Embed Size (px)
Citation preview
Early Infant Diagnosis Programme
By
DR A K Gupta, MD (Pediatrics)
Additional Project Director cum Technical Lead
Delhi State AIDS Control Society
Govt of Delhi

Why early diagnosis is crucial in Infants ?
Rapid HIV progression and higher risk of death in infected infants
CD4 and viral load are poor predictors of disease progression in infants
Without Anti Retroviral treatment:
By age 1, one-third of all HIV-infected children will have
Died
By age 2, half of all HIV-infected children will have died

Mortality of HIV-infected Infants
3
1 Year = 35%
mortality
2 Years = 53%
mortalityNewell ML Newell ML et al Lancet 2004; 364: 1236-43
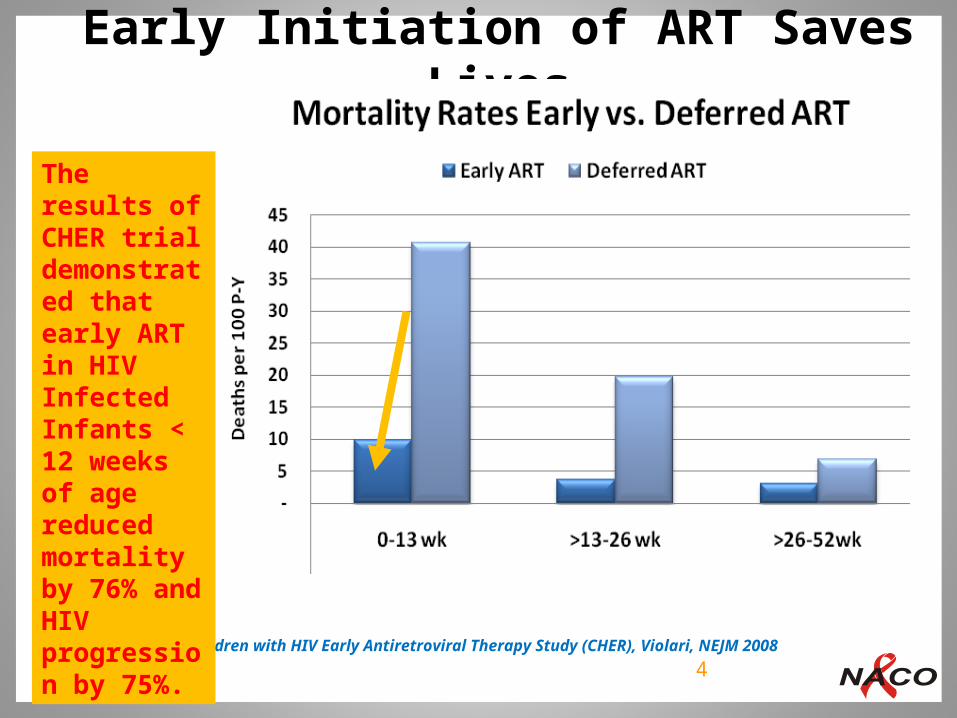
Early Initiation of ART Saves Lives
From the Children with HIV Early Antiretroviral Therapy Study (CHER), Violari, NEJM 2008 4
The results of CHER trial demonstrated that early ART in HIV Infected Infants < 12 weeks of age reduced mortality by 76% and HIV progression by 75%.

5
Goals of Early Infant Diagnosis
To identify the HIV-infected child early, prior to the development of clinical disease during the first months of life. Diagnosis should be early enough so interventions and Anti Retroviral treatment can be started Start ART in all confirmed HIV Infected infants irrespective of clinical or immunological status to reduce pediatric mortality and morbidity

