Embed Size (px)
DESCRIPTION
E C G to continue…. Interval changes assessment. PR (PQ) interval. Normally .12 s - .20 s (that is 3 – 5 mm of horizontal distance) Shorter (e.g.) in preexcitation syndromes Longer (e.g.) in AV block of first degree Dependent of the frequency For 60 beats / s is around 0.45 s. - PowerPoint PPT Presentation
Citation preview
ECG to continue….
Interval changes assessment
PR (PQ) interval• Normally .12 s - .20 s
• (that is 3 – 5 mm of horizontal distance)
• Shorter (e.g.) in preexcitation syndromes
• Longer (e.g.) in AV block of first degree
• Dependent of the frequency
• For 60 beats / s is around 0.45 s
QT interval
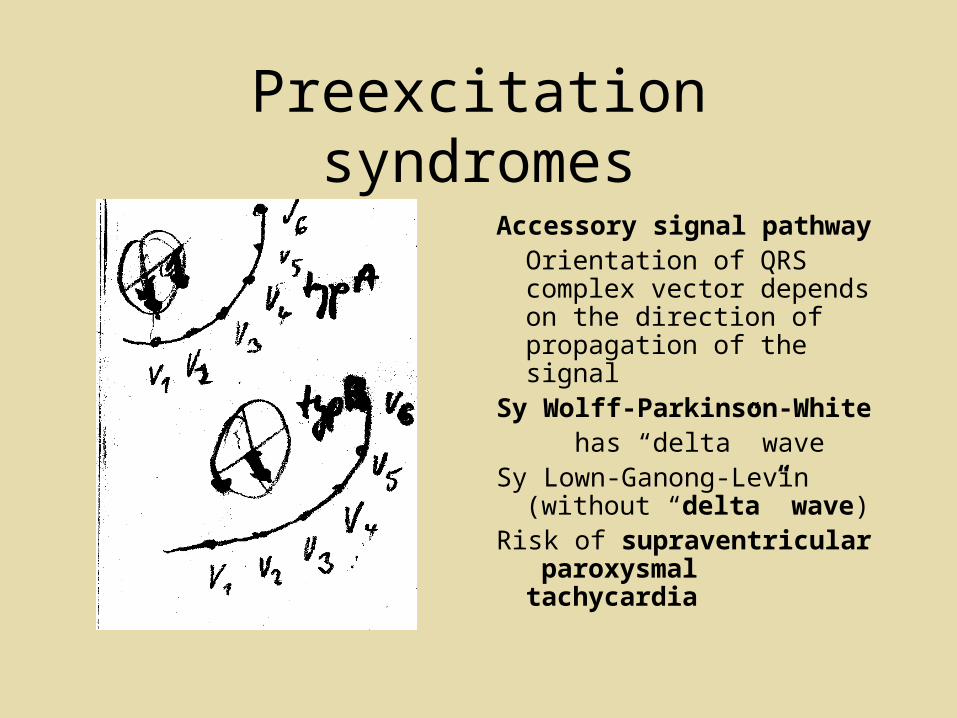
Preexcitation syndromes
Accessory signal pathwayOrientation of QRS complex vector depends on the direction of propagation of the signal
Sy Wolff-Parkinson-White has “delta” waveSy Lown-Ganong-Levin
(without “delta” wave)Risk of supraventricular
paroxysmal tachycardia
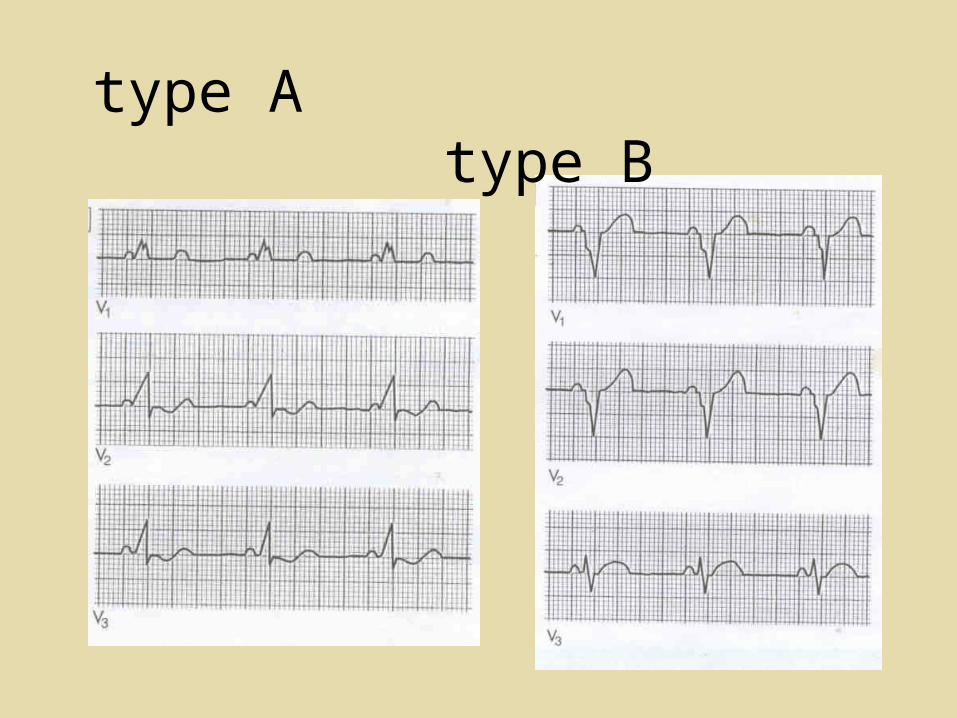
type A type B
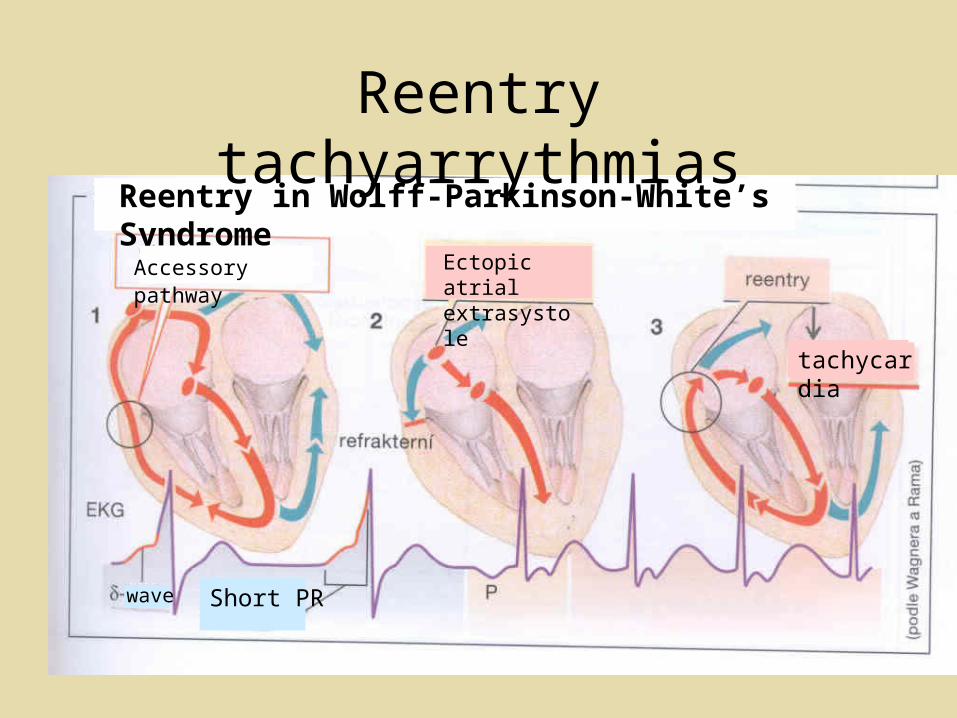
Reentry tachyarrythmiasReentry in Wolff-Parkinson-White’s Syndrome
