Embed Size (px)
Citation preview
The University of Sydney Page 1
Early identification
and intervention in
patients with MSK
injuries in workplace
Presented by
Professor Michael Nicholas, PhD Director, Pain Education and Pain Management Programs
Pain Management Research Institute
Kolling Institute of Medical Research
University of Sydney and Royal North Shore Hospital

The University of Sydney Page 2
2
Main Collaborators/Research Team
Dr Garry Pearce, Dr Mick Gleeson, Dr Rafael Pinto,
Dr Dan Costa
Karen Munk, Tamara Sprod, Rachel Elmes, and
Claims managers & staff at EML
Robert Lloyd, Susan Rafty
Michele Murphy and RTW coordinators at each
hospital
International and Australian partners: Steven Linton (Sweden); William Shaw (USA); Chris
Main (UK); Rob Smeets (Netherlands); Chris Maher (USyd); James McAuley (UNSW); Fiona Blyth
(USyd); Andrew McGarity (NSW Fire & Rescue)
The University of Sydney Page 3
General agreement that work is good for your health
3
Australasian Faculty of Occupational &
Environmental Medicine (AFOEM) Royal Australasian College of Physicians
Consensus Statement (2011)
• Work is generally good for health and wellbeing …
• Long term work absence, work disability and unemployment
generally have a negative impact on health and wellbeing
The University of Sydney Page 4
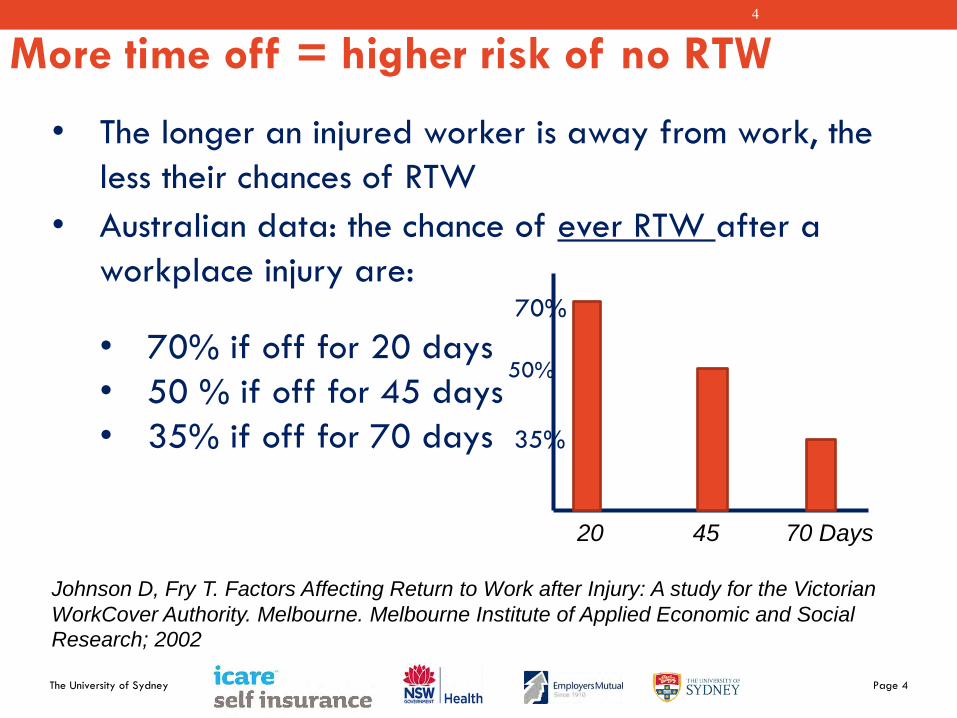
More time off = higher risk of no RTW 4
• The longer an injured worker is away from work, the
less their chances of RTW
• Australian data: the chance of ever RTW after a
workplace injury are: 70%
• 70% if off for 20 days
• 50 % if off for 45 days
• 35% if off for 70 days 35%
20 45 70 Days
Johnson D, Fry T. Factors Affecting Return to Work after Injury: A study for the Victorian
WorkCover Authority. Melbourne. Melbourne Institute of Applied Economic and Social
Research; 2002
50%
The University of Sydney Page 5
5
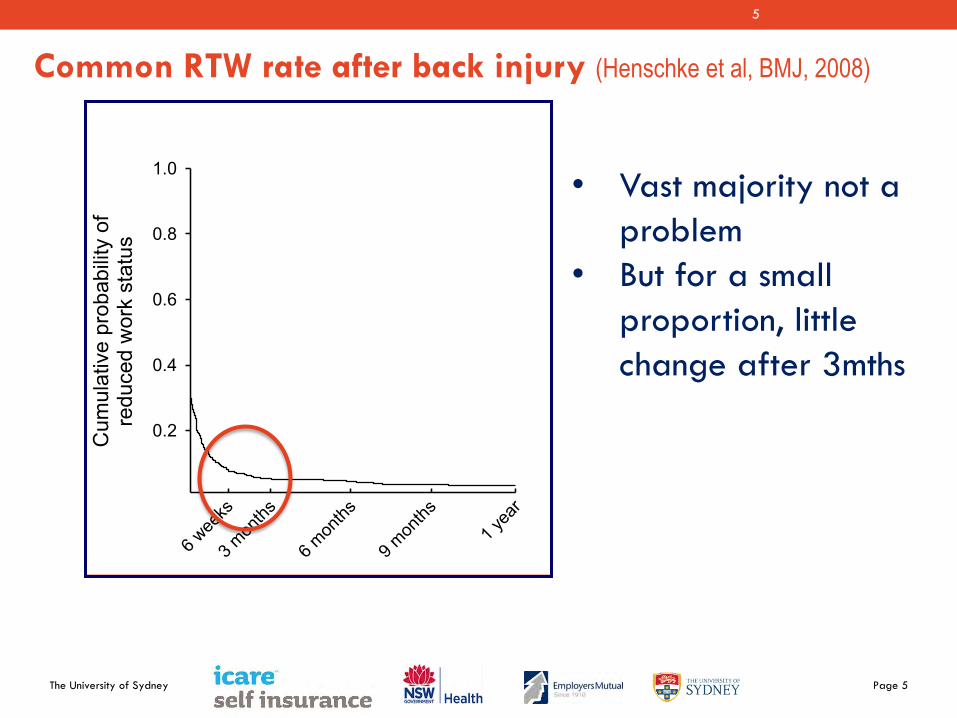
Common RTW rate after back injury (Henschke et al, BMJ, 2008)
6 wee
ks
3 mon
ths
6 mon
ths
9 mon
ths1 y
ear
Cum
ulat
ive
prob
abili
ty o
fre
duce
d w
ork
stat
us
0.2
0.4
0.6
0.8
1.0 • Vast majority not a
problem
• But for a small
proportion, little
change after 3mths
The University of Sydney Page 6
