-
7/27/2019 Early Antipsychotic Response to Aripiprazole in
Adolescents With Schizophrenia
1/13
NEW RESEARCH
Early Antipsychotic Response to Aripiprazolein Adolescents With
Schizophrenia: Predictive
Value for Clinical OutcomesChristoph U. Correll, M.D., Joan
Zhao, Ph.D., William Carson, M.D., Ron Marcus, M.D.,
Robert McQuade, Ph.D., Robert A. Forbes, Ph.D., Raymond
Mankoski, M.D.
Objective: In adults with chronic schizophrenia, most symptom
decreases occur in the firstfew weeks of antipsychotic treatment,
and nonresponse at week 2 predicts a later nonre-sponse. The
trajectory of antipsychotic response and the predictive value of
early anti-psychotic effects were investigated for ultimate outcome
in adolescent schizophrenia, where
such data are still lacking. Method: This post hoc analysis of a
6-week, randomized,double-blinded trial of aripiprazole (n 196)
versus placebo (n 98) evaluated if adolescents13 to 17 years old
with schizophrenia exhibited substantial symptomatic improvement
toaripiprazole in the first few treatment weeks and whether early
response (ER) versus earlynonresponse (ENR) predicted clinically
relevant outcomes. ER decreased at least 20% and ENRdecreased less
than 20% in Positive and Negative Syndrome Scale (PANSS) total
score at week2 (ER2/ENR2) or 3 (ER3/ENR3). Ultimate response
decreased at least 40% in PANSSscore. Results: Nearly 50% of the
PANSS decrease was achieved by week 2 and up to 75% byweek 3.
ER2/ER3 subjects showed significantly greater improvement than ENR
subjects inPANSS total score, PANSS positive and negative subscale
scores, and functionally relevantoutcomes. In general, ER3 had
better sensitivity, specificity, and positive and
negativepredictive values than ER2 for predicting ultimate
response. ER2 subjects were 8.8 times (95%confidence interval
4.019.4) and ER3 subjects were 8.6 times (95% confidence interval
4.516.6)more likely to achieve remission at week 6 (p < .0001)
than ENR2 and ENR3 subjects,
respectively, although adverse events were similar. Conclusions:
Like adults with chronicschizophrenia, adolescents with early-phase
schizophrenia exhibited most symptomaticimprovement early during
aripiprazole treatment, with week 3 improvements having the
best predictive power. Although requiring extension, these
results may inform clinical de-cision making. Clinical trial
registration informationAripiprazole in Adolescents
withSchizophrenia, http://clinicaltrials.gov/, NCT00102063. J. Am.
Acad. Child Adolesc. Psychiatry,2013;52(7):689698. Key Words:
adolescent schizophrenia, antipsychotics, early response,remission,
response prediction
A
bout one third of subjects with schizo-phrenia develop their
first symptomsbefore reaching adulthood, with onset
of symptoms during adolescence being rela-tively common.1 Most
affected individuals havesubstantial lifelong impairment and more
than
50% require continuous support, whether livingin the community
or in institutions.2 In addition,adolescent-onset schizophrenia is
associated
with greater functional impairments than adult-onset
schizophrenia.3,4 For these reasons, earlyrecognition and
interventions are particularlyimportant.5
Antipsychotics are the mainstay of schizo-phrenia treatment, and
their initiation should aimto balance efficacy, tolerability, and
acceptability2
to minimize the risk of exposure to ineffectivetreatments and
the occurrence of unnecessary orunacceptable adverse effects.
Furthermore, earlyprediction of response to a given antipsychotic
is
This article is discussed in an editorial by Dr. Linmarie Sikich
onpage 677.
Clinical guidance is available at the end of this article.
Supplemental material cited in this article is available
online.
JOURNAL OF THE
AMERICAN
ACADEMY OF
CHILD &
ADOLESCENT
PSYCHIATRY
VOLUME 52 NUMBER 7 JULY 2013 www.jaacap.org 689
http://clinicaltrials.gov/http://www.jaacap.org/http://www.jaacap.org/http://clinicaltrials.gov/
-
7/27/2019 Early Antipsychotic Response to Aripiprazole in
Adolescents With Schizophrenia
2/13
important,6,7 because long-term treatment is fun-damental to the
management of schizophreniasymptoms, and time spent on ineffective
treat-ment should be minimized. Recent evidence hasshown that in
adults with chronic schizophrenia,
less than minimal treatment response at weeks 1to 3 predicts an
ultimate nonresponse at studyendpoint with high predictive
validity.8-15
Therefore, identifying adolescents with schizo-phrenia who may
not respond to and/or remit ona chosen treatment could be a
powerful tool thatenables clinicians to formulate treatment
regi-mens that shorten the exposure to ineffectiveagents and that
increase the likelihood ofachieving optimal symptomatic
remission.
