Embed Size (px)
Citation preview
EARLY FREE GRAFTING: THE RESTITUTION OF PARTS COMPLETELY SEPARATED FROM THE BODY
By THOMAS GIBSON, F.R.C.S.Ed., F.R.C.S.Glasg.
Senior Lecturer in Tissue Transplantation, University of Glasgow
" A n d one of them smote the servant of the high priest and cut off his right ear. And Jesus answered and said, Suffer ye this far. And he touched his ear and healed h i m . " - - S t Luke 22, 50-5i.
IN 1869 Reverdin, working in Paris, stumbled accidentally on an essential criterion for successful free grafting, namely that the graft must be thin. Before this time an astonishing amount of experimental work o n " animal "as distinct f rom" plant" grafts had been performed, although most of the results had been partial or complete failures because the pieces of tissue transplanted had been too bulky. The reason for this pre-occupation with large composite grafts was partly the analogy with plants but also because the only free grafts known to have succeeded were parts of the body which had been completely severed and subsequently re-attached. From media:val times onwards an increasing number of instances had been reported in which a finger, a nose, or an ear had been cut off and allegedly successfuUy replaced ; as is so frequently the case, the innumerable failures were forgotten while the rare success, often inadequately described and attested, received wide and misleading publicity.
Almost a century has passed since the young interne in the Hotel Dieu seeded a raw granulating area with small fragments of skin, and it is regrettable that to-day we have advanced only to the extent of using technical adaptations of Reverdin's discovery. Our free skin grafts must still be thin if they are to survive, and a reliable technique for free transplantation of larger composite grafts has yet to be found, Nonetheless, in spite of the failures, it seems incontestible that noses, ears, lips, fingers, or parts thereof have survived replacement after being completely detached although success has been so rare that few casualty surgeons to-day would feel justified in attempting the operation. This study is one of a series on free grafting before Reverdin and, dealing mainly with the literature of that period, was undertaken partly for its intrinsic historical interest and partly to see if it would provide some clue to the criteria for survival of massive free grafts.
EARLY M Y T H AND LEGEND
In an age when few men went abroad without sword or dagger and wars were fought with sharp steel, there can have been no lack of clinical material in the form of noses, ears, fingers, and other bodily parts sliced off, and it is surprising that so few reports of successful reunions have come down to us from the Middle Ages and the Renaissance. There is little doubt that the experiments were tried, and stories did circulate about successful cases. The great majority of attempts must have been failures however, and nearly all the early surgical writers mentioned the subject only to say that it was impossible. As early as the thirteenth century
IA I
2 BRITISH JOURNAL OF PLASTIC SURGERY
Lanfranchi denounced the rttmours with scathing words : "Eos derideo et mendacii impudentissimi arguo," he stormed--" I scorn these men and accuse them of the most impudent lying, who dare to assert that they have held in their hands a nose which had been cut off and which was later restored in place." Guy de Chauliac (13oo-68) in his Chirurgia Magna (1363) concurred : " S i nasus ex toto cecederit amplius non potest reunite " - - " It is not possible to reunite a nose which has been completely cut off." Theodoricus della Cervia (12o5-98) dissented so far as to recommend that the attempt should at least be made ; but his was a lone voice.
One of the earliest successes to be published was the case of Fioravanti (157o). There are several translations available, but Thomson's (1813) is the pithiest: " ' In that time when I was in Africa,' says Phioravant, ' there happened a strange affair and that was this : a certain gentleman, a Spaniard, that was called I1 Signior Andreas Gutiero, of the age of 29 years, upon a time walked in the field and fell at words with a soldier and began to draw; the soldier seeing that, struck him with the left hand and cut off his nose and there it fell down in the sand. I then happened to stand by and took it up and pissed thereon to wash away the sand and dressed it with our balsama artificiato and bound it up and so left it to remain eight or ten days, thinking that it would have come to matter ; nevertheless, when I did unbind it I found it fast conglutinated and then I dressed it only once more and he was perfectly whole so that all Naples did wonder thereat as is well known, for the said Signior Andreas doth live and can testify the same. '" Scepticism, however, continued. The gospels record the incident in which the right ear of Malchus the servant of the high priest was struck off by Peter and later healed by Jesus. Panlo Zacchias (i584--I659), poet, painter, musician, the personal physician of Pope Innocent X and the founder of forensic medicine, discussed this philosophically in his treatise on miracles. He considered that, if the ear were completely detached, this was a miracle of the first order, i.e., one that could only be accomplished supernaturally. I f it were still partially attached, then it was only a second order miracle--one which could feasibly occur by natural processes. This seems a fair summing-up of the opinion of the time.
