-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
1/13
712 MINERVA ANESTESIOLOGICA June 2012
E X P E R T O P I N I O N
S
epsis represents a continuum beginning witha host-pathogen
interaction that triggers a
complex interplay between pro-inflammatory,anti-inflammatory and
apoptotic mediators.1As the disease progresses, organ dysfunction
canresult from circulatory insufficiency from hypo-volemia,
myocardial depression, increased meta-bolic demands and
vasoregulatory perfusion ab-normalities. ese hemodynamic
perturbationslead to an imbalance between systemic oxygensupply and
demand, leading to global tissue hy-poxia and shock. ese pathogenic
events signif-icantly contribute to the morbidity and mortal-
ity in early sepsis.2, 3
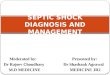
A critical decrease in systemic oxygen delivery(DO2) is followed
by an increase in the systemicoxygen extraction ratio (O2ER) and a
decreasein central venous oxygen saturation (ScvO2) ormixed venous
oxygen saturation (SvO2). is in-crease in OER is a compensatory
mechanism tomatch systemic oxygen demands. When the lim-it of this
compensatory mechanism (OER>50 to60%) is reached, anaerobic
metabolism ensuresleading to lactate production.4In this critical
de-livery dependent or hypodynamic phase, lactateconcentrations are
inversely related to DO2andScvO2/SvO2 (Figure 1).5 is phase can
occur
with normal vital signs and is commonly referred
Early interventions in severe sepsis and septic shock:a review
of the evidence one decade later
E. P. RIVERS 1, M. KATRANJI 2, K. A. JAEHNE 1, S. BROWN 1G. ABOU
DAGHER 1, C. CANNON 3, V. COBA 1
1Department of Emergency Medicine and Surgery, Henry Ford
Hospital, Wayne State University, Detroit, MI, USA;2Department of
Medicine, Pulmonary and Critical Care Medicine, Pontiac Osteopathic
Hospital, Pontiac, MI, USA;3
Department of Emergency Medicine, University of Kansas, Medical
Center, Kansas City, KS, USA
A B S T R A C Te outcomes of acute myocardial infarction,
trauma, and stroke have improved by implementing processes
thatprovide early diagnosis and aggressive interventions at the
most proximal point of disease presentation. A commonfeature in
these conditions is the implementation of early intervention
strategies. One decade ago, a similar approachto sepsis began when
a prospective randomized trial compared early goal-directed therapy
(EGDT) to standard careusing specific criteria for the early
identification of high risk patients with infection. e components
of EGDT werederived from expert consensus opinion to produce a
protocol to reverse the hemodynamic perturbations of hypovo-lemia,
vasodysregulation, myocardial suppression and increased metabolic
demands for patients with severe sepsis inthe intensive care unit
(ICU). However, EGDT was provided at the most proximal phase of
disease presentation in the
Emergency Department (ED). With EGDT, a reduction in mortality
of over 16% was shown over standard care. Sincethe EGDT study was
published a decade ago, significant emphasis worldwide has been
placed on a comprehensiveapproach to the first 6 hours of sepsis
management which is commonly referred to as the resuscitation
bundle (RB).e RB consists of early diagnosis, risk stratification
using lactate levels, hemodynamic response after a fluid
challenge,antibiotics, source control and hemodynamic optimization
or EGDT. is review will examine one decade of evidencefor the
components of the RB examining its impact on systemic inflammation,
the progression of organ failure, healthcare resource consumption
and mortality in severe sepsis and septic shock. (Minerva
Anestesiol 2012;78:712-24)
Key words: Sepsis - Shock, septic - Lactatic acid -
Resuscitation.
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
2/13
EARLY INTERVENTIONS IN SEVERE SEPSIS AND SEPTIC SHOCK RIVERS
Vol. 78 - No. 6 MINERVA ANESTESIOLOGICA 713
to as occult shock, where the patient outwardlyappears less ill.
As a result organ dysfunction andsudden cardiopulmonary collapse
are complica-tions associated with this phase if unrecognizedor
left untreated.2, 6, 7is state predominantlycharacterizes the early
sepsis presentation (Figure2) and is an important distinction from
previousunsuccessful sepsis resuscitation trials performedin the
ICU setting.8-11
After adequate resuscitation, a hyperdynamicphase follows the
hypodynamic phase. Com-pensated sepsis is characterized by an
elevatedScvO2/SvO2 and normal lactate. Later an el-evated lactate
and elevated ScvO2/SvO2denotepathologic delivery dependence or
delivery inde-pendence and is associated with increased
mor-tality.12e failure to increase OER and thus in-crease systemic
oxygen consymption (VO2) maybe secondary to impairment of
microvascularoxygen perfusion or mitochondrial dysfunction.
Origin of the resuscitationbundle (RB) components
e RB and its components are not novelstrategies. Wilson et al.
wrote a series of expertopinions beginning in 1976 that comprised
thetenets of early sepsis management (Figure 2).13ese
recommendations included the following:early identification of high
risk patients, appro-priate cultures, source control, and
appropriateantibiotic administration. is was followed bystrategies
aimed at early hemodynamic opti-mization of oxygen delivery guided
by preload(central venous pressure or surrogate, fluids),
afterload (mean arterial pressure, vasopressors),
arterial oxygen content (packed red blood cells,oxygen), and
contractility (inotropes) if ScvO2remained low (Figure 2).
In the 2001 publication, these componentswhich were also
recommended by a consensus ofexpert opinion 14were applied at the
most proximalsite of hospital presentation mirroring the approachto
trauma, stroke and acute myocardial infarction.14is approach called
early good-directed therapy(EGDT) was tested against standard care
in a ran-domized control trial resulting in a mortality ben-efit of
over 16%. In order to avoid the ethical issues(withholding life
saving therapy), the control orstandard care arm also received
continuous centralvenous pressure (CVP), arterial blood pressure
andurine output monitoring. is was not a standardof care in
emergency department (ED) throughoutthe United States at the time
where baseline mortal-ity was estimated to be over 50%. In regards
to thesuccess of the EGDT group, it must be emphasizedthat control
group therapy also reduced mortality(46.5%) compared to the
historical care mortalitywhich was over 50%.15Over the last decade
thevarious components of EGDT or the resuscitationbundle have been
examined, validated and incorpo-rated into evidence based
guidelines.16, 17
Early risk stratification using bloodpressure and lactate
levels
EGDT begins with early identification of highrisk patients based
on hypotension (systolic bloodpressure 4 mmol/L(Figure 2). Although
it is intuitive, a hypotensiveepisode is associated with an
increase risk for sud-den and unexpected death.18After Aduen et al.
es-tablished the general prognostic value of a lactateof 4 mM/L on
hospital admission; multiple studieshave confirmed the risk
stratification of this levelfor illness severity and mortality in
both the pre-hospital and in-hospital setting.19-23
Antibiotic therapy
Once patients are identified, source controland appropriate
cultures should be obtained.24While there are no prospective
outcome trialsto support early administration of antibiotics,
the animal and retrospective human literature
Figure 1.Oxygen delivery and consumption.
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
3/13
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
4/13
EARLY INTERVENTIONS IN SEVERE SEPSIS AND SEPTIC SHOCK RIVERS
Vol. 78 - No. 6 MINERVA ANESTESIOLOGICA 715
later stage of disease presentation. It may be be-cause of this
that administration and duration ofvasopressors also correlates
with worse outcome.