1. Rapid HIV Antibody Tests 2. RNA PCR 3. DNA PCR4. Point of Care Tests (P24 assay)
Possible Methods of Diagnosis
Rapid Antibody Tests
Limited Value in EID
Due to trans-placental transfer of maternal antibodies from mother to child during pregnancy, childbirth and breastfeeding.
Early Infant Diagnosis
8
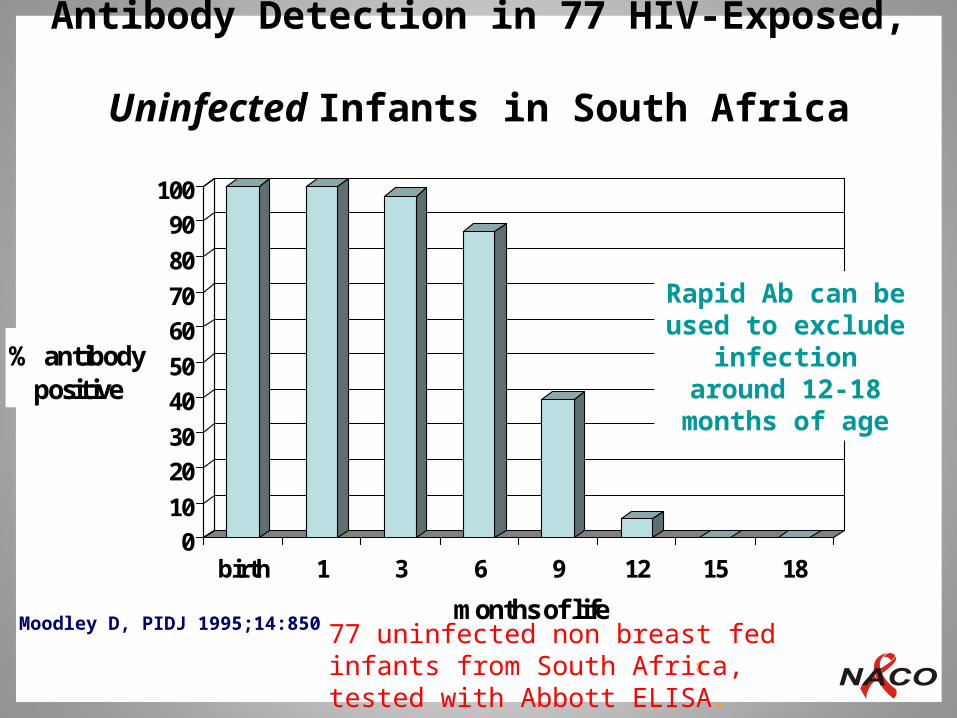
Antibody Detection in 77 HIV-Exposed, Uninfected Infants in South Africa
0
10
20
30
40
50
60
70
80
90
100
% antibody positive
birth 1 3 6 9 12 15 18
months of lifeMoodley D, PIDJ 1995;14:850
Rapid Ab can be used to exclude
infection around 12-18 months of age
77 uninfected non breast fed infants from South Africa, tested with Abbott ELISA.
Limited Value for EID:
(1) Sensitivity of RNA assays is affected if mothers or infants received antiretroviral drugs for PMTCT.
(2) Plasma is required for RNA assays which is difficult to obtain than whole blood required for DNA PCR
RNA PCR can be used for viral load monitoring after established diagnosis.
RNA PCR for Infant Diagnosis-
10
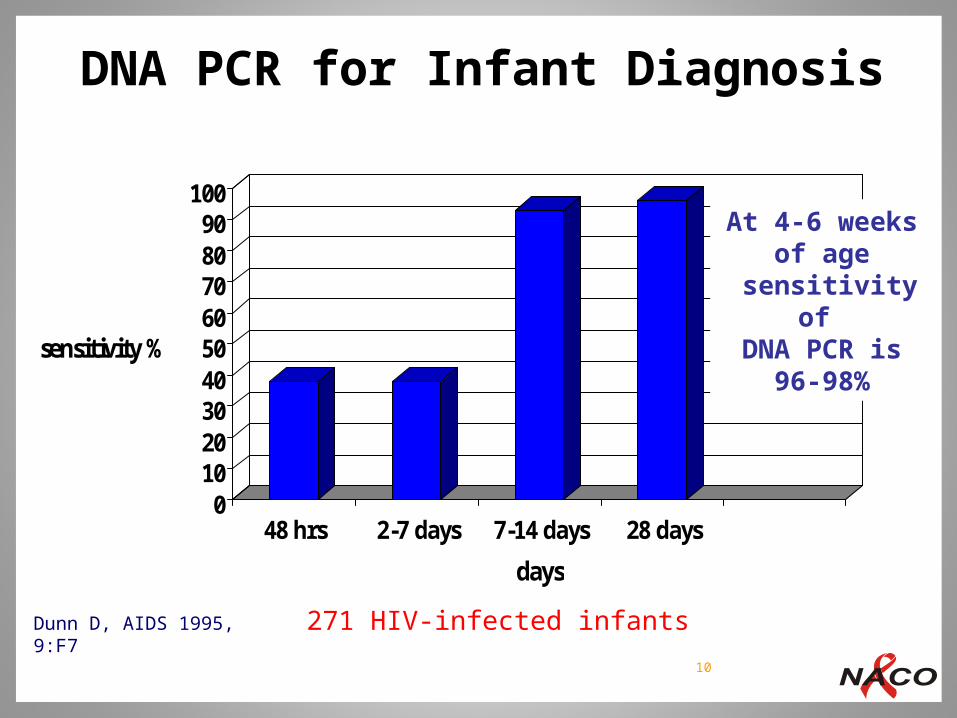
DNA PCR for Infant Diagnosis
0102030405060708090
100
sensitivity %
48 hrs 2-7 days 7-14 days 28 days
days
Dunn D, AIDS 1995, 9:F7
At 4-6 weeks of age
sensitivity of DNA PCR is 96-
98%
271 HIV-infected infants
-HIV p24 antigen is produced at high levels within the first few weeks of infection but quickly becomes bound to specific antibodies which make it unable to be detected by standard antigen-detection serological tests. -Heat treatment of the sample dissociates p24 from these complexes (the First Ultrasensitive POC p24 test). It is a sensitive and highly specific marker for HIV infection Result Time – 1 hour (Northwestern University)-Limitations- Testing at Multiple sites, Extensive Trainings, Monitoring, More Stock outs
Point-of-Care Testing for EID
HIV exposed - Definition:
Infants and children born to mothers infected with HIV, until HIV infection can be reliably excluded or confirmed in them
Infant: Under 12 months
Child: One year-upto 15 years
Early Infant Diagnosis
HIV Exposed Infant / Child
4
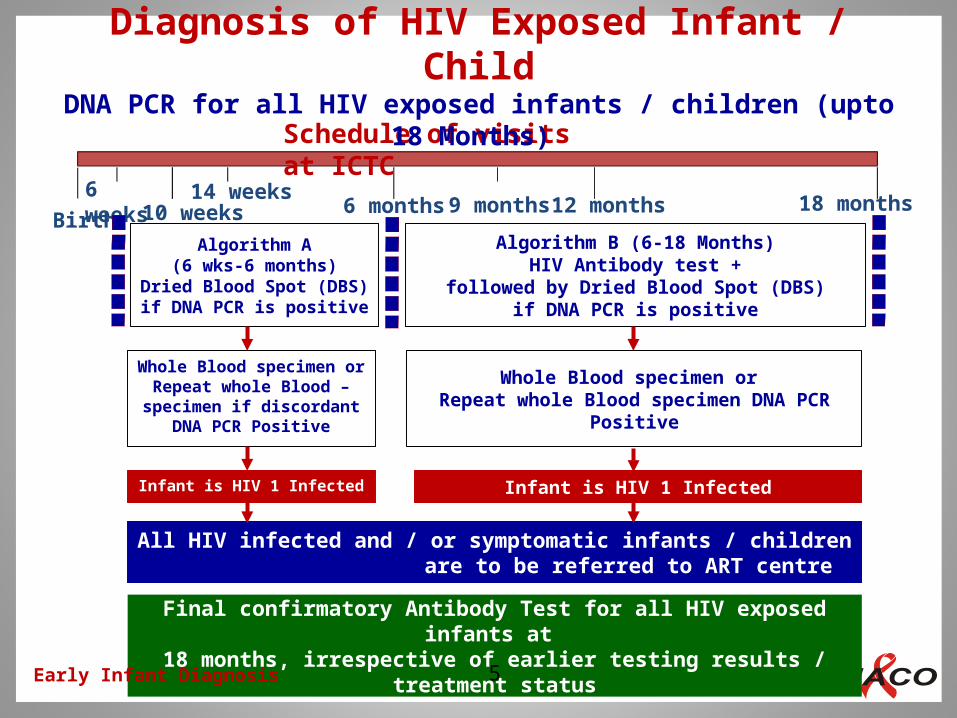
6 weeks10 weeks
14 weeks6 months 9 months 12 months 18 months
All HIV infected and / or symptomatic infants / children are to be referred to ART centre
Final confirmatory Antibody Test for all HIV exposed infants at 18 months, irrespective of earlier testing results / treatment status
Birth
Schedule of visits at ICTC
Algorithm A(6 wks-6 months)
Dried Blood Spot (DBS) if DNA PCR is positive
Algorithm B (6-18 Months)HIV Antibody test +
followed by Dried Blood Spot (DBS)if DNA PCR is positive
Whole Blood specimen or Repeat whole Blood – specimen if discordant
DNA PCR Positive
Whole Blood specimen or Repeat whole Blood specimen DNA PCR
Positive
Infant is HIV 1 Infected Infant is HIV 1 Infected
Diagnosis of HIV Exposed Infant / ChildDNA PCR for all HIV exposed infants / children (upto 18 Months)
Early Infant Diagnosis 5