Amputation of the nose and other extremities was occasionally used as a judicial punishment. In Italy the amputated organ was not confiscated, and in I625 in Venice a criminal whose nose had just been sliced off by the executioner's sword placed it in the centre of a warm fresh loaf and brought it to a surgeon named Molinetti, who sutured it back into place. His son Antonius Molinetti (1675) and his pupil Henricus a Moenichen (1679) vouch for the successful result. In India, where this form of judicial mutilation was more common than in Europe, there appears to have been no doubt that amputated portions could be successfully replaced. Dr William Ruddiman, in a letter to Carpue (1816), says, " I t is usual for malefactors, viz. in cases of petty theft and other minor crimes, to be sentenced to have their noses cut off in the bazar, or market place, by the common chuckler, or executioner ; on which occasion, the executioners always make a point of throwing the amputated nose into the fire ; because, say they, were the offender to have possession of his nose, he would have nothing more to do than, the moment it is cut off, put it into its proper place, well secured ; where it would unite and be as good as ever again. This I have never seen done; but I have often heard it asserted as a fact by the natives."
Sancassani (173 I) is responsible for the story of Gambacurta which is so frequently mentioned in short histories of plastic surgery. It is repeated here in
EARLY FREE GRAFTING
some detail to illustrate its absurdity and the improbability that it had anything to do with free grafting. Gambacurta was a female charlatan in Florence who sold a balsam alleged to have marvellous healing properties. To demonstrate these, she cut off a large piece of flesh from her thigh, placed it on a plate, and showed it throughout the assembled audience ; it was then put back on her leg with an application of the balsam. By the following evening, healing was complete, with hardly a trace of the wound. This stretches credulity too far, and is obviously an example of legerdemain, and not of transplantation. Baronio ~I8O4), commenting on this tale, gives a rather more plausible account of a similar quack in Rovate, a small village in Brescia, whom he witnessed selling a balsam called dell' Armata (the Army's) which he claimed was used by the French army recently occupying this territory. The man cut himself in several places and an attendant clown stabbed him, after which the wounds were immediately healed by the balsam. Baronio was not impressed, and in saying so suggested to the charlatan that he repeat Gambacurta's procedure. This proposal was accepted and the man cut a large piece of skin and muscle from his left arm, and after showing it streaming with blood to the spectators, replaced it and medicated it with dell' Armata. Eight days later he exhibited his arm to the populace and the wound was scarcely visible. It might just possibly be true, but unfortunately Baronio's treatise on animal grafts is embellished elsewhere with flights of fantasy and he cannot be trusted.
The difficulty with the case reports of this period is the impossibility of assessing their veracity. At one extreme, one can dismiss as mythical stories of homograft replacements of noses taken from slaves or even casually-met travellers, which have been reported by Blegny, Dionis, and Dutrochet. At the other, there is the famous case of Garengeot (I73I), which aroused fierce controversy for many years after its publication.
GARENGEOT'S CASE OF THE BITTEN-OFF NOSE
" On the 26th September I724," he writes, " a soldier of the Regiment of Confi of the Company of Malide, coming out of L'I~pde Roiale, a tavern on the corner of the Rue des Deux-I~cus, had a fight with one of his companions, and in the course of this brawl was bitten in such a way that the whole cartilaginous part of the nose was removed. His opponent, feeling the piece of flesh in his mouth, spat it into the gutter and in his anger trod upon it to crush it. The soldier, being no less excited, retrieved the end of his nose and threw it into the shop of my colleague, M. Galin, while he ran after his enemy (Fig. I). During this time, M. Galin examined the nasal tip which had just been thrown into his shop, and since it was covered with filth he washed it at the fountain.
" The soldier came to have himself treated and some wine was warmed to cleanse the wound and his face which was covered in blood ; the nose was put in the wine to warm it a little.
