Embed Size (px)
Citation preview

EASL 2011 31 March 2011 - Berlin, Germany
Impact of IL28B Genotype and Pre-treatment Serum IP-10 in Treatment-Naïve Genotype 1
HCV Patients Treated with TMC435 in Combination with Peginterferon a-2a and
Ribavirin in the PILLAR Study
Jeroen AERSSENS,1 Greg FANNING,2 Annick SCHOLLIERS,3 Oliver LENZ,4 Monika PEETERS,5 Goedele DE SMEDT,6
Michael W FRIED7
1Department of Translational Genomics & Genetics; 2Department of Infectious Disease and Vaccines; 3Department of Enabling Biology; 4Department of Clinical Virology; 5Department of Statistics;
6Department of Clinical Development, Tibotec, Beerse, Belgium; 7University of North Carolina at Chapel Hill, Chapel Hill, NC, USA

Disclosures
Jeroen Aerssens Greg Fanning Annick Scholliers Oliver Lenz Monika Peeters Goedele De Smedt Michael W Fried
TMC435 is an investigational product for hepatitis C virus (HCV) treatment, under development by Tibotec (part of the Janssen Pharmaceutical Companies of Johnson & Johnson)
Employed by Tibotec, stock/shareholder J&J
Employed by Tibotec, stock/shareholder J&J
Employed by Tibotec
Employed by Tibotec, stock/shareholder J&J
Employed by Tibotec, stock/shareholder J&J
Employed by Tibotec, stock/shareholder J&J
Grants/Research Support, Consultant (Roche, Merck, Human Genome Sciences, Vertex, Tibotec, Bristol-Myers Squibb, Anadys, Conatus, Schering, Pharmasset, Glaxo, Novartis), Stock/Shareholder (Pharmasset)

Background: IL28B genotype and virologic response during treatment with PegIFN/RBV
Pro
port
ion
of p
atie
nts
achi
evin
g
viro
logi
c re
spon
se (
%)
cEVR, complete early virologic response; IL28B CC/CT/TT, rs12979860 polymorphism; PegIFN, pegylated interferon α-2a; RBV, ribavirin; RVR, rapid virologic response; SVR, sustained virologic response
Thompson et al. Gastroenterology 2010; 139:120-129
RVR(week 4)
Treatment-naïve, HCV genotype 1, Caucasian patients (n=1171)PegIFN/RBV treatment
cEVR(week 12) SVR
p<0.0001 p<0.0001 p<0.0001
5% 5%
28% 28%
38%
87%
27%33%
69%
TT CT CC TT CT CC TT CT CC

Background: Pre-treatment serum IP-10 and virologic response during treatment with PegIFN/RBV
< 150 150-600
> 6000%
20%
40%
60%
80%
100%
n=47 n=102 n=24
68%
55%
21%
IP-10 at baseline (pg/ml)
p=0.003
p=0.0002
Pro
po
rtio
n o
f p
atie
nts
ach
ievi
ng
vi
rolo
gic
res
po
nse
(%
): S
VR
IP-10 (pg/mL) at baseline
Lagging et al. Hepatology 2006; 44:1617-1625
IP-10, interferon- inducible protein 10; PegIFN, pegylated interferon α-2a; RBV, ribavirin; SVR, sustained virologic response, HCV RNA <25 IU/mL (undetectable)
Treatment-naïve, HCV genotype 1, European patients (n=173)PegIFN/RBV treatment

Background: Pre-treatment serum IP-10 improves predictive value of IL28B for PegIFN/RBV treatment responseIL28B genotype and pre-treatment serum IP-10 are independent and additive factors to predict sustained virologic response (SVR)
IL28B TT/CT/CC, rs12979860 polymorphism; IP-10, interferon- inducible protein 10; PegIFN, pegylated interferon α-2a; RBV, ribavirin
TT
CT
CC
010203040
50
60
70
80
90
< 600 pg/ml
≥ 600 pg/mlSerum IP-10 concentration
IL28B genotype
% p
atie
nts
with
SV
R
20%
89%
79%
64%
24%
48%
ViraHepC cohort (n=210)HCV genotype 1
Overall SVR = 59%
Likelihood ratio Chi2 = 55
p<0.0001
Darling et al. Hepatology 2011; 53:14-22

Evaluate the relationship of IL28B genotype and/or pre-treatment serum IP-10 level with on-treatment virologic response up to Week 24 in the TMC435 PILLAR study– TMC435 is a once-daily oral HCV NS3/4A protease
inhibitor – PILLAR (TMC435-C205; NCT00882908) is a Phase IIb,
randomised, double-blind, placebo-controlled study in treatment-naïve genotype 1 HCV patients treated with TMC435 in combination with PegIFN/RBV
IL28B and IP-10 analyses: Objective
Fried et al. AASLD 2010
IL28B, rs12979860 polymorphism; IP-10, interferon- inducible protein 10; PegIFN, pegylated interferon α-2a; RBV, ribavirin.