6
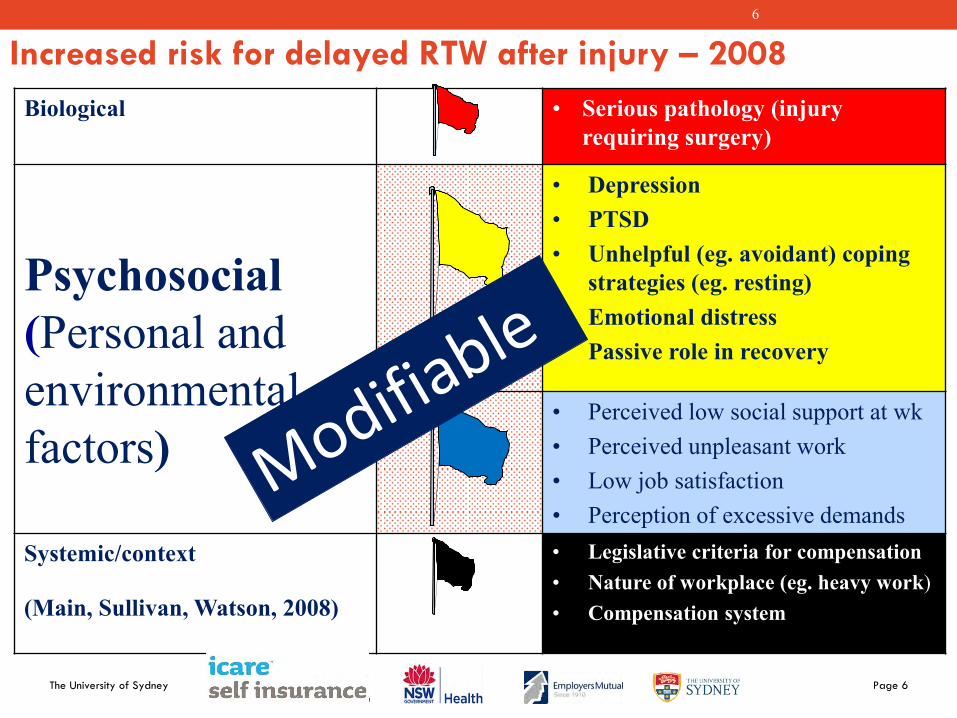
Increased risk for delayed RTW after injury – 2008
Biological • Serious pathology (injury requiring surgery)
Psychosocial (Personal and environmental factors)
• Depression • PTSD • Unhelpful (eg. avoidant) coping
strategies (eg. resting) • Emotional distress • Passive role in recovery
• Perceived low social support at wk • Perceived unpleasant work • Low job satisfaction • Perception of excessive demands
Systemic/context
(Main, Sullivan, Watson, 2008)
• Legislative criteria for compensation • Nature of workplace (eg. heavy work) • Compensation system
The University of Sydney Page 7
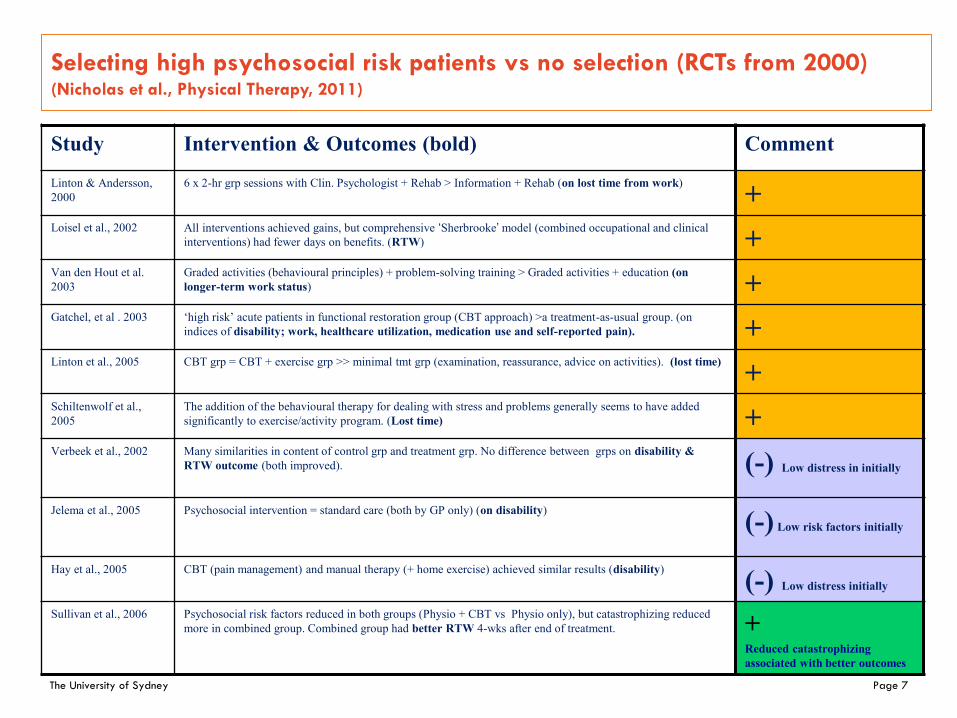
Selecting high psychosocial risk patients vs no selection (RCTs from 2000) (Nicholas et al., Physical Therapy, 2011)
Study Intervention & Outcomes (bold) Comment
Linton & Andersson, 2000
6 x 2-hr grp sessions with Clin. Psychologist + Rehab > Information + Rehab (on lost time from work) +
Loisel et al., 2002
All interventions achieved gains, but comprehensive ‘Sherbrooke’ model (combined occupational and clinical interventions) had fewer days on benefits. (RTW) +
Van den Hout et al. 2003
Graded activities (behavioural principles) + problem-solving training > Graded activities + education (on longer-term work status) +
Gatchel, et al . 2003
‘high risk’ acute patients in functional restoration group (CBT approach) >a treatment-as-usual group. (on indices of disability; work, healthcare utilization, medication use and self-reported pain). +
Linton et al., 2005 CBT grp = CBT + exercise grp >> minimal tmt grp (examination, reassurance, advice on activities). (lost time) + Schiltenwolf et al., 2005
The addition of the behavioural therapy for dealing with stress and problems generally seems to have added significantly to exercise/activity program. (Lost time) +
Verbeek et al., 2002 Many similarities in content of control grp and treatment grp. No difference between grps on disability & RTW outcome (both improved). (-) Low distress in initially
Jelema et al., 2005 Psychosocial intervention = standard care (both by GP only) (on disability) (-) Low risk factors initially