" A s soon as the wound was cleansed, M. Galin adjusted the nose to its natural position and kept it in place by an agglutinative plaster and tapes. From the following day, union appeared to occur and I dressed it myself on the fourth day at M. Galin's place and saw the end of the nose perfectly united and cicatrised. ''1
The contemporary reviewers of Garengeot's book expressed astonishment but not incredulity at this report but it was not long before a certain Monteaulieu,
1 Author's translation.
B R I T I S H JOURNAL OF P L A S T I C SURGERY
under the pseudonym of Philippe d'Alcrippe, launched an attack on Garengeot and held him up to ridicule (Morand, I768). Others followed, and as Percy and Laurent wrote in 18 I9, " One cannot name this surgeon to-day without immediately
FIG. I
" The soldier, being no less excited, retrieved the end of his nose and threw it into the shop . . ." (Garengeot, I73L)
thinking about what has been called 'h is s tory ' and exposing him to further railleries which seem to have effaced all he accomplished for science." Nevertheless the story was included in the second edition of an already popular textbook which had no need of added sensationalism. It seems inconceivable that two surgeons,
EARLY FREE GRAFTING
both established and of good reputation, would lightly jeopardise their careers by perpetuating in this way a fictitious account. 1
It is difficult to separate fact from fiction in pre-nineteenth century literature because of the inadequate clinical details which are given. Throughout this period the feeling seems to have been one of general scepticism with, now and then, traces of revived belief at an occasional reported success. After the turn of the century medical reporting was more accurate and detailed, and with the publication of Balfour's work in Edinburgh in 1814 the possibility of tissue replacement became much more generally accepted. Balfour, well aware of the scorn poured on previous reports, had taken the precaution of having affidavits sworn before a Justice of the Peace to verify the successful outcome.
BALFOUR AND THE EDINBURGH CARPENTER'S FINGER
George Pedie, a house carpenter, cut off part of his left index finger with a single blow of a hatchet on ioth June I814, and was brought by a fellow workman to Dr William Balfour to have the wound dressed. Dr Balfour some years before had replaced on his own son the tips of three fingers which had been almost completely amputated in a door. The success of this venture made him ask for the amputated part, which had been left behind, and Pedie's companion was sent back for it.
The cut had passed obliquely through the second and third phalanges, the longest side of the amputated piece being one and a half inches, the shortest, one inch. It was cleansed of dirt, blood was removed from the stump, and Balfour " t h e n applied, with as much accuracy as possible, the wounded surfaces to each other expressing a confident expectation that reunion would take place." [There is no mention of sutures.--T. G.] The patient, told to attend daily, came the following day and then failed to turn up. It later transpired that he had no faith in the ability of his finger to survive and had visited another practitioner on the second day, demanding that the bandage be removed. " Thus," says Balfour, "were nearly rendered abortive, my attempts at reunion of the parts . . . but fortunately nature had been too busy for even this early interference to defeat her purpose. ADHESION HAD TAKEN PLACE."
When Balfour saw the patient next on 4th July the skin had desquamated and the nail fallen off, but the finger was" the handsomest the man has and has recovered both heat and sensation." As an addendum to his paper there are the affidavits sworn before Duncan Cowan, J.P., by the patient, the man who accompanied him, and an independent medical witness, Dr Peter Reid, who testified to having found that complete reunion had taken place. It should be remembered that at this period there was general agreement that wounds would not adhere and unite by first intention and healing by second intention was the inevitable outcome of wounding ; the case was therefore the more remarkable, and aroused great interest.
In the volume of the Edinburgh Medical and Surgical ffoumal of the following year are no less than three cases of amputated fingers in which Balfour's method had been used with success. In two of them (Hunter and Fletcher) the cut-off portion was admittedly still attached by a tiny bridge, but in Bailey's case the
1 A century after Garengeot, a very similar history was reported by Carlizzi (1834). A " woman of the town " had the soft part of her nose bitten off by a man during a quarrel. Three hours later it was successfully sutured in place. At first it was livid and unheal thy in appearance, but a chemical peeling with silver nitrate restored its natural colour.
