Embed Size (px)
Citation preview
1 Ear Care Guidelines Version 1 June 2016
SH CP 196
Ear Care Guidelines
Version: 1
Summary: These guidelines are to ensure the provision of evidence based practice, which
will ensure that all patients who are require ear care receive the best quality of evidence based care, minimising risk and potential adverse effects and maximising quality of life.
Keywords: Aural toilet, cerumen, ear care, ear examination, ear syringing, ear irrigation,
ear wax, wax softening, wax removal,
Target Audience: This guideline extends to cover those people who are registered with General Practitioners within the geographical Boundaries of Southern Health Foundation Trust (SHFT) and the responsibilities of those staff providing such service.
Next Review Date: October 2018
Approved &
Ratified by:
Quality Improvement and Development
Virtual Policy Group
Date of meeting: April 2016
Date issued: June 2016
Author: Mandy Lyons, Clinical Trainer
Director: Lesley Stevens, Medical Director
2 Ear Care Guidelines Version 1 June 2016
Version Control
Change Record
Date Author Version Page Reason for Change
10/5/18 Review date extended from June 2018 to October 2018
Reviewers/contributors
Name Position Version Reviewed & Date
Steve Coopey Head of Clinical Development Bands 5 and Above V1 - 2016
Sharon Guy Lead Clinical Trainer
V1 - 2016
Wendy Eastman GP Development lead
V1 - 2016
Theresa Lewis
Lead Nurse Infection Prevention & Control V1 - 2016
Marie Corner Medical Device Lead
V1 - 2016
3 Ear Care Guidelines Version 1 June 2016
Contents
Section Title Page
1. Introduction
4
2. Who does this policy apply to?
4
3. Definitions
4
4. Duties and responsibilities
6
5. Main policy content
6
6. Training requirements
10
7. Monitoring compliance
10
8.
Policy review 11
9.
Associated trust documents 11
10.
Supporting references 11
APPENDICES
A1
Training needs analysis 12
A2 Ear care nursing record
13
A3 Procedure for Ear Examination (Otoscopy)
16
A4 Guidance for wax softening
18
A5 Procedure for Aural Toilet
19
A6 Procedure for Ear Irrigation
21
A7 Cleaning guidelines for an Electronic Irrigator
24
A8 Referral guidelines
28
A9 Ear Care Patient Information Leaflet
32
4 Ear Care Guidelines Version 1 June 2016
Ear Care Guidelines 1. Introduction
1.1 The purpose of this guideline is to support staff to provide safe, effective ear care to adults, either
in a clinic or domiciliary setting, in line with best current evidence base. It aims to reduce litigation risk in ear irrigation and to provide the patient with a positive experience of ear care.
1.2 This document provides guidance on the following subjects
Cerumen management
History taking and assessment
Ear examination
Softening agents
Aural toilet/ removal by instrumentation
Ear irrigation
Patient referral and advice
Documentation
1.3 The ‘Ear Care Guidance Document’ (revised in 2014) by The Rotherham Primary Ear Care Centre’ is the nationally recognised protocol for ear care. It is endorsed by The Royal College of General Practitioners, The Royal College of Nursing, and the Medical Devices Agency, and has been recognised as the key evidence base for this guideline.
1.4 Every year in the UK, over two million people have problems with earwax and need it removed.
Complications of syringing are a common cause of complaints and litigation in primary care. A study examining ear syringing in UK general practice estimated that the rate of complications requiring specialist referral was about in 1/1000 ears syringed. These complications included perforation, canal lacerations, and failure of wax removal. Otitis externa may also complicate ear syringing.
2. Who does this policy apply to?
This guideline is intended for all members of staff employed by Southern Health NHS Foundation Trust who are required to undertake ear care. This includes registered nurses in all aspects of ear care, and any Bands 3 and 4 who have undergone specific training and been assessed as competent to undertake ear assessment and examination and give advice regarding management options and the administration of ear drops as appropriate.
3. Definitions and abbreviations
3.1 Areas of tympanic membrane - Pars flaccida, Pars tensa, Anterior recess, Light reflex Handle of malleus 3.2 Audiology - field of health care that deals with hearing and balance disorders 3.3 Aural Toilet (also known as Dry mopping) - a procedure used to clear the External auditory
meatus of debris, discharge, soft wax or excess fluid following irrigation, using cotton wool.
3.4 Aural speculum - A funnel shaped piece of plastic on a light source (otoscope) that is inserted into the auditory canal of the ear, allowing the examiner to look at the ear canal and ear drum.
3.5 Cerumen (Ear wax) - a normal wax-like substance that protects the ear canal
5 Ear Care Guidelines Version 1 June 2016
3.6 Cerumenolytics - agents that soften hardened cerumen (earwax) and make it easier for it to be removed from the ear.
3.7 Crocodile forceps- instrument used in ear care
3.8 Ear Nose and Throat (ENT) - the area of medicine that deals with disorders and conditions of the ear, nose, and throat
3.9 Ear irrigation ( formerly known as ear syringing) - a routine procedure used to remove excess
earwax, or foreign materials from the ear
3.10 External auditory meatus- (EAM) also known as the ear canal- a tunnel running from the outer ear to the middle ear
3.11 Grommets - a tube surgically implanted in the eardrum to drain fluid from the middle ear.
3.12 Hygroscopic foreign bodies - (eg: peas and lentils) will absorb water and expand making removal difficult.
3.13 Jobson Horne- a probe with a serrated end used in ear care
3.14 Mastoid process - a large, bony prominence on the base of the skull behind the ear, containing air spaces that connect with the middle ear cavity
3.15 Microsuction - a wax-removal technique using a binocular operating microscope (which allows depth-perception and magnification) to look straight into the ear canal and a very fine sterile suction device at low pressure to remove the wax.
3.16 Noots tank- a receiver used to collect water during ear irrigation.
3.17 Otitis Externa - inflammation of the external auditory meatus
3.18 Otoscopy - an examination that involves looking into the ear with an instrument called an otoscope (or auriscope). This is performed in order to examine the ear canal– the tunnel that leads from the outer ear (pinna) to the eardrum.
3.19 Pinna - the projecting part of the external ear
3.20 Tinnitus - the word 'tinnitus' comes from the Latin word for 'ringing' and is the perception of hearing sound in the absence of any corresponding external sound.
3.21 Tragus - a cartilaginous projection anterior to the external opening of the ear.
3.22 Tympanic membrane (TM) - also known as the eardrum - a thin membrane that serves as a partition between the external ear and the middle ear, and transmits the motion of sound waves to the small of bones in the middle ear.
3.23 Vertigo - a sensation of dizziness and loss of balance, associated with disease affecting the inner ear or the vestibular nerve.
6 Ear Care Guidelines Version 1 June 2016
4. Duties and responsibilities
4.1 Key goals:
To recognise when ear wax needs to be removed
To remove earwax effectively and safely when indicated
To refer appropriately for specialist assessment and management 4.2 All registered nurses are expected to develop and maintain their competence in accordance with
the NMC Code (2015) and follow Record Keeping (2009) guidelines.
4.3 All healthcare professionals must exercise their own professional judgement when using these guidelines. However, any decision to vary from the guideline should be documented in the patient’s records to include the reason for variance and the subsequent action taken.
5. Main policy content
5.1 Cerumen Management
5.1.1 Cerumen, or wax as it is commonly known, is a normal secretion of the ceruminous glands the
external auditory meatus (EAM), which is generally thought to be protective to the ear. It is slightly acidic, giving bactericidal qualities in both its wet, sticky form (as secreted by Caucasians and African-Caribbeans) and dry, flaky form (as, for example, secreted by people from South East Asia).
5.1.2 In addition to epithelial migration, jaw movement assists the movement of wax to the entrance of
the ear canal where it emerges onto the skin. A small amount of wax is normally found in the EAM and its absence may be a sign that dry skin conditions, infection or excessive cleaning have interfered with the normal production of wax.
5.1.3 It is only when there is an accumulation of excessive wax that removal may need to be
considered.
5.1.4 A build-up of wax is more likely to occur in older adults and patients with learning difficulties (reason unknown), hearing aid users, people who insert implements into the ear or have a narrow EAM. A build-up of wax may also occur as a result of anxiety, stress and dietary or hereditary factors.
5.1.5 Excessive wax should be removed before it becomes impacted, or it can give rise to tinnitus, hearing loss, vertigo, pain and discharge.
5.1.6 If wax is removed due to the presenting complaint of hearing loss, it is important to ascertain whether good hearing is restored after treatment, or consider if the patient would benefit from a formal assessment by the ENT surgeon or Audiologist.
5.1.7 Following assessment and examination the experienced practitioner can use his or her clinical judgement on the best method for wax management and removal. Olive oil may be advised in favour of other cerumenolytics as it is the softening agent with least likelihood of causing irritation. The practitioner may decide that extended use of olive oil is preferable to wax removal procedures.
7 Ear Care Guidelines Version 1 June 2016
5.1.8 Options for removal of impacted wax include:
Use of softening agents
Aural Toilet/ removal of wax by instrumentation/ dry mopping
Ear irrigation with water using an electronic ear irrigation device
Referral to specialist; outcome may include removal of wax by micro suction 5.1.9 Patients should always receive education and advice, to help them to give informed consent for
any procedures, and written advice in the form of a patient leaflet may reduce contributory factors and therefore the need for future ear irrigation or intervention (see Appendix 9).
5.2 History taking and Assessment 5.2.1 Prior to examination of the ear it is essential to talk to the patient and / or their carer to obtain a
detailed history and provide explanation of any examination or procedures. The service user should be fully informed of possible complications of the procedure and effects of ear irrigation, to ensure that the patient understands and gives consent.
