Embed Size (px)
Citation preview

Early Identification Early Identification of Cognitive of Cognitive
Disorders: Impact on Disorders: Impact on Diagnosis and Diagnosis and
TreatmentTreatment
Ohio State UniversityOhio State University
Douglas W. Scharre, MDDouglas W. Scharre, MD

Douglas W. Scharre, MDDisclosures
Research Support
1. National Institutes of Health - NIA
2. Alzheimer’s Disease Cooperative Study
3. Eisai, Elan, Wyeth, Eli Lily, GalxoSmithKline, Bristol Meyers Squibb, Sonexa, Wyeth
Speakers BureauEisai, Novartis, Forest
ConsultantGalaskoSmithKline
I own no stocks or equity in any pharmaceutical company
Objective: Review early identification techniques for cognitive disorders. Review cognitive assessment instruments for MCI and early dementia. Discuss the impact on diagnosis and treatment.

Prevalence of Dementia Prevalence of Dementia Increases with AgeIncreases with Age
3%
19%
47.20%
0%5%
10%15%20%25%30%35%40%45%50%
65 - 74 75 - 84 85 +
Age Group
Evans, et al. JAMA 1989;262:2551-2556

Projected Prevalence of Projected Prevalence of ADAD
16
14
12
0
2
4
6
8
10
2000 2010 2020 2030 2040 2050
45.8
6.88.7
11.3
14.3
Mil
lio
ns
4.5 Million AD Cases Today—4.5 Million AD Cases Today—Over 14 Million Projected Within a GenerationOver 14 Million Projected Within a Generation
Year
Evans DA et al. Milbank Quarterly. 1990;68:267-289.

DefinitionsDefinitions

NormalNormal
Mild Cognitive ImpairmentMild Cognitive Impairment
DementiaDementia

Dementia DefinitionDementia Definition• Syndrome of acquired persistent intellectual Syndrome of acquired persistent intellectual
impairmentimpairment• Persistent deficits in at least three of the following: Persistent deficits in at least three of the following:
memorymemory languagelanguage visuospatialvisuospatial personality or emotional statepersonality or emotional state cognitioncognition• Resulting in impairment in Activities of Daily Living Resulting in impairment in Activities of Daily Living
(ADL)(ADL)

Mild Cognitive Mild Cognitive Impairment (MCI) Impairment (MCI)
DefinitionDefinition• Memory complaint usually corroborated by an Memory complaint usually corroborated by an
informantinformant• Objective memory impairment for age - that represents Objective memory impairment for age - that represents
a change in function for the persona change in function for the person• Essentially preserved general cognitive functionEssentially preserved general cognitive function• Largely intact functional activitiesLargely intact functional activities• Not dementedNot demented• Alzheimer’s disease may start like this but many non-Alzheimer’s disease may start like this but many non-
AD conditions present like this alsoAD conditions present like this also
Petersen J Int Med 2004;256;183-194Petersen J Int Med 2004;256;183-194

MCI: Rates of MCI: Rates of Dementia ConversionDementia Conversion
• Vary from 1% - 25% per year to AD Vary from 1% - 25% per year to AD depending on the definition used and depending on the definition used and measurement instrumentsmeasurement instruments
• 10% - 12% per year to AD is typical10% - 12% per year to AD is typical
• 57% conversion to dementia after 3 years 57% conversion to dementia after 3 years in one studyin one study
• 25% do not convert to dementia even with 25% do not convert to dementia even with long term follow-uplong term follow-up
Chertkow et al. Neurology Chertkow et al. Neurology 2001;56:B462001;56:B46

