Embed Size (px)
Citation preview

DyspnoeaRobert McConnell
Specialty Doctor
St Oswalds Hospice

Aims
• Definition
• Pathophysiology
• Assessment
• Management
• Sputum

• An unpleasant sensation of breathing
• The distressing awareness of the process of breathing
• American Thoracic Society - A subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity. The experience derives from interactions among multiple physiological, psychological, social, and environmental factors, and may induce secondary physiological and behavioural responses
• Whatever the patient describes it as

Prevalence
• COPD 90-95%
• Heart failure 88%
• Lung cancer 90%
• Advanced Malignancy (10-70%)
• End stage renal failure 60%

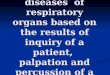
Pathophysiology
• Breathing Centre • Chemoreceptors • Mechanical receptors • Sensory Cortex• Motor Cortex

Breathing Centre

Sense of Tightness - Upper airway receptor- Pulmonary Receptors - Chest wall receptors
Air Hunger - Central
chemoreceptors- Peripheral chemoreceptors
Breathing Centre
Motor Cortex
Lung Disease
Sensory Cortex
Neuromechanical Dissociation
Breathlessness
Emotional Response

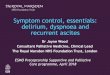
Anxiety
ANXIETY/ FEAR/
PANIC
INCREASED
ANXIETY
CATASTROPHIC
MISINTERPRETATION
DYSPNOEA

Total Breathlessness
PHYSICAL
TOTAL BREATHLESSNESS
PSYCHOLOGICAL SPIRITUAL
SOCIAL


Causes of Breathlessness
Direct Malignant Causes- Primary lung cancer
- Lung Metastases - Pleural Malignancy Non-Malignant Causes
- ILD, COPD, Heart failure, Pneumonina, Pneumonitis, Pulmonary oedema, Chest
wall deformity, Neuromuscular disease,
Anaemia, Anxiety
Indirect Malignant Causes- SVCO
- Pleural effusion - PE
- Ascites- Anaemia
- Airway obstruction - Lymphangitis
Carcinomatosis

Assessment
• Features • Timing
• Onset
• Precipitating factors
• Exacerbating factors
• Relieving factors
• Severity
• Associated symptoms• Cough • Pain • Wheeze• Stridor• Pain • Panic

Assessing Severity
• Impact • Disturbed sleep
• Interfere with normal conversation
• Affect ADLs
• Stairs?
• Does it stop you doing what you want to do?

Examination and Investigation
• Appropriate to • The patients wishes
• The stage of illness
• The likely benefit

Management
Non-PharmacologicalCorrect the correctable
Pharmacological

Management
Symptomatic drug treatment
Non-drug treatment
Correct the correctable
Prognosis months
to years
Prognosis weeks
to months
Prognosis days
to weeks

Case Study - Alan
• 55yr Man with Metastatic pancreatic cancer
• For best supportive care
• 6 weeks progressive breathlessness
• Worse with activity and when lying down
• O/e • Comfortable at rest, Sats 98% OA, Cachectic
• Reduced A/E Right LZ/MZ, Dull percussion

What to do?
• Drain • Therapeutic aspiration
• Chest drain
• Indwelling pleural catheter
Symptomatic drug treatment
Non-drug treatment
Correct the correctable
Prognosis months
to years
Prognosis weeks
to months
Prognosis days
to weeks

Correct the Correctable
• Infection
• PE
• Mass causing airway obstruction
• Diaphragm splinting (Ascites, Abdo mass, Obstruction)
• Anaemia
• Pulmonary Oedema
• Haemoptysis
• Respiratory Failure

Alan 8 weeks later…
• Admitted via A+E with increased SOB
• Increasing episodes of feeling breathless and “panicky”
• Unable to get up the stairs at home, needing help with washing and dressing
• Unable to get out the house due to anxiety about the breathlessness attacks
• Keen to avoid medications “Don’t want to be a
addicted”

What to do?
• Correct the correctable
• Non-Pharmacological management
• Pharmacological management
Symptomatic drug treatment
Non-drug treatment
Correct the correctable
Prognosis months
to years
Prognosis weeks
to months
Prognosis days
to weeks

Non-Pharmacological Management
• Fan
• Support/Education
• OT
• Physiotherapy
• Complimentary therapy
• Nutrition
• Breathing re-training
• Positional changes
• Pulmonary rehab

Breathing techniques
• Macmillan – Relax and breath CD and booklet
• Relaxed Breathing techniques
• “Blow as you go”
• Paced breathing
• Pursed lip breathing
• Square Breathing

Fans
• Simple, Cheap, Portable
• Stimulate upper airway mechanical receptors
• Effectiveness of fan is improved with proper explanation • 15-20cm from the face
• Directed at trigeminal area (Nose and mouth)
• Best used to prevent breathlessness attack
• More effective than oxygen!