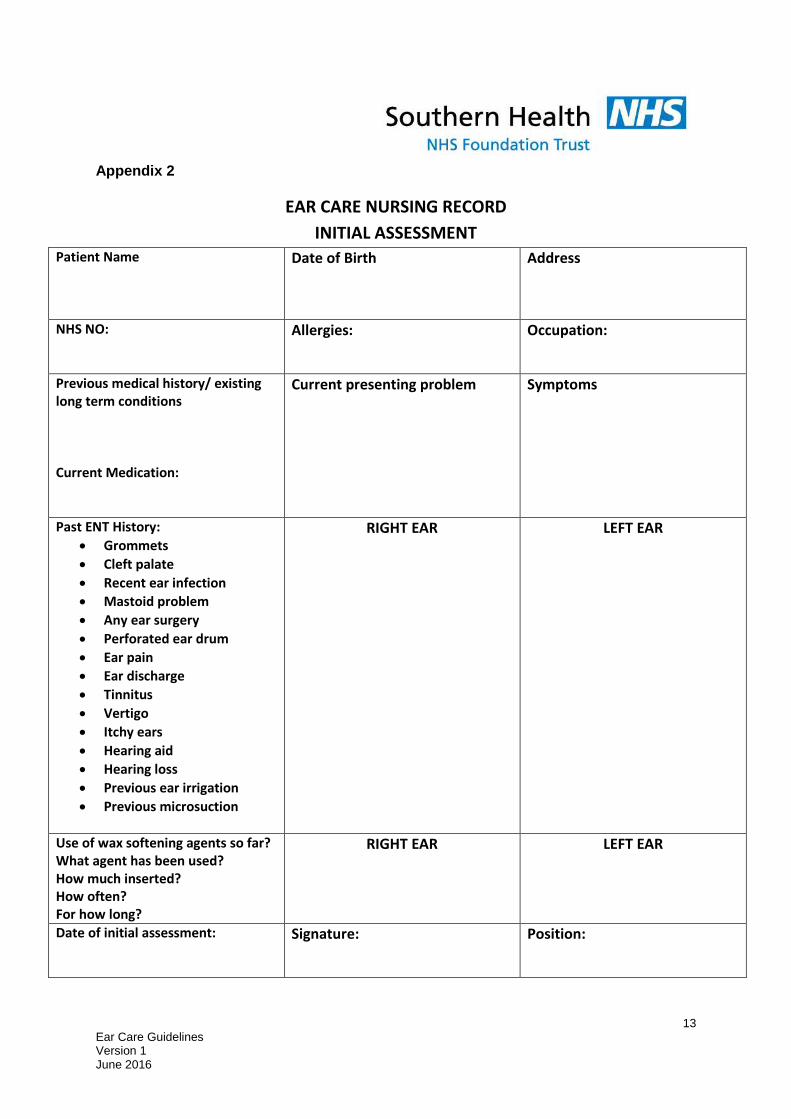
5.2.2 Document the assessment and relevant history on the Ear Care Nursing Record- Initial
Assessment Form (See Appendix 2).
5.2.3 The form should include patient’s personal identification details, including name, date of birth, address or NHS number.
5.2.4 Past medical history should be documented, including existing long term conditions, current medication, allergy status and present or previous occupation. Detailed ENT history should be taken to include the following:
Grommets
Cleft palate
Recent ear infection
Mastoid problem
Any ear surgery
Perforated ear drum
Ear pain
Ear discharge
Tinnitus
Vertigo
Itchy ears
Hearing aid
Hearing loss
Previous ear irrigation
Previous microsuction
5.2.5 Details of the current presenting problem and any symptoms being experienced by the patient should be documented.
5.3 Examination of both ears
5.3.1 The aim of the examination is to assess the amount and position of wax, and to support the
clinical decision making process regarding any procedures or interventions to be carried out.
5.3.2 Careful history taking will exclude any contra-indications to ear irrigation
8 Ear Care Guidelines Version 1 June 2016
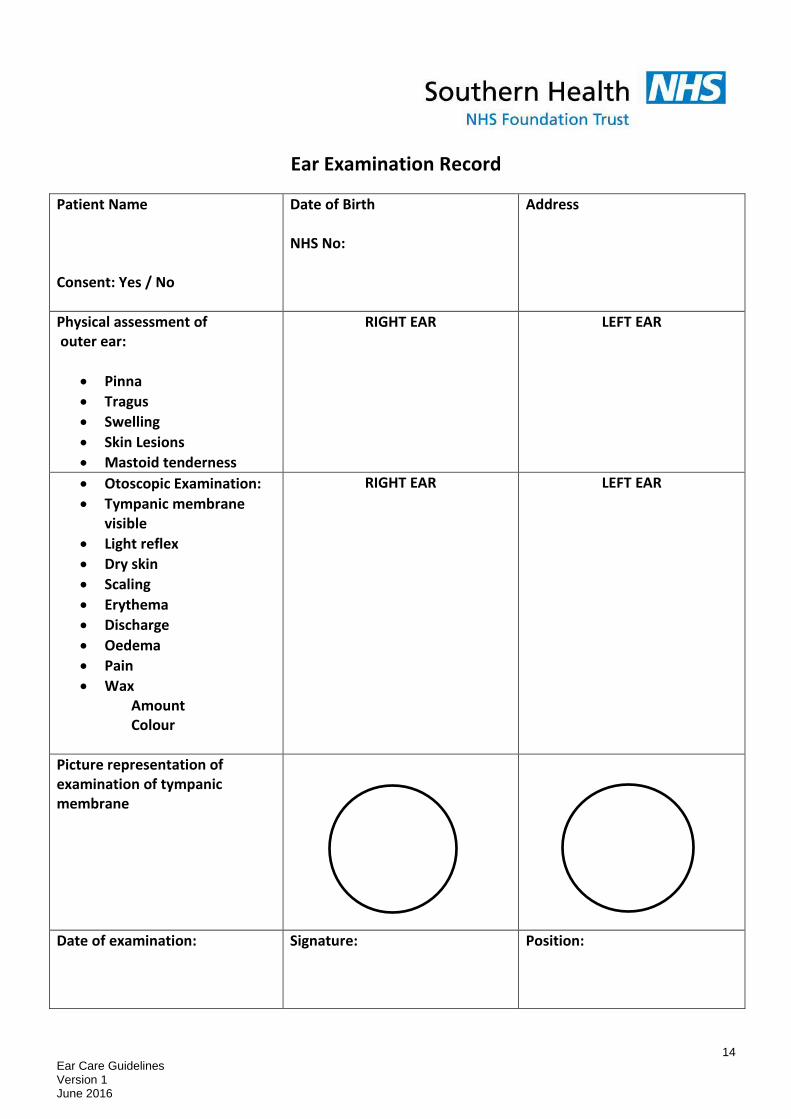
5.3.3 Physical assessment of the outer ear should describe findings relating to the pinna, the tragus any swelling, skin lesions, mastoid tenderness
5.3.4 Otoscopic examination should be carried out by healthcare professionals who have been trained and are competent in this procedure, following the SHFT Ear Examination procedure (see Appendix 3)
5.3.5 Findings from both ears should be documented using the SHFT Nursing record and should include the following: if tympanic membrane visible, light reflex, dry skin, scaling, erythema, discharge, oedema, pain, wax amount & colour.
5.3.6 Any wax softening agents inserted already by patient or carer should be documented, to include what agent has been used, how much has been inserted, how often and for how long?
5.4 Softening agents
5.4.1 Following patient assessment and examination of both ears, if impacted wax is the problem advice needs to be given to the patient/ and or carer regarding wax softening prior to any further procedures being carried out. This is to promote patient safety by reducing risk of procedures, and increasing likelihood of successful wax removal (See Appendix 4: Guidelines for wax softening).
5.4.2 There is no evidence to confirm that any one wax softening agent is superior to another. However, olive oil has been shown to be less irritant in some individuals, so is first line choice.
5.4.3 Olive oil should be at room temperature. Advise patient/ carer to insert olive oil into the affected external auditory canal: Insert 2-3 drops, 2-3 x per day, for a minimum of 5-7 days.
5.4.4 Advise patient to lie on unaffected side, if possible, while olive oil is inserted using a dropper, and to remain on side for 5 minutes afterwards.
5.4.5 Advise patient not to put cotton wool in to ear after olive oil has been inserted, as the cotton wool absorbs the oil which could lead to ineffective wax softening.
5.4.6 The patient should be re-assessed, and ears re-examined after 5-7 days, and consider if any further intervention is required, and document rationale for any procedures.
5.4.7 If further wax softening is required prior to further intervention the patient could be advised to continue with olive oil or an alternative cerumenolytic could be tried eg: Earol spray ( if patient is having problems instilling drops), sodium bicarbonate drops, Earex, or hydrogen peroxide based solutions( eg: Otex).
5.4.8 Care must be taken not to advise any products that may contain nut oils, such as almond oil, if a patient has a nut allergy, to avoid risk of anaphylactic reaction.
5.4.9 Aural Toilet (also known as dry mopping or removal of excessive wax by instrumentation)
5.4.10 This procedure should be carried out following patient assessment and examination, to support patient safety, and determine if procedure is contra indicated (See Appendix 5).
5.4.11 Aural toilet should always be carried out to clear the external auditory meatus of excess fluid following ear irrigation, to reduce risk of infection post irrigation procedure.
5.4.12 This procedure may also be considered as a treatment option to remove debris, discharge or soft wax from the ear as an alternative treatment option, if irrigation is contra indicated, or as an option which may be less traumatic and a more acceptable patient choice.
9 Ear Care Guidelines Version 1 June 2016
5.4.13 The EAM is cleaned with a gentle rotary action, and the cotton wool should be replaced directly it becomes soiled.