Accessory pathway Ectopic atrial extrasystole
tachycardia
Short PRwave
AV block
1-st degree: Long PR inteval
2-nd degree type one
type two
3-rd degree: No connection between atria and ventriculi
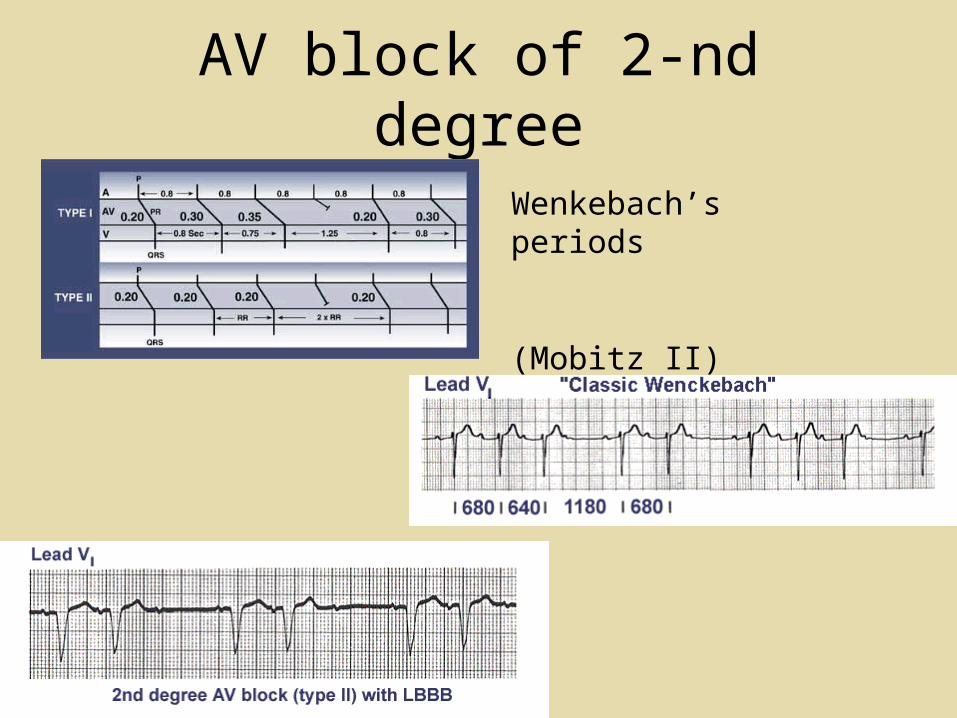
AV block of 2-nd degree
Wenkebach’s periods
(Mobitz II)
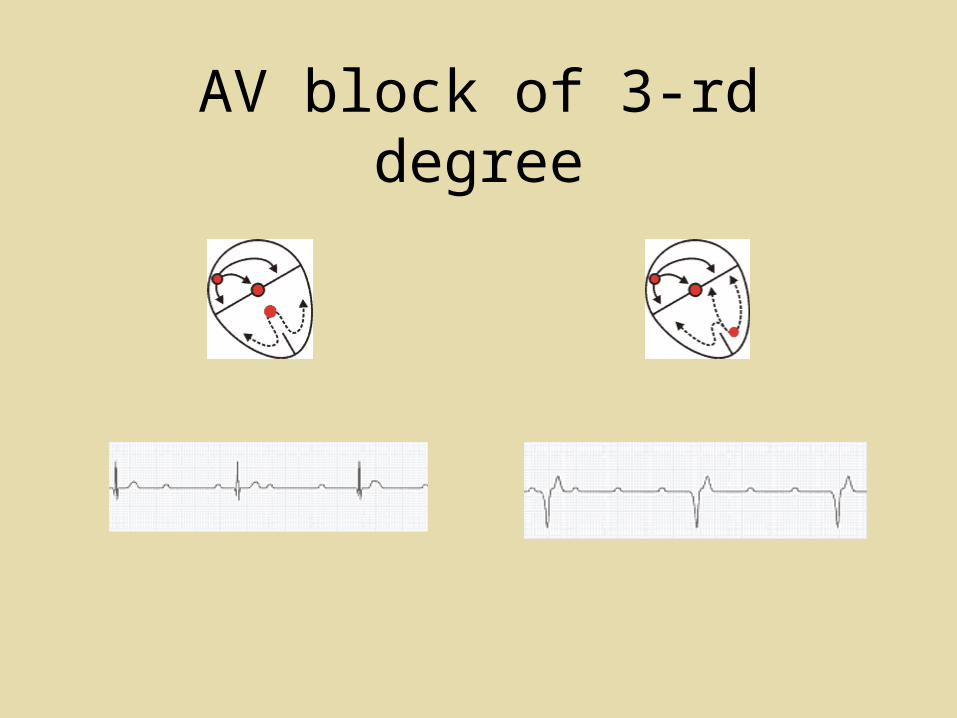
AV block of 3-rd degree
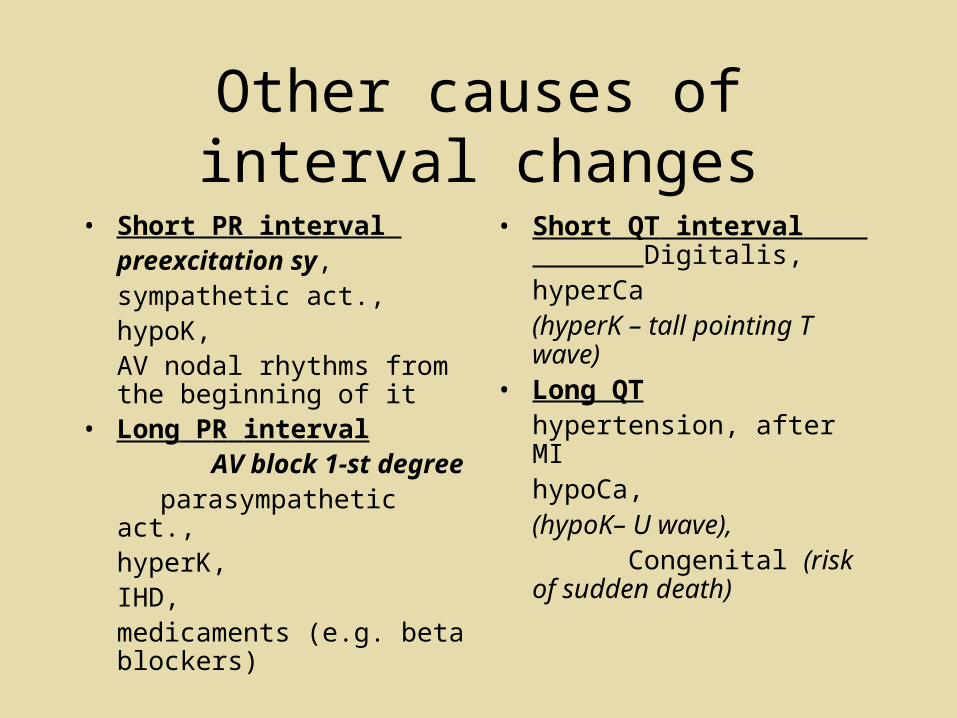
Other causes of interval changes
• Short PR interval preexcitation sy,sympathetic act., hypoK,AV nodal rhythms from the beginning of it
