-
Archives of Disease in Childhood, 1989, 64, 1570-1578
Early diet in preterm babies and developmentalstatus in infancyA
LUCAS,* R MORLEY,* T J COLE,* S M GORE,t J A DAVIS,t M F M
BAMFORD,§AND J F B DOSSETORII*MRC Dunn Nutrition Unit, and
tBiostatistics Unit, Cambridge, and Departments of Paediatrics,
*Universityof Cambridge, MHeath Road Hospital, Ipswich, and IlQueen
Elizabeth Hospital, King's Lynn
SUMMARY Few data from randomised prospective studies address
whether early diet influenceslater neurodevelopment in man. As part
of a larger multicentre trial, 502 low birthweight infantswere
assigned randomly, for a median of 30 days, to receive a preterm
formula or unfortifieddonor breast milk as sole diets or as
supplements to their mothers' expressed milk. Survivinginfants were
assessed at nine months after their expected date of delivery
without knowledge oftheir feeding regimen. The mean developmental
quotient was 0*25 standard deviations lower inthose fed donor
breast milk rather than preterm formula. In infants fed their
mother's expressedmilk, however, the disadvantage of receiving
banked milk compared with preterm formula as asupplement, was
greater when the supplement was over half the total intake, and
approached fivepoints, representing 0O5 standard deviations for
developmental quotient. Infants fed donor breastmilk were at
particular disadvantage following fetal growth retardation, with
developmentalquotients 5.3 points lower.We suggest that the diet
used for low birthweight babies over a brief, but perhaps
critical,
postnatal period has developmental consequences that persist
into infancy; infants who are smallfor gestational age are
especially vulnerable to suboptimal postnatal nutrition.
Whether early diet influences later development is akey question
in infant nutrition that has stimulatednumerous investigations in
animals and man. Mostanimal studies have been in rats, whose young
arevery immature at birth. In such experiments bothprenatal and
early postnatal malnutrition may havesignificant neurological
consequences including aserious loss of brain cells found at
necropsy,l abrain-weight deficit that usually remains after
nutri-tional rehabilitation,=5 and impaired performancein learning
tasks and visual discrimination tests.6
In human infants who have died of severemalnutrition, the total
number of brains cells hasbeen found to be reduced by 15-20%, and
by 60%in those born weighing under 2000 g,7 which suggeststhat all
low birthweight infants (whether or not theyare small for
gestational age) are especially vulner-able to poor postnatal
nutrition. Human studies onearly diet and later neurodevelopment,
however,are difficult to interpret. Much work in humansconcerns the
consequences of malnutrition in
developing countries, where poor diet is associatedwith medical
and social problems that confound anyanalysis. Thus some workers
report behavioural orintellectual benefits from dietary
supplementaionfollowing malnutrition in infancy,8 9 whereas
otherssuggest that stimulation was essential for thesebenefits.")
Evidence indicating that early nutritionmay have lasting
neurodevelopmental effects has,however, come from many other
sources. Theseinclude studies on malnutrition associated
withdisease (for instance, infantile hypertrophic pyloricstenosis,
which has been associated with laterdeficits in attention and
memory") and with theeffects of specific nutrient deficiencies (for
example,iron'2).
Nevertheless it has been difficult to conductcontrolled
randomised trials to test the hypothesisthat early diet is critical
for later neurodevelopmentin humans. We considered that the preterm
infant,born during a phase of rapid brain growth, would bean
important model for such a study; currently used
1570
copyright. on June 23, 2021 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.64.11.1570 on 1 N
ovember 1989. D
ownloaded from
http://adc.bmj.com/
-
Early diet in preterm babies and developmental status in infancy
1571
diets differ greatly in composition and randomiseddietary
assignment is practical. Furthermore a con-clusive outcome trial
would have important implica-tions for clinical management.We have
therefore conducted a prospective,
randomised five centre trial of the effect of diet onlong term
neurodevelopment in infants weighingunder 1850 g at birth. The
cohort will be followedinto adult life; the first formal follow up
was 18months after their expected date of delivery, but inthree
East Anglian centres we also examinedsurviving infants at nine
months after their expecteddate of delivery. Our findings at nine
months arereported here.