PILLAR study design
Pbo24/PR48, placebo and PegIFN/RBV for 24 weeks followed by PegIFN/RBV for 24 weeks; TMC12/PR24, TMC435 + PegIFN/RBV for 12 weeks followed by PegIFN/RBV for 24 weeks (PegIFN/RBV, peginterferon -2a [180 g/wk] + ribavirin [1000–1200 mg/day]); TMC24/PR24, TMC435 + PegIFN/RBV for 24 weeks; all TMC435 doses administered once-daily; FU, follow-up; IL28B, rs12979860 polymorphism; IP-10, interferon- inducible protein 10; ITT, intent to treat; Pbo, placebo; TMC, TMC435.
Week 0 12 24 7248
Pbo & PegIFN/RBV
TMC435 75 mg & PegIFN/RBV
TMC435 75 mg & PegIFN/RBV
TMC435 150 mg & PegIFN/RBV
PegIFN/RBV
N=78
N=75
N=79
N=77
N=ITT
TMC12/PR24 75 mg
TMC24/PR24 75 mg
TMC24/PR24 150 mg
Pbo24 / PR48
Pbo & PegIFN/RBV
TMC435 150 mg & PegIFN/RBV
Pbo & PegIFN/RBV
N=77TMC12/PR24 150 mg
Post-therapy FU
Post-therapy FU
Post-therapy FU
4
N=58
N=51
N=52
N=46
N=55
For IL28B and IP-10 analyses, dose groups were pooled 68% of patients (262 out of 386) consented for DNA research (including IL28B genotyping)
Consented for DNA research
Post-therapy FUPegIFN/RBV
Post-therapy FUPost-therapy FU
Post-therapy FUPegIFN/RBV
Post-therapy FUPost-therapy FU
Post-therapy FUPegIFN/RBV
Post-therapy FUPost-therapy FU
Post-therapy FUPegIFN/RBV
Post-therapy FUPost-therapy FU
* RGT: Response-guided treatment duration in TMC435 arms
RGT*
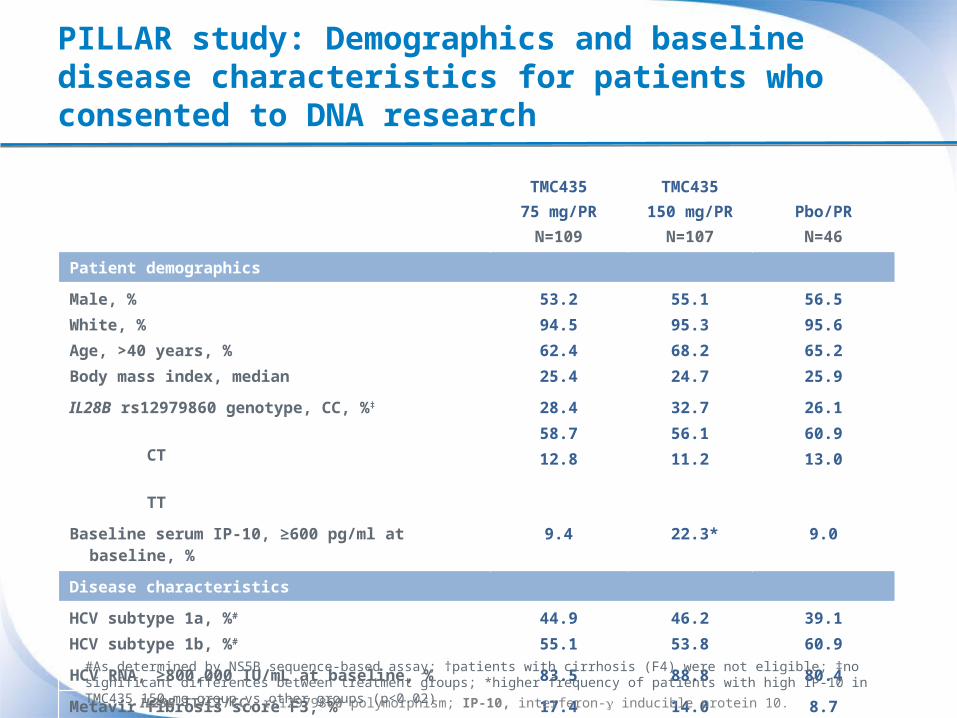
PILLAR study: Demographics and baseline disease characteristics for patients who consented to DNA research
TMC43575 mg/PR
N=109
TMC435150 mg/PR
N=107Pbo/PR
N=46
Patient demographics
Male, %White, %Age, >40 years, %Body mass index, median
53.294.562.425.4
55.195.368.224.7
56.595.665.225.9
IL28B rs12979860 genotype, CC, %‡
CT TT
28.458.712.8
32.756.111.2
26.160.913.0
Baseline serum IP-10, ≥600 pg/ml at baseline, % 9.4 22.3* 9.0
Disease characteristics
HCV subtype 1a, %#
HCV subtype 1b, %#
44.955.1
46.253.8
39.160.9
HCV RNA, ≥800,000 IU/mL at baseline, % 83.5 88.8 80.4
Metavir fibrosis score F3, %† 17.4 14.0 8.7
IL28B TT/CT/CC, rs12979860 polymorphism; IP-10, interferon- inducible protein 10.
#As determined by NS5B sequence-based assay; †patients with cirrhosis (F4) were not eligible; ‡no significant differences between treatment groups; *higher frequency of patients with high IP-10 in TMC435 150 mg group vs other groups (p<0.02)

