Embed Size (px)
Citation preview

297
Early Diagnosis of Basilar Artery OcclusionUsing Magnetic Resonance Imaging
Jos6 Biller, MD, William T.C. Yuh, MD, Galen W. Mitchell, MD,
Askiel Bruno, MD, and Harold P. Adams Jr., MD
Three patients with a clinical diagnosis of pontine infarction probably due to basilar artery occlusionwere studied with magnetic resonance imaging within 24 hours after onset or latest progression ofsymptoms. The earliest changes on magnetic resonance images were an absence of signal void in thebasilar artery suggestive of severe reduction of blood flow or occlusion (flow-void phenomena). Thepresumed basilar artery thrombosis was best demonstrated as a linear structure isointense orhyperintense with the brainstem in the pontine cistern on Tl -weighted parasagittal images and as eitherabsence of flow-void phenomena or higher signal intensity at various levels corresponding to the courseof the basilar artery on the axial T2-weighted images. Brainstem parenchyma! changes characteristicof infarction were not obvious for at least 12 hours after onset or 90 minutes after latest progressionof symptoms and were best shown by both axial and coronal T2-weighted images. Recognition of thesemagnetic resonance imaging findings may allow earlier diagnosis and treatment of acute ischemia inthe vertebrobasilar system. (Stroke 1988; 19:297-306)
Magnetic resonance imaging (MRI) appears tobe superior to computed tomography (CT)in identifying posterior circulation in-
farctions.1"7 Although a great deal of research hasinvolved the use of MRI, its ultimate role in theevaluation of patients with acute stroke is not defined.The questions of separation of the effects of ischemicnecrosis from additional changes, or the MRI distinc-tion between ischemia without infarction and edema,have not been resolved. The interval from the onset orprogression of an ischemic cerebrovascular event untilMRI shows abnormalities is not known. In particular,the usefulness of MRI in detecting lesions of < 24 hoursof age needs to be addressed. To evaluate this westudied three patients who on clinical grounds weresuspected to have an acute occlusion of the basilarartery. We evaluated the ability of MRI to detect acuteischemic lesions in patients with ischemic events in thebasilar artery territory within 24 hours after onset orlatest progression of symptoms and the sequentialchanges in location or size of vascular lesions dem-onstrated by MRI in relation to changes in CT andclinical observation.
Subjects and MethodsThree patients were studied between January and
July 1987. All had a clinical history and a physicalexamination that indicated a strong probability ofbasilar artery territory infarction of <24 hours' dura-tion. All three patients had sequential CT and MRIstudies. The number of MRI examinations was deter-mined by each patient's clinical condition.
From the Departments of Neurology (J.B., G.W.M., A.B.,H.P.A.) and Radiology (W.T.C.Y.), University of Iowa College ofMedicine, Iowa City, Iowa.
Address for reprints: Jose" Biller, MD, Division of Cerebrova-scular Diseases, Department of Neurology, University of IowaHospitals and Clinics, Iowa City, LA 52242.
Received August 14, 1987; accepted October 6, 1987.
All MRI examinations were performed with a 0.5-Tsuperconductive Picker Vista MRI system (Cleveland,Ohio). The images were obtained with parasagittalTl-weighted (repetition time, TR 350-550 msec; echotime, TE 20-26 msec), axial T2-weighted (TR2,000-2,016 msec; TE 100 msec), and coronal T2-weighted (TR 2,000 msec; TE 100 msec) pulsesequences. Slice thickness was 10 mm without gap.
The MRI criteria used to diagnose infarction werethe presence of a focus of abnormally decreased signalintensity on the Tl-weighted images and a correspond-ing area of increased signal intensity on the T2-weighted images. The MRI criteria suggestive of anoccluded basilar artery were the presence of a linearstructure isointense with the brainstem in the pontinecistern on Tl-weighted parasagittal images and ab-sence of flow-void phenomena with high signal inten-sity corresponding to the course of the artery on theT2-weighted axial images at various cuts.
CT images were obtained without infusion of con-trast, using a Siemens DRH unit (Iseline, New Jersey)and 8-mm-thick axial slices.
Results
Case 1A 50-year-old hypertensive man noted the sudden
onset of bifrontal headache, intermittent confusion,vertigo, nausea, vomiting, bilateral tinnitus, and left-sided weakness 22 hours before admission.
On admission, he had a normal mental status. Coarsenystagmus in all directions of gaze was noted as wellas a decreased left corneal reflex and bilateral weakeyelid closure. He had a left hemiparesis and lefthypesthesia.Truncalataxia was noted. UnenhancedCTwas normal.