6 BRITISH JOURNAL OF PLASTIC SURGERY
finger was completely severed through the bone of the distal phalanx. The piece was held in place with adhesive plaster, and small pieces of card were used as sprints. At the end of a week pulsation was felt at the tip ; the bone united but the patient had lost the power of bending the finger and complained of numbness in the tip. Braid in 1816 reported a similar case in the same journal, but from the description much of the amputated part appears to have died.
It would be tedious to detail the many other reported cases of severed portions of fingers being successfully re-attached (Marley, 1821 ; Houlton, 1826 ; Dubroca, 1839 ; Della Fanteria, 1842 ; Denny, 1849 ; Hartshorne, 185o ). They fall into two groups: the majority involve portions of the distal phalanx, and in recent years Douglas (1959) has shown that these will survive replacement if accurately aligned ; cases in which the wound passes through the middle phalanx are much less common and the cut then is usually oblique. I have not come across a convincing case of successful replacement after amputation through the proximal phalanx in the early literature.
HOFFACKER AND THE DUELLING STUDENTS OF HEIDELBERG
In the field of restitution of cut-off parts, there is one surgeon whose experiences must surely remain unique for all time. ~
Gottlieb Wilhelm Hoffacker (1787-I844) held at Heidelberg University the office of Paukdoctor or Paukarzt, medical attendant to the student duellists orpaukern, and his task was to treat the students' wounds and re-attach any pieces excised by the sabres. Duelling at Heidelberg then was more of a sport than a method of settling disputes, and Hirsch (I888) tells us that in twenty-four years Hoffacker attended 20,000 duels, not counting those with firearms. He had begun his studies in Heidelberg in 18IO, but two years later had volunteered for army service, and went with Napoleon on his ill-fated campaign into Russia bringing back as souvenirs a frost-bitten foot and a delicate chest. He had resumed his studies in 1818 and for some time before he qualified in I822 worked as doctor to the duellists to eke out his means. After qualification this became in a sense his " speciality" although he had in addition a flourishing practice. Unfortunately Hoffacker wrote little, and much of his vast experience died with him ; I have been able to trace only two papers from his pen and both are germane to our subject.
In 1828 he published " Observations on the Healing of Cut-off Portions of the Nose and Lips," a series of sixteen case histories from the period 1822-27. There is no introduction, no discussion, no conclusion ; the article begins with the clinical details of a " Herr D., 2I years old, strongly built, brownish- coloured face, black eyes, and thick curly hair," who on I2th May I822 had a portion of his cartilaginous nose replaced with almost complete success ; the sixteenth and last case was also largely successful, although a fifth part of the replaced nasal tip failed to survive. It is this which makes Hoffacker so convincing ; he reports impartially his successes, his partial successes, and his failures. A translation of the report of his second case will suffice to illustrate his style.
" H e r r v. B., 22 years old, tall and slim but not very strongly built, with brown eyes and hair, living a very regular life, had on 26th May 1822 the left ala of the nose, five lines (i.e., five-twelfths of an inch) broad at the base, completely cut off to the centre of the tip. The upper lip and part of the lower lip were split open to the gums by the same sword cut in a direction from left to right. In each
EARLY FREE G R A F T I N G 7
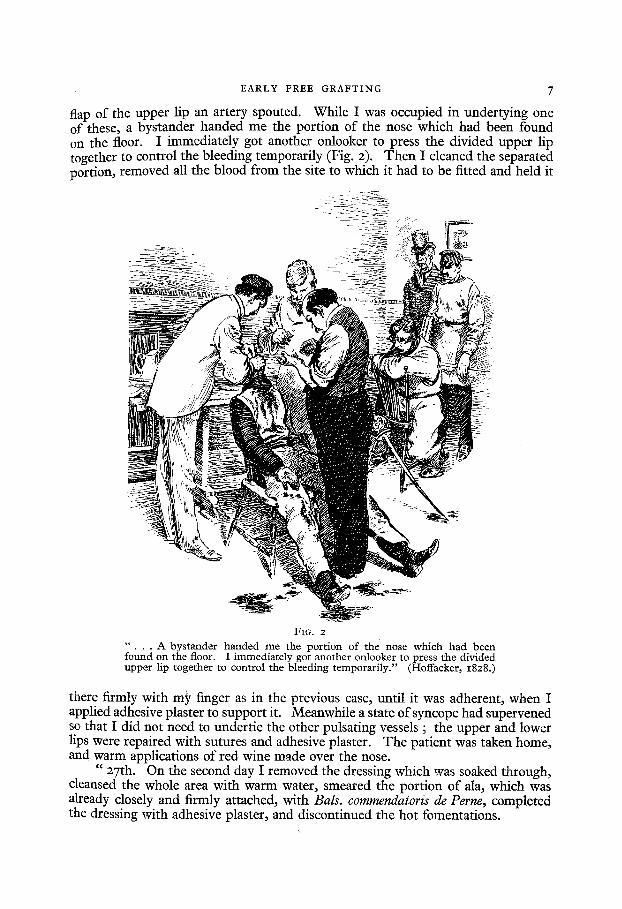