Hay et al., 2005 CBT (pain management) and manual therapy (+ home exercise) achieved similar results (disability) (-) Low distress initially
Sullivan et al., 2006
Psychosocial risk factors reduced in both groups (Physio + CBT vs Physio only), but catastrophizing reduced more in combined group. Combined group had better RTW 4-wks after end of treatment.
+ Reduced catastrophizing associated with better outcomes
The University of Sydney Page 8
Implications of early intervention trials
• Low psychosocial risk factors, usual care sufficient
(Usual care seems effective in “uncomplicated cases of LBP” – Jallema et al., 2006)
• High psychosocial risk factors, need to target these aspects more than usual care
• So, you don’t have to intervene early in most cases • Just those in higher risk category • But, you have to identify them
The University of Sydney Page 9
9
To identify high risk cases:
Brief OMPSQ - developed and published 2011
• 24-item version promoted by WorkCover since 2005 • New version: 10-items • High correlation with long form of OMPSQ (24 items) • Scores > 50 able to predict 85% long-term sick leave
within next year
The University of Sydney Page 10
But problem of delayed RTW not just to do with
injured worker – the workplace important too
Supporting evidence strongest for treatment providers engaging with workplace – RTW as part of treatment, not after treatment
The University of Sydney Page 11
More recent systematic review (2017) similar to
Franche et al (2005), but stronger evidence (more than
just the worker)
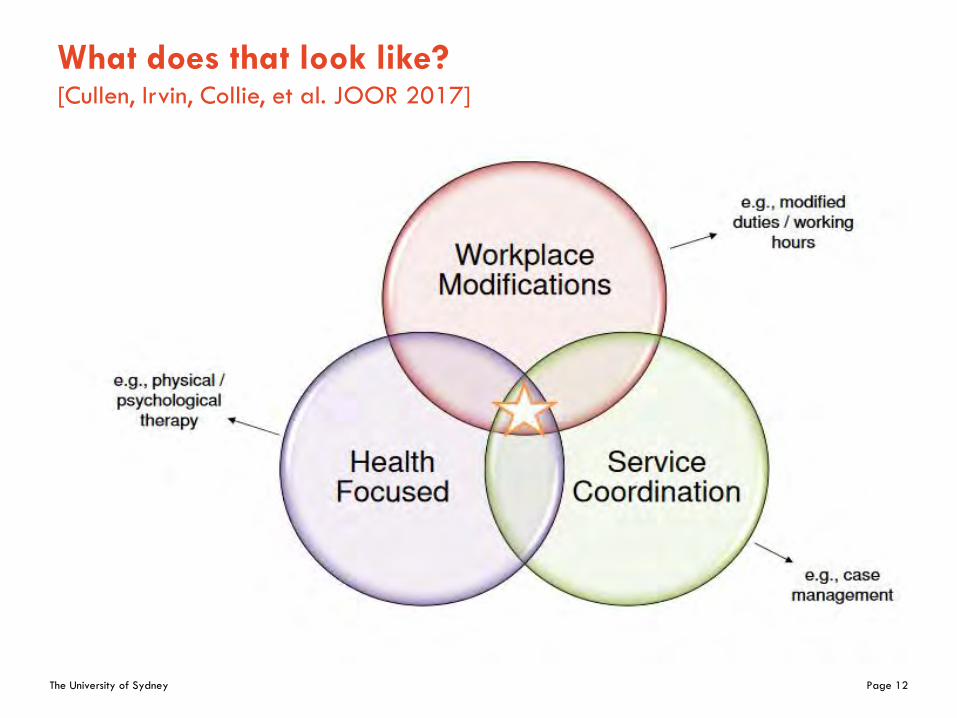
Strong level of evidence for multidomain interventions (service coordination, work modification and improving worker health) for reducing lost time from injuries. Moderate level of evidence for improving work functioning after RTW and reducing costs
Recommendation:
Implement a multi-domain intervention to help reduce lost time for MSK and pain-related conditions.
The University of Sydney Page 12
What does that look like? [Cullen, Irvin, Collie, et al. JOOR 2017]
The University of Sydney Page 13
13
New study (WISE) launched mid-2013
• Soft-tissue injuries account for a significant proportion of workers compensation injuries (53% for 2011–12).