Collect and send Whole Blood Specimen for HIV-1 DNA PCR (At ART Centre)
HIV-1 DNA detected
Infant is HIV-1 infected
HIV-1 DNA not detected
Refer to ART Centre
A. Infants Less than 6 months old and born to HIV positive Mother
Establish definitive diagnosis at 18 months by 3 Rapid HIV antibody tests
HIV-1 DNA not detectedHIV-1 DNA detected
Collect and Send Dried Blood Spot (DBS) of babies between 6 weeks to <6 months of age for HIV -1 DNA PCR (AT ICTC)
Infant in follow up- retesting at six months if asymptomatic or earlier if they become symptomatic
Lab will request for Fresh Whole Blood specimen from ART Centre if result is discordant and rely on the final whole blood test result
Infant is HIV-1 uninfected
HIV-1 DNA not detectedHIV-1 DNA detected
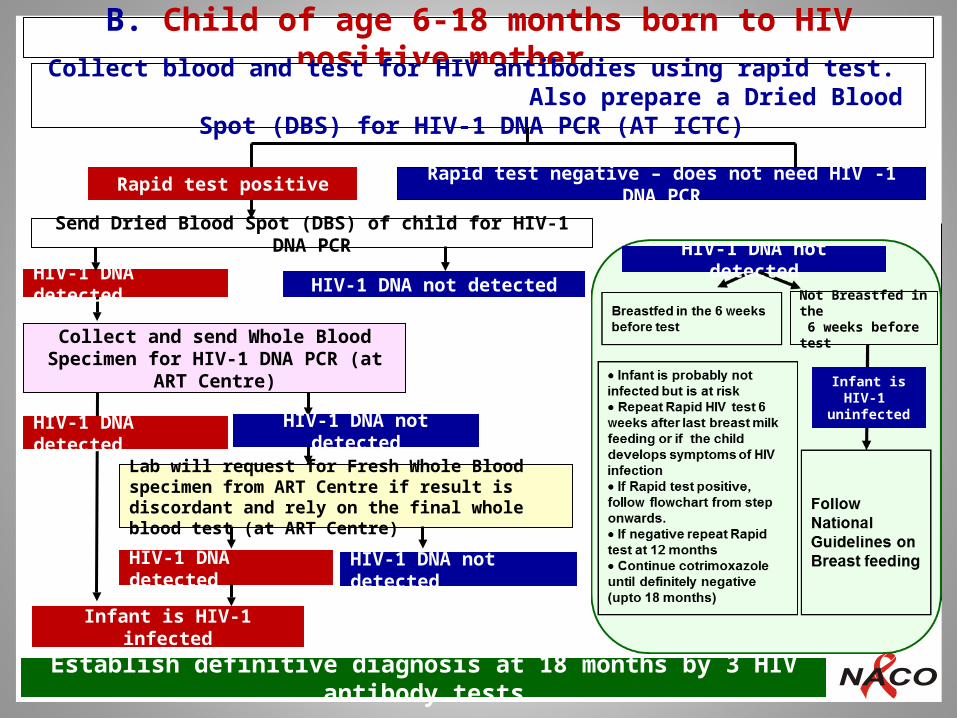
B. Child of age 6-18 months born to HIV positive mother
HIV-1 DNA not detected
HIV-1 DNA detected
Collect and send Whole Blood Specimen for HIV-1 DNA PCR (at ART Centre)
HIV-1 DNA detected
Send Dried Blood Spot (DBS) of child for HIV-1 DNA PCR
Infant is HIV-1 infected
Lab will request for Fresh Whole Blood specimen from ART Centre if result is discordant and rely on the final whole blood test (at ART Centre)
HIV-1 DNA detected HIV-1 DNA not detected
HIV-1 DNA not detected
Collect blood and test for HIV antibodies using rapid test. Also prepare a Dried Blood Spot (DBS) for HIV-1 DNA PCR (AT ICTC)
Rapid test negative – does not need HIV -1 DNA PCRRapid test positive
Early Infant DiagnosisEstablish definitive diagnosis at 18 months by 3 HIV antibody tests
Infant is HIV-1 uninfected
Not Breastfed in the 6 weeks before test
HIV-1 DNA not detected

Discordance among the EID results and Rapid tests at 18 months
Early Infant Diagnosis
Continue ART irrespective of Antibody Test results at 18 months, if ART had been initiated on the basis Positive DNA-PCR Result any time between 6 weeks and 18 Months
This discordance needs further evaluation
A Discordance Evaluation Algorithm is as below:
If negative at 18 months, repeat 3 antibody tests at the same testing site after 1 month
If Positive, Continue ART
If still negative, Continue ART, do DNA PCR
If DNA-PCR negative, still Continue ART But refer to CoE for viral load testing and decision on a case-to-case basis: Refer to NACEP for further advice
9
Clinical Assessment of Symptomatic Infants and Children
Based on:
Clinical history and Physical examination
Signs and symptoms as per IMNCI-HIV guidelines
Nutritional evaluation
Clinical Criterion for Presumptive diagnosis of severe HIV disease in infants/children < 18 month:
HIV Exposed infant/child + Ab Test Positive + AIDS defining illness /or 2 or more of following:
Oral thrush, Severe pneumonia, Severe sepsis, persistent diarrhea, enlarged lymph nodes, Ear Infections, Parotid enlargement, malnutrition
IMNCI: Integrated Management of Neonatal and Childhood IllnessesEarly Infant Diagnosis 7
Components of Care of HIV-Exposed Infant / Child
Immediate Care at Birth
Infant feeding
ARV prophylaxis
Cotrimoxazole preventive Therapy (CPT)
Immunization and Vitamin A Supplementation
Growth and Development
Early infant diagnosis
Follow up
Early Infant Diagnosis 10
Immediate Care at Birth
Follow universal precautions
Do not milk the cord
The cord should be clamped soon after birth
Cover the cord with gloved hand and gauze before cutting to avoid blood splattering
Initiate feeding within the first hour of birth in accordance with the preferred and informed choice of the mother
Early Infant Diagnosis 11

Infant Feeding
Counselling for infant feeding should begin in the antenatal period.
All HIV infected pregnant women should be informed about infant feeding options, viz. exclusive breast feeding or exclusive replacement feeding. Breast feeding is the preferred choice in developing countries as it maximises the chances of survival of the infant. Breast-feeding provides the infant with all required nutrients and immunological factors that help to protect against common infections
Breast feeding is generally begun within an hour in a normal vaginal delivery and within first 4 hours in a LSCS delivery
Mixed feeding i.e. breast milk and replacement feeds combined increases the risk of transmission of HIV and should be avoided at all cost
The health care providers and counsellors should be trained to help the pregnant women in reaching the right decision and to support them in implementing breast feeding
Early Infant Diagnosis 12