flap of the upper lip an artery spouted. While I was occupied in undertying one of these, a bystander handed me the portion of the nose which had been found on the floor. I immediately got another onlooker to press the divided upper lip together to control the bleeding temporarily (Fig. 2). Then I cleaned the separated portion, removed all the blood from the site to which it had to be fitted and held it
FIG. 2
" . . . A bys tander h a n d e d m e the por t ion of the nose wh ich had been found on the floor. I immedia te ly got another onlooker to press the divided uppe r lip together to control the bleeding temporar i ly . " (Hoffacker, z828.)
there firmly with my finger as in the previous case, until it was adherent, when I applied adhesive plaster to support it. Meanwhile a state of syncope had supervened so that I did not need to undertie the other pulsating vessels ; the upper and lower lips were repaired with sutures and adhesive plaster. The patient was taken home, and warm applications of red wine made over the nose.
"27th. On the second day I removed the dressing which was soaked through, cleansed the whole area with warm water, smeared the portion of ala, which was already closely and firmly attached, with Bals. commendatoris de Perne, completed the dressing with adhesive plaster, and discontinued the hot fomentations.
8 BRITISH JOURNAL OF PLASTIC SURGERY
" 28th. The patient had slept interruptedly, partly because of the blockage of nasal secretions and a slight burning in the wound which set in soon after dressing, and partly from headache and fever. The diet was strictly antiphlogistic, the patient having taken nothing but lemonade. When the dressing was removed the piece appeared brownish-red but very warm to the touch. I discontinued the applications of the balsam and did not reapply any dressing, recommending only rest and appropriate temperature.
"29th. The patient had passed the greater part of the night sleeping, without being disturbed by headache, fever, etc. The piece appeared very reddish brown and the surface felt hard but warm. At the margins there was some purulent discharge which, however, did not reappear after it had been removed ; also, the piece remained attached at all points, which encouraged me to hope for healing. I now took some fresh egg-yolk and some of the above-mentioned balsam, mixed them together, and had the piece frequently smeared with it.
" 3oth and 3ISt. A separation of the superficial skin was effected, and to my pleasure, underneath showed perfect vitality. Complete healing was accomplished in twelve to fourteen days." 1
The size of the detached portion in this case was nearing the possible maximum for composite-graft restoration of the ala and accords with modern experience. What is particularly noteworthy is the apparently firm adhesion which rapidly occurred when the two parts were pressed together ; no sutures were used, although some support was given by strapping.
Three of Hoffacker's sixteen cases were complete failures, three were partial failures in so far as small areas necrosed, and ten were successful, although in many the superficial skin was shed. In some instances stitches were used : in others he relied on natural adhesion plus adhesive plaster.
Hoffacker's second paper (I836) is entitled "Case History of a Severed Portion of the Nose which was Completely Detached from the Body for Twenty-five Minutes." The account at first differs little from those in the earlier series except in respect of the delay caused by three divided arteries, from which blood spurted several feet into the air ; these proved difficult to control and in the end they had to be undertied. The detached portion consisted of part of the right ala, the tip, part of the columella, and most of the left ala, and thirteen stitches "placed with the greatest precision" were used to fix it in position. There was some superficial blistering, particularly at the site of the ligatures, but the end result was good.