Twenty-four hours later he developed dysarthria,dysphagia, decreased hearing on the right, bilateralhorizontal gaze palsies, and quadriparesis. MRI com-
by guest on May 27, 2018
http://stroke.ahajournals.org/D
ownloaded from

298 Stroke Vol 19, No 3, March 1988
I ft I
FIGURE 1. Parasagittal Tl-weighted magnetic resonance im-ages (repetition time, TR 483msec; echo time, TE 20 msec) ofCase 1 show linear structure(white arrows and black arrows)isointense with brainstem in pon-tine cistern suggestive of basilarartery thrombosis. Small lineararea of higher intensity due toeither slow flow or subacute in-traluminal clot (arrowhead, up-per right image) is noted.
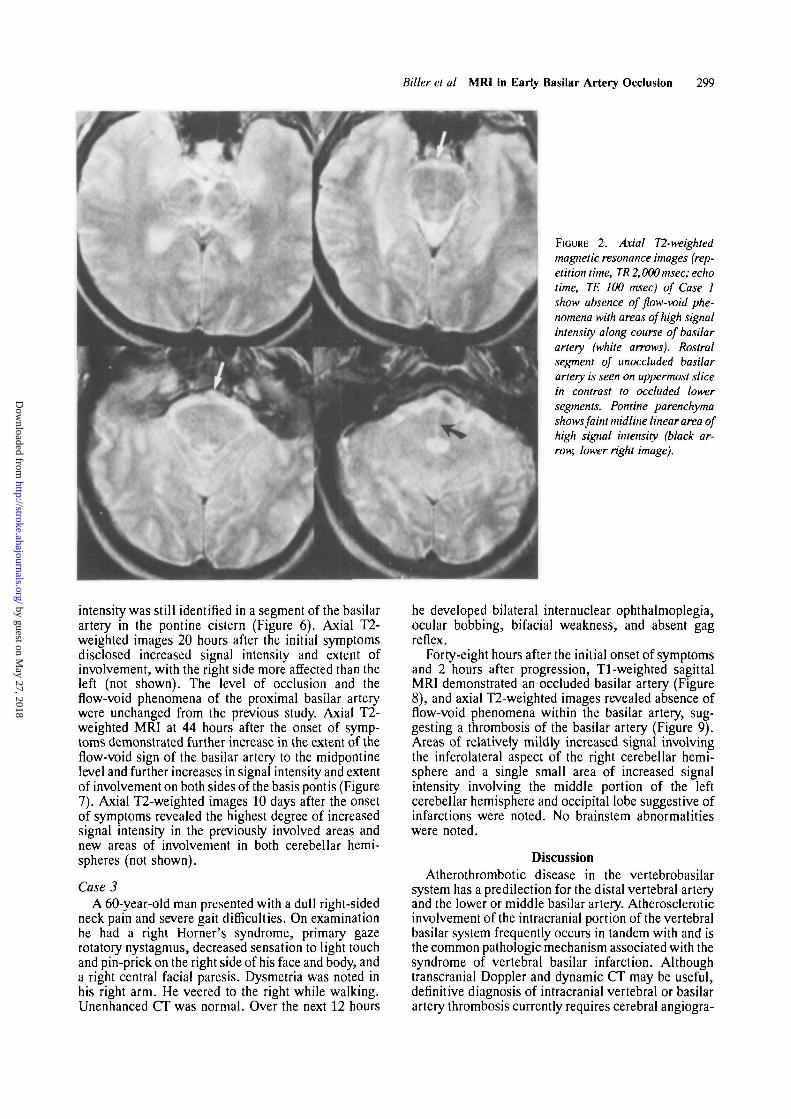
pleted within 90 minutes after the onset of neurologicdeterioration demonstrated possible thrombosis(Figure 1) and absence of flow-void phenomena in thebasilar artery suggestive of complete occlusion(Figures 1 and 2). No evidence of cerebellar or cerebralparenchymal abnormalities was noted on either Tl- orT2-weighted images. There was a faint midline high-signal-intensity area in the pons (Figure 2). This wasnoted retrospectively, only after discovering thechanges on follow-up MRI.