Methods of Methods of ScreeningScreening

Screening with Screening with BiomarkersBiomarkers

Biomarkers in ADBiomarkers in AD• Cerebrospinal fluid (CSF) biomarkersCerebrospinal fluid (CSF) biomarkers
– Tau Tau (( in CSF in AD) in CSF in AD)
– AA42 42 (( in CSF in AD) in CSF in AD)
– Neural thread protein (NTP)Neural thread protein (NTP)– Homocysteine Homocysteine (( level, level, risk of AD) risk of AD)
– Isoprostanes Isoprostanes (oxidative/nitrative damage - (oxidative/nitrative damage - levels in blood and levels in blood and CSF in AD)CSF in AD)
– Sulfatide Sulfatide ((in CSF in AD)in CSF in AD)
• Blood and urine biomarkersBlood and urine biomarkers
– Genetic blood tests and genotypingGenetic blood tests and genotyping
– Plasma APlasma A42, Homocysteine, isoprostanes, sulfatide42, Homocysteine, isoprostanes, sulfatide
– Urine neural thread protein (NTP)Urine neural thread protein (NTP)
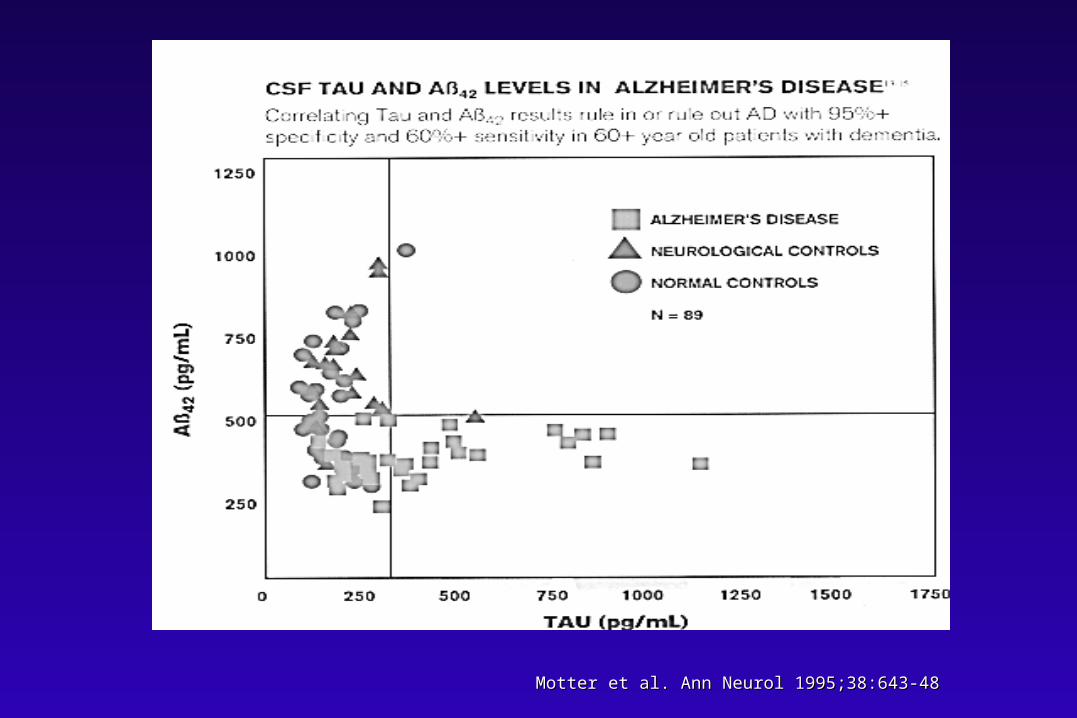
Motter et al. Ann Neurol 1995;38:643-48Motter et al. Ann Neurol 1995;38:643-48

Screening with Screening with NeuroimagingNeuroimaging

Early Diagnosis: Early Diagnosis: Structural Structural
NeuroimagingNeuroimaging• Volumetric measurement of hippocampus and Volumetric measurement of hippocampus and
entorhinal cortex atrophy with MRI is sensitive entorhinal cortex atrophy with MRI is sensitive (95%) but not specific (40%) for AD(95%) but not specific (40%) for AD
• Change in MRI hippocampal volume may be Change in MRI hippocampal volume may be predictive over time in both MCI and predictive over time in both MCI and individuals at genetic risk for ADindividuals at genetic risk for AD
• 7-Tesla and 8-Tesla MRI being used in AD 7-Tesla and 8-Tesla MRI being used in AD researchresearch
Laakso et al. Neurology 1996;46:678-81Laakso et al. Neurology 1996;46:678-81Golomb et al. Neurology 1996;47:810-3Golomb et al. Neurology 1996;47:810-3
Whitaker et al. Society for Neuroscience 2001Whitaker et al. Society for Neuroscience 2001
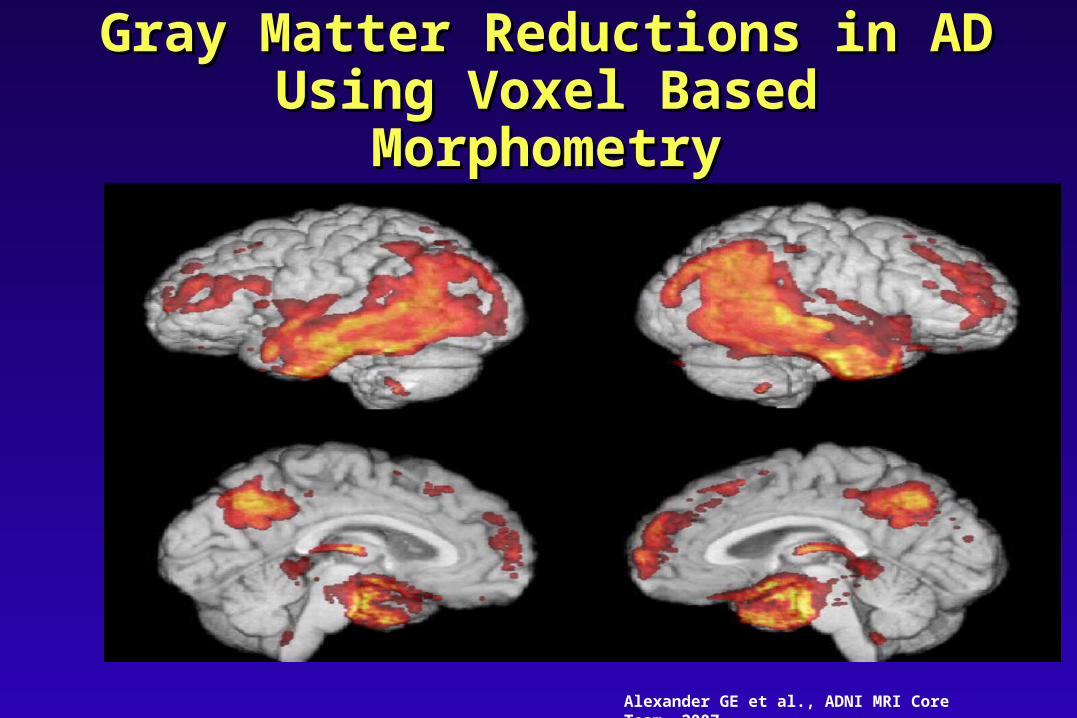
Gray Matter Reductions in AD Gray Matter Reductions in AD Using Voxel Based Using Voxel Based
MorphometryMorphometry
Alexander GE et al., ADNI MRI Core Team, 2007