10 principles of infant feeding for HIV-infected women
1. All HIV positive pregnant women should have PPTCT interventions provided early in pregnancy as far as possible. The interventions include maternal ART and infant ARV prophylaxis
2. Exclusive breast feeding is the recommended infant feeding choice in the first 6 months
3. Only in situations where breastfeeding cannot be done or on individual parents’ informed decision, then replacement feeding may be considered only if all the 6 criteria for replacement feeding are met
4. Mixed feeding should not be practiced for the first six months at any cost, as it enhances the risk of transmission of HIV to the infant
5. Exclusive breast feeding should be done for first 6 months, after which complementary feeding should be introduced gradually, irrespective of whether the infant is diagnosed with HIV infection or is uninfected by early infant diagnosis
Early Infant Diagnosis 13

10 principles of infant feeding for HIV-infected women
6. Mother should be adherent to ART not only for the whole duration of breast feeding but for the entire duration of her life
7. Breast feeding should be stopped once a nutritionally adequate and safe diet without breast milk can be provided
8. For breast feeding infants who are diagnosed HIV uninfected, breast feeding should be continued till 12 months of age ONLY
9. For breast feeding infants diagnosed HIV infected, ART should be started and breast feeding should be continued till 2 years of age
10.Abrupt stopping of breast feeding should NOT be done. Mothers who decide to stop breast feeding should stop gradually taking comfort level of mother and infant into consideration
Early Infant Diagnosis 14

Safer Infant FeedingNACO Recommendations
Early Infant Diagnosis 15
Found HIV positive through EID algorithm:
For these infants, exclusive breast feeding is to be done till 6 months. Breast feeding should be continued up to 24 months.
Found HIV Negative through EID algorithm:
Exclusive breast feeding is to be done till 6 months and start complimentary feeding at 6 months of age. Breastfeeding should continue up till 12 months ONLY. Mothers who decide to stop breast feeding should stop gradually taking comfort level of mother and infant into consideration
HIV testing needs to be done again after cessation of breastfeeding according to the EID protocol

6 criteria for replacement feeding
1. Safe water and sanitation are assured at the household level and in the community
2. The mother or other caregiver can reliably afford to provide sufficient replacement feeding (milk), to support normal growth and development of the infant
3. The mother or caregiver can prepare replacement feeding frequently enough in a clean manner, so that it is safe and carries a low risk of Diarrhoea and malnutrition
4. The mother or caregiver can, in the first six months exclusively give replacement feeding
5. The family is supportive of this practice
6. The mother or caregiver can access health care that offers comprehensive child health services
Early Infant Diagnosis 16

Dose and Duration of Infant Daily NVP Prophylaxis
Birth WeightNVP daily dose
(in mg)NVP daily dose
(in ml)Duration
Infants with birth weight <2000 gm
2 mg/kg once daily
0.2 ml/kg once daily
Upto minimum 6 weeksirrespective ofexclusivelybreast fed or exclusiveReplacement fed and extended to 12 weeks if the duration of ART of mother is less than 24 weeks and she is breast feeding
Birth weight 2000 – 2500 gm
10 mg once daily
1 ml once daily
Birth weight >2500 gm
15 mg once daily
1.5 ml once daily
Early Infant Diagnosis 17
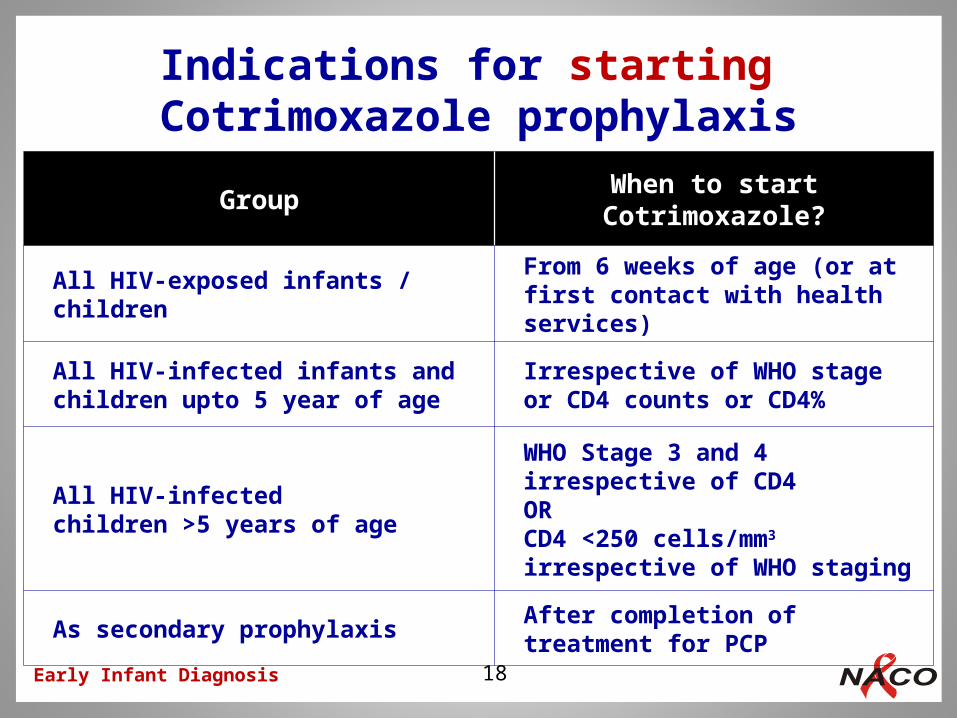
Indications for starting Cotrimoxazole prophylaxis
GroupWhen to start
Cotrimoxazole?
All HIV-exposed infants /children
From 6 weeks of age (or at first contact with health services)
All HIV-infected infants and children upto 5 year of age
Irrespective of WHO stageor CD4 counts or CD4%
All HIV-infectedchildren >5 years of age
WHO Stage 3 and 4 irrespective of CD4ORCD4 <250 cells/mm3
irrespective of WHO staging
As secondary prophylaxisAfter completion oftreatment for PCP
Early Infant Diagnosis 18
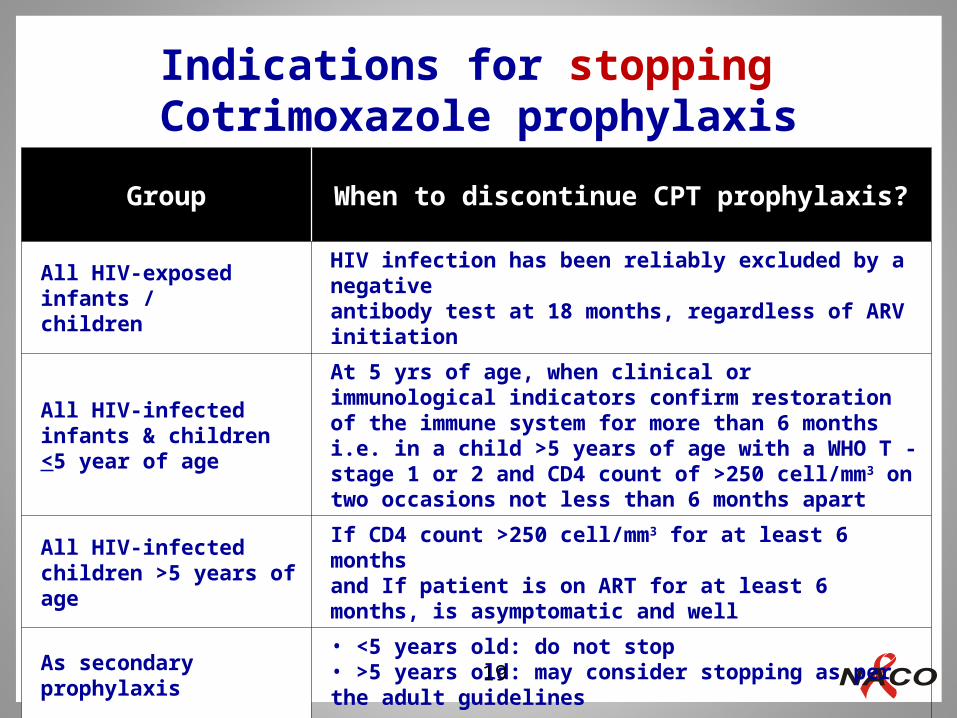
Indications for stopping Cotrimoxazole prophylaxis
Early Infant Diagnosis
Group When to discontinue CPT prophylaxis?
All HIV-exposed infants /children
HIV infection has been reliably excluded by a negativeantibody test at 18 months, regardless of ARV initiation
All HIV-infected infants & children <5 year of age
At 5 yrs of age, when clinical or immunological indicators confirm restoration of the immune system for more than 6 months i.e. in a child >5 years of age with a WHO T - stage 1 or 2 and CD4 count of >250 cell/mm3 on two occasions not less than 6 months apart
All HIV-infectedchildren >5 years of age
If CD4 count >250 cell/mm3 for at least 6 monthsand If patient is on ART for at least 6 months, is asymptomatic and well
As secondary prophylaxis
• <5 years old: do not stop• >5 years old: may consider stopping as per the adult guidelines
19