• Long PR interval AV block 1-st degree parasympathetic act.,
hyperK,IHD, medicaments (e.g. beta blockers)
• Short QT interval Digitalis,hyperCa (hyperK – tall pointing T wave)
• Long QT hypertension, after MI
hypoCa, (hypoK– U wave),
Congenital (risk of sudden death)
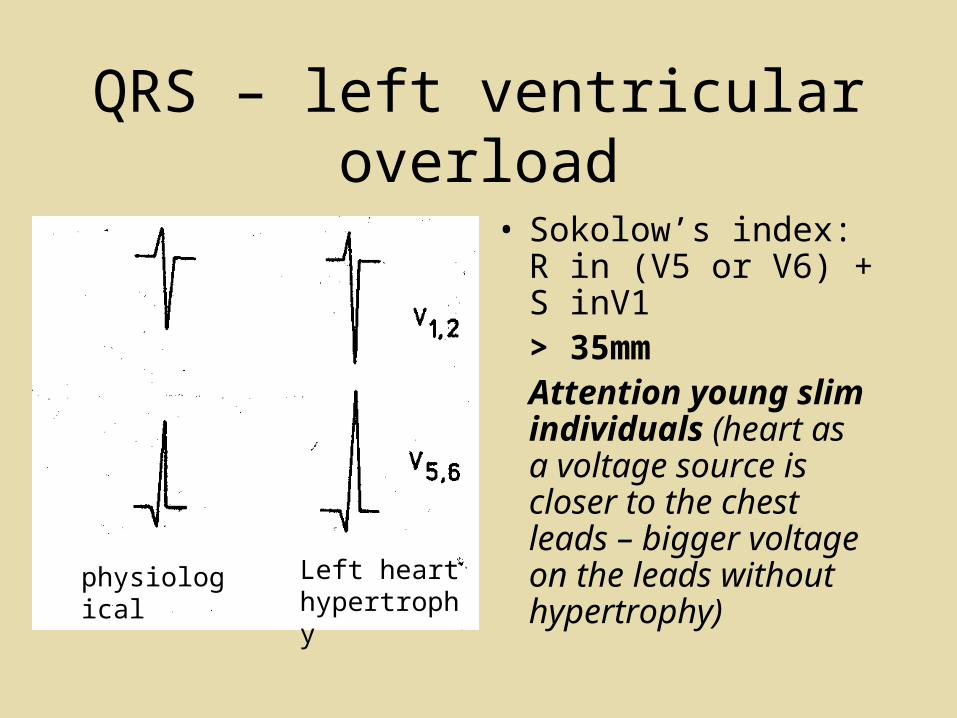
QRS – left ventricular overload
• Sokolow’s index: R in (V5 or V6) + S inV1 > 35mmAttention young slim individuals (heart as a voltage source is closer to the chest leads – bigger voltage on the leads without hypertrophy)
physiological Left heart hypertrophy