• For NSW Health (69% for 2011–12). • Vast majority RTW rapidly, but those who don’t = higher
costs • NSW Health’s 2012–13 workers compensation premium
increased by $24m to $181m (15%) A key reason: Increased time away from work!
Background - in NSW
The University of Sydney Page 14
Key feature of the WISE study
• It was not about treatment as such
• But a protocol for stratified responses to
workplace injuries
• Theoretical basis in implementation science
The Consolidated Framework For Implementation Research (CFIR) (Damshroder et al., 2009)
The University of Sydney Page 15
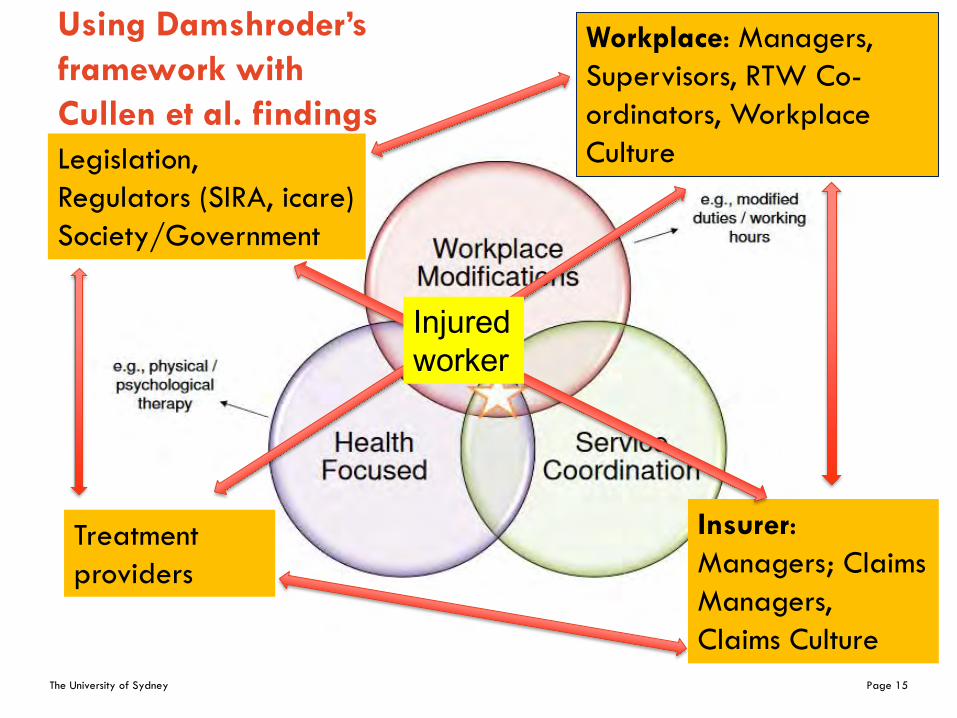
Using Damshroder’s
framework with
Cullen et al. findings
Workplace: Managers,
Supervisors, RTW Co-
ordinators, Workplace
Culture
Treatment
providers
Insurer:
Managers; Claims
Managers,
Claims Culture
Legislation,
Regulators (SIRA, icare)
Society/Government
Injured worker
The University of Sydney Page 16
16
• The statutory organisation responsible for public sector workers compensation in NSW (icare) (under Ministry for Finance, Services & Property)
• The regulator (was Workcover, now SIRA) • The employer (NSW Health + Hospital management),
with support from Unions • The Insurance agent (EML) – managers, claims teams • Individual psychologists (recruited for study) • Independent occupational physicians • Independent specialist physiotherapist • General Practitioners (for each injured worker)