Cotrimoxazole once a day
Weight (kg)
Syrup 5 ml (40mg TMP/200 SMX)
Child dispersible tablet (20mg TMP/100mg SMX)
<5 2.5 ml (½ teaspoon) 1 tablet
5 – 10 5 ml (1 teaspoon) 2 tablets
10 – 15 7.5 ml (1½ teaspoon) 3 tablets
15 – 22 10 ml (2 teaspoon) 4 tablets
Refer to Paediatric ART Guidelines 2013, NACO
Early Infant Diagnosis
Cotrimoxazole Dosage
20
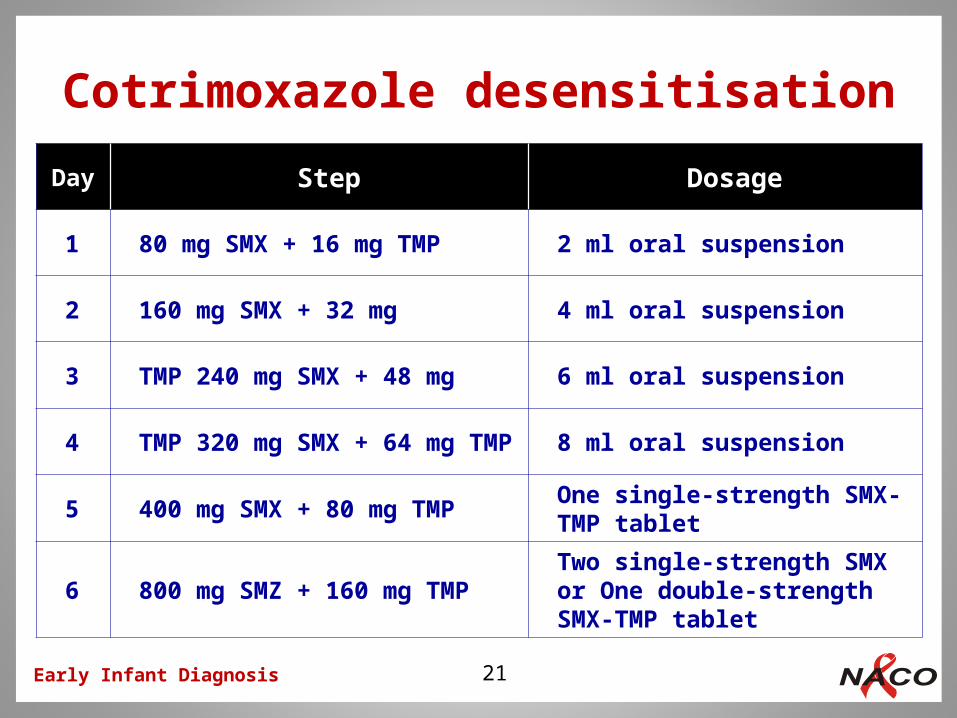
Cotrimoxazole desensitisation
Day Step Dosage
1 80 mg SMX + 16 mg TMP 2 ml oral suspension
2 160 mg SMX + 32 mg 4 ml oral suspension
3 TMP 240 mg SMX + 48 mg 6 ml oral suspension
4 TMP 320 mg SMX + 64 mg TMP 8 ml oral suspension
5 400 mg SMX + 80 mg TMPOne single-strength SMX-TMP tablet
6 800 mg SMZ + 160 mg TMPTwo single-strength SMX or One double-strengthSMX-TMP tablet
Early Infant Diagnosis 21
Assessment and management after confirmed HIV infection in the child
Assess growth, development and nutritional status using standard techniques and scales, and assess the intervention needs. WHO growth charts should be used for assessment of growth
Assess immunisation status and provide appropriate immunisation as per the National Immunisation Schedule
Assess for signs and symptoms of opportunistic infections including tuberculosis (TB). If Opportunistic Infections are suspected, then diagnosis and treatment of OIs take priority over ART initiation. Screening for TB is strongly recommended in all HIV infected children as it is an important aspect of pre-ART care
Assign WHO clinical stage
Early Infant Diagnosis 22