Functional Neuroimaging: Functional Neuroimaging: PETPET
• PET shows hypometabolism in PET shows hypometabolism in bilateral parietal, temporal, and bilateral parietal, temporal, and posterior cingulate cortex in AD posterior cingulate cortex in AD subjects and those who are subjects and those who are asymptomatic but at increased risk for asymptomatic but at increased risk for AD (those with Apo E AD (those with Apo E 4) 4)
• PET predicted 94% of mild cognitive PET predicted 94% of mild cognitive impairment (MCI) subjects whose impairment (MCI) subjects whose disease progressed to dementia disease progressed to dementia during a 3 year periodduring a 3 year period
Minoshima et al. J Nucl Med 1995;36:1238-48Minoshima et al. J Nucl Med 1995;36:1238-48Minoshima et al. Ann Neurol 1997;42:85-94Minoshima et al. Ann Neurol 1997;42:85-94
Small et al. JAMA 1995;273:942-47Small et al. JAMA 1995;273:942-47

Typical AD PET ScanTypical AD PET Scan
Provided courtesy of M. Mega, MD, PhD, Department ofNeurology, UCLA School of Medicine.
Normal Brain AD Brain

Preliminary FDG PET Comparisons: Regional Hypometabolism in Probable
AD (purple) & MCI (blue)
Chen, K, et al., ADNI PET Coordinating Center, 2007
PET with Pittsburgh PET with Pittsburgh Compound B (PIB)Compound B (PIB)
• PIB is a hydroxylated PIB is a hydroxylated benzothiozole PET tracerbenzothiozole PET tracer
• Attaches to the amyloid Attaches to the amyloid beta peptidebeta peptide
• MCI patients have more MCI patients have more amyloid than normals and amyloid than normals and less that AD patientsless that AD patients
Klunk et al. Ann Neurol 2004;55(1)Klunk et al. Ann Neurol 2004;55(1)
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Cognitive Cognitive ScreeningScreening

Treatment of Alzheimer’s DiseaseTreatment of Alzheimer’s Disease
Source: Decision Resources, March 2000.
0
1
2
3
4
5
Prevalence Diagnosed Treated*
Pat
ien
ts (
mil
lio
ns)
* Any drug treatment, not limited to acetylcholinesterase inhibitors.

Barriers to Early Barriers to Early Diagnosis of MCI and Diagnosis of MCI and
DementiaDementia• Patients with MCI and early dementia have Patients with MCI and early dementia have
impaired insightimpaired insight• First present to the doctor an average of 3.5 First present to the doctor an average of 3.5
years after cognitive symptoms startyears after cognitive symptoms start• Physicians may not notice subtle cognitive Physicians may not notice subtle cognitive
deficits in routine office visitsdeficits in routine office visits• Little reimbursement for cognitive screensLittle reimbursement for cognitive screens• Often too much time or personnel resources Often too much time or personnel resources
required to administer testingrequired to administer testingBarker WWBarker WW et al. Alzheimer Dis Assoc Disord 2005;19:1-7

Examples of Brief Examples of Brief Cognitive Cognitive
Assessment/Screening Assessment/Screening TestsTests• MMSEMMSE
• Clock Drawing TestClock Drawing Test• Mini-CogMini-Cog• AD8AD8• 7-minute Screen7-minute Screen• Montreal Cognitive Assessment (MoCA)Montreal Cognitive Assessment (MoCA)• Self-Administered Gerocognitive Self-Administered Gerocognitive
Examination (SAGE)Examination (SAGE)

MMSEMMSE• Score: 0 (worst) - 30 (best)Score: 0 (worst) - 30 (best)• Tests orientation, attention, mental control, calculations, Tests orientation, attention, mental control, calculations,
delayed memory (no clueing), language, and constructional delayed memory (no clueing), language, and constructional praxispraxis
• Easy to use, well knownEasy to use, well known• Not great for frontal or executive functionsNot great for frontal or executive functions• Sensitivity 78% and specificity 84% for dementia with a cutoff Sensitivity 78% and specificity 84% for dementia with a cutoff
of 26/30of 26/30• Takes 7 to 10 minutes; needs examinerTakes 7 to 10 minutes; needs examiner• PAR bought rights - costs about $1 per usePAR bought rights - costs about $1 per use
Folstein et al. J Psychiat Res 1975;12:189-98Folstein et al. J Psychiat Res 1975;12:189-98Feher et al. Arch Neurol 1992;49:87-92Feher et al. Arch Neurol 1992;49:87-92

