-
DYSTOCIA
-
L.D.27 y/omarriedJehovas witnessTandang Sora, Quezon CityMarch
1, 2010
CC: for induction of labor
-
HPIPatient is G2P1 (0-0-1-0) at 40 4/7 wks AOG
2 weeks PTA occasional uterine contractions no bloody/watery
vaginal discharge good fetal movement went for prenatal checkup IE:
done showed 1 cm cervical dilatation, posterior cervix, 30%
effaced, floating, (+)BOW observation and follow up
Few hours same symptoms prenatal checkup done showed same IE
advised admission for induction of labor
-
OBSTETRICAL HISTORY
LMP: May 21, 2009AOG: 40 4/7EDD: Feb 28, 2009G2P1 (0-0-1-0) G1:
D&C, 2008, blighted ovum, 8 weeks AOG, TMC G2: present
pregnancyPrenatal check-ups: >10 with OBScreening done:
Hepatitis: nonreactive OGCT: normal
-
Past Medical History(-) DM(-) HPN(-) Asthma(-) Allergies(-)
Previous Surgeries
-
Family History
(-) HPN/DM(-) Asthma(-) CA
-
Personal and Social History
Non-smokerNonalcoholic beverage drinkerDenies use of illicit
drugs
-
ROS(-) anorexia, weight change, weakness, fever, sweats(-)
shortness of breath, cough, hemoptysis(-)chest pain, easy
fatigability, dypsnea, palpitations, tremors(-)nausea, retching,
vomiting, diarrhea, food intolerance, flatulence, abdominal
distension, constipation(-) anxiety, depression
-
Physical ExaminationConscious, coherent, ambulatory, not in
cardiorespiratory distressBP 130/80 PR 68 RR 20 T36.8CHt 53 Wt 66.8
kgsWarm, moist skin, no active dermatosesPink palpebral
conjunctiva, anicteric scleraSymmetrical chest expansion, clear
breath sounds, no crackles or wheezesAdynamic precordium,regular
rate and rhythm, no murmurs
-
Physical ExaminationAbdomen: FH 34 cm FHT: 140 bpm Leopolds
Maneuver: LM1- breech LM2- fetal back, maternal left LM3- cephalic
LM4- not engagedPelvic exam:IE: Cervix 2cm, 50% effaced, floating,
(+) BOWClinical pelvimetry: sacral promontory not accessible,
slightly prominent ischial spines, pelvic side walls not
convergent, sacrum curve
Pulses full & equal, no cyanosis, no edema
-
Admitting CTGReactive, baseline FHR 140s, many accelerations, no
decelerations, no contractions, many fetal movements
-
Assessment
Pregnancy uterine 40 4/7 weeks AOG, cephalic in beginning labor;
G2P0 (0-0-1-0)
-
Lab exams
CBCHgb113Hct0.34Rbc3.74Wbc11.1Platelets348Neutrophils79Lymphocytes13Monocytes08
URINALYSISRbcnegativeproteinnegativesugarnegativewbc3epithelial1cast0bacteria44
-
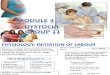
Patient was admitted to LR (1 PM)NPOIVF: D5NR 1L x 8 hoursHNBB
1amp/IV q4 VS: BP 110-130/70-80, HR 68-88, T 36.5FHT: 140-160
bpmIE: 1cm, 50%, station -3, +BOW
-
10
9
8
7
6
5
4
3
2
1
0cm
-5
-4
-3
-2
-1
0
+1
+2
+3
+4
+5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 StationCervical dilatationNo.
