Embed Size (px)
Citation preview
Earlier detection of amblyopia and strabismus by ophthalmologic screening card attached to the vaccination card
Tatjana Filipovic,*t MD, PhD; Renata Grzetic,* MD; Daniela Sviderek-Stalekar, * MD
ABSTRACT • RESUME
Background: In 1983, in Rijeka, Croatia, an ophthalmologic screening card was introduced for the detection and prevention of ophthalmologic diseases, including amblyopia and strabismus, in children. The card was attached to the vaccination card. The main goal of this study was to investigate whether this model of screening decreased the age at which children were first admitted to our Department of Strabismus and Pediatric Ophthalmology.
Methods: We randomly selected I00 of the 225 children who underwent examination for the first time in the Department of Pediatric Ophthalmology and Strabismus of a clinical hospital centre in Rijeka in 1980, and I 00 of the 412 examined for the first time in 1990. Only children aged 5 years or less who were born in the maternity hospital in Rijeka were included in the study. We reviewed the records for these groups, noting the sex, age, diagnosis, refraction and visual acuity.
Results: The average age of the children examined in 1980 was 4.4 (standard deviation 1.4) years, compared with 2.5 (standard deviation 1.2) years in 1990, a statistically significant difference (p < 0.0 I, Student's t-test). In 1980, 17% of the children were under 3 years, compared with 80% in 1990 (p << 0.0 I).
Interpretation: The ophthalmologic screening card contributed to reducing the age at which strabismus and amblyopia are detected. This method of detection has been applied to the entire child population, and detection is performed continuously.
Contexte : En 1983, on introduisait a Rijeka, en Croatie, une carte de selection ophtalmologique pour favoriser le depistage et la prevention des maladies oculaires, y compris l'amblyopie et le strabisme, chez les enfants. La carte est jointe au certificat de vaccination. La presente etude avait pour objet principal d'etablir si ce modele de depistage permettait d'abaisser l'age des enfants admis pour la premiere fois a notre departement de strabisme et d'ophtalmologie pediatrique.
Methodes : Nous avons choisi au hasard I00 enfants parmi les 225 qui s'etaient presentes en 1980 pour un premier examen clinique au departement d'ophtalmologie pediatrique et de strabisme d'un hopital de Rijeka et I00 autres parmi les
From *the Clinic of Ophthalmology, Clinical Hospital Centre, and tthe Reprint requests to: Dr. Tatjana Filipoviec, Mate Balote 59, 51000 Faculty of Medicine, University of Rijeka, Rijeka, Croatia Rijeka, Croatia; fax +385-51-621 425; [email protected]
This article has been peer-reviewed. Originally received Sept. 18, 2002 Accepted for publication Aug. 4, 2003 Can JOphthalmol 2003;38:587-92
Ophthalmologic screening card-Filipovic et al 587
Ophthalmologic screening card-Filipovic et al
412 qui y avaient subi un premier examen en 1990. Seuls les enfants de 5 ans ou mains qui etaient nes a la maternite de Rijeka ont ete retenus pour l'etude. Nous avons examine les dossiers des deux groupes, relevant le sexe, l'age, le diagnostic, la refraction et l'acuite visuelle.
Resultats : L'age moyen des enfants examines etait de 4,4 ans (ecart type 1,4) en 1980, comparativement a2,5 ans (ecart type 1,2) en 1990, ce qui marquait une difference statistiquement significative (p < 0,0 I, test t de Student). En 1980, 17 % des enfants avaient mains de 3 ans, comparativement a80 % en 1990 (p << 0,0 I).
Interpretation : La carte de selection ophtalmologique a aide a reduire l'age ou le strabisme et l'amblyopie sont depistes. Cette methode de depistage a ete appliquee a toute la population enfantine et le depistage se poursuit regulierement.