Clinical decision making usually tries tobalance efficacy and
tolerability. Atypical anti-psychotics have been favored in the
treatmentof adolescents with psychotic disorders,16 be-cause in
adults and adolescents they are at leastas efficacious as typical
antipsychotics3,16-20 andare associated with a decreased risk of
devel-oping extrapyramidal symptoms (EPSs), adverseeffects to which
pediatric subjects are particu-larly vulnerable.1,18,21-23 However,
atypical anti-psychotics have been associated with differentdegrees
of weight gain and metabolic abnor-malities, and pediatric subjects
also seem to beparticularly vulnerable to these
effects.20-22,24,25
Such safety concerns with atypical antipsy-
chotics have been highlighted through findingsfrom the Treatment
of Early-Onset Schizo-phrenia Spectrum Disorders (TEOSS)
study,20
although during maintenance treatment differ-ences to typical
antipsychotics became lesspronounced.26 The decreased incidence of
EPSsobserved with atypical antipsychotics as a classhas been
associated with their binding affinityto dopamine-2 and their
antagonist activity atserotonin-2A receptors. In addition, weight
gainand metabolic abnormalities have been attrib-uted to several
receptor systems, including theserotonin-2C, dopamine-2, and
histaminer-
gic and cholinergic receptors.25,27 However, thereceptor-binding
affinity varies among antipsy-chotics,28-30 which is likely the
reason for differ-ences in adverse-effect profiles that have
beensuggested as the main guiding principle formaking a treatment
choice in the absence ofgeneral efficacy differences among most
anti-psychotics in adults30,31 and in youths.21 Never-theless, in
the event that early nonresponse(ENR) to a specific agent and in a
given patient issufficiently predictive of ultimate
nonresponse,
this individual response pattern can be used tomore precisely
balance observed efficacy withtolerability effects.
Aripiprazole is a partial agonist of dopamine-2,dopamine-3, and
serotonin-2A receptors.32-35
Together with olanzapine, paliperidone, quetia-pine, and
risperidone, aripiprazole is approved bythe U.S. Food and Drug
Administration for thetreatment of adolescents with
schizophrenia.16,36
Although these agents have each demonstratedefficacy in at least
one placebo-controlled trial,more information is needed to help
refine thetreatment decision process to identify adolescentswith
schizophrenia who may not respond and/orremit on a chosen treatment
to shorten their ex-posure to ineffective agents and to increase
thelikelihood of achieving optimal symptomaticremission. Therefore,
the objective of the presentanalysis was to assess if, analogous to
observa-tions in adults with chronic schizophrenia,adolescents
receiving aripiprazole for the treat-ment of schizophrenia exhibit
symptomatic de-creases early during treatment and whether
earlyresponse (ER) versus ENR (at week 2 or 3 oftreatment) is a
useful marker to predict relevantclinical outcomes at a later time
point. To theauthors knowledge, this is the first such analysisfor
any antipsychotic to be published on an ado-lescent population.
METHODStudy Design and SubjectsThis was a post hoc analysis of
data from a phaseIII, multinational, multicenter, 6-week,
randomized,double-blinded, placebo-controlled, fixed-dose
trialinvestigating the efficacy of aripiprazole (10 or 30 mg)in
adolescents with schizophrenia. Full details of thestudy design and
inclusion and exclusion criteria have
been published previously.37
In brief, eligible subjects were adolescents 13 to17 years old
with an Axis I primary diagnosis ofschizophrenia (DSM-IV).38 The
diagnosis was con-firmed by a child psychiatrist at the time of
screening,
using the Schedule for Affective Disorders andSchizophrenia for
School-Age ChildrenPresent andLifetime Version,39 and subjects were
required to havea baseline Positive and Negative Syndrome
Scale(PANSS)40 total score of at least 70. Exclusion
criteriaincluded a history or current diagnosis of
mentalretardation, major depressive episodes, and schizo-affective
disorder. Subjects also were excluded if 2previous trials of
different antipsychotics had failed.
Prohibited medications, including mood
stabilizers,antidepressants, and other psychotropics, were
dis-continued at least 3 days before initiating treatment.
JOURNAL OF THE
AMERICAN
ACADEMY OF
CHILD &
ADOLESCENT
PSYCHIATRY
690 www.jaacap.org VOLUME 52 NUMBER 7 JULY 2013
CORRELL et al.
http://www.jaacap.org/http://www.jaacap.org/
-
7/27/2019 Early Antipsychotic Response to Aripiprazole in
Adolescents With Schizophrenia
3/13
Subjects were permitted to receive rescue
medications(benzodiazepine or anticholinergic medications) dur-ing
the study for relief of transient symptoms.
Written informed consent was obtained from allsubjects guardians
or legal representatives and writtenassent was obtained from each
adolescent subject. Theprotocol, procedures, consent, and assent
statementswere approved by the institutional review board orethics
committee of each participating center.
Efficacy AssessmentsThe primary efficacy endpoint was mean
change from
baseline to week 6 (last observation carried forward[LOCF]) in
the PANSS total score. Other efficacyoutcome measurements included
the PANSS positiveand negative subscales, Clinical Global
ImpressionsImprovement (CGI-I) scale, CGISeverity scale(CGI-S),41
Childrens Global Assessment Scale,42
and the Pediatric Quality of Life Enjoyment and
Satisfaction Scale.43
Safety AssessmentsSafety outcomes included frequency of adverse
eventsand changes in weight and metabolic measurements.Drug-related
movement disorders were assessed withthe Simpson-Angus Scale,44 the
Barnes AkathisiaRating Scale,45 and the Abnormal Involuntary
Move-ment Scale46 at every study week.