of Hours
-
4th hour (5pm)Contractions every 4-5mins, moderate, lasting 50
secondsVS: stableIE: 2cm, 60%, station -3, (+)BOW
-
10
9
8
7
6
5
4
3
2
1
0cm
-5
-4
-3
-2
-1
0
+1
+2
+3
+4
+5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 StationCervical
dilatationNo. of Hours
-
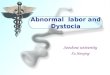
6th hour (7pm): D5NR 1L +10 u oxytocin started at 8
gtts/minUterine contractions every 4-5mins, moderate to strong
lasting 50 secondsVS: stableFHT: 150-160IE: 3 cm, 60%, station -3,
+BOW
-
10
9
8
7
6
5
4
3
2
1
0cm
-5
-4
-3
-2
-1
0
+1
+2
+3
+4
+5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 StationCervical
dilatationNo. of Hours
-
7th hour (8pm)IE: 4cm, 70% station -3, +BOWD5NR 1L +10 u
oxytocin increased at 10 gtts/minVS: stableUterine contractions
every 3 minutes, moderate to strong lasting 50 secondsFHT:
150-160
-
10
9
8
7
6
5
4
3
2
1
0cm
-5
-4
-3
-2
-1
0
+1
+2
+3
+4
+5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 StationCervical
dilatationNo. of Hours
-
8th hour (9pm)AROM was done: clear amniotic fluidIE: 4cm, 70%
station -3, +BOW
-
10
9
8
7
6
5
4
3
2
1
0cm
-5
-4
-3
-2
-1
0
+1
+2
+3
+4
+5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 StationCervical
dilatationNo. of Hours
-
10th hour (11pm)Contractions every 2-3 minutes, strong lasting
for 60 secondsFHT : 127-150 bpmIE: 5cm, 70% -3, -BOW
-
10
9
8
7
6
5
4
3
2
1
0cm
-5
-4
-3
-2
-1
0
+1
+2
+3
+4
+5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 StationCervical
dilatationNo. of Hours
-
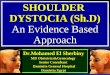
12th hour (1am)CEA inductedContractions every 2-3 minutes,
strong lasting for 60 secondsFHT: 127-144IE: 5cm, 70%, -2, -BOW
-
10
9
8
7
6
5
4
3
2
1
0cm
-5
-4
-3
-2
-1
0
+1
+2
+3
+4
+5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 StationCervical
dilatationNo. of Hours
-
13th hour (2am)Contractions every 2-3 minutes, strong lasting
for 60 secondsIE: 5cm, 70%, -2, -BOWCTG: baseline 140s, many
accelerations, (+) variable decelerations, contractions every 2-3
mins strong, many fetal movements
-
10
9
8
7
6
5
4
3
2
1
0cm
-5
-4
-3
-2
-1
0
+1
+2
+3
+4
+5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 StationCervical
dilatationNo. of Hours
-
Manner of Delivery:Stat Primary Low Transverse Cesarean Section
for Arrest of Cervical Dilatation for 3hours
-
MOTHERBABY
ConditionawakePostpartum VSstableUteruscontractedEBL
-
ACTIVITYDATETIMEOnset of laborMarch 1, 20101 pmOxytocin
dripMarch 1, 20107pmRuptured BOWMarch 2, 20109 pmFull Cervical
dilatation-----------Baby deliveredMarch 2, 20102:40 amPlacenta
deliveredMarcj 2, 20102:42am
-
DYSTOCIAdifficult laborcephalopelvic disproportion/failure to
progressmost common current indication for primary cesarean
delivery
-
DYSTOCIAArises from distinct abnormalities: Power- expulsive
forces, uterine contractility and maternal effort Passage- maternal
pelvisPassenger- presentation, position, devt of fetusPain
-
POWER:
Fundal dominanceLower limit of contraction pressure: 15 mmHg 200
montevideo units
-
POWER: Abnormalities of the expulsive forces2 types of uterine
dysfunction:1. Hypotonic uterine dysfunction: - no basal
hypertonus, synchronous pattern but pressure is insufficient2.