Early treatment of amblyopia and strabismus is crucial. Thirty-percent of all cases of strabismus
appear during the first year of life, and 35% appear before age 2. Treatment of amblyopia produces the best results before the child's second birthday, with a success rate of 95%. 1 Factors that seem most closely related to successful treatment of amblyopia are the child's age, the type of amblyopia (strabismic, anisometropic or visual-deprivation) and depth of amblyopia.2 The impulse for the development of binocular sight is strongest before the age of 3 years. 3
Amblyogenic factors, such as visual deprivation (due to conditions such as congenital cataract or corneal degeneration), strabismus, ametropia, anisometropia and nystagmus, are already present at birth or appear during the first year of life.4
Experiments with young animals show that artificial strabismus, unilateral closure of the eye and artificially induced bilateral symmetric deprivation of form perception result in the reduction of cortical binocular neurons, necessary for stereopsis.5- 9 Stereopsis disorders may appear not only in strabismic children while the visual system is immature but also in children without strabismus. However, hypermetropia exceeding 4.00 dioptres should be corrected before the age of 4 years as it may result in deprivation of form perception.10
The detection and prevention of strabismus, amblyopia and other eye diseases in children is organized in different countries according to their respective
15policies and resources. 11 - Two approaches are available: traditional vision screening and photorefractive screening. In 1983, in Rijeka, Croatia, an ophthalmologic screening card that was attached to the vaccination card was introduced for the detection and prevention of ophthalmologic diseases in children. The main goal of this study was to investi
gate whether this model of screening decreased the age at which children were first admitted to our Department of Strabismus and Pediatric Ophthalmology.
METHODS
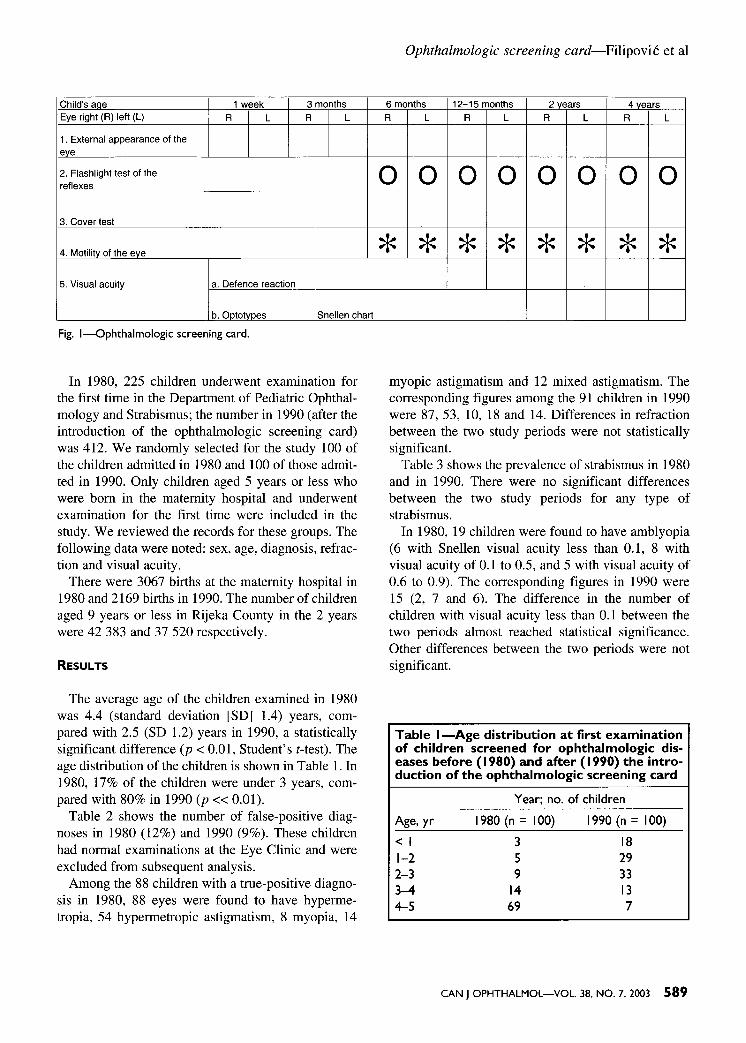
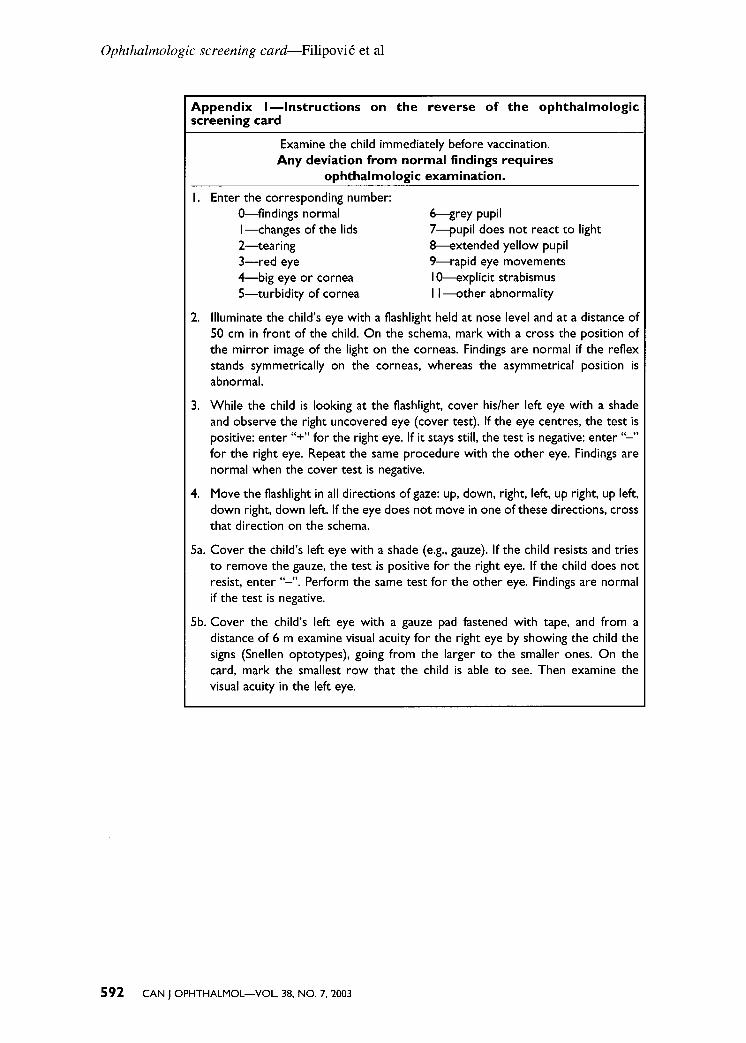
As of 1983, each child born in the maternity hospital in Rijeka was assigned an ophthalmologic screening card (Fig. 1), which was attached to his or her vaccination card (vaccination is compulsory in Croatia). The children were examined in accordance with the instructions printed on the back of the ophthalmologic screening card (Appendix 1), and the test results were recorded on the front of the card. Eye disease screening was