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Folstein et al. Folstein et al. J Psychiat Res J Psychiat Res 1975;12: 1975;12: 189-98189-98
MMSEMMSE

Mini-Mental State Mini-Mental State Examination:Examination:
Typical change over timeTypical change over time
0
5
10
15
20
25
30
0 1 2 3 4 5 6 7 8 9 10 11 12
Years since diagnosis
MMSE Score
Average change is 3 points/year without treatment between MMSE of 23 to 5
Mild Cognitive Impairment (MCI)

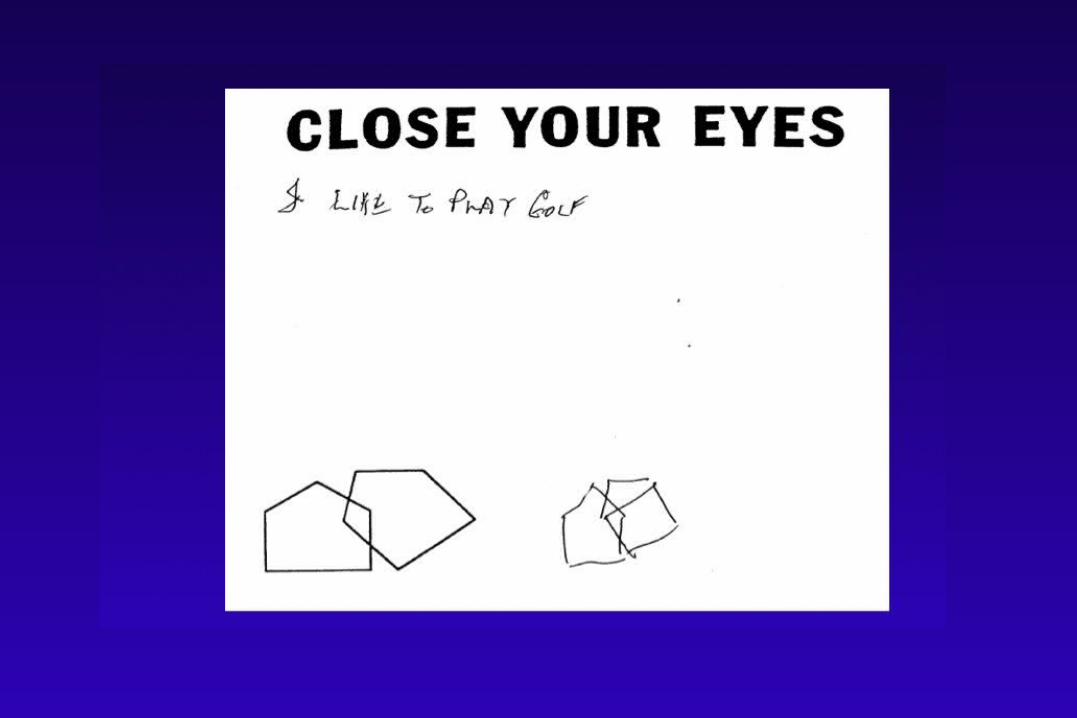
Clock Drawing TestClock Drawing Test
• Various scoring methodsVarious scoring methods• Tests constructional praxis, visuospatial skills, Tests constructional praxis, visuospatial skills,
and executive functioningand executive functioning• Easy to use, well knownEasy to use, well known• Limited in evaluating other cognitive domainsLimited in evaluating other cognitive domains• Sensitivity 83% and specificity 72% for ADSensitivity 83% and specificity 72% for AD• Takes 1 minute; needs no examinerTakes 1 minute; needs no examiner
Shulman et al. Int Geriatr Psychiatry 1986;1:135-40Shulman et al. Int Geriatr Psychiatry 1986;1:135-40Cahn et al. Arch Clin Neuropsych 1996;11:529-39Cahn et al. Arch Clin Neuropsych 1996;11:529-39

Early Diagnis: Early Diagnis: Cognitive ScreeningCognitive Screening

Mini-CogMini-Cog
• 3-item recall and clock drawing3-item recall and clock drawing• Easy to useEasy to use• Limited in evaluating other cognitive domainsLimited in evaluating other cognitive domains• Sensitivity 76% and specificity of 89% for Sensitivity 76% and specificity of 89% for
dementiadementia• Score not influenced by language or Score not influenced by language or
educationeducation• Takes 3 minutes; needs examinerTakes 3 minutes; needs examiner
Borson S et al. Int J Geriatr Psychiatry 2000;15:1021-1027Borson S et al. Int J Geriatr Psychiatry 2000;15:1021-1027Borson S et al. JAGS 2003;51:1451-1454Borson S et al. JAGS 2003;51:1451-1454