Statistical AnalysisThe focus of this study was to characterize
and predictthe trajectory of treatment response to aripiprazole
in
adolescents with schizophrenia. For the time course
ofsymptomatic improvement, analyses were performedseparately for
the 10-mg and the 30-mg arms becausethe time course of separation
from placebo in the 2arms was different in the original study.37
However,
because the results of the predictive value of ERversus ENR were
similar for the 10-mg and 30-mgdose arms, the 2 doses were combined
in the anal-yses to lessen the complexity of the presented
data.Although this was a placebo-controlled trial, as inprior
analyses of adult studies, this report focuses onthe antipsychotic
response pattern to inform treatmentdecisions.
For the purpose of this post hoc analysis, ER was
defined as a decrease of at least 20% in PANSS totalscore at
study week 2 (ER2) or study week 3 (ER3).ENR was defined as a
decrease less than 20% in PANSStotal score at study week 2 (ENR2)
or study week 3(ENR3). Ultimate response (UR) was defined asa
decrease in PANSS total score at study endpoint(week 6, LOCF) of at
least 20% (UR20), at least 30%(UR30), or at least 40% (UR40). These
cutoffs were used
because they had been used in prior studies, andbecause a
decrease of at least 20% in the PANSS totalscore correlates roughly
with minimally improvedon the CGI-I, whereas a decrease of at least
40% to 50%
corresponds to much improved on the CGI-I.47
Remission was defined cross-sectionally as a score ofno higher
than 3 (mild or less) on the following 8PANSS items at the end of
the study (LOCF afterweek 2 assessment), using the remission
criteria byAndreasen et al.48: P1 (delusions), P2
(conceptualdisorganization), P3 (hallucinatory behavior), G9
(un-usual thought content), G5 (mannerisms/posturing),N1 (blunted
affect), N4 (social withdrawal), and N6(lack of spontaneity/flow of
conversation). For com-parisons with prior studies on this topic,
the percent-ages of decrease in the total PANSS score
usinguncorrected PANSS scores, i.e., without subtraction ofthe 30
points representing absent symptoms, werecalculated.
The ER and ENR groups were compared usingdescriptive statistics
for patient demographics and
baseline characteristics and mixed models repeatedmeasures
analyses to compare the ER and ENR groups
on the PANSS total, positive, and negative scores,CGI-S, CGI-I,
Pediatric Quality of Life Enjoymentand Satisfaction Scale scores,
and Childrens GlobalAssessment Scale scores. Odds ratios were
calculat-ed for comparisons of endpoint response status(!20%, !30%,
!40%, and !50% decreases in PANSStotal score) and cross-sectional
remission at LOCFstudy endpoint beyond week 2 for the ER2
versusENR2 and the ER3 versus ENR3 groups.
Sensitivity, specificity, positive predictive value(PPV), and
negative predictive value (NPV) wereevaluated to determine the
accuracy of ER/ENR2 andER/ENR3 in predicting different levels of UR
at week6 (LOCF) and to determine the accuracy of predicting
remission for the ER2 and ER3 groups.Moreover, receiver
operating characteristic (ROC)
curves for ERs at weeks 2 and 3 with respect to de-crease in
PANSS total score (predicting !20%, !30%,or !40% or at week 6) were
calculated to determine thePANSS total score threshold at weeks 2
and 3 with the
best predictive power for UR at week 6.
RESULTSIn total, 302 adolescents with schizophrenia(1317 years
old) participated in this 6-week,randomized, double-blinded,
placebo-controlledtrial of aripiprazole versus placebo. Relevant
data
were available for 196 subjects who received ari-piprazole 10 mg
(n 99) or 30 mg (n 97) andhad a baseline PANSS total score of 94.0
and95.0, respectively. Overall, 32.7% (n 64) ach-ieved ER status at
week 2, and 48.9% (n 96)achieved ER status at week 3. Baseline
patientand illness characteristics of subjects with ER2/ENR2 and
ER3/ENR3 to aripiprazole treatmentwere similar (Table 1).
Patient disposition has been described indetail previously.37
Overall, 83% of aripiprazole-
JOURNAL OF THE
AMERICAN
ACADEMY OF
CHILD &
ADOLESCENT
PSYCHIATRY
VOLUME 52 NUMBER 7 JULY 2013 www.jaacap.org 691
EARLY RESPONSE TO ARIPIPRAZOLE IN ADOLESCENTS
http://www.jaacap.org/http://www.jaacap.org/
-
7/27/2019 Early Antipsychotic Response to Aripiprazole in
Adolescents With Schizophrenia
4/13
treated subjects completed the study. The mainreasons for
discontinuation for subjects receiv-ing aripiprazole were
withdrawal of consent(4.0% and 11.8% for the 10-mg and 30-mg
arms,respectively), adverse events (7.0% and 3.9%,respectively),
and lack of efficacy (5.0% and1.0%, respectively).
