and community organisations within five London boroughs - Waltham Forest, Tower Hamlets, Newham, Hackney and City of London.
Five Year Forward View (5YFV)
The NHS Five Year Forward View was published in October 2014 and set out the shared vision for the future of the NHS based around the new models of care.
Health Information Exchange (HIE)
The mobilisation of health care information electronically across organisations within a region, community, or care system. An effective HIE is a recognised key building block in sharing clinical information to enable
improved patient care.
Interoperability The ability to share data, guidelines, insights and analytics bi-directionally across the continuum of care.
Master Patient Index
(MPI)
An electronic medical database that holds information on every patient
registered at participating healthcare providers.
National Information Board (NIB)
The role of the National Information Board is to put data and technology safely to work for patients, service users, citizens and the professionals who serve them.
Patient-Level Information and Costing Systems (PLICS)
Costing methodology in the NHS based on actual interactions and events related to individual patients along with any associated costs
Population Health Population health aims to improve the health of a human population via health outcomes, patterns of health determinants, and policies and
interventions. One of the main aims is to reduce health inequalities among different population groups.
Population Health
Analytics Capabilities
The maturity of population health analytics capability should be considered against the six core capabilities, highlighted below.
Interoperability, Integration, HIE: Connects healthcare information
and data via Application Programming Interfaces (APIs), Health Information Exchange (HIE) or messaging protocols across the ACSs for clinicians and patients to access.

44 Deloitte Confidential: Public Sector – For Approved External Use
Data Aggregation and Management: Aggregates data from disparate sources to improve transparency
Analytics (including Risk Stratification): Enables Insight driven analysis that is both descriptive and prescriptive
Reporting: Delivers a self-serve solution for performance management
Clinical Workflow: Orchestrates the execution of activities from disparate systems constituting care continuum
Patient Activation: Enables the patient to manage their own care
needs and drives required clinical workflow.
We have used this taxonomy, developed through extensive use in US health systems, to inform our assessment of the existing portfolio of analytics
functions across ELHCP.
Risk Stratification A tool for identifying and predicting population groups which are high risk and prioritising the management of their care.
Secondary Uses Service (SUS)
A repository for healthcare data in England which enables a range of reporting and analyses to support the NHS in the delivery of healthcare services.
Service Line Reporting (SLR)
Provides data on financial performance, quality, staffing etc. based along service line management structures.
Sustainability and Transformation Plans (STPs)
NHS and local councils working in partnership in 44 areas across England to develop proposals for improvement to health and care across the country.
Vanguard Programme As part of the new care models programme, 50 organisations were selected as vanguards to take the first steps towards delivering the Five Year Forward View and supporting improvement and integration of services. There are five
vanguard types: integrated primary and acute care systems; multi-specialty community providers; enhanced health in care homes; urgent and emergency care; and acute care collaborations.

45 Deloitte Confidential: Public Sector – For Approved External Use
Statement of Responsibility
We take responsibility for this report which is prepared on the basis of the limitations set out below. The matters
raised in this report are only those which came to our attention during the course of our work and are not necessarily
a comprehensive statement of all the weaknesses that may exist or all improvements that might be made. Any
recommendations made for improvements should be assessed by you for their full impact before they are
implemented.
Other than as stated below, this document is confidential and prepared solely for your information and that of other
beneficiaries of our advice listed in our engagement letter. Therefore you should not, refer to or use our name or
this document for any other purpose, disclose them or refer to them in any prospectus or other document, or make
them available or communicate them to any other party. If this document contains details of an arrangement that
could result in a tax or National Insurance saving, no such conditions of confidentiality apply to the details of that
arrangement (for example, for the purpose of discussion with tax authorities). In any event, no other party is entitled
to rely on our document for any purpose whatsoever and thus we accept no liability to any other party who is shown
or gains access to this document.
Deloitte LLP
London
February 2018
Deloitte LLP is a limited liability partnership registered in England and Wales with registered number OC303675 and
its registered office at 2 New Street Square, London EC4A 3BZ, United Kingdom.
Deloitte LLP is the United Kingdom affiliate of Deloitte NWE LLP, a member firm of Deloitte Touche Tohmatsu Limited,
a UK private company limited by guarantee (“DTTL”). DTTL and each of its member firms are legally separate and
independent entities. DTTL and Deloitte NWE LLP do not provide services to clients. Please see
www.deloitte.com/about to learn more about our global network of member firms.
© 2018 Deloitte LLP. All rights reserved.