Embed Size (px)
Citation preview

Early Head Start – Child Care Partnerships
Comprehensive Services Part II:Health, Mental Health, Nutrition, and Disabilities
Presenters
Marco Beltran, DrPH
Program Specialist,
Office of Head Start
Tatiana Tucker, MSA
Program Specialist,
Office of Child Care
Health & Safety Learning & School Readiness
• Sick children are away from program activities, leading to regression in cognitive & general knowledge
• Time out due to illness will impact the amount of time needed to develop relationships and or form attachments
Objectives
1. To provide information to potential applicants on the Head Start health, mental health, nutrition and disabilities services
2. To identify the Program Performance Standards related to all of the Head Start health services
3. To identify resources that help support the Head Start health services
4. To provide background information about the Child Care and Development Fund (CCDF)
5. To identify the Health and Safety requirements for CCDF
6. To understand the key roles of Child Care Health Consultants
Head Start Program Performance Standards
• Determine a child’s current health status • Screen for developmental, sensory, and
behavioral concerns • Provide ongoing health care • Monitor health and safety issues • Provide nutrition services • Individualize to each child• Provide mental health consultation or
disability services, if needed• Communicate between staff and parents
Health Services Set the Stage
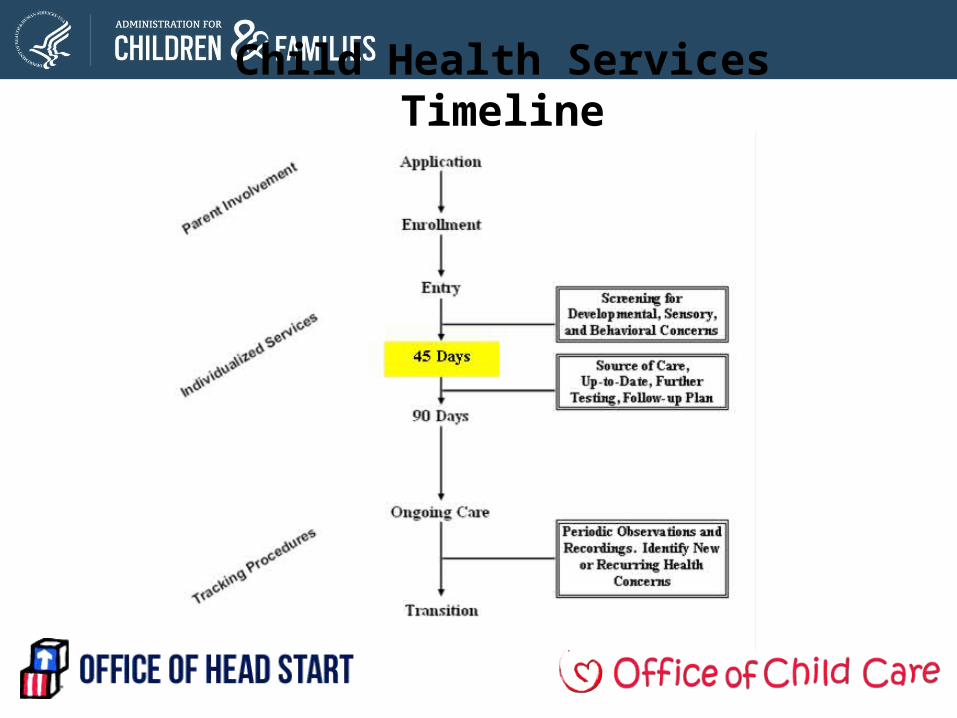
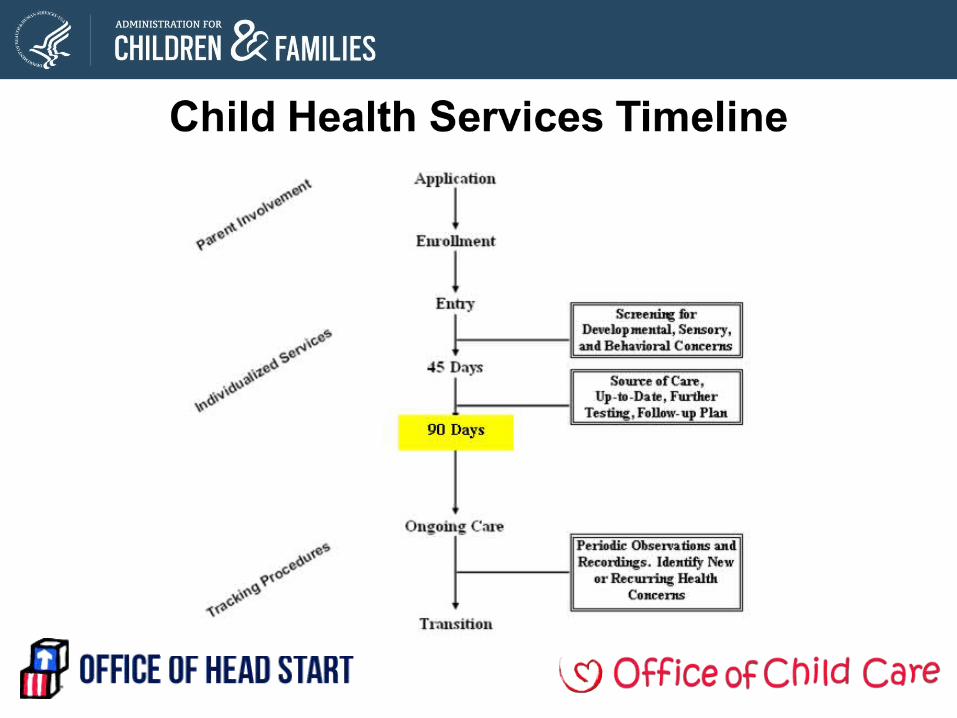
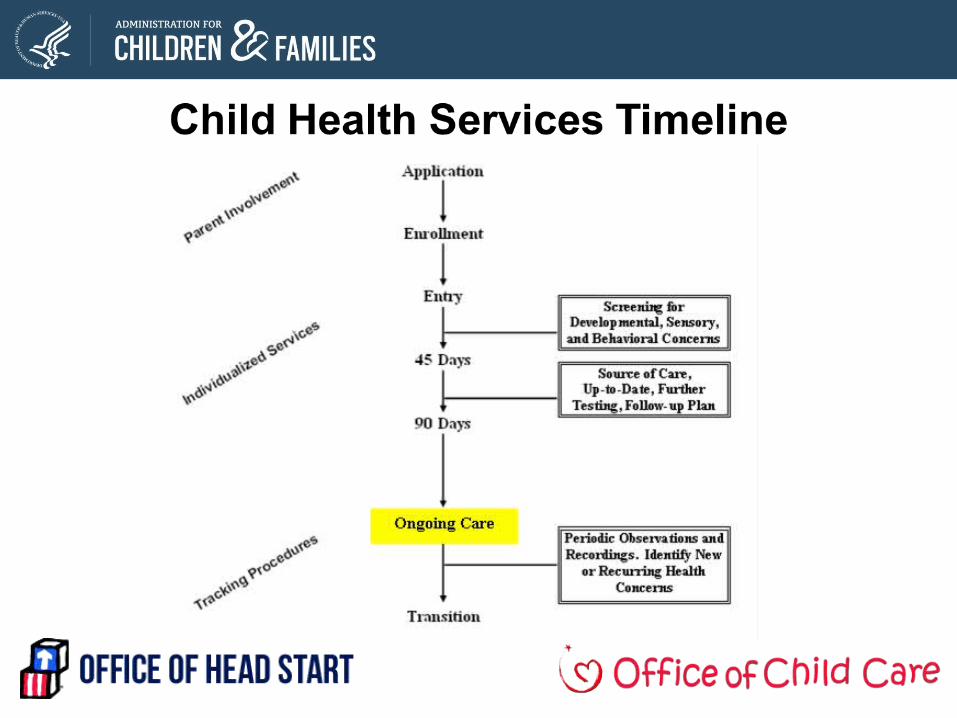
Child Health Services Timeline
Screening Standards
1304.20 (2)(b) Screening for developmental, sensory, and behavioral concerns
Within in 45 days…identify concerns regarding a child’s developmental, sensory (visual and auditory), behavioral, motor, language, social, cognitive, perceptual, and emotional skills
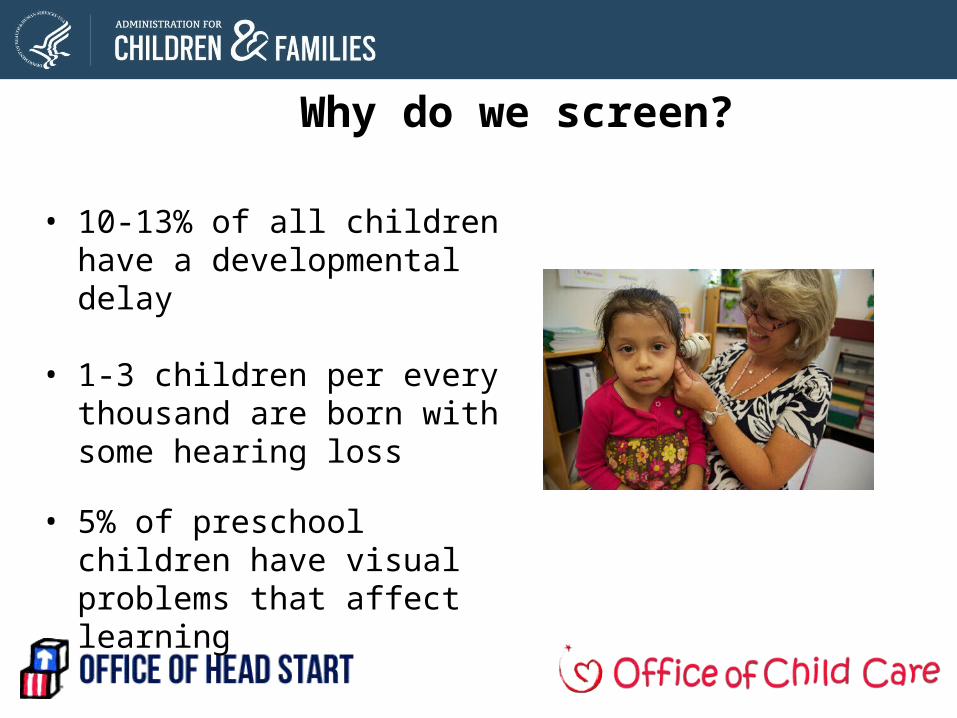
Why do we screen?