Levy et al. has shown that the delayed use of va-sopressor
therapy for cardiovascular support isincrementally associated with
a significantlyhigher mortality than any other organ failurebeyond
the first 24 hours of sepsis.3One of theattributes of early volume
therapy is a significantreduction in vasopressor therapy which
furtherreduced need for vasopressin and corticosteroidtherapy.3,14,
39-41 De Backer et al. showed thatthere was no significant
difference in the rate ofdeath between patients treated with
dopamineas the first-line vasopressor agent and those whowere
treated with norepinephrine, however, theuse of dopamine was
associated with a greaternumber of adverse events.42
Central venous and tissue oxygen saturation
Many of the salutary effects of ScvO2moni-toring are based on
its ability to detect imbal-ances of DO2 to VO2 in the delivery
depend-ent phase even with normal vitals signs.6In thepresence of a
low value, therapeutic maneuversto increase DO2or decrease VO2are
required tonormalize this number. us, ScvO2becomes atrigger for
increasing inspired oxygen concentra-tion (arterial hypoxia), red
blood cell transfusion(decreased arterial oxygen content),
inotropetherapy (myocardial suppression), and mechani-cal
ventilation (increased oxygen demands).43-46Multiple studies have
compared ScvO2 withSvO2showing that there is an absolute
difference(5%) between the two sites.47, 48While there isa
difference, the clinical utility of both sites iscomparable and
validated by outcome studies.48In a multicenter study, Pope et al.
found that thefailure to reach a ScvO2greater than 70% withinthe
first six hours is associated with significantlyincreased (14%)
mortality.12Castellanos-Ortegaet al. examined all of the sepsis
bundle elementsat 6 and 24 hours of sepsis and found that
theattainment of an ScvO2 >70% had the statisti-cally most
significant impact on survival thanall other bundle elements.49 In
a meta-analysisexamining five studies comprising over 11000
patients, it was shown that patients reaching this
administration was associated with a significant-ly reduced
hospital length of stay and hospitalcosts.30
Central venous pressure and fluid therapy
While some question the accuracy of CVPin assessing volume
status; equivalent outcomeshave been shown when compared to the
pul-monary artery catheter for assessment of fluidstatus in acute
lung injury.31CVP measurementis indicative of fluid responsiveness
in the low-er ranges and a CVP >10 is the upper limit
foralgorithms of fluid challenges.32 CVP has beenshown to have a
significant association with 30-day mortality.33 Ferrer et al.34
and Boyd et al.concluded a negative impact on survival whenCVP was
used as a guide to fluid management.35e use of CVP appears to be
time sensitive.Early, aggressive fluid therapy which is
associatedwith improved outcomes must be distinguishedfrom late
aggressive fluid therapy.36e adminis-tered volume in the EGDT group
within the first6 hours was significantly greater compared
tostandard therapy group, but over 72 hours therewere no
differences in the amount of fluid be-tween the two groups. In a
meta-analysis, the useof albumin is associated with lower
mortality.37
Mean arterial pressure and vasopressor use
e mean arterial blood pressure target inEGDT is supported by
Varpula and Dunser etal.33, 38ey examined hemodynamic variablesin
septic shock patients during the first 24-48h of treatment and
found a MAP below 60-65mmHg to be most predictive of 28-30-day
mor-tality and organ function. It is preferable thatthis endpoint
be met with fluid versus vasopres-sor therapy. EGDT is associated
with greater vol-ume administration and diminished vasopressoruse
over first 6 hours of resuscitation. However,an equal amount of
fluid is used over the first72 hours of hospitalization. In the
absence of di-minished early volume therapy, there was an in-crease
in the incidence of sudden hemodynamicdeterioration and vasopressor
use.
ese observations reveal that hypotension
is more refractory to fluid administration at the
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
5/13
RIVERS EARLY INTERVENTIONS IN SEVERE SEPSIS AND SEPTIC SHOCK
716 MINERVA ANESTESIOLOGICA June 2012
with altered capillary perfusion at baseline.57While there are
many publications that incrimi-nate RBC transfusions with worse
outcome, a
recent large observational study found that RBCtransfusion was
associated with decreased mor-tality rates.58Further studies are
needed to sup-port the current recommendation for a hemo-globin of
10 mg/dL during septic shock.59
Myocardial dysfunction and inotrope therapy
e early recognition of myocardial dysfunc-tion requiring
inotropic use was found to be at a12.9% greater frequency in the
EGDT versusthecontrol group in the original EGDT study andthis
incidence is consistent with previous find-ings by Parrillo et
al.60Grissom et al. establishedthat physical examination findings
of inadequatecirculation are not useful for predicting low car-diac
index or ScvO2.51Afessa et al. examined 962patients using a
propensity score for each bundleelement and found that compliance
with lactatemeasurement and inotrope administration
wasindependently associated with decreased risk ofmortality.61 Shah
et al. performed a retrospec-tive review of 183 sepsis episodes in
patientswith pre-existing echocardiograms (prior to thesepsis
event) documenting systolic dysfunction.In the 135 patients who did
not meet EGDTadherence requirements, the mortality rate was36.3%
and in the 48 patients who met EGDTadherence requirements, the
mortality rate was16.67%, P
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
6/13
EARLY INTERVENTIONS IN SEVERE SEPSIS AND SEPTIC SHOCK RIVERS
Vol. 78 - No. 6 MINERVA ANESTESIOLOGICA 717
ScvO2) where the production of lactate exceedsits clearance and
the serum lactate levels beginto rise.4erefore, SvO2is more
sensitive at de-
tecting impending tissue hypoxia than lactate.Continuous ScvO2
monitoring provides a realtime assessment, more efficient
attainment of re-suscitation endpoints and greater mortality
ben-efit than intermittent sampling.47, 52In an ICUbased study,
Jansen et al. randomly allocatedpatients with an elevated lactate
(>3 mm/L) todecrease lactate by 20% or more per two hoursfor the
initial eight hours in the lactate group.In the control group, the
treatment team had noknowledge of lactate levels (except for the
ad-mission value). e lactate group received morefluids and
vasodilators. However, there were nosignificant differences in
lactate clearance be-tween treatment groups. Hospital mortality
wassignificantly reduced from 43.5% in the controlgroup versus
33.9% in the lactate group. In thelactate group, there was a
decrease in organ fail-ure, duration of inotrope therapy,
mechanicalventilation from 7-72 hours and ICU length ofstay.70e
lactate group treatment did not re-sult in faster reduction of
lactate when comparedwith control group therapy. is might
actuallyargue against lactate as a target of hemodynamictherapy.
However, given that ScvO2monitoringwas mandatory in the lactate
group and faculta-tive in the control group, this study could
notexclude the possibility that this had an impacton the observed
outcome difference. e distur-bances of lactate metabolism that
occur duringsepsis are probably more complex than an iso-lated
defect of cellular oxygenation.71 Furthera normal lactate in
isolation does not excludethe presence of tissue hypoperfusion.
Twenty to50% of septic shock patients will never elevatelactate
levels at presentation or during the clini-cal course and
frequently develop multi-systemorgan failure.72-74 ese observations
indicatethat using lactate and ScvO2are complimentaryendpoints and
not mutually exclusive.
