Embed Size (px)
Citation preview

1
Umeå University Medical Dissertations
New Series No 1302 * ISSN 0346-6612-1302 * ISBN 978-91-7264-884-5
___________________________________________________________________________
From the Department of Clinical Sciences, Pediatrics
Umeå University, SE-901 85 Umeå, Sweden
Early Arterial Disease of the Lower Extremities in
Diabetes - Diagnostic Evaluation and Risk Markers
David Sahli
Umeå 2009

2
ISBN 978-91-7264-884-5 © Copyright: David Sahli
From the Department of Clinical Sciences, Pediatrics
Umeå University, SE-901 85 Umeå, Sweden
Printed in Sweden by Print & Media, Umeå, 2009
•

3
TABLE OF CONTENTS
ABSTRACT ........................................................................................................................................... 4
LIST OF PAPERS ................................................................................................................................. 5
SAMMANFATTNING PÅ SVENSKA ................................................................................................ 6
ABBREVIATIONS ............................................................................................................................... 8
INTRODUCTION ................................................................................................................................. 9
LOWER EXTREMITY ARTERIAL DISEASE (LEAD) .......................................................................................... 9
CLASSIFICATION AND CLINICAL STAGES OF LEAD ........................................................................................ 9
NATURAL COURSE OF LEAD ........................................................................................................................ 10
Asymptomatic LEAD ...................................................................................................................................11
Symptomatic LEAD (Intermittent claudication) ............................................................................11
Critical leg ischemia ....................................................................................................................................11
PATHOPHYSIOLOGY OF LEAD ...................................................................................................................... 12
Patients with diabetes ................................................................................................................................13
Mediasclerosis ................................................................................................................................................13
DIAGNOSTIC METHODS .................................................................................................................................. 13
RISK MARKERS AND RISK FACTORS FOR LEAD .......................................................................................... 17
Modifiable risk factors ...............................................................................................................................18
Non-modifiable risk factors .....................................................................................................................19
SCREENING, PREVENTION AND CLINICAL MANAGEMENT OF LEAD ......................................................... 20
RESEARCH QUESTIONS AND SPECIFIC AIMS ........................................................................ 21
METHODS ......................................................................................................................................... 22
STUDY COHORTS ............................................................................................................................................ 22
BLOOD PRESSURE MEASUREMENTS (STUDY I- IV)..................................................................................... 23
BLOOD AND URINE CHEMISTRY (STUDY I-IV) ............................................................................................ 25
STATISTICAL ANALYSES ................................................................................................................................. 26
SUMMARY OF RESULTS ................................................................................................................ 27
DISCUSSION ...................................................................................................................................... 28
DIFFERENT DEFINITIONS OF LEAD ............................................................................................................. 28
REPRODUCIBILITY OF ABSOLUTE BLOOD PRESSURES VS. INDICES ............................................................ 30
MODIFIED ELEVATION TEST (“POLE –TEST”) ............................................................................................ 31
NOVEL CLINICAL AND BIOCHEMICAL BIOMARKERS AS PREDICTORS OF LEAD ....................................... 31
ASPECTS ON SCREENING FOR EARLY, ASYMPTOMATIC LEAD USING TOE BLOOD PRESSURE ................. 32
CONCLUDING REMARKS .............................................................................................................. 34
ACKNOWLEDGEMENTS ................................................................................................................ 36
REFERENCES .................................................................................................................................... 37

4
ABSTRACT
The aim of the present thesis was to assess the occurrence of early lower extremity arterial disease (LEAD) in patients with diabetes and to assess novel potential risk markers for development or worsening of LEAD in the same patients. In parallel different measures of impaired peripheral circulation were evaluated.
The measurement of ankle-to- brachial blood pressure index (ABI) to screen for asymptomatic LEAD in diabetic subjects is unreliable since a large proportion of patients have stiff ankle arteries (mediasclerosis) and thus may display a too high ABI. We studied type 1-, type 2 diabetic and non-diabetic subjects without a previous history of LEAD and a composite variable of ankle – plus toe blood pressures and indices was compared to ABI alone in detecting LEAD. Significantly more subjects with reduced peripheral circulation were detected using the composite variable compared to ABI alone. This was particularly true in diabetic subjects, about 30% of whom had signs of impaired peripheral circulation. Thus, it was found that toe blood pressure measurements, alone or in combination with ankle blood pressure measurements, increase the sensitivity for finding early asymptomatic LEAD in diabetic subjects. No significant difference in reproducibility between measurements of absolute ankle- and toe blood pressure and indices was found, but a correlation between systemic (brachial) and toe blood pressure variations over time may suggest that indices are more correct in assessing peripheral arterial circulation. Furthermore, toe blood pressure measurements can be performed using either the great toe or dig II and a strong concordance is found between these measurements. In addition, since the pole-test, another non-invasive method to measure peripheral blood pressure which is less sensitive to the presence of mediasclerosis compared to ABI, correlated significantly with toe blood pressure measurements this method may be used as an alternative screening method in subjects with previously known LEAD.
Age, hypertension and glycemic control are well known risk factors and, in addition, high tissue plasminogen activator (tPA) activity turned out to be a novel early marker for asymptomatic LEAD in diabetic subjects, particularly in patients with type 2 diabetes. Age and hyperglycemia are the most important risk factors for development and progression of subclinical lower extremity arterial disease in type 2 diabetic subjects. No independent associations between markers of inflammation, such as CRP, interleukin-6 and TNF-α and early asymptomatic LEAD were seen among non-diabetic or diabetic subjects.
In conclusion, impaired arterial circulation in the lower extremities is common in diabetic subjects even in the absence of symptoms. Including toe blood pressure measurement when screening for asymptomatic LEAD in diabetic subjects improves the ability to detect reduced peripheral circulation and this method avoids falsely elevated blood pressures readings due to mediasclerosis in the ankle arteries. Moreover, an altered fibrinolytic activity should be further evaluated as an early marker of atherosclerosis and LEAD.
Keywords: Diabetes mellitus, ankle blood pressure, toe blood pressure, screening, risk markers, mediasclerosis, macroangiopathy, fibrinolysis, inflammation.
•

5
LIST OF PAPERS
I. Sahli D, Eliasson B, Svensson M, Blohmé G, Eliasson M, Samuelsson P, Ojbrandt K, Eriksson JW. Assessment of toe blood pressure is an effective screening method to identify diabetes patients with lower extremity arterial disease. Angiology. 2004;55:641-51.
II. Sahli D, Svensson M, Lidgren J, Ojbrandt K, Eriksson JW. Evaluation of simple non-
invasive techniques for assessment of lower extremity arterial disease. Clin Physiol Funct Imaging. 2005;25:129-34. Erratum in: Clin Physiol Funct Imaging. 2005;25:311.
III. Sahli D, Eriksson JW, Boman K, Svensson MK. Tissue plasminogen activator (tPA) activity is a novel and early marker of asymptomatic LEAD in type 2 diabetes. Thromb Res. 2009;123:701-6.
IV. Sahli D, Eriksson JW, Svensson MK. Age and hyperglycemia are the most important risk factors for development and progression of subclinical lower extremity arterial disease in diabetic and non-diabetic subjects - a prospective study. Submitted

6
SAMMANFATTNING PÅ SVENSKA
Diabetes innebär ökad risk för åderförkalkning (arterioskleros) i kroppens
blodkärl och kan orsaka hjärtinfarkt, stroke eller perifer benartärsjukdom (BAS). Syftet med denna avhandling var att värdera två enkla mätmetoder för att tidigt upptäcka benartärsjukdom (BAS) och undersöka olika riskmarkörer för utveckling av BAS hos patienter med diabetes
Vanligaste symptomet på BAS är smärtor i benen, ofta i samband med promenader. Patienter med diabetes har ofta nedsatt känsel i benen pga. nervskador och då kan ett fotsår vara första tecknet på BAS. Ca 1/3 av alla patienter med BAS har diabetes och risken att utveckla BAS ökar 2-4 gånger vid samtidig diabetes. Vid BAS hittar man ofta arterioskleros även i andra blodkärl och patienter med BAS har en ökad risk att insjukna i hjärtinfarkt och stroke. De flesta med BAS har inga symtom och det är därför viktigt att ta fram enkla mätmetoder för att hitta dessa patienter. Genom att upptäcka BAS tidigt skulle man kunna påbörja behandling tidigare. Dessutom skulle man hitta personer med ökad risk för annan hjärt-kärlsjukdom.
Oftast använder man blodtrycksmätning på överarmen och vid ankeln för att upptäcka BAS. Om det uppmätta blodtrycket i överarmen delat med det i ankeln, s.k. ankel-brachial index (ABI) är <0.9 ställer man diagnosen BAS. Patienter med diabetes har ofta ”förstyvad kärlvägg”, s.k. mediaskleros, i benens större blodkärl. Mediaskleros innebär att blodkärlen inte kan tryckas ihop vid blodtrycksmätning och att man då uppmäter ett blodtryck som är högre än det sanna. Hos patienter med diabetes och normalt blodtryck i benen kan därför ett falskt förhöjt ankelblodtryck uppmätas. Ännu viktigare är att en försämring av blodtrycket i benen kan maskeras. En alternativ metod att mäta blodtrycket i benen är mätning av tåblodtryck. Mätning av tåblodtryck påverkas inte av mediaskleros i samma utsträckning som vid mätning av ankelblodtryck.
I det första delarbetet mättes arm-, ankel, och tåblodtryck hos 437 personer (134-icke-diabetiker, 166 typ 1- och 137 typ 2 diabetiker). Vi jämförde en kombination av ankel-, tåtryck och index med att enbart mäta ankel-brachial index (ABI) och vi fann då en större andel patienter med nedsatt cirkulation i benen (24 och 31 % vs. 9 och 11 % vid typ 1- resp. typ 2-diabetes). Onormalt låga tåblodtryck och tå-brachial index (TBI) var vanligare än låga ankelblodtryck och ankel-brachial index hos patienter med diabetes. Tåblodtryck ensamt eller i kombination med ankelblodtryck ökar möjligheten att hitta patienter med tidig BAS.
Normalt varierar blodtrycket både i kroppen och i benen, vilket gör att man kan uppmäta olika ankel- eller tåblodtryck vid olika tillfällen. Att använda sig av blodtrycksindex i stället för absoluta blodtryck anses minska denna variation. Vi hittade ingen tydlig skillnad mellan index och absoluta tryck men eftersom vi fann ett samband mellan förändringen i system- och tåblodtryck över tid talar det ändå för att användning av blodtrycksindex skulle kunna minska variationen mellan olika mättillfällen.
Trots fördelarna med mätning av tåblodtryck lämpar sig inte denna metod för alla. Hos personer med en tjock eller kort tåbas, sår eller amputation av stortån kan det ibland vara svårt att använda en tåtrycksmanchett. I det andra delarbetet fann vi att dig II kan användas för mätning av tåtryck.
En annan metod som inte påverkas nämnvärt av mediaskleros är hydrostatisk blodtrycksmätning, den s.k. pole-test eller ”pole-pox”metoden, där patientens ben lyfts till dess att cirkulationen i foten upphör och pulsen inte längre kan registreras med en doppler penna eller pulsoximeter. Ju högre blodtryck i benet desto högre kan patientens
•

7
ben lyftas innan pulsen försvinner. Blodtrycket i tårna kan då beräknas med en formel. I andra delarbetet jämförde vi pole-test metoden med ankel- och tåblodtryck uppmätta med blodtrycksmanschett hos patienter med diabetes och känd BAS och fann då att de båda metoderna överensstämde väl och att pole-test metoden därför kan användas hos patienter med diabetes och känd BAS.
Hög ålder, rökning, diabetes, höga blodfetter och högt blodtryck är välkända riskfaktorer för att utveckla BAS . Även störningar i kroppens förmåga att lösa upp blodproppar (fibrinolys) och ökad inflammation skulle kunna öka risken att utveckla BAS. I tredje delarbetet undersökte vi om aktiviteten i fibrinolyssystemet var kopplad till förekomst av BAS. Vi fann att fibrinolysaktivteten var ökad hos patienter med typ 2-diabetes och BAS jämfört med de som inte hade BAS. Detta trots att patienter med typ 2-diabetes som grupp betraktat hade en nedsatt blodproppslösande förmåga.
I fjärde delarbetet studerade vi faktorer av betydelse för utveckling och försämring av BAS och fann att ålder och blodsockerkontroll är de viktigaste riskfaktorerna för utveckling eller försämring av tidig, symptomfri BAS bland patienter med typ 2 diabetes.
Sammanfattningsvis hittar man fler patienter med nedsatt cirkulation i benen genom att mäta tåblodtryck och detta gäller framförallt hos patienter med diabetes. Hos de patienter där stortån inte kan användas för att mäta tåtryck kan man istället använda dig II. Trots att blodtrycksindex teoretiskt borde minska variationen i mätningar mellan olika mättillfällen fann vi ingen skillnad mellan att använda index och absoluta tryck i vår studie. Den s.k. pole-test metoden är en alternativ metod att undersöka BAS hos patienter med diabetes och känd BAS. En ökad aktivitet i kroppens blodproppslösande system kan vara ett tidigt tecken på nedsatt cirkulation i benen hos patienter med typ 2 diabetes men ålder och blodsockerkontroll är de viktigaste riskfaktorerna för utveckling eller försämring av tidig, symptomfri BAS.

