Embed Size (px)
Citation preview
Early Mandibular Distraction Osteogenesisin Pierre Robin Sequence
Pierre Robin Sequence• Pierre Robin case report 1926• one in 9000 births• micrognathi, glossoptosis, cleft palate. • Theories:
– fetal head positioning, frequently associated with oligohydramnios.
– a delay in neurological maturation – rhombencephalic dysneurulation
• rare familial cases reported - localized intrinsic failure of mandibular growth may be a factor in some cases.
• Catchup mandibular growth in most, but mandibular dimensions will remain below age-matched norms.
Early Considerations• varying degrees of airway obstruction and
feeding difficulties.• mechanism - falling back of the tongue into the
oral pharynx. • Immediate supportive measures required in over
70 percent of affected infants. • Caouette-Laberge ( 1994) clinical classification of
respiratory symptoms:– group I, adequate respiration in prone position and
bottle feeding;– group II, adequate respiration in prone position but
feeding difficulties requiring NGT;– group III, children with respiratory distress requiring
respiratory support and NGT.

Early Management
• Supportive measures • Lying prone• Tongue-lip adhesion
– Kirschner (2003) - >40% Group III infants required tracheostomy after tongue-lip adhesion
– Denny (2004) - additional 1.9 secondary procedures
• Nasopharyngeal airway• Tracheostomy (12-42%)• K wire fixation, genioglossus stripping
Problems with tracheostomy
• Increased morbidity– Donnelly, Int J Pediatr Otorhinolaryngol. 1996
• n=29; 41% complication rate (<1yo- 64%)• 25 months average decannulation
– Midwinter, J Laryngol Otol. 2002 • n-=143; 46% complication rate• 25 months mean decannulation• Mortality 2.7%
– Carr, Laryngoscope. 2001• N=142; 43% serious complications• Mortality 0.7%
Problems with tracheostomy
• Poorer Speech Outcomes– Jiang, Int J Pediatr Otorhinolaryngol. 2003
• Affects speech and language development in those with and without neurological disorders.
• Risk factors: age at tracheostomy, and duration.• Better outcome with early decannulation
– Simon, Int J Pediatr Otorhinolaryngol. 1983• All children decannulated during the linguistic stage
exhibited specific spoken language delays • phonological impairment proportional to duration
Problems with tracheostomy• Prolonged
– Tomaski, Laryngoscope 1995• Average 3 years decannulation in PRS
• Carer Impact
• Financial Burden
• Developmental Problems– Singer, Dev Med Child Neurol. 1989
• n=130• Slower growth rate• Higher risk of behavioural problems• Most will require special educational intervention
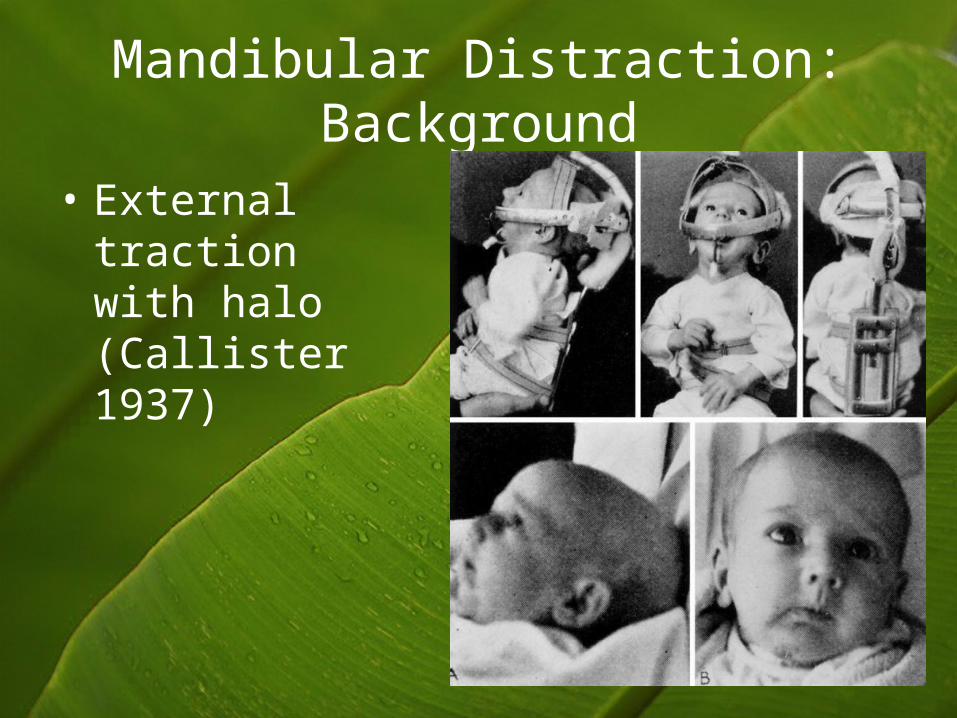
Mandibular Distraction: Background