5.4.14 Care must be taken not to touch the tympanic membrane.
5.4.15 Intermittently re-examine the meatus, using the otoscope, during cleaning to check for any debris/discharge/crusts which remain in the meatus at awkward angles.
5.4.16 Any wax, debris, dry skin or clearly visible foreign objects not removed by dry mopping could be removed by instrumentation, for example using a wax hook, or crocodile forceps, but only if the registered nurse has considerable experience and competence in ear care.
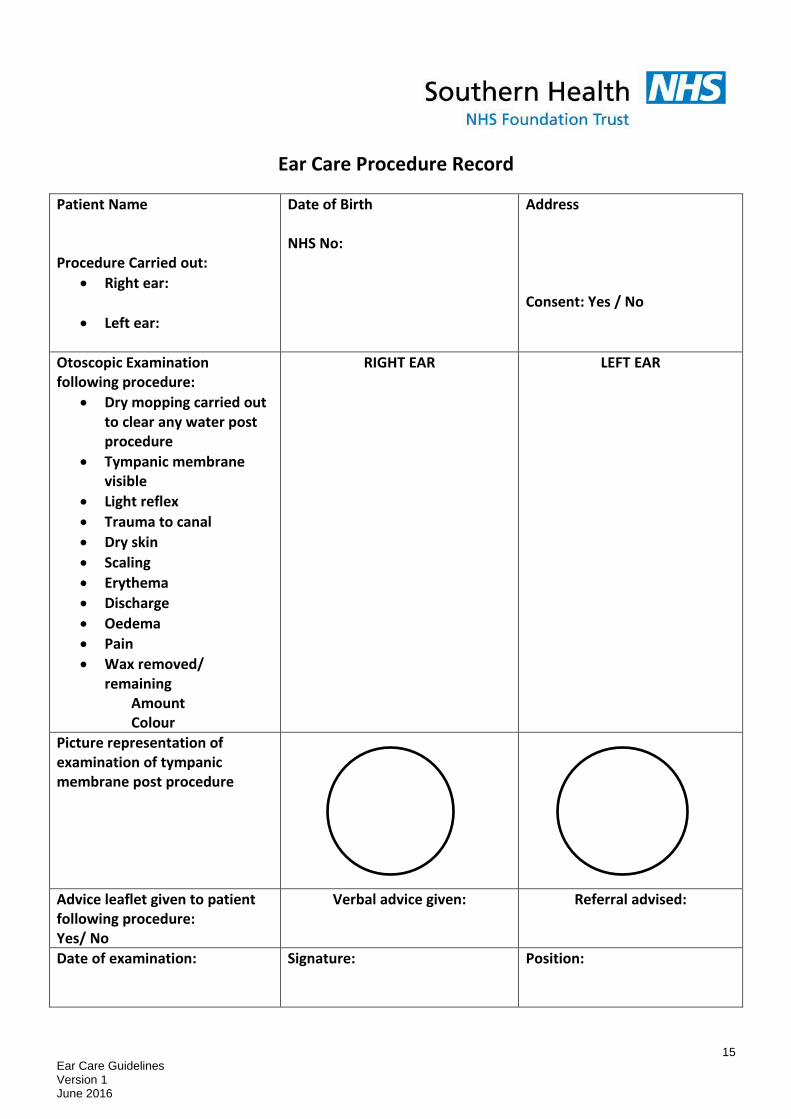
5.4.17 Document the procedure and what was observed in both ears, including the condition of the tympanic membrane and external auditory meatus using SHFT Ear Care documentation record.
5.5 Ear Irrigation
5.5.1 Ear irrigation is undertaken for the purpose of removing wax from the external auditory meatus where this is thought to be causing a hearing deficit and/or discomfort, or restricts vision of the tympanic membrane preventing examination. (See Appendix 6).
This procedure should only be carried out by a registered nurse who has undergone training and can demonstrate competency in accordance with NMC Code, to support safe clinical practice. Nurses performing the procedure should understand the normal and abnormal anatomy and physiology of the ear and be aware of the complications and contraindications of ear irrigation.
5.5.2 This procedure should only be carried out following patient assessment and examination of both ears, to ensure patient safety, and determine if the procedure is contra indicated. Consent needs to be obtained and the rationale for carrying out the procedure documented in individual care plan.
5.5.3 This procedure should not be used for the removal of hygroscopic foreign bodies such as peas and lentils, as these will absorb water and expand, making removal difficult.
5.5.4 Before commencing procedure ensure electronic irrigation machine has been maintained and cleaned in accordance with manufacturer’s instructions. (See Appendix 7: Guidelines for cleaning electronic irrigator). This is to promote patient safety and reduce risk of infection or trauma during procedure.
5.5.5 This procedure should be carried out with both participants seated and under direct vision, using a headlight or head mirror and light source, to aid visibility and support comfort and safety.
5.5.6 The tap water used for this procedure should be at body temperature to aid patient comfort and reduce risk of problems, such as dizziness or trauma.
5.5.7 The pressure on the irrigation machine should be set at minimum and, using the foot control, point the jet tip to direct a stream of water along the roof of the EAM and towards the posterior wall (direct towards the back of the patient’s head), increasing the pressure control gradually if there is difficulty removing the wax.
5.5.8 It is advisable that a maximum of one reservoir of water per ear is used in any one irrigation procedure to prevent trauma or patient discomfort.
5.5.9 Periodically inspect the EAM with the otoscope and inspect the solution running into the receiver, to monitor progress of the procedure, and minimise time and amount of water used for irrigation.
10 Ear Care Guidelines Version 1 June 2016
5.5.10 After removal of wax or debris, dry mop and remove excess water from the meatus under direct vision using the Jobson Horne probe and best quality cotton wool (See Appendix 5), as stagnation of water in the ear canal and any abrasion of skin during the procedure predispose to infection. Removing the water with the cotton wool tipped probe reduces the risk of post procedure infection.
5.5.11 Irrigation may be uncomfortable but it should NEVER CAUSE PAIN. STOP IMMEDIATELY if:
Patient complains of pain
Water comes down the nose
Patient swallows excessively
Bleeding occurs
5.5.12 Advise of possible complications following procedure, such as dizziness, infection, tinnitus, to ensure an effective outcome for the patient and support continuity of care.
5.5.13 Refer patients if necessary following local referral guidelines (see Appendix 8)
5.6 On-going patient advice
5.7.1 Give advice to patient regarding on going ear care and provide SHFT written patient information leaflet (see Appendix 9).
5.7.2 Patient should be advised that the only reason for carrying out ear irrigation is when hearing is reduced due to wax impacted on the eardrum. Regular or routine irrigation is not recommended.
5.7.3 If wax has been removed due to the presenting complaint of hearing loss, they should check whether good hearing is restored after treatment or would they benefit from a formal hearing assessment by the audiologist.
5.7.4 Advise patients that wax protects the ear and that the ear is self-cleaning and does not need poking with flannels and direct streams from the shower head or cotton buds or keys.
5.7.5 Ear candles are not a safe option of wax removal as they may result in serious injury.
5.7.6 To prevent build-up of excessive wax, if this is a recurrent problem, it may be helpful to instil olive oil in to the ear canal once or twice a week and wear ear plugs when in water.
6. Training requirements
All staff undertaking ear care should have attended SHFT Ear Care Training provided by the LEaD Clinical Training Team, or an alternative recognised ear care training course, and be able to demonstrate confidence and competence in carrying out safe and effective ear care using the Southern Health Competency Framework Tool. It is advised that any health care professional learning to carry out a new clinical skill, such as ear care, be supervised initially by a mentor in practice who is already competent in ear care.
7. Monitoring compliance
Element to be monitored
Lead Tool Frequency Reporting arrangements
Competency in Ear Care
Line manager
Competency Framework tool
Every two years
Annual appraisal
11 Ear Care Guidelines Version 1 June 2016
8. Policy review
This policy will be reviewed every three years 9. Associated trust documents Infection prevention and control policy Hand Hygiene and Aseptic and Clean Technique Procedures.
Management and Decontamination of Medical devices
10. Supporting references
Ear Care Guidance Document (revised 2014) The Rotherham NHS Foundation Trust Primary Ear Care Centre. http://earcarecentre.com.
National institute for health & excellence (NICE) Clinical knowledge summary (CKS): Earwax (2012) http://cks.nice.org.uk/earwax
http://www.tinnitus.org.uk/what-is-tinnitus REFERENCES (EAR CARE GUIDELINES)
Ear care guidelines: Worcestershire Primary Care Trust (2006)
The Royal Marsden Manual of Clinical Nursing Procedures (9th Edition) 2015, Edited by Dougherty, L & Lister, S. Wiley Blackwell, W Sussex.