Alan...
• 1 week later breathing has improved with fan and breathing techniques
• However still suffering with panicked episodes where he becomes acutely breathless
• “Is there anything else I can try? Would oxygen help?”

Oxygen
• Only in hypoxia
• No benefit over air in non-hypoxic ptnts
• LTOT/SBOT
• Problems • Dry mouth/nose
• Hypercapnic respiratory failure
• Fire risk
• Trip/Fall risk
• Reduction in mobility
• Skin damage
• Difficult discharge

Pharmacological – Opiates
• Largest evidence base for managing breathlessness
• Occasional episodic breathlessness – Shorting acting opiates PO/SC
• General/Recurrent breathlessness – Long acting opiate/CSCI
• Side effects • Constipation
• Drowsy
• Nausea
• Resp depression

Pharmacological – Benzo’s
• Lorazepam, Diazepam, Midazolam
• No benefit in relief of breathlessness
• However recommended in reducing anxiety associated with breathlessness
• Used at the end of life for ptnts
already on an opioid for pain
ANXIETY/ FEAR/
PANIC
INCREASED
ANXIETY
CATASTROPHIC
MISINTERPRETATION
DYSPNOEA

Sputum
THICKEN THEM
LOOSEN THEM
Hyoscine ButylbromideHyoscine Hydrobromide
GlycopironiumCarbocisteineSaline Nebs

Alan …
• Had continue to deteriorate over the next week
• Called urgently to review
• Having an episode of severe breathlessness
• Panicked, Gasping for breath, Blue discolouration of lips
• Terminal event

Symptomatic drug treatment
Non-drug treatment
Correct the correctable
Prognosis months
to years
Prognosis weeks
to months
Prognosis days
to weeks

Severe Frightening Breathlessness
• ABCDE…..Midaz
• Stay with patient, Reassurance
• Midazolam• 5mg S/c
• Repeated at 30min intervals
• Once calm Midazolam 20mg/24hrs CSCI with 5mg PRNs (15-30mins)
• In the community plan if possible • Discuss with - Family/Carers/Patient
• EHCP
• Anticipatory medications (?Buccal midazolam)

Air Hunger - Central
chemoreceptors- Peripheral chemoreceptors
Breathing Centre
Motor Cortex
Lung Disease
Sensory Cortex
Neuromechanical Dissociation
Breathlessness
Sense of Tightness - Upper airway receptor- Pulmonary Receptors - Chest wall receptors Emotional Response
Opiates
Benzos
Fan
Breathing
Opiates
Benzos
Benzos
Breathing

Summary
• Breathlessness is a complex, multifactorial and very common symptom in malignant and non-malignant illnesses
• Treat the treatable, Reverse the reversable and Cloak the untreatable and irreversible
• Non-pharmacological, Psychological and Pharmacological interventions carry different weighting at different stages of illness
• Oxygen only if hypoxic
• Try to plan and prepare for breathlessness (EHCP/Breathlessness plan)

Useful resources
• Cancer Research - Patient information re breathing positions and techniques
http://www.cancerresearchuk.org/about-cancer/lung-cancer/living-with/coping-with-breathlessness
• Macmillan – Patient information, Free Breathing CD
http://www.macmillan.org.uk/information-and-support/coping/side-effects-and-symptoms/breathlessness/tips-to-help-you-breathe-more-easily.html#5002
• Deciding Right – Info on EHCP and future planning
http://www.necn.nhs.uk/common-themes/deciding-right/resources/

Thankyou!




![Exertional dyspnoea in chronic heart failure: the role of the lung … · dyspnoea, even in this population, increases relatively linearly with exercise capacity [3]. Less data are](https://img.pdfslide.us/doc/110x75/5f77135db43c296df7390ec6/exertional-dyspnoea-in-chronic-heart-failure-the-role-of-the-lung-dyspnoea-even.jpg)

















![[Int. med] dyspnoea](https://img.pdfslide.us/doc/110x75/55ce4f2cbb61eb4d528b4758/int-med-dyspnoea.jpg)