Patients and methods
All infants weighing less than 1850 g admitted to theneonatal
units in Cambridge, Ipswich, or King'sLynn over the three year
period 1982-4 wereentered into this study. Babies were excluded
only ifthey had a major congenital abnormality known toimpair
growth or development (for example,trisomy), or if they died before
randomisation(within the first 48 hours). Approval was obtainedfor
the study from the local ethics committee in eachof the trial
centres. An important aspect of thisstudy is that after detailed
explanation of the studyto the guardian(s), consent for the infant
to takepart was never withheld, so that there was noselection bias
in the cohort.
Each mother was asked whether or not she wishedto provide
expressed breast milk for her infant. If amother chose not to
provide her milk, the infant wasrandomly allocated either banked
donor breast milkor preterm formula as the sole diet (trial 1).
Infantswhose mothers elected to provide breast milk wererandomly
allocated (trial 2) either banked donorbreast milk or preterm
formula as a supplement tobe used when mothers were unable to
providesufficient milk to meet their infants' enteral feedvolume
requirements. The median intake of mater-nal milk in this
'supplement trial' was 53% of theinfants' feed volume during the
study. Randomisa-tion, by permuted blocks of variable length,
wasstratified by centre and birth weight; infants whosebirth weight
was below 1200 g were randomisedseparately. Full details of the
randomisation, feedingregimens, and preterm formula composition
havebeen published elsewhere,'13 but briefly, the pretermformula
contained 2 g protein, 0-335 MJ (80 kcal),35 mg phosphorus, 70 mg
calcium, and 45 mgsodium 100 ml. Before the start of the study in
1982all infants in the three centres were fed on humanmilk (banked,
or mothers' own, or a combination).
Extensive data were collected on obstetric, fetal,
and neonatal factors. The Registrar General's classi-fication
was used to code social class'4; birth rank isthe infant's birth
order in the living children of thefamily, infants from multiple
births being assignedequal rank.The assigned diet was discontinued
at the time of
discharge from the neonatal unit or when a weight of2000 g had
been attained. After discharge from theneonatal unit mothers fed
their infants as they andtheir local advisers chose.
Children were invited for follow up examinationnine months after
their expected date of delivery.The median age at follow up was
40-4 weeks (lowerquartile 39-6, upper quartile 41.7). Full history
andphysical examination were undertaken by RM inCambridge and
King's Lynn, and by MB in Ipswich.Knobloch et al's developmental
screening inven-
tory was given to each child to assess five fields ofbehaviour:
adaptive, gross motor, fine motor, lan-guage, and personal-social.
15 For each field aquotient adjusting for prematurity was
calculated asfollows: observed maturational age divided byattained
age from expected date of delivery multi-plied by 100; an overall
developmental quotient wascalculated as the mean of the five scores
for eachsubject. It should be emphasised that the assessmentat this
and subsequent periods was done with theassessor having no access
to data on previous dietaryassignment.
In addition to developmental testing, the infantswere assessed
neurologically by the same examinerwith the method described by
Amiel-Tison andGrenier.'6 Infants were categorised as
neurologic-ally normal, equivocal, or impaired. The tests
layparticular emphasis on abnormalities in tone in thediagnosis of
neurological impairment. Although 18month developmental data are
not reported here,we have included the assessment of
neurologicalimpairment that was made at 18 months with thesame
tests.Developmental scores for neurologically impaired
infants can be a poor measure of their intellectualdevelopment,
as many test items require manipula-tive skills appropriate for
age. Results have there-fore been analysed separately for infants
diagnosedas being impaired at nine months. Statistical analysiswas
by Student's t test; results are also shown as95% confidence
intervals. Tests for interaction wereperformed to determine whether
the dietary effecton development differed significantly between
con-trasting subgroups (for example, boys comparedwith girls, or
small compared with appropriate sizefor gestational age). The
significance of this inter-action was assessed by comparing the
differences indietary effect between two subgroups, again
byStudent's t test.