Framework for the WISE Study: we engaged
The University of Sydney Page 17
17
1. Time lost from work over two years post-injury
2. Cost of claims
Primary outcomes for WISE Study
The University of Sydney Page 18
18
WISE Study : selection criteria
• Injured health workers • ‘Significant’ soft tissue injuries (work-related) • Off work with medical approval • No injuries that required surgery • Claim accepted by EML • Injured worker had to agree to participate
(voluntary) – explained by Claims manager • If agreeable, screening questions delivered over
phone within 7 days of injury • Screening (OMPSQ-10: Linton et al., Spine 2011),
cut off: scores >50/100
The University of Sydney Page 19
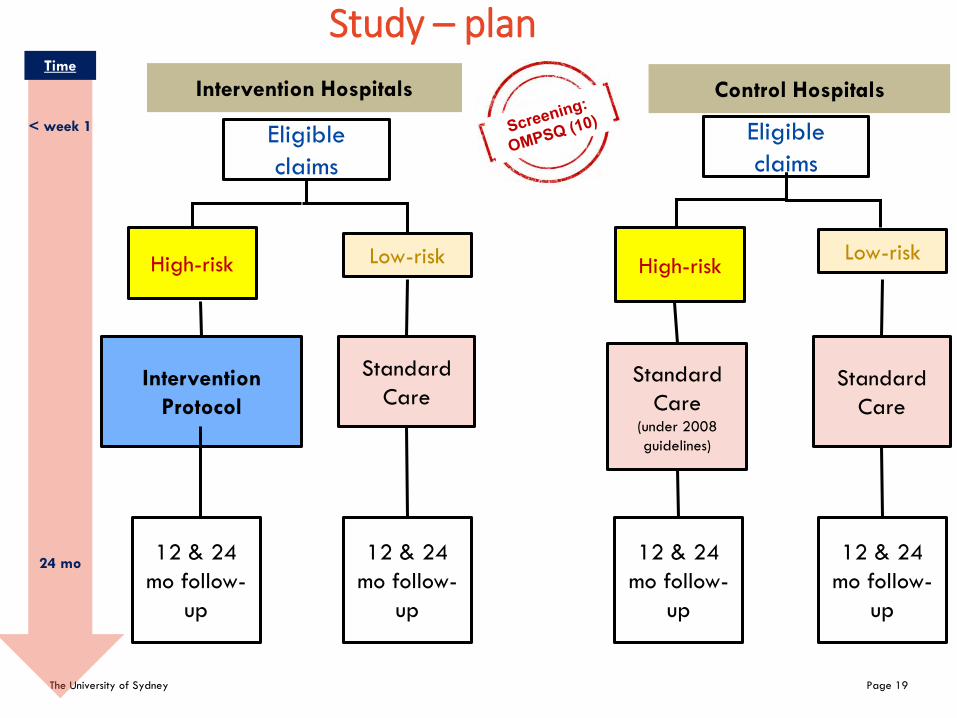
Eligible
claims
Eligible
claims
High-risk Low-risk
< week 1
24 mo
Time
Intervention
Protocol
Standard
Care
12 & 24
mo follow-
up
12 & 24
mo follow-
up
Intervention Hospitals Control Hospitals
High-risk Low-risk
Standard
Care (under 2008
guidelines)
Standard
Care
12 & 24
mo follow-
up
12 & 24
mo follow-
up
Study – plan
The University of Sydney Page 20
20
•
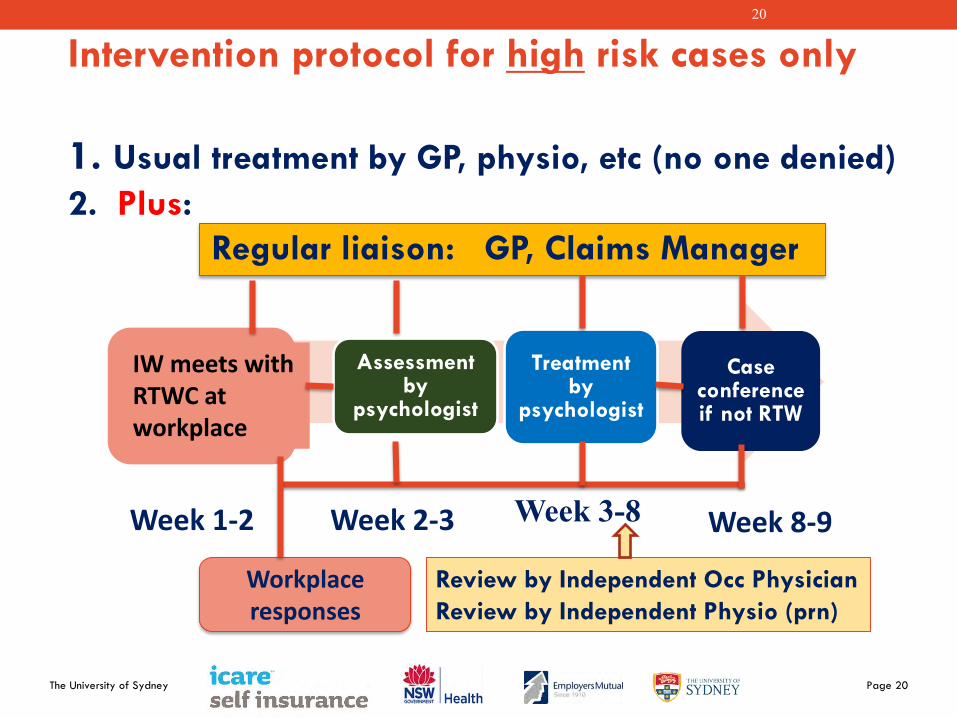
Intervention protocol for high risk cases only