Sharp JF, Wilson JA, Ross L, Barr-Hamilton RM (December 1990). "Ear wax removal: a survey of current practice". BMJ 301 (6763): 1251–3
12 Ear Care Guidelines Version 1 June 2016
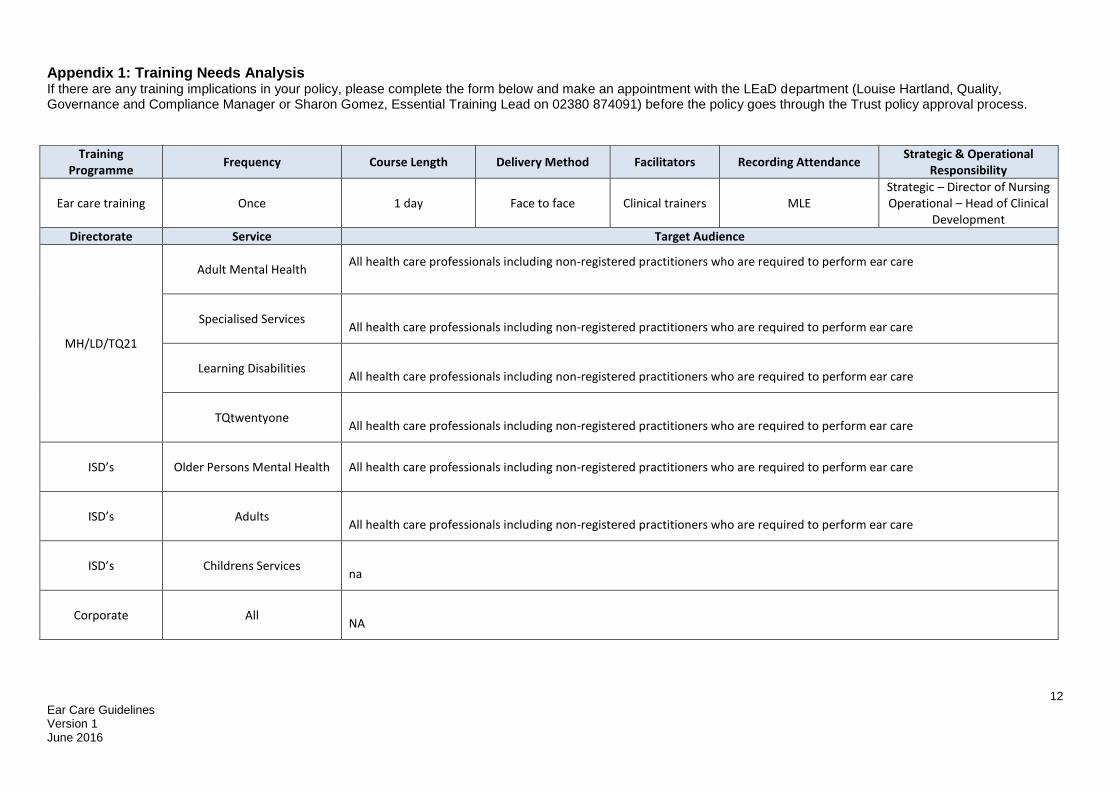
Appendix 1: Training Needs Analysis If there are any training implications in your policy, please complete the form below and make an appointment with the LEaD department (Louise Hartland, Quality, Governance and Compliance Manager or Sharon Gomez, Essential Training Lead on 02380 874091) before the policy goes through the Trust policy approval process.
Training Programme
Frequency Course Length Delivery Method Facilitators Recording Attendance Strategic & Operational
Responsibility
Ear care training Once 1 day Face to face Clinical trainers MLE Strategic – Director of Nursing Operational – Head of Clinical
Development
Directorate Service Target Audience
MH/LD/TQ21
Adult Mental Health
All health care professionals including non-registered practitioners who are required to perform ear care
Specialised Services
All health care professionals including non-registered practitioners who are required to perform ear care
Learning Disabilities
All health care professionals including non-registered practitioners who are required to perform ear care
TQtwentyone
All health care professionals including non-registered practitioners who are required to perform ear care
ISD’s
Older Persons Mental Health
All health care professionals including non-registered practitioners who are required to perform ear care
ISD’s
Adults
All health care professionals including non-registered practitioners who are required to perform ear care
ISD’s
Childrens Services
na
Corporate
All
NA
13 Ear Care Guidelines Version 1 June 2016
Appendix 2
EAR CARE NURSING RECORD
INITIAL ASSESSMENT Patient Name
Date of Birth Address
NHS NO:
Allergies: Occupation:
Previous medical history/ existing long term conditions Current Medication:
Current presenting problem
Symptoms
Past ENT History:
Grommets
Cleft palate
Recent ear infection
Mastoid problem
Any ear surgery
Perforated ear drum
Ear pain
Ear discharge
Tinnitus
Vertigo
Itchy ears
Hearing aid
Hearing loss
Previous ear irrigation
Previous microsuction
RIGHT EAR LEFT EAR
Use of wax softening agents so far? What agent has been used? How much inserted? How often? For how long?
RIGHT EAR LEFT EAR
Date of initial assessment:
Signature: Position:
14 Ear Care Guidelines Version 1 June 2016
Ear Examination Record
Patient Name Consent: Yes / No
Date of Birth NHS No:
Address
Physical assessment of outer ear:
Pinna
Tragus
Swelling
Skin Lesions
Mastoid tenderness
RIGHT EAR LEFT EAR
Otoscopic Examination:
Tympanic membrane visible
Light reflex
Dry skin
Scaling
Erythema
Discharge
Oedema
Pain
Wax Amount Colour
RIGHT EAR LEFT EAR
Picture representation of examination of tympanic membrane
Date of examination:
Signature: Position:
15 Ear Care Guidelines Version 1 June 2016
Ear Care Procedure Record
Patient Name Procedure Carried out:
Right ear:
Left ear:
Date of Birth NHS No:
Address Consent: Yes / No
Otoscopic Examination following procedure:
Dry mopping carried out to clear any water post procedure
Tympanic membrane visible
Light reflex
Trauma to canal
Dry skin
Scaling
Erythema
Discharge
Oedema
Pain
Wax removed/ remaining
Amount Colour
RIGHT EAR LEFT EAR
Picture representation of examination of tympanic membrane post procedure
Advice leaflet given to patient following procedure: Yes/ No
Verbal advice given: Referral advised:
Date of examination:
Signature: Position:
16 Ear Care Guidelines Version 1 June 2016
APPENIDX 3
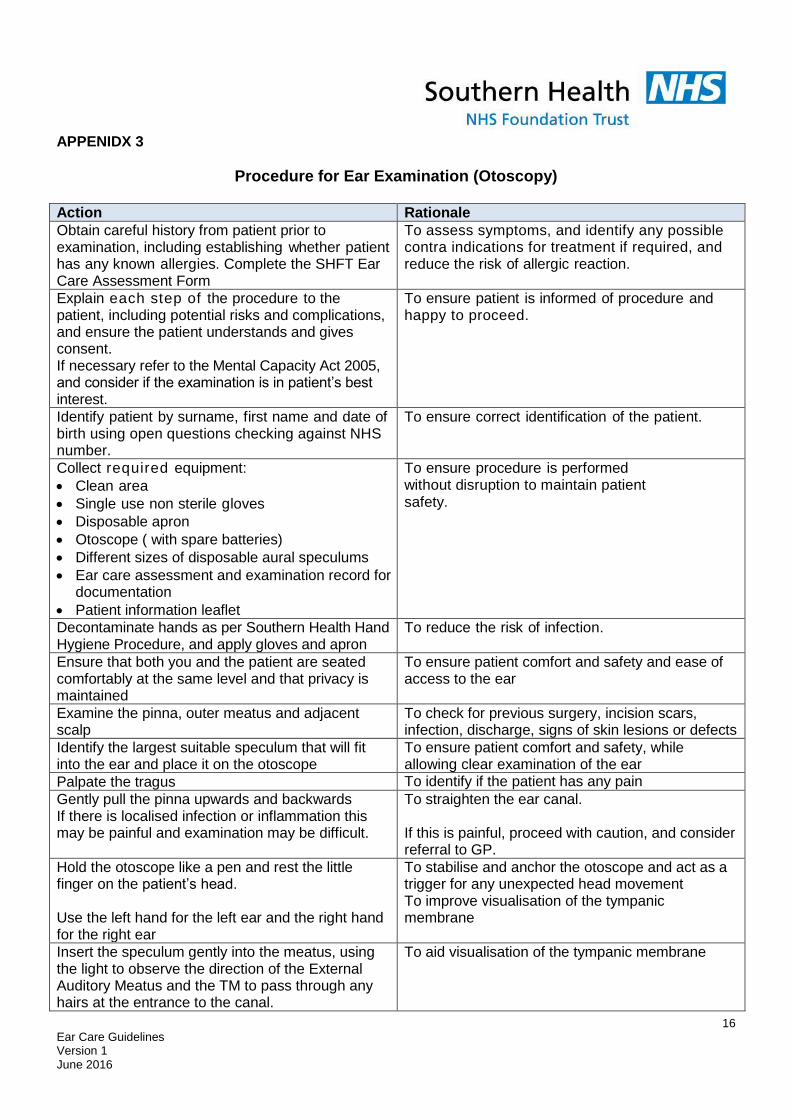
Procedure for Ear Examination (Otoscopy)
Action Rationale
Obtain careful history from patient prior to examination, including establishing whether patient has any known allergies. Complete the SHFT Ear Care Assessment Form
To assess symptoms, and identify any possible contra indications for treatment if required, and reduce the risk of allergic reaction.
Explain each step of the procedure to the patient, including potential risks and complications, and ensure the patient understands and gives consent. If necessary refer to the Mental Capacity Act 2005, and consider if the examination is in patient’s best interest.
To ensure patient is informed of procedure and happy to proceed.
Identify patient by surname, first name and date of birth using open questions checking against NHS number.
To ensure correct identification of the patient.
Collect required equipment:
Clean area
Single use non sterile gloves
Disposable apron
Otoscope ( with spare batteries)
Different sizes of disposable aural speculums
Ear care assessment and examination record for documentation
Patient information leaflet
To ensure procedure is performed without disruption to maintain patient safety.
Decontaminate hands as per Southern Health Hand Hygiene Procedure, and apply gloves and apron
To reduce the risk of infection.
Ensure that both you and the patient are seated comfortably at the same level and that privacy is maintained
To ensure patient comfort and safety and ease of access to the ear
Examine the pinna, outer meatus and adjacent scalp
To check for previous surgery, incision scars, infection, discharge, signs of skin lesions or defects
Identify the largest suitable speculum that will fit into the ear and place it on the otoscope
To ensure patient comfort and safety, while allowing clear examination of the ear
Palpate the tragus To identify if the patient has any pain
Gently pull the pinna upwards and backwards If there is localised infection or inflammation this may be painful and examination may be difficult.