8
ABBREVIATIONS
ABI= Ankle brachial index ABP = Ankle blood pressure ATA= Anterior tibial artery ATP=Posterior tibial artery CHD=coronary heart disease CLI= Critical leg ischemia CVD= Cardiovascular disease IC= Intermittent claudication LEAD=Lower extremity arterial disease ND=Non-diabetic subjects PAI-1=plasminogen activator inhibitor-1 PTA = Percutaneous transluminal angioplasty T1D=Type 1 diabetic patients T2D=Type 2 diabetic patients TBI= Toe brachial index TBP = Toe blood pressure tPA=tissue plasminogen activator
•

9
INTRODUCTION
Lower extremity arterial disease (LEAD)
LEAD is often one of the first signs of a generalized atherosclerotic disease and is characterized by reduced blood pressure in the lower extremities [1]. Coronary heart disease (CHD), cerebrovascular disease (CVD) and lower extremity arterial disease (LEAD) are all manifestations of atherosclerosis and patients with intermittent claudication (IC) or critical leg ischemia (CLI) often have other atherosclerotic manifestations as well [2-5].
LEAD is common, but the prevalence varies between studies due to differences in classification of LEAD and clinical characteristics of the populations studied. In large population-based studies LEAD is present in 3-10% of adults and the prevalence increases to 15- 20% in subjects older than 70 years [6-8]. Due to a growing elderly population, an increase in the prevalence of diabetes but also as a result of better diagnostic methods and an overall improved awareness, the number of patients diagnosed with LEAD is expected to rise [9].
LEAD is a significant socio-economic burden to society and a severe impairment to quality of life in patients affected. Health care costs in Sweden due to this condition have been estimated to around 1 billion Swedish crowns (SEK) [10]. A diabetic foot ulcer leading to amputation has been estimated to cause direct costs for medical care of about 300 000 SEK [11] but a marked reduction in the number of major amputations is feasible by a multidisciplinary team approach for screening, prevention and treatment of diabetic foot problems [12].
Classification and clinical stages of LEAD
LEAD is a manifestation of atherosclerosis, thrombosis or emboli causing obstruction of the large arteries in the lower extremities. LEAD can be either asymptomatic or symptomatic. The Fontaine classification (table 1), introduced by Dr René Fontaine in 1954, was the first classification of LEAD and is still in use, dividing the disease into four clinical stages. Stage 1 includes asymptomatic patients where LEAD is verified by objective testing; i.e. absence of foot pulse, reduction of peripheral blood pressure, abnormal pulsoxymeter readings, and imaging of reduced arterial blood flow or reduced artery lumen area or clinical signs of paraesthesia or cold extremities. In stage II symptoms of intermittent claudication (pain, weakness or numbness in the muscle group distal to the diseased arterial segment) triggered by exercise evolve. Depending on how far a patient is able to walk without experiencing discomfort they are further divided into IIa (>200m) and IIb (<200m). In stage III rest pain and poor wound healing capability is present and in stage IV patients have critical leg ischemia with ulceration and/or gangrene.

10
I Asymptomatic, absence of foot pulse, ABI < 0.9
IIa Mild intermittent claudication, walking distance >200m
IIb
Moderate/severe intermittent claudication, walking distance <200m
III Daily rest pain
IV Critical leg ischemia with ulceration and/or gangrene. Focal tissue necrosis
LEAD = Lower extremity arterial disease; ABI = ankle-to-brachial index.
Table 1. The Fontaine Stage Classification of LEAD
LEAD can also be classified into non-critical and critical limb ischemia (CLI). CLI is equivalent to Fontaine stage III-IV with ischemic rest pain or ischemic skin lesions, either ulcers or gangrene. CLI is only used in chronic disease (>2 weeks of symptoms), and is not applied to acute ischemia [13].
Natural course of LEAD
Since most patients with known LEAD receive prevention or active treatment, the natural course of LEAD is difficult to study [13]. It is assumed that LEAD progresses from asymptomatic to claudication and from claudication to critical ischemia (CLI), but as many as 1/3 of the patients with CLI have had no symptoms prior to diagnosis of CLI and especially in patients with diabetes a foot ulcer may be the first sign of advanced LEAD [14]. The prognosis is correlated to the severity of LEAD, defined by walking distance before onset of claudication and by physical findings. Patients with ischemic ulcers or rest pain and diabetes or persistent smoking have the worst prognosis [15]. In a study by Leng et al only 10% of patients with asymptomatic LEAD progressed to claudication or CLI over a 5-year period [16]. 25% of patients with intermittent claudication had a worsening of symptoms and 4-7% required active treatment, i.e. revascularization or amputation [16]. For patients with CLI the prognosis is poor. At 6 months of follow-up 35 % were leg-amputated and 20% had died [17]. Smoking cessation is by far the most effective action to avoid an amputation since almost none of the patients that ceased smoking, but > 10% of those who continued were amputated. Not surprisingly, most amputations occur in the high risk group, but even so, nearly 70% remained stable or improved and altogether only 15% needed an amputation [18-20].
But, mortality rates, both overall and cardiovascular, are high in patients with LEAD. Interestingly, patients with asymptomatic LEAD have a similar increase in cardiovascular risk as those with intermittent claudication [21, 22]. The 15-year survival is low, 22 % as compared to 78 % in age-matched control subjects [17, 23]. Compared to patients with CHD or CVD those with LEAD had a similar incidence of myocardial infarction or stroke, but a higher incidence of critical limb ischemia, amputation and death [20].
•

11
Asymptomatic LEAD
The relation between asymptomatic and symptomatic LEAD is approx 4:1 [13]. The prevalence of early, asymptomatic LEAD, defined as an ABI<0.9, varies between 9-25% in different studies [8, 24, 25] with the highest prevalence in the elderly [13, 24, 26, 27]. In other studies of subjects aged 44-74 and 18-83 years, respectively, the prevalence was lower, approx 9% [6, 7, 25]. Since asymptomatic LEAD is based on the absence of subjective symptoms it is not necessarily related to the severity of atherosclerotic process but to the patient’s degree of activity.
Symptomatic LEAD (Intermittent claudication)
Pain, numbness or muscle cramps precipitated by exercise and resolved after rest, i.e. intermittent claudication, are the most common symptom of LEAD. Symptoms are often localized to the calf, but may also affect the thigh, buttocks or foot [13]. Since oxygen demand at rest remains relatively low even pronounced atherosclerotic changes give little symptoms until oxygen demand increases due to exercise [28, 29].
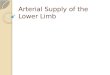
The prevalence of symptomatic LEAD varies between 2-7% in different studies [7, 8, 24, 25, 30]. Pasternak et al reported that the prevalence of intermittent claudication was 1% in the age-group 40-59 years, 4% in 60-69 years and 10% in those older than 80 years, thus showing an increase in prevalence with age [31]. A recent Swedish epidemiological study have shown an overall prevalence of symptomatic LEAD of 1.5% in subjects 50-59 years, 3.2% in subjects 60-69 years, 7.1% in subjects 70-79 years and 14.3% in subjects 80-90 years (fig 1) [32].
There are several reasons for the differences in prevalence between studies. Apart from differences in clinical characteristics between the populations studied, i.e. age, occupation, ethnicity and co-morbidities, different ways of diagnosing intermittent claudication have been used. Many studies have used questionnaires [6, 8, 13], a method that may be too insensitive since as many as 87% of patients with intermittent claudication have been reported to have atypical claudication [33]. A surprising finding in population-based studies is that between 10-50% of patients with intermittent claudication never have consulted a doctor for their symptoms [13, 34].
Critical leg ischemia
Severe LEAD and critical leg ischemia is associated with rest pain or ulceration and occurs when ABI is <0.4 or the absolute ankle blood pressure is below 50-70 mmHg or toe pressure below 30-50 mmHg [13]. The term “critical limb ischemia” is used for all patients with chronic ischemic rest pain, ulcers, or gangrene attributable to objectively proven LEAD [35]. Without any intervention 40% will have an amputation [13]. Similar to other forms of LEAD the prevalence of critical leg ischemia increases with age. In a large Norwegian population-based study the prevalence among subjects aged 40-69 years was approx 0.2% [36].

12
Fig. 1. Prevalence of different stages of LEAD at different ages in a Swedish population-based cohort.
Pathophysiology of LEAD
Atherosclerosis is characterized by plaque formation with an accumulation of macrophages (white blood cells) containing phagocyted low density lipoproteins (LDL) [37], impaired vascular endothelial function [38], aggregation of thrombocytes and disturbances in the local fibrinolytic system [39-41].
Circulating inflammatory cytokines such as TNF-α, IL-6, CRP stimulate the expression of endothelium adhesion molecules (ICAM-1, VCAM-1 and E-selectin) that promote the migration of macrophages into the sub-endothelium and endothelial intima [42]. These macrophages accumulate lipoproteins via their scavenger receptors and transform into “foam cells”. Endothelial foam cells are found in advanced stages of LEAD [43, 44]. Endothelial dysfunction is present at all stages of the atherosclerotic process. Normally, endothelial cells release several vasoactive substances including nitric oxide, prostacyclins and tissue plasminogen activator (tPA) [45] but in a atherosclerotic vessel oxygen radicals inactivate nitric oxide and inhibit prostanoid synthesis and thus acting as vasoconstrictors. Increased production of endothelin-1, angiotensin II, plasminogen activator inhibitor-1 (PAI-1) and von Willebrand factor, promotes thrombosis formation [46-48].
•

13
Initially fatty streaks evolve and, with time, an atherosclerotic plaque is formed and protrudes into the vascular lumen obstructing the blood flow. In the centre of the atherosclerotic plaque dead macrophages accumulate extracellular lipids. Covering this lipid formation is a fibrous cap with an outer layer of a thin endothelial membrane. Degenerative processes in combination with changes in “shear stress” may eventually make the plaque rupture thereby exposing the central lipid store. Without the protective endothelium, clot formation is promoted and a thrombus is formed [49, 50].
Patients with diabetes
In many chronic diseases, such as diabetes, obesity, renal failure, and smoking, various growth factors and inflammatory cytokines (IL-6, IL-1, IL-8, TNF-alpha and CRP) are released. These factors are related to an increased risk of plaque formation and rupture [51]. Hyperglycemia interferes with the endothelial production of nitric oxide (NO). NO stimulates vasodilatation, limits inflammation and platelet activation, inhibits vascular smooth muscle cell migration/proliferation and PAI-1 production, thus the loss of normal NO homeostasis may be important in inducing atherosclerosis and LEAD [52]. Fibrinolysis is reduced in type 2 diabetes [53] and hyperglycemia also increases the production of vasoconstricting substances, especially endothelin [54]. The atherogenesis of the intima (innermost part of the arterial wall), is similar to the atherosclerosis found in non-diabetic subjects but tend to develop at an earlier age and the course is often more aggressive with more distal and wide-spread lesions which may be more difficult to circumvent with by surgical means [52, 55].
Mediasclerosis
Mediasclerosis or Mönckeberg sclerosis is often found in patients with diabetes. This is a calcification of the tunica media layer of the arterial wall [56]. It commonly affects medium size muscular arteries and has been described in femoral, tibial, radial, coronary, cerebral, and visceral arteries [57].
Isolated mediasclerosis does not cause narrowing of the blood vessel [58] and the disease is usually asymptomatic [59]. Although mediasclerosis in itself seldom causes occlusion it complicates the diagnosis of LEAD since it causes the arteries to stiffen and they then gradually become more incompressible making ankle blood pressure measurements unreliable in patients with diabetes since a high proportion have stiff ankle arteries and thus may display a too high ABI [60].
Diagnostic methods
Diagnostic methods can be divided into clinical examination, non-invasive blood pressure measurements, imaging or functional diagnostic methods, microcirculation assessment, and exercise tolerance tests (see table 2). Patient history/questionnaires
Patient questionnaires used in screening for LEAD are often highly specific but only moderately sensitive, since asymptomatic LEAD is more common than symptomatic in the general population and thus, the ability to identify patients at risk of LEAD is poor. The most commonly used questionnaires are the WHO questionnaires and

14
the Edinburgh Claudication Questionnaire, an improved version of the WHO/Rose Questionnaire for use in epidemiological surveys [61].
Clinical examination
Clinical signs of LEAD are cold feet, decreased hair growth, hypertrophied/slow-growing nails, muscle/skin atrophy, absence of foot pulse and poor wound healing capacity. The TASC guidelines recommend that patients at risk for LEAD or patients with reduced limb function should have a vascular examination evaluating peripheral pulses and those patients with a history or examination suggestive of LEAD should proceed to objective testing including an ankle-to-brachial index (ABI) to confirm diagnosis [13]. Palpation of peripheral pulse is easily done and requires no extra equipment, but the examination is skill-dependent and studies have shown that even with 2 detectable foot pulses, the peripheral blood pressure can be reduced in ~10% of patients with diabetes [62, 63]. In addition, congenital absence of the dorsalis pedis pulse is found in 4-12% in the general population [63]. Non-invasive blood pressure measurements
Blood pressure can be measured at different levels but ankle- and toe blood pressure measurements are most commonly used to confirm the diagnosis of LEAD. Ankle blood pressure
Ankle-to-brachial blood pressure index (ABI) is used as an objective measure of lower extremity arterial perfusion. ABI is considered to be the “gold-standard” for non-invasive detection of LEAD [64]. ABI is painless, highly reproducible, and cost-efficient and provides strong evidence of systemic atherosclerosis and increased risk for myocardial infarction, stroke or cardiovascular death [2-4, 65]. Most epidemiological studies have used an ABI <0.9 to define LEAD [6-8, 21, 34, 63, 66-70]. This method is approx 95% sensitive in detecting arteriogram-positive LEAD and almost 100% specific in identifying LEAD in healthy subjects [13, 71].
Ankle blood pressure measurements both at rest and after exercise (walking speed until symptoms occur) may detect patients with high demands of functionality who have symptoms of claudication without having a ABI<0.9 at rest [24]. A decrease in ABI of 15–20% after exercise is diagnostic for LEAD [13].
The variability and reproducibility of ankle blood pressure measurements are observer-dependent. It has been shown that up to 30% of measurements performed by inexperienced observers lie outside the accepted range of variability (15%) for ABI measurements [72, 73]. Kaiser et al reported that the inter-observer variability among clinicians was 12%, but could be improved by training [74]. ABI is also affected by gender, choice of artery (tibialis ant/post) and choice of extremity (left/right) such that male gender, tibialis posterior and right leg giving slightly higher blood pressure readings [75].
Calcification of the media layer in the arterial vessel, i.e. mediasclerosis, with resulting non-compressible arteries should be suspected in subjects with abnormally and falsely elevated ankle blood pressure readings. The definition of incompressible arteries varies somewhat but is often defined as a systolic BT ≥250 mmHg or an ankle-to-brachial blood pressure index (ABI) >1.3 or 1.4 [35, 76]. Thus a person with manifest mediasclerosis may have an elevated or normal ankle blood pressure or ABI measurement but in fact have impairment of peripheral circulation. Patients with
•

15
diabetes and/or renal failure or heavy smokers have the highest risk of developing mediasclerosis [77, 78]. As mentioned previously, resting ABI may be insensitive for mild LEAD [79] and in order to enhance ABI sensitivity treadmill tests (6 minute) are sometimes used [80], but this test is more cumbersome for the patient and unsuitable for obese patients or patients having difficulty maintaining walking speed due to other medical reasons, i.e. arthrosis.
Toe blood pressure
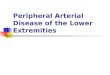
Toe blood pressure measurements are done in a similar manner as ankle blood pressure measurements. A smaller cuff suited for the toe circumference is used in combination with a pulse oximetry probe for pulse detection as shown in figure 2. The recommended blood pressure cuff-dimension has been evaluated in a recent study and found to be 2,5x13 cm [81]. Toe blood pressure readings probably better reflect the peripheral circulation in the lower extremities as they are less affected by mediasclerosis [57, 78]. The toe blood pressure is normally approx 30 mmHg less than the ankle blood pressure and a toe-to-brachial blood pressure (TBI< 0.7) indicates LEAD. The main limitation of the method is inability to fasten the toe cuff due to a short and wide toe or lesions on the great toe.
Fig. 2. Toe blood pressure measurement using a small blood pressure cuff and pulse oximetry for pulse detection.