• 10-13% of all children have a developmental delay
• 1-3 children per every thousand are born with some hearing loss
• 5% of preschool children have visual problems that affect learning
A comprehensive screening approach …
• Multiple sources of information– Family– Teacher/Caregiver/Home Visitor observations– Health, emotional state, and energy levels of the child– A standardized tool
• Culturally and linguistically appropriate
Also check out:
www.hhs.gov/watchmethrive
Child’s Health Status Standards
1304.20 (a)(1)(i)-(iii) Determine child health status
No later than 90 calendar days… from the child's entry
• Determine if each child has an ongoing source of continuous, accessible health care
• Obtain from a health care professional a determination as to whether the child is up-to-date on a schedule of age-appropriate preventive and primary health care…and the latest immunization recommendations…
An EPSDT well-child exam may include:
− Screening (i.e., vision, hearing, medical and dental)− Immunizations− Laboratory tests− Diagnostic or treatment services− Vision and hearing services− Other health care
Remember: Each screen and each state has its own “periodicity schedule”
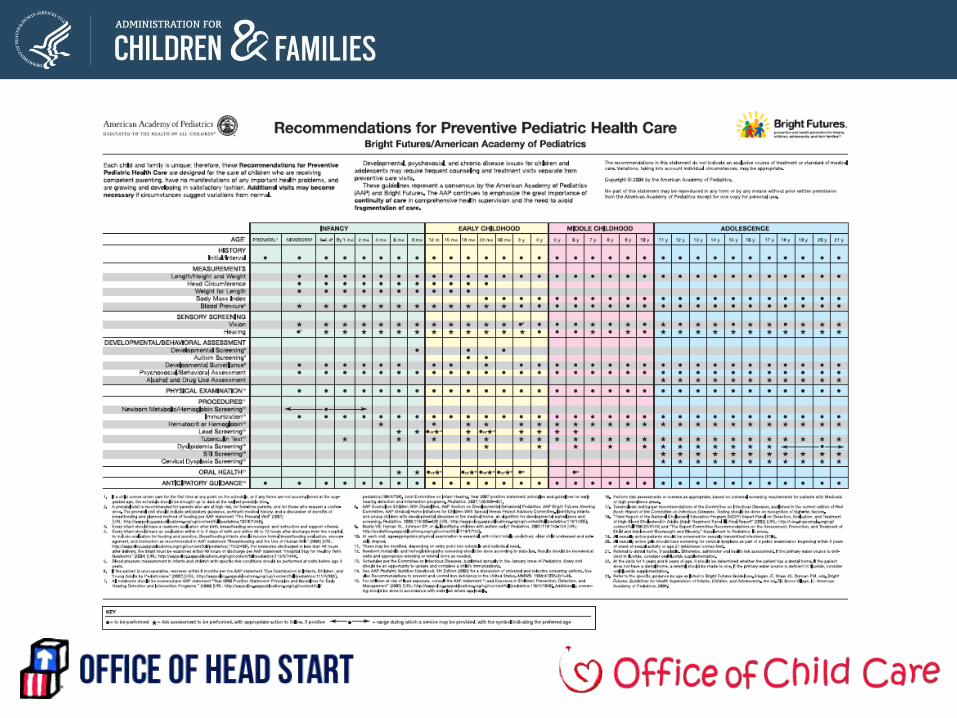
Schedule of Well Child Care
Follow-Up Plan and Tracking Standards
1304.20 (a)(1)(C)(iii)(iv) …must establish procedures to track the provision of health care services
• Obtain or arrange further diagnostic testing, examination, and treatment by an appropriate licensed or certified professional for each child with an observable, known or suspected health or developmental problem
• Develop and implement a follow-up plan for any condition identified…so that any needed treatment has begun
Ongoing Care
• Implement ongoing procedures by which staff can identify any new or recurring medical, dental, or developmental concerns
• Procedures must include: periodic observations and recordings, as appropriate, of individual children's developmental progress, changes in physical appearance (e.g., signs of injury or illness) and emotional and behavioral patterns
Individualization of the Program
• Determine how the program can best respond to each child's individual characteristics, strengths and needs using a variety of sources
• Support individualization for children with disabilities through implementation of an IEP/IFSP
• Children’s needs for early intervention, special education, or related services are identified promptly
Services for Children with Disabilities
• Enrolled over 136,000 children with disabilities
• Nearly 12% of Head Start’s enrollment
• Over 21,000 were infants and toddlers enrolled in EHS and MSHS
Services for Infants and Toddlers with DisabilitiesLanguage in the Head Start Program Performance Standards - 45 CFR1304.20 (f) (1) (i) – requires that Head Start program serving infants and toddlers must provide services for infants and toddlers with disabilities and their families that support the attainment of the expected outcomes contained in the Individualized Family Service Plan (IFSP) for children identified under Part C of the Individuals with Disabilities Education Act (IDEA).