Mini-CogMini-Cog

AD8AD8• Score: 0 (best) - 8 (worst)Score: 0 (best) - 8 (worst)• Informant rates changes in the patient’s judgment, Informant rates changes in the patient’s judgment,
interests, memory, functioning, and orientationinterests, memory, functioning, and orientation• Easy to useEasy to use• Does not measure patient cognitionDoes not measure patient cognition• Sensitivity 84% and specificity 80% for dementia Sensitivity 84% and specificity 80% for dementia
with a cutoff of 2 or greaterwith a cutoff of 2 or greater• Takes 3 minutes; needs examiner and informantTakes 3 minutes; needs examiner and informant
Folstein et al. J Psychiat Res 1975;12:189-98Folstein et al. J Psychiat Res 1975;12:189-98Feher et al. Arch Neurol 1992;49:87-92Feher et al. Arch Neurol 1992;49:87-92

AD8AD8
Galvin et al. Galvin et al. Neurology Neurology 2006;67:1942-19482006;67:1942-1948

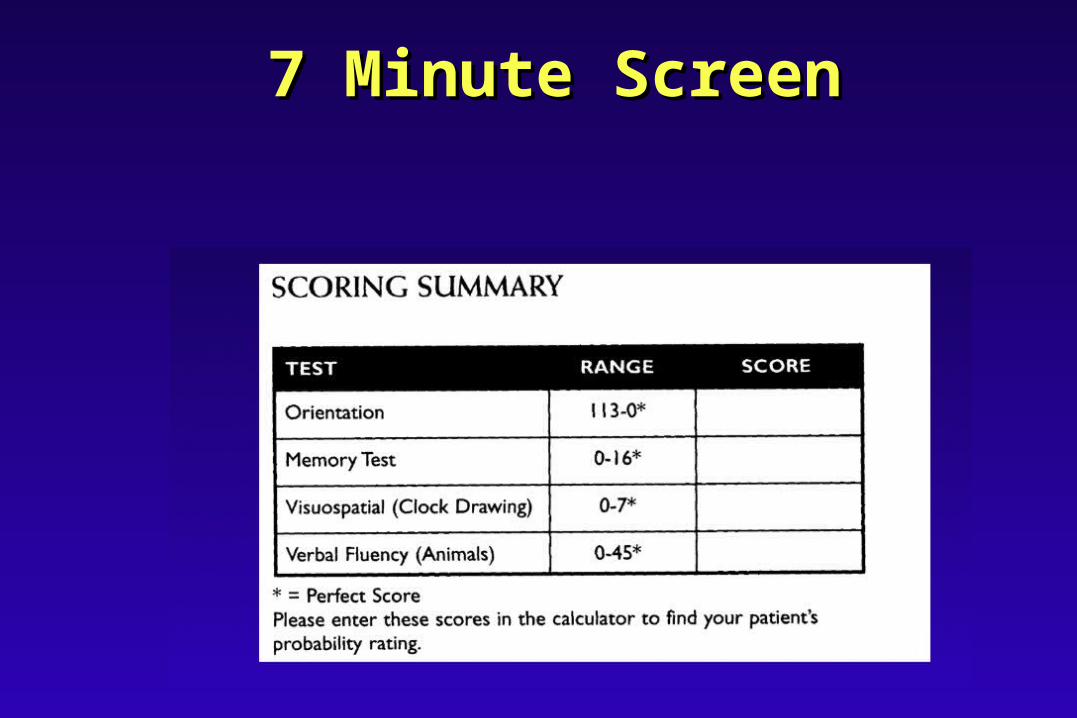
7 Minute Screen7 Minute Screen• Special scoring calculator requiredSpecial scoring calculator required• Tests orientation, memory, clock drawing, Tests orientation, memory, clock drawing,
verbal fluencyverbal fluency• Not easy to use in primary care officeNot easy to use in primary care office• Low scores very specific for ADLow scores very specific for AD• Sensitivity 92% and specificity 96% for AD Sensitivity 92% and specificity 96% for AD
vs normal controlsvs normal controls• Takes 7 - 12 minutes; needs examinerTakes 7 - 12 minutes; needs examiner
Solomon et al. Arch Neurol 1998;55:349-55Solomon et al. Arch Neurol 1998;55:349-55
7 Minute Screen7 Minute Screen

Montreal Cognitive Montreal Cognitive Assessment (MOCA)Assessment (MOCA)
• Score: 0 (worst) - 30 (best)Score: 0 (worst) - 30 (best)• Tests orientation, memory, clock drawing, Tests orientation, memory, clock drawing,
constructions, verbal fluency, naming, constructions, verbal fluency, naming, repetition, attention, abstraction, calculations, repetition, attention, abstraction, calculations, executive (trails B)executive (trails B)
• Not easy to give in primary care officeNot easy to give in primary care office• Sensitivity 100% and specificity 87% for AD vs Sensitivity 100% and specificity 87% for AD vs
normal controls with a cutoff of 26/30normal controls with a cutoff of 26/30• Takes 10-13 minutes; needs examinerTakes 10-13 minutes; needs examiner
Nasreddine et al. J Am Geriatr Soc 2005;53:695-699Nasreddine et al. J Am Geriatr Soc 2005;53:695-699