16
Absolute blood pressures vs. blood pressure indices Usually, the arterial blood pressure is slightly higher in the legs than in the arms
[82]. A stenotic lesion causes a decrease in blood pressure distal to the lesion and will thus decrease the index between the systemic and the peripheral blood pressure. An ankle-to-brachial blood pressure index (ABI) <0.9 [70] or a toe-to-brachial blood pressure index (TBI) <0.7 [83] indicates a significantly reduced blood pressure in the lower extremities.
A single absolute peripheral blood pressure is of relatively small clinical use, instead the comparison between the systemic and the peripheral blood pressure is of importance. Microcirculatory assessments
Tissue microcirculation can be assessed by different non-invasive methods, such as capillaroscopy, laser Doppler (LD) fluxmetry and transcutaneous measurement of oxygen tension (tcPO2) [84, 85]. Studies have shown that these methods can be used to assess tissue viability and be prognostic of wound-healing (Ubbink 1999, Wahlberg 1993). Currently, these methods are used in research settings and not in clinical practice [10].
Angiography
Angiographic imaging is commonly considered as the “gold-standard”, especially prior to invasive therapy. A catheter is placed proximal to the suspected occlusion. A contrast agent is injected and the vessels are then visualized by different x-ray techniques (conventional x-ray, magnetic resonance imaging or processing computed tomography information). The extent of vessel occlusion is graded by comparing the affected vessel to adjacent non-occluded vessels. A reduced intraluminal area of 50% is considered as significant.
The invasiveness, relatively high cost, the required iodine -contrast which can induce contrast-nephropathy (especially in the elderly or diabetic patients with renal impairment), bleeding in conjunction to arterial puncture and vessel occlusion after localized injuries of the catheter on the vessel wall are the limitations with this technique. Adverse events coupled to angiography are found in approx 3% of investigations performed [86, 87]. Duplex Doppler
Duplex-Doppler is a non-invasive technique to visualize and calculate flow velocities in blood vessels. The narrowing of the artery will produce an increased flow-velocity making it possible to grade the degree of occlusion. A significant arterial stenosis increases the flow velocity 2-2.5-fold. This technique is skill-dependent with acceptable reproducibility in the hands of experienced technicians [88]. The role of duplex-Doppler has expanded as a diagnostic and preoperative method in favor of angiographic investigations [89]. Stress tests
Some patients with poor wound healing, exercise related pains or even rest pains may have a normal ABI at rest. Stein et al. showed that 1 in 3 patients with symptoms of LEAD but normal ABI at rest had a post-exercise ABI<0.9 [79]. Subsequently, in patients with atypical symptoms or a normal ABI with typical symptoms of claudication,
•

17
functional testing with a graded treadmill may help to diagnose LEAD [79]. Patients with claudication will typically exhibit a 20-mmHg drop in ankle pressure after exercise. Treadmill testing may also be used to evaluate efficacy of different treatments and assess physical function [79].
Method Cost Invasiveness
Reliability
General population
Patients with diabetes
History/ questionnaires Low No Low-Medium Low
Clinical examination with pulse palpation
Low No Medium Medium
Ankle blood pressure index (ABI)
Low No High Medium
Toe blood pressure index (TBI)
Low No High High
Microcirculatory measurement
Medium No Medium Medium
Angiography High Yes High High
Duplex Doppler High No High High
Stress tests Medium No Medium-High Medium-High
Table 2. Pros and cons of different diagnostic techniques in LEAD.
Risk markers and risk factors for LEAD
Information on risk markers and risk factors emerge from epidemiologic and clinical experimental studies of potential mechanisms. In epidemiological studies risk markers are identified as statistical associations between an outcome such as LEAD and a given variable such as smoking, blood pressure, age etc. If a risk marker can be linked to a potential mechanism involved in disease development or if altering the factor (intervention) influences the development or course of LEAD it is defined as a risk factor.
Risk factors for LEAD are similar to those for other manifestations of atherosclerosis, i.e. coronary heart disease (CHD) and stroke, but differences in impact can be detected as shown in fig. 3. For instance, smoking is a relatively stronger risk factor for LEAD as compared to CHD [13, 90, 91] and, in contrast, hypertension a relatively stronger predictor for CHD than for LEAD [13, 91]. Several studies have shown that hypertension, smoking, diabetes and dyslipidemia are the major risk factors for LEAD. A study by Selvin et al showed that 95% of individuals with LEAD (ABI <0.9) had at least one, and 70 % at least two, of these risk factors [92].

18
Modifiable risk factors
Diabetes 30-40% of all patients with LEAD have diabetes and diabetes increases the risk of
developing symptomatic LEAD 2-4-fold [93]. Glycemic control is of importance and in the UKPDS an increase in HbA1c by 1% increased the risk of LEAD by 28% [94]. No differences in risk factor pattern for LEAD were found between type 1- and type 2 diabetic subjects [95]. In Sweden, approx half of the amputations performed on the lower extremities are done in people with diabetes [96, 97]. Smoking
Smoking is the single most important modifiable risk factor for the development of LEAD [52] and several studies have shown that smoking is a strong risk factor for LEAD [24, 98-100]. Smokers present with LEAD at an earlier age compared to non- smokers and the severity of LEAD is related to the amount of cigarettes consumed [99, 101]. Heavy smokers have a 4-8-fold risk of developing symptomatic LEAD as compared to non-smokers [13]. Smoking increases the risk of atherosclerosis but is 2-3 times more likely to cause LEAD than CHD [13, 90, 91]. Hypertension
Hypertension is associated with a 2-3-fold increased risk of developing LEAD but the association is not as strong as for the development of CHD [13]. LEAD and hypertension often coincide and 50-80% of patients with LEAD have hypertension [102, 103]. Numerous studies show an association between hypertension and LEAD even when adjusting for age, smoking and diabetes [21, 104].
Elevated systemic systolic blood pressure in patients with LEAD is often due to increased arterial stiffness [105, 106]. In addition, Esteban at al showed that 15% of patients with severe LEAD also had a renal artery stenosis of > 60% but there was no difference in prevalence of hypertension between those with or without renal artery stenosis [107]. Hyperlipidemia Several studies have confirmed the relationship between dyslipidemia and LEAD. Increased triglycerides, LDL-cholesterol, total cholesterol and decreased HDL-cholesterol contribute to the development of LEAD [108-110]. The risk of developing LEAD is increases by approx 5-10% for each 10 mg/dL (0.3 mmol/L) rise in total cholesterol [75] and in the Framingham study, a fasting cholesterol level > 7 mmol/L was associated with a doubling of the incidence of IC [104]. Patients with IC generally have higher levels of total and LDL-cholesterol and lower levels of HDL-cholesterol compared to those without LEAD [109, 111, 112]. But, total cholesterol levels are often only marginally elevated. The lipoprotein profile in patients with LEAD is characterized by more prominent elevations in triglycerides and decreased levels of HDL-cholesterol [113, 114]. In addition, studies have suggested that in patients with CHD dietary and pharmacological normalization of LDL-cholesterol can slow the progression of femoral arterial atherosclerosis and reduce symptomatic claudication [112, 115, 116]. Dyslipidemia is also associated with hypercoagulability and increased platelet activity [117].
•

19
Impaired fibrinolysis Impaired fibrinolysis has been described as a risk marker or risk factor for LEAD
[118-121] and both tPA and PAI-1 mass levels have been suggested as indicators of vascular damage [120, 122, 123]. In addition, studies have indicated an association between the presence or development LEAD and an impaired fibrinolytic potential [119, 124-128]. An increase in tPA mass level and a decrease in tPA-activity have been correlated to increased severity of LEAD [119] and low levels of tPA-mass at baseline have been correlated with the development of LEAD [126]. The relationship between fibrinolytic factors and LEAD is influenced by other risk factors [122] and after adjustment for other risk factors and risk markers, i.e age, tPA-PAI-1 complex, and fibrinogen, no independent association was found between fibrinolytic factors and LEAD by Maser et al [127].
In addition to being a risk marker of vascular damage, altered or impaired fibrinolysis has also been suggested to contribute to the progression of atherosclerotic lesions [129] and it has also been shown that elevated fibrinogen levels in high risk patients with LEAD indicate an increased risk for poor outcome, particularly for fatal cardiovascular complications [54]. Inflammation
Circulating inflammatory markers (IL-6, CRP and fibrinogen) correlate to risk of cardiovascular events [130]. Plasma levels of inflammatory markers, such as CRP, are higher in patients with LEAD than in healthy control subjects and CRP seems to be a strong predictor for future development of LEAD [131]. Ridker et al. showed that CRP was elevated in subjects who later developed LEAD. The risk of developing LEAD in the highest quartile of baseline CRP was more than twice that in the lowest quartile [131]. Interestingly, studies have shown that inflammatory markers (CRP, fibrinogen, white blood cell count) increase during exercise related pain [132].
In addition, elevated plasma levels of fibrinogen may predict the future risk of death and myocardial infarction in patients with stable LEAD [133] and the severity of LEAD has been shown to increase with the level of fibrinogen [134].
Non-modifiable risk factors
In younger age-groups LEAD is more common among men [13] but this difference is not found in older subjects as postmenopausal women seem to be at equal risk compared to men [135].
Age is a well established and independent risk factor for LEAD (as previously mentioned).
Several studies have assessed the impact of ethnicity on the development of LEAD [67, 136, 137]. The Cardiovascular Health Study (CHS) showed that African-Americans have a higher risk for LEAD compared to whites even after adjusting for several other risk factors such as age, diabetes, current smoking, pack-years of smoking, hypertension, total cholesterol, HDL-cholesterol, creatinine, BMI, and forced vital capacity [138]. Other studies have found similar results [67, 139]. In contrast other studies have not found ethnic differences in development of LEAD [136, 140].
It is of interest to note that Aboyans et al found ethnic and gender-related differences in ABI also in healthy subjects and concluded that such differences, although

20
small in magnitude, are highly significant and can influence population estimates of LEAD [141].
Screening, prevention and clinical management of LEAD
Screening Studies have shown that while patients are often asked concerning cardiac
symptoms many physicians neglect asking for LEAD-related symptoms [142]. The Trans-Atlantic Inter-Society Consensus Document on Management of
Peripheral Arterial Disease (TASC)[13], recommends screening in patients who have exercise-related leg symptoms, in patients between the age of 50–69 with cardiovascular risk factors (particularly diabetes or smoking), in patients aged ≥70 years regardless of risk factor profile and in patients with a Framingham risk score >10%–20%. The Framingham risk score [143] is based on age, blood lipids, blood pressure, and presence of smoking or diabetes.
The American diabetes association (ADA) [144] recommends routine screening of LEAD in all patients with diabetes >50 years of age. Diabetes and atherosclerosis (including LEAD, CHD and stroke) share a similar risk factor profile and subsequently clinical guidelines for prevention are almost identical.
Screening in the general population is not recommended as studies show that 95% of individuals with LEAD (defined by an ABI <0.9) will have at least one, and 70 % will have at least two, of the following classical risk markers for LEAD; hypertension, smoking, diabetes and dyslipidemia [92] and thus already be eligible for prevention.
Prevention Prevention and risk factor modification includes smoking cessation, optimizing
blood glucose and lipid levels, and treatment of hypertension, but the National Diabetes Register (NDR) in Sweden have shown that only about 50% of patients with diabetes reach target levels of HbA1c or recommended lipid levels and even less (38%) have a blood pressure <130/80mmHg [145].
Clinical management In patients with diabetes and LEAD, the aim is to aggressively modify
cardiovascular risk factors, relieve symptoms of intermittent claudication, improve function, and to treat and prevent foot ulcers and thus reduce the risk of critical ischemia and tissue loss, however, studies have shown that <50% of patients with diabetes and LEAD in the United States receive treatments according to accepted and published guidelines [146].
Dedicated “diabetic multidisciplinary foot-teams” involving a diabetologist, a infectious disease specialist, a vascular surgeon, an orthopaedic surgeon, a podiatrist and a nurse specialized in foot care have reduced the number of amputations [147] . The indications for revascularization are disabling claudication or critical limb ischemia (rest pain or tissue loss) refractive to conservative therapy [52].
For asymptomatic LEAD there is no treatment recommendation beyond the preventive measures mentioned above. Exercise have been shown to be beneficial
•

21
among patients with intermittent claudication but regular training for at least three month are needed to achieve significant results [148-150].
RESEARCH QUESTIONS AND SPECIFIC AIMS
LEAD is common and prevalence is expected to rise further in the future. Patients
with diabetes are more prone to develop LEAD and the clinical consequences of LEAD in patients with diabetes are especially severe. In Sweden, half of the lower extremity amputations carried out annually is made on patients with diabetes. Not only does LEAD contribute to severe foot complications but it also reflects the state of generalized atherosclerosis serving as a potential risk marker for cardiovascular and cerebrovascular disease. At the base of all scientific research as well as for improvement and validation of clinical management lies our ability to detect, measure and quantify LEAD disease in all its manifestations.
The aim of the present thesis was to evaluate non-invasive diagnostic methods for detection of early lower extremity arterial disease (LEAD) among diabetic patients and to assess novel, potential risk markers for development or worsening of LEAD. Specific aims 1: To evaluate if the use of toe blood pressure (TBP) compared to the use of ankle blood pressure (ABP) improve sensitivity in finding lower extremity arterial disease in diabetic patients, and whether TBP should be included in the clinical screening for LEAD (study I). 2: To compare the reproducibility of absolute blood pressure measurements and blood pressure indices taken in the lower extremities among non-diabetic and diabetic patients without previously known LEAD (study II). 3: To compare the sensitivity of using pulse palpation vs. peripheral blood pressure readings to detect people with early asymptomatic LEAD (study I). 4: To evaluate the pole-test method in patients with diabetes and previously known LEAD (study II). 5: To assess the concordance between toe blood pressure measurements at the great toe and dig II, and to study how change in systemic blood pressure over time correlate to change in toe blood pressure (study II). 6: To assess the relationship between asymptomatic impairment of peripheral circulation in the lower extremities, i.e. signs of early, asymptomatic LEAD, and markers of fibrinolysis (study III). 7: To study the relationship between development and progression of impairment of peripheral circulation in the lower extremities (LEAD) over time and clinical, metabolic and inflammatory characteristics at baseline (study IV).

