Embed Size (px)
Citation preview

EARLY STROKE DIAGNOSIS
Dr. Peter M. Mativo KAP – March 2012
Aga Khan University Hospital Nairobi

Stroke
• Classification
• Risk Factors
• Signs and Symptoms
• Management
– Prehospital
– In-hospital

Definitions
• Stroke – WHO – “rapidly developing clinical signs of focal (at times
global) disturbance of cerebral function, lasting more than 24 hours or leading to death with no apparent cause other than that of vascular origin”.
• TIA – Neuro deficits that resolve within 24 hours with no
Neuroimaging abnormality
• Reversible ischemic Neurological Deficit – Neuro deficits that last more than 24 hours and less than 3
weeks

Classification of Stroke
• Ischemic Stroke (75% “Brain Infarct”)
– Occlusive:
• Thrombosis
• Embolism
– Anterior Circulation
• Occlusion of carotid artery involve cerebral hemispheres
– Posterior Circulation
• Vertebro-basilar artery distribution involve brainstem, Thalamus or cerebellum

Classification of Stroke
• Hemorrhagic Stroke
– Subarachnoid
• Aneurysm (most common)
• Arteriovenous malformation
– Intracerebral
• Hypertension (most common)
• Amyloid angiopathy in elderly

Stroke – Risk Factors • Modifiable
– Hypertension
– Tobacco use
– Hx of TIA’s
– Heart Disease
– Diabetes Mellitus
– Hypercoagulopathy • Pregnancy, cancer, etc.
– Sickle Cell and increased RBC
– Hx of carotid Bruit
• Unmodifiable
– Age
– Gender
– Race
– Previous CVA
– Heredity

Warning Signs of a Stroke1
• SUDDEN numbness or weakness of face, arm or leg – especially on one side of the body.
• SUDDEN confusion, trouble speaking or understanding.
• SUDDEN trouble seeing in one or both eyes.
• SUDDEN trouble walking, dizziness, loss of balance or coordination.
• SUDDEN severe headache with no known cause.

Stroke – Signs and Symptoms
• Ischemic – Carotid Circulation
• Unilateral paralysis (opposite side)
• Numbness (opposite side)
• Language disturbance – Aphasia – difficult comprehension, nonsense, difficult
reading/writing
– Dysarthria – slurred speech, abnormal pronunciation.
• Visual disturbance (opposite side)
• Monocular blindness (same side)

Stroke – Signs and Symptoms • Ischemic
– Vertebrobasilar Circulation • Vertigo
• Visual disturbance – Both eyes simultaneously
• Diplopia – Ocular palsy – inability to move to one side
– Dysconjugate gaze – asynchronous movement
• Paralysis
• Numbness
• Dysarthria
• Ataxia


Netter; Atlas of Human Anatomy

Stroke – Signs and Symptoms • Hemorrhagic
– Subarachnoid hemorrhage
• Sudden severe HA
• Transient LOC
• Nausea/Vomiting
• Neck pain
• Intolerance of noise/light
• AMS
– Intracerebral hemorrhage
• Focal sx w/ LOC, N/V
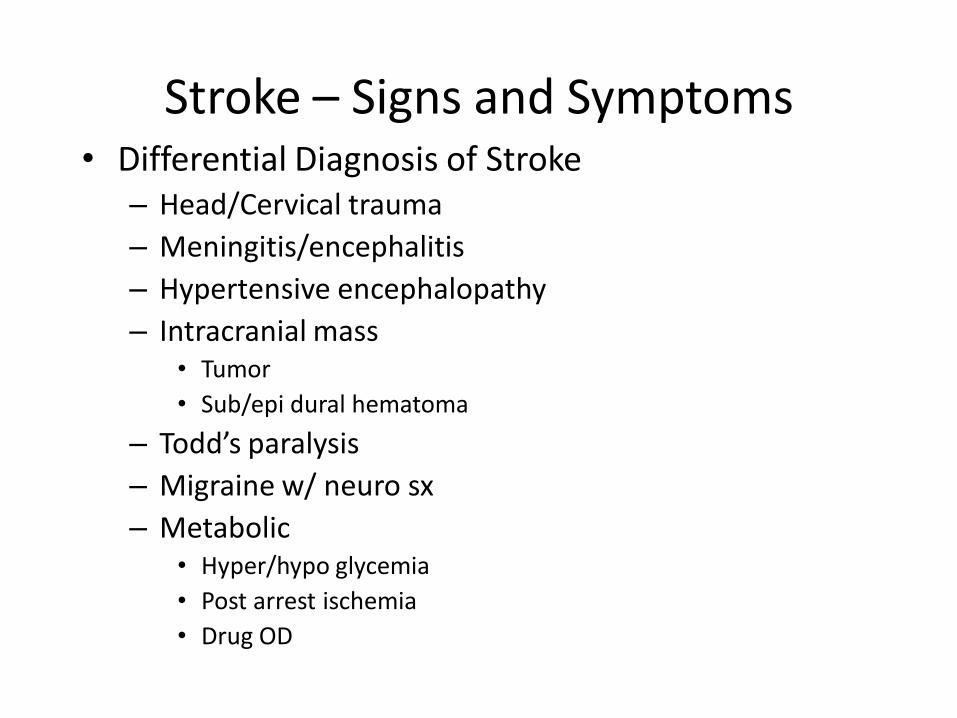
Stroke – Signs and Symptoms • Differential Diagnosis of Stroke
– Head/Cervical trauma
– Meningitis/encephalitis
– Hypertensive encephalopathy
– Intracranial mass • Tumor
• Sub/epi dural hematoma
– Todd’s paralysis
– Migraine w/ neuro sx
– Metabolic • Hyper/hypo glycemia
• Post arrest ischemia
• Drug OD