To straighten the ear canal. If this is painful, proceed with caution, and consider referral to GP.
Hold the otoscope like a pen and rest the little finger on the patient’s head. Use the left hand for the left ear and the right hand for the right ear
To stabilise and anchor the otoscope and act as a trigger for any unexpected head movement To improve visualisation of the tympanic membrane
Insert the speculum gently into the meatus, using the light to observe the direction of the External Auditory Meatus and the TM to pass through any hairs at the entrance to the canal.
To aid visualisation of the tympanic membrane
17 Ear Care Guidelines Version 1 June 2016
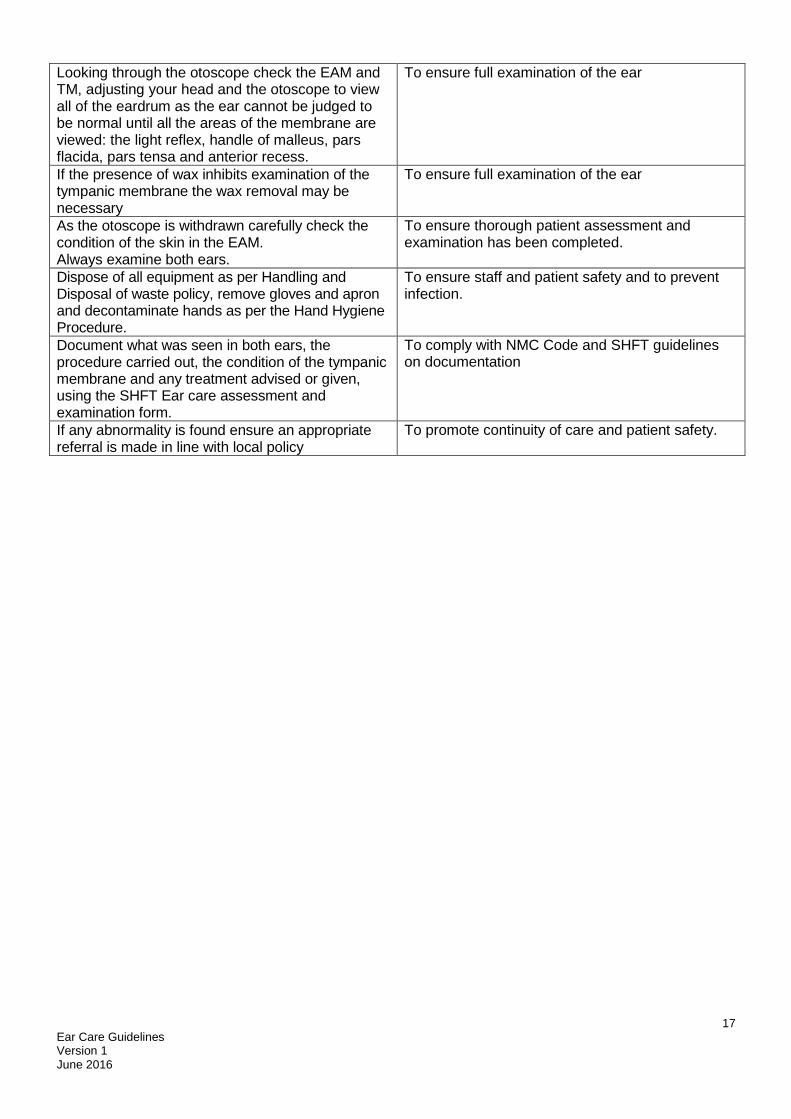
Looking through the otoscope check the EAM and TM, adjusting your head and the otoscope to view all of the eardrum as the ear cannot be judged to be normal until all the areas of the membrane are viewed: the light reflex, handle of malleus, pars flacida, pars tensa and anterior recess.
To ensure full examination of the ear
If the presence of wax inhibits examination of the tympanic membrane the wax removal may be necessary
To ensure full examination of the ear
As the otoscope is withdrawn carefully check the condition of the skin in the EAM. Always examine both ears.
To ensure thorough patient assessment and examination has been completed.
Dispose of all equipment as per Handling and Disposal of waste policy, remove gloves and apron and decontaminate hands as per the Hand Hygiene Procedure.
To ensure staff and patient safety and to prevent infection.
Document what was seen in both ears, the procedure carried out, the condition of the tympanic membrane and any treatment advised or given, using the SHFT Ear care assessment and examination form.
To comply with NMC Code and SHFT guidelines on documentation
If any abnormality is found ensure an appropriate referral is made in line with local policy
To promote continuity of care and patient safety.
18 Ear Care Guidelines Version 1 June 2016
Appendix 4
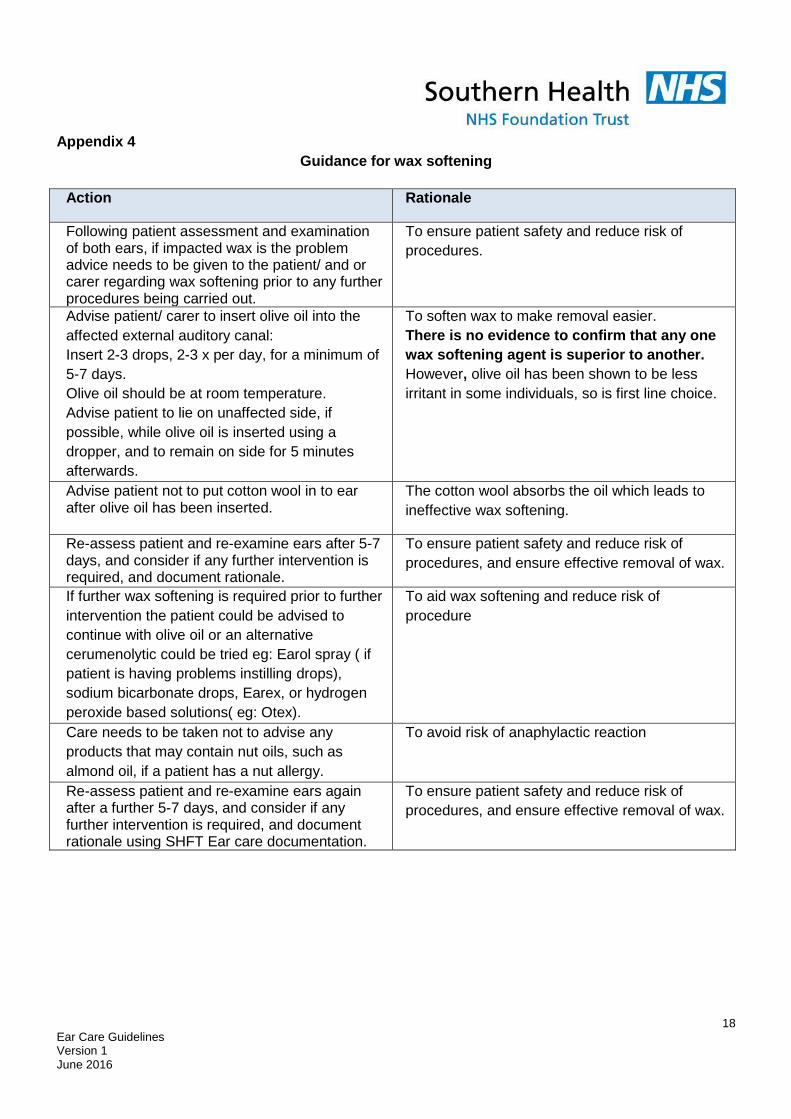
Guidance for wax softening
Action Rationale
Following patient assessment and examination of both ears, if impacted wax is the problem advice needs to be given to the patient/ and or carer regarding wax softening prior to any further procedures being carried out.
To ensure patient safety and reduce risk of
procedures.
Advise patient/ carer to insert olive oil into the
affected external auditory canal:
Insert 2-3 drops, 2-3 x per day, for a minimum of
5-7 days.
Olive oil should be at room temperature.
Advise patient to lie on unaffected side, if
possible, while olive oil is inserted using a
dropper, and to remain on side for 5 minutes
afterwards.
To soften wax to make removal easier.
There is no evidence to confirm that any one
wax softening agent is superior to another.
However, olive oil has been shown to be less
irritant in some individuals, so is first line choice.
Advise patient not to put cotton wool in to ear after olive oil has been inserted.
The cotton wool absorbs the oil which leads to
ineffective wax softening.
Re-assess patient and re-examine ears after 5-7 days, and consider if any further intervention is required, and document rationale.
To ensure patient safety and reduce risk of
procedures, and ensure effective removal of wax.
If further wax softening is required prior to further
intervention the patient could be advised to
continue with olive oil or an alternative
cerumenolytic could be tried eg: Earol spray ( if
patient is having problems instilling drops),
sodium bicarbonate drops, Earex, or hydrogen
peroxide based solutions( eg: Otex).
To aid wax softening and reduce risk of
procedure
Care needs to be taken not to advise any
products that may contain nut oils, such as
almond oil, if a patient has a nut allergy.
To avoid risk of anaphylactic reaction
Re-assess patient and re-examine ears again after a further 5-7 days, and consider if any further intervention is required, and document rationale using SHFT Ear care documentation.
To ensure patient safety and reduce risk of
procedures, and ensure effective removal of wax.