22
METHODS
Study cohorts
Study I: 437 subjects (134 ND, 166 T1D, and 137 T2D) without previously known LEAD were recruited in Umeå and Gothenburg. Inclusion of subjects began in 1997and ended in 1999 and participants were scheduled for regular visits every 2 years for a total of 10 years. Inclusion criteria were age between 30-70 years and no previously known or suspected LEAD. Eligible patients with T1D or T2D were consecutively asked by their ordinary physician whether they wished to participate. All patients gave a positive response. Non-diabetic subjects were recruited among hospital staff and by advertisements in local newspapers.
Study IIa: The reproducibility between indices and absolute blood pressure and concordance between the great toe and dig II was studied in 25 subjects; 13 healthy, non-diabetic subjects and 12 patients with diabetes (10 with T2D and 2 with T1D). Inclusion criteria and inclusion procedures were identical to study I.
Study IIb: The pole-test was evaluated in 11 patients with diabetes and previously diagnosed LEAD (8 T2D and 3 T1D) were recruited from the “foot clinic” at the outpatient clinic, Diabetes Unit at Umeå University Hospital.
Study III: Only participants recruited from Umeå were included (74 T1D, 69 T2D and 80 ND).
Study IV: Subjects included in study III were re-examined after approx 6 years of follow-up, 179 subjects (57 type 1-, 55 type 2- and 67 non-diabetic subjects) were included.
•

23
Fig. 3. Schematic illustration of study cohorts in studies I-IV.
Blood pressure measurements (study I- IV)
Blood pressures were measured in the supine position after a five minutes rest. Systolic and diastolic (Korotkoff phase V) blood pressures were assessed in the right arm. Systolic ankle blood pressures (ABP) were assessed with a cuff placed just above the ankle. Thereafter a Doppler pen (Hadeco MiniDoppler ES-100X and a 5 MHz probe; Arima, Miyamae-Ku, Kawasaki-Shi, Japan) was used to detect the dorsalis pedis/tibialis anterior (ATA) and the tibialis posterior arteries (ATP), respectively.
To determine toe blood pressure (TBP) a 2.5 x 13 cm blood pressure cuff was put on the proximal part of the toe and a sensor of a pulse oximeter (Biox 3700™, BOC Ohmeda, Helsingborg, Sweden) was placed on the tip of the great toe. Before measuring toe blood pressures, the skin temperature was assessed. The cuff was connected to a Tycos™ sphygmomanometer (Levimed AB, Höganäs, Sweden). When an appropriate pulse signal was obtained with the pulse oximeter, the cuff was inflated until the pulse signal had completely disappeared. Then, the cuff pressure was gradually released and it was continuously monitored. When the regular pulse signal reappeared, a pressure reading was performed to the nearest 2 mmHg, and this was considered to represent the systolic toe blood pressure. If the temperature was below 27.0°C, the feet were gently warmed with a heating pad.

24
At all the locations, e.g. arm, ankle and toe, the mean of two blood pressure readings was calculated. Indices were obtained by dividing each pressure by the systemic systolic blood pressure in the right arm.
Repeated measurements of ankle blood pressure (ABP), ankle-to-brachial index (ABI), toe blood pressure (TBP) and toe blood pressure index (TBI) have shown a coefficients of variation (CV%) between 4-9%[151].
Reduced peripheral blood pressure, i.e. signs of LEAD, was defined as at least one ankle (ABP) or toe blood pressure (TBP) or one ankle- to-brachial (ABI) or toe-to-brachial blood pressure index (TBI) below the normal range, defined as ankle <98 mmHg, toe <79 mmHg or ABI (ATA) < 0.90, ABI (ATP) <0.95, TBI <0.74 [62].
The modified pole-test (the “pole-pox method”) (study II)
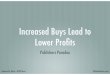
The pole test is a non-invasive method to measure ankle blood pressures without interference of mediasclerosis. This method has previously been described in detail by Smith et al [152]. In brief, the leg is elevated until the blood pressure at ankle level falls to zero and no pulse can be detected with pulse oxymetry, at this point, the gravitational pull on the blood column is equal to the systolic blood pressure and the height to which the foot is raised can be translated into the systolic arterial blood pressure by using the following formula: systolic blood pressure (mmHg) = [(Height (cm)-18)/1.3], 18 being a proxy for the distance between the bench and the patient’s heart in cm and 1.3 a correction coefficient for the relative density of blood and gravity (fig. 4). This method can only be used in patients with an ankle blood pressure <60 mmHg, equivalent to an elevation of about 100 cm, since a higher elevation of the leg usually is not feasible due to anatomical limitations. In this study measurements were performed in eleven patients. However, due to various reasons, i.e. amputation and technical difficulties, measurements were unachievable in three legs. In two of the patients measurements were done on two separate occasions and both values are used in the analysis.
•

25
Fig. 4. Schematic drawing of the modified pole-test technique Physical foot examination (study I- IV)
Physical foot examination was performed according to a standardized protocol. Foot pulses (a. dorsalis pedis and a. tibialis posterior), vibration perception thresholds and plantar reflexes as well as skin color, temperature, hair growth, nails and foot deformities were assessed.
Blood and urine chemistry (study I-IV)
Venous blood samples were collected in the morning between 7.00 and 9.00 am after an over-night fast (at least10 h). Plasma was obtained by centrifugation at 2500 g for 15 minutes, aliquot, and stored frozen at –80° C until analysis.
Blood glucose was determined using the HemoCue glucose system (HemoCue AB, Ängelholm, Sweden). HbA1c was measured by high-pressure liquid chromatography (Integral 4000, BioRad, Anaheim, CA, USA) (normal range 3.6-5.0%). Analyses of markers of fibrinolysis were made within one year of sampling in stored, frozen samples. Venous blood samples for haemostatic assays were drawn without stasis into Biopool stabilyte tubes. Mass concentrations of PAI-1 and tPA-PAI-1 complex were determined by ELISA, Imulyse™ PAI-1 for PAI-1 and sTintElize™ tPA/PAI-1 for tPA-PAI-1 complex. tPA mass was determined by Imulyse™ t-PA or TintElize™ tPA. Activity of tPA and PAI-1 were determined by a bio immunoassay (BIA), Chromolize™ t-PA for tPA and Chromolize™ PAI-1 for PAI-1. All reagent kits were purchased from Biopool AB (Umeå, Sweden).

26
Plasma TNF-α and IL-6 levels were determined using highly sensitive commercial immunoassay kits (Qantikine HS Human TNF-α Immunoassay and Qantikine HS Human IL-6 Immunoassay, R&D Systems Inc., Minneapolis, USA). High sensitive c-reactive protein (hs-CRP) was measured by using CRP (Latex) HS Tina-quant from Roche/Hitachi (Roche Diagnostics, Mannheim, Germany). Plasma adiponectin levels were determined using a commercial human adiponectin ELISA kit of sandwich type (Linco Research, St Charles, Missouri, USA).
Albumin excretion rate (AER) was measured in a timed overnight urine sample at study entry. The urine collection was performed without any changes in ongoing medication. Urine albumin concentration was measured with immune turbidimetry (Hitachi 911 multianalyser, Boeringer Mannheim Diagnostica, Mannheim, Germany).
Analyses of serum triglycerides and cholesterol were performed by routine methods at the Department of Clinical Chemistry, University Hospital of Umeå.
Statistical analyses
Statistical analyses were performed using StatView® statistics software (SAS Institute Inc.) (study I), SPSS v 10.0.7 (SPSS Inc., Chicago, IL, USA) (study II), SPSS v12.0.1 (study II, III and IV).
Data are presented as mean ± standard deviation or standard error of the mean [117] as indicated. The Kolmogorow-Smirnov test was used to assess the normality of distribution of data for individual subgroups and for all participants taken together. Differences in mean values between groups were analysed using the Student’s two-tailed t-test for normally distributed data. For variables not normally distributed the non-parametric Mann-Whitney U test was used. Differences in proportions were tested using Fisher’s exact test.
In study III and IV univariate logistic regression was used to assess relationships between measured variables and presence, development or worsening of LEAD. Alterations within individuals over time were assessed using Paired Samples T-Test for normally distributed variables and 2 Related Samples Test (Wilcoxon rank test) for variables not normally distributed. To assess linear relationships Pearson's Linear Correlation Coefficient were used for normally distributed and Spearman's rank correlation coefficient for not normally distributed variables. If not otherwise specifically stated a p-value less than 0.05 was considered statistically significant.
To examine the coefficients of variation (CV) we obtained ABP and TBP with corresponding indices on two occasions one week apart. Measurements were made by the same investigator in the manner described above. Individual CVs were calculated for the right and left leg, respectively and a mean was then computed. The formula used for calculating the CV were: CV% =sd/(mean*100), where sd were calculated from [ (x-m)2/n] and where x-m is the pressure difference between visit 1 and 2 and n is the total number of measurements performed at these two occasions
•

27
SUMMARY OF RESULTS
Paper I
In this study we evaluated a screening program for lower extremity arterial disease (LEAD) in diabetic patients and focused on the value of toe blood pressure assessment.
The proportion of patients with reduced peripheral blood pressures or indices below normal (< mean –2 SD for controls) was higher among diabetic patients; (24% of T1D and 31% of T2D), as compared to non-diabetic subjects (6%). These subjects were mainly identified by using the toe-to-brachial index (TBI). TBI was independently and negatively associated with fasting blood glucose in both patient groups, and with smoking, age, and diabetes duration in T1D. The mean ABP was higher in the T1D and T2D compared to ND, whereas overall TBP, TBI, and ABI were similar in the groups.
Low TBI was significantly more common than low ABI among diabetic subjects (p<0.001), and this was true also for TBP vs. ABP (p<0.05). also In addition, it was shown that 8–10% of the lower extremities of diabetic patients but only 1–2% of control subjects exhibited a low TP or TI despite normal AP and AI, whereas the opposite, e.g. a low AP or AI combined with a normal TP and TI, was seen in only ~2% in all groups. Furthermore, low peripheral pressures or indices in combination with 2 normal foot pulses were found in 9–12% of the lower limbs of diabetics compared to 5% among controls, and in combination with at least 1 normal pulse in 18–19% vs. 5%.
Main conclusions: Especially among diabetes patients, LEAD may exist despite two palpable foot pulses. It is beneficial to include assessment of toe blood pressure and toe-to-brachial blood pressure index (TBI) to detect early, asymptomatic LEAD in diabetic subjects. Ankle blood pressure and indices alone are less efficient, probably due to mediasclerosis in diabetic subjects. Up to 30% of diabetic subjects with no ischemic symptoms may have signs of impaired or reduced lower extremity arterial circulation. Paper II
No significant difference in reproducibility between absolute blood pressure measurements and indices (coefficients of variation (CV %) <9%) was found. A non-significant improvement with 4-8% in the sensitivity in detecting LEAD was seen when blood pressure indices were used instead of absolute blood pressure. Our data showed a significant correlation in the variation over time between systemic blood pressure and toe blood pressure, (r=0.34, p=0.015). There was a strong concordance between TBP measured at toe 1 and 2, respectively (r=0.99, p<0.001). TBP measured with a modified pole-test, i.e. the so-called pole-pox method were significantly correlated with measurements made by the ordinary cuff technique (r=0.75, p<0.001).
Main conclusions: The use of toe and ankle blood pressure indices instead of absolute blood pressure does not improve the reproducibility but may improve the sensitivity to detect LEAD, especially in subjects with diabetes. The pole-pox method may be used as an alternative screening method in patients with diabetes and previously known LEAD.
Paper III
In this study we assessed the relationship between early, asymptomatic reduction of peripheral circulation in the lower extremities, i.e. signs of early LEAD, and markers of fibrinolysis. In univariate logistic regression analyses age, glycemic level (HbA1c), male

28
gender (only in type 1 diabetic subjects), hypertension and tPA activity (only in type 2 diabetic subjects) were positively associated with LEAD. When markers of fibrinolysis were entered into a multivariate model adjusting for age, hypertension, and HbA1c, only tPA activity remained independently associated with LEAD (p=0.01) and this was also found in type 2 diabetic subjects (p=0.05). In type 1 diabetic subjects the increase in odds ratio was non-significant.
Main conclusions: Tissue plasminogen activator (tPA) activity may be an independent and early marker for asymptomatic lower extremity arterial disease in diabetic subjects, particularly in type 2 diabetes. Thus an altered fibrinolytic activity could be an early marker of atherosclerosis development in the lower extremities but the cause-effect relationship remains unclear. Paper IV
31 (17%) subjects developed subclinical LEAD or a progression of previously known LEAD during follow-up (8 ND, 12 T1D and 11 T2D subjects). In all subjects taken together age (p<0.001), weight (p=0.04), height (p=0.003) and female gender (p=0.04) were significantly associated with the development or progression of LEAD (WLEAD). Significant or near-significant associations between HbA1c (p=0.01), LDL-cholesterol (p=0.06), IL-6 (p=0.02), adiponectin (p=0.03), leptin (p=0.04) and WLEAD were also found. When entering all these variables into a multivariate model, adjusting for age and gender, only age and glycemic control (HbA1c) were significantly and independently associated with development or progression of LEAD among patients with type 2 diabetes.
Main conclusions: In this study we confirm that age and glycemic control was independently associated with the development or progression of early and subclinical LEAD in type 2 diabetic subjects.
DISCUSSION
Different definitions of LEAD
Different definitions of LEAD have been used in clinical studies. A commonly used definition of LEAD is an ABI <0.9 [6-8, 13, 21, 34, 63, 68-70, 153, 154] and this definition correlates well with angiographic signs of LEAD [13, 71].
In this thesis (study I-IV) we use a novel definition of LEAD, i.e. at least one ABP or TBP or ABI or TBI below the normal range, as assessed in healthy control subjects [62]. Since this definition of LEAD is based on a normal distribution in non-diabetic subjects (mean -2sd) it does not necessarily equal clinical disease but rather indicate that the blood pressure deviates from presumed “normality”. In these studies we have not validated our definition of LEAD against a golden standard, i.e. angiography or doppler investigation. Nor have we been able to correlate our definition to development of clinical symptoms since only 4 subjects developed symptomatic LEAD after 6 years of follow up. However, in support of this definition is that the cut-off value for the indices of the anterior tibial artery is similar as the most commonly used definition, i.e. ABI<0.9.
A recent study assessed the relation between a low ABI and high-grade stenoses in the pelvic and leg arteries in the general elderly population [155] and concluded that an ABI <0.9 may underestimate the prevalence of LEAD. In another study it was shown that a large portion (31%) of individuals with symptoms of LEAD but a normal ABI will
•