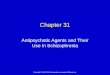
Efficacy OutcomesSymptom decrease was greatest in the first 2 to
3weeks of treatment. By week 1, subjects in the
10-mg arm had attained 24% of the decrease thatthey ultimately
achieved in their PANSS totalscore at week 6. These subjects
attained decreasesof 51% by week 2 and 68% by week 3. Subjects
inthe 30-mg arm exhibited 33% of their overalldecrease at week 1, a
decrease of 49% by week 2,and a decrease of 75% by week 3. In the 2
arms,after week 3, incremental gains were less than15% for each
subsequent week (Figure 1).
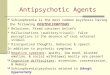
The decrease in PANSS total score was signif-icantly greater for
ER2 versus ENR2 subjects from
week 1 to week 6 at each time point (Figure 2a).At week 6, PANSS
total score changes were 41.6versus 22.0 (p < .0001; Table 2).
Results weresimilar when using week 3 to determine ER status(Figure
2b), with endpoint decreases of 40.6versus 16.5 (p < .0001) for
ER3 versus ENR3subjects, respectively (Table 2). Similar
findingswere observed across each time point from week1 to week 6
for PANSS positive subscale scores(Figure S1, available online).
Except for PediatricQuality of Life Enjoyment and Satisfaction
Scale
overall score in the ER/ENR2 groups, all otherrelevant
measurements of efficacy similarlydemonstrated highly statistically
significant andclinically meaningful differences favoring ERversus
ENR subjects (Table 2).
For subjects with an ER2, proportionsachieving UR at week 6 were
95.3% for UR20,82.8% for UR30, and 67.2% for UR40. For subjectswith
an ER3, proportions achieving UR at week6 were 97.9%, 82.3%, and
61.5% for UR20,UR30, and UR40, respectively. UR rates were
TABLE 1 Baseline Demographic and Psychiatric Characteristics of
Subjects With an Early Response Versus EarlyNonresponse at Study
Week 2 or 3
Week 2 Week 3Aripiprazole Aripiprazole
(N 196) (N 196)
Early Nonresponder Early Responder Early Nonresponder Early
Responder(n 132) (n 64) (n 100) (n 96)
Age (y), mean (SD) 15.5 (1.3) 15.5 (1.4) 15.5 (1.2) 15.4
(1.5)Race, n (%)
Caucasian 78 (59.0) 34 (53.1) 65 (65.0) 47 (48.9)Black/African
American 20 (15.2) 8 (12.5) 13 (13.0) 15 (15.6)Asian 16 (12.1) 12
(18.8) 10 (10.0) 18 (18.8)Other 18 (13.6) 10 (15.6) 12 (12.0) 16
(16.7)
Ethnicity, n (%)Non-Hispanic/Latino 114 (86.4) 55 (85.9) 87
(87.0) 82 (85.4)
Weight (kg), mean (SD) 62.8 (15.7) 66.1 (20.9) 62.3 (14.4) 65.6
(20.4)BMI (kg/m2), mean (SD) 22.8 (4.7) 24.0 (6.7) 22.6 (4.6) 23.9
(6.2)Psychiatric characteristics
Disease duration (y), mean (SD) 1.3 (1.9) 1.5 (2.1) 1.5 (2.1)
1.3 (1.8)Age at onset (y), mean (SD) 14.2 (2.2) 14.1 (2.6) 14.1
(2.3) 14.2 (2.3)Onset before age 13 years, n (%) 19 (14.4) 11
(17.2) 15 (15.0) 15 (15.6)On any psychotropic treatment before
study entry, n (%)96 (72.7) 49 (76.6) 74 (74.0) 71 (74.0)
Used antipsychotic before studyentry, n (%)
61 (46.2) 37 (57.8) 41 (41.0) 57 (59.4)
PANSS total, mean (SD) 94.3 (15.6) 94.4 (15.8) 93.4 (15.9) 95.3
(15.3)PANSS positive, mean (SD) 22.8 (5.1) 22.8 (4.9) 22.9 (5.4)
22.7 (4.6)PANSS negative, mean (SD) 25.1 (6.6) 25.3 (6.2) 24.7
(6.0) 25.6 (7.0)CGI-S, mean (SD) 4.5 (0.7) 4.5 (0.8) 4.5 (0.7) 4.5
(0.7)
Note: Subjects with an early response showed a decrease of at
least 20% from baseline to endpoint (last observation carried
forward) in Positive and
Negative Syndrome Scale (PANSS) total score. BMI body mass
index; CGI-S Clinical Global ImpressioneSeverity.
JOURNAL OF THE
AMERICAN
ACADEMY OF
CHILD &
ADOLESCENT
PSYCHIATRY
692 www.jaacap.org VOLUME 52 NUMBER 7 JULY 2013
CORRELL et al.
http://www.jaacap.org/http://www.jaacap.org/
-
7/27/2019 Early Antipsychotic Response to Aripiprazole in
Adolescents With Schizophrenia
5/13
significantly higher for ER than for ENR subjectsat each level
of UR and for the 2 ER time points(Table 2).