1. Usual treatment by GP, physio, etc (no one denied)
2. Plus:
Regular liaison: GP, Claims Manager
Assessment by
psychologist
Treatment by
psychologist
Case conference if not RTW
Week 1-2 Week 2-3 Week 3-8 Week 8-9
Review by Independent Occ Physician
Review by Independent Physio (prn)
Workplace responses
IW meets with RTWC at workplace
The University of Sydney Page 21
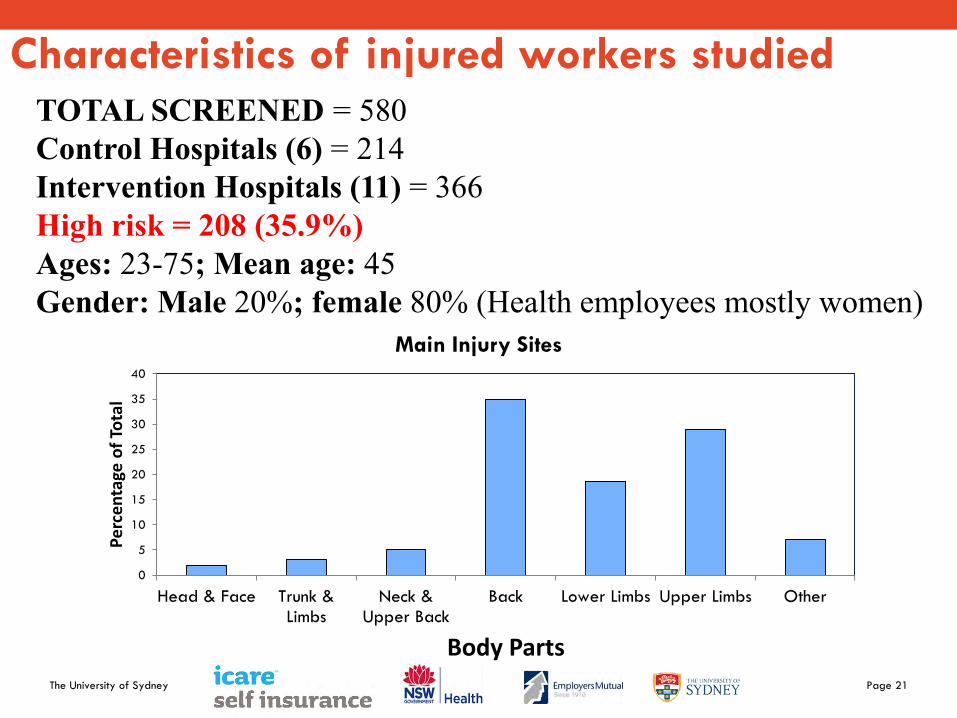
Characteristics of injured workers studied
0
5
10
15
20
25
30
35
40
Head & Face Trunk &Limbs
Neck &Upper Back
Back Lower Limbs Upper Limbs Other
Per
cen
tage
of
Tota
l
Body Parts
Main Injury Sites
TOTAL SCREENED = 580 Control Hospitals (6) = 214 Intervention Hospitals (11) = 366 High risk = 208 (35.9%) Ages: 23-75; Mean age: 45 Gender: Male 20%; female 80% (Health employees mostly women)
The University of Sydney Page 22
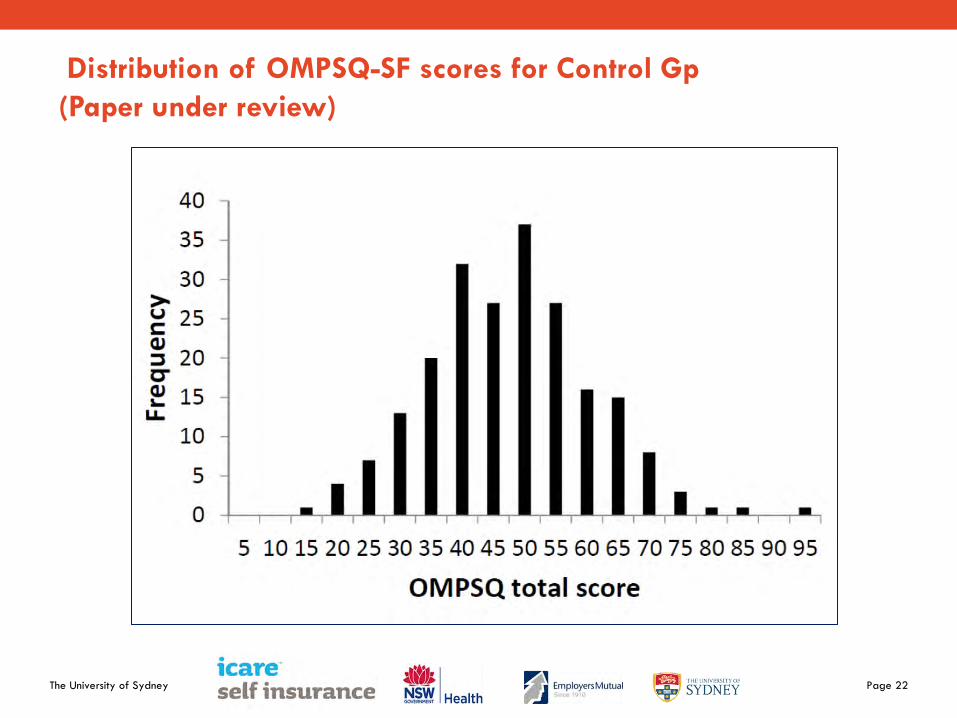
Distribution of OMPSQ-SF scores for Control Gp
(Paper under review)
The University of Sydney Page 23
23
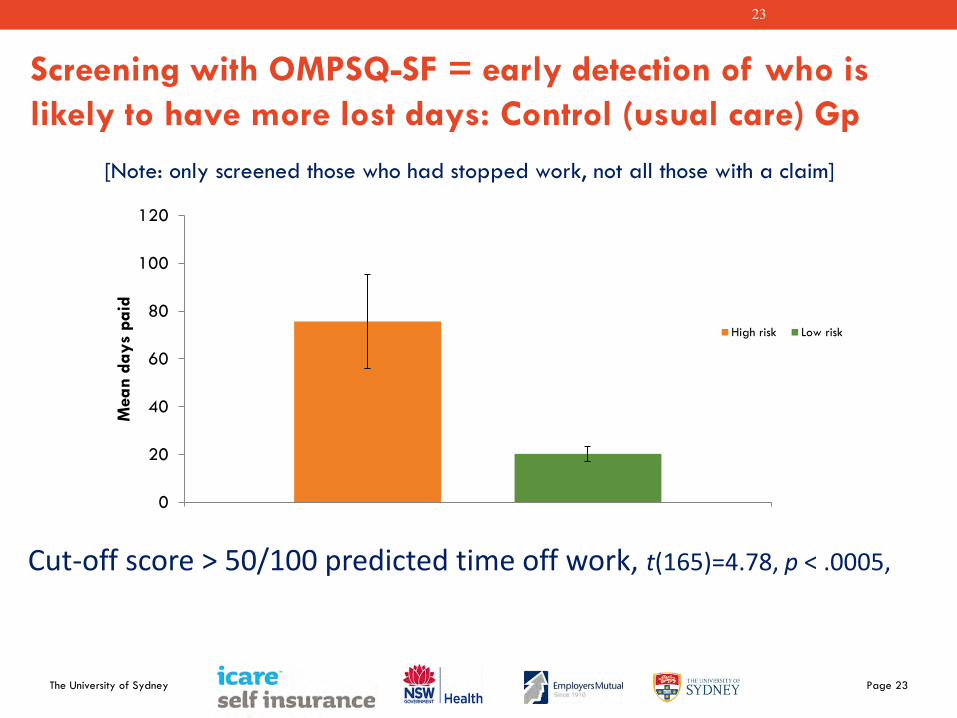
Screening with OMPSQ-SF = early detection of who is
likely to have more lost days: Control (usual care) Gp
Cut-off score > 50/100 predicted time off work, t(165)=4.78, p < .0005,
0
20
40
60
80
100
120
Mean d
ays
paid
High risk Low risk
[Note: only screened those who had stopped work, not all those with a claim]