29
decrease significantly in ABI during a treadmill test, a clear indication of impairment of the peripheral circulation [79]. In summary there is no consensus on how to define asymptomatic LEAD and the definition of asymptomatic LEAD used in this thesis seems reasonable and may hopefully be clinical relevant in future studies.
The use of toe blood pressure in screening for LEAD
In study I diabetic subjects with impaired toe and ankle blood pressures or indices were identified despite the presence of one or two foot pulses. Almost 20% of diabetic subjects and 5% in the control group presented with at least one normal pulse even though a low pressure or index was measured at least one ankle artery or on the toe. Even in subjects with two detectable foot pulses reduced peripheral blood pressure was found in, ~10 % of diabetic subjects. Thus, in comparison to using foot pulses alone, absolute toe blood pressure or index markedly improved the sensitivity to detect LEAD in diabetic subjects, especially in type 2 diabetes. However, it is currently not known if the screening methods used in this study are superior to a simpler physical examination. This has to be further evaluated. In addition, it should be acknowledged, that no patient had a critically low peripheral blood pressure, and all subjects had a TBP above 50 mmHg.
The findings in study I also suggest that assessments of toe blood pressures offer significant advantages compared to ankle blood pressure measurements and be more efficient in detecting diabetic subjects with early, subclinical LEAD. The relationships between toe- and ankle blood pressure indices are shown in fig. 6. This is probably explained by an overestimation of ankle blood pressure due to the presence of mediasclerosis, which is more common and widespread in the ankle than in toe arteries [156, 157]. These findings are slightly contradictory to those reported by Brooks et al [158] where toe-to-brachial index did not seem to add clinical information beyond that obtained by using ankle-to-brachial index as long as the ABI is not abnormally high, i.e. above 1.3. However, in that study not separate analysis was done in subjects with impaired peripheral circulation. In study I a significant proportion of diabetic patients had a low TBI despite normal ABI (fig. 5). Moreover, an abnormally low intraluminal pressure coupled with a moderately advanced mediasclerosis must not result in an abnormally high ABI (i.e. 1.3) since ABI may be within the normal range (fig. 5). Our results are supported by Johansson et al ([159] who found that ankle Doppler blood pressure measurements overestimated LEAD in a primary care population. In addition, they showed that toe blood pressure measurements provided significantly more pathological indices as compared to ankle blood pressure measurements with Doppler [159].
Furthermore, Aso et al [160] have shown that a low TBI has a stronger association with markers of cardiovascular disease and vascular inflammation than a low ABI in type 2 diabetic patients. The differences between ankle and toe blood pressure measurement, with respect to cardiovascular risk, may not only be due to less mediasclerosis in arteries at the toe level but there could also be potential differences in the pathology in small vs. larger arteries [161].
Study I also indicates that TBI is better than the absolute TBP in identifying diabetic subjects with impaired peripheral circulation. This could be due to a higher systemic blood pressure in diabetic that would result in a higher TBP, and that this elevation in blood pressure is adjusted for by using the toe-to-brachial index. In clinical practice, the use of both TBP and TBI may be recommended.

30
Fig. 5. Diagram showing the relationship between toe- and ankle blood pressure indices artery in non-diabetic (n=134), type 1 -(n=166) and type 2-diabetic subjects (n=137) in study I. aSahli et.al 2004, bNorgren et al. 2007, c Brooks et al. 2001.
Even though the techniques to measure ankle- and toe blood pressure are similar,
i.e. both are cheap, quickly performed and non-invasive methods, measurement of toe blood pressure requires fastening of a blood pressure cuff on the great toe. This may be cumbersome in patients with short/wide toe base, ulcerations or amputation of the great toe. In study II we show that it is feasible to use dig II. These results are further supported by data from Hirai et al. who showed that in limbs with claudication but not gangrene, there is only a small variation in toe blood pressure between the five toes, suggesting that any of the five toes could be used for toe blood pressure measurements [162].
Reproducibility of absolute blood pressures vs. indices
Blood pressure indices are used instead of absolute blood pressures to correct for high systemic blood pressure and variations in the systemic blood pressure over time. However, in study II no difference in reproducibility was found between absolute blood pressures and indices at the ankle and toe level measured one week apart. This is in
•

31
accordance with a previous study by Faccenda et al [163]. However, since the systemic systolic blood pressure variation in our material was small and none of these patients had previously known LEAD it cannot be ruled out that index may contribute to a better reproducibility in such patients. This can be supported by the correlation found between the difference in systemic and toe blood pressures over time. In addition, it is noteworthy that the reproducibility for blood pressure measurements was similar at the ankle and toe level. Moreover, both the absolute blood pressures and indices were reproducible over a wide span of systemic blood pressures, indicating that this method could be used for screening purposes in the general population. The reproducibility (CV <9%) found in our study is reasonable and comparable with other previous studies [163, 164], but it is well-known that that reproducibility is influenced by the investigator’s experience [165] and the mode of calculation [166]. Inter-observer variability may also influence reproducibility; however, this was not examined in this study.
Modified elevation test (“Pole –test”)
A strong correlation was found between the pole-test and toe blood pressure measurements by ordinary cuff technique. In contrast, no significant correlation was found between the pole-test and ankle blood pressure measurements. This finding is most likely due to the fact that there were three patients with very high ankle pressures values obtained through cuff technique (mediasclerosis).
The usefulness of the pole-test is limited by the fact that a patients leg cannot be raised more than about 1 meter this corresponds to a pressure of <60–70 mmHg. Therefore the pole-test is limited to patients with leg ischemia. Our findings suggest that “pole-test” can be used, as an alternative to toe blood pressure measurements in diagnosing and following patients with CLI without the risk of obtaining falsely elevated pressure readings due to mediasclerosis.
Novel clinical and biochemical biomarkers as predictors of LEAD
High age, hyperglycemia, smoking, hypertension, male gender, obesity and dyslipidemia are well known risk factors and predictors for development and progression of LEAD [167]. In addition, inflammation and haemostatic alterations have been suggested as novel risk markers or predictors for LEAD [118-120, 128, 132, 160, 168-170]. In a cross-sectional study (study III) we assessed the relationship between fibrinolysis markers and the presence or absence of early asymptomatic LEAD and in a prospective study (study IV), the relationship between baseline risk markers and development or progression of LEAD was evaluated.
In study III we found an association between elevated tPA-activity and early signs of LEAD. tPA-activity remained an independent risk marker also after adjusting for the “classic” risk factors; i.e. age, hypertension and glycemic control. This was seen especially in type 2 diabetic subjects (T2D) where the relationship was significant despite a general hypofibrinolysis, as indicated by higher overall tPA-mass, PAI-1 activity and tPA-PAI-1 complex than in type 1- and non-diabetic subjects. Somewhat in contrast, previous studies have indicated an association between the presence or development LEAD and impaired fibrinolytic potential [119, 124-128, 167]. In addition, to being a risk marker of vascular damage, altered or impaired fibrinolysis has also been suggested to contribute to the progression of atherosclerotic lesions [129].

32
A highly speculative explanation for the elevation in tPA-activity found in subjects with early, asymptomatic, signs of LEAD might be that this is a compensatory mechanism to sustain circulation in compromised subjects and that this may be found early on in disease progression when the endothelium still is a major source of tPA [167, 171]. It remains unclear whether tPA has a direct effect on thrombotic risk or if acts as an inflammation or endothelial damage marker. It should be noted that systemic levels of fibrinolytic markers were measured and that these levels might not be representative for the actual levels in proximity to an atherosclerotic lesion. However, the finding that the elevation of tPA-activity was detectable in the systemic circulation could indicate a more general alteration in the vascular response. Despite our findings we could not confirm any association between tPA-activity and development or progression of LEAD in this cohort after 6 years of follow-up, as presented in study IV.
Despite numerous reports on associations between LEAD and inflammatory markers (CRP, IL-6 and TNF-α) [131, 132, 169, 170, 172] no such independent association was found in study IV. In this study age and hyperglycemia, were the main independent risk factors associated with development or progression of early, asymptomatic and subclinical LEAD among patients with type 2 diabetes. This finding is further supported by the fact that age and hyperglycemia also were independent predictors of reduction in toe blood pressure index (TBI) over time. Similar to the findings in this study, the Edinburgh Artery Study, a prospective longitudinal population-based study, showed a weak association between IL-6 and the development of LEAD, but this correlation was attenuated when adjusting for other CVD risk factors such as cholesterol, diabetes, hypertension, smoking and BMI [172]. Most previous studies have focused on elderly subjects with symptomatic LEAD whereas this study included middle-aged diabetic and non-diabetic subjects without previous signs or symptoms of LEAD. This is of importance since previous studies have suggested that inflammatory markers are elevated in subjects with symptomatic and critical leg ischemia, but not in subjects with less severe forms of LEAD [169]. The fact that we were able to confirm that the well known risk factors age and hyperglycemia in T2D were associated with development or progression of LEAD in this relatively small study indicate that the type 2 diabetic study population is representative and, in addition, supports the importance of these risk factors in development and progression of early, asymptomatic LEAD.
Aspects on screening for early, asymptomatic LEAD using toe blood pressure
One aim of this thesis was to evaluate the feasibility of a potential screening program for diabetic subjects based on a use of ankle blood pressure (ABP), toe blood pressure (TBP) measurements and blood sampling to assess risk factors related to LEAD. A screening program for early, asymptomatic and subclinical LEAD can be evaluated from both a cost-benefit and an ethical viewpoint. The World Health Organization (WHO) guidelines state that the condition screened for should be an important health problem and that there should be treatment for the condition. Facilities for diagnosis and treatment should be available and there should be a latent stage of the disease and, in addition, there should be a test or examination for the condition and the test should be acceptable to the population. Furthermore, the natural history of the disease should be adequately understood and there should be an agreed policy on who to treat. Finally, the total cost of finding a case should be economically
•

33
balanced in relation to medical expenditure as a whole and “case-finding” should be a continuous process.
LEAD is an important health problem in diabetic subjects. LEAD among diabetic patients is the leading cause of non-traumatic lower extremity amputations [97] and approx half of the lower extremity amputations performed in Sweden are done on patients with diabetes [97]. LEAD is also associated with increased overall morbidity and mortality [20, 173]. LEAD is common in patients with diabetes (30-40%), and the risk of developing LEAD is increased 2-4 fold compared to the general population [93].
There are preventive measures and treatments for LEAD such as smoking cessation, lipid-, glycemic- and blood pressure and antiplatelet therapy that in addition also reduces overall CV risk. Treatment for LEAD is already an established part of our health organization, from preventive measures in primary care to surgical intervention at specialized units.
Facilities for diagnosis and treatment are available at health care centers and outpatient diabetes clinics.
The natural history is understood and asymptomatic LEAD constitutes a latent phase for symptomatic LEAD. Ankle blood pressure measurements of the lower extremities are currently used as a diagnostic test. Ankle- and toe blood pressure measurement can be performed at any level of medical care and the equipment for is fairly cheap. Equipment for ankle- and toe blood pressure measurements cost approx 3500 SEK. An ABI examination takes approx 15 minutes, including a 5-minute pretest rest in the supine position[153]. The test is acceptable to the population as it is non-invasive with minimal discomfort [174]. The cost-benefit of finding LEAD, especially among diabetic patients who may have advanced stages of LEAD without clear symptoms has been evaluated and found to be motivated using ABI as a screening tool [52]. There is to our knowledge no cost-effective evaluation of screening for LEAD with TBI. It should be acknowledged that, using toe blood pressure measurements in addition to ABI will increase sensitivity and as such probably also result in additional costs for medication and further investigations. In summary, screening with ankle- and toe blood pressure measurements meet most of the criteria for a screening program but further evaluation of potential health benefits, cost-effectiveness and validity of this method not only in the prevention of LEAD related events but also, and perhaps more importantly, in finding patients at risk for cardiovascular and cerebrovascular disease is needed.
Limitations of studies
Information on medication and presence of cardiovascular disease was collected from the participants and later confirmed from their medical records. Having had the same study nurse/interviewer at each visit using a structured questionnaire and a standardized protocol have minimize problems with interpretation of data and the inter-observer variability in blood pressure measurements.
In addition, the power of studies III and IV to detect associations and make assumptions on subgroups were limited. However, the fact that we were able to confirm that well known risk factors, i.e age, hyperglycemia and hypertension, were associated with development or progression of LEAD in our relatively small material indicate that our study population seems representative and, in addition, supports the importance of these “classic” risk factors also in early, asymptomatic LEAD.
Including relatively young participants with no previously known or suspected LEAD in combination with our broadened definition of development or progression of