copyright. on June 23, 2021 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.64.11.1570 on 1 N
ovember 1989. D
ownloaded from
http://adc.bmj.com/
-
1572 Lucas, Morley, Cole, Gore, Davis, Bamford, and Dossetor
Results
Altogether 502 infants were enrolled in this study.The mothers
of 343 (68%) chose to provide theirbreast milk, those of 159 (32%)
elected not to do so.Table 1 shows the mortality before nine
monthsafter the expected date of delivery, and the demo-graphic and
clinical details of surviving infants ineach group who were
successfully followed up at thisage. Fifty nine surviving children
were not seen;seven had moved overseas, nine refused follow up,and
43 were either untraced or unable to keep theirappointment (47 of
these 59 were subsequently seenat 18 months, when 96% of survivors
were seen).There were no significant differences between
feed groups in follow up rate, mean length ofgestation, birth
weight, size for gestational age, sexdistribution, Apgar score at
five minutes, theproportion of infants requiring mechanical
ventila-tion for 24 hours or more. social class, mother'seducation,
or the infant's birth rank (data for a
selection of these factors are shown in table 1). Themedian
number of days (lower and upper quartile)to discontinuation of the
assigned diet for infants feddonor milk (as sole diet or
supplement) were 31 (22,49), and the corresponding values for
infants fedpreterm formula were 28 (19, 40). There was
nosignificant difference in the percentage of supple-ment received
between infants fed formula or donormilk, 43-8% compared with
51-3%, respectively(SD 36%).The numbers of infants in each group
diagnosed
as neurologically normal, equivocal, or impairedare shown in
table 2. There are no significantdifferences in the incidence of
neurological impair-ment.
Table 3 shows mean developmental scores for allfive fields of
development and for overall develop-mental quotient in the
randomised comparisons.These data do not include scores for
neurologicallyimpaired infants, which are considered
separately.When the two trials were combined the infants
Table 1 Comparisoni of preterm7 infants randomlY assignied to
recei'e baniked breast milk or preterm formula as solediet or as
supplemenits to their mnothers' milk
As sole diet
Baniked breast Preteonlmwilk fo nls7 (1
As sutpplemlentt to their mothers' milk
Ban,ked breast Pretermnmnilk fornula
No randomisedNo who died before the age of 9 months*No (%) seen
nine months after the
expected date of delivervCharacteristics of infants seen at ninc
months:Mean (SD) gestational age (weeks)Mean (SD) birth weight
(g)No (%) weighing I dayMedian (quartiles) No of days to full
feeds
837
66/76 (87)
312 (2X8)1392 (298)18 (27)24 (36)31 (47)14 (21)27 (41)6
(5.8)
769
17012
56/67 (84)
30S8 (2X8)1364 (300)17 (30)20 (36)26 (46)14 (25)27 (48)9
(6.16)
140/158 (89)
30(9 (2-7)1385 (297)36 (26)37 (26)75 (54)49 (35)51 (36)6
(5.9)
17315
138/158 (87)
30 9 (2-4)1386 (275)38 (28)49 (36)84 (61)54 (39)55 (40)8
(6.10)
*Fifteen of the 43 deaths occurred before enteral feeds had been
started. ,birth weight less than 10th centile.
Table 2 Neurological status, at nine months and at 18 months
after the expected date of delivery assessed withoutknowledge of
the feeding regimen by the methods of Amnel-Tison and Grenier16
As sole diet As supplement to their mother's mnilk
Banked breast Pretermn Banked breast Pretermnmilk formula milk
formnula
Total assessed for impairment 66 56 140 138At nine months:
Impaired 4 8 7 12Equivocal 0 1 8 3Total 4 9 15 15
Impaired at 18 months 4 7 11 10
copyright. on June 23, 2021 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.64.11.1570 on 1 N
ovember 1989. D
ownloaded from
http://adc.bmj.com/
-
Early diet in preterm babies and developmental status in infancy
1573
Table 3 Developmental scores at nine months after the expected
date ofdelivery for infants born preterm who had beenrandomly
assigned during the early weeks after birth to receive banked
breast milk orpreterm formula as: sole diets orsupplements to
mothers milk (trials 1 and 2 combined); as sole diets (trial 1); or
as supplements to their mothers' milk(trial 2). Data include
overall developmental quotient and scores forfive individual fields
ofdevelopment, expressed asmean (SD) with 95% confidence intervals
for benefit from preterm formula
Banked Preterm Difference-95%breast milk formula confidence
interval
Trials 1 and 2 combined:No of infants 195 174Overall
developmental quotient 97-9 (9-6) 100-4 (10-7) 0-4 to 4-6**Adaptive
101-3 (11-1) 104-0 (11-6) 0-4 to 5-1**Gross motor 99-9 (17-2) 102-3