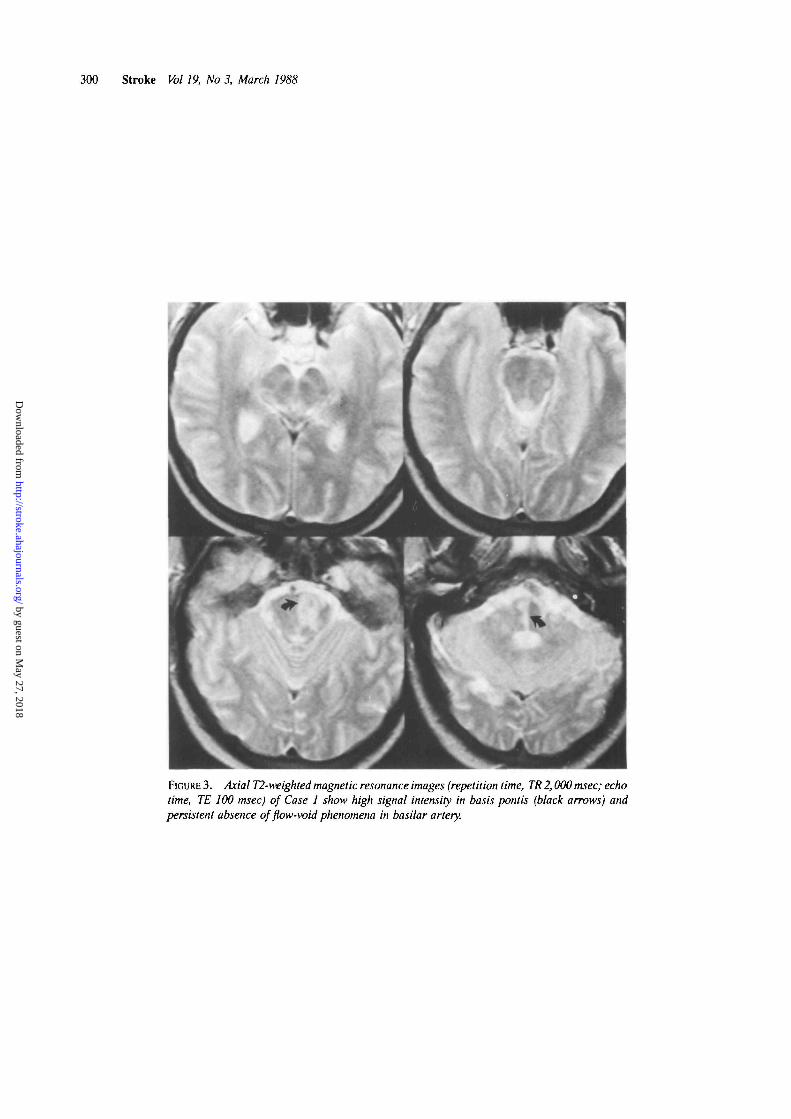
MRI obtained 3 days after initial symptoms, 2 daysafter the initial study, showed persistent lack offlow-void phenomena in the basilar artery. In addition,there was abnormal signal intensity, with the rightgreater than the left, with basis pontis involvement onboth Tl- and T2-weighted images. Collateral circula-tion was also demonstrated (Figure 3).
Case 2A 43-year-old man developed a sudden, brief, severe
occipital headache the evening before admission. Hewent to bed only to awaken 2 hours later with agitation,confusion, dysarthria, and vomiting. He presented atthe local emergency room with a very unsteady gait andwas transferred to University of Iowa Hospitals. CTwithout infusion of contrast was normal.
Upon arrival, he was diaphoretic and had a bloodpressure of 130/70 mm Hg, a regular pulse of 90/min,
a rectal temperature of 37° C, and shallow respirationsat 20/min. He required ventilatory assistance. He couldvoluntarily open and close his eyes, but he had onlyvertical eye movements in response to commands, tooculocephalic reflex testing, and to ice-water caloricstimulation. There was bifacial weakness, ocularbobbing, and absent corneal and gag reflexes. Heexhibited flaccid quadriplegia with intermittent bilat-eral extensor posturing.
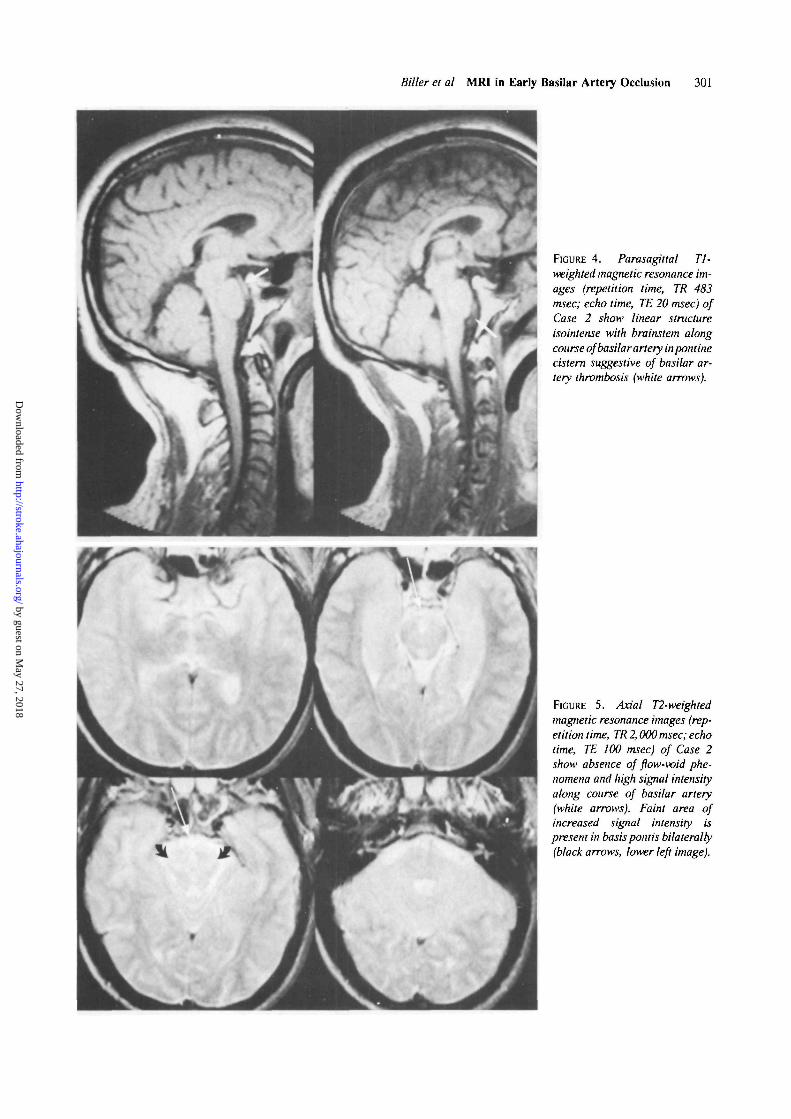
MRI obtained 12 hours after the initial symptomsdemonstrated a linear structure on Tl-weighted para-sagittal images isointense with the brainstem in thepontine cistern (Figure 4). On T2-weighted axialimages, there was absence of flow-void phenomena andevidence of high signal intensity in the pontine cisternsuggestive of an occluded basilar