Hypertonic uterine dysfunction: -more force in the midsegment than
the fundus -incoordinate, complete asynchronism of impulses
-
CAUSES OF UTERINE DYSFUNCTION:Epidural
anesthesiaChorioamnionitisMaternal position
-
Abnormalities of Power:
Active phase disorders
Second stage disorders
-
Active-phase disordersProtraction disorder- slower than
normalArrest disorder- complete cessation
Both criteria should be met: Cervix is dilated 4cm or more
Uterine contraction pattern of 200 Montevideo units or more in a 10
minute period for 2 hours without cervical change
-
LABOR PATTERNPRIMIPARAMULTIPARATREATMENTEXCEPTIONAL
TREATMENTLatent PhaseProlonged Latent Phase>20 hours>14
hoursBed restOxytocin or CS if there is an urgent
problemProtraction DisordersActive Phase2 hoursArrest of
descent>1 hour>1 hourFailure to descendStill no descent after
deceleration phase or second stage of labor
-
76543210 3 6 9 12 15 18 21 24 27
-5-4-3-2-10+1+2+3+4+51098PROLONGED LATENT PHASE
-
76543210 1 2 3 4 5 6 7 8 9 10
-5-4-3-2-10+1+2+3+4+51098PROTRACTED ACTIVE PHASE OF DILATATION
-
76543210 1 2 3 4 5 6 7 8 9 10
-5-4-3-2-10+1+2+3+4+51098PROTRACTED DESCENT
-
76543210 1 2 3 4 5 6 7 8 9 10 -5-4-3-2-10+1+2+3+4+51098PROLONGED
DECELERATION PHASE
-
76543210 1 2 3 4 5 6 7 8 9 10 -5-4-3-2-10+1+2+3+4+51098ARREST IN
CERVICAL DILATATION
-
76543210 1 2 3 4 5 6 7 8 9 10 -5-4-3-2-10+1+2+3+4+51098ARREST OF
DESCENT
-
76543210 1 2 3 4 5 6 7 8 9 10 -5-4-3-2-10+1+2+3+4+51098FAILURE
OF DESCENT
-
Complications of DYSTOCIAMaternal complications: intrapartum
chorioamnionitis, postpartum pelvic infections, hemorrhage, uterine
rupture, fistula formations, pelvic floor injury, postpartum lower
extremity nerve injury Perinatal complications: infection,
mechanical injuries (caput succedaneum, molding, cephalohematoma,
skull fracture)
-
THANK YOU
**********IE was 1cm dilatation, 50% effaced*IE was 2 cm, 60% ,
-3*3cm, 60%, -3 intact BOw***5cm, 70%, -3**5cm 70% -2*5cm,
70%,-2*When a woman experiences emotional stress in labor, the
catecholamines in her body rise. The excessive level of
catecholamines in her body will reduce circulation to the placenta
and the uterus during labor which will cause ineffective
contractions to take place. If ineffective contractions become the
consistent labor pattern, an induction may become necessary,
therefore increasing the chance of a cesarean.*The purpose of the
partogram is: (1) To prevent obstructed labour and ruptured uterus
(which cause 70% of maternal deaths in some areas) by enabling
peripheral health workers to monitor labour, so as to detect
deviations from the normal more effectively, and thus to refer
mothers at the optimum momentbefore it is too late. This is the
purpose of the alert line. Ideally, the partogram should only be
used to monitor those labours which are expected to be normal;
mothers with risk factors should have already been referred. (2) To
monitor all labours in hospital, so that you know when to
intervene. This is the purpose of the action line. If the progress
line of a mothers cervical dilatation moves to the right of the
alert line, be extra vigilant. If she reaches the action line you
must do something, if you have not already done it (see below).The
partogram depends on the principles that: (1) The latent phase of
labour should not last longer than 8 hours, hence the thick
vertical line at this point. (2) The latent phase ends and the
active phase starts when her cervix is 3 cm dilated (4 cm is
sometimes used). (3) During the active phase her cervix should
dilate at not less than 1 cm per hour. (4) A lag time of 4 hours is
usually acceptable between the slowing of labour and the need to
intervene; this is the distance between the alert and the action
lines. The WHO partogram uses fixed alert and action lines and
transfers her to the alert line as soon as she reaches 3 cm, as has
been done for Mother C, in Fig. 18-2a.Dilatation of the cervix and
its relation to the action line is only one of the factors
measuring the progress of labour, and the necessity to intervene.
It and the descent of the babys head are the only two factors
plotted on the cervicograph. Although they are the most useful and
the most easily plotted ones, there are others which determine what
you should do and when you should do it, they include: his
presentation, his moulding score, his condition (fetal distress),
his mothers condition, and the strength and frequency of her
contractions. Consider all these factors, and dont be guided only
by the dilatation of her cervix in relation to the action line and
by the descent of his head, critical though these are.*