Modified versions of the resuscitation bundle
Lin et al. employed a modified EGDT proto-col in a medical ICU
without the use of ScvO2
compared to a control group. Targeting CVP,
to early restoration of the balance between DO2and VO2.
Lactate clearance
Nguyen et al. found that the clearance of lac-tate over the
first six hours after presentation wasassociated with a significant
decrease in pro- andanti-inflammatory biomarkers, improved or-gan
function and reduced mortality.42, 43 iswas based on previous
investigations using lac-tate clearance over 24 and 72 hours in the
ICUsetting.67 In a recent prospective multicentertrial of EGDT
implementation, Nguyen et al.showed that when patients received
EGDT, themortality reduction was further enhanced
whenretrospectively grouped by improving levels oflactate
clearance.68Jones et al. declared that lac-tate clearance is
equivalent to ScvO2using theEGDT algorithm in a noninferiority
study.69Inthis study, patients assigned to the ScvO2groupwere
resuscitated to normalize central venouspressure, mean arterial
pressure, and ScvO2of 70% while patients in the lactate
clearancegroup were resuscitated to normalize centralvenous
pressure, mean arterial pressure, andachieve a lactate clearance of
at least 10%. estudy protocol was continued until all goals
wereachieved or for up to six hours. ey concludedthat lactate
clearance guided resuscitation wasnon-inferior or equivalent to a
ScvO2 guidedresuscitation based on no difference in mortal-ity.
Compared to the EGDT study, the patientsenrolled by Jones et al.
were of a lower illnessseverity, in a more supply independent phase
atbaseline (ScvO2and lower lactate levels at studybaseline), more
frequently in vasodilatory shock(vasopressor dependent) and less
mechanicallyventilated, Figure 1. More importantly, only30
interventions were made in only 10% of thepatient population. It is
these patients (deliverydependent or hypodynamic phase) that
requireadditional interventions such as supplementaloxygen, packed
red blood cells, inotropes andmechanical ventilation which are
physiologi-cally triggered by ScvO2. ese interventions re-duce
sudden cardiopulmonary complications by50%; an issue not addressed
by Jones et al. ese
events signal reaching the critical OER (low
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
7/13
RIVERS EARLY INTERVENTIONS IN SEVERE SEPSIS AND SEPTIC SHOCK
718 MINERVA ANESTESIOLOGICA June 2012
inflammation.76e observation of a 15% reduc-tion in mechanical
ventilation over 72 hours is anexample of preventing this second
hit.73Adjunc-tive therapies to further modulate the inflamma-tory
response when used early may enhance thebeneficial effects of
EGDT.77erapeutic effortstargeting the microcirculation are in
progress butto date having not shown outcome benefit.78Ki-ers et
al. found that a delay in achieving hemo-dynamic goals of EGDT was
significantly associ-ated with the development of acute kidney
injury
(P=0.02) and resulted in a 3.4% greater creatininelevel rise per
hour (P=0.03) in patients admittedfrom the hospital ward.79In a
subanalysis of pa-tients enrolled in the Fluid and Catheter
Treat-ment Trial (FACTT) of the National Institutesof Health, Acute
Respiratory Distress SyndromeNetwork, an improved SvO2was
significantly as-sociated with improved mortality and decrease
induration of mechanical ventilation.51ese find-ings support the
observations of a decreased needfor mechanical ventilation over the
first 72 hours
of presentation in the original EGDT trial.
Outcome evidence in adult patients
Over the last decade, the external validityand generalizability
of the RB containing vary-ing versions of EGDT has been established
inmultiple studies. ese studies comprise over 50publications
containing over 18000 adult pa-tients (Table I).8, 41, 49, 68,
80-128e outcome ben-efit of these studies combined equal or
exceed
the reduction in mortality found in the original
MAP, hemoglobin and urine output, not onlyled to a significant
decrease of the mortality rate,but also to shortening the length of
ICU stay,duration of mechanical ventilator support andduration of
antibiotic administration. ere wasmore rapid reversal of shock and
less delayedvasopressor administration. For medical ICUswithout
facility to monitor ScvO2, this modi-fied therapeutic protocol
provides an alterna-tive that reduces mortality, ICU stay,
ventilatorsupport duration, and tissue hypoperfusion as-
sociated major organ dysfunction. e authorsadded that with
ScvO2measurement there wasa chance of improving clinical outcomes
further.
Impact on inflammation, themicrocirculation and organ
failure
e association between global tissue hypoxiaand inflammation has
been well described in vivomodels. Boulos et al. have shown that
SvO2 issignificantly associated with mitochondrial func-
tion and that inflammatory mediators in septicpatients can
significantly alter mitochondrialfunction.75 In a further analysis
of EGDT pa-tients, Rivers also showed that the persistence ofglobal
tissue hypoxia (increased lactate and lowScvO2) correlates
significantly with the activity ofinflammatory mediators. In
patients treated withEGDT, alteration of the inflammatory cascadeis
evidenced by significantly lower IL-8 levels.When untreated, this
pathogenic mechanism ofinflammation can lead to a second hit
phe-
nomenon of multi-organ failure and worsening
T I.Comparison of sepsis intervention studies using the
resuscitation bundle compared to the original EGDTstudy.8, 41, 49,
68, 80-128
Summary of implementation study Rivers et al.
Before or control After Control EGDT
Number of patients 9527 9884 133 130APACHE II score 24.24 24.2
20.4 21.4Sex, % Males 58.15 57.3 50.4 50.8Age (years) 63.84 62.9
64.4 67.1Mortality before (SD)** 46.8 (26)% 29.1 (12)% 46.5%
30.5%Relative risk reduction 0.37 0.34Absolute risk reduction 18.3%
16.0%NNT 5.45 6.25
*Includes before and after and concurrent implementation
studies. **e average mortality of each study. NNT=number needed to
treat.
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
8/13
EARLY INTERVENTIONS IN SEVERE SEPSIS AND SEPTIC SHOCK RIVERS
Vol. 78 - No. 6 MINERVA ANESTESIOLOGICA 719
plying with the goals of EGDT on patient out-comes when
completed beyond the six-hour rec-ommendation period. Compliance
was assessed
at 6, 18 and 24 hours after diagnosis of severesepsis or septic
shock. e compliers at 18 h hadan absolute 10.2% significantly lower
in-hospi-tal mortality compared to the non-compliers at18 h (37.1%
vs. 47.3%). When adjusted for dif-ferences in baseline illness
severity, the compliersat 18 h had a greater reduction in predicted
mor-tality of 26.8% versus9.4% (P 4 mm/L Systolic blood pressure 8
mmHg MAP >65 mmHg Hematocrit >30% ScvO2>70%
reshold for red blood cell transfusion Need for inotropic
therapy Indication for and response to mechanical ventilation
Is not equivalent to lactate clearance
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
9/13
RIVERS EARLY INTERVENTIONS IN SEVERE SEPSIS AND SEPTIC SHOCK
720 MINERVA ANESTESIOLOGICA June 2012
12. Pope JV, Jones AE, Gaieski DF, Arnold RC, Trzeciak S,Shapiro
NI. Multicenter study of central venous oxygensaturation (ScvO2) as
a predictor of mortality in patientswith sepsis. Ann Emerg Med
2010;55:40-6,e41.