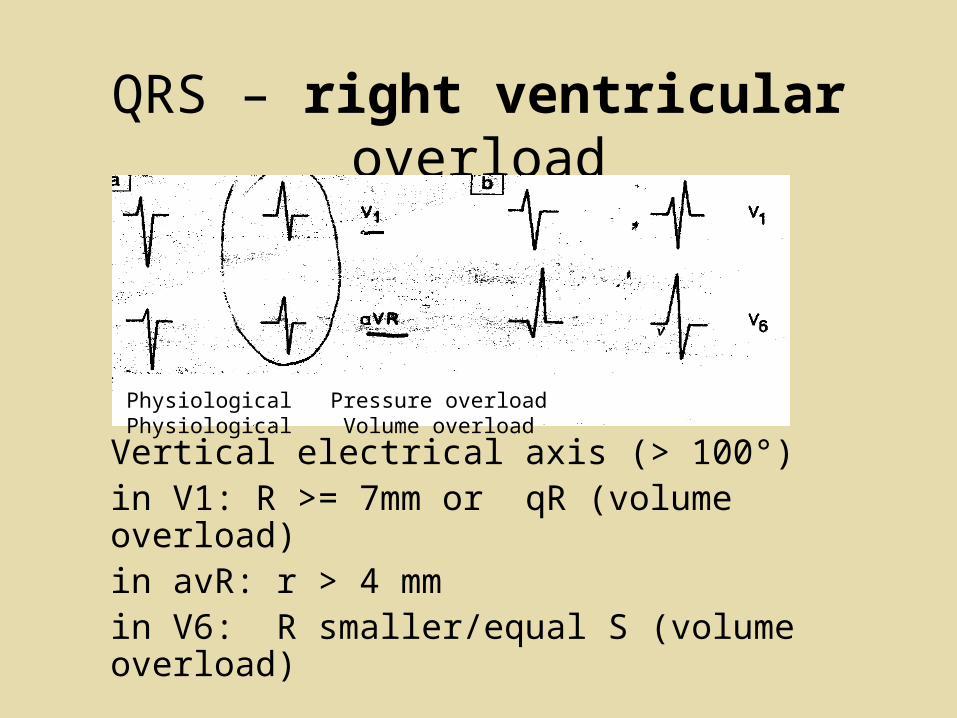
QRS – right ventricular overload
Vertical electrical axis (> 100°)in V1: R >= 7mm or qR (volume overload)in avR: r > 4 mm in V6: R smaller/equal S (volume overload)
Physiological Pressure overload Physiological Volume overload
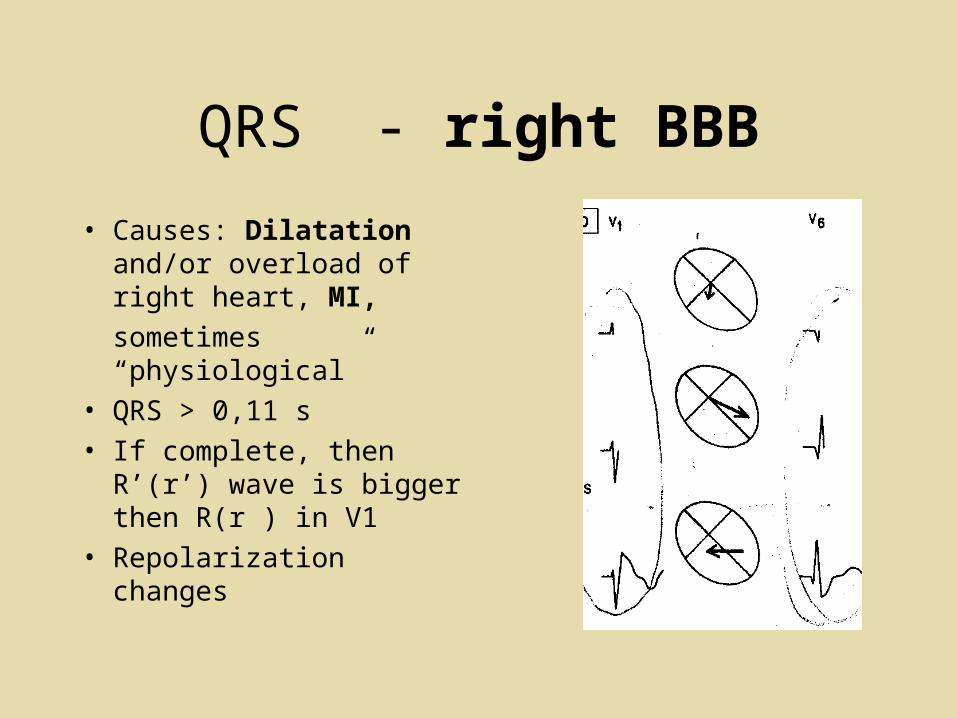
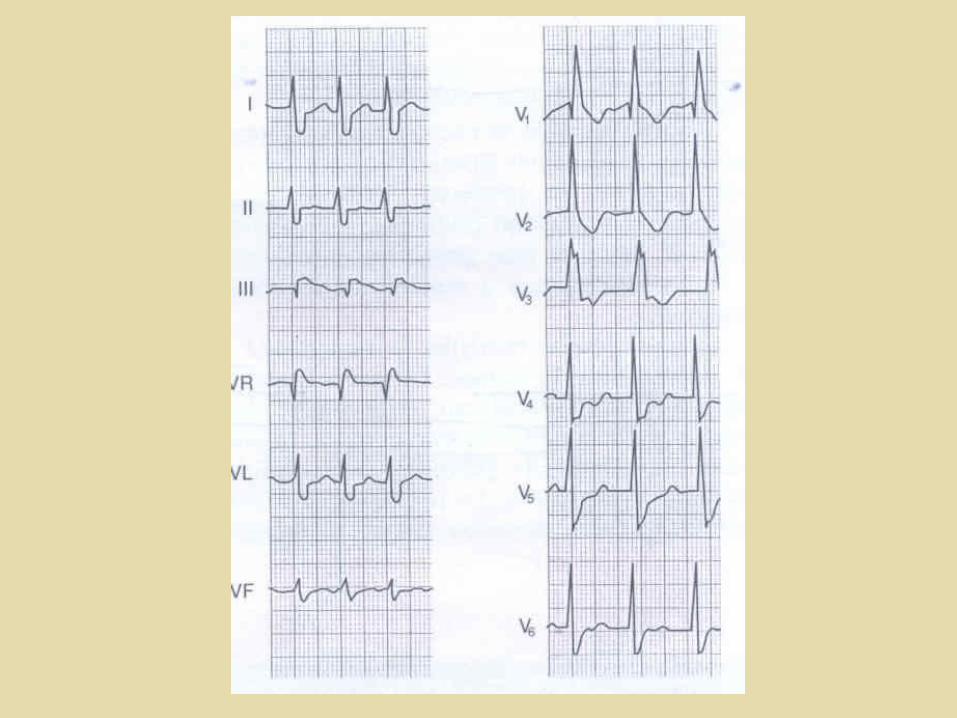
QRS - right BBB
• Causes: Dilatation and/or overload of right heart, MI,
sometimes “physiological”
• QRS > 0,11 s
• If complete, then R’(r’) wave is bigger then R(r ) in V1
• Repolarization changes
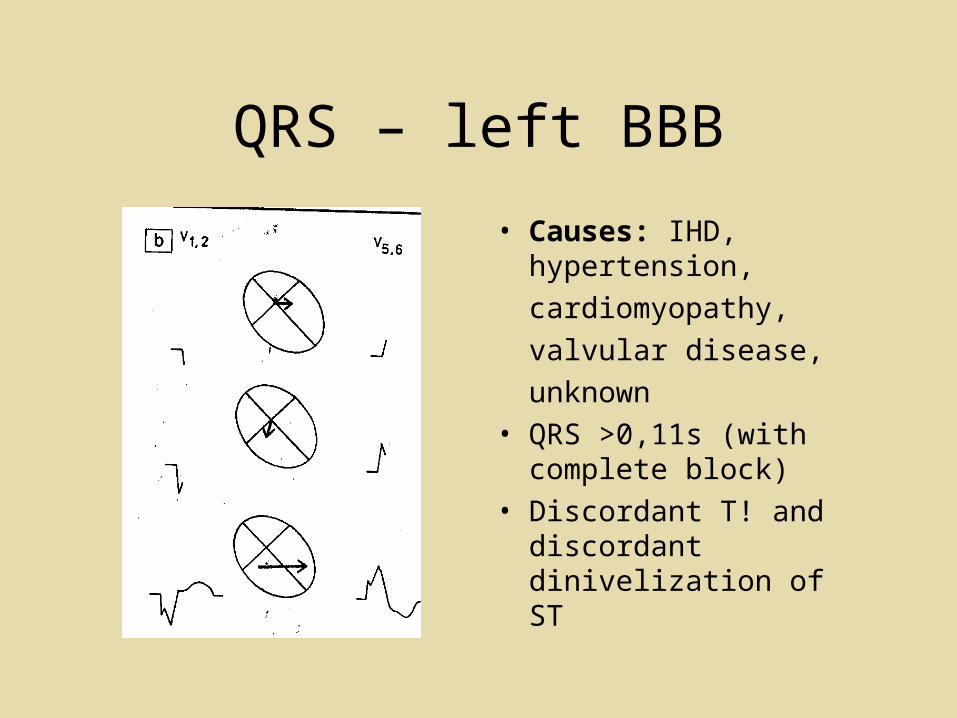