34
LEAD may have resulted in a selection of relatively healthy participants with earlier and more discrete LEAD compared to other studies.
The study cohorts In paper I, III and IV patients with diabetes were consecutively enrolled from the
outpatient diabetes units in Göteborg and Umeå. Patients with type 1 diabetes (T1D) should be representative of the whole T1D population in the two cities since all patients with T1D attend the diabetic outpatient clinics, however, in contrast, the enrolled patients with type 2 diabetes are probably somewhat selected, since only those with a need for intensive treatment or with severe diabetic complications are referred to outpatient diabetes units, i.e. patients with more advanced disease and longer duration as compared to the overall population of patients with diabetes within primary care.
Healthy, non-diabetic, subjects were recruited among hospital staff and by advertisements in local newspapers. This might involve a certain bias since medical staff might differ from the general population. However, a comparison of the healthy subjects in these papers with the participants of the northern Sweden MONICA Study population surveys from 1994 and 1999 indicate that the these subjects were a valid sample of the general, non-diabetic, population with respect to cardiovascular risk factors, i.e. body mass index (BMI), systolic and diastolic blood pressure, serum cholesterol and high-density lipoprotein (HDL) cholesterol, plasma glucose, and insulin levels with one exception, smoking, where the prevalence was unexpectedly low compared to the MONICA population (12 vs. 19%) (M. Eliasson et al, unpubl data). Future studies
To our knowledge, there are currently no studies published on the validity of a screening program based on toe blood pressure measurements or a combination of lower extremity blood pressures, in comparison to the ABI, angiography or duplex-doppler methods, and there is no general consensus regarding cut-off values for toe indices. After 10 year of follow up, we will hopefully have sufficient hard endpoints (clinical symptoms or signs of LEAD) to be able to calculate sensitivity and specificity for this toe blood pressure-based screening method and also be able to evaluate is toe blood pressure is a better predictor of future cardiovascular events than ankle blood pressure. In addition, prospective randomized controlled intervention studies in patients with early, asymptomatic LEAD are warranted. It would be of great interest to study life-style interventions, i.e. light exercise and smoking secession in such subjects.
CONCLUDING REMARKS
In this thesis we have evaluated a new method to assess impaired lower extremity arterial circulation in diabetic subjects and found that including assessment of toe blood pressure and toe-to-brachial blood pressure index (TBI) to detect early, asymptomatic LEAD increases sensitivity and case-finding. Ankle blood pressure measurement and indices alone are less reliable, especially in diabetic subjects where mediasclerosis is common. Furthermore, toe blood pressure measurements can be performed using either the great or dig II. In addition, since the modified elevation test may be used as an alternative screening method in subjects with previously known LEAD. An altered fibrinolytic activity could be an early marker of atherosclerotic development in the
•

35
lower extremities but the cause-effect relationship remains unclear. Old age and poor glycemic control are the most important risk factors for development and progression of early, subclinical LEAD among patients with type 2 diabetes.

36
ACKNOWLEDGEMENTS
There are several people without whom this thesis would not have been possible, my deep and heartfelt gratitude goes out to all of you and especially to: My supervisor Maria Svensson for so much more than one could ask. You have always been there for me, giving advice and encouragement. It has been an honor to work with you. If ever the lost soul of a PhD student should fall into my hands your example will be my golden standard. Co-supervisors; Jan Eriksson and Gisela Dahlquist for hard questions and soft words as well as helpful comments throughout this process. To all my colleagues at the pediatric clinic and the staff at Metabolenheten, it has been a pleasure working with you all. Special thanks go to Kristina Öjbrandt, who I believe is the main reason our study participants kept coming year after year. Great job! All the participants in our studies without whom this work would not have been possible. Mediha Novo, from the moment of our first meeting I found an old friend. I will continue to knock on your door for advice. Roland och Irene Eriksson, John Stark for all the good times we have had, see you in Zakynthos. Karin Moström for kind and skillful assistance with various papers and applications that needed to be sent yesterday. My parents Adam and Mona Sahli, for your faith in me and for making me love life even during hard times. My brothers, for fixing my computer on numerous occasions and to Ann-Catherine for helping me with illustrations (it should be obvious which are yours). Finally I want to thank my beloved wife, Nora and our wonderful children Adam, Selma and Elias for, during the last months, letting me live like a bachelor without really making me one. The encouragement and support from you has kept me sane (or close enough) during the work with this thesis. These studies were performed at the Metabolic Unit, Dept of public Health and Clinical Medicine and at the Department of Clinical Sciences, Pediatrics, Umeå University Hospital. Financial support was given by the Swedish Research Council (Medicine, projects 12663 and 14287), the Torsten and Ragnar Söderberg Foundation, the Swedish Diabetes Association, the Göteborg Diabetes Association, the Umeå University Medical Faculty Foundations, Eli Lilly Sweden AB, the Northern Sweden County Councils (VisareNorr) as well as the Salus, Elsa and Folke Sahlberg, Loo and Hans Osterman, Sigurd and Elsa Golje, and Trygg-Hansa and Novo-Nordisk Foundations. Additionally, study III and IV were conducted with the support from the Department of Clinical Sciences, Pediatrics in Umeå who partly funded my research time.
•

37
REFERENCES
1. Heald, C.L., F.G. Fowkes, G.D. Murray, et al., Risk of mortality and cardiovascular disease
associated with the ankle-brachial index: Systematic review. Atherosclerosis, 2006. 189(1): p. 61-9.
2. Hooi, J.D., A.D. Kester, H.E. Stoffers, et al., Asymptomatic peripheral arterial occlusive disease predicted cardiovascular morbidity and mortality in a 7-year follow-up study. J Clin Epidemiol, 2004. 57(3): p. 294-300.
3. Ogren, M., B. Hedblad, S.O. Isacsson, et al., Non-invasively detected carotid stenosis and ischaemic heart disease in men with leg arteriosclerosis. Lancet, 1993. 342(8880): p. 1138-41.
4. van der Meer, I.M., M.L. Bots, A. Hofman, et al., Predictive value of noninvasive measures of atherosclerosis for incident myocardial infarction: the Rotterdam Study. Circulation, 2004. 109(9): p. 1089-94.
5. Newman, A.B., D.S. Siscovick, T.A. Manolio, et al., Ankle-arm index as a marker of atherosclerosis in the Cardiovascular Health Study. Cardiovascular Heart Study (CHS) Collaborative Research Group. Circulation, 1993. 88(3): p. 837-45.
6. Aboyans, V., P. Lacroix, and M. Laskar, Prevalence of symptomatic and asymptomatic peripheral arterial disease in primary care patients. Atherosclerosis, 2004. 175(1): p. 183-4; author reply 185-6.
7. Fowkes, F.G., E. Housley, E.H. Cawood, et al., Edinburgh Artery Study: prevalence of asymptomatic and symptomatic peripheral arterial disease in the general population. Int J Epidemiol, 1991. 20(2): p. 384-92.
8. Diehm, C., A. Schuster, J.R. Allenberg, et al., High prevalence of peripheral arterial disease and co-morbidity in 6880 primary care patients: cross-sectional study. Atherosclerosis, 2004. 172(1): p. 95-105.
9. Lloyd-Jones, D., R. Adams, M. Carnethon, et al., Heart disease and stroke statistics--2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation, 2009. 119(3): p. e21-181.
10. SBU, S.r.r.f.g.s., SBU. 2007. 11. Apelqvist, J., G. Ragnarson-Tennvall, U. Persson, et al., Diabetic foot ulcers in a
multidisciplinary setting. An economic analysis of primary healing and healing with amputation. J Intern Med, 1994. 235(5): p. 463-71.
12. Larsson, J., J. Apelqvist, C.D. Agardh, et al., Decreasing incidence of major amputation in diabetic patients: a consequence of a multidisciplinary foot care team approach? Diabet Med, 1995. 12(9): p. 770-6.
13. Norgren, L., W.R. Hiatt, J.A. Dormandy, et al., Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Eur J Vasc Endovasc Surg, 2007. 33 Suppl 1: p. S1-75.
14. Matzke, S. and M. Lepantalo, Claudication does not always precede critical leg ischemia. Vasc Med, 2001. 6(2): p. 77-80.
15. Zeymer, U., K.G. Parhofer, D. Pittrow, et al., Risk factor profile, management and prognosis of patients with peripheral arterial disease with or without coronary artery disease: results of the prospective German REACH registry cohort. Clin Res Cardiol, 2009. 98(4): p. 249-56.
16. Leng, G.C., A.J. Lee, F.G. Fowkes, et al., Incidence, natural history and cardiovascular events in symptomatic and asymptomatic peripheral arterial disease in the general population. Int J Epidemiol, 1996. 25(6): p. 1172-81.
17. Dormandy, J.A. and R.B. Rutherford, Management of peripheral arterial disease (PAD). TASC Working Group. TransAtlantic Inter-Society Consensus (TASC). J Vasc Surg, 2000. 31(1 Pt 2): p. S1-S296.

38
18. Cacoub, P.P., M.T. Abola, I. Baumgartner, et al., Cardiovascular risk factor control and outcomes in peripheral artery disease patients in the Reduction of Atherothrombosis for Continued Health (REACH) Registry. Atherosclerosis, 2009. 204(2): p. e86-92.
19. Welten, G.M., O. Schouten, S.E. Hoeks, et al., Long-term prognosis of patients with peripheral arterial disease: a comparison in patients with coronary artery disease. J Am Coll Cardiol, 2008. 51(16): p. 1588-96.
20. Monreal, M., L. Alvarez, B. Vilaseca, et al., Clinical outcome in patients with peripheral artery disease. Results from a prospective registry (FRENA). Eur J Intern Med, 2008. 19(3): p. 192-7.
21. Hooi, J.D., A.D. Kester, H.E. Stoffers, et al., Incidence of and risk factors for asymptomatic peripheral arterial occlusive disease: a longitudinal study. Am J Epidemiol, 2001. 153(7): p. 666-72.
22. Hooi, J.D., H.E. Stoffers, A.D. Kester, et al., Risk factors and cardiovascular diseases associated with asymptomatic peripheral arterial occlusive disease. The Limburg PAOD Study. Peripheral Arterial Occlusive Disease. Scand J Prim Health Care, 1998. 16(3): p. 177-82.
23. Skau, T. and B. Jonsson, Prevalence of symptomatic leg ischaemia in a Swedish community--an epidemiological study. Eur J Vasc Surg, 1993. 7(4): p. 432-7.
24. Meijer, W.T., A.W. Hoes, D. Rutgers, et al., Peripheral arterial disease in the elderly: The Rotterdam Study. Arterioscler Thromb Vasc Biol, 1998. 18(2): p. 185-92.
25. Sigvant, B., K. Wiberg-Hedman, D. Bergqvist, et al., A population-based study of peripheral arterial disease prevalence with special focus on critical limb ischemia and sex differences. J Vasc Surg, 2007. 45(6): p. 1185-91.
26. Lange, S.F., H.J. Trampisch, D. Pittrow, et al., Profound influence of different methods for determination of the ankle brachial index on the prevalence estimate of peripheral arterial disease. BMC Public Health, 2007. 7: p. 147.
27. [Ankle-brachial index to be measured more often. Every fifth patient over 65 has peripheral arterial occlusive disease]. MMW Fortschr Med, 2003. 145(50): p. 55.
28. Kemp, G.J., L.J. Hands, G. Ramaswami, et al., Calf muscle mitochondrial and glycogenolytic ATP synthesis in patients with claudication due to peripheral vascular disease analysed using 31P magnetic resonance spectroscopy. Clin Sci (Lond), 1995. 89(6): p. 581-90.
29. Immke, D.C. and E.W. McCleskey, Lactate enhances the acid-sensing Na+ channel on ischemia-sensing neurons. Nat Neurosci, 2001. 4(9): p. 869-70.
30. Stoffers, H.E., P.E. Rinkens, A.D. Kester, et al., The prevalence of asymptomatic and unrecognized peripheral arterial occlusive disease. Int J Epidemiol, 1996. 25(2): p. 282-90.
31. Pasternak, R.C., M.H. Criqui, E.J. Benjamin, et al., Atherosclerotic Vascular Disease Conference: Writing Group I: epidemiology. Circulation, 2004. 109(21): p. 2605-12.
32. Sigvant, B., K. Wiberg-Hedman, D. Bergqvist, et al., Risk factor profiles and use of cardiovascular drug prevention in women and men with peripheral arterial disease. Eur J Cardiovasc Prev Rehabil, 2009. 16(1): p. 39-46.
33. Ogren, M., B. Hedblad, G. Engstrom, et al., Leg blood flow and long-term cardiovascular prognosis in men with typical and atypical intermittent claudication. Eur J Vasc Endovasc Surg, 2003. 26(3): p. 272-9.
34. Management of peripheral arterial disease (PAD). TransAtlantic Inter-Society Consensus (TASC). Eur J Vasc Endovasc Surg, 2000. 19 Suppl A: p. Si-xxviii, S1-250.
35. Hirsch, A.T., Z.J. Haskal, N.R. Hertzer, et al., ACC/AHA Guidelines for the Management of Patients with Peripheral Arterial Disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Associations for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (writing committee to develop guidelines for the management of patients with peripheral arterial disease)--summary of recommendations. J Vasc Interv Radiol, 2006. 17(9): p. 1383-97; quiz 1398.
•