Assessment and management after confirmed HIV infection in the child
A baseline and annual fundoscopic examination for evidence of CMV retinitis is recommended
Ensure that the child is on cotrimoxazole prophylaxis as per guidelines
Identify any concomitant medication use that may have drug interactions with ART
Perform baseline and six monthly follow up CD4 count or CD4%
CD4 counts should be also done, if clinically indicated and advised, by the paediatrician even if done within the last 6 months
Cascade screening - Screen the family for HIV and other OIs
Early Infant Diagnosis 23
Assessment and management after confirmed HIV infection in the child
Psychosocial and family background assessment by the counsellor to identify primary caregiver for the child and his/her ability and willingness to adhere to follow up and administer medications, especially ART
Assess family members’ understanding of HIV disease and treatment and family’s financial status including ability to pay for transportation to clinic
Ability to afford adequate food / nutritional supplements for the child; ability to pay for any treatment needed etc.
Assess disclosure of HIV status within the family (whether the child knows his/her status and whether anyone else knows, and also if the child knows the parent/s’ HIV status)
Early Infant Diagnosis 24
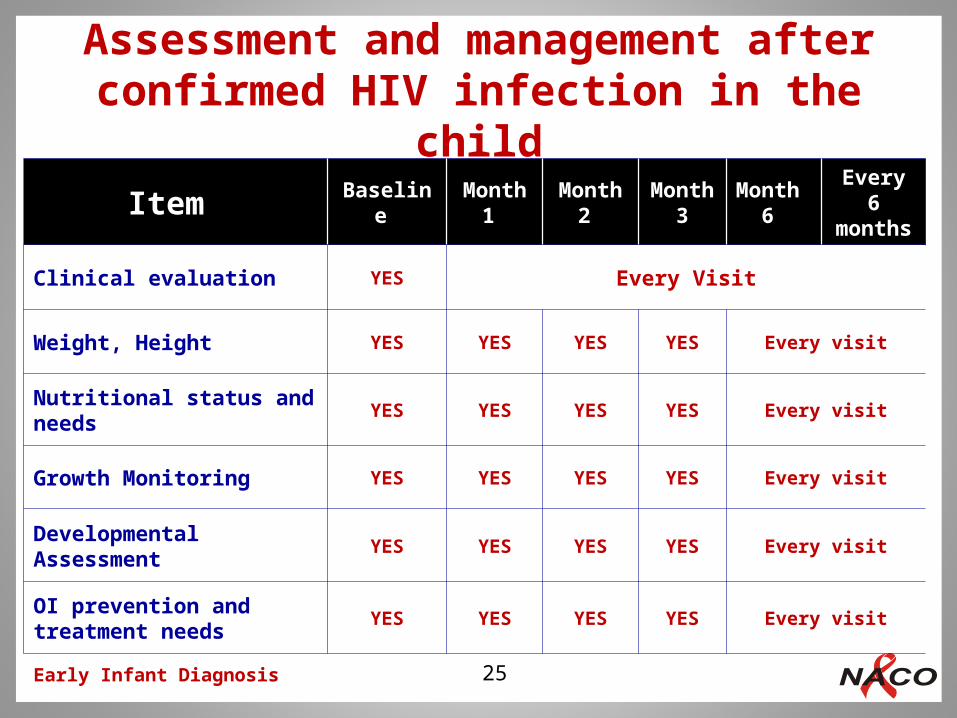
Assessment and management after confirmed HIV infection in the child
Early Infant Diagnosis
Item Baseline
Month 1
Month 2
Month 3
Month 6
Every 6
months
Clinical evaluation YES Every Visit
Weight, Height YES YES YES YES Every visit
Nutritional status and needs
YES YES YES YES Every visit
Growth Monitoring YES YES YES YES Every visit
Developmental Assessment YES YES YES YES Every visit
OI prevention and treatment needs
YES YES YES YES Every visit
25

Assessment and management after confirmed HIV infection in the child
Early Infant Diagnosis
Item Baseline
Month 1
Month 2
Month 3
Month 6
Every 6
months
Immunisation To be Discussed in the next slide
Clinical Screening for TB YES Every visit
Cotrimoxazole needs and adherence
YES Every visit
CD4 % or counts YES YES YES
Pre-ART care and ART initiation
26
Refer to Paediatric ART Guidelines 2013, NACO