included as part of screening and vaccination for other diseases and regular checkups. The eye examination either immediately preceded vaccination or was part of the general checkup. Eye examination was first performed by neonatologists in the maternity hospital and later by pediatricians or trained nurses under the supervision of a pediatrician. The entire child population was examined, in accordance with one of the first postulates of preventive medicine. Since vaccination and checkups of children take place several times during the preschool period (at the age of 1 week, 3 months, 12 to 15 months, 2 years and 4 years), detection is performed continuously.
Before the ophthalmologic screening card was introduced, several lectures were held for pediatricians on amblyopia and strabismus and their detection with the use of the screening card. In addition, nurses from pediatric ambulances come to the Department of Pediatric Ophthalmology and Strabismus of the Clinical Hospital Centre, Rijeka, for training on the testing procedure.
588 CAN JOPHTHALMOL-VOL. 38, NO. 7, 2003
Ophthalmologic screening card-Filipovic et al
Child's acie Eye right (R) left (L)
1 week R L
3 months R L
1. External appearance of the eve
2. Flashlight test of the reflexes
3. Cover test
4. Motilitv of the eve
5. Visual acuity a. Defence reaction
b. Oototvoes Snellen chart
Fig. I-Ophthalmologic screening card.
In 1980, 225 children underwent examination for the first time in the Department of Pediatric Ophthalmology and Strabismus; the number in 1990 (after the introduction of the ophthalmologic screening card) was 412. We randomly selected for the study 100 of the children admitted in 1980 and 100 of those admitted in 1990. Only children aged 5 years or less who were born in the maternity hospital and underwent examination for the first time were included in the study. We reviewed the records for these groups. The following data were noted: sex, age, diagnosis, refraction and visual acuity.
There were 3067 births at the maternity hospital in 1980 and 2169 births in 1990. The number of children aged 9 years or less in Rijeka County in the 2 years were 42 383 and 37 520 respectively.
RESULTS
The average age of the children examined in 1980 was 4.4 (standard deviation [SD] 1.4) years, compared with 2.5 (SD 1.2) years in 1990, a statistically significant difference (p < 0.01, Student's t-test). The age distribution of the children is shown in Table 1. In 1980, 17% of the children were under 3 years, compared with 80% in 1990 (p << 0.01).