13. Wilson RF, Wilson JA, Gibson D, Sibbald WJ. Shock in
the emergency department. JACEP 1976;5:678-90. 14. Task Force of
the American College of Critical Care Medi-cine, Society of
Critical Care Medicine. Practice param-eters for hemodynamic
support of sepsis in adult patientsin sepsis. Crit Care Med
1999;27:639-60.
15. Ander D, Rivers EP, Jaggi M, Massura. A comparison
ofstandard versus goal directed therapy in resuscitation
ofcritically ill emergency department patients. Acad EmergMed
1997;4:402-3.
16. Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM,Jaeschke
R et al. Surviving Sepsis Campaign: Internation-al guidelines for
management of severe sepsis and septicshock: 2008. Crit Care Med
2008;36:296-327.
17. Ferrer R, Artigas A. Effectiveness of treatments for
severesepsis: data from the bundle implementation programs.Minerva
Anestesiol 2011;77:360-5.
18. Jones AE, Yiannibas V, Johnson C, Kline JA.
Emergencydepartment hypotension predicts sudden
unexpectedin-hospital mortality: a prospective cohort study.
Chest2006;130:941-6.
19. Aduen J, Bernstein WK, Khastgir T, Miller J, Kerzner
R,Bhatiani A et al. e use and clinical importance of a sub-e use
and clinical importance of a sub-strate-specific electrode for
rapid determination of bloodlactate concentrations. JAMA
1994;272:1678-85.
20. Mikkelsen ME, Miltiades AN, Gaieski DF, Goyal M,Fuchs BD,
Shah CV et al. Serum lactate is associated withmortality in severe
sepsis independent of organ failure andshock. Crit Care Med
2009;37:1670-7.
21. Trzeciak S, Dellinger RP, Chansky ME, Arnold RC,Schorr C,
Milcarek B et al. Serum lactate as a predictor ofmortality in
patients with infection. Intensive Care Med2007;33:970-7.
22. Shapiro NI, Howell MD, Talmor D, Nathanson LA, Lis-bon A,
Wolfe RE et al. Serum lactate as a predictor of mor-tality in
emergency department patients with infection.
Ann Emerg Med 2005;45:524-8. 23. Pearse RM. Extending the role
of lactate measurement into
the prehospital environment. Crit Care 2009;13:115. 24. Marshall
JC, al Naqbi A. Principles of source control in the
management of sepsis. Crit Care Clin
2009;25:753-768,viii-ix.
25. Siddiqui S, Razzak J. Early versus late pre-intensive care
unitadmission broad spectrum antibiotics for severe sepsis
inadults. Cochrane Database Syst Rev 2010;10:CD007081.
26. Gaieski DF, Mikkelsen ME, Band RA, Pines JM, MassoneR, Furia
FF et al. Impact of time to antibiotics on survivalin patients with
severe sepsis or septic shock in whom earlygoal-directed therapy
was initiated in the emergency de-
partment. Crit Care Med 2010;38:1045-53. 27. Natanson C, Danner
RL, Reilly JM, Doerfler ML, Hoff-man WD, Akin GL et al. Antibiotics
versus cardiovascularsupport in a canine model of human septic
shock. Am JPhysiol 1990;259(5 Pt 2):H1440-7.
28. Kumar A, Ellis P, Arabi Y, Roberts D, Light B, Parrillo JE
etal. Initiation of inappropriate antimicrobial therapy resultsin a
fivefold reduction of survival in human septic shock.Chest
2009;136:1237-48.
29. Puskarich MA, Trzeciak S, Shapiro NI, Arnold RC, Hor-ton JM,
Studnek JR et al. Association between timing ofantibiotic
administration and mortality from septic shockin patients treated
with a quantitative resuscitation proto-col. Crit Care Med
2011;39:2066-71.
30. Hutchison RW, Govathoti DA, Fehlis K, Zheng Q, Cot-trell JH,
Franklin N et al. Improving severe sepsis out-comes: cost and time
to first antibiotic dose. Dimens CritCare Nurs 2011;30:277-82.
telemedicine and comprehensive CQI feedbackis feasible, modifies
clinician behavior and is as-sociated with decreased hospital
mortality.41, 87,103, 122, 126, 143
Conclusions
One decade later, multiple studies (Table II)have not only
validated the RB and its elementsbut also provide evidence that
this therapymodulates inflammation, decreases organ
failureprogression and conserves health care resourceconsumption.
is approach consistently saves 1out of every 6 lives for patients
presenting with
severe sepsis and septic shock. While implemen-tation remains
challenging, the RB remains oneof the most effective interventions
in the man-agement of severe sepsis and septic shock.
References
1. Rackow EC, Astiz ME. Pathophysiology and treatment ofseptic
shock. JAMA 1991;266:548-54.
2. Brun-Buisson C, Doyon F, Carlet J, Dellamonica P, GouinF,
Lepoutre A et al. Incidence, risk factors, and outcome ofsevere
sepsis and septic shock in adults. A multicenter pro-spective study
in intensive care units. French ICU Groupfor Severe Sepsis. JAMA
1995;274:968-74.
3. Levy MM, Macias WL, Vincent JL, Russell JA, Silva E,Trzaskoma
B et al. Early changes in organ function pre-dict eventual survival
in severe sepsis. Crit Care Med2005;33:2194-201.
4. Kasnitz P, Druger GL, Yorra F, Simmons DH. Mixed ve-nous
oxygen tension and hyperlactatemia. Survival in se-vere
cardiopulmonary disease. JAMA 1976;236:570-4.
5. Astiz ME, Rackow EC, Weil MH. Oxygen delivery andutilization
during rapidly fatal septic shock in rats. CircShock
1986;20:281-90.
6. Rady MY, Rivers EP, Nowak RM. Resuscitation of thecritically
ill in the ED: responses of blood pressure, heartrate, shock index,
central venous oxygen saturation, andlactate. Am J Emerg Med
1996;14:218-25.
7. Vincent JL, De Backer D. Oxygen uptake/oxygen
supplydependency: fact or fiction? Acta Anaesthesiol Scand
Suppl1995;107:229-37.
8. Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A,Knoblich B
et al. Early goal-directed therapy in the treat-ment of severe
sepsis and septic shock. N Engl J Med2001;345:1368-77.
9. Friedman G, De Backer D, Shahla M, Vincent JL. Oxygensupply
dependency can characterize septic shock. IntensiveCare Med
1998;24:118-23.
10. Rahal L, Garrido AG, Cruz RJ Jr, Silva E,
Poli-de-Figue-iredo LF. Fluid replacement with hypertonic or
isotonicsolutions guided by mixed venous oxygen saturation in
ex-perimental hypodynamic sepsis. J Trauma 2009;67:1205-12.
11. Astiz ME, Rackow EC, Kaufman B, Falk JL, Weil
MH.Relationship of oxygen delivery and mixed venous oxy-genation to
lactic acidosis in patients with sepsis and acutemyocardial
infarction. Crit Care Med 1988;16:655-8.
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
10/13
EARLY INTERVENTIONS IN SEVERE SEPSIS AND SEPTIC SHOCK RIVERS
Vol. 78 - No. 6 MINERVA ANESTESIOLOGICA 721
sis bundles as processes of care: A meta-analysis. Aust CritCare
2011;24:229-43.