Visit Birth6
wks.10
wks.14
wks.9
Months15
Months18
Months4.5 to 5
Yrs*
Immunisation BCG
OPV 0HBV 0
OPV 1DPT 1HBV 1Hib1
OPV 2DPT 2HBV2Hib 2
OPV 3DPT 3HBV 3Hib 3
OPV 4Measle
sMMR
OPVDPT (B)
OPVDPT
Vitamin ASupplementation
Vit A(1 lakh
IU)
Vit A (2 lakh
IU)
Follow the current National and State Immunisation Protocols
Early Infant Diagnosis
Immunisation
27
* Information of immunisation beyond 18 months provided for the completion sake
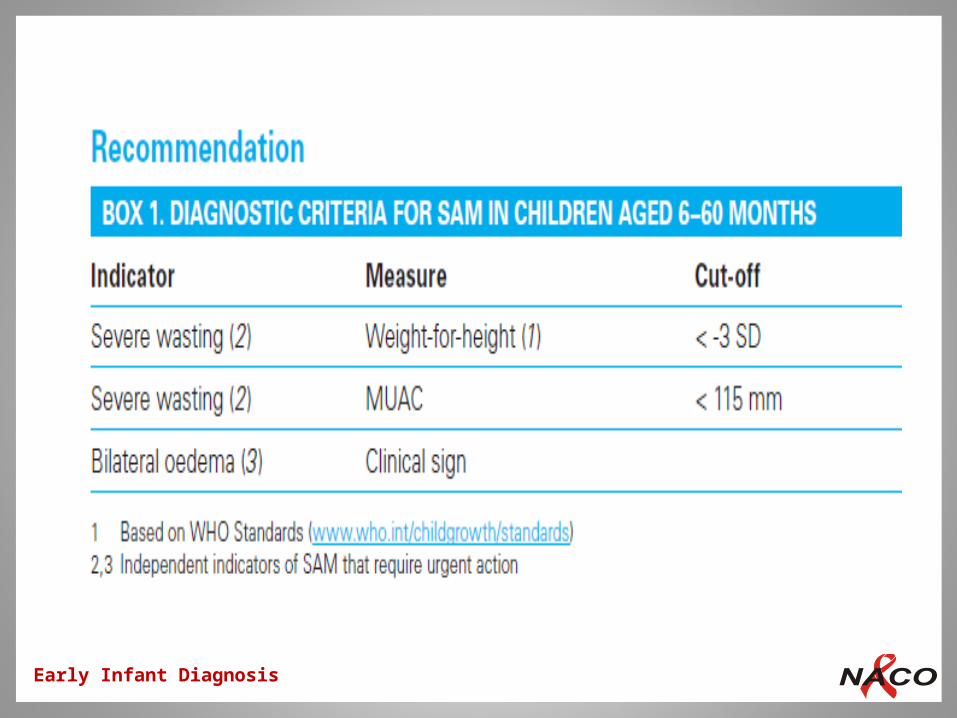
History and physical examination
Use of growth charts
WHO Weight for age charts for girls & boys (0-2yrs)
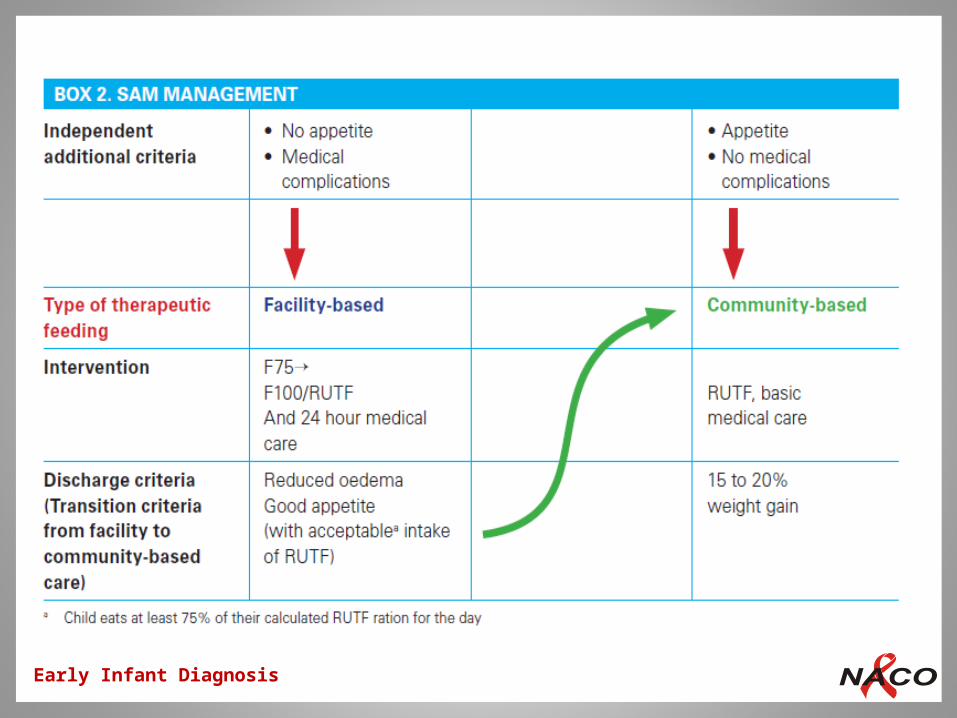
Identifying child at risk of malnutrition
History (Ask); Physical Examination (Look & Feel)
Assess growth according to:
Signs (wasting, bipedal oedema, weight for age) / Mid Upper Arm Circumference (MUAC) / growth curve
Classify as Severe Malnutrition / Poor weight gain / growing appropriately for action
Growth and Nutritional Evaluation
Early Infant Diagnosis 28

Growth and Nutritional EvaluationPatient Treatment (White) card
Early Infant Diagnosis 29

Weight for age growth chart for boys
Early Infant Diagnosis 30
Early Infant Diagnosis
Early Infant Diagnosis
Developmental Assessment
Early Infant Diagnosis
Abnormal development raises concerns of HIV encephalopathy
Developmental assessment at each visit includes assessment of:
Motor / Fine motor
Language
Social skills
If milestones are delayed – refer to Paediatrician
31

Developmental AssessmentPatient Treatment (White) card
Early Infant Diagnosis 32
Laboratory assessment
Haemoglobin
White blood cell count (Total and differential count)
ALT/AST (if available)
BUN / S. Creatinine (if available)
Screening for TB and other major treatable HIV co-infections and HIV-related Opportunistic Infections as clinically indicated
CD4 Count / Percentage
Additional tests (as clinically indicated)
Early Infant Diagnosis 33

Deciding which ART regimen for HIV-infected infants and children <18 months of age
Infants and children <18 months of age with HIV DNA PCR detected or positive HIV antibody test
Comprehensive Assessment at ART centre
ART indicated irrespective of any CD4 count or CD4%
Assess history for previous exposure to single dose NVP or PPTCT regimens containing NVP or EFV
Early Infant Diagnosis
Haemoglobin Regimen
>9G% AZT+3TC+LPV/r
<9 G% ABC+3TC+LPV/r
34
Key Points
Early Infant Diagnosis 35
Diagnosis of HIV exposed Infants & Children <18 months of age depends on testing infant’s blood through Dried Blood Spot (DBS) and confirmed by repeating the test on a Whole Blood Specimen by performing DNA PCR
Breast feeding modifies the diagnostic algorithm; however, exclusive breast feeding for the first 6 months should be advocated in all infants
HIV infection has to be confirmed by antibody tests at the age of 18 months. However, in discordant cases, further evaluation and referral to NACEP is required
All the HIV confirmed infants and children (<5 years) shall be initiated on ART as per NACO guidelines and those less than three years need to be on LPV/r based ART irrespective of prior NVP exposure in mother
Review of Performance of EID programme of Delhi (2011-12)
What proportion of pregnant women testing HIV+ get their HIV-exposed infants tested and at what age?
How long does it take for an EID sample to reach the lab, and for the result to reach the site? the family?
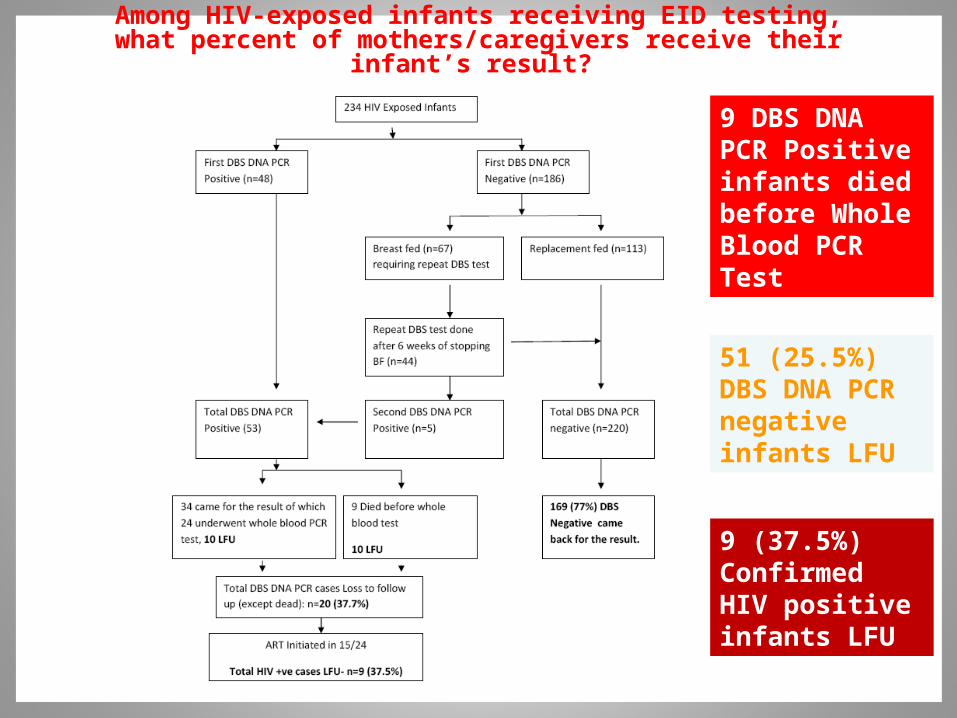
Among HIV-exposed infants receiving EID testing, what percent of mothers/caregivers receive their infant’s result?
Among all confirmed HIV-infected infants, what proportion initiates ART and at what age?
Among those initiated ART, proportion initiated correct regimen as per National Guidelines?
1. Total 234 children were enrolled for EID [≥ 6 weeks < 18 months], 166 of which were born during 2011-12 2. There was missed testing opportunity for 137(45.2%) known HIV exposed infants out of 303 HIV +ve deliveries in 2011-12.3. Age of first DBS DNA PCR test – At 6 weeks-114 (48.7%) > 6 weeks - ≤ 6 months- 75 > 6 months -< 18 mths- 45
.
What proportion of pregnant women testing HIV+ get their HIV-exposed infants tested and at what
age?