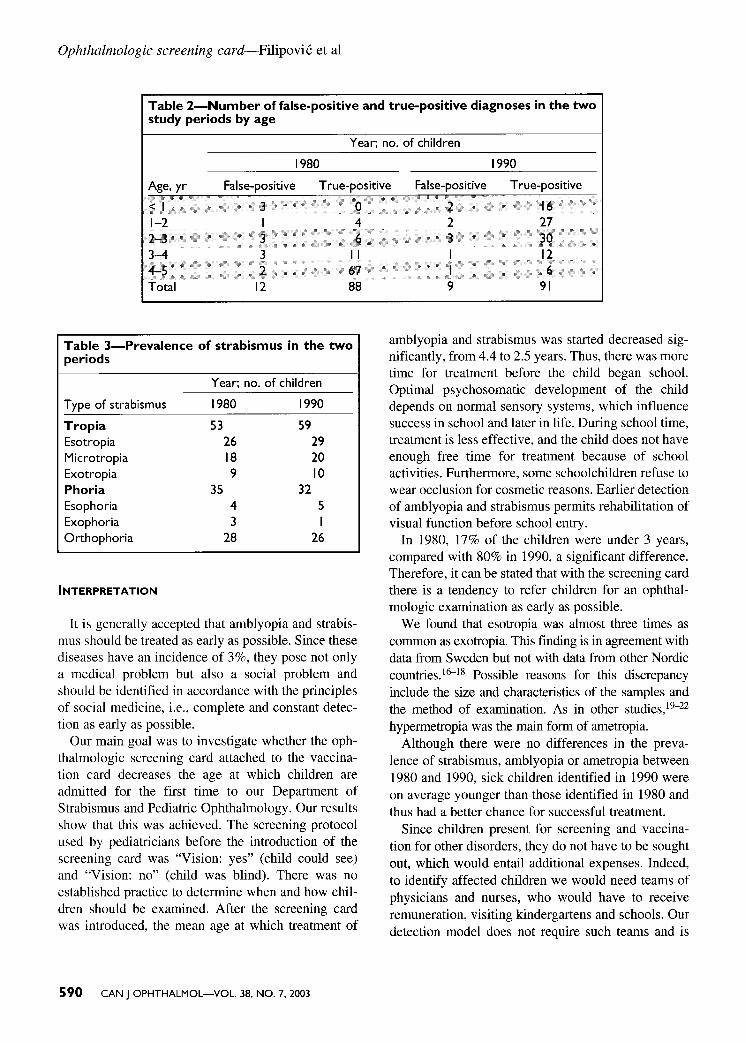
Table 2 shows the number of false-positive diagnoses in 1980 (12%) and 1990 (9%). These children had normal examinations at the Eye Clinic and were excluded from subsequent analysis.
Among the 88 children with a true-positive diagnosis in 1980, 88 eyes were found to have hypermetropia, 54 hypermetropic astigmatism, 8 myopia, 14
6 months 12-15 months 2 vears 4 vears R L R L R L R L
0 0 0 0 0 0 0 0
* * * * * * * *
myopic astigmatism and 12 mixed astigmatism. The corresponding figures among the 91 children in 1990 were 87, 53, 10, 18 and 14. Differences in refraction between the two study periods were not statistically significant.
Table 3 shows the prevalence of strabismus in 1980 and in 1990. There were no significant differences between the two study periods for any type of strabismus.
In 1980, 19 children were found to have amblyopia (6 with Snellen visual acuity less than 0.1, 8 with visual acuity of 0.1 to 0.5, and 5 with visual acuity of 0.6 to 0.9). The corresponding figures in 1990 were 15 (2, 7 and 6). The difference in the number of children with visual acuity less than 0.1 between the two periods almost reached statistical significance. Other differences between the two periods were not significant.
Table I-Age distribution at first examination of children screened for ophthalmologic diseases before ( 1980) and after ( 1990) the introduction of the ophthalmologic screening card
Year; no. of children
Age, yr 1980 (n = 100) 1990 (n =100) <I 3 18 1-2 5 29 2-3 9 33 3-4 14 13 4-5 69 7
CAN JOPHTHALMOL-VOL. 38, NO. 7, 2003 589
Ophthalmologic screening card-Filipovic et al
Table 2-Number of false-positive and true-positive diagnoses in the two study periods by age
Year; no. of children
1980 1990 Age, yr False-positive True-positive False-positive True-positive
<I 3 0 1-2 I 4 2-3 3 6 3-4 3 11 4-5 2 67 Total 12 88
Table 3-Prevalence of strabismus in the two periods
Year; no. of children
Type of strabismus 1980 1990 Tropia 53 59 Esotropia 26 29 Microtropia 18 20 Exotropia 9 10 Phoria 35 32 Esophoria 4 5 Exophoria 3 Orthophoria 28 26
INTERPRETATION
It is generally accepted that amblyopia and strabismus should be treated as early as possible. Since these diseases have an incidence of 3%, they pose not only a medical problem but also a social problem and should be identified in accordance with the principles of social medicine, i.e., complete and constant detection as early as possible.