Remission at study endpoint was achieved by55.6% (n 109/196) of
subjects receiving aripi-prazole, 53.5% (n 53/99) in the 10-mg arm,
and57.7% (n 56/97) in the 30-mg arm. ER2 subjectshad significantly
higher rates of remission thanENR2 subjects (86.0% versus 41.0%; p
< .0001).The same was true for ER3 versus ENR3 subjects
(80.0% versus 32.0%; p2-week) antipsychotic treatment in
adolescentswith schizophrenia. Future studies with
otherantipsychotics in youth with schizophrenia areneeded to better
characterize the predictive valueof ER/ENR to antipsychotics in
youth withearly-onset schizophrenia. &
Accepted May 1, 2013.
Dr. Correll is with the Zucker Hillside Hospital, Hofstra North
ShoreLong Island Jewish School of Medicine, and Albert Einstein
College ofMedicine. Drs. Zhao, Carson, McQuade, and Forbes are with
OtsukaPharmaceutical Development and Commercialization. Dr. Marcus
iswith Bristol-Myers Squibb. Dr. Mankoski is with Genzyme.
This study was supported by Bristol-Myers Squibb and Otsuka
Phar-maceutical Co., Ltd.
Editorial support for the preparation of this manuscript was
provided byOgilvy Healthworld Medical Education; funding was
provided byBristol-Myers Squibb. The authors thank the participants
and theirfamilies for their involvement in this study.
Disclosure: Dr. Correll has received grant or research support
from theNational Institute of Mental Health, Bristol-Myers
Squibb/Otsuka, theFeinstein Institute for Medical Research,
Janssen/Johnson and Johnson,and the National Alliance for Research
in Schizophrenia andDepression. He has served as a consultant to
Actelion, Alexza, theAmerican Academy of Child and Adolescent
Psychiatry, AstraZeneca,Bristol-Myers Squibb, Eli Lilly and Co.,
Genentech, the Gerson LehrmanGroup, IntraCellular Therapies,
Lundbeck, Medavante, Medscape,Merck, National Institute of Mental
Health, Janssen/Johnson and
Johnson, Otsuka, Pfizer, ProPhase, Roche, Sunovion, Takeda,
Teva,
and Vanda. He has served on the speakers
bureau of Merck (non-promotional lectures only). He owns stock
in Alexza. He has partici-pated in Continuing Medical Education
article preparation forMedscape. He is a member of the Data Safety
Monitoring Boardsfor Cephalon, Janssen/Johnson and Johnson,
Lundbeck, Pfizer,Takeda, and Teva. Dr. Forbes is a former employee
of Genentech.Dr. Mankoski is a former employee and stockholder of
Bristol-MyersSquibb. Drs. Zhao, Carson, Marcus, and McQuade report
nobiomedical financial interests or potential conflicts of
interest.
Correspondence to Christoph U. Correll, M.D., Division of
PsychiatryResearch, The Zucker Hillside Hospital, Glen Oaks, NY
11004;e-mail: [email protected]
0890-8567/$36.00/2013 American Academy of Child andAdolescent
Psychiatry
http://dx.doi.org/10.1016/j.jaac.2013.04.018
REFERENCES1. Young CM, Findling RL. Pharmacologic treatment of
adolescent
and child schizophrenia. Expert Rev Neurotherapeut.
2004;4:53-60.
2. Mattai AK, Hill JL, Lenroot RK. Treatment of early-onset
schizo-phrenia. Curr Opin Psychiatry. 2010;23:304-310.
3. Sikich L. Efficacy of atypical antipsychotics in early-onset
schizo-phrenia and other psychotic disorders. J Clin Psychiatry.
2008;69(suppl 4):21-25.
4. American Academy of Child and Adolescent Psychiatry.
Practiceparameter for the assessment and treatment of children
andadolescents with schizophrenia. J Am Acad Child
AdolescPsychiatry. In press.
5. Bodnar M, Malla A, Joober R, Lepage M. Cognitive markers
ofshort-term clinical outcome in first-episode psychosis. Br
J Psychiatry. 2008;19 3:297-304.6. Salimi K, Jarskog LF,
Lieberman JA. Antipsychotic drugs for first-
episode schizophrenia: a comparative review. CNS Drugs.
2009;23:837-855.
7. Agid O, Kapur S, Arenovich T, Zipursky RB.
Delayed-onsethypothesis of antipsychotic action: a hypothesis
tested and rejec-ted. Arch Gen Psychiatry. 2003;60:1228-1235.
8. Kinon BJ, Chen L, Ascher-Svanum H, et al. Predicting response
toatypical antipsychotics based on early response in the treatment
ofschizophrenia. Schizophr Res. 2008;102:230-240.
9. Correll CU, Malhotra AK, Kaushik S, McMeniman M, Kane
JM.Early prediction of antipsychotic response in schizophrenia.
Am
J Psychiatry. 2003;16 0:2063-2065.10. Leucht S, Busch R, Hamann
J, Kissling W, Kane J. Early-onset
hypothesis of antipsychotic drug action: a hypothesis
tested,confirmed and extended. Biol Psychiatry.
2005;57:1543-1549.
Clinical Guidance
In youth with multiepisode schizophrenia who haveless than
minimal improvement despite a 3-week trialwith an adequately dosed
antipsychotic agent withconfirmed adherence (e.g., supervised
medicationingestion), a switch to another antipsychotic shouldbe
considered, unless clear triggers for the psychosis(such as
environmental, substances, [partial] non-adherence) exist that
should be addressed first.