51. Grissom CK, Morris AH, Lanken PN, Ancukiewicz M,Orme JF Jr,
Schoenfeld DA et al. Association of physicalexamination with
pulmonary artery catheter parameters in
acute lung injury. Crit Care Med 2009;37:2720-6. 52. Ising P,
Smith TW, Simpson SQ. Effect of intermittent vscontinuous ScvO2
monitoring on sepsis bundle compli-ance and mortality. Chest
2009;136:21S.
53. Napoli AM, Machan JT, Forcada A, Corl K. Tissue oxy-genation
does not predict central venous oxygenation inemergency department
patients with severe sepsis and sep-tic shock. Acad Emerg Med
2010;17:349-52.
54. Colin G, Nardi O, Polito A, Aboab J, Maxime V, ClairB et al.
Masseter tissue oxygen saturation predicts normalcentral venous
oxygen saturation during early goal-direct-ed therapy and predicts
mortality in patients with severesepsis. Crit Care Med
2012;40:435-40.
55. Mesquida J, Masip J, Gili G, Artigas A, Baigorri F. -enar
oxygen saturation measured by near infrared spec-troscopy as a
non-invasive predictor of low central venous
oxygen saturation in septic patients. Intensive Care
Med2009;35:1106-9. 56. Walden AP, Young JD, Sharples E. Bench to
bedside: A
role for erythropoietin in sepsis. Crit Care 2010;14:227. 57.
Sakr Y, Chierego M, Piagnerelli M, Verdant C, Dubois
MJ, Koch M et al. Microvascular response to red blood
celltransfusion in patients with severe sepsis. Crit Care
Med2007;35:1639-44.
58. Vincent JL, Sakr Y, Sprung C, Harboe S, Damas P. Areblood
transfusions associated with greater mortality rates?Results of the
sepsis occurrence in acutely ill patients study.
Anesthesiology 2008;108:31-9.59. Hebert PC, Tinmouth A, Corwin
HL. Controversies in
RBC transfusion in the critically ill. Chest
2007;131:1583-90.
60. Parrillo JE. Cardiovascular dysfunction in septic shock:
new
insights into a deadly disease. Int J Cardiol 1985;7:314-21. 61.
Afessa B. Elements of the sepsis resuscitation bundle notequally
associated with reduced mortality. Crit Care Med2011;39:252-8.
62. Krafft P, Steltzer H, Hiesmayr M, Klimscha W, Ham-merle AF.
Mixed venous oxygen saturation in criticallyill septic shock
patients. e role of defined events. Chest1993;103:900-6.
63. Ebihara S, Hussain SN, Danialou G, Cho WK, Gott-fried SB,
Petrof BJ. Mechanical ventilation protectsagainst diaphragm injury
in sepsis: interaction of oxida-tive and mechanical stresses. Am J
Respir Crit Care Med2002;165:221-8.
64. Hussain SN, Simkus G, Roussos C. Respiratory musclefatigue:
a cause of ventilator failure in septic shock. J ApplPhysiol
1985;58:2033-40.
65. Manthous CA, Hall JB, Kushner R, Schmidt GA, RussoG, Wood
LD. e effect of mechanical ventilation on oxy-gen consumption in
critically ill patients. Am J Respir CritCare Med
1995;151:210-4.
66. Papazian L, Forel JM, Gacouin A, Penot-Ragon C, Per-rin G,
Loundou A et al. Neuromuscular blockers inearly acute respiratory
distress syndrome. N Engl J Med2010;363:1107-16.
67. Falk JL, Rackow EC, Leavy J, Astiz ME, Weil MH. De-layed
lactate clearance in patients surviving circulatoryshock. Acute
care 1985;11:212-5.
68. Nguyen HB, Kuan WS, Batech M, Shrikhande P, Ma-hadevan M, Li
CH et al. Outcome effectiveness of thesevere sepsis resuscitation
bundle with addition of lactateclearance as a bundle item: a
multinational evaluation. CritCare 2011;15:R229.
69. Jones AE, Shapiro NI, Trzeciak S, Arnold RC, ClaremontHA,
Kline JA. Lactate clearance vs central venous oxygen
31. National Heart, Lung, and Blood Institute Acute
Respira-National Heart, Lung, and Blood Institute Acute
Respira-tory Distress Syndrome (ARDS) Clinical Trials Network,
Wiedemann HP, Wheeler AP, Bernard GR, ompson BT,Hayden D,
deBoisblanc B et al. Comparison of two fluidmanagement strategies
in acute lung injury. N Engl J Med
2006;354:2564-75. 32. Magder S, Bafaqeeh F. e clinical role of
central venouspressure measurements. J Intensive Care Med
2007;22:44-51.
33. Varpula M, Tallgren M, Saukkonen K, Voipio-Pulkki LM,Pettila
V. Hemodynamic variables related to outcome inseptic shock.
Intensive Care Med 2005;31:1066-71.
34. Ferrer R, Artigas A, Suarez D, Palencia E, Levy MM,
Aren-zana A et al. Effectiveness of treatments for severe sepsis:
aprospective multicenter observational study. Am J RespirCrit Care
Med 2009;180:861-6.
35. Boyd JH, Forbes J, Nakada TA, Walley KR, Russell JA.Fluid
resuscitation in septic shock: a positive fluid balanceand elevated
central venous pressure are associated with in-creased mortality.
Crit Care Med 2011;39:259-65.
36. Murphy CV, Schramm GE, Doherty JA, Reichley RM,
Gajic O, Afessa B et al. e importance of fluid manage-e
importance of fluid manage-ment in acute lung injury secondary to
septic shock. Chest2009;136:102-9.
37. Delaney AP, Dan A, McCaffrey J, Finfer S. e role ofalbumin
as a resuscitation fluid for patients with sepsis:a systematic
review and meta-analysis. Crit Care Med2011;39:386-91.
38. Dnser MW, Takala J, Ulmer H, Mayr VD, Luckner G,Jochberger S
et al. Arterial blood pressure during earlysepsis and outcome.
Intensive Care Med 2009;35:1225-33.
39. Kampmeier TG, Rehberg S, Westphal M, Lange M. Va-sopressin
in sepsis and septic shock. Minerva Anestesiol2010;76:844-50.
40. Cohen R. Use of corticosteroids in septic shock.
MinervaAnestesiol 2011;77:190-5.
41. Micek ST, Roubinian N, Heuring T, Bode M, WilliamsJ,
Harrison C et al. Before-after study of a standardizedhospital
order set for the management of septic shock. CritCare Med
2006;34:2707-13.
42. De Backer D, Biston P, Devriendt J, Madl C, ChochradD,
Aldecoa C et al. Comparison of dopamine and nore-pinephrine in the
treatment of shock. N Engl J Med2010;362:779-89.
43. Vallet B, Robin E, Lebuffe G. Venous oxygen saturation asa
physiologic transfusion trigger. Crit Care 2010;14:213.
44. Shah S, Ouellette DR. Early goal-directed therapy for
sepsisin patients with preexisting left ventricular dysfunction:
aretrospective comparison of outcomes based upon protocoladherence.
Chest 2010;138(4 MeetingAbstracts):897A.