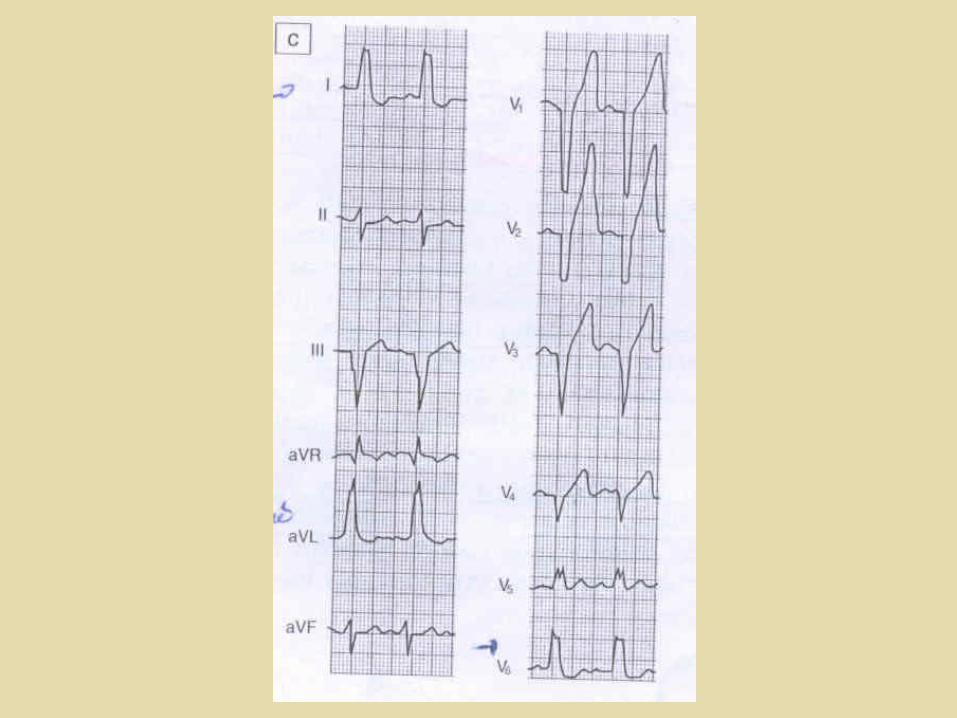
QRS – left BBB
• Causes: IHD, hypertension,
cardiomyopathy,
valvular disease,
unknown
• QRS >0,11s (with complete block)
• Discordant T! and discordant dinivelization of ST
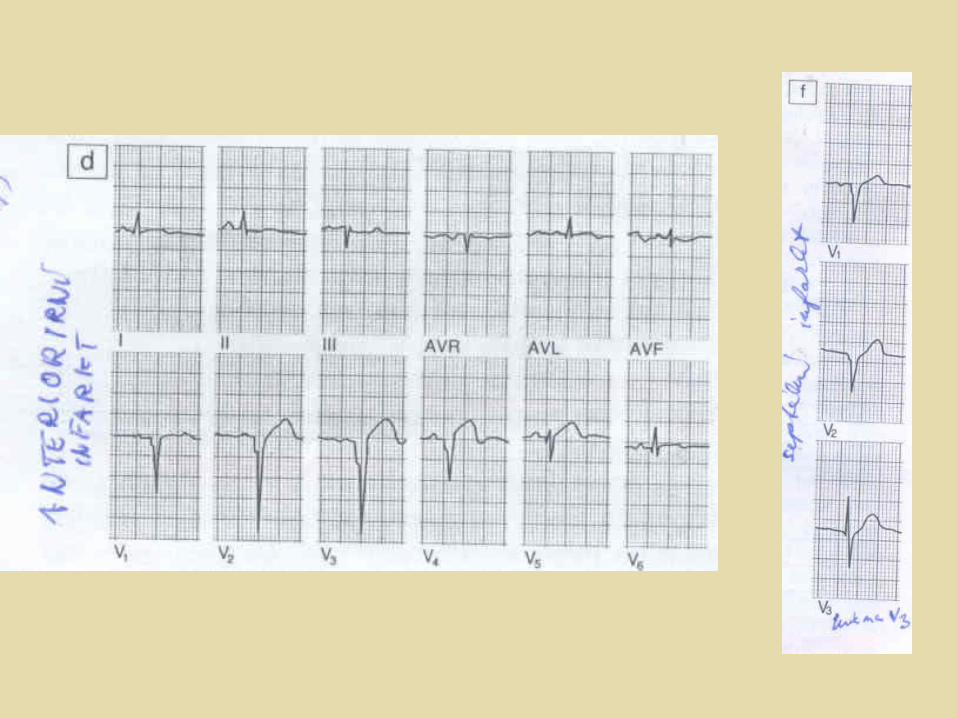
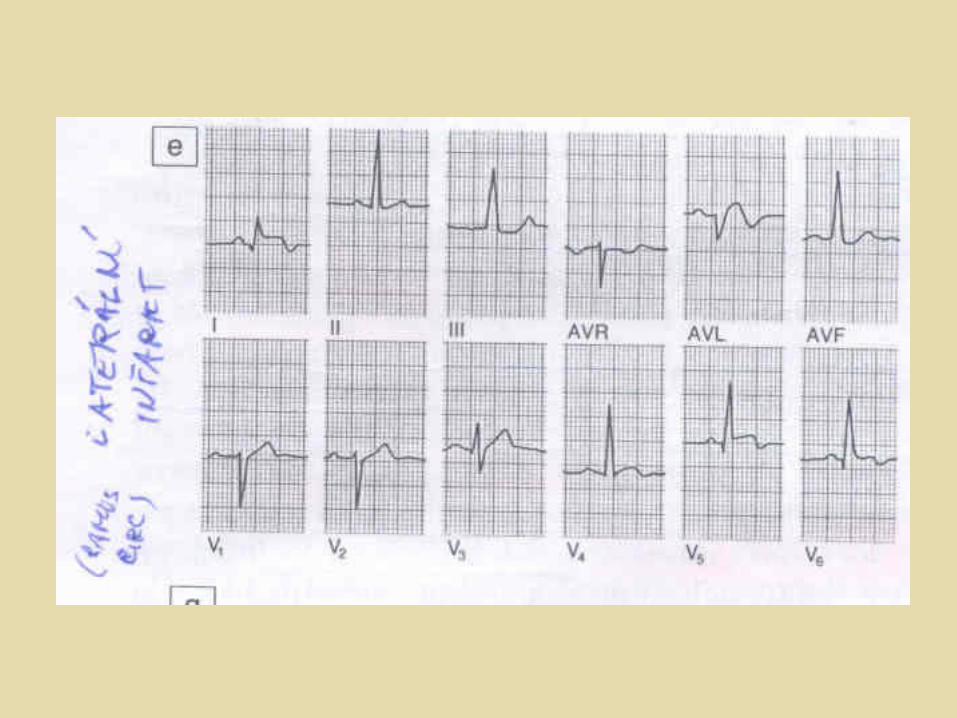
QRS – Q wave myocardial infarction
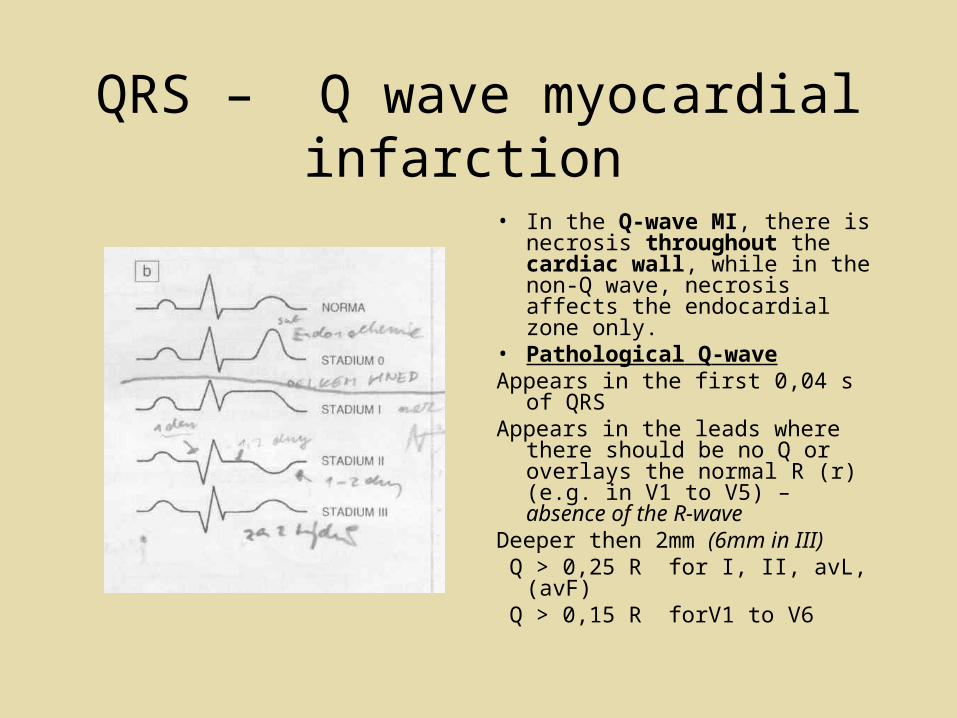
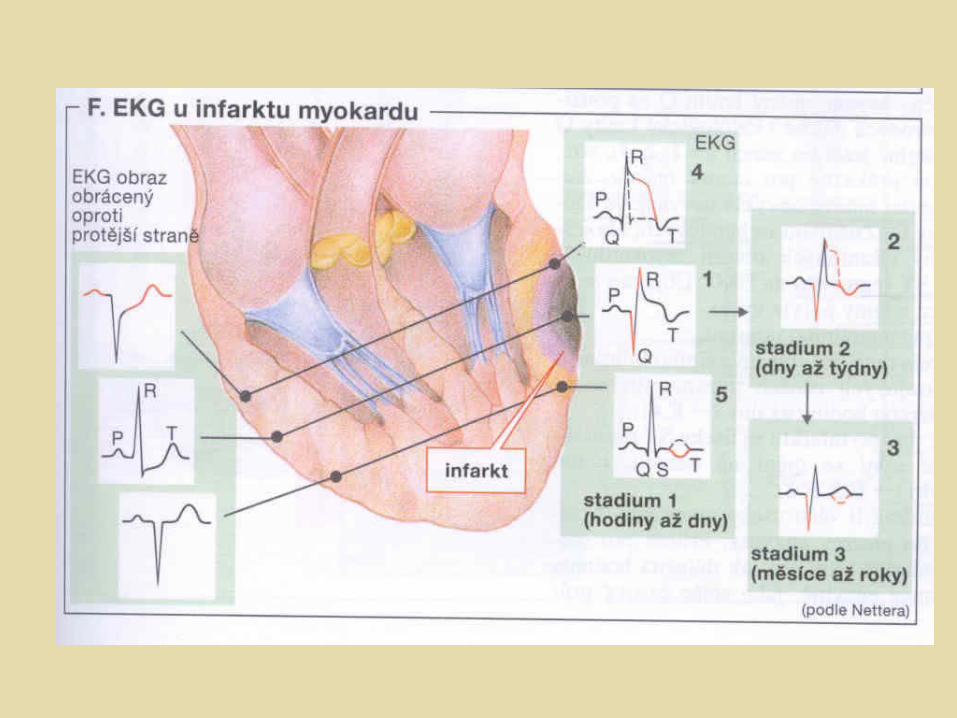
• In the Q-wave MI, there is necrosis throughout the cardiac wall, while in the non-Q wave, necrosis affects the endocardial zone only.