(17-7) -1-2 to 5-9Fine motor 96-6 (12-2) 99-2 (13-5) 0-0 to 5
3*Language 93-3 (10-0) 95-6 (12-4) 0-0 to 4-6*Personal-social 98-0
(11-4) 100-6 (12-6) 0-2 to 5-1*
Trial 1-Banked milk compared with preterm formula as sole
diets:No of infants 62 48Overall developmental quotient 97-2 (8-5)
98-2 (II 0) -2-7 to 4-8Adaptive 99-5 (10-2) 101-6 (10-5) -1-8 to
6-0Gross motor 98-9 (16-2) 98-7 (15.2) -6-2 to 5-6Fine motor 95-2
(11-0) 97-1 (14-5) -3-1 to 6-8Language 93-8 (11-0) 95-2 (15-0) -3-7
to 6-4Personal-social 98-5 (8.5) 98 5 (11-0) -4-7 to 4-6
Trial 2-Banked milk compared with preterm formula as
supplements:No of infants 133 126Overall developmental quotient
98-2 (10.1) 101-2 (10-5) 0 5 to 5.6**Adaptive 102-1 (11-4) 105-0
(11-9) 0-0 to 5.7*Gross motor 100 4 (17.7) 103-7 (18-4) -1-2 to
7-7Fine motor 97-2 (12-8) 100-0 (13-1) -0-3 to 6-0Language 93-1
(9-6) 95 8 (11-3) 0-1 to 5.3*Personal-social 97-7 (11-6) 101-5
(12-2) 0-8 to 6.6**
Data from infants with neurological impairment are excluded here
and reported separately in the text (*=p
-
1574 Lucas, Morley, Cole, Gore, Davis, Bamford, and Dossetor
infants. In this 'supplement trial', however, mothersprovided
varying proportions of their infants' milkvolume requirements. When
mothers provided mostof the infants' feed volume, the nature of
therandomly assigned supplement could not be ex-pected to make a
major difference to outcome. Thusany difference in outcome between
donor milk andpreterm formula given as supplements to maternalmilk
would be blunted. We planned in advancetherefore to analyse the
results separately for infantsof mothers providing up to half of
the enteralintake and those whose mothers provided more thanhalf.
As expected, developmental advantages forinfants given preterm
formula rather than bankedmilk were greater for those infants where
thesupplement comprised more than half of their milkvolume
requirement, with a 4 9 point advantage indevelopmental quotient
for those receiving the for-mula rather than donor milk (101-4 (SD
10-5)compared with 96*5 (9.9), p
-
Early diet in preterm babies and developmental status in infancy
1575
Size appropriate forgestational age
(n 1;33) rin 106)
I i
;irls
(rn 93) (n 77)
:95: C:z 1-6 to 4171lVentilated < 24 hours
(n --1 l 5) (n=99)
T
(95% Cl -0-8 to 4-3)
Banked Pretermbreast formulamilk
Small for gestational age
(rl 62) /n 68)
II(95% Cl 2.0 to 8-6)
Boys
(n 102) (n-97)
1 (95% Cl 0-4 to 6-1)
Ventilated B 24 hours
(n=80) (n=75)
31
(95% Cl 0-1 to 7-4)
Banked Pretermbreast formulamilk
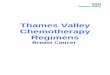
Fig 2 Mean developmental quotient at nine months afterthe
expected date ofdelivery in preterm infants randomlyassigned to
receive either banked breast milk or pretermformula as sole diets
or supplements to their mothers' milk.Values shown as mean (SEM)
and 95% confidence intervals(CI) are given for the differences: (a)
size appropriate forgestational age (left), and smallfor
gestational age (right);(b) girls (left), and boys (right); and (c)
ventilated
-
1576 Lucas, Morley, Cole, Gore, Davis, Bamford, and Dossetor
found that the diet assigned during the early weeksafter birth
had a significant effect on developmentalstatus nine months after
the expected date ofdelivery. Infants fed a special cows' milk
basedpreterm formula, had a significantly higher
overalldevelopmental quotient (when assessed by someonewho was
unaware of the randomisation) than thosefed banked donor breast
milk, when these dietswere used alone and in combination with
mothers'expressed milk. Though preterm formula feedingwas
associated with particular advantages in certainfields of
development and subgroups of infants, inno specific instance was
there any advantage fordonor breast milk. These data have
importantbiological implications and are pertinent to the
longstanding debate on whether unfortified maturehuman milk meets
the nutritional requirements ofpremature babies.13The developmental
screening inventory of Knob-
loch et al that was used in this study consists ofselected items
from the Gesell developmentalschedules.16 When Gesell developmental
quotientand Stanford-Binet intelligence quotient at schoolage are
compared, the Pearson correlation coeffi-cient (r) is 0 70, rising
to 0-84 after weighting forsocioeconomic state and incidence of
convulsiveseizures.'6 We expect that the correlation betweenmean
development quotient and later mean intelli-gence quotient in
randomised groups may be evenbetter than correlations based on
individuals. Thelonger term significance of our findings, however,
isto be assessed at future follow up throughoutchildhood and
beyond.