45. Hernandez G, Pea H, Cornejo R, Rovegno M, RetamalJ, Navarro
JL et al. Impact of emergency intubation on
central venous oxygen saturation in critically ill patients:
amulticenter observational study. Crit Care 2009;13:R63. 46. Perner
A, Haase N, Wiis J, White JO, Delaney A. Central
venous oxygen saturation for the diagnosis of low cardiacoutput
in septic shock patients. Acta Anaesthesiol
Scand2010;54:98-102.
47. Bronicki RA. Venous oximetry and the assessment of oxy-gen
transport balance. Pediatr Crit Care Med 2011;12.
48. Blasco V, Leone M, Textoris J, Visintini P, Albanese
J,Martin C. [Venous oximetry: physiology and
therapeuticimplications]. Ann Fr Anesth Reanim 2008;27:74-82.
49. Castellanos-Ortega A, Suberviola B, Garca-AstudilloLA,
Holanda MS, Ortiz F, Llorca J et al. Impact of thesurviving sepsis
campaign protocols on hospital length ofstay and mortality in
septic shock patients: Results of a3-year follow-up
quasi-experimental study. Crit Care Med2010;38:1036-43.
50. Chamberlain DJ, Willis EM, Bersten AB. e severe sep-
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
11/13
RIVERS EARLY INTERVENTIONS IN SEVERE SEPSIS AND SEPTIC SHOCK
722 MINERVA ANESTESIOLOGICA June 2012
with hypoperfusion]. Zhonghua Wai Ke Za Zhi (ChineseJournal of
Surgery) 2006;44:1193-6.
87. Nguyen HB, Corbett SW, Steele R, Banta J, Clark RT,Hayes
SRet al. Implementation of a bundle of quality in-dicators for the
early management of severe sepsis and sep-
tic shock is associated with decreased mortality. Crit CareMed
2007;35:1105-12. 88. Chen ZQ, Jin YH, Chen H, Fu WJ, Yang H, Wang
RT.
[Early goal-directed therapy lowers the incidence, severityand
mortality of multiple organ dysfunction syndrome].Nan Fang Yi Ke Da
Xue Xue Bao 2007;27:1892-5.
89. Jones AE, Focht A, Horton JM, Kline JA. Prospective
ex-ternal validation of the clinical effectiveness of an emergen-cy
department-based early goal-directed therapy protocolfor severe
sepsis and septic shock. Chest 2007;132:425-32.
90. Sebat F, Musthafa AA, Johnson D, Kramer AA, ShoffnerD,
Eliason M et al. Effect of a rapid response system forpatients in
shock on time to treatment and mortality dur-ing 5 years. Crit Care
Med 2007;35:2568-75.
91. El Solh AA, Akinnusi ME, Alsawalha LN, Pineda LA.Outcome of
septic shock in older adults after implementa-
tion of the sepsis bundle. J Am Geriatr Soc 2008;56:272-8. 92.
He ZY, Gao Y, Wang XR, Hang YN. [Clinical evaluation
of execution of early goal directed therapy in septic
shock].Zhongguo Wei Zhong Bing Ji Jiu Yi Xue 2007;19:14-6.
93. Castro R, Regueira T, Aguirre ML, Llanos OP, BruhnA, Bugedo
G et al. An evidence-based resuscitation algo-rithm applied from
the emergency room to the ICU im-proves survival of severe septic
shock. Minerva Anestesiol2008;74:223-31.
94. Zambon M, Ceola M, Almeida-de-Castro R, Gullo A,Vincent JL.
Implementation of the Surviving Sepsis Cam-paign guidelines for
severe sepsis and septic shock: wecould go faster. J Crit Care
2008;23:455-60.
95. Zubrow MT, Sweeney TA, Fulda GJ, Seckel MA, EllicottAC,
Mahoney DD et al. Improving care of the sepsis pa-
tient. Jt Comm J Qual Patient Saf 2008;34:187-91. 96. Peel M.
Care bundles: resuscitation of patients with severesepsis. Nurs
Stand 2008;23:41-6.
97. Focht A, Jones AE, Lowe TJ. Early goal-directed ther-apy:
improving mortality and morbidity of sepsis in theemergency
department. Jt Comm J Qual Patient Saf2009;35:186-91.
98. Moore LJ, Jones SL, Kreiner LA, McKinley B, Sucher JF,Todd
SR et al. Validation of a screening tool for the
earlyidentification of sepsis. J Trauma
2009;66:1539-1546;discussion 1546-37.
99. Puskarich MA, Marchick MR, Kline JA, Steuerwald MT,Jones AE.
One year mortality of patients treated with anemergency department
based early goal directed therapyprotocol for severe sepsis and
septic shock: a before andafter study. Crit Care 2009;13:R167.
100. Ferrer R, Artigas A, Levy MM, Blanco J, Gonzlez-Daz
G,Garnacho-Montero J et al. Improvement in process of careand
outcome after a multicenter severe sepsis educationalprogram in
Spain. JAMA 2008;299:2294-303.
101. Girardis M, Rinaldi L, Donno L, Marietta M, CodeluppiM,
Marchegiano P et al. Effects on management and out-come of severe
sepsis and septic shock patients admittedto the intensive care unit
after implementation of a sepsisprogram: a pilot study. Crit
Care2009;13:R143.
102. Wang JL, Chin CS, Chang MC, Yi CY, Shih SJ, Hsu JY etal.
Key process indicators of mortality in the implementa-tion of
protocol-driven therapy for severe sepsis. J FormosMed Assoc
2009;108:778-87.
103. iel SW, Asghar MF, Micek ST, Reichley RM, DohertyJA, Kollef
MH. Hospital-wide impact of a standardizedorder set for the
management of bacteremic severe sepsis.Crit Care Med
2009;37:819-24.
104. Pestaa D, Espinosa E, Sangesa-Molina JR, Ramos R, P-
saturation as goals of early sepsis therapy: a
randomizedclinical trial. JAMA 2010;303:739-46.
70. Jansen TC, van Bommel J, Schoonderbeek FJ, Sleeswi-Jansen
TC, van Bommel J, Schoonderbeek FJ, Sleeswi-jk Visser SJ, van der
Klooster JM, Lima AP et al. Earlylactate-guided therapy in
intensive care unit patients: a
multicenter, open-label, randomized controlled trial. AmJ Respir
Crit Care Med 2010;182:752-61. 71. James JH, Luchette FA, McCarter
FD, Fischer JE. Lactate
is an unreliable indicator of tissue hypoxia in injury or
sep-sis. Lancet 1999;354:505-8.
72. Dugas D, Mackenhauer J, Joyce N, Donnino M. Prevalenceand
characteristics of nonlactate and lactate expressors inseptic
shock. Crit Care Med 2009;37(Suppl.):A227.
73. Cannon CM, for the Multicenter Severe S, SepticShock
Collaborative G. e GENESIS Project (GEN-eralization of Early Sepsis
InterventionS): A MulticenterQuality Improvement Collaborative.
Acad Emerg Med2010;17:1258.
74. Na S, Joshi M, Li C-h, et al. Implementation of a
6-hoursevere sepsis bundle in multiple Asian countries is
associ-ated with decrease mortality. Chest 2009;136:20S-e.
75. Boulos M, Astiz ME, Barua RS, Osman M. Impairedmitochondrial
function induced by serum from septicshock patients is attenuated
by inhibition of nitric oxidesynthase and poly(ADP-ribose)
synthase. Crit Care Med2003;31:353-8.