The importance of this article, however, lies in the discussion which follows, " A word about the behaviour of similar previous cases." He describes in less detail three successful cases in which replacement of the severed piece of nose had been delayed for thirty to forty-five minutes, and mentions " several other cases." These demonstrated that the generally held view that t he" vitality " o f an amputated portion was rapidly lost was untrue, and that vitality probably persisted for some hours. He was also convinced that there was considerable advantage in delaying re-application. Immediately after excision the raw surface of the detached portion is crumpled and shrunken, partly, he surmises, from the effect of the cutting instrument, and partly from the action of the air ; no cut blood-vessels can be seen and the portion seems too small for the defect. This state of contraction, and the continuing h~morrhage from the wound, are most important factors in preventing healing when immediate replacement is attempted. There is a much greater
Author 's translation.
EARLY FREE GRAFTING
chance of success if re-application is delayed until bleeding has ceased and the contraction has worn off so that the lymph exuding from the wound may enter the now open ends of the blood-vessels.
These are remarkable observations for that period and it seems a great pity that Hoffacker did not write more about his experiences. His two short papers
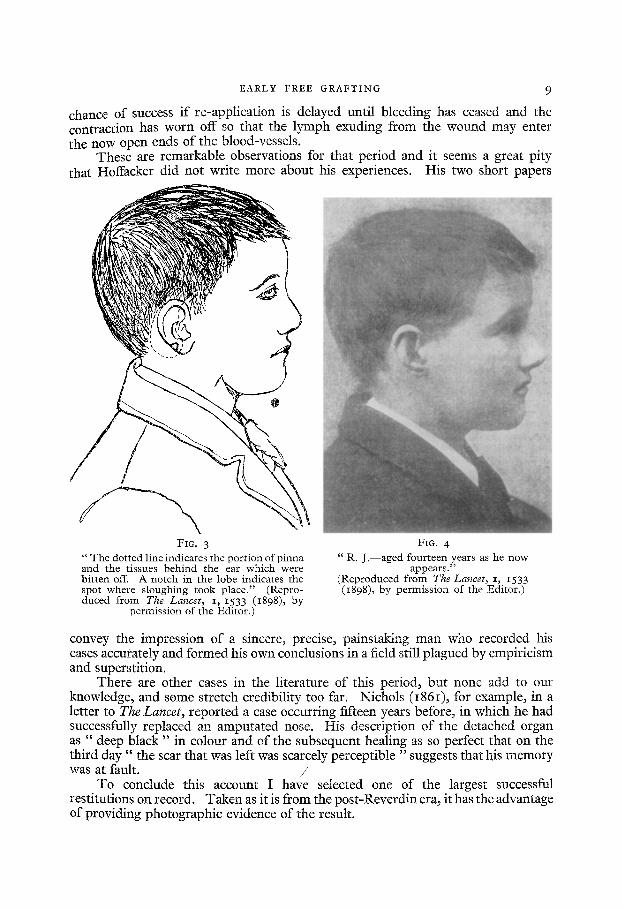
FIG. 3 " T h e dotted line indicates the portion of pinna and the tissues behind the ear which were bitten off. A notch in the lobe indicates the spot where sloughing took place." (Repro- duced from The Lancet, I, I533 (I898), by
permission of the Editor.)