Language in the Head Start Act - 645A (b) 11 – clearly states that programs ensure formal linkages with providers of early intervention services for infants and toddlers with disabilities with the State interagency coordinating council, as established in part C of the Individuals with Disabilities Education Act (20 U.S.C. 1431 et seq.), and with the agency responsible for administering section 106 of the Child Abuse Prevention and Treatment Act (42 U.S.C. 5106a).
Disabilities Services
• At least 10% of Head Start enrollment is for children determined eligible for services under the Individuals with Disabilities Education Act (IDEA)
• Children with disabilities and their families are included in the full range of Head Start program activities
• Parents of children with disabilities are supported and engaged as decision-makers, receiving information and assistance to address their child’s special needs and to advocate for them
Mental Health Standards
1304.21 Education and ECD
1304.24 Child Mental Health
1304.40 Family Partnerships
Mental Health
• Promote social and emotional development• Build trust, foster independence, encourage self-control • Support and respect home language, culture, family
composition • Involve parents in mental health interventions• Provide mental health education for staff, parents,
families• Facilitate opportunities for parent to participate in
counseling programs
Mental Health
1304.24 (a)(2) and (3) Child Mental Health
…secure the services of mental health professional on a schedule of sufficient frequency to enable the timely and effective identification of and intervention in family and staff concerns about a child’s mental health . . .
Mental health program services must include a regular schedule of onsite mental health consultation…
Programs find mental health consultant/providers through…
• Local mental health agencies/providers
• State children’s mental health directors
• Universities, colleges, and community colleges – departments of social work, child psychology, child psychiatry, special education, and their counseling centers
http://ecmhc.org/materials_consultants.html
Nutrition Standards
1304.23 Child Nutrition
• Staff and families must work together to identify each child’s nutritional needs
• Use nutrition related assessment data• Use information about family eating patterns, cultural
preferences, dietary requirements and feeding requirements
• Feeding schedules• Use information about community nutritional issues
Nutrition Services
• Design and implement a nutrition program that meets the nutritional needs and feeding requirements of each child
• Use funds from USDA Food and Consumer Services Child Nutrition Programs as the primary source of payment
• Funds may be used to cover those allowable costs not covered by the USDA
Also check out:
http://www.cditeam.org/table/family_style_dining/practices.htm
Nutrition Services
• Serve a variety of foods - consider cultural and ethnic preferences
• Promote effective dental hygiene among children in conjunction with meals
• Include opportunities to assist individual families with food preparation and nutritional skills
• Involve parents in planning, implementing, and evaluating the agencies' nutritional services
Meal Service• Ensure services contribute to child’s development and
socialization • Serve foods that broadens food experiences• Food is not used as punishment or reward• Allow sufficient time for each child to eat• Family style dining - children and staff eat together family
style and share the same menu to the extent possible• Hold infants while feeding; do not lay infant down to sleep