artery. No paren-chymal abnormalities were noted, although in retro-spect and only with the benefit of subsequent studies,a suspicious area of abnormal signal intensity involvingthe basis pontis was probably present on the Tl- andT2-weighted images (Figure 5).
Axial T2-weighted images obtained 16 hours afterthe initial symptoms showed new evidence of flow-voidphenomena near the junction of the distal vertebral andproximal basilar arteries, with persistent absence offlow-void phenomena of the rest of the basilar artery.Areas of mildly increased signal intensity were notedin the middle of the basis pontis bilaterally. High signal
by guest on May 27, 2018
http://stroke.ahajournals.org/D
ownloaded from
Biller et al MRI In Early Basilar Artery Occlusion 299
FIGURE 2. Axial T2-weightedmagnetic resonance images (rep-etition time, TR 2,000 msec; echotime, TE 100 msec) of Case 1show absence of flow-void phe-nomena with areas of high signalintensity along course of basilarartery (white arrows). Rostralsegment of unoccluded basilarartery is seen on uppermost slicein contrast to occluded lowersegments. Pontine parenchymashows faint mid line linear area ofhigh signal intensity (black ar-row, lower right image).
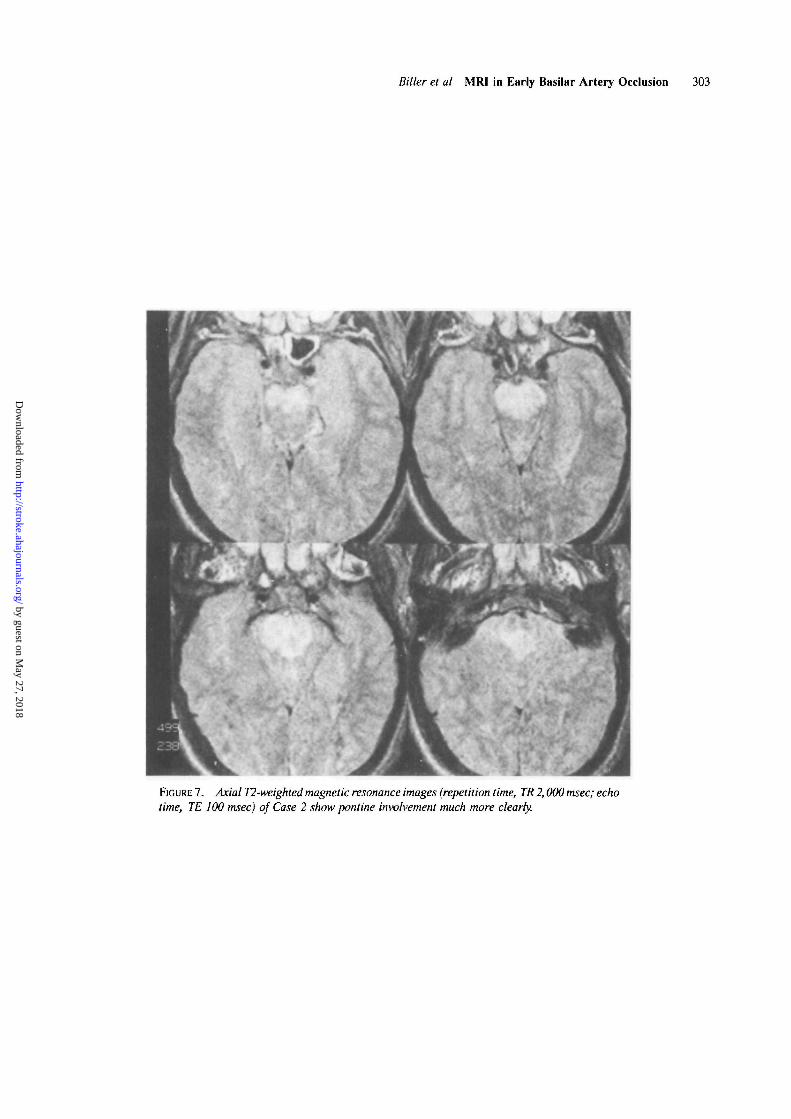
intensity was still identified in a segment of the basilarartery in the pontine cistern (Figure 6). Axial T2-weighted images 20 hours after the initial symptomsdisclosed increased signal intensity and extent ofinvolvement, with the right side more affected than theleft (not shown). The level of occlusion and theflow-void phenomena of the proximal basilar arterywere unchanged from the previous study. Axial T2-weighted MRI at 44 