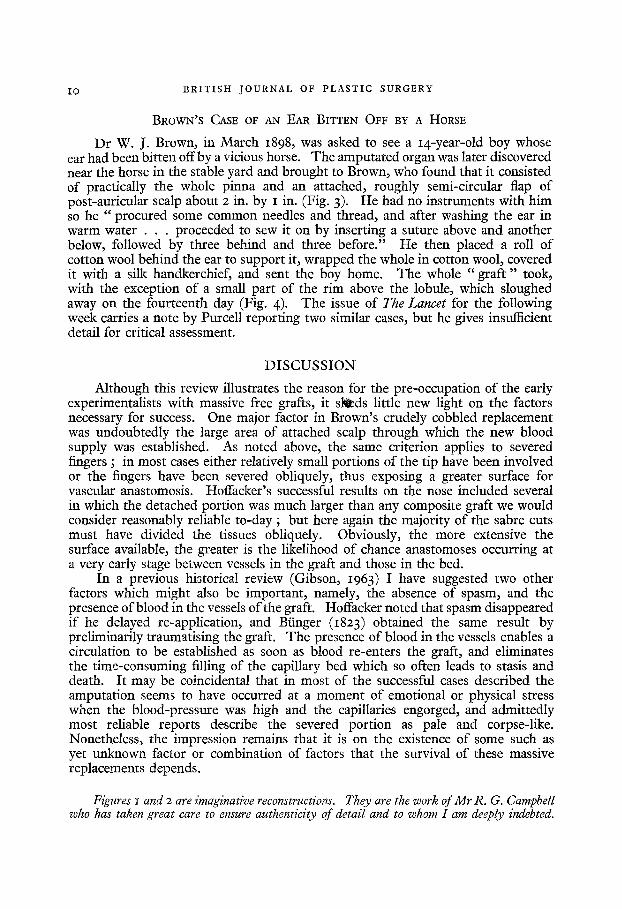
FIG. 4 " R. J . - -aged fourteen years as he now
appears." (Reproduced from The Lancet, i, 1533 (I898), by permission of the Editor.)
convey the impression of a sincere, precise, painstaking man who recorded his cases accurately and formed his own conclusions in a field still plagued by empiricism and superstition.
There are other cases in the literature of this period, but none add to our knowledge, and some stretch credibility too far. Nichols (I86I), for example, in a letter to The Lancet, reported a case occurring fifteen years before, in which he had successfully replaced an amputated nose. His description of the detached organ as " deep black" in colour and of the subsequent healing as so perfect that on the third d a y " the scar that was left was scarcely perceptible "suggests that his memory was at fault. /
To conclude this account I have selected one of the largest successful restitutions on record. Taken as it is from the post-Reverdin era, it has the advantage of providing photographic evidence of the result.
IO BRITISH JOURNAL OF PLASTIC SURGERY
BROWN'S CASE OF AN EAR BITTEN OFF BY A HORSE
Dr W. J. Brown, in March 1898, was asked to see a I4-year-old boy whose ear had been bitten off by a vicious horse. The amputated organ was later discovered near the horse in the stable yard and brought to Brown, who found that it consisted of practically the whole pinna and an attached, roughly semi-circular flap of post-auricular scalp about 2 in. by I in. (Fig. 3)- He had no instruments with him so he " p r o c u r e d some common needles and thread, and after washing the ear in warm water . . . proceeded to sew it on by inserting a suture above and another below, followed by three behind and three before." He then placed a roll of cotton wool behind the ear to support it, wrapped the whole in cotton wool, covered it with a silk handkerchief, and sent the boy home. The whole "graf t " took, with the exception of a small part of the rim above the lobule, which sloughed away on the fourteenth day (Fig. 4)- The issue of The Lancet for the following week carries a note by Purcell reporting two similar cases, but he gives insufficient detail for critical assessment.
DISCUSSION
Although this review illustrates the reason for the pre-occupation of the early experimentalists with massive free grafts, it s l tds little new light on the factors necessary for success. One major factor in Brown's crudely cobbled replacement was undoubtedly the large area of attached scalp through which the new blood supply was established. As noted above, the same criterion applies to severed fingers ; in most cases either relatively small portions of the tip have been involved or the fingers have been severed obliquely, thus exposing a greater surface for vascular anastomosis. Hoffacker's successful results on the nose included several in which the detached portion was much larger than any composite graft we would consider reasonably reliable to-day ; but here again the majority of the sabre cuts must have divided the tissues obliquely. Obviously, the more extensive the surface available, the greater is the likelihood of chance anastomoses occurring at a very early stage between vessels in the graft and those in the bed.
In a previous historical review (Gibson, 1963) I have suggested two other factors which might also be important, namely, the absence of spasm, and the presence of blood in the vessels of the graft. Hoffacker noted that spasm disappeared if he delayed re-application, and Bringer (1823) obtained the same result by preliminarily traumatising the graft. The presence of blood in the vessels enables a circulation to be established as soon as blood re-enters the graft, and eliminates the time-consuming filling of the capillary bed which so often leads to stasis and death. It may be coincidental that in most of the successful cases described the amputation seems to have occurred at a moment of emotional or physical stress when the blood-pressure was high and the capillaries engorged, and admittedly most reliable reports describe the severed portion as pale and corpse-like. Nonetheless, the impression remains that it is on the existence of some such as yet unknown factor or combination of factors that the survival of these massive replacements depends.