• External traction with halo (Callister 1937)
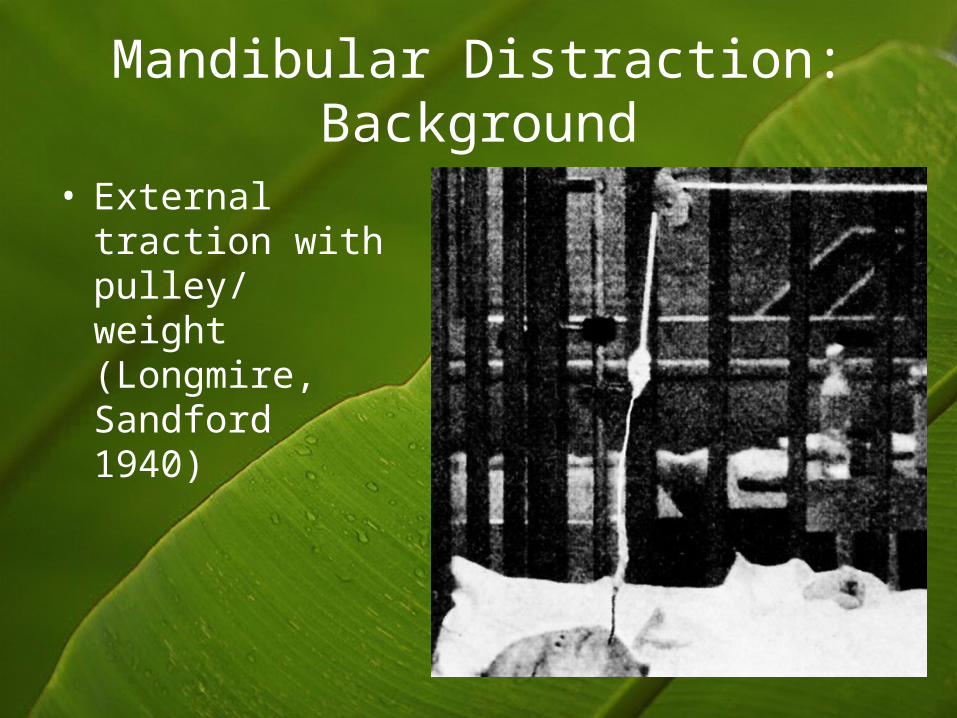
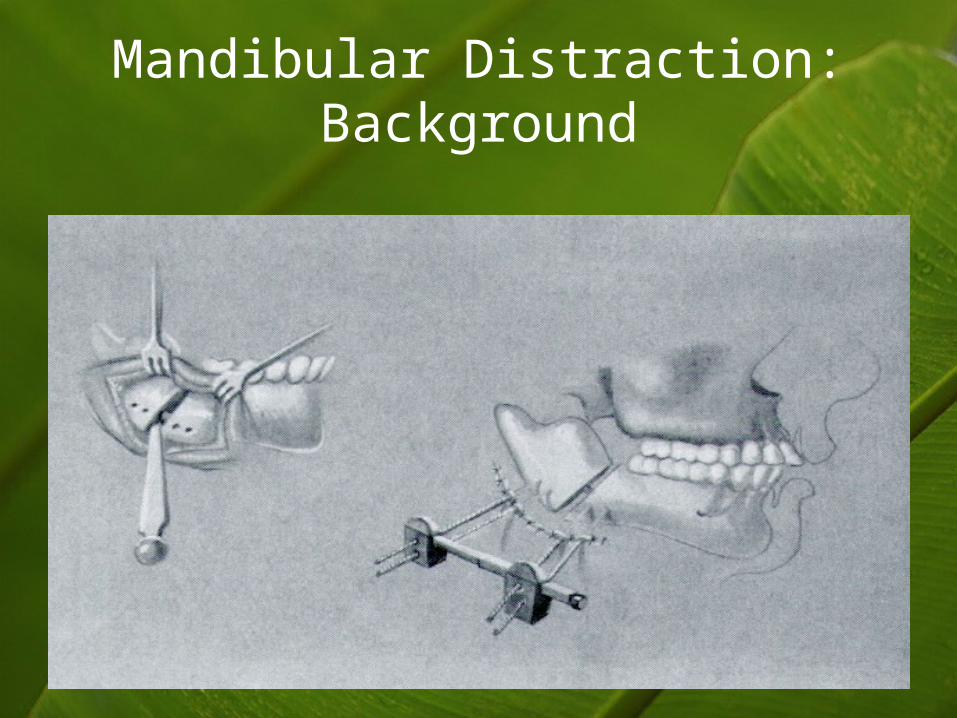
Mandibular Distraction: Background
• External traction with pulley/ weight (Longmire, Sandford 1940)
Mandibular Distraction: Background
• Mandibular DOG– McCarthy 1992, Molina/Ortiz-Monasterio 1995
• Use in children with airways obstruction– Moore, David 1994– Cohen 1999
• Use in Pierre Robin– Denny 2001,2002– Monasterio 2002– Burstein 2005 (internal resorbable device)
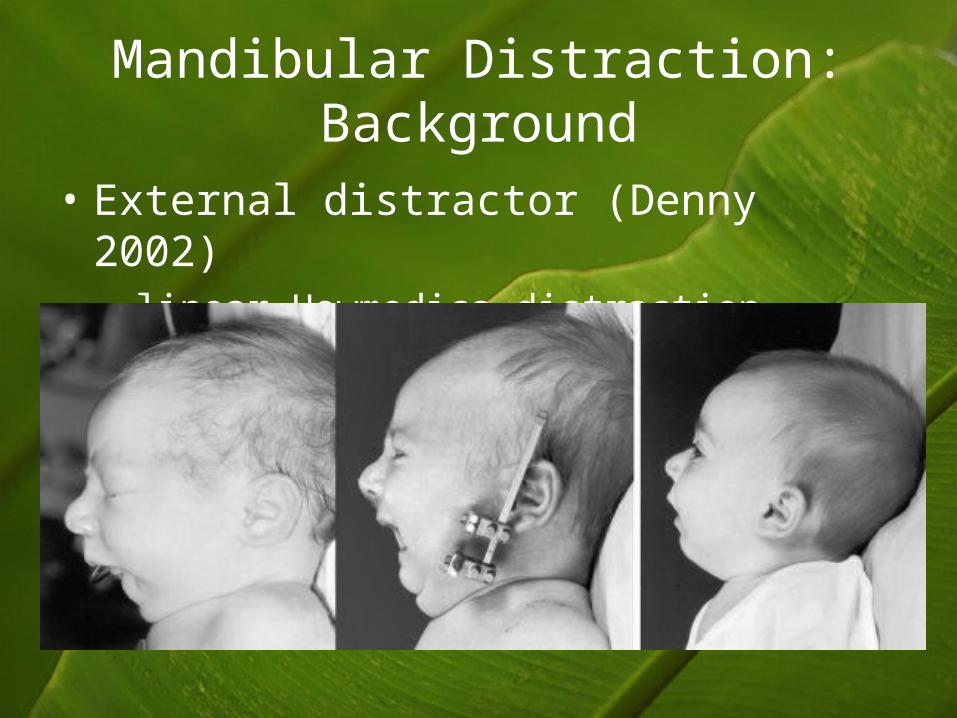
Mandibular Distraction: Background
• External distractor (Denny 2002)– linear Howmedica distraction device
Mandibular Distraction: Background
Mandibular Distraction: Background

Mandibular Distraction: Background
• Internal resorbable device
Early Distraction: Controversies
• Conservative management alone– 20-40% will not respond to positioning or glossopexy
• Rapid distraction– 2mm/day vs 1mm/day– In goats – demyelination noted at 2mm/day (Hu, J Oral
Maxillo Surg 2001)
• Effect on dentition– Screw holes– Infraalveolar nerve
• Effect on subsequent mandibular growth• Facial scarring
Indications for early distraction in Pierre Robin
• Failure of conservative measures to improve respiration and feeding
• Documented tongue base obstruction
• Center with expertise In distraction