with a bottleAlso check out:
http://www.cditeam.org/table/family_style_dining/practices.htm
Food Safety and Sanitation
• Post evidence of compliance with all applicable Federal, State, Tribal, and local food safety and sanitation laws, including those related to the storage, preparation and service of food and the health of food handlers
• Contract only with food service vendors that are licensed in accordance with State, Tribal or local laws
• Facilities must be available for the proper storage and handling of breast milk and formula
Involving Parents in Health Services
• Consult with parents immediately when child health or developmental problems are suspected or identified
• Familiarize parents with health and developmental procedures; obtain advance authorization
• Share diagnostic results and treatment procedures and ongoing care
• Assist parents to enroll and participate in a system of ongoing family health care and encourage parents to be active partners in their children's health care process
Health and Safety Standards
• Foundation for high quality care
• Over 100 individual standards related to health and safety
• Found in each section of HSPPS
Health and Safety Standards
Prevent illness by maintaining healthy environments
45 CFR 1304.22(a); 1304.22(c); 1304.22(e); 1304.23(e); 1304.52(l)(3)(i); 1304.53; 1306.35
Prevent childhood injurieso Identify and report child abuse and neglecto Implement injury prevention strategies
45 CFR 1301.31(e); 1304.22(a)(5); 1304.22(b); 1304.22(f); 1304.23(e); 1304.52(e)-(h); 1304.52(i)(iii)-(iv); 1304.52(l)(3)(i); 1034.52(l)(4); 1304.53; 1306.35; 1310.11; 1310.16
Health and Safety Standards
Provide education for children, families, staff and volunteers on injury prevention practices 45 CFR 1304.22(d); 1304.40f)(3)(iii); 1310.17; 1310.21
Conduct inspections of any facility, equipment and materials used by the program 45 CFR 1304.22(f); 1306.30(c)
Develop, practice and use emergency plans 45 CFR 1304.22(a); 1304.40(b)(1)(i);
1306.35(b)(1)
Staff Qualifications
• Health services must be supported by staff or consultants that have training and experience in public health, nursing, health education, maternal and child health, or health administration. In addition, when a health procedure must be performed only by a licensed/certified health professional, the agency must assure that the requirement is followed [HSPPS 45 CFR 1304.52(d)(2)].
• Nutrition services must be supported by staff or consultants that are registered dieticians or nutritionists [HSPPS 45 CFR 1304.52(d)(3)].
• Mental Health services must be supported by staff or consultants that are licensed or certified mental health professionals with experience and expertise in serving young children and their families [HSPPS 45 CFR 1304.52(d)(4)].
• Disabilities must be supported by staff or consultants that have training and experience in securing and individualizing needed services for children with disabilities [HSPPS 45 CFR 1304.52(d)(7)].
• Content area experts including managers, coordinators or consultants who work with infant and toddler staff need the capacity to assist them in appropriately implementing and adapting the services for children from birth to 36 months of age.
CCDF Overview Grantees. 50 States, DC, Territories, and 260 Tribal entities Funding. Jointly financed by Federal and State governments. CCDF program
combined federal funding for FY 2012 - $5.2 billion. Flexibility. CCDF provides flexibility to States, Territories, and Tribes in
establishing policies that support families’ access to child care through subsidies.