Our main goal was to investigate whether the ophthalmologic screening card attached to the vaccination card decreases the age at which children are admitted for the first time to our Department of Strabismus and Pediatric Ophthalmology. Our results show that this was achieved. The screening protocol used by pediatricians before the introduction of the screening card was "Vision: yes" (child could see) and "Vision: no" (child was blind). There was no established practice to determine when and how children should be examined. After the screening card was introduced, the mean age at which treatment of
590 CAN JOPHTHALMOL-VOL. 38, NO. 7, 2003
2 16 2 27 3 30
12 6
9 91
amblyopia and strabismus was started decreased significantly, from 4.4 to 2.5 years. Thus, there was more time for treatment before the child began school. Optimal psychosomatic development of the child depends on normal sensory systems, which influence success in school and later in life. During school time, treatment is less effective, and the child does not have enough free time for treatment because of school activities. Furthermore, some schoolchildren refuse to wear occlusion for cosmetic reasons. Earlier detection of amblyopia and strabismus permits rehabilitation of visual function before school entry.
In 1980, 17% of the children were under 3 years, compared with 80% in 1990, a significant difference. Therefore, it can be stated that with the screening card there is a tendency to refer children for an ophthalmologic examination as early as possible.
We found that esotropia was almost three times as common as exotropia. This finding is in agreement with data from Sweden but not with data from other Nordic countries.16--18 Possible reasons for this discrepancy include the size and characteristics of the samples and
22the method of examination. As in other studies, 19
hypermetropia was the main form of ametropia. Although there were no differences in the preva
lence of strabismus, amblyopia or ametropia between 1980 and 1990, sick children identified in 1990 were on average younger than those identified in 1980 and thus had a better chance for successful treatment.
Since children present for screening and vaccination for other disorders, they do not have to be sought out, which would entail additional expenses. Indeed, to identify affected children we would need teams of physicians and nurses, who would have to receive remuneration, visiting kindergartens and schools. Our detection model does not require such teams and is

therefore more economical, which is an important consideration.2
Only children who were born in Rijeka were included in our study. Since the rural population was not included, the sample is not considered representative of the Croatian child population. The Croatian population is mainly rural, and health care is not available to the rural population to the same extent as to the urban population.
It is evident that our screening model as well as all other screening models involve a degree of inaccuracy. Investigation is needed to determine whether this can be avoided or whether it must be accepted as inevitable. The fundamental question, however, is not whether to accept screening but, rather, the best way of doing it.
REFERENCES
1. Pincon F, Badoche J. Early treatment of strabismus between the age of 4 months and 4 years. In: Mein J, Moore S, editors. Transactions of the Fourth International Orthoptic Congress, Berne, Switzerland, 1979. London: H. Kimpton; 1979. p. 228-30.
2. Flynn JT, Schiffman J, Feuer W, Corona A. The therapy of amblyopia: an analysis of the results of amblyopia therapy utilizing the pooled data of published studies. Trans Am Ophthalmol Soc 1998;96:431-50; discussion 450-3.
3. MacLellan AV, Wortham C, Janee C. The critical age? In: Mein J, Moore S, editors. Transactions of the Fourth International Orthoptic Congress, Berne, Switzerland, 1979. London: H. Kimpton; 1979. p. 225-8.
4. von Noorden GK, Dowling JE. Experimental amblyopia in monkeys. Behavioral studies in strabismic amblyopia. Arch Ophthalmol 1970;84:215-8.
5. Crawford MLJ, Smith EL 3rd, Harwerth RS, von Noorden GK. Stereoblind monkeys have few binocular neurons. Invest Ophthalmol Vis Sci 1984;25 :779-811.
6. Barker FH, Grigg P, von Noorden GK. Effect of visual deprivation and strabismus on the response of neurons in the visual cortex of monkey, including studies on the striate and prestriate cortex in the normal animal. Brain Res 1974;66: 185-8.
7. von Noorden GK, Crawford MLJ. Form deprivation without light deprivation produces the visual deprivation syndrome in Macaca mulatta. Brain Res 1977;129:37-44.
Ophthalmologic screening card-Filipovic et al
8. Crawford MLJ, von Noorden GK. Optically induced comitant strabismus in monkeys. invest Ophthalmol Vis Sci 1980;19:1105-8.