Stroke - Management • Stroke Chain of Survival
– Detection • Early sx recognition
– Dispatch • Prompt EMS response
– Delivery • Transport, approp, prehospital care, prearrival notification
– Door • ER Triage
– Data • ER evaluation incl, CT, etc.
– Decision • Appropriate therapies
– Drug/Therapy

Stroke - Management
• Detection: Early Recognition
– Public education of Stroke sx
– Early access to medical care
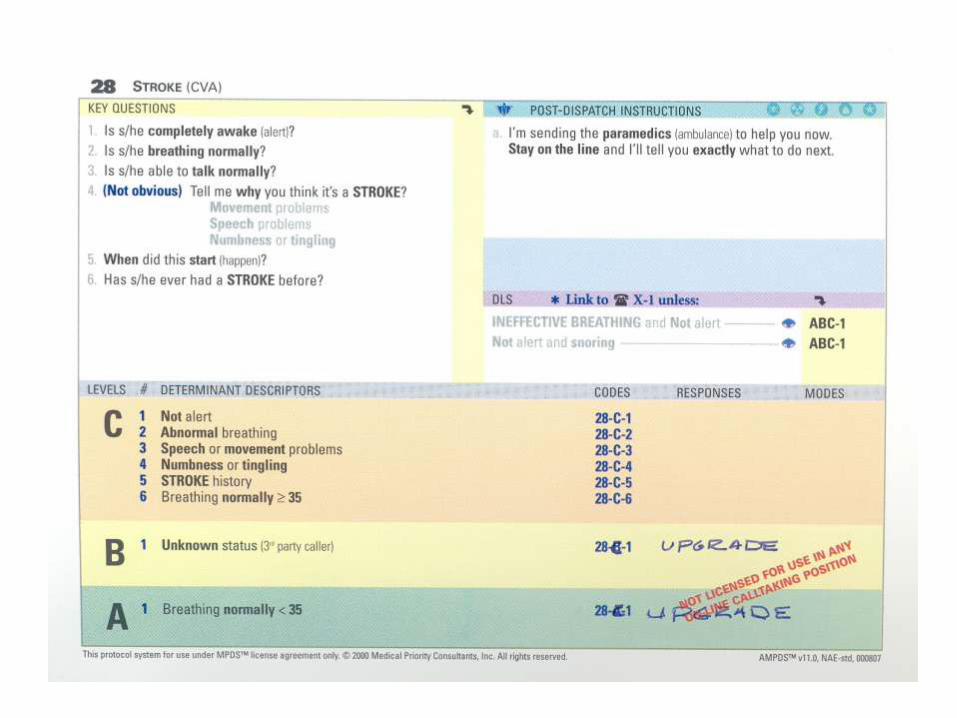
• Dispatch: Early EMS and PDI’s
– Caller triage
• EMD recognition of Stroke sx

Stroke - Management
• Delivery: Prehospital Transport and Management
– Prehospital stroke scale
• Facial Droop
• Arm Drift
• Speech

Cincinnati Prehospital Stroke Scale
• National Stroke Association – Act FAST
– F – Face
– A – Arms
– S – Speech
– T – Time
• Cincinnati Prehospital Stroke Scale

CINCINNATI STROKE SCALE
• Identifies patients with strokes.
• It evaluates three major physical findings.
– Facial droop
– Motor arm weakness
– Speech abnormalities

Facial Droop
• Have the patient show their teeth or smile.
• Normal – both sides of the face move equally well
• Abnormal – one side of the face does not move as well as the other side