This suggested guidance for youth withschizophrenia is currently
based on 1 aripiprazoletrial and needs to be considered in the
context ofrecent American Academy of Child and AdolescentPsychiatry
guidelines, which state that a 6-week trialof an adequately dosed
antipsychotic should beconducted before switching to a different
antipsy-chotic agent.4
Dosing/titration schedules need to be factored intothe timing of
declaring whether a patient is an earlyresponder or
nonresponder.
JOURNAL OF THE
AMERICAN
ACADEMY OF
CHILD &
ADOLESCENT
PSYCHIATRY
VOLUME 52 NUMBER 7 JULY 2013 www.jaacap.org 697
EARLY RESPONSE TO ARIPIPRAZOLE IN ADOLESCENTS
mailto:[email protected]://dx.doi.org/10.1016/j.jaac.2013.04.018http://www.jaacap.org/http://www.jaacap.org/http://dx.doi.org/10.1016/j.jaac.2013.04.018mailto:[email protected]
-
7/27/2019 Early Antipsychotic Response to Aripiprazole in
Adolescents With Schizophrenia
10/13
11. Leucht S, Busch R, Kissling W, Kane JM. Early prediction
ofantipsychotic nonresponse among patients with schizophrenia.
J Clin Psychiatry. 2007;68:352-360.12. Kinon BJ, Chen L,
Ascher-Svanum H, et al. Early response
to antipsychotic drug therapy as a clinical marker of
subse-quent response in the treatment of schizophrenia.
Neuro-psychopharmacology. 2010;35:581-590.
13. Chang YC, Lane HY, Yang KH, Huang CL. Optimizing
earlyprediction for antipsychotic response in schizophrenia. J
ClinPsychopharmacol. 2006;26:554-559.
14. Ascher-Svanum H, Nyhuis AW, Faries DE, Kinon BJ, Baker
RW,Shekhar A. Clinical, functional, and economic ramifications
ofearly nonresponse to antipsychotics in the naturalistic treatment
ofschizophrenia. Schizophr Bull. 2008;34:1163-1171.
15. Lin C, Chou L, Lin C, Hsu C, Chen Y, Lane HY.
Earlyprediction of clinical response in schizophrenia patients
re-ceiving the atypical antipsychotic zotepine. J Clin
Psychiatry.2007;68:1522-1527.
16. Correll CU, Kratochvil CJ, March JS. Developments in
pediatricpsychopharmacology: focus on stimulants, antidepressants,
andantipsychotics. J Clin Psychiatry. 2011;72:655-670.
17. Fraguas D, Correll CU,Merchan-Naranjo J, et al. Efficacy
andsafetyof second-generation antipsychotics in children and
adolescentswith psychotic and bipolar spectrum disorders:
comprehensivereview of prospective head-to-head and
placebo-controlled com-
parisons. Eur Neuropsychopharmacol. 2011;21:621-645.18. Kumra S,
Oberstar JV, Sikich L, et al. Efficacy and tolerability of
second-generation antipsychotics in children and adolescents
withschizophrenia. Schizophr Bull. 2008;34:60-71.
19. Sikich L, Hamer RM, Bashford RA, Sheitman BB, Lieberman JA.A
pilot study of risperidone, olanzapine, and haloperidol inpsychotic
youth: a double-blind, randomized, 8-week trial.
Neu-ropsychopharmacology. 2004;29:133-145.
20. Sikich L, Frazier JA, McClellan J, et al. Double-blind
comparison offirst- and second-generation antipsychotics in
early-onset schizo-phrenia and schizo-affective disorder: findings
from the Treatmentof Early-Onset Schizophrenia Spectrum Disorders
(TEOSS) study.Am J Psychiatry. 2008;165:1420-1431.
21. Correll CU. Antipsychotic use in children and adolescents:
mini-mizing adverse effects to maximize outcomes. J Am Acad
ChildAdolesc Psychiatry. 2008;47:9-20.
22. Correll CU. Assessing and maximizing the safety and
tolerabilityof antipsychotics used in the treatment of children and
adoles-
cents. J Clin Psychiatry. 2008;69(suppl 4):26-36.23. Correll CU,
Kane JM. One-year incidence rates of tardive dyski-
nesia in children and adolescents treated with
second-generationantipsychotics: a systematic review. J Child
Adolesc Psycho-pharmacol. 2007;17:647-656.
24. Correll CU, Manu P, Olshanskiy V, Napolitano B, Kane
JM,Malhotra AK. Cardiometabolic risk of second-generation
anti-psychotic medications during first-time use in children
andadolescents. JAMA. 2009;302:1765-1773.
25. De Hert M, Dobbelaere M, Sheridan EM, Cohen D, Correll
CU.Metabolic and endocrine adverse effects of
second-generationantipsychotics in children and adolescents: a
systematic reviewof randomized, placebo controlled trials and
guidelines for clinicalpractice. Eur Psychiatry.
2011;26:144-158.