MOCAMOCA
Nasreddine et al. J Nasreddine et al. J Am Geriatr Soc Am Geriatr Soc 2005;53:695-6992005;53:695-699

Self-Administered Self-Administered Gerocognitive Exam Gerocognitive Exam
(SAGE)(SAGE)• Score: 0 (worst) - 22 (best) Score: 0 (worst) - 22 (best) • Tests orientation, memory, language, fluency, Tests orientation, memory, language, fluency,
naming, visuospatial, abstraction, calculations, naming, visuospatial, abstraction, calculations, executive functioning, and problem solvingexecutive functioning, and problem solving
• Self-administered, easy to useSelf-administered, easy to use• Limited memory evaluation; excellent executive Limited memory evaluation; excellent executive
measuresmeasures• Takes 10 to 15 minutes; needs no examinerTakes 10 to 15 minutes; needs no examiner
Scharre et al. Alzheimer Dis Assoc Disord 2009 at sagetest.osu.eduat sagetest.osu.edu

SAGESAGEPage 1Page 1
Scharre et al. Alzheimer Dis Assoc Disord 2009 at at sagetest.osu.edusagetest.osu.edu

SAGESAGEPage 2Page 2
Scharre et al. Alzheimer Dis Assoc Disord 2009 at sagetest.osu.eduat sagetest.osu.edu

Scharre et al. Alzheimer Dis Assoc Disord 2009 at at sagetest.osu.edusagetest.osu.edu
SAGESAGEPage 3Page 3

Scharre et al. Alzheimer Dis Assoc Disord 2009 at sagetest.osu.eduat sagetest.osu.edu
SAGESAGEPage 4Page 4

SAGE: Validity Against SAGE: Validity Against Neuropsychologic TestsNeuropsychologic Tests
Scharre et al. Alzheimer Dis Assoc Disord 2009

SAGE Validity StudySAGE Validity Study
• Correlation between SAGE & neuropsychology Correlation between SAGE & neuropsychology battery was 0.84 (0.76 for MMSE) battery was 0.84 (0.76 for MMSE)
• Cognitive impaired group = MCI + dementiaCognitive impaired group = MCI + dementia
• ROC analysis for SAGE, normal vs cognitive ROC analysis for SAGE, normal vs cognitive impaired: impaired: sensitivitysensitivity is is 95%95% (90% for MMSE) and (90% for MMSE) and specificityspecificity is is 79%79% (71% for MMSE) with a cut off (71% for MMSE) with a cut off score of 17/22score of 17/22
Scharre et al. Alzheimer Dis Assoc Disord 2009 at sagetest.osu.eduat sagetest.osu.edu

ROC for SAGE: ROC for SAGE: Differentiating normal vs Differentiating normal vs
MCI + DementiaMCI + Dementia
Scharre et al. Alzheimer Dis Assoc Disord 2009 at sagetest.osu.eduat sagetest.osu.edu

Self-Administered Self-Administered Gerocognitive Exam Gerocognitive Exam
(SAGE)(SAGE)• Validity against neuropsychological tests: r = 0.85 Validity against neuropsychological tests: r = 0.85 • Inter-rater reliability: correlation coefficient = 0.96Inter-rater reliability: correlation coefficient = 0.96• Test-retest reliability: correlation coefficient = 0.86Test-retest reliability: correlation coefficient = 0.86• Age, gender, and version of SAGE (4 different Age, gender, and version of SAGE (4 different
forms available) had no effect on SAGE scoreforms available) had no effect on SAGE score• Education had a moderate effect on SAGE score Education had a moderate effect on SAGE score
(p = 0.025) only in those less than 12 years of (p = 0.025) only in those less than 12 years of schoolingschooling
Scharre et al. Alzheimer Dis Assoc Disord 2009 at sagetest.osu.eduat sagetest.osu.edu
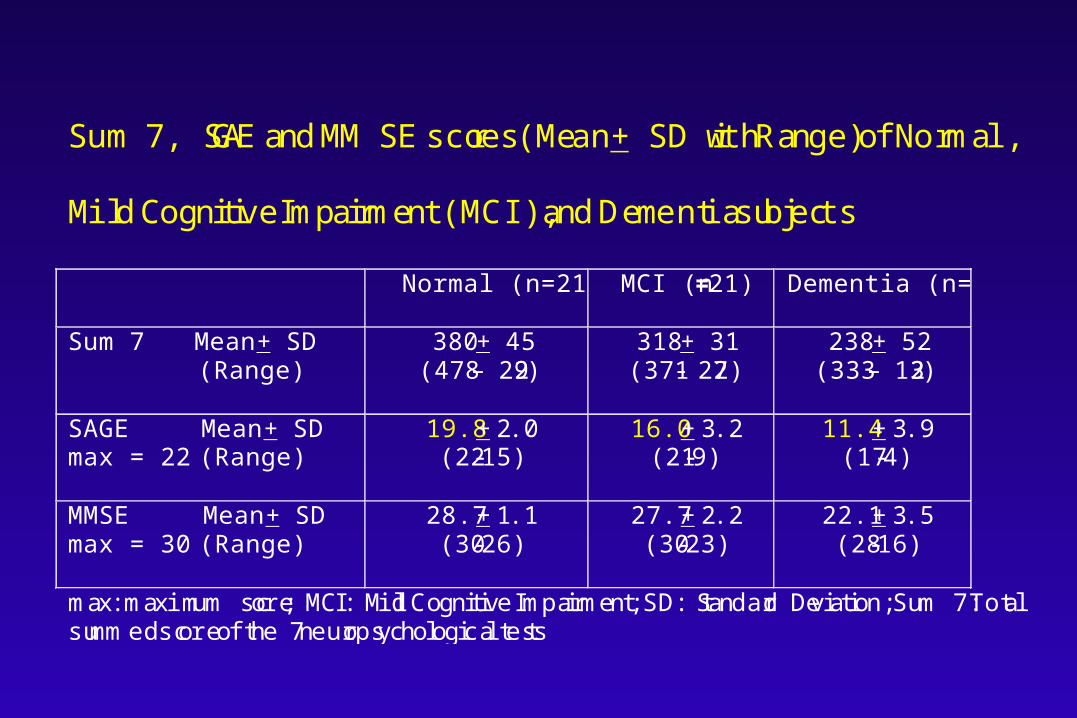
Sum 7, SAGE and MMSE scores (Mean + SD with Range) of Normal,
Mild Cognitive Impairment (MCI), and Dementia subjects
Normal (n=21)
MCI (n=21) Dementia (n=21)
Sum 7 Mean + SD (Range)
380 + 45 (478 – 292)
318 + 31 (371- 272)
238 + 52 (333 – 132)
SAGE Mean + SD max = 22 (Range)
19.8 + 2.0 (22-15)
16.0 + 3.2 (21-9)
11.4 + 3.9 (17-4)
MMSE Mean + SD max = 30 (Range)
28.7 + 1.1 (30-26)
27.7 + 2.2 (30-23)
22.1 + 3.5 (28-16)
max: maximum score; MCI: Mild Cognitive Impairment; SD: Standard Deviation; Sum 7: Total summed score of the 7 neuropsychological tests