19 Ear Care Guidelines Version 1 June 2016
Appendix 5
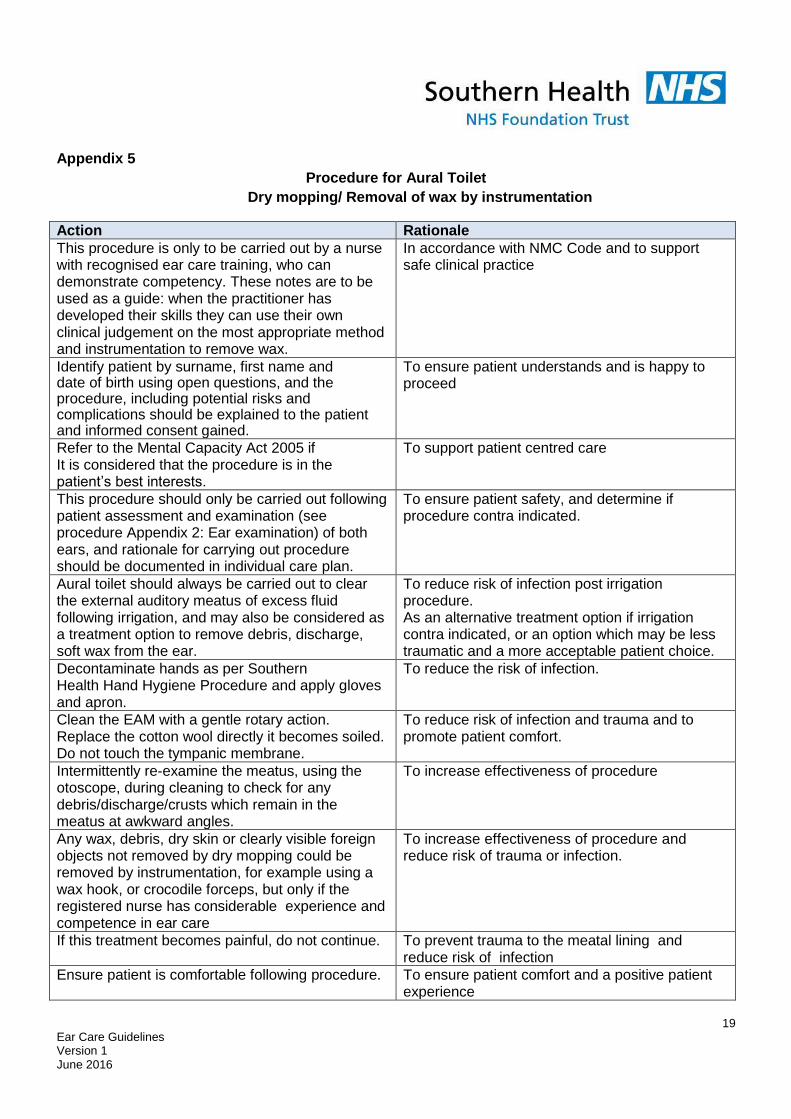
Procedure for Aural Toilet
Dry mopping/ Removal of wax by instrumentation
Action Rationale
This procedure is only to be carried out by a nurse with recognised ear care training, who can demonstrate competency. These notes are to be used as a guide: when the practitioner has developed their skills they can use their own clinical judgement on the most appropriate method and instrumentation to remove wax.
In accordance with NMC Code and to support safe clinical practice
Identify patient by surname, first name and date of birth using open questions, and the procedure, including potential risks and complications should be explained to the patient and informed consent gained.
To ensure patient understands and is happy to proceed
Refer to the Mental Capacity Act 2005 if It is considered that the procedure is in the patient’s best interests.
To support patient centred care
This procedure should only be carried out following patient assessment and examination (see procedure Appendix 2: Ear examination) of both ears, and rationale for carrying out procedure should be documented in individual care plan.
To ensure patient safety, and determine if procedure contra indicated.
Aural toilet should always be carried out to clear the external auditory meatus of excess fluid following irrigation, and may also be considered as a treatment option to remove debris, discharge, soft wax from the ear.
To reduce risk of infection post irrigation procedure. As an alternative treatment option if irrigation contra indicated, or an option which may be less traumatic and a more acceptable patient choice.
Decontaminate hands as per Southern Health Hand Hygiene Procedure and apply gloves and apron.
To reduce the risk of infection.
Clean the EAM with a gentle rotary action. Replace the cotton wool directly it becomes soiled. Do not touch the tympanic membrane.
To reduce risk of infection and trauma and to promote patient comfort.
Intermittently re-examine the meatus, using the otoscope, during cleaning to check for any debris/discharge/crusts which remain in the meatus at awkward angles.
To increase effectiveness of procedure
Any wax, debris, dry skin or clearly visible foreign objects not removed by dry mopping could be removed by instrumentation, for example using a wax hook, or crocodile forceps, but only if the registered nurse has considerable experience and competence in ear care
To increase effectiveness of procedure and reduce risk of trauma or infection.
If this treatment becomes painful, do not continue. To prevent trauma to the meatal lining and reduce risk of infection
Ensure patient is comfortable following procedure.
To ensure patient comfort and a positive patient experience
20 Ear Care Guidelines Version 1 June 2016
Dispose of equipment as per the disposal and handling of waste policy. Remove apron and gloves. Decontaminate hands as per Hand Hygiene procedure.
To ensure patient and staff safety.
Document procedure and what was observed in both ears, including the condition of the tympanic membrane and external auditory meatus using SHFT Ear Care documentation record.
Findings should be documented following the NMC guidelines on record keeping and accountability to support effective patient centred care
21 Ear Care Guidelines Version 1 June 2016
Appendix 6
Procedure for Ear Irrigation
Action Rationale This procedure should only be carried out by a registered nurse who has undergone training and can demonstrate competency.
In accordance with NMC Code and to support safe clinical practice
Identify patient by surname, first name and date of birth using open questions, and the procedure, including potential risks and complications should be explained to the patient and informed consent gained.
To ensure patient understands and is happy to proceed
Refer to the Mental Capacity Act 2005 if It is considered that the procedure is in the patient’s best interests.
To support patient centred care
This procedure should only be carried out following patient assessment and examination of both ears (see Appendix 2: Ear examination procedure), and rationale for carrying out procedure should be documented in individual care plan.
To ensure patient safety, and determine if procedure contra indicated.
This procedure should not be used for the removal of hygroscopic foreign bodies such as peas and lentils.
These will absorb water and expand making
removal difficult.
Ensure electronic irrigation machine has been maintained and cleaned in accordance with manufacturer’s instructions prior to use ( See Appendix: Guidelines for cleaning electronic irrigator)
To ensure patient safety and reduce risk of infection or trauma during procedure.
Gather together all equipment necessary to carry out procedure. Equipment required:
Hand washing facilities/ tap water
Otoscope and a variety of sizes of single use speculae
Electronic irrigator eg: Propulse III or NG.
Disposable jet tips
Head torch
Noots trough/ receiver
Jobson Horne Probe and cotton wool
Disposable waterproof cape and paper towels/ tissues
Disposable apron and non sterile gloves
Rubbish bag
To provide continuity of care and reduce interruption, and improve patient experience.
Decontaminate hands as per Southern Health Hand Hygiene Procedure and apply gloves and apron.
To reduce the risk of infection.
This procedure should be carried out with both participants seated and under direct vision, using a headlight or head mirror and light source.
To aid visibility and support comfort and safety.
Place the protective cape and paper towel on the To protect patient’s clothing
22 Ear Care Guidelines Version 1 June 2016
patient’s shoulder and under the ear to be irrigated. Ask the patient to hold the receiver under the same ear.
Check the temperature of the water with the patient to ensure it is warm enough, and fill the reservoir of the irrigator.
The water should be at body temperature to aid patient comfort and reduce risk of problems, such as dizziness or trauma, during procedure.
Set the pressure at minimum on the irrigation machine. Connect a new disposable jet tip applicator to the tubing of the machine with a firm ‘push/twist’ action. Push until a "click" is felt.
To avoid cross infection, and to ensure the jet tip does not fall off causing potential injury to canal during procedure.
Direct the irrigator tip into the Noots receiver and switch on the machine for 10-20 seconds to discard the initial flow of water. Check the temperature of the water again.
To remove any static water remaining in the tube, circulate the water through the system and eliminate any trapped air or cold water. This also offers the opportunity for the patient to become accustomed to the noise of the machine.
Twist the jet tip so that the water can be aimed along the posterior wall of the External Auditory Meatus- EAM (towards the back of the patient’s head)
To minimise risk of trauma during the procedure
Gently pull the pinna upwards and outwards. To straighten the EAM, and to hold the ear steady to prevent injury
Warn the patient that you are about to start irrigating and that the procedure will be stopped if he/she feels dizzy and/or experiences any pain.
To prevent trauma or patient discomfort
Ensure that the light is directed down the EAM. Place the tip of the nozzle into the EAM entrance and, using the foot control, direct a stream of water along the roof of the EAM and towards the posterior wall (direct towards the back of the patient’s head).
To prevent trauma or patient discomfort
Increase the pressure control gradually if there is difficulty removing the wax, and use the foot control to manage the stream of water.
To prevent trauma or patient discomfort, and increase likelihood of an effective outcome.
It is advisable that a maximum of one reservoir of water per ear is used in any one irrigation procedure.
To prevent trauma or patient discomfort
You may find it beneficial to instil water into both ears (if both require irrigation with water) and return to the procedure after a rest of 15 minutes.
There is evidence to suggest that leaving water in the canal for 15 minutes will increase the chance of success.
Periodically inspect the EAM with the otoscope and inspect the solution running into the receiver.
To monitor progress of procedure, and minimise time and amount of water used for irrigation
After removal of wax or debris, dry mop and remove excess water from the meatus under direct vision using the Jobson Horne probe and best quality cotton wool. (see Apendix: Procedure for aural toilet/ dry mopping)
Stagnation of water and any abrasion of skin during the procedure predispose to infection. Removing the water with the cotton wool tipped probe reduces the risk of post procedure infection.
Examine the ear, both meatus and tympanic membrane, and document what was observed in both ears, the procedure carried out, the condition of the tympanic membrane and external auditory meatus and treatment given. Use the SHFT Ear care nursing record.