• Pathological Q-waveAppears in the first 0,04 s of QRSAppears in the leads where there
should be no Q or overlays the normal R (r) (e.g. in V1 to V5) – absence of the R-wave
Deeper then 2mm (6mm in III) Q > 0,25 R for I, II, avL, (avF) Q > 0,15 R forV1 to V6
QRS – Q wave MI
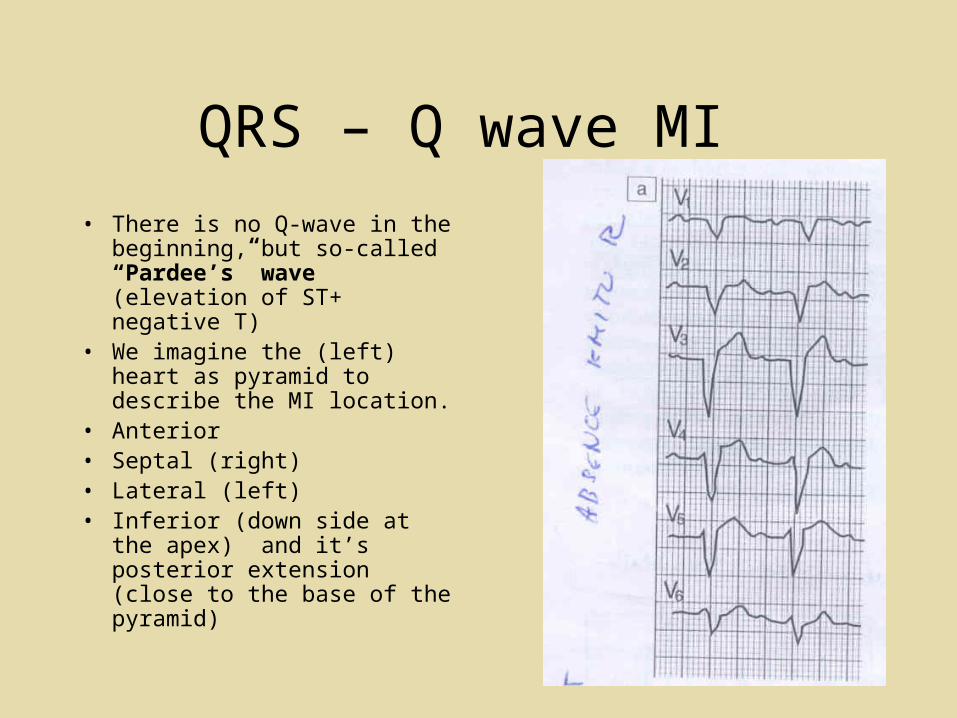
• There is no Q-wave in the beginning, but so-called “Pardee’s” wave (elevation of ST+ negative T)
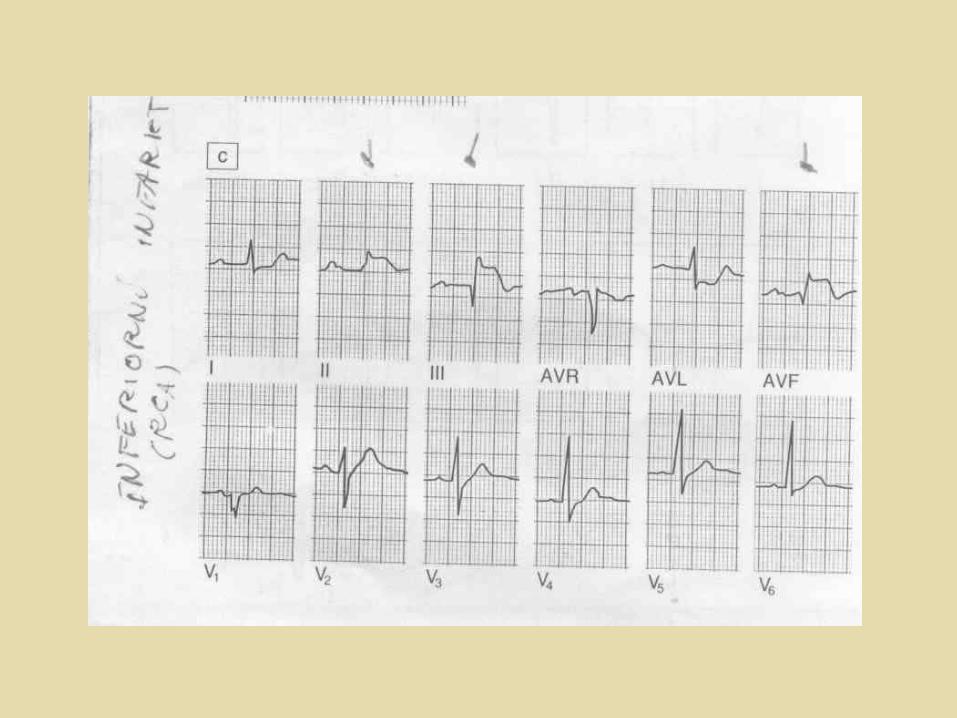
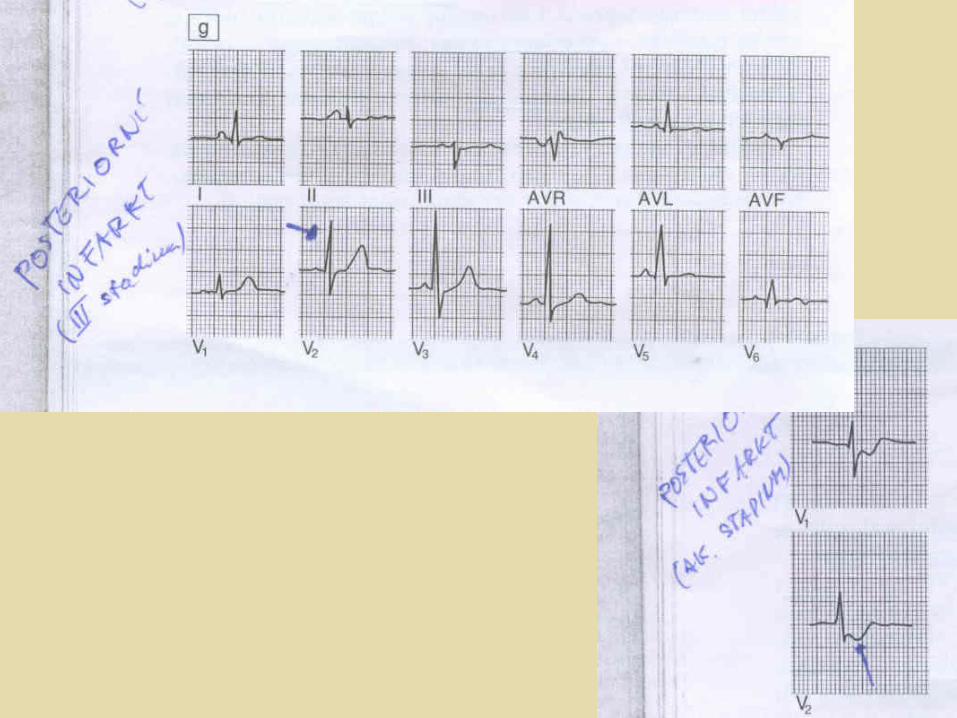
• We imagine the (left) heart as pyramid to describe the MI location.