39
36. Jensen, S.A., L.J. Vatten, and H.O. Myhre, The prevalence of chronic critical lower limb ischaemia in a population of 20,000 subjects 40-69 years of age. Eur J Vasc Endovasc Surg, 2006. 32(1): p. 60-5.
37. Antohe, F., Endothelial cells and macrophages, partners in atherosclerotic plaque progression. Arch Physiol Biochem, 2006. 112(4-5): p. 245-53.
38. Arosio, E., S. De Marchi, M. Prior, et al., Activity of cardiopulmonary baroreceptors, peripheral resistance and cutaneous microcirculation in patients with peripheral obstructive arterial disease. J Intern Med, 2000. 247(4): p. 471-8.
39. Guimaraes, A.H., E.L. de Bruijne, T. Lisman, et al., Hypofibrinolysis is a risk factor for arterial thrombosis at young age. Br J Haematol, 2009. 145(1): p. 115-20.
40. Vague, P., D. Raccah, and V. Scelles, Hypofibrinolysis and the insulin resistance syndrome. Int J Obes Relat Metab Disord, 1995. 19 Suppl 1: p. S11-5.
41. Worthley, S.G., G. Helft, A.G. Zaman, et al., Atherosclerosis and the vulnerable plaque--pathogenesis: Part I. Aust N Z J Med, 2000. 30(5): p. 600-7.
42. Glass, C.K. and J.L. Witztum, Atherosclerosis. the road ahead. Cell, 2001. 104(4): p. 503-16. 43. Constantinescu, E., D. Alexandru, V. Alexandru, et al., Endothelial cell-derived foam cells
fail to express adhesion molecules (ICAM-1 and VCAM-1) for monocytes. J Submicrosc Cytol Pathol, 2000. 32(2): p. 195-201.
44. Simionescu, M. and F. Antohe, Functional ultrastructure of the vascular endothelium: changes in various pathologies. Handb Exp Pharmacol, 2006(176 Pt 1): p. 41-69.
45. Pearson, J.D., Endothelial cell function and thrombosis. Baillieres Best Pract Res Clin Haematol, 1999. 12(3): p. 329-41.
46. Davies, M.G. and P.O. Hagen, The vascular endothelium. A new horizon. Ann Surg, 1993. 218(5): p. 593-609.
47. Blann, A.D. and D.A. Taberner, A reliable marker of endothelial cell dysfunction: does it exist? Br J Haematol, 1995. 90(2): p. 244-8.
48. Celermajer, D.S., Endothelial dysfunction: does it matter? Is it reversible? J Am Coll Cardiol, 1997. 30(2): p. 325-33.
49. Furman, C., C. Copin, M. Kandoussi, et al., Rosuvastatin reduces MMP-7 secretion by human monocyte-derived macrophages: potential relevance to atherosclerotic plaque stability. Atherosclerosis, 2004. 174(1): p. 93-8.
50. Libby, P., Y.J. Geng, M. Aikawa, et al., Macrophages and atherosclerotic plaque stability. Curr Opin Lipidol, 1996. 7(5): p. 330-5.
51. Ramos, A.M., L.C. Pellanda, I. Gus, et al., Inflammatory markers of cardiovascular disease in the elderly. Arq Bras Cardiol, 2009. 92(3): p. 221-8, 227-34.
52. American_Diabetes_Association, Peripheral arterial disease in people with diabetes. Diabetes Care, 2003. 26(12): p. 3333-41.
53. Standeven, K.F., R.A. Ariens, and P.J. Grant, The molecular physiology and pathology of fibrin structure/function. Blood Rev, 2005. 19(5): p. 275-88.
54. Doweik, L., T. Maca, M. Schillinger, et al., Fibrinogen predicts mortality in high risk patients with peripheral artery disease. Eur J Vasc Endovasc Surg, 2003. 26(4): p. 381-6.
55. Hoyt, R.E., Peripheral arterial disease in people with diabetes: response to consensus statement. Diabetes Care, 2004. 27(8): p. 2095; author reply 2095.
56. Mackey, R.H., L. Venkitachalam, and K. Sutton-Tyrrell, Calcifications, arterial stiffness and atherosclerosis. Adv Cardiol, 2007. 44: p. 234-44.
57. Lachman, A.S., T.L. Spray, D.M. Kerwin, et al., Medial calcinosis of Monckeberg. A review of the problem and a description of a patient with involvement of peripheral, visceral and coronary arteries. Am J Med, 1977. 63(4): p. 615-22.
58. Neubauer, B., N.J. Christensen, T. Christensen, et al., Diabetic macroangiopathy. Medial calcifications, narrowing, rugosities, stiffness, norepinephrine depletion and reduced blood flow capacity in the leg arteries. Acta Med Scand Suppl, 1984. 687: p. 37-45.
59. Sucker, C. and P. Lanzer, [Arteriosclerosis and media sclerosis. A comparison of 2 calcifying vascular diseases]. Med Klin (Munich), 2000. 95(4): p. 207-10.

40
60. Raines, J.K., R.C. Darling, J. Buth, et al., Vascular laboratory criteria for the management of peripheral vascular disease of the lower extremities. Surgery, 1976. 79(1): p. 21-9.
61. Leng, G.C. and F.G. Fowkes, The Edinburgh Claudication Questionnaire: an improved version of the WHO/Rose Questionnaire for use in epidemiological surveys. J Clin Epidemiol, 1992. 45(10): p. 1101-9.
62. Sahli, D., B. Eliasson, M. Svensson, et al., Assessment of toe blood pressure is an effective screening method to identify diabetes patients with lower extremity arterial disease. Angiology, 2004. 55(6): p. 641-51.
63. Bonham, P.A., Get the LEAD out: noninvasive assessment for lower extremity arterial disease using ankle brachial index and toe brachial index measurements. J Wound Ostomy Continence Nurs, 2006. 33(1): p. 30-41.
64. Carmo, G.A., A. Mandil, B.R. Nascimento, et al., Can we measure the ankle-brachial index using only a stethoscope? A pilot study. Fam Pract, 2009. 26(1): p. 22-6.
65. Fowkes, F.G., G.D. Murray, I. Butcher, et al., Ankle brachial index combined with Framingham Risk Score to predict cardiovascular events and mortality: a meta-analysis. JAMA, 2008. 300(2): p. 197-208.
66. Dieter, R.S., W.W. Chu, J.P. Pacanowski, Jr., et al., The significance of lower extremity peripheral arterial disease. Clin Cardiol, 2002. 25(1): p. 3-10.
67. Criqui, M.H., V. Vargas, J.O. Denenberg, et al., Ethnicity and peripheral arterial disease: the San Diego Population Study. Circulation, 2005. 112(17): p. 2703-7.
68. Beckman, J.A., M.R. Jaff, and M.A. Creager, The United States preventive services task force recommendation statement on screening for peripheral arterial disease: more harm than benefit? Circulation, 2006. 114(8): p. 861-6.
69. Leng, G.C., F.G. Fowkes, A.J. Lee, et al., Use of ankle brachial pressure index to predict cardiovascular events and death: a cohort study. BMJ, 1996. 313(7070): p. 1440-4.
70. Yao, S.T., J.T. Hobbs, and W.T. Irvine, Ankle systolic pressure measurements in arterial disease affecting the lower extremities. Br J Surg, 1969. 56(9): p. 676-9.
71. Greenland, P., J. Abrams, G.P. Aurigemma, et al., Prevention Conference V: Beyond secondary prevention: identifying the high-risk patient for primary prevention: noninvasive tests of atherosclerotic burden: Writing Group III. Circulation, 2000. 101(1): p. E16-22.
72. Baker, J.D. and D.E. Dix, Variability of Doppler ankle pressures with arterial occlusive disease: an evaluation of ankle index and brachial-ankle pressure gradient. Surgery, 1981. 89(1): p. 134-7.
73. Ray, S.A., P.D. Srodon, R.S. Taylor, et al., Reliability of ankle:brachial pressure index measurement by junior doctors. Br J Surg, 1994. 81(2): p. 188-90.
74. Kaiser, V., A.D. Kester, H.E. Stoffers, et al., The influence of experience on the reproducibility of the ankle-brachial systolic pressure ratio in peripheral arterial occlusive disease. Eur J Vasc Endovasc Surg, 1999. 18(1): p. 25-9.
75. Hiatt, W.R., S. Hoag, and R.F. Hamman, Effect of diagnostic criteria on the prevalence of peripheral arterial disease. The San Luis Valley Diabetes Study. Circulation, 1995. 91(5): p. 1472-9.
76. Hirschl, M., M. Francesconi, and M.M. Hirschl, [Moenckeberg media sclerosis: clinical aspects in diabetic patients]. Vasa, 1991. 20(3): p. 216-21.
77. Novo, S., Classification, epidemiology, risk factors, and natural history of peripheral arterial disease. Diabetes Obes Metab, 2002. 4 Suppl 2: p. S1-6.
78. Williams, D.T., K.G. Harding, and P. Price, An evaluation of the efficacy of methods used in screening for lower-limb arterial disease in diabetes. Diabetes Care, 2005. 28(9): p. 2206-10.
79. Stein, R., I. Hriljac, J.L. Halperin, et al., Limitation of the resting ankle-brachial index in symptomatic patients with peripheral arterial disease. Vasc Med, 2006. 11(1): p. 29-33.
80. Montgomery, P.S. and A.W. Gardner, The clinical utility of a six-minute walk test in peripheral arterial occlusive disease patients. J Am Geriatr Soc, 1998. 46(6): p. 706-11.
•

41
81. Pahlsson, H.I., C. Laskar, K. Stark, et al., The optimal cuff width for measuring toe blood pressure. Angiology, 2007. 58(4): p. 472-6.
82. Mohler, E.R., 3rd, Peripheral arterial disease: identification and implications. Arch Intern Med, 2003. 163(19): p. 2306-14.
83. Jaff, M.R., Lower extremity arterial disease. Diagnostic aspects. Cardiol Clin, 2002. 20(4): p. 491-500, v.
84. Jorneskog, G., M. Kalani, J. Kuhl, et al., Early microvascular dysfunction in healthy normal-weight males with heredity for type 2 diabetes. Diabetes Care, 2005. 28(6): p. 1495-7.
85. Fagrell, B., G. Jorneskog, and M. Intaglietta, Disturbed microvascular reactivity and shunting - a major cause for diabetic complications. Vasc Med, 1999. 4(3): p. 125-7.
86. Hessel, S.J., D.F. Adams, and H.L. Abrams, Complications of angiography. Radiology, 1981. 138(2): p. 273-81.
87. Balduf, L.M., M. Langsfeld, J.M. Marek, et al., Complication rates of diagnostic angiography performed by vascular surgeons. Vasc Endovascular Surg, 2002. 36(6): p. 439-45.
88. Ihlberg, L., A. Alback, W.D. Roth, et al., Interobserver agreement in duplex scanning for vein grafts. Eur J Vasc Endovasc Surg, 2000. 19(5): p. 504-8.
89. Lujan, S., E. Criado, E. Puras, et al., Duplex scanning or arteriography for preoperative planning of lower limb revascularisation. Eur J Vasc Endovasc Surg, 2002. 24(1): p. 31-6.
90. Freund, K.M., A.J. Belanger, R.B. D'Agostino, et al., The health risks of smoking. The Framingham Study: 34 years of follow-up. Ann Epidemiol, 1993. 3(4): p. 417-24.
91. Price, J.F., P.I. Mowbray, A.J. Lee, et al., Relationship between smoking and cardiovascular risk factors in the development of peripheral arterial disease and coronary artery disease: Edinburgh Artery Study. Eur Heart J, 1999. 20(5): p. 344-53.
92. Selvin, E. and T.P. Erlinger, Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999-2000. Circulation, 2004. 110(6): p. 738-43.
93. Marso, S.P. and W.R. Hiatt, Peripheral arterial disease in patients with diabetes. J Am Coll Cardiol, 2006. 47(5): p. 921-9.
94. Adler, A.I., R.J. Stevens, A. Neil, et al., UKPDS 59: hyperglycemia and other potentially modifiable risk factors for peripheral vascular disease in type 2 diabetes. Diabetes Care, 2002. 25(5): p. 894-9.
95. Zander, E., P. Heinke, J. Reindel, et al., Peripheral arterial disease in diabetes mellitus type 1 and type 2: are there different risk factors? Vasa, 2002. 31(4): p. 249-54.
96. Eneroth, M. and B.M. Persson, Amputation for occlusive arterial disease. A prospective multicentre study of 177 amputees. Int Orthop, 1992. 16(4): p. 383-7.
97. Apelqvist, J. and J. Larsson, What is the most effective way to reduce incidence of amputation in the diabetic foot? Diabetes Metab Res Rev, 2000. 16 Suppl 1: p. S75-83.
98. von Knorring, J. and M. Lepantalo, Effect of risk factors on outcome in patients with peripheral arterial occlusive disease. Ann Chir Gynaecol, 1992. 81(2): p. 103-6.
99. Willigendael, E.M., J.A. Teijink, M.L. Bartelink, et al., Influence of smoking on incidence and prevalence of peripheral arterial disease. J Vasc Surg, 2004. 40(6): p. 1158-65.
100. Jensen, S.A., L.J. Vatten, T.I. Nilsen, et al., The association between smoking and the prevalence of intermittent claudication. Vasc Med, 2005. 10(4): p. 257-63.
101. Fielding, J.E., Smoking: health effects and control (1). N Engl J Med, 1985. 313(8): p. 491-8. 102. Meijer, W.T., D.E. Grobbee, M.G. Hunink, et al., Determinants of peripheral arterial disease
in the elderly: the Rotterdam study. Arch Intern Med, 2000. 160(19): p. 2934-8. 103. Makin, A., G.Y. Lip, S. Silverman, et al., Peripheral vascular disease and hypertension: a
forgotten association? J Hum Hypertens, 2001. 15(7): p. 447-54. 104. Murabito, J.M., R.B. D'Agostino, H. Silbershatz, et al., Intermittent claudication. A risk
profile from The Framingham Heart Study. Circulation, 1997. 96(1): p. 44-9. 105. van Popele, N.M., D.E. Grobbee, M.L. Bots, et al., Association between arterial stiffness and
atherosclerosis: the Rotterdam Study. Stroke, 2001. 32(2): p. 454-60.