Findings should be documented following the NMC guidelines on record keeping and accountability to support effective patient centred care
Ensure patient is comfortable following procedure. To ensure patient comfort and a positive patient
23 Ear Care Guidelines Version 1 June 2016
Dispose of equipment as per the disposal and handling of waste policy. Remove apron and gloves. Decontaminate hands as per Hand Hygiene procedure.
experience To ensure patient and staff safety.
If any abnormality is found a referral should be made following local referral pathway.
To ensure effective outcome for patient and support continuity of care.
Irrigation may be uncomfortable but it should NEVER CAUSE PAIN. STOP IMMEDIATELY if:
Patient complains of pain
Water comes down the nose
Patient swallows excessively
Bleeding occurs
To prevent damage to ear and trauma to patient.
Give advice to patient regarding on going ear care and provide SHFT written patient information leaflet, and advise of possible complications following procedure, such as dizziness, infection, tinnitus.
To ensure effective outcome for patient and support continuity of care.
Document procedure and what was observed in both ears, including the condition of the tympanic membrane and external auditory meatus using SHFT Ear Care documentation record.
Findings should be documented following the NMC guidelines on record keeping and accountability to support effective patient centred care
24 Ear Care Guidelines Version 1 June 2016
Appendix 7
Cleaning guidelines for an Electronic Irrigator
Ear irrigation is a clean procedure.
Disposable jet tips must be used with the electronic irrigator.
The frequency for decontamination of Propulse Electronic Ear Irrigator pumps and waterways should be once a day only and take place prior to the first use.
Stage 1: BEFORE USE
• Before use, the electronic irrigator must be disinfected using a solution of Sodium
Dichloroisocyanurate 0.1% (NaDCC). This is available in the form of Chlor-Clean tablets, or
Presept. These or similar products should be used according to manufacturer’s instructions, to
make a solution which provides 1000 parts (NaDCC) per million (0.1%). Chlor-Clean is
mentioned particularly because it contains a surfactant (i.e. detergent) in addition to a
disinfectant. Any damage caused to the propulse electronic irrigator by not using the
recommended cleaning agent will invalidate the manufacturer’s warranty.
• Place 1 propulse cleaning tablet into the reservoir, fill with warm water to the 500ml mark and
wait for the tablet to completely dissolve.
• Run the irrigation system for a few seconds to allow the solution to fill the pump and flexible
tubing.
• Leave to stand for 10 minutes.
• DO NOT leave the solution in the unit for longer than stated.
• Empty the reservoir of the solution, and then fill the reservoir with either cool boiled water or well-
run cold tap water and flush through the whole system to ensure no cleaning solution remains.
• This procedure should be carried out prior to each day’s usage of the ear irrigator.
Stage 2: AFTER USE
• After use empty the reservoir and operate the device to purge any residual water.
• The manufacturer’s guidelines do not ask that it is disinfected again at the end of the day, but to
ensure that is thoroughly dry before putting away for storage.
(Adapted from The Rotherham Primary Ear Care Centre guidelines: 2014 and the Propulse NG user manual: 2012)
25 Ear Care Guidelines Version 1 June 2016
DATA SHEET: Sodium Dichloroisocyanurate (NaDCC) 1. Hazards identification HARMFUL if swallowed. Irritating to eyes and respiratory system. Contact with acid liberates toxic gas. On contact with moisture, NaDCC readily decomposes to Chlorine, Hypochlorous Acid & Cyanuric Acid. 2. First aid measures Eye Contact: Immediately flush with plenty of clean water for at least 15 minutes. If irritation persists, seek medical attention. Skin Contact: Promptly wash thoroughly with water for at least 15 minutes whilst removing contaminated clothing. Wash any contaminated clothing well, before re-use. Ingestion: Immediately rinse mouth, then drink plenty of water or milk. Do not induce vomiting. Seek medical attention. Inhalation: Move to fresh air. If irritation persists, seek medical attention. 3. Fire-fighting measures Special Fire or Explosion Hazards: Product is not flammable itself, but contact with combustible material may cause fire. Product combustible if dehydrated by drying. Decomposes above 250OC with release of chlorine & other toxic fumes. A thermal decomposition can be extinguished by flooding with copious amounts of water or by isolating the decomposing material in open air and allowing it to be consumed. Use self-contained breathing apparatus and goggles. Do not approach from leeward. Suitable Extinguishing Media: Pressurised water or dry powder. Do not use dry fire extinguishers containing ammonium compounds. Other Recommendations: Remove the product if it is safe to do so, before using water for fire fighting, in order to minimise hazards from release of toxic fumes. It will often be safer to let the fire burn itself out. Where it is decided to fight the fire with water, large quantities must be used. If insufficient water is used there may be an explosion hazard associated with hot damp material. NaDCC may generate nitrogen trichloride when it is left under damp conditions. 4. Accidental release measures Any spillage should be cleaned up as soon as possible to prevent contamination with foreign materials with which it may react - see section 8 (Stability and Reactivity) below. Handle spillage carefully, do not return spilled material to original container. If tablets are dry and uncontaminated, collect into heavy-duty plastic bag; where possible and suitable, use material as originally intended. Wash away any residue with copious amounts of water. If tablets are contaminated they should be transferred to waste ground, spread thinly and covered with a thin layer of earth; a smell of chlorine will be noted until the material has degraded. Keep people, vehicles and animals away from the disposal area. If tablets become damp they will effervesce, evolving carbon dioxide and may decompose to give off chlorine fumes; transfer spillage to unsealed plastic bags, avoiding any large masses of material within the bags, and remove to waste ground for immediate treatment/disposal as above; avoid breathing fumes. Wash away residue with copious amounts of water. If spillage of tablets is large (more than 100Kg), place into bins lined with polythene bags and eliminate in accordance with locally valid disposal regulations.
26 Ear Care Guidelines Version 1 June 2016
5. Handling and storage Recommended Storage Conditions: Store away from all incompatibles and combustibles - see section 8 (Stability and Reactivity) below. Store in a cool, dry, well-ventilated place. Moisture sensitive. Avoid high humidity levels. Do not allow water to get into container. Keep away from fire, heat, flame & direct sunlight. Keep container tightly closed. Keep out of reach of children. Never store damp or contaminated material. Recommended Handling Precautions: Avoid contact with eyes, skin & clothing. When handling large quantities of tablets, wear chemical resistant gloves and safety goggles. Avoid breathing any dust. Wash thoroughly after handling. Use protective equipment recommended in section 6 (Exposure controls/personal protection). Do not eat, drink or smoke when handling this material. 6. Exposure controls/personal protection Occupational Exposure Limits (EH40/2002): Long Term Exposure Limit to Chlorine – (8 hours TWA) 0.5ppm 1.5mgm-3. Short Term Exposure Limit to Chlorine – (10 minutes) 1ppm 2.9mgm-3 Long term exposure Limit to amorphous silica – (8 hours TWA) - 6mgm-3 Respiratory Protection: Where any dust in the breathing zone cannot be controlled with ventilation, wear an officially approved respirator (NIOSH/MSHA or equivalent agency) for protection against airborne dust. Ventilation: Use local exhaust ventilation where appropriate. Eye Protection: If airborne dust concentrations are high, wear appropriate protective goggles. Wash eyes with clean water where there is potential eye contact. Skin Protection: When handling large bulk quantities wear protective gloves. Wash immediately if skin is contaminated. Remove and wash contaminated clothing and clean up equipment before re-use. Wash thoroughly with soap and water after handling. 7. Physical and chemical properties Appearance: White flat bevelled tablet Oxidising Properties: Non-Oxidising Odour: Characteristic Chlorine Odour Flash point: Not flashing pH: As is - not applicable Flammability: Not flammable pH: In solution - 5.0 - 6.0 approx. Autoflammability: Not autoflammable Solubility: Freely soluble Explosion Properties: Not explosive 8. Stability and reactivity Conditions to Avoid: Do not store on or near heat sources or naked flame. Avoid moisture. NaDCC decomposes at temperatures above 240OC liberating toxic gases. Materials to Avoid: Contact with water liberates chlorine, and with nitrogen compounds may cause explosion. Avoid organic materials, oils, grease, sawdust, reducing agents, nitrogen-containing compounds, calcium hypochlorite, other oxidizers, acids, alkalis, cationic and certain non-ionic surfactants.
27 Ear Care Guidelines Version 1 June 2016
9. Toxicological information Route of entry: inhalation, skin contact & ingestion. Inhalation of NaDCC is irritating to the nose, mouth, throat and lungs. Ingestion of NaDCC can cause irritation and or/burns to the gastrointestinal tract. Skin & Eye Contact with NaDCC can cause severe irritation and/or burns, characterized by redness, swelling and scab formation. May cause impairment of vision and corneal damage. Toxicological Data: NaDCC Acute toxicity Oral LD50 (rat) ca. 1825mg/kg Eye Irritation (rabbit) Severe irritant Rabbit dermal LD50 >20,000mg/kg Carcinogenicity: This chemical is not considered to be carcinogenic by any reference source. 10. Ecological information NaDCC is highly toxic to fish. Do not discharge into lakes, ponds, streams or public water unless in accordance with the permit of official regulations. 11. Disposal considerations Disposal should be carried out in accordance with all official regulations. If material is dry, incineration is recommended.