Children and Families Served. Approximately 1.6M low-income children and families receive child care subsidies per month
Coordination. CCDF allows States, Territories, and Tribes to serve families through a single, integrated child care subsidy program under the rules of the CCDBG Act. States coordinate CCDF with Head Start, pre-kindergarten, and other early childhood programs.
Child Care and Development Fund (CCDF)
OCC Vision
• More children in low-income families able to access high quality care
CCDF Purpose
• Assists low-income working families obtain child care so they can work or attend training/education
• Improves quality of child care and promotes coordination among early childhood development and afterschool programs
CCDF Law
• Child Care and Development Block Grant Act (CCDBG) of 1990• Section 418 of Social Security Act
OCC Quality FrameworkPathways to
Program Quality
Pathways to
Professional
Development
Children’s Healthy Development and
School Readines
s and Success
Health and Safety
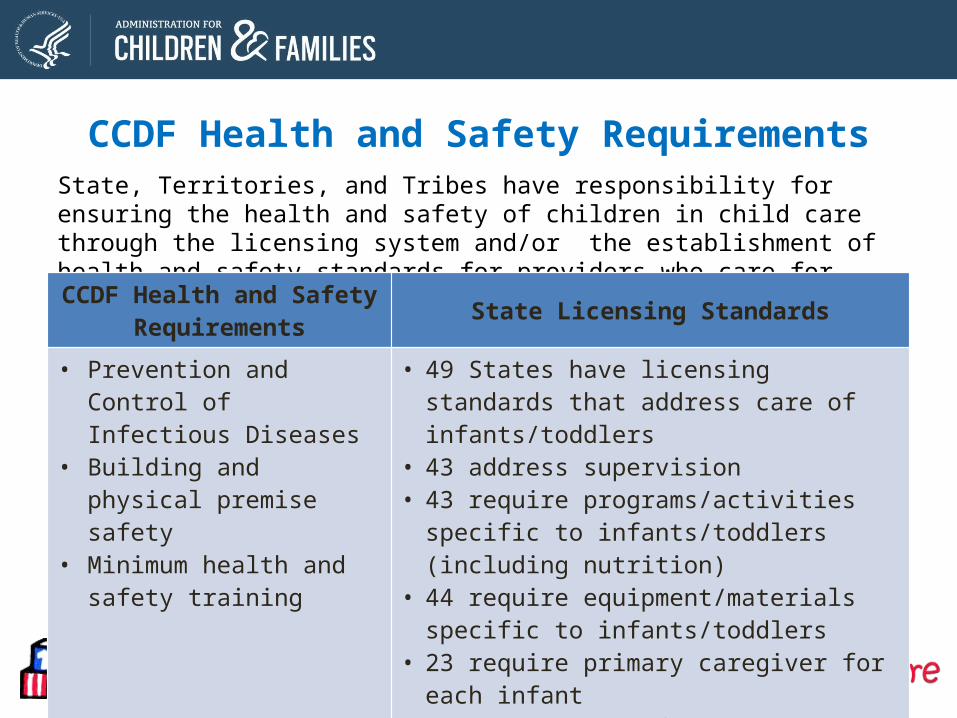
State, Territories, and Tribes have responsibility for ensuring the health and safety of children in child care through the licensing system and/or the establishment of health and safety standards for providers who care for children receiving CCDF funds.
CCDF Health and Safety Requirements State Licensing Standards
• Prevention and Control of Infectious Diseases
• Building and physical premise safety
• Minimum health and safety training
• 49 States have licensing standards that address care of infants/toddlers
• 43 address supervision• 43 require programs/activities specific to
infants/toddlers (including nutrition)• 44 require equipment/materials specific to
infants/toddlers• 23 require primary caregiver for each infant• 17 require specific qualifications for staff
CCDF Health and Safety Requirements
$1 billion a year spent on quality improvement activities. Lead Agencies are required to spend at least 4% of CCDF allocation on these
activities. Actual State spending was 12% in FY2010Includes $100M specifically set-aside by Congress for infants and toddler care
Examples of Activities Supported by Quality Funds: Scholarships for providers to obtain accreditation of continuing education and
training Grants or loans to help programs meet quality and health and safety standards Health consultants working with early care and education programs Enforcement of health and safety requirements Infant and Toddler Specialists
CCDF Quality Investments
Child Care Health Consultants
• Child Care Health Consultants are health professionals who have received specialized training in child health, child development, and health and safety in child care settings
• In 2012, approximately 30 States reported using health consultants in child care
• CCHCs and child care staff work together to promote healthy and safe environments for young children
Role of a CCHCA CCHC can help improve the health and safety of children in child care and head start programs by:
• Meeting on-site with child care providers about health and safety
• Reviewing health records of children and child care providers
• Helping to manage the care of children with special health care needs
• Identifying children with developmental delays
Other Resources to help providers meet Health and Safety Standards
– Healthy Child Care America• http://www.healthychildcare.org/ResourcesHP.html
– Provides resources and online trainings to early care and education providers on the health and safety of children in out-of-home child care.