42
106. Safar, M.E., S. Laurent, R.E. Asmar, et al., Systolic hypertension in patients with arteriosclerosis obliterans of the lower limbs. Angiology, 1987. 38(4): p. 287-95.
107. Esteban, C., A. Presas, J. Ara, et al., [Prevalence of renal artery stenosis in patients with critical limb ischemia]. Med Clin (Barc), 2007. 128(15): p. 561-4.
108. Kannel, W.B. and D.L. McGee, Update on some epidemiologic features of intermittent claudication: the Framingham Study. J Am Geriatr Soc, 1985. 33(1): p. 13-8.
109. Norata, G.D., S. Raselli, L. Grigore, et al., Small dense LDL and VLDL predict common carotid artery IMT and elicit an inflammatory response in peripheral blood mononuclear and endothelial cells. Atherosclerosis, 2009.
110. Dionyssiou-Asteriou, A., M. Papastamatiou, I. Vatalas, et al., Serum Lp(a) lipoprotein levels in patients with atherosclerotic occlusive disease of the lower extremities. Eur J Vasc Endovasc Surg, 2000. 20(1): p. 57-60.
111. Dormandy, J., L. Heeck, and S. Vig, The fate of patients with critical leg ischemia. Semin Vasc Surg, 1999. 12(2): p. 142-7.
112. Ghosh, S. and W.S. Aronow, Utilization of lipid-lowering drugs in elderly persons with increased serum low-density lipoprotein cholesterol associated with coronary artery disease, symptomatic peripheral arterial disease, prior stroke, or diabetes mellitus before and after an educational program on dyslipidemia treatment. J Gerontol A Biol Sci Med Sci, 2003. 58(5): p. M432-5.
113. Olin, J.W., M.D. Cressman, J.R. Young, et al., Lipid and lipoprotein abnormalities in lower-extremity arteriosclerosis obliterans. Cleve Clin J Med, 1992. 59(5): p. 491-7.
114. Mowat, B.F., E.R. Skinner, H.M. Wilson, et al., Alterations in plasma lipids, lipoproteins and high density lipoprotein subfractions in peripheral arterial disease. Atherosclerosis, 1997. 131(2): p. 161-6.
115. Buchwald, H., R.L. Varco, J.P. Matts, et al., Effect of partial ileal bypass surgery on mortality and morbidity from coronary heart disease in patients with hypercholesterolemia. Report of the Program on the Surgical Control of the Hyperlipidemias (POSCH). N Engl J Med, 1990. 323(14): p. 946-55.
116. Khan, F., S.J. Litchfield, P.A. Stonebridge, et al., Lipid-lowering and skin vascular responses in patients with hypercholesterolaemia and peripheral arterial obstructive disease. Vasc Med, 1999. 4(4): p. 233-8.
117. Opper, C., C. Clement, H. Schwarz, et al., Increased number of high sensitive platelets in hypercholesterolemia, cardiovascular diseases, and after incubation with cholesterol. Atherosclerosis, 1995. 113(2): p. 211-7.
118. Schneider, D.J., T.K. Nordt, and B.E. Sobel, Attenuated fibrinolysis and accelerated atherogenesis in type II diabetic patients. Diabetes, 1993. 42(1): p. 1-7.
119. Killewich, L.A., A.W. Gardner, R.F. Macko, et al., Progressive intermittent claudication is associated with impaired fibrinolysis. J Vasc Surg, 1998. 27(4): p. 645-50.
120. Caputo, M., G. Mantini, I. Floriani, et al., Tissue plasminogen activator, tissue plasminogen activator inhibitor and lipoprotein(a) in patients with coronary, epiaortic and peripheral occlusive artery disease. Eur Heart J, 1996. 17(9): p. 1329-36.
121. Sahli, D., J.W. Eriksson, K. Boman, et al., Tissue plasminogen activator (tPA) activity is a novel and early marker of asymptomatic LEAD in type 2 diabetes. Thromb Res, 2009. 123(5): p. 701-6.
122. Smith, F.B., A.J. Lee, A. Rumley, et al., Tissue-plasminogen activator, plasminogen activator inhibitor and risk of peripheral arterial disease. Atherosclerosis, 1995. 115(1): p. 35-43.
123. Speiser, W., P. Speiser, E. Minar, et al., Activation of coagulation and fibrinolysis in patients with arteriosclerosis: relation to localization of vessel disease and risk factors. Thromb Res, 1990. 59(1): p. 77-88.
124. Cortellaro, M., E. Cofrancesco, C. Boschetti, et al., Association of increased fibrin turnover and defective fibrinolytic capacity with leg atherosclerosis. The PLAT Group. Thromb Haemost, 1994. 72(2): p. 292-6.
•

43
125. Johansson, J., N. Egberg, H. Johnsson, et al., Serum lipoproteins and hemostatic function in intermittent claudication. Arterioscler Thromb, 1993. 13(10): p. 1441-8.
126. Lapolla, A., F. Piarulli, G. Sartore, et al., Peripheral artery disease in type 2 diabetes: the role of fibrinolysis. Thromb Haemost, 2003. 89(1): p. 91-6.
127. Maser, R.E., D. Ellis, J.R. Erbey, et al., Do tissue plasminogen activator-plasminogen activator inhibitor-1 complexes relate to the complications of insulin-dependent diabetes mellitus? Pittsburgh Epidemiology of Diabetes Complications Study. J Diabetes Complications, 1997. 11(4): p. 243-9.
128. Tzoulaki, I., G.D. Murray, J.F. Price, et al., Hemostatic factors, inflammatory markers, and progressive peripheral atherosclerosis: the Edinburgh Artery Study. Am J Epidemiol, 2006. 163(4): p. 334-41.
129. Vaughan, D.E., PAI-1 and atherothrombosis. J Thromb Haemost, 2005. 3(8): p. 1879-83. 130. Sattar, N., H.M. Murray, P. Welsh, et al., Are markers of inflammation more strongly
associated with risk for fatal than for nonfatal vascular events? PLoS Med, 2009. 6(6): p. e1000099.
131. Ridker, P.M., M.J. Stampfer, and N. Rifai, Novel risk factors for systemic atherosclerosis: a comparison of C-reactive protein, fibrinogen, homocysteine, lipoprotein(a), and standard cholesterol screening as predictors of peripheral arterial disease. JAMA, 2001. 285(19): p. 2481-5.
132. Signorelli, S.S., M.C. Mazzarino, L. Di Pino, et al., High circulating levels of cytokines (IL-6 and TNFalpha), adhesion molecules (VCAM-1 and ICAM-1) and selectins in patients with peripheral arterial disease at rest and after a treadmill test. Vasc Med, 2003. 8(1): p. 15-9.
133. Banerjee, A.K., J. Pearson, E.L. Gilliland, et al., A six year prospective study of fibrinogen and other risk factors associated with mortality in stable claudicants. Thromb Haemost, 1992. 68(3): p. 261-3.
134. Lassila, R., S. Peltonen, M. Lepantalo, et al., Severity of peripheral atherosclerosis is associated with fibrinogen and degradation of cross-linked fibrin. Arterioscler Thromb, 1993. 13(12): p. 1738-42.
135. Jensen, S.A., L.J. Vatten, P.R. Romundstad, et al., The prevalence of intermittent claudication. Sex-related differences have been eliminated. Eur J Vasc Endovasc Surg, 2003. 25(3): p. 209-12.
136. Collins, T.C., N.J. Petersen, M. Suarez-Almazor, et al., Ethnicity and peripheral arterial disease. Mayo Clin Proc, 2005. 80(1): p. 48-54.
137. Weatherley, B.D., J.J. Nelson, G. Heiss, et al., The association of the ankle-brachial index with incident coronary heart disease: the Atherosclerosis Risk In Communities (ARIC) study, 1987-2001. BMC Cardiovasc Disord, 2007. 7: p. 3.
138. Newman, A.B. and D. Siscovick, The Cardiovascular Health Study: risk factors, subclinical disease, and clinical cardiovascular disease in older adults. Am J Geriatr Cardiol, 2004. 13(2): p. 59-60.
139. Kullo, I.J., K.R. Bailey, S.L. Kardia, et al., Ethnic differences in peripheral arterial disease in the NHLBI Genetic Epidemiology Network of Arteriopathy (GENOA) study. Vasc Med, 2003. 8(4): p. 237-42.
140. Hobbs, S.D., A.B. Wilmink, and A.W. Bradbury, Ethnicity and peripheral arterial disease. Eur J Vasc Endovasc Surg, 2003. 25(6): p. 505-12.
141. Aboyans, V., M.H. Criqui, R.L. McClelland, et al., Intrinsic contribution of gender and ethnicity to normal ankle-brachial index values: the Multi-Ethnic Study of Atherosclerosis (MESA). J Vasc Surg, 2007. 45(2): p. 319-27.
142. McLafferty, R.B., G.L. Dunnington, M.A. Mattos, et al., Factors affecting the diagnosis of peripheral vascular disease before vascular surgery referral. J Vasc Surg, 2000. 31(5): p. 870-9.
143. Kivimaki, M., G.D. Batty, A. Singh-Manoux, et al., Validating the Framingham Hypertension Risk Score: results from the Whitehall II study. Hypertension, 2009. 54(3): p. 496-501.

44
144. (ADA), A.D.A., Preventive foot care in people with diabetes. American Diabetes Association. Foot Ankle Int, 2000. 21(1): p. 76-7.
145. Gudbjörnsdottir, S., M. Miftaraj, A. Svensson, et al. Årsrapport 2008 års resultat NATIONELLA DIABETESREGISTRET (NDR). 2009.
146. Saydah, S.H., J. Fradkin, and C.C. Cowie, Poor control of risk factors for vascular disease among adults with previously diagnosed diabetes. JAMA, 2004. 291(3): p. 335-42.
147. Frykberg, R.G., The team approach in diabetic foot management. Adv Wound Care, 1998. 11(2): p. 71-7.
148. Larsen, O.A. and N.A. Lassen, Effect of daily muscular exercise in patients with intermittent claudication. Scand J Clin Lab Invest Suppl, 1967. 99: p. 168-71.
149. Leng, G.C., B. Fowler, and E. Ernst, Exercise for intermittent claudication. Cochrane Database Syst Rev, 2000(2): p. CD000990.
150. Watson, L., B. Ellis, and G.C. Leng, Exercise for intermittent claudication. Cochrane Database Syst Rev, 2008(4): p. CD000990.
151. Sahli, D., M. Svensson, J. Lidgren, et al., Evaluation of simple non-invasive techniques for assessment of lower extremity arterial disease. Clin Physiol Funct Imaging, 2005. 25(3): p. 129-34.
152. Smith, F.C., C.P. Shearman, M.H. Simms, et al., Falsely elevated ankle pressures in severe leg ischaemia: the pole test- -an alternative approach. Eur J Vasc Surg, 1994. 8(4): p. 408-12.
153. Mourad, J.J., P. Cacoub, J.P. Collet, et al., Screening of unrecognized peripheral arterial disease (PAD) using ankle-brachial index in high cardiovascular risk patients free from symptomatic PAD. J Vasc Surg, 2009.
154. Ramos, R., M. Quesada, P. Solanas, et al., Prevalence of Symptomatic and Asymptomatic Peripheral Arterial Disease and the Value of the Ankle-brachial Index to Stratify Cardiovascular Risk. Eur J Vasc Endovasc Surg, 2009.
155. Wikstrom, J., T. Hansen, L. Johansson, et al., Ankle brachial index <0.9 underestimates the prevalence of peripheral artery occlusive disease assessed with whole-body magnetic resonance angiography in the elderly. Acta Radiol, 2008. 49(2): p. 143-9.
156. Goebel, F.D. and H.S. Fuessl, Monckeberg's sclerosis after sympathetic denervation in diabetic and non-diabetic subjects. Diabetologia, 1983. 24(5): p. 347-50.
157. Niskanen, L., O. Siitonen, M. Suhonen, et al., Medial artery calcification predicts cardiovascular mortality in patients with NIDDM. Diabetes Care, 1994. 17(11): p. 1252-6.
158. Brooks, B., R. Dean, S. Patel, et al., TBI or not TBI: that is the question. Is it better to measure toe pressure than ankle pressure in diabetic patients? Diabet Med, 2001. 18(7): p. 528-32.
159. Johansson, K.E., B.R. Marklund, and J.H. Fowelin, Evaluation of a new screening method for detecting peripheral arterial disease in a primary health care population of patients with diabetes mellitus. Diabet Med, 2002. 19(4): p. 307-10.
160. Aso, Y., K. Okumura, T. Inoue, et al., Results of blood inflammatory markers are associated more strongly with toe-brachial index than with ankle-brachial index in patients with type 2 diabetes. Diabetes Care, 2004. 27(6): p. 1381-6.
161. Kalogeropoulou, K., G. Mortzos, I. Migdalis, et al., Carotid atherosclerosis in type 2 diabetes mellitus: potential role of endothelin-1, lipoperoxides, and prostacyclin. Angiology, 2002. 53(3): p. 279-85.
162. Hirai, The Value of Toe Blood Pressure Measurement in Arterial Reconstructive Surgery Vasc Endovascular Surg. , 1981. 15: p. 380-387. 163. Faccenda, F., P. Rubba, O. Vaccaro, et al., Reproducibility of non-invasive vascular diagnosis
in patients with diabetes mellitus. Artery, 1989. 16(4): p. 189-207. 164. Smith, F.C., C.P. Shearman, M.H. Simms, et al., Falsely elevated ankle pressures in severe leg
ischaemia: the pole test--an alternative approach. Eur J Vasc Surg, 1994. 8(4): p. 408-12.
•

45
165. Matzke, S., M. Franckena, A. Alback, et al., Ankle brachial index measurements in critical leg ischaemia--the influence of experience on reproducibility. Scand J Surg, 2003. 92(2): p. 144-7.
166. Aboyans, V., P. Lacroix, A. Lebourdon, et al., The intra- and interobserver variability of ankle-arm blood pressure index according to its mode of calculation. J Clin Epidemiol, 2003. 56(3): p. 215-220.
167. Kennedy, M., C. Solomon, T.A. Manolio, et al., Risk factors for declining ankle-brachial index in men and women 65 years or older: the Cardiovascular Health Study. Arch Intern Med, 2005. 165(16): p. 1896-902.
168. Calles-Escandon, J. and M. Cipolla, Diabetes and endothelial dysfunction: a clinical perspective. Endocr Rev, 2001. 22(1): p. 36-52.
169. Danielsson, P., L. Truedsson, K.F. Eriksson, et al., Inflammatory markers and IL-6 polymorphism in peripheral arterial disease with and without diabetes mellitus. Vasc Med, 2005. 10(3): p. 191-8.
170. McDermott, M.M., K. Liu, L. Ferrucci, et al., Circulating blood markers and functional impairment in peripheral arterial disease. J Am Geriatr Soc, 2008. 56(8): p. 1504-10.
171. Kooistra, T., Y. Schrauwen, J. Arts, et al., Regulation of endothelial cell t-PA synthesis and release. Int J Hematol, 1994. 59(4): p. 233-55.
172. Tzoulaki, I., G.D. Murray, A.J. Lee, et al., Inflammatory, haemostatic, and rheological markers for incident peripheral arterial disease: Edinburgh Artery Study. Eur Heart J, 2007. 28(3): p. 354-62.
173. Aronow, H. and W.R. Hiatt, The burden of peripheral artery disease and the role of antiplatelet therapy. Postgrad Med, 2009. 121(4): p. 123-35.
174. Criqui, M.H., M.J. Alberts, F.G. Fowkes, et al., Atherosclerotic Peripheral Vascular Disease Symposium II: screening for atherosclerotic vascular diseases: should nationwide programs be instituted? Circulation, 2008. 118(25): p. 2830-6.

•