hours after the onset of symp-toms demonstrated further increase in the extent of theflow-void sign of the basilar artery to the midpontinelevel and further increases in signal intensity and extentof involvement on both sides of the basis pontis (Figure7). Axial T2-weighted images 10 days after the onsetof symptoms revealed the highest degree of increasedsignal intensity in the previously involved areas andnew areas of involvement in both cerebellar hemi-spheres (not shown).
Case 3A 60-year-old man presented with a dull right-sided
neck pain and severe gait difficulties. On examinationhe had a right Horner's syndrome, primary gazerotatory nystagmus, decreased sensation to light touchand pin-prick on the right side of his face and body, anda right central facial paresis. Dysmetria was noted inhis right arm. He veered to the right while walking.Unenhanced CT was normal. Over the next 12 hours
he developed bilateral internuclear ophthalmoplegia,ocular bobbing, bifacial weakness, and absent gagreflex.
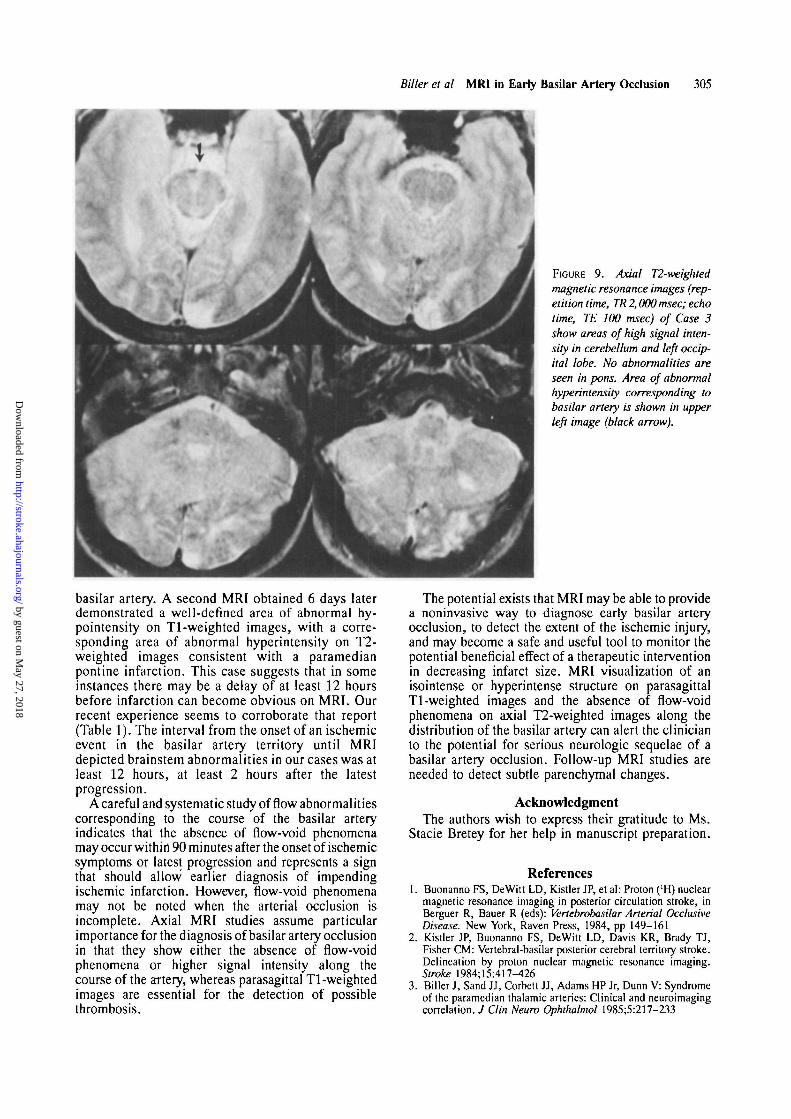
Forty-eight hours after the initial onset of symptomsand 2 hours after progression, Tl-weighted sagittalMRI demonstrated an occluded basilar artery (Figure8), and axial T2-weighted images revealed absence offlow-void phenomena within the basilar artery, sug-gesting a thrombosis of the basilar artery (Figure 9).Areas of relatively mildly increased signal involvingthe inferolateral aspect of the right cerebellar hemi-sphere and a single small area of increased signalintensity involving the middle portion of the leftcerebellar hemisphere and occipital lobe suggestive ofinfarctions were noted. No brainstem abnormalitieswere noted.