» Medical administration» Preventing Infectious Diseases » Safe Sleep Practices/SIDS
– Let’s Move Child Care • http://www.healthykidshealthyfuture.org/welcome.html
– Help providers adopt best practices for physical activity and nutrition through interactive online tools
– Let’s Move Child Care Training Modules» http://
extension.psu.edu/youth/betterkidcare/news/2014/new-lets-move-child-care-lessons
Where To Go for More Information and Resources
https://childcareta.acf.hhs.gov
http://eclkc.ohs.acf.hhs.gov/hslc/hs/grants/ehs-ccp

http://eclkc.ohs.acf.hhs.gov/hslc/tta-system/health
Resourceshttp://ecmhc.org/materials_consultants.html
www.hhs.gov/watchmethrive
http://www.cditeam.org/table/family_style_dining/practices.htm
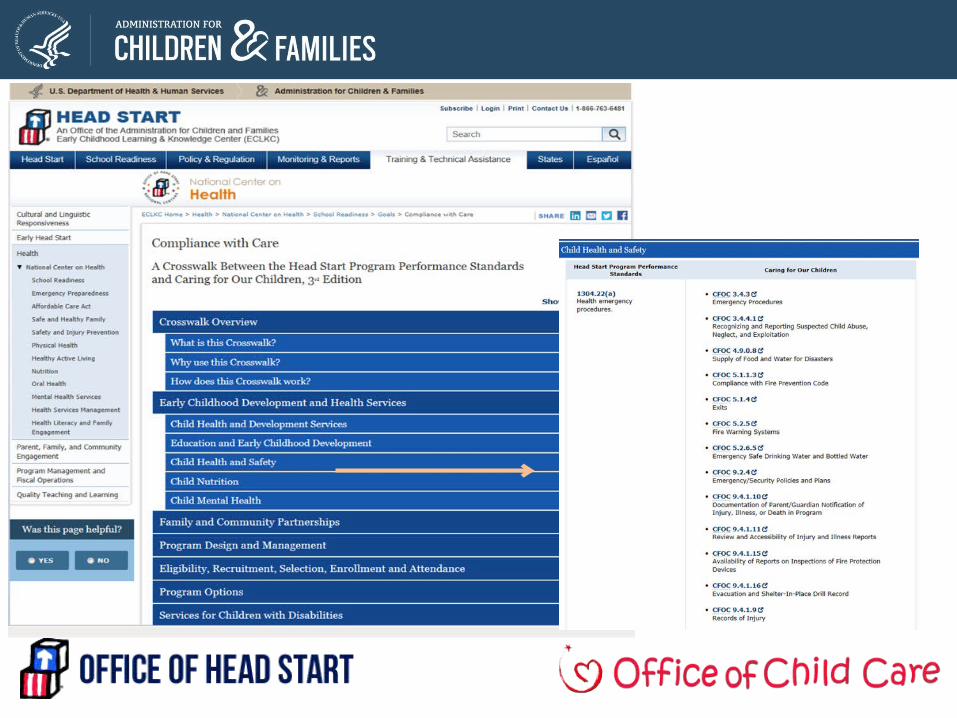
http://eclkc.ohs.acf.hhs.gov/hslc/tta-system/health/center/school-readiness/goals/crosswalk.html
http://www.healthykidshealthyfuture.org/welcome.html
• http://eclkc.ohs.acf.hhs.gov/hslc/tta-system/health
• www.safekids.org
• www.brightfutures.org
• www.nrckids.org
• www.cpsc.gov
• www.cdc.gov
Are You Planning To Apply?
• Register with Grants.gov Only the Applicant organization needs to register The registration process can take one to three weeks
depending on your organization, so start now! You will receive notifications based on Funding Opportunity
Number (FON)A FON is a number that a federal agency assigns to each specific grant announcement
• Obtain Data Universal Numbering System (DUNS) Number
• Register in System for Award Management (SAM) Eligibility Requirements
• Visit: http://www.acf.hhs.gov/grants/register-and-get-ready
STAY TUNED
For the next webinar in the series:
• Comprehensive Services Part III: Family and Community EngagementFriday, March 28, 2 p.m. EDT
• Maximizing Resources and the Role of GovernanceMonday, March 31, 2 p.m. EDT
THANK YOU