SAGE ScoresSAGE Scores
17-22:17-22: Very likely to be normal - no Very likely to be normal - no further evaluationfurther evaluation
15-16: 15-16: Likely to have MCI - staged Likely to have MCI - staged screening evaluation screening evaluation recommendedrecommended
0-14:0-14: Likely to have a dementia Likely to have a dementia condition - staged screening condition - staged screening evaluation recommendedevaluation recommended

Staged Staged Screening: Screening: Impact of Impact of DiagnosisDiagnosis

Screening for Screening for Cognitive ImpairmentCognitive Impairment
• No cognitive screening test is diagnosticNo cognitive screening test is diagnostic• If normal, serious conditions are less likelyIf normal, serious conditions are less likely• The “worried well” can be relieved that they The “worried well” can be relieved that they
were “tested” and they did finewere “tested” and they did fine• Serial screening could be suggested over Serial screening could be suggested over
timetime• If abnormal, further evaluation may be If abnormal, further evaluation may be
consideredconsidered

Staged Screening Staged Screening Approach for Approach for
Cognitive ImpairmentCognitive Impairment• One single test or score should not be One single test or score should not be
the only criteria to embark on an the only criteria to embark on an expensive dementia evaluationexpensive dementia evaluation
• Doing a screening process in stages may Doing a screening process in stages may provide better evidence for diagnosis of provide better evidence for diagnosis of MCI or dementiaMCI or dementia
• A staged screening process is A staged screening process is recommendedrecommended

Staged Screening ApproachStaged Screening Approach
SAGE Test
Age over 65? Screen if concerns
Schedule appointment with patient and informant
Consider dementia evaluation Re-screen in one year or consider neuropsychological testing
<17
17-22
No
Yes
Re-screen yearly
AD8 > 1 MOCA < 26
AD8 < 2 MOCA > 25
Re-screen in 2 years
Age over 80?
No Yes

Impact on Impact on TreatmentTreatment

Importance of Early Importance of Early Diagnosis of MCI and Diagnosis of MCI and
DementiaDementia• Amyloid plaques probably start 20 years Amyloid plaques probably start 20 years
before clinical symptoms of ADbefore clinical symptoms of AD• 16 million projected to have AD by 205016 million projected to have AD by 2050• Current AD meds work better if started Current AD meds work better if started
earlierearlier• Disease modifying agents are comingDisease modifying agents are coming• Preventing or delaying AD could save Preventing or delaying AD could save
billions of dollars and lead to improved billions of dollars and lead to improved quality of life for patients and familiesquality of life for patients and families

Raskind et al. Neurology. 2000.
Galantamine: Mean Change From Galantamine: Mean Change From Baseline in ADAS-cogBaseline in ADAS-cog
Open-Open-ExtensionExtension
Double-blindDouble-blind
galantamine 24 mg/galantamine 24 mg(n = 212/116)
Historical placebo group
*P < .05 vs placebo/galantamineand not statistically different from baseline.
ImprovementImprovement
DeterioratioDeteriorationn
0 3 6 9 12
Mean (± SE)Mean (± SE)Change From Change From Baseline inBaseline inADAS-cogADAS-cogScoreScore
–4
–3
–2
–1
0
1
2
3
45
6
7
MonthsMonths
Placebo/galantamine 24 mg (n = 213/135)
*