DiscussionAtherothrombotic disease in the vertebrobasilar
system has a predilection for the distal vertebral arteryand the lower or middle basilar artery. Atheroscleroticinvolvement of the intracranial portion of the vertebralbasilar system frequently occurs in tandem with and isthe common pathologic mechanism associated with thesyndrome of vertebral basilar infarction. Althoughtranscranial Doppler and dynamic CT may be useful,definitive diagnosis of intracranial vertebral or basilarartery thrombosis currently requires cerebral angiogra-
by guest on May 27, 2018
http://stroke.ahajournals.org/D
ownloaded from
300 Stroke Vol 19, No 3, March 1988
FIGURE 3. Axial T2-weighted magnetic resonance images (repetition time, TR 2,000 msec; echotime, TE 100 msec) of Case 1 show high signal intensity in basis pontis (black arrows) andpersistent absence of flow-void phenomena in basilar artery.
by guest on May 27, 2018
http://stroke.ahajournals.org/D
ownloaded from
Biller et al MRI in Early Basilar Artery Occlusion 301
Yy
FIGURE 4. Parasagittal Tl-weighted magnetic resonance im-ages (repetition time, TR 483msec; echo time, TE 20 msec) ofCase 2 show linear structureisointense with brainstem alongcourse of basilar artery inpontinecistern suggestive of basilar ar-tery thrombosis (white arrows).
FIGURE 5. Axial T2-weightedmagnetic resonance images (rep-etition time, TR 2,000 msec; echotime, TE 100 msec) of Case 2show absence of flow-void phe-nomena and high signal intensityalong course of basilar artery(white arrows). Faint area ofincreased signal intensity ispresent in basis pont is bilaterally(black arrows, lower left image).
by guest on May 27, 2018
http://stroke.ahajournals.org/D
ownloaded from

302 Stroke Vol 19, No 3, March 1988
FIGURE 6. Axial T2-weighted magnetic resonance images (repetition time, TR 2,000 msec; echotime, TE 100 msec) of Case 2 show areas of mildly increased signal intensity in basis pontis.Absence of flow-void phenomena and area of high signal intensity is again demonstrated alongcourse of basilar artery (black arrows). New area of signal flow-void phenomena is visualizedat vertebrobasilar junction (white arrow, lower right image).
by guest on May 27, 2018
http://stroke.ahajournals.org/D
ownloaded from
Biller et al MRI in Early Basilar Artery Occlusion 303
FIGURE 7. Axial T2-weighted magnetic resonance images (repetition time, TR 2,000 msec; echotime, TE 100 msec) of Case 2 show pontine involvement much more clearly.