76. Rivers EP, Kruse JA, Jacobsen G, Shah K, Loomba M,Otero R et
al. e influence of early hemodynamic opti-mization on biomarker
patterns of severe sepsis and septicshock. Crit Care Med
2007;35:2016-24.
77. Zagli G, Bonizzoli M, Spina R, Cianchi G, Pasquini
A,Anichini V et al. Effects of hemoperfusion with an immo-bilized
polymyxin-B fiber column on cytokine plasma lev-els in patients
with abdominal sepsis. Minerva Anestesiol2010;76:405-12.
78. Boerma EC, Koopmans M, Konijn A, Kaiferova K, BakkerAJ, van
Roon EN et al. Effects of nitroglycerin on sublin-
gual microcirculatory blood flow in patients with
severesepsis/septic shock after a strict resuscitation protocol:
adouble-blind randomized placebo controlled trial. CritCare Med
2010;38:93-100.
79. Kiers HD, Griesdale DE, Litchfield A, Reynolds S, GibneyRT,
Chittock Det al. Effect of early achievement of physi-ologic
resuscitation goals in septic patients admitted fromthe ward on the
kidneys. J Crit Care 2010;25:563-9.
80. Gao F, Melody T, Daniels DF, Giles S, Fox S. e impactof
compliance with 6-hour and 24-hour sepsis bundles onhospital
mortality in patients with severe sepsis: a prospec-tive
observational study. Crit Care 2005;9:R764-70.
81. Sebat F, Johnson D, Musthafa AA, Watnik M, Moore S,Henry K
et al. A multidisciplinary community hospitalprogram for early and
rapid resuscitation of shock in non-trauma patients. Chest
2005;127:1729-43.
82. Kortgen A, Niederprum P, Bauer M. Implementation ofan
evidence-based standard operating procedure andoutcome in septic
shock. Crit Care Med 2006;34:943-9.
83. Shapiro NI, Howell MD, Talmor D, Lahey D, Ngo L, Bu-ras J et
al. Implementation and outcomes of the MultipleUrgent Sepsis
erapies (MUST) protocol. Crit Care Med2006;34:1025-32.
84. Trzeciak S, Dellinger RP, Abate NL, Cowan RM, StaussM,
Kilgannon JH et al. Translating research to clinicalpractice: a
1-year experience with implementing early goal-directed therapy for
septic shock in the emergency depart-ment. Chest
2006;129:225-32.
85. Lin SM, Huang CD, Lin HC, Liu CY, Wang CH, KuoHP. A modified
goal-directed protocol improves clinicaloutcomes in intensive care
unit patients with septic shock:a randomized controlled trial.
Shock 2006;26:551-7.
86. Qu HP, Qin S, Min D, Tang YQ. [e effects of
earlierresuscitation on following therapeutic response in
sepsis
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
12/13
EARLY INTERVENTIONS IN SEVERE SEPSIS AND SEPTIC SHOCK RIVERS
Vol. 78 - No. 6 MINERVA ANESTESIOLOGICA 723
121. Casserly B, Baram M, Walsh P, Sucov A, Ward NS, LevyMM.
Implementing a collaborative protocol in a sepsis in-tervention
program: lessons learned. Lung 2011;189:11-9.
122. Schramm GE, Kashyap R, Mullon JJ, Gajic O, Afessa B.Septic
shock: A multidisciplinary response team and week-
ly feedback to clinicians improve the process of care
andmortality. Crit Care Med 2011;39:252-8.123. Suarez D, Ferrer R,
Artigas A, Azkarate I, Garnacho-
Montero J, Gom G et al. Cost-effectiveness of the Sur-viving
Sepsis Campaign protocol for severe sepsis: a pro-spective
nation-wide study in Spain. Intensive Care Med2011;37:444-52.
124. Shiramizo SC, Marra AR, Durao MS, Paes AT, EdmondMB, Pavao
dos Santos OF. Decreasing mortality in severesepsis and septic
shock patients by implementing a sepsisbundle in a hospital
setting. PLoS ONE 2011;6:e26790.
125. Tromp M, Tjan DH, van Zanten AR, Gielen-Wijffels SE,Goekoop
GJ, van den Boogaard M et al. e effects ofimplementation of the
Surviving Sepsis Campaign in theNetherlands. Neth J Med
2011;69:292-8.
126. Winterbottom F, Seoane L, Sundell E, Niazi J, Nash T.
Im-
proving sepsis outcomes for acutely Ill adults using
inter-disciplinary order sets. Clin Nurse Spec 2011;25:180-5.127.
Jeon K, Shin TG, Sim MS, Suh GY, Lim SY, Song HG et
al. Improvements in compliance of resuscitation bundlesand
achievement of end points after an educational pro-gram on the
management of severe sepsis and septic shock.Shock
2012;37:463-7.
128. Bastani A, Galens S, Rocchini A, Walch R, Shaqiri B,Palomba
K et al. ED identification of patients with severesepsis/septic
shock decreases mortality in a communityhospital. Am J Emerg Med
2011 [Epub ahead of print].
129. Rivers EP. Point: adherence to early goal-directed
therapy:does it really matter? Yes. After a decade, the
scientificproof speaks for itself. Chest 2010;138:476-80.
130. Daniels R. Surviving the first hours in sepsis: getting
thebasics right (an intensivists perspective). J Antimicrob
Chemother 2011;66(Suppl 2):ii11-23.131. Perel A, Segal E.
Management of sepsis. N Engl J Med2007;356:1178; author reply
1181-1172.
132. de Oliveira CF, de Oliveira DS, Gottschald AF, Moura
JD,Costa GA, Ventura AC et al. ACCM/PALS haemodynamicsupport
guidelines for paediatric septic shock: an outcomescomparison with
and without monitoring central venousoxygen saturation. Intensive
Care Med 2008;34:1065-75.
133. Maitland K, Kiguli S, Opoka RO, Engoru C, Olupot-Olupot P,
Akech SO et al. Mortality after fluid bolus in
African children with severe infection. N Engl J
Med2011;364:2483-95.
134. Carcillo JA, Davis AL, Zaritsky A. Role of early fluid
resus-citation in pediatric septic shock. JAMA 1991;266:1242-5.
135. de Oliveira CF. Early goal-directed therapy in treatment
of
pediatric septic shock. Shock 2010;34(Suppl 1):44-7.136.
Brierley J, Carcillo JA, Choong K, Cornell T, Decaen A,Deymann A et
al. Clinical practice parameters for hemo-dynamic support of
pediatric and neonatal septic shock:2007 update from the American
College of Critical CareMedicine. Crit Care Med 2009;37:666-88.
137. Aneja RK, Carcillo JA. Differences between adult
andpediatric septic shock. Minerva Anestesiol 2011;77:986-92.
138. Andrews R, Elixhauser A. e national hospital bill:
growthtrends and 2005 update on the most expensive conditionsby
payer. Healthcare Cost and Utilization Project. [cited2012 April
18]. Available at:
http://www.hcup-us.ahrq.gov/reports/statbriefs/sb42.pdf
139. Shorr AF, Micek ST, Jackson WL Jr, Kollef MH. Eco-nomic
implications of an evidence-based sepsis protocol:can we improve
outcomes and lower costs? Crit Care Med2007;35:1257-62.
rez-Fernndez E, Duque M et al. Compliance with a sepsisbundle
and its effect on intensive care unit mortality insurgical septic
shock patients. J Trauma 2010;69:1282-7.