In trial 1, banked milk and preterm formula wereassigned
randomly as sole diets; in trial 2, they weregiven as supplements
to the mothers' expressedbreast milk (in volumes according to
maternalsuccess in providing sufficient milk to meet theinfants'
total feed volume requirement). Because inboth trials the dietary
assignment was random,demographic and clinical factors other than
dietwere equally represented between the two groups.Moreover, the
combination of trials 1 and 2 was abalanced addition so that banked
milk (as sole dietor supplement) compared with preterm formula
(assole diet or supplement) was still a randomisedcomparison.We
suggest that the observed significant differ-
ences in developmental scores between randomiseddiet groups are
biologically important. Unlike in-telligence quotient, the overall
standard deviationfor developmental quotient at nine months was
only10 points. In the whole cohort the overall disadvan-tage in
developmental quotient on donor milk was0-25 SD and in several
major subgroups (see below)this disadvantage was 5 to 8 points
(>0.5 SD).
Although other factors (such as very low gestationalage or
severe respiratory disease) are associatedwith larger differences
in developmental status atthis age, diet is one of the few
potential influenceson development that can be manipulated in
clinicalpractice.Given that donor breast milk conferred a later
developmental disadvantage overall, it was surpris-ing that no
significant differences were found in thecomparison of banked donor
breast milk or pretermformula as sole diets (trial 1). This was the
smaller ofthe two trials, however, and the trend was
generallytowards a reduced developmental quotient on donormilk. The
randomised comparison between donormilk and preterm formula as
supplement tomother's milk, based on a much larger sample,showed a
significant developmental disadvantagefor the infants fed on donor
breast milk. In infantswhose mothers provided their own milk,
thedevelopmental disadvantage for those receivingdonor milk rather
than preterm formula as asupplement was greater when the intake of
supple-ment was more than half the feed volume require-ments. This
'dose response' association furthersupports the evidence for an
early dietary effect ondevelopment.
In addition to effects of diet on overall develop-mental
quotient, the randomised groups (trials 1plus 2) differed
significantly in performance on fourof the five individual
subscales (adaptive, finemotor, language, and personal-social
skills) but notin gross motor skills. The standard deviation on
thegross motor score, however, was large (table 3),suggesting that
preterm infants are selectivelydamaged in this respect, and a large
populationwould have been required to detect a diet
relateddifference in this subscale. Nevertheless, grossmotor scores
were significantly influenced by diet ininfants born with retarded
growth.