by guest on May 27, 2018
http://stroke.ahajournals.org/D
ownloaded from
304 Stroke Vol 19, No 3, March 1988
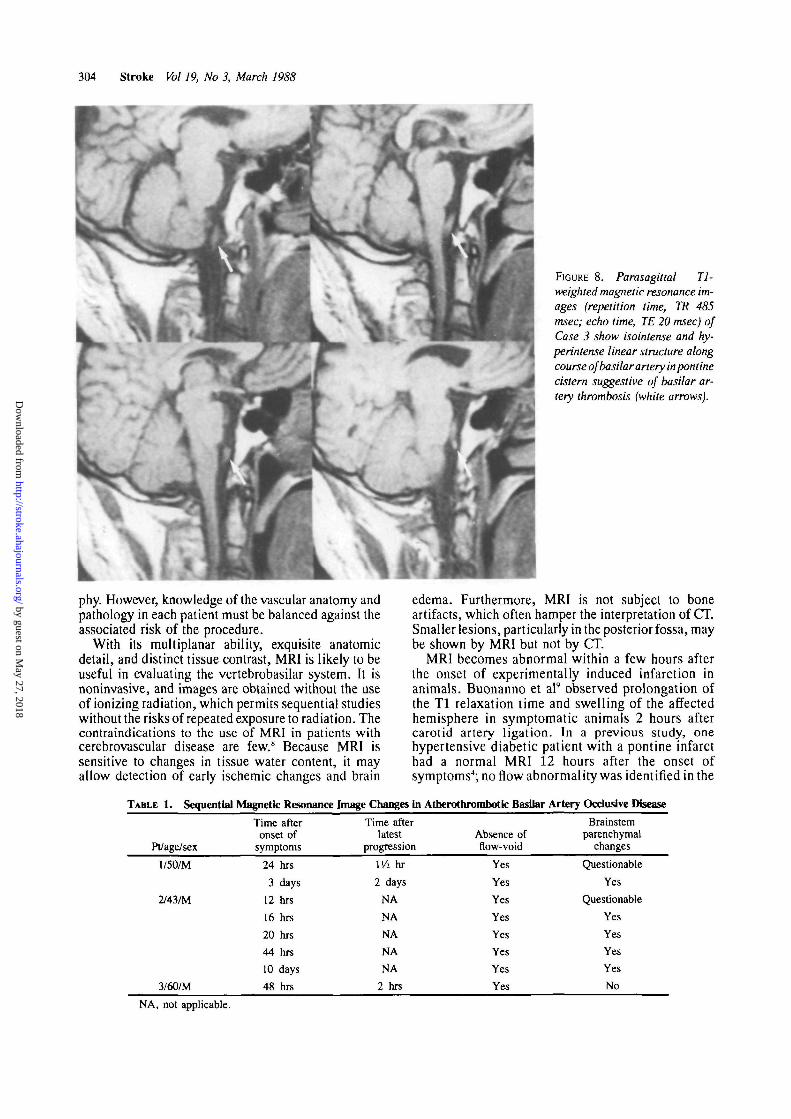
FIGURE 8. Parasagittal Tl-
weighted magnetic resonance im-ages (repetition time, TR 485msec; echo time, TE 20 msec) ofCase 3 show isointense and hy-perintense linear structure alongcourse of basilar artery inpontinecistern suggestive of basilar ar-tery thrombosis (white arrows).
phy. However, knowledge of the vascular anatomy andpathology in each patient must be balanced against theassociated risk of the procedure.
With its multiplanar ability, exquisite anatomicdetail, and distinct tissue contrast, MRI is likely to beuseful in evaluating the vertebrobasilar system. It isnoninvasive, and images are obtained without the useof ionizing radiation, which permits sequential studieswithout the risks of repeated exposure to radiation. Thecontraindications to the use of MRI in patients withcerebrovascular disease are few.8 Because MRI issensitive to changes in tissue water content, it mayallow detection of early ischemic changes and brain
edema. Furthermore, MRI is not subject to boneartifacts, which often hamper the interpretation of CT.Smaller lesions, particularly in the posterior fossa, maybe shown by MRI but not by CT.
MRI becomes abnormal within a few hours afterthe onset of experimentally induced infarction inanimals. Buonanno et al9 observed prolongation ofthe Tl relaxation time and swelling of the affectedhemisphere in symptomatic animals 2 hours aftercarotid artery ligation. In a previous study, onehypertensive diabetic patient with a pontine infarcthad a normal MRI 12 hours after the onset ofsymptoms4; no flow abnormality was identified in the
TABLE 1. Sequential Magnetic Resonance Image Changes in Atberothrombotic Basilar Artery Ocdusive Disease
Pt/age/sex
1/50/M
2/43/M
3/60/M
Time afteronset of
symptoms
24 hrs
3 days
12 hrs
16 hrs
20 hrs
44 hrs
10 days
48 hrs
Time afterlatest
progression
Wi hr
2 days
NA
NA
NA
NA
NA
2 hrs
Absence offlow-void
Yes
Yes
Yes
Yes
Yes
Yes
YfeS
Yes
Brainstemparenchymal
changes
Questionable
Yes
Questionable
Yes
Yes
Yes
Yes
No
NA, not applicable.
by guest on May 27, 2018
http://stroke.ahajournals.org/D
ownloaded from
Biller et al MRI in Early Basilar Artery Occlusion 305
FIGURE 9. Axial T2-weighted
magnetic resonance images (rep-etition time, TR 2,000 msec; echotime, TE 100 msec) of Case 3show areas of high signal inten-sity in cerebellum and left occip-ital lobe. No abnormalities areseen in pons. Area of abnormalhyperintensity corresponding tobasilar artery is shown in upperleft image (black arrow).
basilar artery. A second MRI obtained 6 days laterdemonstrated a well-defined area of abnormal hy-pointensity on Tl-weighted images, with a corre-sponding area of abnormal hyperintensity on T2-weighted images consistent with a paramedianpontine infarction. This case suggests that in someinstances there may be a delay of at least 12 hoursbefore infarction can become obvious on MRI. Ourrecent experience seems to corroborate that report(Table 1). The interval from the onset of an ischemicevent in the basilar artery territory until MRIdepicted brainstem abnormalities in our cases was atleast 12 hours, at least 2 hours after the latestprogression.