Figures I and 2 are imaginative reconstructions. They are the work of Mr R. G. Campbell who has taken great care to ensure authenticity of detail and to whom I am deeply indebted.
EARLY FREE GRAFTING II
REFERENCES
BALFOUR, W. (1814). Edinb. reed. surg. J., IO, 421. BARONIO, G. (I8O4). " Degli innesti animali." Milano : Stamperia e Fonderia del
Genio. BLEGNY~ N. DE (1682). " Zodiacus medico-gallicus," vol. 4. B~ID, J. (1816). Edinb. med. surg. J. , 12, 428. BROWN, W. J. (1898). Lancet, i, 1533. B~GER, C. H. (1823). ft. Chit. Augenheilk., 4, 569 • CA~IZZI, F. M. (1834-35). Lancet, x, 437. CA~UE, J. C. (1816). " Account of Two Successful Operations for restoring a Lost
Nose from the Integuments of the Forehead." London : Longmans. DELLA FANTERIA (I842). Brit. foreign med. Rev., July I842. DENNY, J. (1849). Lancet, 2, 295. DlOmS~ P. (17o8). " Cours d'op6rations de chirurgie." Bruxelles: A. Claudinot. DOUGLAS, B. (1959). Plast. reconstr. Surg., 23, 213. DU~ROCA (1839). Gaz. mdd. (Paris), p. 6Ol. DUTROCHET, H. (1817). Gaz. Santd, Paris, 35, 91. FIORAVANTI, L. (157o). " Tesoro della vita humana." Venetia : appresso gli heredi
di M. Sessa. GA~NGEOT, R. J. C. DE (1731). " Traitd des op6rations de chirurgie," 2nd ed., Tome
I I I , p. 55. Paris : Huart. GIBSON, T. (1963). Brit. J. plast. Surg., I3, 195. GuY DE CHAULIAC (Guido de Cauliaco) (1572). " Chirurgia." Lugduni: apud S.
Beraud. HARTSHOBNE, H. (185o). Amer. J. reed. Sci., n.s., 19, 112. HIRSCH, A. (1884-88). " Biographisches Lexikon." Wien and Leipzig : Urban &
Schwarzenberg. HOFrACKER, W. (1828). Heidelb. din. Ann., 4, 232. - - (1836). Medicinische Annalen, 2, 149. HOtmTON, J. (1826). Lond. reed. Reposit., n.s., 2, 258. LaNFF~ANCHI (e. 14OO). Quoted by Zacchias (1651). MARLEY, M. (1821). Lond. med. phys. J., 45, 134. MOtNICHEN, H. A. (1679). " Observationes medico-chirurgicm." Frankfurt. Quoted
by Zeis. MOLINETTI, ANTONIUS (1675). " Dissertationes anatomico-pathologica~." Venetia:
apud. P. Balleonium. Quoted by Zeis. MORAND, M. (1768). " Opuscules de chirurgie." Paris : Desprez. NICHOLS, J. (1861). Lancet, 2, 195. PERCY~ P. F., LAURENT, C. (1819). Dictionnaire des sciences mddicales, 36, 87. ~3RCELL, F. A. (1898). Lancet, I, 1616. REVERDIN (1870). Bull. Soc. Chit., Paris, 2 ser., io, 511. SANCASSANI, D. A. (1731). " Dilueidazione fisico-mediche." Roma: G. Vaccave. THEODORICUS DELLA CERVIA (1519). " Cyrurgia edita et compiiata a Domino Fratre
Theodorico episcopo cerviensi ordinis pr~edicatorum, in collectia Veneta." Venetia. Quoted by Zeis.
THOMSON, J.~(i813). " Lectures on Inflammation," p. 230. Edinburgh : Blackwood. ZACCHIAS, PAULO (I65I). " Questiones medico-legales." Editio tertia. Amstelmdami. ZEIS, E. (1863). " D i e Literatur und Geschichte der plastischen Chirurgie."
Leipzig : Engelmann.
Submitted for publication, November 1963.