9. Crawford MLJ, de Faber JT, Harwerth RS, Smith EL 3rd, von Noorden GK. The effect of reverse monocular deprivation in monkeys. II. Electrophysiological and anatomical studies. Exp Brain Res 1989;74(2):338-47.
10. von Noorden GK, Avilla CW. Accommodative convergence in hypermetropia. Am J Ophthalmol 1990;110: 287-92.
11. Weinstock VM, Weinstock DJ, Kraft SP. Screening for childhood strabismus by primary care physicians. Can Fam Physician 1998;44:337-43.
12. Hodi S. Screening of infants for significant refractive error using videorefraction. Ophthalmic Physiol Opt 1994; 14(3):310-3.
13. Barry JC, Hartmann A, Pongs UM, Jackel M. [Model for cost-benefit relations of amblyopia screening.] Ophthalmologe 1998;95(1):19-27.
14. Simons K. Preschool vision screening: rationale, methodology and outcome. Surv Ophthalmol 1996;41(1):3-30.
15. Moore B, Lyons SA, Walline J. A clinical review of hyperopia in young children. The Hyperopic Infants' Study Group. J Am Optom Assoc 1999;70(4):215-24.
16. Kvarnstrom G, Jakobsson P, Lennerstrand G. Visual screening of Swedish children: an ophthalmological evaluation. Acta Ophthalmol Scand 2001 ;79(3):240-4.
17. Laatikainen L, Erkkila H. Refractive errors and other ocular findings in school children. Acta Ophthalmol (Copenh) 1980;58: 129-36.
18. Rantanen A, Tommila V. Prevalence of strabismus in Finland. Transactions of the Danish Ophthalmological Society. Acta Ophthalmol (Copenh) 1971;49:506-7.
19. Frandsen AD. Occurrence of squint. Acta Ophthalmol Suppl (Copenh) 1960;62:52-69.
20. Preslan MW, Novak A. Baltimore Vision Screening Project. Ophthalmology 1996; 103: 105-9.
21. Attebo K, Mitchell P, Cumming R, Smith W, Jolly N, Sparkes R. Prevalence and causes of amblyopia in an adult population. Ophthalmology 1998;105:154-9.
22. Vinding T, Gregersen E, Jensen A, Rindziunski E. Prevalence of amblyopia in old people without previous screening and treatment. An evaluation of the present prophylactic procedures among children in Denmark. Acta Ophthalmol (Copenh) 1991;69:796-8.
Key words: amblyopia, strabismus, detection, prevention
Continued on p. 592
CAN JOPHTHALMOL-VOL. 38, NO. 7, 2003 591
Ophthalmologic screening card-Filipovic et al
Appendix I-Instructions on the reverse of the ophthalmologic screening card
Examine the child immediately before vaccination. Any deviation from normal findings requires
ophthalmologic examination. I. Enter the corresponding number:
0-findings normal 6-grey pupil I-changes of the lids 7-pupil does not react to light 2-tearing 8-extended yellow pupil 3-red eye 9-rapid eye movements 4-big eye or cornea I0-explicit strabismus S-turbidity of cornea I I-other abnormality
2. Illuminate the child's eye with a flashlight held at nose level and at a distance of SO cm in front of the child. On the schema, mark with a cross the position of the mirror image of the light on the corneas. Findings are normal if the reflex stands symmetrically on the corneas, whereas the asymmetrical position is abnormal.
3. While the child is looking at the flashlight, cover his/her left eye with a shade and observe the right uncovered eye (cover test). If the eye centres, the test is positive: enter "+" for the right eye. If it stays still, the test is negative: enter "-" for the right eye. Repeat the same procedure with the other eye. Findings are normal when the cover test is negative.
4. Move the flashlight in all directions of gaze: up, down, right, left, up right, up left, down right, down left. If the eye does not move in one of these directions, cross that direction on the schema.
Sa. Cover the child's left eye with a shade (e.g., gauze). If the child resists and tries to remove the gauze, the test is positive for the right eye. If the child does not resist, enter"-". Perform the same test for the other eye. Findings are normal if the test is negative.
Sb. Cover the child's left eye with a gauze pad fastened with tape, and from a distance of 6 m examine visual acuity for the right eye by showing the child the signs (Snellen optotypes), going from the larger to the smaller ones. On the card, mark the smallest row that the child is able to see. Then examine the visual acuity in the left eye.
592 CAN JOPHTHALMOL-VOL. 38, NO. 7, 2003