Cognitive Rx in ADCognitive Rx in AD
Efficacy of Cholinesterase InhibitorsEfficacy of Cholinesterase Inhibitors
• Donepezil, Rivastigmine, GalantamineDonepezil, Rivastigmine, Galantamine• All of them workAll of them work• Up to 80% of patients show no decline after 6 months Up to 80% of patients show no decline after 6 months
of Rx and 50% no decline after 1 year of Rx and 50% no decline after 1 year • Need to give for at least 6 to 12 months to determine Need to give for at least 6 to 12 months to determine
utilityutility• Side effects: weight loss, diarrhea, nauseaSide effects: weight loss, diarrhea, nausea• Always titrate to highest doseAlways titrate to highest dose

Cognitive Rx in ADCognitive Rx in AD
NMDA Antagonists: Memantine NMDA Antagonists: Memantine
• N-methyl-D-aspartate (NMDA) N-methyl-D-aspartate (NMDA) antagonists potentially prevent neuronal antagonists potentially prevent neuronal injury by reducing excitatory amino acid injury by reducing excitatory amino acid toxicity by glutamatetoxicity by glutamate
• Side effects include headache, Side effects include headache, dizziness, fatigue, confusiondizziness, fatigue, confusion
• Titrate to 10 mg bidTitrate to 10 mg bid
Phase III Studies: Phase III Studies: Rx StrategiesRx Strategies
• SB-742457: 5-HT6 receptor antagonist - SB-742457: 5-HT6 receptor antagonist - increases release of Ach and glutamateincreases release of Ach and glutamate
• LY450139, BMS708163: gamma secretase LY450139, BMS708163: gamma secretase inhibitorsinhibitors
• Bapineuzumab : Passive immunotherapyBapineuzumab : Passive immunotherapy

Proteolytic Cleavages of Proteolytic Cleavages of Amyloid Precursor Protein Amyloid Precursor Protein
(APP) That Produce A(APP) That Produce A PeptidePeptide
Selkoe DJ et al. JAMA. 2000;283:1615-1617.
-amyloid precursor protein
-secretase
A peptide
-secretase
Extracellular space
TM Cytoplasm
COOHNH2

Immunization: Immunization: Bapineuzumab (Phase III)Bapineuzumab (Phase III)
• Passive immunotherapyPassive immunotherapy• Monoclonal antibody against beta-amyloid Monoclonal antibody against beta-amyloid
peptide administered intravenously (IV)peptide administered intravenously (IV)• Binds and removes beta-amyloid peptide that Binds and removes beta-amyloid peptide that
accumulates in plaquesaccumulates in plaques

Future Rx Future Rx StrategiesStrategies
• Anti-amyloid strategiesAnti-amyloid strategies
• Combined drug treatmentsCombined drug treatments
• Tau interventions (methylene blue: Tau interventions (methylene blue:
Phase II trials - disrupts tau aggregation)Phase II trials - disrupts tau aggregation)
• Gene therapyGene therapy
• Brain transplantsBrain transplants

Importance of Early Importance of Early Diagnosis of MCI and Diagnosis of MCI and
DementiaDementia• Leads to earlier treatmentLeads to earlier treatment• Reduces patient poor judgment with finances, Reduces patient poor judgment with finances,
driving, medication use, symptom reportingdriving, medication use, symptom reporting• Lead to increased supervision of individuals Lead to increased supervision of individuals
to adequately perform their activities of daily to adequately perform their activities of daily livingliving
• Improves treatment compliance rates of other Improves treatment compliance rates of other chronic medical conditionschronic medical conditions
• Reduces medication errorsReduces medication errors
Importance of Early Importance of Early Diagnosis of MCI and Diagnosis of MCI and
DementiaDementia• Decreases hospital admissions or Decreases hospital admissions or
emergency room visitsemergency room visits• Improves quality of life of patient and Improves quality of life of patient and
caregivercaregiver• Reduces burden and chronic stress effects Reduces burden and chronic stress effects
on caregiverson caregivers• Preventing or delaying AD could save Preventing or delaying AD could save
billions of dollarsbillions of dollars

SummarySummary• Cognitive disorders are increasingCognitive disorders are increasing• MCI and early AD are under recognizedMCI and early AD are under recognized• Biomarkers (serum and CSF) and neuroimaging Biomarkers (serum and CSF) and neuroimaging
are too expensive for screeningare too expensive for screening• Cognitive screening with a staged approach Cognitive screening with a staged approach
should be doneshould be done• More study is needed to identify which MCI More study is needed to identify which MCI
subjects will progress to dementia or ADsubjects will progress to dementia or AD• Treatment and increased supervision should be Treatment and increased supervision should be
started as soon as possible after MCI or dementia started as soon as possible after MCI or dementia identificationidentification

Questions and Questions and AnswersAnswers