The University of Sydney Page 24
24
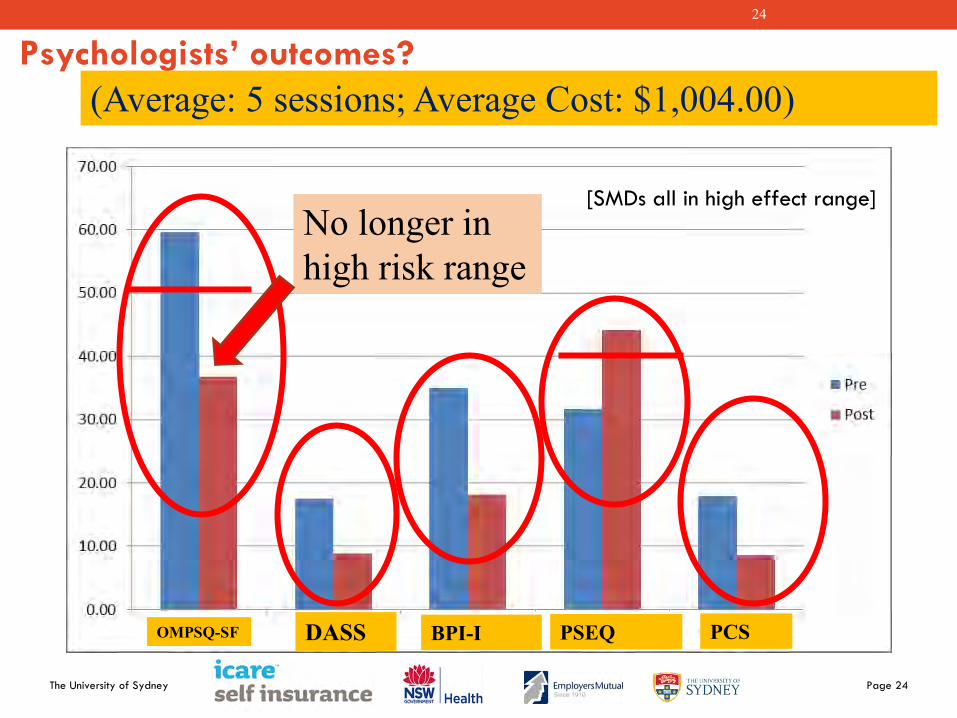
Psychologists’ outcomes?
(Average: 5 sessions; Average Cost: $1,004.00)
No longer in high risk range
OMPSQ-SF DASS BPI-I PSEQ PCS
[SMDs all in high effect range]
The University of Sydney Page 25
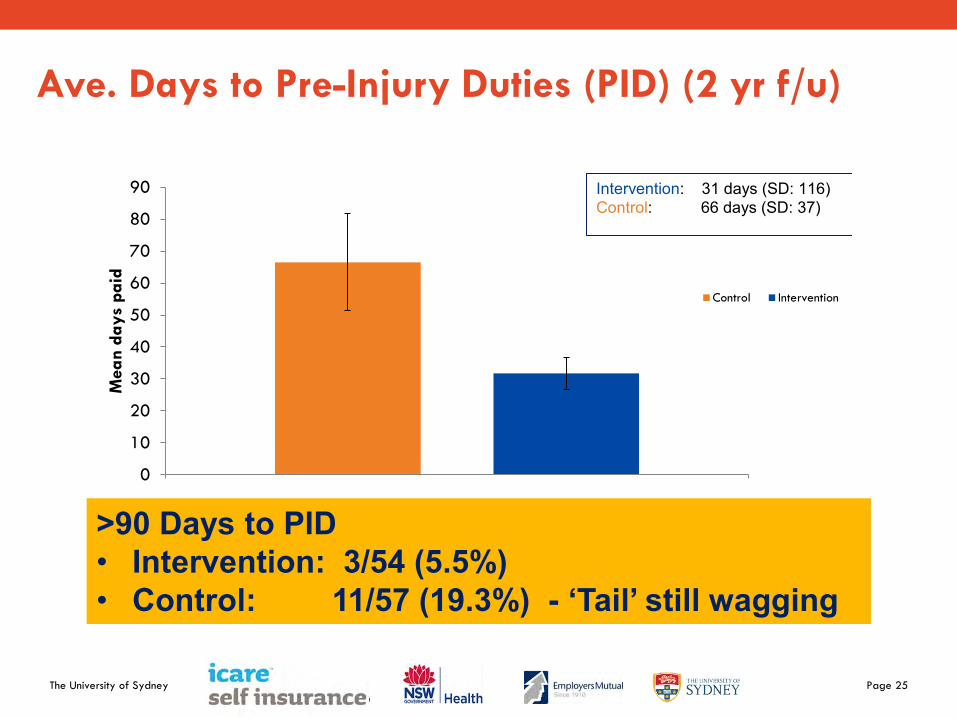
Ave. Days to Pre-Injury Duties (PID) (2 yr f/u)
>90 Days to PID • Intervention: 3/54 (5.5%) • Control: 11/57 (19.3%) - ‘Tail’ still wagging
0
10
20
30
40
50
60
70
80
90
Mean d
ays
paid
Control Intervention
Intervention: 31 days (SD: 116) Control: 66 days (SD: 37)
The University of Sydney Page 26
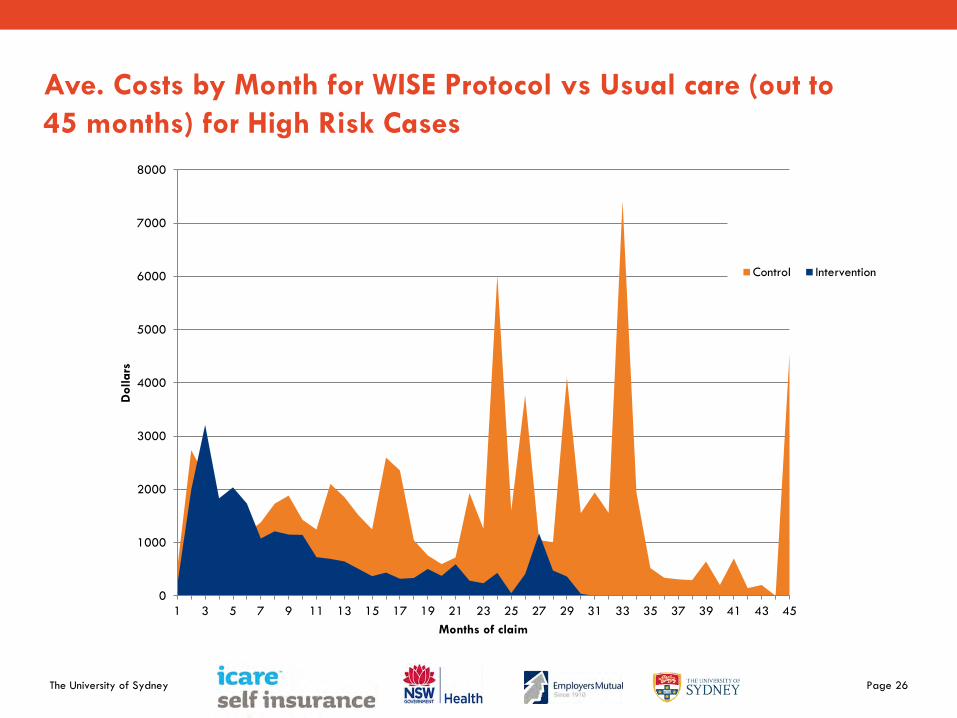
Ave. Costs by Month for WISE Protocol vs Usual care (out to
45 months) for High Risk Cases
0
1000
2000
3000
4000
5000
6000
7000
8000
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45
Dollars
Months of claim
Control Intervention
The University of Sydney Page 27
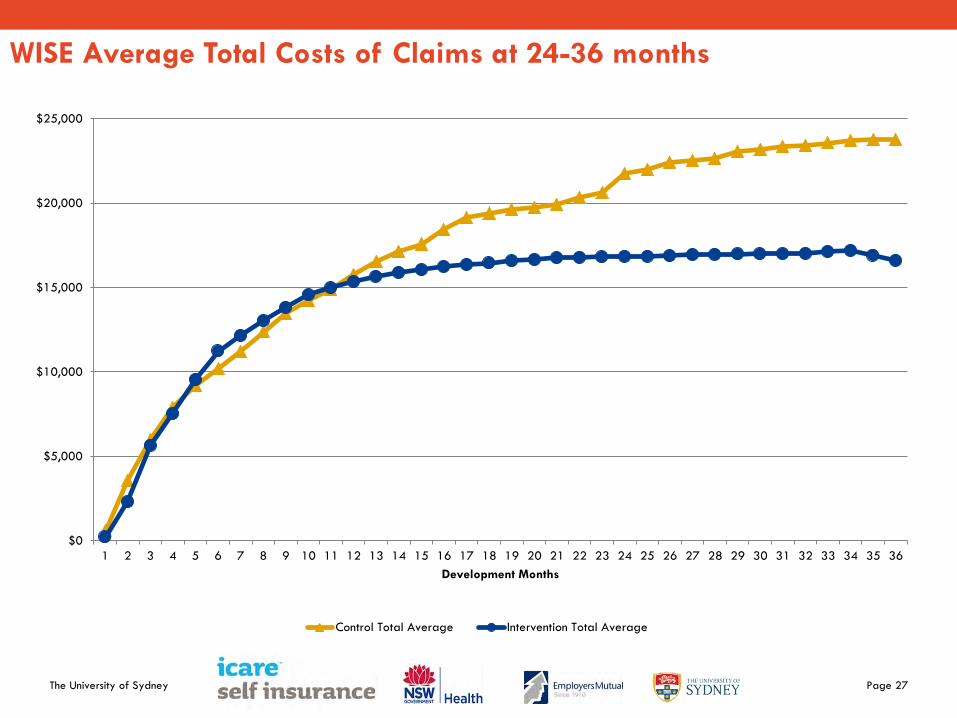
WISE Average Total Costs of Claims at 24-36 months
$0
$5,000
$10,000
$15,000
$20,000
$25,000
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36
Development Months
Control Total Average Intervention Total Average
The University of Sydney Page 28
Summary of overall outcomes
• Average savings (on total costs) at 2 years: 30%