How long does it take for an EID sample to reach the lab, and for the result to reach the site?
Among HIV-exposed infants receiving EID testing, what percent of mothers/caregivers receive their infant’s result?
9 (37.5%) Confirmed HIV positive infants LFU
51 (25.5%) DBS DNA PCR negative infants LFU
9 DBS DNA PCR Positive infants died before Whole Blood PCR Test

Among all confirmed HIV-infected infants, what proportion initiates ART and at what age?
15/24 (62.5%) confirmed HIV Infected Infants Initiated on Anti Retroviral Treatment
Nine (37.5%) children could not be initiated ART. -One Died in pre-ART, -6 were LFU -2 parents refused
Delayed start of ART resulted in OIs in 5/15 (33.3%) children
None of infant could beinitiated ART by 3 months of age
In 3 infants tested at 6 weeks of age ART was initiated at 4 mth, 9 mth and 11 mth of age.
Eleven (73.3%) of 15 HIV positive children were initiated first line ARV regimen.
Four NVP exposed children were given 2nd line ARV regimen containing LPV/r with 2 NRTIs at Regional Pediatric ART Centre.
However, 6 /11 (54.5%) children initiated First Line Regimen were NVP exposed but ART Centres had incorrect information about their NVP status. One NVP exposed child initiated first line regimen died within 1 month of treatment due to TB meningitis.
Among those initiated ART, proportion initiated correct regimen as per National Guidelines?
Issues and Challenges Ensuring entry of all HIV exposed infants in the EID cascadeEnsuring testing at 6 weeks of age of all HIV exposed infants to serve the very purpose of EIDTraining of pediatric providers on PICT and referral of symptomatic cases who missed opportunity of EID.Reducing Turn Around Times of DNA PCR testing- change in national guideline of only 2 days /month of sending samples to reference lab. Better coordination between ICTC and ART centers regarding NVP exposure statusImproving follow up of BF first DBS negative exposed infants Early Initiation of ART in confirmed HIV infected infants before signs / symptoms of HIV develop i.e by 12 weeks of age
Strategy to Address the issues

1. All 234 HIV exposed infants initiated CPT2. However, 5 HIV Infected infants developed OIs due to late initiation of ART. Were these infants on regular CPT ? 3. ICTC/PPTCT Counselor should conduct proper counsleing of mother at the time of starting CPT at 6 weeks of age. ART Counselor should also check for adherence to CPT. 4. Monitor for CPT adherence - DBS Negative infants by ICTC Counselor and WB PCR reactive infants initaited ART by ART Counselor 5. Provide stock sufficient till the next imunization visit (10 weeks, 14 weeks). After 14 weeks provide CPT for 2 months and call mother every 2 months to receive supply. Inform mother when CPT will be discontinued.
Ensuring Adherence to CPT

1. 13/74 (17.6% ) BF children were mixed fed despite infant feeding counseling.
2. Infant feeding counseling should be done at 3 crtitical steps:a. Within 24 hours of birth of HIV exposed babyb. At 6 weeks of age at the time of EID c. At about 6 months of age (weaning in BF infants)
Infant feeding Counselling- is it really happening ?

Day 1-3 : Ensure first DBS DNA PCR test at 6 weeks of age & Send sample to NCDC within 2 days (ICTC/PPTCT)
Day 31/32: ART Centre call parents to start ART in confirmed HIV +ve infants within 7 days ie < =12 weeks of age
Day-10 Ensure result of DBS test is collected within 7 days of test (ICTC/PPTCT)Day-17 Ensure infant reaches ARTC for Whole Blood Test (ICTC/PPTCT)
Day -17/18: Ensure whole blood sample is collected and sent to NCDC on same day
Day 23/24: ARTC to ensure that result of Whole blood test is collected on 4th day of submitting sample.

Improving Follow-up Swaziland Expérience (2010)-Makaria Reynolds et al
50 HIV Infected
Not coming
For ART
Contacted
Active Follow up through Phone Calls • Phone calls were effective
• Staff invested significant time in calling patients
• Many clients had incorrect information recorded
• Some infants had died
57
Getting Results to Families
ICTC/ARTC Counselor must ensure following:
• Emphasize parent /caregivers the need of prompt follow up for diagnosis and treatment
• Record correct contact information of parent / caregiver
• Contact families for follow-up by phone call and if reqd. home visit, may also take help of ORWs. DSACS will provide travel allowance.
• Record in Register when result was provided to /parent caregiver.
• Add program indicators on % PCR results given to families and percent of PCR positive initiating treatment
58





