• Anterior • Septal (right)• Lateral (left)• Inferior (down side at the apex)
and it’s posterior extension (close to the base of the pyramid)
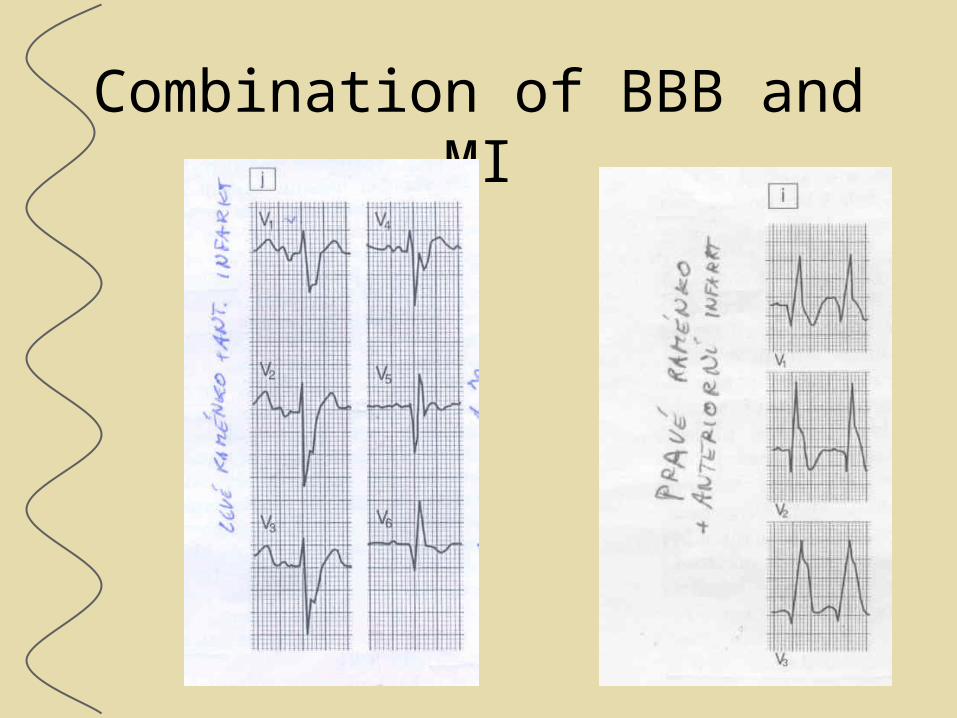
Combination of BBB and MI
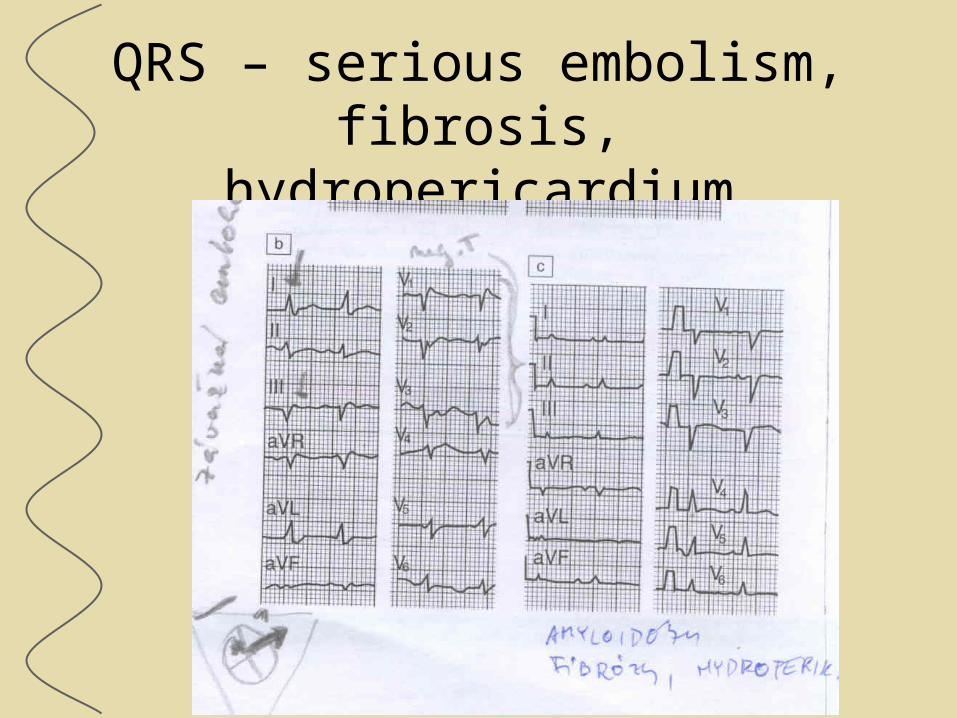
QRS – serious embolism, fibrosis, hydropericardium
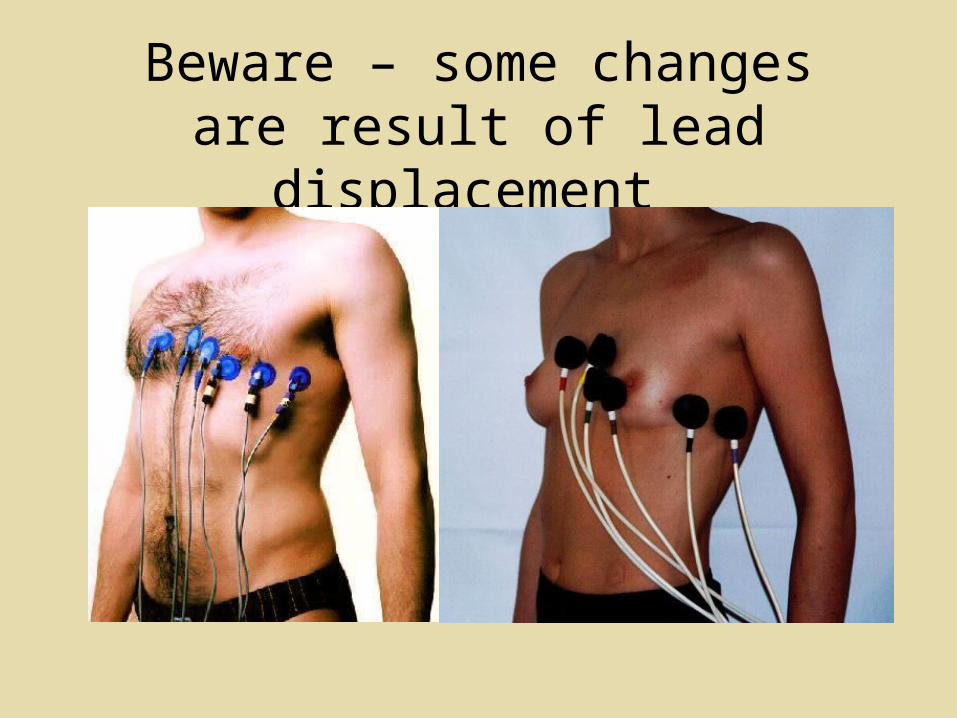
Beware – some changes are result of lead displacement






![é éC · ; " " 5 " " kej g jcbgj c? gg g g j ec cc]" g b pc xu sk!vco "jjc ccnmnl x "e c gc l g gpc! g" gc, pcx q !cjxg"l ~|} ~|} ~|} ~| ~| c k c ," gcbg g x g c g c](https://img.pdfslide.us/doc/110x75/5f056f827e708231d412f3ad/-c-5-kej-g-jcbgj-c-gg-g-g-j-ec-cc-g-b.jpg)