Arm Drift
• Have the patient close his/her eyes and hold both arms out.
• Normal – both arms move the same way, or both arms do not move at all.
• Abnormal – one arm does not move or one arm drifts down compared to the other arm.
Other findings such as pronater grip, may be helpful

Speech
• Have the patient say “You can’t teach an old dog new tricks.”
• Normal – patient uses correct words with no slurring.
• Abnormal – patient slurs words, uses inappropriate words, or is unable to speak

Cincinnati Prehospital Stroke Scale
• Patients with 1 of these 3 findings -as a new event - have a 72% probability of an ischemic stroke.
• If all 3 findings are present the probability of an acute stroke is more than 85%
• Immediately contact medical control and the destination ED and provide prearrival notification.

Los Angeles Prehospital Stroke Screen
• LOS ANGELES Patient Name: ____________________________ • PREHOSPITAL Rater Name: ____________________________ • STROKE SCREEN (LAPSS) Date: ____________________________ • Screening Criteria Yes No
– 4. Age over 45 years ____ ____ – 5. No prior history of seizure disorder ____ ____ – 6. New onset of neurologic symptoms in last 24 hours ____ ____ – 7. Patient was ambulatory at baseline (prior to event) ____ ____ – 8. Blood glucose between 60 and 400 ____ ____
• 9. Exam: look for obvious asymmetry • Normal Right Left • Facial smile / grimace: Droop Droop • Grip: Weak Grip No Grip Weak Grip No Grip • Arm weakness: Drifts Down Falls Rapidly Drifts Down Falls Rapidly
• Based on exam, patient has only unilateral (and not bilateral) weakness: Yes No • 10. If Yes (or unknown) to all items above LAPSS screening criteria met: Yes No
– 11. If LAPSS criteria for stroke met, call receiving hospital with “CODE STROKE”, if not then return to the appropriate treatment protocol. (Note: the patient may still be experiencing a stroke if even if LAPSS criteria are not met.)

ABCD Score
• ABCD Score • Used to predict the risk of stroke during the first seven days after a TIA. Researchers
found there to be over 30% risk of stroke in TIA patients with an 'ABCD score' of six, as compared to no strokes in those with a low ABCD score. Can be used in routine clinical practice to identify high-risk individuals who require emergency investigation and treatment.
• ABCD Score – Risk factor Category Score
• A Age of patient Age >/= 60 1 • Age < 60 0 • B Blood pressure at SBP > 140 or DBP >/= 90 1 • Assessment Other 0 • C Clinical Features Unilateral weakness 2 • presented with Speech disturbance (no weakness) 1 • Other 0 • D Duration of TIA >/= 60 minutes 2 • symptoms 10-59 minutes 1 • <10 minutes 0 • ________ • TOTAL 6

Stroke - Management
• Airway – Potential problems
• Paralysis of airway structures
• Vomiting esp. w/ hemorrhagic stroke
• Coma
• Seizures
• Cervical trauma due to pt. collapse
– Manage Aggressively • RSI/ETT prn /High flow O2

Stroke - Management
• Breathing
– Potential Problems
• Irregular respiratory pattern – Cheyne-Stokes
– Central Neurogenic hyperventilation
• Paralysis of muscles of respiration
– Manage Aggressively
• RSI/ETT/High flow O2

Stroke - Management • Circulation
– Management is supportive
• Other Treatment
– EKG • Treat dysrhythmias
– IV access • Balanced salt solution
– Glucometer • Correct hypoglycemia
– Prompt Transport • Alert receiving facility of potential Stroke patient

Stroke – Management In Review:
Prehospital Critical Actions
• Assess and support cardiorespiratory function
• Assess and support blood glucose
• Assess and support oxygenation and ventilation
• Assess neurologic function
• Determine precise time of symptom onset
• Determine essential medical information
• Provide rapid emergent transport to ED
• Notify ED that a possible stroke patient is en route

Stroke - Management • Door: ER Triage
– Stroke evaluation targets for stroke patients who are thrombolytic candidates
Door-to–doctor first sees patient…….………… 10 min
Door-to–CT completed …….………………….. 25 min
Door-to–CT read ...…………..………………… 45 min
Door-to–fibrinolytic therapy starts…………….. 60 min
Neurologic expertise available* …..…………… 15 min
Neurosurgical expertise available* …………… 2 hours
Admitted to monitored bed ..……...…………… 3 hours *By phone or in person