Prenatal and neonatal malnutrition have eachbeen shown to be
associated with a 15% reduction inthe total number of brain cells
in rats; yet when'doubly deprived', with both prenatal and
postnatalmalnutrition, they suffered a 60% reduction in thetotal
number of brain cells by the time of weaning.'7Though such data
have uncertain relevance to man,we speculate that the infants in
this study who weresmall for gestational age could be regarded
asdoubly deprived if, after intrauterine growth re-tardation, they
were then fed an 'unfortified' dietsuch as banked breast milk (as a
sole diet orsupplement to maternal milk). Our previousstudies'3
have indicated that human milk did notsupport intrauterine rates of
somatic or head growthduring the neonatal period, even in infants
ofnormal birth weight, and certainly did not provide
copyright. on June 23, 2021 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.64.11.1570 on 1 N
ovember 1989. D
ownloaded from
http://adc.bmj.com/
-
Early diet in preterm babies and developmental status in infancy
1577
adequate nutrition for catch up growth in mostof the infants
born *after growth had beenretarded.The significant interaction
between diet and fetal
growth retardation for developmental outcome indi-cates that
infants in whom growth is retarded areespecially vulnerable to
postnatal undernutrition.Preterm formula fed infants had similar
develop-mental quotients whether they were small or ofappropriate
size for gestational age, whereas infantsfed donor milk were at a
significant disadvantage ifthey were in the small for gestational
age subgroup(fig 2(a)). Thus our data indicate that even withmodern
neonatal care, with emphasis on providingearly nutrition, some
available dietary regimens(especially when fed to neonates who are
small forgestational age) may not permit achievement of
fulldevelopmental potential in infancy.
Smart points out that in animal studies onundernutrition the
effects on subsequent growth andbehaviour are generally more
pronounced in malesthan in females. '8 Interestingly, we showed
agreater dietary association with development inmale children.
Furthermore, sick infants who wereventilated for more than 24 hours
showed a greaterdisadvantage on donor breast milk than
thosereceiving minimal or no ventilatory assistance. Forthese
differential effects on development to havemore than speculative
importance it would benecessary to show significant interactions
betweendiet and sex, or diet and ventilation. We identified ahighly
significant interaction between diet andventilation for language
development (sick ventilatedinfants on donor milk showed a 6-2
point disadvan-tage). For overall developmental quotient, how-ever,
significant interactions with diet were notidentified for either
sex or ventilation, though toexclude such effects would have
required a muchlarger number. Nevertheless, the consistency of
thedata with those in animals, together with the moreconvincing
findings in infants whose growth wasretarded, supports the view
that it is the 'vulnerable'male infant who is prenatally
malnourished, or sick,who is most severely disadvantaged if fed on
an'unfortified' diet.Our multicentre study should be viewed as
a
group of 'management trials'. They were designedto answer the
question: does the diet chosen for apreterm infant in the neonatal
unit influence longterm outcome? No attempt has been made
toinfluence dietary management in the time periodbetween discharge
from the neonatal unit and thefollow up examination. As the groups
were assignedrandomly, differences in feeding practice in
thisintervening period should not have occurred unlesspart of the
effect of the initial diet was to induce
some persistent change influencing the way the babywas
subsequently fed.Viewed solely as a management trial our study
should not be expected to provide an explanationfor any benefit
in outcome that emerged. We haveincluded a number of physiological
and behaviouralstudies within these trials and our future
analysesmay shed light on the mechanisms responsible forobserved
outcomes. It seems plausible, however,that the developmental
effects observed were adirect consequence of early nutrition,
perhaps relat-ing to an important dietary influence on early
head,and therefore brain, growth.'3 19 The explanationmight,
however, have been entirely different; forinstance, the faster
growth rate13 and hence earlierdischarge home in preterm formula
fed infants couldhave influenced the mother's behaviour towards
thechild, with consequent effects on development. Itshould be
emphasised that donor milk and pretermformula differ both in
nutrient and non-nutrientcontents; an overall advantage for preterm
formulamay represent the sum of both benefits and dis-advantages.
Whether breast milk would confer asignificant benefit over preterm
formula if fortifiedto the same nutrient content is an
importantquestion requiring a further outcome trial. Regard-less of
the mechanism, it was surprising that a briefperiod of dietary
manipulation (median 30 days)could have such prolonged
consequences. It isunlikely that a comparable period of
suboptimalnutrition in later childhood would have any
lastingclinical significance. We suggest that the weeksimmediately
after birth constitute a 'critical period'for nutritional
management.The effects of early diet on later development
shown in these infants have important implicationsfor the
dietary management of low birthweightinfants, and bear on the more
general issue ofwhether early diet has persistent
neurodevelopmentalconsequences in man. Clearly future planned
followup of this cohort will permit us to examine thesignificance
of our observations in terms of laterperformance.