105. Lefrant JY, Muller L, Raillard A, Jung B, Beaudroit
L,Favier L et al. Reduction of the severe sepsis or septic
shock
associated mortality by reinforcement of the recommenda-tions
bundle: A multicenter study. Ann Fr Anesth Reanim2010;29:621-8.
106. Cardoso T, Carneiro AH, Ribeiro O, Teixeira-Pinto
A,Costa-Pereira A. Reducing mortality in severe sepsis withthe
implementation of a core 6-hour bundle: results fromthe Portuguese
community-acquired sepsis study (SACiU-CI study). Crit Care
2010;14:R83.
107. [e effect of early goal-directed therapy on treatmentof
critical patients with severe sepsis/septic shock: a mul-ti-center,
prospective, randomized, controlled study].Zhongguo Wei Zhong Bing
Ji Jiu Yi Xue 2010;22:331-4.
108. Patel GW, Roderman N, Gehring H, Saad J, Bartek W.Assessing
the effect of the surviving sepsis campaign treat-ment guidelines
on clinical outcomes in a community hos-pital (November). Ann
Pharmacother 2010;44:1733-8.
109. Crowe CA, Mistry CD, Rzechula K, Kulstad CE. Evalua-tion of
a modified early goal directed therapy protocol. AmJ Emerg Med
2010;28:689-93.
110. Daniels R, Nutbeam T, McNamara G, Galvin C. e sepsissix and
the severe sepsis resuscitation bundle: a prospectiveobservational
cohort study. Emerg Med J 2011;28:507-12.
111. Gerber K. Surviving sepsis: a trust-wide approach. A
mul-ti-disciplinary team approach to implementing evidence-based
guidelines. Nurs Crit Care 2010;15:141-51.
112. Gurnani PK, Patel GP, Crank CW, Vais D, Lateef O,Akimov S
et al. Impact of the implementation of a sep-sis protocol for the
management of fluid-refractory septicshock: A single-center,
before-and-after study. Clin er2010;32:1285-93.
113. Levy MM, Dellinger RP, Townsend SR, Linde-ZwirbleWT,
Marshall JC, Bion J et al. e Surviving Sepsis Cam-
paign: results of an international guideline-based perform-ance
improvement program targeting severe sepsis. CriticalCare Medicine
2010;38:367-74.
114. Macredmond R, Hollohan K, Stenstrom R, Nebre R, Jas-wal D,
Dodek P. Introduction of a comprehensive manage-ment protocol for
severe sepsis is associated with sustainedimprovements in
timeliness of care and survival. Qual SafHealth Care
2010;19:e46.
115. Mikkelsen ME, Gaieski DF, Goyal M, et al. Factors
associ-ated with non-adherence with early goal-directed therapyin
the Emergency Department. Chest 2010.
116. Coba V, Whitmill M, Mooney R, Horst HM, Brandt MM,Digiovine
B et al. Resuscitation bundle compliance in se-vere sepsis and
septic shock: improves survival, is betterlate than never. J
Intensive Care Med 2011 [Epub ahead ofprint].
117. Sivayoham N, Rhodes A, Jaiganesh T, van Zyl Smit
N,Elkhodhair S, Krishnanandan S. Outcomes from imple-menting early
goal-directed therapy for severe sepsis andseptic shock: a 4-year
observational cohort study. Eur JEmerg Med 2011 [Epub ahead of
print].
118. Westphal GA, Koenig , Caldeira Filho M, Feij J, de
Ol-iveira LT, Nunes F et al. Reduced mortality after the
im-plementation of a protocol for the early detection of
severesepsis. J Crit Care 2011;26:76-81.
119. Castellanos-Ortega A, Suberviola B, Garcia-Astudillo
LA,Ortiz F, Llorca J, Delgado-Rodriguez M. Late compliancewith the
sepsis resuscitation bundle: impact on mortality.Shock
2011;36:542-7.
120. ONeill R, Morales J, Jule M. Early goal-directed
therapy(EGDT) for severe sepsis/septic shock: which componentsof
treatment are more difficult to implement in a com-munity-based
emergency department? J Emerg Med 2011[Epub ahead of print].
-
8/13/2019 Early Interventionsin Severesepsis and Septic Shock
JOB
13/13
RIVERS EARLY INTERVENTIONS IN SEVERE SEPSIS AND SEPTIC SHOCK
724 MINERVA ANESTESIOLOGICA June 2012
to meeting early goal-directed therapy using telemedicine.Crit
Care Nurs Q 2011;34:187-99.
144. Kumar A, Ellis P, Arabi Y, Roberts D, Light B, Parrillo JE
etal. Initiation of inappropriate antimicrobial therapy resultsin a
5-fold reduction of survival in human septic shock.
Chest 2009;136:1237-48.145. Estenssoro E, Gonzalez F, Laffaire
E, Canales H, Senz G,Reina R et al. Shock on admission day is the
best predic-tor of prolonged mechanical ventilation in the ICU.
Chest2005;127:598-603.
146. Stahl W, Radermacher P, Georgieff M, Bracht H.
Centralvenous oxygen saturation and emergency intubation--an-other
piece in the puzzle? Crit Care 2009;13:172.
140. Talmor D, Greenberg D, Howell MD, Lisbon A, No-vack V,
Shapiro N. e costs and cost-effectiveness ofan integrated sepsis
treatment protocol. Crit Care Med2008;36:1168-74.
141. Cannon C, Holthaus C, Rivers E, et al. Improving out-
come in severe sepsis and septic shock: results of a
prospec-tive multicenter collaborative. J Emerg Med
2009;37:217-36.
142. Ferrer RMD, Artigas AMDP, Levy MMMDF, et al. Im-provement
in process of care and outcome after a multi-center severe sepsis
educational program in Spain. JAMA2008;299:2294-303.
143. Loyola S, Wilhelm J, Fornos J. An innovative approach
Conflicts of interest.None related to this publication. Dr.
Rivers receives research support from the National Institute of
Health, Aggennixand Alere Corporation. In the past four years, he
has been a onetime consultant for Aggennix, Esai Pharmaceuticals
Idaho Technologies,
Astra Zeneca, Massimo and Sangard. Dr. Rivers has never
personally owned any patents or Early Interventions in Severe
Sepsis and SepticShock: e Evidence One Decade Later received
royalties, stock or research support associated with the EGDT
study. Dr. Cannon hasreceived consulting fees from Eisai
Pharmaceuticals.
Received on May 3, 2011 - Accepted for publication on March 21,
2012.Corresponding author: E. P. Rivers, MD, MPH, Vice Chairman and
Research Director, Department of Emergency Medicine, Senior
StaffAttending in Surgical Critical Care and Emergency Medicine,
Clinical Professor, Wayne State University, 270-Clara Ford
Pavilion, HenryFord Hospital, 2799 West Grand Boulevard, Detroit,
MI 48202, USA. E-mail: [email protected] article is freely
available at www.minervamedica.it


















![Septic Shock [EDocFind.com]](https://img.pdfslide.us/doc/110x75/55cf8fb1550346703b9edc7d/septic-shock-edocfindcom.jpg)