PILLAR: On-treatment virologic response up to Week 24 by IL28B genotype
The data analysis excluded missing values.CC/CT/TT, rs12979860 polymorphism; N.S., not significant; PegIFN, pegylated interferon α-2a; RBV, ribavirin.
n=28
Virologic response: HCV RNA <25 IU/ml (detectable or undetectable)
Pearson Chi2 test
Pro
port
ion
of p
atie
nts
(%)
p<0.04p<0.01N.S.
n=6
n=12
Placebo + PegIFN/RBV

PILLAR: On-treatment virologic response up to Week 24 by IL28B genotype
Virologic response: HCV RNA <25 IU/ml (detectable or undetectable)
n=64
n=6
n=28
n=12
n=12n=60
n=35
n=14
n=31
TMC435 75 mg + PegIFN/RBV
TMC435 150 mg + PegIFN/RBV
Pro
port
ion
of p
atie
nts
(%)
N.S. p<0.003p<0.003 N.S. N.S.N.S.Pearson Chi2 test
N.S. p<0.04p<0.01
The data analysis excluded missing values.CC/CT/TT, rs12979860 polymorphism; N.S., not significant; PegIFN, pegylated interferon α-2a; RBV, ribavirin.
Placebo + PegIFN/RBV

PILLAR: On-treatment virologic response up to Week 24 by baseline serum IP-10
n=4
n=40
N.S. N.S.N.S.
Virologic response: HCV RNA <25 IU/ml (detectable or undetectable)
Low (<600 pg/mL)High (≥600 pg/mL)
Baseline IP-10
Pro
port
ion
of p
atie
nts
(%)
The data analysed excluded missing values.IP-10, interferon- inducible protein 10; N.S., not significant; PegIFN, pegylated interferon α-2a; RBV, ribavirin.
Placebo + PegIFN/RBV
Pearson Chi2 test

PILLAR: On-treatment virologic response up to Week 24 by baseline serum IP-10
n=96
n=4
n=40
n=23n=80
n=10
N.S. N.S.N.S. N.S. N.S.N.S. N.S. N.S.N.S.
Pearson Chi2 test
Virologic response: HCV RNA <25 IU/ml (detectable or undetectable)
Low (<600 pg/mL)High (≥600 pg/mL)
Baseline IP-10
Pro
port
ion
of p
atie
nts
(%)
The data analysed excluded missing values.IP-10, interferon- inducible protein 10; N.S., not significant; PegIFN, pegylated interferon α-2a; RBV, ribavirin.
Placebo + PegIFN/RBV
TMC435 75 mg + PegIFN/RBV
TMC435 150 mg + PegIFN/RBV