We thank Dr R G Whitehead for help and encouragement, thestaff
of the special care baby units at Cambridge, Ipswich, andKing's
Lynn for their assistance and cooperation, and FarleyHealth
Products for the manufacture of the preterm formula andfinancial
and technical assistance.
References
Smart JL, Dobbing J, Adlard BPF, et al. Vulnerability
ofdeveloping brain: relative effects of growth restriction
duringthe fetal and suckling periods on behaviour and brain
composi-tion of adult rats. J Nutr 1973;103:1327-38.
copyright. on June 23, 2021 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.64.11.1570 on 1 N
ovember 1989. D
ownloaded from
http://adc.bmj.com/
-
1578 Lucas, Morley, Cole, Gore, Davis, Bamford, and Dossetor2
Stewart CA. Weights of various parts of the brain in normal
andunderfed albino rats at different ages. J Comp Neurol
1918;29:511-28.
3 Siassi F, Siassi B. Differential effects of protein-calorie
restric-tion and subsequent repletion on neuronal and
nonneuronalcomponents of cerebral cortex in newborn rats. J Nutr
1973;103:1625-33.
4 Widdowson EM, McCance RA. Some effects of acceleratinggrowth.
I. General somatic development. Proc R Soc Lond1960;152:
188-206.
5 Bedi KS, Thomas YM, Davies CA, Dobbing J. Synapse-to-neuron
ratios of the frontal and cerebellar cortex of 30-day-oldand adult
rats undernourished during early postnatal life.J Comp Neurol
1980;193:49-56.
6 Smart JL. Early life malnutrition and later learning ability:
acritical analysis. In: Oliverio A, ed. Genetics, environment
andintelligence. Amsterdam: Elsevier, 1977:215-35.
7 Winick M. Malnutrition and brain development. Oxford:
OxfordUniversity Press, 1976:115.
8 Chavez A, Martinez C. Neurological maturation and perfor-mance
on mental tests. Quoted in: Early nutrition and laterachievement.
London: Academic Press, 1987:138-9.
9 Freeman HE, Klein RE, Townsend JW, et al. Nutrition
andcognitive development among rural Guatemalan children. Am
JPublic Health 1980;70:1277-85.
"O Sinisterra L. Studies on poverts, human growth and
develop-ment: the Cali experience. In: Dobbing J, ed. Early
nutritionand later development. London: Academic Press,
1987:208-33.Klein PS, Forbes GB, Nadar PR. Effects of starvation in
infancy(pyloric stenosis) on subsequent learning abilities. J
Pediatr1975;87:8-15.
12 Ankett MA, Parks YA, Scott PH, Wharton BA. Treatment withiron
increases weight gain and psychomotor development. ArchDis Child
1986;61:849-57.
13 Lucas A, Gore SM, Cole TJ, et al. Multicentre trial on
feedinglow birthweight infants: effects of diet on early growth.
Arch DisChild 1984;59:722-30.
14 Office of Population Censuses and Surveys. Classification
ofoccupations 1980. London: HMSO, 1980.
15 Knobloch H, Pasamanick B, Sherard ES. A
developmentalscreening inventory for infants. Pediatrics
1966;38:1095-108.
6 Ameil-Tison C, Grenier G. Neurological assessment during
thefirst year of life. Oxford: Oxford University Press, 1986.
17 Minkowski A, Roux J-M, Tordet-Caridroit C.
Pathophysiologicchanges in intrauterine malnutrition. In: Winick M,
ed. Nutri-tion and fetal development. Vol 2. New York: John
Wiley,1974:45-55.
18 Smart JL. Undernutrition, learning and memory: review
ofexperimental studies. In: Taylor TG, Jenkins NK, eds.
Proceed-ings of Xlii International Congress of Nutrition.
London:Libbey, 1986:74-8.
19 Cooke RWI, Lucas A, Yudkin PLN, Pryse-Davies J.
Headcircumference as an index of brain weight in the fetus
andnewborn. Early Hum Dev 1977;1:145-9.
Correspondence to Dr A Lucas, Dunn Nutritional
Laboratory,Downham's Lane, Milton Road, Cambridge CB4 IXJ.
Accepted 1 June 1989
copyright. on June 23, 2021 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.64.11.1570 on 1 N
ovember 1989. D
ownloaded from
http://adc.bmj.com/