26. Findling RL, Johnson JL, McClellan J, et al. Double-blind
mainte-nance safety and effectiveness findings from the Treatment
ofEarly-Onset Schizophrenia Spectrum (TEOSS) study. J Am AcadChild
Adolesc Psychiatry. 2010;49:583-594; quiz 632.
27. Correll CU, Lencz T, Malhotra AK. Antipsychotic drugs
andobesity. Trends Mol Med. 2011;17:97-107.
28. Stahl SM, Shayegan DK. The psychopharmacology of
ziprasidone:receptor-binding properties and real-world psychiatric
practice.
J Clin Psychiatry. 2003;64(suppl 19):6-12.29. Farah A.
Atypicality of atypical antipsychotics. Prim Care
Companion J Clin Psychiatry. 2005;7:268-274.30. Correll CU. From
receptor pharmacology to improved outcomes:
individualising the selection, dosing, and switching of
antipsy-chotics. Eur Psychiatry. 2010;25(suppl 2):S12-S21.
31. KaneJM, CorrellCU. Past andpresent progress in
thepharmacologictreatment of schizophrenia. J Clin Psychiatry.
2010;71:1115-1124.
32. Burris KD, Molski TF, Xu C, et al. Aripiprazole, a novel
antipsy-chotic, is a high-affinity partial agonist at human
dopamine D2receptors. J Pharmacol Exp Ther. 2002;302:381-389.
33. Tadori Y, Forbes RA, McQuade RD, Kikuchi T. Characterization
ofaripiprazole partial agonist activity at human dopamine D
receptors. Eur J Pharmacol. 2008;597:27-33.34. Jordan S,
Koprivica V, Dunn R, Tottori K, Kikuchi T, Altar CA.In vivo effects
of aripiprazole on cortical and striatal dopami-nergic and
serotonergic function. Eur J Pharmacol. 2004;483:45-53.
35. Jordan S, Koprivica V, Chen R, Tottori K, Kikuchi T, Altar
CA. Theantipsychotic aripiprazole is a potent, partial agonist at
the human5-HT(1A) receptor. Eur J Pharmacol. 2002;441:137-140.
36. Kuehn BM. FDA panel OKs 3 antipsychotic drugs for
pediatricuse, cautions against overuse. JAMA. 2009;302:833-834.
37. Findling RL, Robb A, Nyilas M, et a l. A
multiple-center,randomized, double-blind, placebo-controlled study
of oral ari-piprazole for treatment of adolescents with
schizophrenia. Am JPsychiatry. 2008;165:1432-1441.
38. American Psychiatric Association. Diagnostic and
StatisticalManual of Mental Disorders. 4th ed, text rev.
Washington, DC:American Psychiatric Publishing; 2000.
39. Kaufman J, Birmaher B, Brent D, et al. Schedule for
AffectiveDisorders and Schizophrenia for School-Age
Children-Present and
Lifetime Version (K-SADS-PL): initial reliability and validity
data.J Am Acad Child Adolesc Psychiatry. 1997 ;36:980-988.
40. Kay SR, Opler LA, Lindenmayer JP. Reliability and validity
of thepositive and negative syndrome scale for schizophrenics.
Psychi-atry Res. 1988;23:99-110.
41. Guy W. Clinical Global Impressions (CGI). ECDEU
AssessmentManual for Psychopharmacology. US Department of
Health,Education, and Welfare Publication (ADM) 76-338. Rockville,
MD:National Institute of Mental Health; 1976; 218-222.
42. Shaffer D, Gould MS, Brasic J, et al. A Childrens Global
Assess-ment Scale (CGAS). Arch Gen Psychiatry.
1983;40:1228-1231.
43. Endicott J, Nee J, Yang R, Wohlberg C. Pediatric Quality of
LifeEnjoyment and Satisfaction Questionnaire (PQ-LES-Q):
reliabilityand validity. J Am Acad ChildAdolesc
Psychiatry.2006;45:401-407.
44. Simpson GM, Angus JW. A rating scale for extrapyramidal
sideeffects. Acta Psychiatr Scand Suppl. 1970;212:11-19.
45. Barnes TR. A rating scale for drug-induced akathisia. Br
JPsychiatry. 1989;154:672-676.
46. Guy W. Abnormal Involuntary Movement Scale (AIMS).
USDepartment of Health Education and Welfare. ECDEU Assess-ment
Manual for Psychopharmacology. Rockville, MD: NationalInstitute of
Mental Health; 1976; 534-537.
47. Leucht S, Kane JM, Etschel E, Kissling W, Hamann J, Engel
RR.Linking the PANSS, BPRS, and CGI: clinical implications.
Neu-ropsychopharmacology. 2006;31:2318-2325.
48. Andreasen NC, Carpenter WT Jr, Kane JM, Lasser RA, Marder
SR,Weinberger DR. Remission in schizophrenia: proposed criteriaand
rationale for consensus. Am J Psychiatry. 2005;162:441-449.
49. Schimmelmann BG, Schmidt SJ, Carbon M, Correll CU.
ARational, Evidence Informed Approach to Psychopharmacologyfor
Adolescents with Early Onset, First Episode Psychoses. CurrOpin
Psychiatry. 2013;26:219-230.