Stroke - Management • Data: ER Evaluation and Management
– Assessment Goal: in first 10 minutes
• Assess ABCs, vital signs
• Provide oxygen by nasal cannula
• Obtain IV access; obtain blood samples (CBC, ’lytes, coagulation studies)
• Obtain 12-lead ECG, check rhythm, place on monitor
• Check blood sugar; treat if indicated
• Alert Stroke Team: neurologist, radiologist, CT technician
• Perform general neurologic screening assessment

Stroke - Management Assessment Goal: in first 25 minutes
• Review patient history
• Establish symptom onset (<6 hours required for fibrinolytics)
• Perform physical examination
– Perform neurologic exam
– Determine level of consciousness (Glasgow Coma Scale)
– Determine level of stroke severity (NIHSS or Hunt and Hess Scale)
• Order urgent non-contrast CT scan/angiogram if non-hemorrhage (door-to–CT scan performed: goal <25 min from arrival)
• Read CT scan (door-to–CT read: goal <45 min from arrival)
• Perform lateral cervical spine x-ray (if patient comatose/trauma history)

Stroke - Management
• ER Diagnostic Studies
– CT scan – done w/in 25 mins, read w/in 45 mins • r/o hemorrhage
• Often normal early in ischemic stroke
– Lumbar puncture
– EKG • Changes may be caused by or cause of stroke
– MRA (Magnetic Resonance Angiography)
– Cerebral Angiography

Hypodense area:
• Ischemic area with edema,
swelling
• Indicates >3 hours old
• No fibrinolytics!

(White areas indicate hyperdensity = blood)
Large left frontal intracerebral hemorrhage.
Intraventricular bleeding is also present
No fibrinolytics!

Acute subarachnoid
hemorrhage
Diffuse areas of white
(hyperdense) images
Blood visible in ventricles
and multiple areas on
surface of brain

Stroke - Management
• Decision: Specific Therapies
– General Care
• ABC’s, O2
• IV w/ BSS – Treat hypotension
– Avoid over-hydration
– Monitor input/output
• Normalize BGL
– Manage Elevated BP?

Stroke - Management
• Indications for Antihypertensive therapy In general:
• Consider: absolute level of BP? – If BP: >185/>110 mm Hg = fibrinolytic therapy contraindicated
• Consider: other than BP, is patient candidate for fibrinolytics? – If patient is candidate for fibrinolytics: treat initial
BP >185/>110 mm Hg
• Consider: response to initial efforts to lower BP in ED? – If treatment brings BP down to <185/110 mm Hg: give fibrinolytics
• Consider: ischemic vs hemorrhagic stroke? – Treat BP in the 180-230/110-140 mm Hg range the same
– The obvious: no fibrinolytics for hemorrhagic stroke

Stroke - Management
• Decision: Specific Therapies (cont.) – Management of Seizures
• Benzodiazepines
• Long-acting anticonvulsants
– Management of Increased ICP • Maintain PaCO2 30mm Hg
• Mannitol/Diuretics
• Barbiturates
• Neurosurgical decompression

Stroke - Management • Drugs: Thrombolytic Therapy
– Fibrinolytic Therapy Checklist Ischemic Stroke
Candidates for Neurointerventional Therapy
Age 18 years or older
Acute signs and symptoms of CVA <6 hours onset.
No contraindications.

Stroke - Management
Contraindications for Interventional Therapy
Absolute
Evidence of intracranial hemorrhage on non-contrast head CT
Patient with early infarct signs on CT scan.
Relative
Recent (w/in 2 mo’s) cranial or spinal surgery, trauma, or injury
Known bleeding disorder and/or risk of bleeding including:
- Current anticoagulant therapy, prothrombin time >15 sec.
- Heparin within 48 hrs of admission, PTT elevated
- Platelet count <100,000/mm
Active internal bleeding w/in the previous 10 days
Known or suspected pregnancy
History of stroke w/in past 6 weeks

Stroke - Management Contraindications for Interventional Therapy (cont.)
Relative
Patient comatose
>85 years old
Diabetic hemorrhagic retinopathy or other opthalmic hemorrhagic disorder
Advanced liver or kidney disease
Other pathology with a propensity for bleeding
Infectiouse endocarditis
Severe EKG disturbance, uncontrolled angina or acute MI

Stroke - Management
• Thrombolytic Agents
– TPA
• NINDS trial
– Streptokinase
• VEGGIE trial
• Anticoagulant Therapy
– Heparin
– ASA/Warfarin/Ticlodipine


Stroke - Management • Management of Hemorrhagic Stroke
– Subarachnoid • Neurosurgical intervention
• Nimodipine
– Intracerebral • Management of ICP
• Neurosurgical decompression
– Cerebellar • Surgical evacuation
– Often associated with good outcome
– Lobar • Surgical evacuation

ASANTE SANA