PILLAR: On-treatment virologic response up to Week 24 by IL28B genotype/baseline serum IP-10 combined: Placebo + PegIFN/RBV
IL28B CC/CT/TT, rs12979860 polymorphism; IP-10, interferon- inducible protein 10;PegIFN, pegylated interferon α-2a; RBV, ribavirin
Virologic response: HCV RNA <25 IU/ml (detectable or undetectable)
TT
CT
CC
0
20
40
60
80
100
< 600 pg/ml
≥ 600 pg/ml
TT
CT
CC
0
20
40
60
80
100
< 600 pg/ml
≥ 600 pg/mlTT
CT
CC
0
20
40
60
80
100
< 600 pg/ml
≥ 600 pg/ml
20%
5%
17%
0%
40%
57%
100%
25%
40%
77%
100%
50%
Week 4 Week 12 Week 24
IL28
B
IP-10
IL28
B
IL28
B
IP-10IP-10
Pro
por
tion
of p
atie
nts
(%)
nIL28B
TT CT CCIP-10 Low 5 23 12IP-10 High 0 4 0

PILLAR: On-treatment virologic response up to Week 24 by IL28B genotype/baseline serum IP-10 combined: TMC435 75 mg + PegIFN/RBV
Virologic response: HCV RNA <25 IU/ml (detectable or undetectable)
TT
CT
CC
0
20
40
60
80
100
< 600 pg/ml
≥ 600 pg/ml
TT
CT
CC
0
20
40
60
80
100
< 600 pg/ml
≥ 600 pg/ml
67%
96%
100%
100%
100%100%
IL28
B
IP-10
TT
CT
CC
0
20
40
60
80
100
< 600 pg/ml
≥ 600 pg/ml
67%
100%
100%100%
67%
96%
100%
100%86%
93%100%
100%
IL28
B
IL28
B
IP-10IP-10
Week 4 Week 12 Week 24
Pro
por
tion
of p
atie
nts
(%)
nIL28B
TT CT CCIP-10 Low 12 56 28IP-10 High 1 6 3
n=1n=1n=1
IL28B CC/CT/TT, rs12979860 polymorphism; IP-10, interferon- inducible protein 10;PegIFN, pegylated interferon α-2a; RBV, ribavirin

PILLAR: On-treatment virologic response up to Week 24 by IL28B genotype/baseline serum IP-10 combined: TMC435 150 mg + PegIFN/RBV
TT
CT
CC
0
20
40
60
80
100
< 600 pg/ml
≥ 600 pg/ml
83%
95%
100%
100%
100%
90%
TT
CT
CC
0
20
40
60
80
100
< 600 pg/ml
≥ 600 pg/ml
100%
95%100%
100%
100%
77%
TT
CT
CC
0
20
40
60
80
100
< 600 pg/ml
≥ 600 pg/ml
100%100%
77%
100%95%96%
Week 4 Week 12 Week 24
Virologic response: HCV RNA <25 IU/ml (detectable or undetectable)
IL28
B
IP-10
IL28
B
IL28
B
IP-10IP-10
Pro
por
tion
of p
atie
nts
(%)
nIL28B
TT CT CCIP-10 Low 19 100 55IP-10 High 5 19 9IL28B CC/CT/TT, rs12979860 polymorphism; IP-10, interferon- inducible protein 10;
PegIFN, pegylated interferon α-2a; RBV, ribavirin

Summary
During the first 24 weeks of treatment in the PILLAR study:
– In the control group, treated with placebo and PegIFN/RBV, IL28B CC genotype and low baseline serum IP-10 levels were associated with the highest virologic response
– In patients treated with TMC435 in combination with PegIFN/RBV, high virologic response rates were observed, regardless of IL28B genotype and/or baseline serum IP-10
– The highest response for IL28B TT genotype was observed in TMC435 150 mg group
IL28B, rs12979860 polymorphism; IP-10, interferon- inducible protein 10; PegIFN, pegylated interferon α-2a; RBV, ribavirin

Conclusions
The addition of TMC435 to PegIFN/RBV reduces the impact of IL28B genotype and/or baseline serum IP-10 on virologic response up to 24 weeks of treatment
Evaluation of the potential impact of these markers on sustained virologic response (SVR) in triple combination therapy will be assessed in the Phase IIb and Phase III trials
IL28B, rs12979860 polymorphism; IP-10, interferon- inducible protein 10; PegIFN, pegylated interferon α-2a; RBV, ribavirin