28 Ear Care Guidelines Version 1 June 2016
Appendix 8
REFERRAL GUIDELINES This guideline will provide information on the management of the following common conditions which can affect the ear, and when to refer to the GP for referral on to the local ENT department:
Wax Impaction
Otitis Externa
Recurrent Acute Otitis Media
Otitis Media with Effusion (Glue Ear)
Dizziness
Tinnitus
Deafness Wax Impaction Treatment: Wax can be removed by ear irrigation, aural toilet or microsuction. Olive oil or other cerumenolytics can reduce build up and soften wax, although water and saline drops have been shown to be as good as more costly products. A Guide to the Management and Referral of When to refer: Refer to the routine ENT clinic if there is difficulty removing the wax despite olive oil. Refer if a patient is uncooperative or there is uncertainty about the condition of the tympanic membrane. The local ENT department may have a direct referral ear care clinic. Patients will require microsuction if contraindications to irrigation exist such as: indications to irrigation: • The patient has a tympanic membrane perforation or a mucoid discharge which may suggest a perforation. • The patient has had otitis media or acute otitis externa in the last six weeks. • The patient has had previous ear surgery, seek advice. • The patient has suffered complications with previous ear irrigation. • The patient has a profound hearing loss in the other ear as it would be inadvisable to risk complications in the only hearing ear. • The patient has had a cleft palate as he is more prone to middle ear disease. Contra Otitis Externa Otitis externa is extremely common. Predisposing factors are scratching of the external canal with cotton buds or other implements and narrow external auditory canals. A particularly important factor is wet ears (humid climates, swimming, syringing without drying the canal, frequent hair washing or lying in the bath to wash the hair). Symptoms and signs: Whatever the predisposing factor, the skin of the external auditory canal becomes oedematous. Otalgia, otorrhoea and a blocked sensation in the ears with a mild hearing loss are common in the acute stage. In the chronic form itching is a frequent complaint. Treatment: It is essential that debris in the ear canal is removed so that the ear drops can penetrate effectively. If the practice nurse is not trained in aural toilet, the patient may need to be referred for suction clearance. Systemic antibiotics are not usually required unless there are signs of associated lymphadenitis, perichondritis or cellulitis. Advise the patient to keep the ears dry and not to insert implements.
29 Ear Care Guidelines Version 1 June 2016
The first line of treatment is a combination steroid and antibiotic (eg. neomycin) drop or spray. If the patient does not respond to this within a few days, take a swab, change to an alternative antibiotic / steroid combination and repeat the aural toilet. Consider fungal infection. For recurrent mild conditions, proprietary diluted acetic acid can be used in primary care to prevent the condition progressing. When to refer: If the patient does not respond to the second line treatment, refer to the emergency ENT clinic. Refer if there is persistent discharge or pain, diagnostic doubt about the condition of the tympanic membrane or if the patient is immuno-compromised or a poorly controlled diabetic as there is a risk of “malignant “ otitis externa (temporal bone osteomyelitis). If the skin of the external canal is so swollen that drops will patently not enter the canal, then a dressing or wick may need to be inserted. Dizziness The majority of dizziness in the elderly is of vascular or degenerative origin. Unsteadiness and lightheadedness are usually non-otological. Medical: Cardiovascular, metabolic and neurological conditions, anaemia, ocular disease, medications and cervical spine problems. Psychological: Anxiety and hyperventilation. Otological: Benign paroxysmal positional vertigo, acute vestibular failure (labyrinthitis), Mèniére’s disease, some middle ear disease and very rarely acoustic neuroma. Symptoms: If the symptoms are from the inner ear then the patient will describe a hallucination of movement, usually rotational in nature and frequently accompanied by nausea, vomiting and nystagmus. Mèniére’s syndrome consists of a triad of episodic vertigo, associated tinnitus and a fluctuating hearing loss. In benign paroxysmal positional vertigo (BPPV), short-lived episodes of rotational vertigo usually occur when turning over in bed. Loss of consciousness is unlikely to be caused by inner ear problems. Treatment: A general medical examination, a careful history and blood pressure measurement may point to the cause of the dizziness. If “the room is spinning” the patient may find it helpful to focus on a fixed object. Maintain hydration if nausea and vomiting are a feature. Vestibular sedatives such as Prochlorperazine or Cinnarizine are usually helpful in acute vertigo (eg. acute labyrinthitis, acute episode of Mèniére’s), but long term use does not help with vestibular rehabilitation. Longer term treatment with Betahistine may be helpful in Mèniére’s disease. A Guide to the Management and Referral of When to refer: Some ENT departments run special neurotology clinics. Refer to ENT if there are ear symptoms or signs such as a discharging ear as some chronic ear disease can cause vertigo. For patients with BPPV,most can be helped by “repositioning” manoeuvres, performed in the ENT/audiology department. In the absence of otological signs or symptoms accompanying the dizziness the patient may benefit from a neurological opinion. Tinnitus Tinnitus is the sensation of sound which does not come from an external source. Tinnitus is a troublesome and common condition which is not always curable. It can occur in any age group but is more common with increasing age. Persistent tinnitus occurs in about 10% of the population. It is essential to exclude serious pathology (such as an acoustic neuroma if the tinnitus is unilateral) and then to treat and to support the sufferer as best one can. Aetiology Local: Any hearing loss. General: Hyperdynamic circulations (as in hypertension or anaemia), carotid bruits (associated with a carotid artery stenosis).
30 Ear Care Guidelines Version 1 June 2016
Drugs : eg. NSAIDs, caffeine, alcohol. Symptoms: Tinnitus affects people in different ways. On the one hand it may be non intrusive, or on the other hand it can contribute to suicide. Most patients recognise the link between their level of emotional and physical stress and the perceived “loudness” of the tinnitus. Treatment: A full otological and general history must be taken to exclude other pathologies. Exclude obvious local causes such as wax impaction. A pure tone audiogram is of use in establishing the degree of hearing loss that may be associated with the tinnitus. The importance of unilateral tinnitus (versus bilateral symmetrical tinnitus) is that it is sometimes a symptom of an acoustic neuroma. Direct the patient towards specialised help such as a hearing therapist, self help groups and the British Tinnitus Association. Relaxation techniques help some patients. When to refer: Refer to the routine ENT clinic if the tinnitus becomes intrusive (sleep disturbance), if it is unilateral, or if the tympanic membranes are abnormal. Common Ear Conditions Adult Deafness Sudden-onset conductive hearing loss (usually unilateral) After URTI / air flights / diving. The patient is unable to ‘pop’ the ear (no movement of the drum on performing the Valsalva manoeuvre). There may be the appearance of fluid behind the drum. The bone conduction is better than air conduction in that ear. Treatment: Decongest the nose and encourage auto-inflation of the ears. When to refer: If there are continued problems despite nasal treatment then refer to a routine ENT clinic. Sudden–onset unilateral sensori-neural hearing loss The patient will usually report suddenly going deaf in one ear. There is a normal looking tympanic membrane. Treatment: Treatment remains controversial because of the lack of high quality evidence. Many doctors in the UK use a short course of prednisolone, possibly combined with antivirals. Spontaneous recovery is seen in 50% of patients. When to refer: Refer to the ENT emergency clinic within a week of onset. Presbyacussis : A symetrical, gradual, high frequency hearing loss in old age. When to refer: Direct referral to the audiology department should be used if this facility exists. If the hearing loss is asymetrical then refer routinely to ENT as further investigations may be required to exclude an acoustic neuroma. Recurrent Acute Otitis Media (RAOM) Approximately 40% of children will suffer one or more episodes before the age of 7 years. At least 85% will resolve within 72 hours without treatment and it is uncommon in adults. A significant proportion of children with RAOM failing medical management appear to have a partial maturational IgA deficiency. Children with RAOM may require long-term low-dose antibiotic treatment or grommet insertion until they grow out of the condition. Grommet surgery in children with RAOM can prevent infection, pain and the need for antibiotics.
31 Ear Care Guidelines Version 1 June 2016
Symptoms and signs: Earache, hearing loss and a red bulging drum prior to tympanic membrane rupture. The child may be irritable with a fever and sickness. After rupture there will be relief of pain and a purulent discharge. Treatment: Analgesia such as a combination of ibuprofen and Paracetamol. If unresolved after three days prescribe amoxicillin or erythromycin. If antibiotics are prescribed the length of the course should be reviewed after three days. Encourage nose blowing. If treatment fails with the first line antibiotics, prescribe co-Amoxiclav or Clarithromycin. When to refer: Refer to a routine ENT clinic if: a) there is a failure of the infection to resolve despite the above treatment. b) there is a persistent perforation. c) there are more than 6 attacks in one year for a period of more than one year. Otitis Media with Effusion (OME) ‘Glue Ear’ 85% of children experience glue ear at some stage. 50% will resolve spontaneously within three months. Peak ages are two and five years and a hearing assessment quantifies severity. Winter, URTIs, child care settings and passive smoking are accepted environmental risk factors. Symptoms and signs: There will be a noticeable hearing impairment and/or speech and language difficulties and behavioral problems. There may be an association with recurrent acute otitis media. The key features on examination are a drum that appears dull, retracted or poorly mobile. There may be an air-fluid level or bubbles visible behind the tympanic membrane. Treatment: Reduce exposure to cigarette smoke. Persistent effusions do not respond to oral decongestants or mucolytics. Treatment of rhinitis may be appropriate and helpful. Auto-inflation of the eustachian tube has been shown to produce short term improvement in older children. Generally, a three month period of watchful waiting is recommended prior to referral. If the condition persists and there is a clinically obvious effect on speech, language, learning or behaviour, then children over 3 1/2 years may benefit from adenoidectomy and/or ventilation tube (grommet) insertion. When to refer: Refer children to the routine ENT clinic if there have been 8-12 weeks of hearing problems, associated speech delay or behavioural problems (4 weeks if the child has other disabilities making correction of the hearing loss more urgent). Referral should take into account parental concerns or those raised by the school or health visitor. Refer adults urgently if there is no history of URTI or barotrauma and especially if oriental (higher risk of nasopharyngeal carcinoma). Adapted from: A Guide to the Referral of Common ENT Conditions Paul Harkness Consultant ENT Surgeon Rotherham General Hospital Revised 2011
32 Ear Care Guidelines Version 1 June 2016
Appendix 9