50. Gallego JA, Robinson DG, Sevy SM, et al. Time to
treatmentresponse in first-episode schizophrenia: should acute
treatmenttrials last several months? J Clin Psychiatry.
2011;72:1691-1696.
51. Derks EM, Fleischhacker WW, Boter H, Peuskens J, Kahn
RS.Antipsychotic drug treatment in first-episode psychosis:
shouldpatients be switched to a different antipsychotic drug after
2, 4, or6 weeks of nonresponse? J Clin Psychopharmacol.
2010;30:176-180.
52. Emsley R, Rabinowitz J, Medori R. Time course for
antipsychotictreatment response in first-episode schizophrenia. Am
J Psychi-atry. 2006;163:743-745.
53. Emsley R, Oosthuizen PP, Kidd M, Koen L, Niehaus DJ,Turner
HJ. Remission in first-episode psychosis: predictor vari-ables and
symptom improvement patterns. J Clin Psychiatry.
2006;67:1707-1712.
JOURNAL OF THE
AMERICAN
ACADEMY OF
CHILD &
ADOLESCENT
PSYCHIATRY
698 www.jaacap.org VOLUME 52 NUMBER 7 JULY 2013
CORRELL et al.
http://www.jaacap.org/http://www.jaacap.org/
-
7/27/2019 Early Antipsychotic Response to Aripiprazole in
Adolescents With Schizophrenia
11/13
FIGURE S1 Mean change from baseline to endpoint in Positive and
Negative Syndrome Scale (PANSS) positivesubscale scores for
subjects receiving aripiprazole treatment exhibiting (a) early
response at week 2 (ER2) versus earlynonresponse at week 2 (ENR2)
and (b) ER3 versus ENR3 by study week. Note: p< .0001 at each
time point. Meanbaseline PANSS positive subscale scores for ER2
(aripiprazole): 22.8; ENR2 (aripiprazole): 22.8; ER3
(aripiprazole):22.7; ENR3 (aripiprazole): 22.9.
JOURNAL OF THE
AMERICAN
ACADEMY OF
CHILD &
ADOLESCENT
PSYCHIATRY
VOLUME 52 NUMBER 7 JULY 2013 www.jaacap.org 698.e1
EARLY RESPONSE TO ARIPIPRAZOLE IN ADOLESCENTS
http://www.jaacap.org/http://www.jaacap.org/
-
7/27/2019 Early Antipsychotic Response to Aripiprazole in
Adolescents With Schizophrenia
12/13
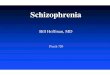
FIGURE S2 Percentage of receiver operating characteristic curve
results for early response (ER) to aripiprazole atweeks 2 and 3
predicting decreases of at least 20%, 30%, and/or 40% Positive and
Negative Syndrome Scale (PANSS)total score at endpoint (week 6).
Note: The distance between the red points and the perfect predictor
points (0% on x axisand 100% on y axis) are very short, indicating
that a decrease of at least 20% in PANSS total score carries
goodpredictive capability for ultimate response similar to the
exact optimal point.
JOURNAL OF THE
AMERICAN
ACADEMY OF
CHILD &
ADOLESCENT
PSYCHIATRY
698.e2 www.jaacap.org VOLUME 52 NUMBER 7 JULY 2013
CORRELL et al.
http://www.jaacap.org/http://www.jaacap.org/
-
7/27/2019 Early Antipsychotic Response to Aripiprazole in
Adolescents With Schizophrenia
13/13
TABLE S1 Safety and Tolerability by Week for Subjects Achieving
an Early Response Versus Early Nonresponse at Week2 or an Early
Response Versus Early Nonresponse at Week 3
Week 2, n (%) Week 3, n (%)
ENR2 ER2 ENR3 ER3
(n
132) (n
64) (n
100) (n
96)Akathisia 13 (10) 4 (6) 10 (10) 7 (7)Restlessness 14 (11) 4
(6) 11 (11) 7 (7)Insomnia 17 (13) 6 (9) 13 (13) 10 (10)Nausea,
vomiting 19 (14) 5 (8) 12 (12) 12 (13)Parkinsonian eventa 28 (21)
19 (30) 18 (18) 29 (30)Somnolence, sedation 22 (17) 12 (19) 16 (16)
18 (19)Weight gain !7% 6 (5) 3 (5) 5 (5) 4 (4)Weight change (kg)
0.2 0.0 0.3 0.1Mean change from baselineb
SAS 0.3 0.2 0.2 0.3BARS 0.1 0.0 0.1 0.0AIMS 0.2 0.2 0.1 0.2
Note: AIMS
Abnormal Involuntary Movement Scale; BARS
Barnes Akathisia Rating Scale; ER2
early response at week 2; ER3
early response atweek 3; ENR2 early nonresponse at week 2; ENR3
early nonresponse at week 3; SAS Simpson-Angus Scale.aParkinsonism
event includes extrapyramidal disorder and tremor.bLast observation
carried forward results.
OURNAL OF THE
AMERICAN
ACADEMY OF HILD &
ADOLESCENT SYCHIATRY
EARLY RESPONSE TO ARIPIPRAZOLE IN ADOLESCENTS