Acknowledgements
New Zealand
• Ed Gane, Auckland
• Catherine Stedman, Christchurch
• Graeme Dickson, Hamilton
Norway
• Trond Bruun, Bergen
• Bent von der Lippe, Kirkeveien
• Zbigniev Konopski, Trondheimsveien
• Kjell Block Hellum, Sykehusveien
• Jon Florholmen, Tromso
Poland
• Robert Flisiak, Bialystok
• Andrzej Horban, Warszawa
• Waldemar Halota, Bydgoszcz
• Wieslaw Kryczka, Kielce
• Maciej Jablkowski, Lodz
• Ewa Janczewska-Kazek, Czeladz
Russia
• Alexey A. Yakovlev, Saint Petersburg
• Vladimir V. Rafalskiy, Smolensk
• Evgeny E. Voronin, Saint Petersburg
• N Zakharova, Saint Petersburg
• Igor G. Nikitin, Moscow
• Pavel O. Bogomolov, Moscow
• Vladimir T. Ivashkin, Moscow
• Vyacheslav G. Morozov, Samara
The patients and their families The PILLAR investigators and their study staff
• Olga V. Korochkina, Nizhny
• Novgorod
Spain
• Maria Buti, Barcelona
• Moises Diago, Valencia
• Ricardo Moreno-Otero, Madrid
• Manuel Romero, Sevilla
• Jose Luis Calleja, Madrid
Germany
• Keikawus Arasteh, Berlin
• Thomas Berg, Berlin
• Peter Buggisch, Hamburg
• Hartwig Klinker, Würzburg
• Andreas Trein, Stuttgart
• Tobias Goeser, Köln
• Stefan Mauss, Düsseldorf
• Dr Jens Rasenack, Freiburg
• Stefan Zeuzem, Frankfurt
• Hans-Jürgen Stellbrink, Hamburg
USA
• Daniel Pambianco, Charlottesville
• Edwin DeJesus, Orlando
• Kyle Etzkron, Jacksonville
• Michael Fried, Chapel Hill
• Andrei Gasic, Longview
• Nigel Girgrah, New Orleans
• Ira M. Jacobson, New York
• Donald M. Jensen, Chicago
• Mark E. Jonas, Cincinnati
• Fred Poordad, Los Angeles
• Coleman Smith, Plymouth
• Jawahar Taunk, Palm Harbor
• Lawrence Wruble, Germantown
• Ziad Younes, Germantown
Canada
• Pierre Cote, Montreal
• Gideon Hirschfield, Toronto
• Maged Peter Ghali, Montreal
• Sam Lee, Calgary
• Morris Sherman, Toronto
Australia
• Greg Dore, Darlinghurst
• Paul Desmond, Fitzroy
• Stuart Roberts, Melbourne
• Jacob George, Westmead
• Graeme Macdonald, Woolloongabba
• Alice Lee, Concord
Austria
• Peter Ferenci, Wien
• Hermann Laferl, Wien
Michael Gschwantler, Wien
Belgium
• F. Nevens, Leuven
• Y. Horsmans, Bruxelles
• C. Moreno, Bruxelles
• H. Van Vlierberghe, Ghent
• P. Michielsen, Edegem
• H. Orlent, Brugge
• H. Reynaert, Bruxelles
• J. Decaestecker, Roeselare
Denmark
• Jan Gerstoft, Copenhagen
• Alex Lund Laursen, Aarhus
• Lars Mathiesen, Hvidovre
• Axel Møller, Kolding
• Peer Brehm Christensen, Odense
France
• Yves Benhamou, Paris
• Christian Trepo, Lyon
• Jean Pierre Bronowicki, Vandoeuvre Les Nancy
• Christophe Hezode, Creteil
• Patrick Marcellin , Clichy
• Jean-Didier Grange, Paris
• Jean Pierre Zarski, Grenoble
• Albert Tran, Nice
• Editorial support was provided by Dr. Bethan Lowder at Complete Medical Communications, funded by Tibotec.
• Maria Beumont-Mauviel, Joan Cannon, Ronald Kalmeijer, Eric Lefebvre, Karen Lindsay, Karen Manson, Gaston Picchio and Vanitha Sekar contributed to development of the presentation.