Outcomes are not just about the numbers: • All Intervention sites wanted to maintain WISE protocol • Since June 2015, NSWHealth has implemented WISE
protocol across state for all public hospitals • In 2016 NSWHealth premiums declined
The University of Sydney Page 29
29
WISE study – key lessons: A system intervention
Key features:
• Use of agreed protocol (closely monitored /reinforced)
• Identify those at risk due to psychosocial factors
• Access to help for modifying these risk factors
• Coordinated support and input by all stakeholders
(insurer, workplace, health care providers, injured
workers)
In essence:
• Helping the injured worker and workplace (vs treating
the injury alone) – consistent with Cullen et al (2017)
The University of Sydney Page 30
30
To describe it graphically But, if one player doesn’t do their bit ….???

The University of Sydney Page 31
31
Acknowledgements
Steve Hunt
John Roach
Hospitals and Area Health Management
Westmead Sutherland Dubbo Base
Blacktown Wagga Wagga Nowra
Mt Druitt Orange Base Sydney
Nepean St George Royal Hospital
St Vincents Prince of Wales for Women
Wollongong Royal Prince Alfred Broken Hill Base
Bega District
And, all those injured health workers who agreed to participate
Independent Physiotherapy Consultant: Dr Rob Boland
Research Assistant: Leigh-Anne Funnell