A careful and systematic study of flow abnormalitiescorresponding to the course of the basilar arteryindicates that the absence of flow-void phenomenamay occur within 90 minutes after the onset of ischemicsymptoms or latest progression and represents a signthat should allow earlier diagnosis of impendingischemic infarction. However, flow-void phenomenamay not be noted when the arterial occlusion isincomplete. Axial MRI studies assume particularimportance for the diagnosis of basilar artery occlusionin that they show either the absence of flow-voidphenomena or higher signal intensity along thecourse of the artery, whereas parasagittal Tl-weightedimages are essential for the detection of possiblethrombosis.
The potential exists that MRI may be able to providea noninvasive way to diagnose early basilar arteryocclusion, to detect the extent of the ischemic injury,and may become a safe and useful tool to monitor thepotential beneficial effect of a therapeutic interventionin decreasing infarct size. MRI visualization of anisointense or hyperintense structure on parasagittalTl-weighted images and the absence of flow-voidphenomena on axial T2-weighted images along thedistribution of the basilar artery can alert the clinicianto the potential for serious neurologic sequelae of abasilar artery occlusion. Follow-up MRI studies areneeded to detect subtle parenchymal changes.
AcknowledgmentThe authors wish to express their gratitude to Ms.
Stacie Bretey for her help in manuscript preparation.
References1. Buonanno FS, DeWitt LD, Kistler JP, et al: Proton ('H) nuclear
magnetic resonance imaging in posterior circulation stroke, inBerguer R, Bauer R (eds): Vertebrobasilar Arterial OcclusiveDisease. New York, Raven Press, 1984, pp 149-161
2. Kistler JP, Buonanno FS, DeWitt LD, Davis KR, Brady TJ,Fisher CM: Vertebral-basilar posterior cerebral territory stroke.Delineation by proton nuclear magnetic resonance imaging.Stroke 1984; 15:417-426
3. Biller J, Sand JJ, Corbett JJ, Adams HP Jr, Dunn V: Syndromeof the paramedian thalamic arteries: Clinical and neuroimagingcorrelation. J Clin Neuro Ophthalmol 1985;5:217-233
by guest on May 27, 2018
http://stroke.ahajournals.org/D
ownloaded from

306 Stroke Vol 19, No 3, March 1988
4. Biller J, Adams HP Jr, Dunn V, Simmons Z, Jacoby CG:Dichotomy between clinical findings and MR abnormalities inpontine infarction. J Comput Assist Tomogr 1986;10:379—385
5. Ross MA, Biller J, Adams HP Jr, Dunn V: Magnetic resonanceimaging in Wallenberg's lateral medullary syndrome. Stroke1986;17:542-545
6. Simmons Z, Biller J, Adams HP Jr, Dunn V, Jacoby CG:Cerebellar infarction: Comparison of computed tomography andmagnetic resonance imaging. Ann Neurol 1986;19:291-293
7. Biller J, Graff-Radford N, Smoker WRK, Adams HP Jr,Johnston P: MR imaging in "lacunar" hemiballismus. / ComputAssist Tomogr 1986;10:793-797
8. McMullough EC, Baker HLJ Jr: Nuclear magnetic resonance.Radiol Clin North Am 1982;20:3
9. Buonanno FS, Pykett IL, Vielma J, BradyTJ, Burt CT, GoldmanMR, Newhouse JH, New PFJ, Hinshaw WS, Pohost GM, KistlerJP: Proton NMR imaging of normal and abnormal brain, inWitcofski RL, Karstasdt N, Partain CL (eds): NMR Imaging.Proceedings of an International Symposium on Nuclear Mag-netic Resonance Imaging. Winston-Salem, NC, Bowman GraySchool of Medicine Press, 1982, pp 147-157
KEY WORDS • basilar artery• magnetic resonance imaging
cerebral artery diseases
by guest on May 27, 2018
http://stroke.ahajournals.org/D
ownloaded from

J Biller, W T Yuh, G W Mitchell, A Bruno and H P Adams, JrEarly diagnosis of basilar artery occlusion using magnetic resonance imaging.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1988 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.19.3.297
1988;19:297-306Stroke.
http://stroke.ahajournals.org/content/19/3/297World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 27, 2018
http://stroke.ahajournals.org/D
ownloaded from












![INDEX [link.springer.com]978-0-306-48526-8/1.pdfAcidosis, 169 Actuarial recipient survival rate, 210 ... Barbiturate overdose poisoning, 208 Basal forebrain, 233 Basilar artery occlusion,](https://img.pdfslide.us/doc/110x75/5e66ac1c8cc8791ec3325b48/index-link-978-0-306-48526-81pdf-acidosis-169-actuarial-recipient-survival.jpg)
















